Patient characteristics and stroke and bleeding events in nonvalvular atrial fibrillation patients treated with apixaban and vitamin K antagonists: a Spanish real-world study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the risk of stroke, systemic thromboembolism and bleeding, in patients initiating apixaban or acenocoumarol for the treatment of nonvalvular atrial fibrillation. Methods: An observational, retrospective study was performed using medical records of patients who initiated apixaban or acenocoumarol between 2015 and 2017. Propensity score matching was used to match patients; stroke, systemic thromboembolism, major and minor bleeding events were compared between the matched patients. Results: Patients who were prescribed apixaban had a lower rate of systemic embolism/stroke (hazard ratio [HR] = 0.54; 95% CI: 0.38–0.78; p = 0.001), minor bleeding (HR = 0.64; 95% CI: 0.52–0.79; p < 0.001) and major bleeding (HR = 0.51; 95% CI: 0.37–0.72; p < 0.001). Conclusion: Patients prescribed apixaban for the treatment of nonvalvular atrial fibrillation had lower rates of thromboembolic events and minor/major bleeding than patients on acenocoumarol.
Atrial fibrillation (AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation and ineffective atrial contraction [1]. The prevalence of AF was 0.05% in Spanish individuals aged 18–45 years in 2018 and 4.4% in the general Spanish population aged >40 years [2–4]. Patients with AF may have valvular heart disease or not. AF without valvular heart disease is known as nonvalvular atrial fibrillation (NVAF) [1,5].
NVAF has long been identified as a significant risk factor for disabling or fatal ischemic stroke and systemic embolism [1]. Specifically, NVAF is associated with a fivefold increase in stroke risk, which is considered as more severe than non-AF-associated stroke [6]. Prevention of systemic embolization, even after the first episode of AF, is the cornerstone of treatment. Anticoagulant treatments have been evaluated in clinical trials [6–9]. Anticoagulation with vitamin K antagonists (VKA), acenocoumarol and warfarin has demonstrated a reduction in the incidence of clinical stroke, with an acceptable risk of bleeding compared with aspirin, in patients with AF at moderate and high risk of thromboembolic events [1,7]. In patients with NVAF, novel oral anticoagulants (NOACs) have demonstrated a better risk–benefit profile than VKA in clinical trials [10]. Available NOACs include dabigatran, rivaroxaban, apixaban and edoxaban [11–15]. No head-to-head clinical trials have compared NOACs, although observational studies suggest differences in the risk–benefit profile between them [11].
Real-world studies have been performed in different populations to clarify whether clinical trial results are also observed in clinical practice [11,12,16–18]. To our knowledge, no real-world study has assessed this issue in a representative Spanish population. The aim of this study was to describe NVAF patients treated with apixaban compared with conventional VKA in terms of bleeding, stroke and systemic embolic events in daily clinical practice in Spain.
Material & methods
Design & study population
An observational, multicenter, retrospective longitudinal study was carried out through review of medical records (computerized databases, with dissociated data). The study population was obtained from the records of health providers from various primary and hospital centers in Spain (unified in the dissociated, anonymized BIG-PAC® database, 2017 Real Life Data) [19]. Data came from computerized medical records and other supplementary databases of financing/provision of public services from nine Spanish autonomous communities (2.9 million potential patients).
Study periods, inclusion & exclusion criteria
Patients who requested care and began new anticoagulant treatment with apixaban or VKA (acenocoumarol or warfarin) between 1 January 2015 and 31 December 2017 (inclusion period) for the treatment of NVAF were included. Date of treatment initiation in the inclusion period was the index date. Patients prescribed apixaban who had switched from VKA and vice versa were eligible for inclusion. In Spain, authorization for prescription of a NOAC is required before starting treatment.
Inclusion criteria were as follows: age ≥18 years; patients active in the database for ≥12 months before study initiation (baseline period); inclusion in the program of chronic prescriptions (with a record of the daily dose, the time interval and the duration of each treatment administered, and ≥2 prescriptions during the follow-up period); regular patient monitoring (≥2 health records in the computer system). Exclusion criteria were as follows: subjects being transferred to other centers, displaced or out of area; permanently institutionalized patients; a history of transient AF (thyrotoxicosis, pericarditis), heart surgery, venous thromboembolism, hip or knee surgery in the previous 6 weeks, valvular heart disease and/or pregnancy; subjects with valvular AF (with prosthetic valves); and end-stage renal disease, dialysis or kidney transplant. Patients who started treatment with VKA and were switched to a NOAC other than apixaban during the follow-up period were also excluded. Depending on the analysis, patients were followed from index date until death, treatment interruption, the end of the study period (31 December 2018), 12 months or an event the first (stroke, thromboembolism or major/minor bleeding), whichever occurred first. Patients were classified into two cohorts depending on treatment initiated in inclusion period: apixaban and VKA.
Definition of diagnosis, demographic variables & comorbidities
Patients with a diagnosis of AF (International Classification of Disease, 9th Revision, Clinical Modification [ICD-9-CM]: 427.31) with no valvular heart disease (ICD-9-CM: 394.x, 396.0, 396.1, 396.8, 396.9, 424.0, 745.x, V42.2, V43.3) prior to the index date were included (Table 1). The sociodemographic and comorbidity variables collected are detailed in Table 3. The Charlson Comorbidity Index [20] was used as a summary variable of general comorbidity. These variables were obtained at baseline. For each patient, the CHA2DS2 -VASc and HAS-BLED [10] scores were obtained at baseline. The operational definition of these scales in this dataset is detailed in Supplementary Table 1.
| Outcomes/others | ICD-9-CM codes |
|---|---|
| Stroke or systemic embolism | |
| Ischemic stroke, TIA | 433.x1, 434.x1, 436, 435.x |
| Systemic embolism | 444.x, 445.x |
| Minor bleeding | |
| Other sites | 285.1, 360.43, 362.43, 362.81, 363.61, 363.62, 363.72, 364.41, 372.72, 374.81, 376.32, 377.42, 379.23, 423.0x, 719.1x, 782.7, 784.7, 784.8, 786.3x, 958.2, 997.02, 998.11, 99.04 |
| Genito-urinary | 596.7x, 599.7x, 602.1x, 620.1, 621.4, 626.2, 626.5, 626.7, 626.8, 626.9 |
| Major bleeding | |
| Intracranial bleeding, hemorrhagic stroke | 430, 431, 432.x, 852.x, 853.x |
| Gastrointestinal bleeding | 456.0, 456.20, 530.21, 530.7, 530.82, 531.0x, 531.2x, 531.4x, 531.6x, 532.0x, 532.2x, 532.4x, 532.6x, 533.0x, 533.2x, 533.4x, 533.6x, 534.0x, 534.2x, 534.4x, 534.6x, 535.01, 535.11, 535.21, 535.31, 535.41, 535.51, 535.61, 535.71, 537.83, 537.84, 562.02, 562.03, 562.12, 562.13, 568.81, 569.3, 569.85, 578.x |
| Bleeding from other sites | 423.0, 459.0, 596.7, 599.71, 719.1x, 784.8, 786.3 |
| Others | |
| Atrial fibrillation | 427.31 |
| Valvular heart disease | 394.x, 396.0, 396.1, 396.8, 396.9, 424.0, 745.x, V42.2, V43.3 |
ICD-9-CM: International Classification of Disease, 9th Revision, Clinical Modification; TIA: Transient ischemic attack.
Medication administered & treatment persistence/duration
Data were obtained from records of the pharmacological dispensation of medicines. The choice of medication for a specific patient was at the physician’s discretion (clinical practice). Drugs were coded according to the Anatomical Therapeutic Chemical Classification System [21]: VKA (B01AA) and NOAC (apixaban, B01AF02), anticoagulant treatment (B01A) including heparin (B01AB) and platelet aggregation inhibitors (B01AC). The time from diagnosis of NVAF until the first prescription and the doses prescribed in the record of the first prescription issued were also collected.
Treatment persistence or duration was calculated from the start date until the discontinuation date (in days). The start date was the start of treatment (apixaban or acenocoumarol/warfarin), and the discontinuation date was the first between: the end date of the follow-up period (1 year), death, switch to an antiplatelet/anticoagulant treatment other than the inclusion medication and medication interruption/abandonment (≥60 days without renewing the medication). Treatment persistence was assessed at 6 and 12 months of follow-up. The date of interruption was 30 days from the last prescription end date.
Outcomes: effectiveness/safety
Clinical effectiveness was assessed according to episodes of ischemic stroke and systemic thromboembolism and safety according to major and minor bleeding. Major bleeding included intracranial, gastrointestinal and other sites (liver, ocular, splenic) and was defined as bleeding that required hospital admission for acute or subacute clinically manifest bleeding. These events were identified from 30 days after the initiation of anticoagulant medication (until the date of treatment discontinuation). Episodes were obtained using the ICD-9-CM codes shown in Table 1.
Confidentiality of information/ethical aspects
The confidentiality of records (anonymous and dissociated) was respected according to the Law of Protection of Personal Data, Regulation (EU) 2016/679 of the European Parliament and the Council of 27 April 2016 on Data Protection and Organic Law 3/2018, of 5th December, on the Protection of Personal Data and Guarantee of Digital Rights. The study was classified by the Spanish Agency for Medicines and Health Products (EPA-OD) and approved by the Research Ethics Committee of the Hospital de Terrassa (Barcelona).
Statistical analysis
Data were subject to exploratory analysis and preparation, inspecting the frequency distributions and searching for possible registration or coding errors in the data sources and the BIG-PAC database to guarantee data quality. A descriptive-univariate analysis was carried out. Categorical data were described using absolute and relative frequencies and continuous data using means, standard deviation, medians and percentiles 25 and 75 of the distribution (interquartile range). The 95% CI for the estimate of parameters were based on the total number of subjects with nonmissing values. The normality of distributions was checked using the Kolmogorov–Smirnov test. Propensity score matching (PSM) was used to pair patients (apixaban/VKA) on baseline variables that were significantly different between groups (analyzed age, gender, Charlson index [20], CHA2DS2 -VASc [10] score and HAS-BLED score [10]). There was no multicollinearity between these variables. The tolerance of the model (PSM) was 1, with sampling with substitution and giving priority to exact matches (randomly). To measure treatment persistence/duration, a Kaplan–Meier survival analysis was performed, testing for differences using log-rank tests. Cox proportional hazards regression was used to compare events occurring during follow-up (hazard ratio [HR], with censored data). The rate of events of interest were expressed as percentages, equivalent to a rate per 100 persons–year (incidence rate, accumulated risk). The data were censored in the absence of the event. Characteristics were compared between matched apixaban and warfarin patients using standardized differences. The analysis was made using SPSSWIN, version 23 software. Statistical significance was set at p < 0.05.
Results
Of the initial population of 2.9 million, 65,327 received anticoagulant treatment between 1 January 2015 and 31 December 2017 and, of these, 45,794 were diagnosed with AF. In total, 32,925 patients met the inclusion/exclusion criteria and could be followed during the study period (apixaban: N = 2160 vs acenocoumarol/warfarin: N = 30,765). Table 2 shows the general characteristics of these patients overall showing significant differences. PSM yielded 2160 patients paired in each group (Figure 1). No patient was paired with warfarin, since it only accounted for 5.8% of the total VKA population.
| Study groups | Apixaban | Acenocoumarol/warfarin | p-value |
|---|---|---|---|
| Number of patients | N = 2160 | N = 30,765 | |
| Sociodemographic characteristics | |||
| Mean age (SD), years | 71.2 (12.8) | 73.8 (13.1) | <0.001 |
| Gender (male) | 47.6% | 50.2% | <0.001 |
| General comorbidity | |||
| Mean number of diagnoses (SD) | 10.1 (6.3) | 12.1 (6.7) | <0.001 |
| Charlson index (SD) | 2.5 (2.0) | 2.8 (2.2) | <0.001 |
| Scales | |||
| CHA2-DS2-VASc | 3.3 (1.9) | 3.8 (1.9) | <0.001 |
| HAS-BLED | 2.0 (1.3) | 2.5 (1.1) | <0.001 |
N = 32,925. Values expressed as a percentage or mean. p-value represents the statistical significance.
SD: standard deviation.

Figure 1. Study flow diagram.
A retrospective observational study was carried out based on review of medical records (computerized databases with anonymized and dissociated data) of patients diagnosed with non-valvular atrial fibrillation prescribed apixaban and acenocoumarol/warfarin.
NOAC: Novel oral anticoagulant.
Table 3 shows general patient characteristics according to the matched study groups. The mean age was 71.4 years and 47.7% were male. High blood pressure, dyslipidemia and diabetes were the most frequent comorbidities. There was a high degree of comparability between the matched apixaban and acenocoumarol groups: Charlson index (2.5 vs 2.6; p = 0.758), CHA2DS2 -VASc (3.3 vs 3.4; p = 0.148) and HAS-BLED (2.0 vs 2.1; p = 0.221).
| Study groups, PSM | Apixaban | Acenocoumarol | p-value | Standardized difference |
|---|---|---|---|---|
| Number of patients | N = 2160 | N = 2160 | ||
| Sociodemographic characteristics | ||||
| Mean age (SD), years | 71.2 (12.8) | 71.6 (10.1) | 0.271 | -0.041 |
| Ranges: 40–64 years | 20.2% | 21.6% | 0.552 | -0.014 |
| 65–74 years | 38.6% | 37.8% | 0.391 | 0.009 |
| ≥75 years | 41.2% | 40.6% | 0.475 | 0.005 |
| Gender (male) | 47.6% | 47.8% | 0.903 | -0.003 |
| General comorbidity | ||||
| Mean number of diagnoses (SD) | 10.1 (6.3) | 10.4 (5.3) | 0.163 | 0.024 |
| Charlson Index (SD) | 2.5 (2.0) | 2.6 (1.9) | 0.758 | 0.016 |
| – 0 | 15.5% | 15.1% | 0.874 | 0.010 |
| – 1 | 24.1% | 24.2% | 0.557 | -0.003 |
| – 2 | 38.3% | 38.5% | 0.673 | -0.007 |
| – 3+ | 22.1% | 22.2% | 0.675 | -0.002 |
| Associated comorbidities | ||||
| Arterial hypertension | 70.9% | 71.1% | 0.893 | -0.021 |
| Mellitus diabetes | 31.7% | 30.6% | 0.430 | 0.012 |
| Dyslipidemia | 45.0% | 45.6% | 0.714 | -0.006 |
| Obesity | 22.8% | 22.2% | 0.662 | 0.007 |
| Active smoking | 6.5% | 5.2% | 0.080 | 0.028 |
| Alcohol ingestion | 2.6% | 2.8% | 0.707 | -0.006 |
| Ischemic heart disease | 23.0% | 22.2% | 0.560 | 0.009 |
| Cerebrovascular accident | 14.8% | 15.2% | 0.733 | -0.005 |
| Heart failure | 20.2% | 19.8% | 0.761 | 0.004 |
| Renal failure | 10.9% | 10.7% | 0.845 | 0.013 |
| Asthma | 8.9% | 8.8% | 0.998 | 0.017 |
| COPD | 15.0% | 15.2% | 0.865 | -0.023 |
| Depressive syndrome | 13.7% | 13.3% | 0.722 | 0.025 |
| Malignant neoplasms | 10.7% | 10.4% | 0.692 | 0.006 |
| Liver decompensation | 5.0% | 5.2% | 0.782 | -0.014 |
| Previous bleeding | 14.6% | 14.5% | 0.887 | 0.058 |
| Anemia | 10.3% | 9.7% | 0.222 | 0.022 |
| Scales | ||||
| CHA2-DS2-VASc | 3.3 (1.9) | 3.4 (1.7) | 0.148 | -0.015 |
| HAS-BLED | 2.0 (1.3) | 2.1 (1.1) | 0.221 | -0.017 |
Values expressed as a percentage or mean. p-value represets the statistical significance.
COPD: Chronic obstructive pulmonary disease; PSM: Propensity score matched; SD: Standard deviation.
The medication administered and treatment persistence by study groups is shown in Table 4. Totally, 28.2% of patients who began treatment with apixaban had previously received acenocoumarol and 71.8% were ‘de novo.’ Totally, 77.5% of apixaban patients initiated a dose of 10 mg/day. The mean dose/day of acenocoumarol users was 3.4 mg/day. There were no significant differences in the use of concomitant medication between apixaban and acenocoumarol patients: platelet aggregation inhibitors (13.2 vs 11.3%; p = 0.065) and nonsteroidal anti-inflammatory drugs (9.5 vs 10.1%; p = 0.284). Treatment persistence with apixaban was 71.1% compared with 60.6% with acenocoumarol at 12 months of follow-up (p < 0.001). The hazard ratio (HR) of apixaban relative to acenocoumarol was 1.3 (1.1–1.4), p = 0.012. Figure 2 shows the Kaplan–Meier curves of treatment persistence. Of the patients who discontinued treatment with apixaban, 11.3% changed to a platelet aggregation inhibitor and 6.5% to heparin. In contrast, 17.2% of patients on acenocoumarol changed to another NOAC.
| Study groups, PSM | Apixaban | Acenocoumarol | p-value |
|---|---|---|---|
| Number of patients | N = 2160 | N = 2160 | |
| Time since diagnosis, years | |||
| – Mean (SD) | 0.9 (1.4) | 0.9 (1.5) | 0.611 |
| – Median (P25–P75) | 0.1 (0.0–1.8) | 0.1 (0.0–1.9) | |
| BMI, kg/m2 | |||
| – Mean (SD) | 27.7 (3.2) | 27.9 (4) | 0.189 |
| – Median (P25–P75) | 27.3 (26.3–28.4) | 27.2 (26.0–28.4) | |
| Previous use of antithrombotic medication | |||
| – Acenocoumarol initial | 28.2% | 100.0% | <0.001 |
| – Apixaban | 71.8% | 0.0% | <0.001 |
| Daily dose | |||
| – 5 mg | 22.5% | – | |
| – 10 mg | 77.5% | – | |
| – Mean (SD) | 8.6 (2.2) | 3.4 (0.7) | <0.001 |
| – Median (P25–P75) | 10.0 (5.0–10.0) | 3.0 (2.8–4.0) | |
| Weekly dose | |||
| – Mean (SD) | 60.2 (2.2) | 22.3 (4.3) | <0.001 |
| – Median (P25–P75) | 10.0 (5.0–10.0) | 20.0 (18.0–22.0) | |
| Use of concomitant medication | |||
| – Antiplatelet | 13.2% | 11.3% | 0.065 |
| Nonsteroidal anti-inflammatory drugs | 9.5% | 10.1% | 0.284 |
| Treatment duration, days | |||
| – Mean (SD) | 300.3 (104.0) | 266.4 (121.1) | <0.001 |
| – Median (P25–P75) | 330 (216–365) | 304 (136–365) | |
| – Not treatment persistent at 1 year | 28.9% | 39.4% | <0.001 |
| – Treatment abandonment | 5.6% | 5.2% | 0.570 |
| – Dose reduction | 2.2% | 7.2% | <0.001 |
| – Switch to heparin | 6.5% | 5.5% | 0.421 |
| – Switch to antiplatelet | 11.3% | 4.3% | <0.001 |
| – Switch to other NOAC | 3.3% | 17.2% | <0.001 |
| Treatment persistence | |||
| – 6 months | 79.8% | 70.4% | <0.001 |
| – Hazard ratio (95% CI) | 1.2 (1.0–1.3) | 0.006 | |
| – 12 months | 71.1% | 60.6% | <0.001 |
| – Hazard ratio (95% CI) | 1.3 (1.1–1.4) | 0.012 | |
†Cox proportional hazards regression.
Values expressed as a percentage or mean. Reference medicine: apixaban. p-value represents the statistical significance as a percentile.
PSM: Propensity score matched; SD: Standard deviation.
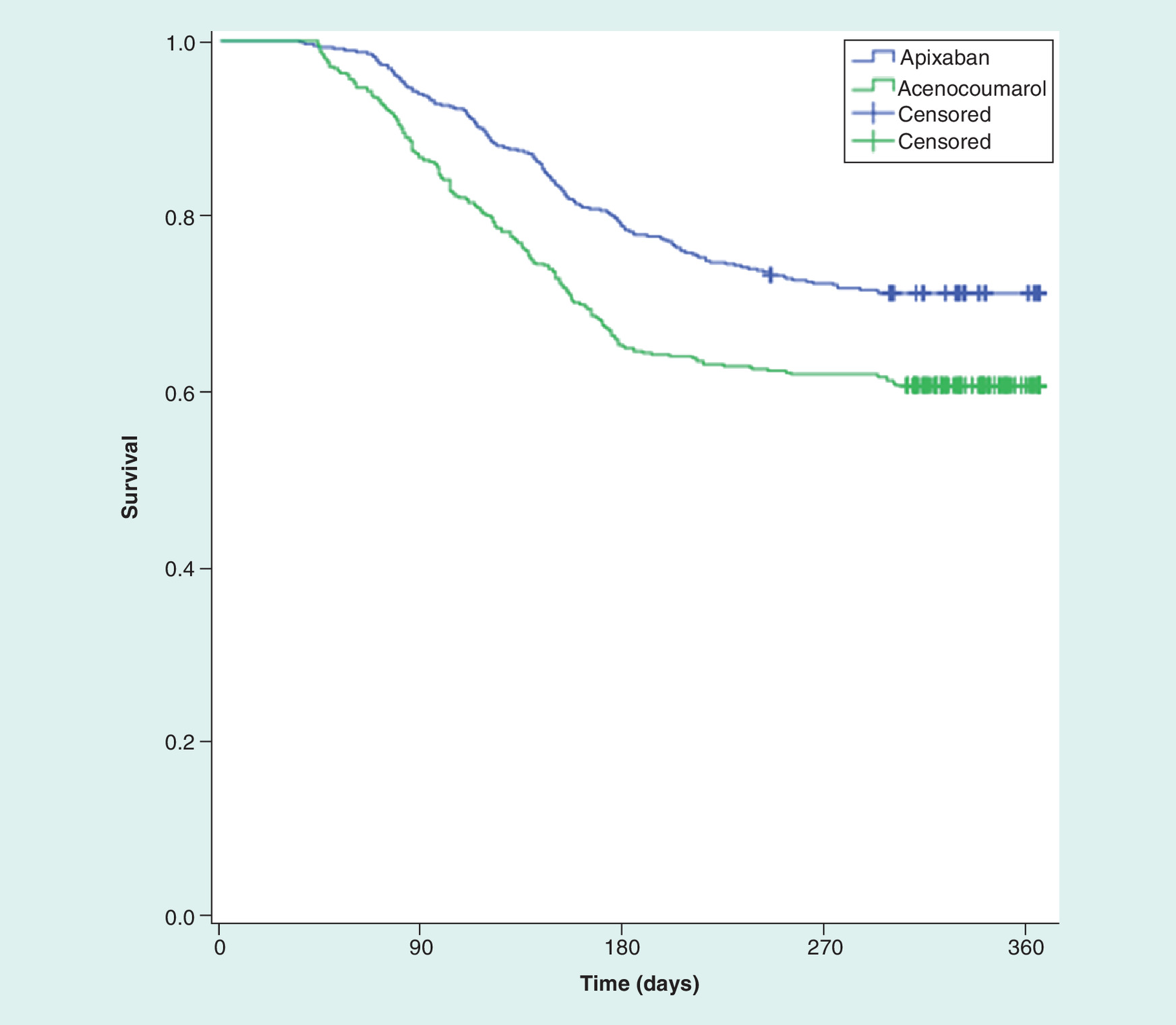
Figure 2. Kaplan–Meier curves of treatment persistence at 12 months of follow-up by study groups.
Kaplan–Meier curves: Log Rank procedure (Mantel–Cox). Pairwise comparison: Chi-square = 65.858, p < 0.001. Treatment persistence: apixaban 71.1% vs acenocoumarol 60.6%.
Table 5 shows strokes/embolisms and minor/major bleeding, during the follow-up by study groups. Patients prescribed apixaban had a lower rate of events compared with acenocoumarol, both in systemic embolism and stroke (2.0 vs 3.7%; HR = 0.54; p = 0.001), minor bleeding (7.2 vs 10.9%; HR = 0.64; p < 0.001) and major bleeding (2.4 vs 4.6%; HR = 0.51; p < 0.001). Figures 3 & 4 show the Kaplan–Meier curves of embolic events (stroke or embolism), and major and minor bleeding at the end of the study in the two study groups. Patients who were prescribed apixaban de novo versus apixaban with previous acenocoumarol use showed a similar event rate: major bleeding, 2.3 vs 2.4% (p = 0.832); systemic embolism and stroke, 1.9 vs 2.0% (p = 0.811); apixaban de novo vs apixaban with previous acenocoumarol, respectively. Some of the characteristics of these patients (de novo) were: mean age 70.3 years, male 47.7%, Charlson index 2.3, CHA2DS2 -VASc 3.2 and HAS-BLED 2.1.
| Study groups, PSM | Percentage of events † | Hazard ratio (95% CI) ‡ | p-value | |
|---|---|---|---|---|
| Apixaban | Acenocoumarol | |||
| Stroke and systemic embolism | 2.0% | 3.7% | 0.54 (0.38–0.78) | 0.001 |
| N = 124; 44 vs 80 | ||||
| – Ischemic stroke | 1.4% | 2.8% | ||
| – Thromboembolism | 0.6% | 0.9% | ||
| Minor bleeding | 7.2% | 10.9% | 0.64 (0.52–0.79) | <0.001 |
| N = 392; 156 vs 236 | ||||
| – Genitourinary | 4.1% | 5.4% | ||
| – Other minor bleeding | 3.1% | 5.6% | ||
| Major bleeding | 2.4% | 4.6% | 0.51 (0.37–0.72) | <0.001 |
| N = 152; 52 vs 100 | ||||
| – Gastrointestinal | 1.7% | 3.2% | ||
| – Others | 0.1% | 0.5% | ||
| – Cerebral, hemorrhagic stroke | 0.6% | 0.9% | ||
†
Percentage of equivalent events per 100 person–years.
‡
Cox proportional hazards regression.
Reference medicine: apixaban. p-value represents the statistical significance.
PSM: Propensity score matched.
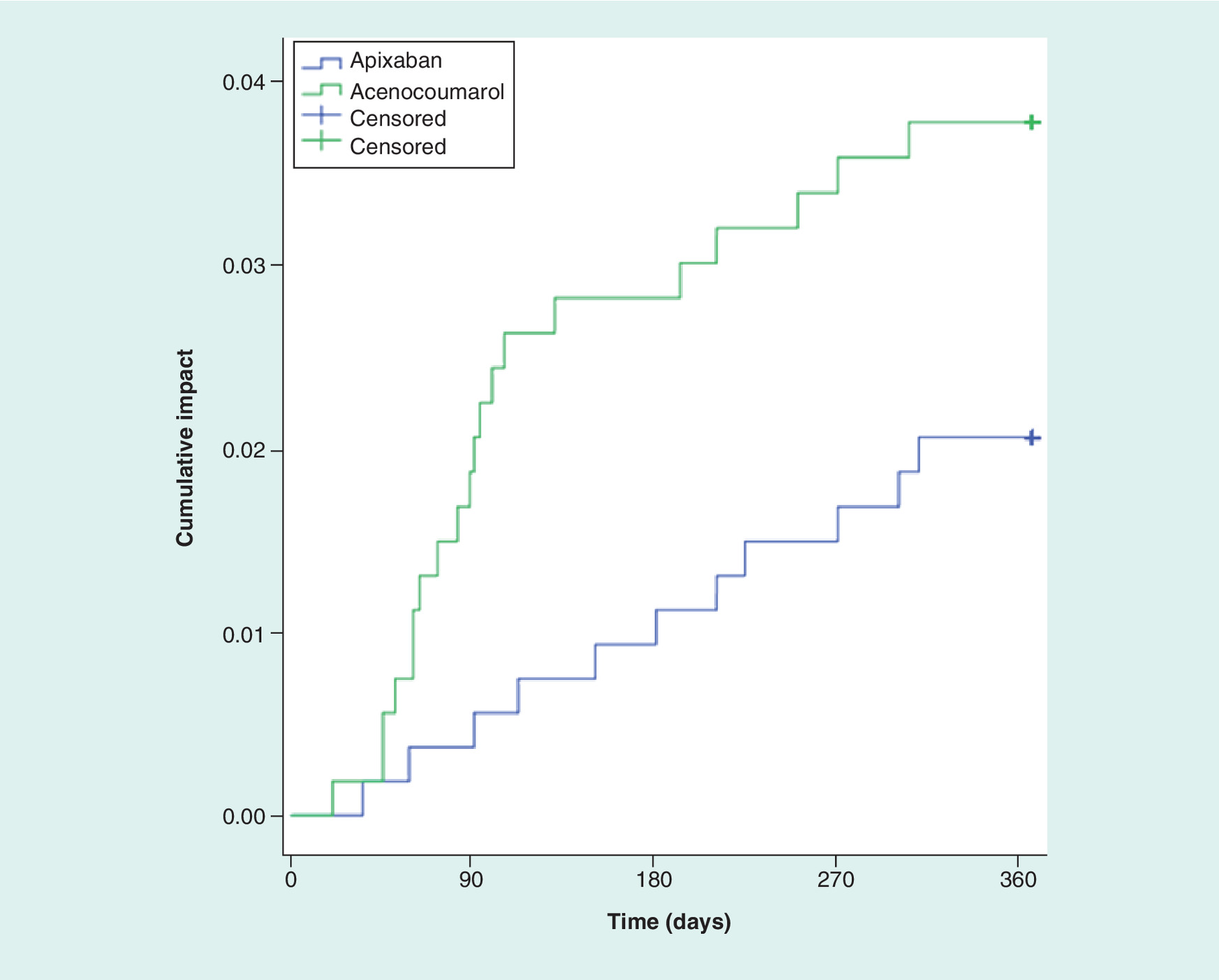
Figure 3. Kaplan–Meier curves (Log Rank procedure: Mantel–Cox) of embolic events (stroke/systemic embolism) at 12 months of follow-up by study groups.
Pairwise comparison: Chi-square = 10.937, p = 0.001.
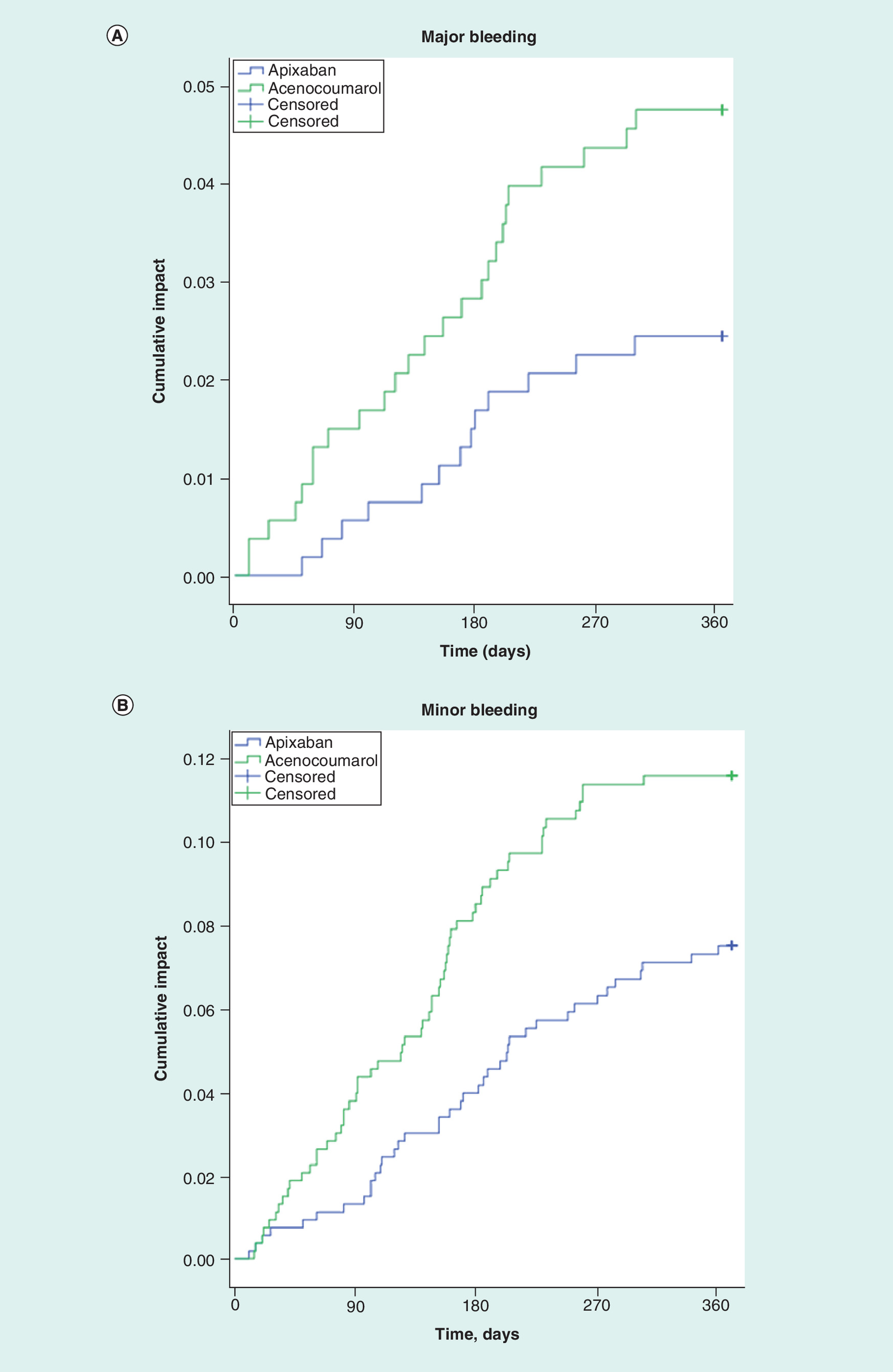
Figure 4. Kaplan–Meier curves (Log Rank procedure: Mantel–Cox) of major and minor bleeding at 12 months of follow-up by study groups.
Pairwise comparison (A) Chi-square = 15.793, p < 0.001. (B) Chi-square = 18.819; p < 0.001.
Discussion
This study found that patients who were prescribed apixaban for the treatment of NVAF had lower rates of thromboembolic events (clinical effectiveness) and minor/major bleeding (safety) than patients receiving acenocoumarol. The lack of Spanish real-life observational studies makes it difficult to compare the results but enhances the value of the present study [3,4,22,23]. The representativeness of the results is, likewise, enhanced by the inclusion of patients from various centers throughout Spain. Other studies carried out in routine clinical practice with a similar methodology to ours have found similar effectiveness and safety results [11,12,24–29]. In general, possible differences in the results could be related to differences in study populations, time periods and, especially, the number of patients included. These results in usual clinical practice are also consistent with those of randomized clinical trials [22].
Only 28.2% of patients who began treatment with apixaban had previously received acenocoumarol. This finding is similar to another Spanish study (23.2%) [22], but also may be due to an unexpected random effect or to the fact that, as it is a very recent study, there may be greater awareness by physicians of the benefits of apixaban, especially in complex chronic patients and elderly or polymedicated patients. Intracranial bleeding is considered the most prominent and potentially fatal complication in patients on oral anticoagulants [1,10]. As apixaban may have greater clinical benefits than acenocoumarol, this may have been accepted by physicians when selecting anticoagulant treatment [13–15]. Likewise, 77.5% of patients initiated apixaban at a dose of 10 mg/day, consistent with other studies [11,12].
The possible limitations of the study are those inherent to retrospective studies, such as under recording (missing data) or the possible intrinsic variations in physicians and patients due to the observational design, the methods of measurement used, the main study variables or possible classification/selection bias. Therefore, given the observational nature of the study, associations and not causal relationships can be identified. In this regard, the possible inaccuracy of the diagnostic coding of NVAF and the lack of some variables that could influence the final results (socioeconomic level, evolution of the prescribed pharmacological dose, concomitant medication, left ventricle ejection fraction values, renal filtration levels, etc.) should also be considered as limitations [30]. Using the ICD-9-CM codes did not allow differentiation of the type of permanent, persistent and/or paroxysmal AF, which may be considered a limitation of the database used. In addition, PSM minimizes potential bias between the variables analyzed, other, unmeasured factors, such as the use of aspirin, glucocorticoids, etc., either over the counter or by private prescription might have affected the between-group comparisons. We were unable to obtain data on the degree of anticoagulation control in patients on acenocoumarol (time in therapeutic range), an important factor given the relationship between this parameter and the efficacy/safety of this medication. However, the main limitation was indication bias by the attending physician at the initiation of treatment with apixaban or acenocoumarol, since, as usual in real-life situations, it was not random. Another limitation was that disaggregated results were not obtained from the study centers due to the high degree of confidentiality and anonymization of all study data; however, without this condition the study would not have been possible. In conclusion, patients prescribed apixaban for the treatment of NVAF had lower rates of thromboembolic events and minor/major bleeding than those receiving acenocoumarol, although further studies are required to validate our results.
•
Patients with atrial fibrillation (AF) have up to a fivefold increased risk of stroke.
•
Anticoagulation therapy is offered to patients for stroke prevention; however, these treatments can lead to an increased risk of bleeding.
•
Vitamin K antagonists (VKA) have up until recently been the main anticoagulation agent available. Recent advances in AF treatment have led to the availability of novel or direct oral anticoagulants, such as apixaban.
•
Given the availability of newer treatments, it is unclear how patients are currently treated in the ‘real-world’ in Spain.
•
In this investigation, we sought to describe AF patients receiving either VKAs or apixaban and to compare the risk of major bleeding and stroke in these groups of patients.
•
After controlling for differences in patient characteristics, the risk of major bleeding and stroke was significantly less in patients taking apixaban as compared with patients taking VKAs.
Author contributions
SV Ramagopalan and C Polanco-Sanchez conceived the study. The study was designed by A Sicras-Mainar and JF de Bobadilla. Data collection and statistical analysis was led by A Sicras-Mainar and the interpretation of the data, writing, review and approval of the submitted manuscript was undertaken by all authors.
Financial & competing interests disclosure
The study was sponsored by Bristol-Myers Squibb and Pfizer. S Ramagopalan, C Polanco-Sanchez and R Carroll are employees of Bristol-Myers Squibb. A Sicras is an independent consultant in relation to the development of this manuscript. J Fernández de Bobadilla is an independent author in relation to the development of this manuscript. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_data.docx)
- Download
- 20.11 KB
References
1.
January CT, Wann LS, Alpert JS et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 64, e1–e76 (2014).
2.
Rodríguez-Capitán J, Fernández-Meseguer A, Romero-González E, Calvo-Bonacho E, Gómez-Doblas JJ, De Teresa-Galván E. Frequency of atrial fibrillation in a large sample of young adults selected from the Spanish working population. Rev. Esp. Cardiol. (Engl. Ed.) 71, 498–500 (2018).
3.
Baena-Díez JM, Grau M, Forés R et al. Prevalence of atrial fibrillation and its associated factors in Spain: an analysis of 6 population-based studies. DARIOS Study. Rev. Clin. Esp. 214, 505–512 (2014).
4.
Gómez-Doblas JJ, Muñiz J, Martin JJ et al. Prevalence of atrial fibrillation in Spain. OFRECE study results. Rev. Esp. Cardiol. (Engl. Ed.) 67, 259–269 (2014).
5.
Anguita M, Dávalos A, López de Sá E et al. Novel oral anticoagulants in non-valvular atrial fibrillation: how to improve its management in Spain. Semergen 45, 109–116 (2019).
6.
Apenteng PN, Murray ET, Holder R, Hobbs FD, Fitzmaurice DA. An international longitudinal registry of patients with atrial fibrillation at risk of stroke (GARFIELD): the UK protocol. BMC Cardiovasc. Disord. 13, 31 (2013).
7.
Lip GY, Potpara T, Boriani G, Blomström-Lundqvist C. A tailored treatment strategy: a modern approach for stroke prevention in patients with atrial fibrillation. J. Intern. Med. 279, 467–476 (2016).
8.
Dzeshka MS, Lane DA, Lip GY. Stroke and bleeding risk in atrial fibrillation: navigating the alphabet soup of risk-score acronyms (CHADS2, CHA2 DS2 -VASc, R2 CHADS2, HAS-BLED, ATRIA, and more). Clin. Cardiol. 37, 634–644 (2014).
9.
Ruff CT, Giugliano RP, Braunwald E et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 383, 955–962 (2014).
10.
Kalra L, Lip GY. Guideline Development Group for the NICE clinical guideline for the management of atrial fibrillation. Heart 93, 39–44 (2007).
11.
Yao X, Abraham NS, Sangaralingham LR et al. Effectiveness and safety of dabigatran, rivaroxaban, and apixaban versus warfarin in nonvalvular atrial fibrillation. J. Am. Heart Assoc. 5, e003725 (2016).
12.
Lip GY, Keshishian A, Kamble S et al. Real-world comparison of major bleeding risk among non-valvular atrial fibrillation patients initiated on apixaban, dabigatran, rivaroxaban, or warfarin. A propensity score matched analysis. Thromb. Haemost. 116, 975–986 (2016).
13.
Hernandez I, Zhang Y, Saba S. Comparison of the effectiveness and safety of apixaban, dabigatran, rivaroxaban, and warfarin in newly diagnosed atrial fibrillation. Am. J. Cardiol. 120, 1813–1819 (2017).
14.
Martinez BK, Sood NA, Bunz TJ, Coleman CI. Effectiveness and safety of apixaban, dabigatran, and rivaroxaban versus warfarin in frail patients with nonvalvular atrial fibrillation. J. Am. Heart Assoc. 7, e008643 (2018).
15.
Tepper PG, Mardekian J, Masseria C et al. Real-world comparison of bleeding risks among non-valvular atrial fibrillation patients prescribed apixaban, dabigatran, or rivaroxaban. PLoS ONE 13, e0205989 (2018).
16.
Briere JB, Bowrin K, Coleman C et al. Real-world clinical evidence on rivaroxaban, dabigatran, and apixaban compared with vitamin K antagonists in patients with nonvalvular atrial fibrillation: a systematic literature review. Expert Rev. Pharmacoecon. Outcomes Res. 19, 27–36 (2019).
17.
Deitelzweig S, Lip GYH. Real-world clinical evidence on rivaroxaban, dabigatran, and apixaban compared with vitamin K antagonists in patients with non-valvular atrial fibrillation: a systematic literature review. Expert Rev. Pharmacoecon. Outcomes Res. 19, 243–244 (2019).
18.
Deitelzweig S, Farmer C, Luo X et al. Risk of major bleeding in patients with non-valvular atrial fibrillation treated with oral anticoagulants: a systematic review of real-world observational studies. Curr. Med. Res. Opin. 33, 1583–1594 (2017).
19.
Sicras-Mainar A, Sánchez-Álvarez L, Navarro-Artieda R, Darbà J. Treatment persistence and adherence and their consequences on patient outcomes of generic versus brand-name statins routinely used to treat high cholesterol levels in Spain: a retrospective cost-consequences analysis. Lipids Health Dis. 17, 277 (2018).
20.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45, 613–619 (1992).
21.
The Anatomical Therapeutic Chemical Classification System with Defined Daily Doses (ATC/DDD): World Health Organization (2019) www.who.int/classifications/atcddd/en
22.
Gomez-Lumbreras A, Cortes J, Giner-Soriano M, Quijada-Manuitt MA, Morros R. Characteristics of apixaban-treated patients, evaluation of the dose prescribed, and the persistence of treatment: a cohort study in catalonia. J. Cardiovasc. Pharmacol. Ther. 23, 494–501 (2018).
23.
Anguita Sánchez M, Bertomeu Martínez V, Ruiz Ortiz M et al. FANTASIIA study investigators. Direct oral anticoagulants versus vitamin K antagonists in real-world patients with nonvalvular atrial fibrillation. The FANTASIIA study. Rev. Esp. Cardiol. (Engl. Ed.) (2019) (Epub ahead of print).
24.
Granger CB, Alexander JH, McMurray JJ et al. ARISTOTLE committees and investigators. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 365, 981–992 (2011).
25.
Raskob GE, Gallus AS, Pineo GF et al. Apixaban versus enoxaparin for thromboprophylaxis after hip or knee replacement: pooled analysis of major venous thromboembolism and bleeding in 8464 patients from the ADVANCE-2 and ADVANCE-3 trials. J. Bone Joint Surg. Br. 94, 257–264 (2012).
26.
Li XS, Deitelzweig S, Keshishian A et al. Effectiveness and safety of apixaban versus warfarin in non-valvular atrial fibrillation patients in ‘real-world’ clinical practice. A propensity-matched analysis of 76,940 patients. Thromb. Haemost. 117, 1072–1082 (2017).
27.
Himmler S, Müller M, Ostwald D, Seddik A, Basic E, Hradetzky E. Long-term health benefits of stroke prevention with apixaban versus vitamin K antagonist warfarin in patients with non-valvular atrial fibrillation in Germany: a population-based modelling study. Expert Rev. Pharmacoecon. Outcomes Res. 19, 223–230 (2019).
28.
Ramagopalan S, Allan V, Saragoni S et al. a LHUs group. Patient characteristics and bleeding events in nonvalvular atrial fibrillation patients treated with apixaban or vitamin K antagonists: real-world evidence from Italian administrative databases. J. Comp. Eff. Res. 7, 1063–1071 (2018).
29.
Kohsaka S, Katada J, Saito K, Terayama Y. Safety and effectiveness of apixaban in comparison to warfarin in patients with nonvalvular atrial fibrillation: a propensity-matched analysis from Japanese administrative claims data. Curr. Med. Res. Opin. 34, 1627–1634 (2018).
30.
Sicras-Mainar A, Fernández de Bobadilla J, Navarro-Artieda R, Rejas-Gutiérrez J. All-cause mortality and incidence of major cardiovascular events in hypertensive patients with ASCOT-type profile in a Spanish population setting. Aten Primaria 42, 420–430 (2010).
Information & Authors
Information
Published In
Pages: 1201 - 1212
PubMed: 31333045
Copyright
© 2019 Sreeram Ramagopalan et al. This work is licensed under the Attribution-NonCommercial 4.0 Unported License
History
Received: 20 June 2019
Accepted: 5 July 2019
Published online: 23 July 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Patient characteristics and stroke and bleeding events in nonvalvular atrial fibrillation patients treated with apixaban and vitamin K antagonists: a Spanish real-world study. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0079
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ma Carmen Montero-Balosa, Juan A. Limón-Mora, Ana Leal-Atienza, Beatriz García-Robredo, Pablo Sánchez-Villegas, Rebeca Isabel-Gómez, Ma José Aguado-Romeo, Luis Gabriel Luque Romero, Ma Teresa Molina-López, Comparative clinical outcomes of acenocoumarol versus direct oral anticoagulants (DOACs) and warfarin in patients with atrial fibrillation: real-world-evidence (SIESTA-A study), Frontiers in Pharmacology, 10.3389/fphar.2025.1548298, 16, (2025).
- Allie Cichewicz, Shantanu Jawla, Priccila Zuchinali, Morodoluwa Akin-Fajiye, Daniela Massierer, Italo Porto, Xavier Garcia-Moll, Real-world evidence comparing oral anticoagulants for NVAF in Europe: a systematic review and network meta-analysis, Future Cardiology, 10.1080/14796678.2025.2484119, 21, 6, (371-390), (2025).
- Manuel Anguita, Francisco Marín, Javier Soto, Susana Fernández de Cabo, Darío Rubio-Rodríguez, Carlos Rubio-Terrés, Cost-effectiveness of apixaban in non-valvular atrial fibrillation (NVAF) based on effectiveness data from a Spanish study in clinical practice (real-world evidence), Expert Review of Cardiovascular Therapy, 10.1080/14779072.2025.2464180, 23, 1-2, (45-51), (2025).
- Juan Cosín-Sales, Manuel Anguita Sánchez, Carmen Suárez, Carlos Arias-Cabrales, Luisa Martínez-Sanchez, Savana Research Group Savana Research Group, Daniel Arumi, Susana Fernández de Cabo, Safety and Effectiveness of Oral Anticoagulants in Atrial Fibrillation: Real-World Insights Using Natural Language Processing and Machine Learning, Journal of Clinical Medicine, 10.3390/jcm13206226, 13, 20, (6226), (2024).
- J. Cosín-Sales, M. Anguita, C. Suárez, C. Arias-Cabrales, L. Martínez-Sanchez, D. Arumi, S. Fernández de Cabo, Oral anticoagulant treatment in atrial fibrillation: the AFIRMA real-world study using natural language processing and machine learning, Revista Clínica Española (English Edition), 10.1016/j.rceng.2024.06.002, 224, 7, (428-436), (2024).
- J. Cosín-Sales, M. Anguita, C. Suárez, C. Arias-Cabrales, L. Martínez-Sanchez, S.R. group, D. Arumi, S. Fernández de Cabo, Tratamiento anticoagulante oral en la fibrilación auricular: AFIRMA, el estudio de vida real realizado mediante procesamiento de lenguaje natural y aprendizaje automático, Revista Clínica Española, 10.1016/j.rce.2024.05.005, 224, 7, (428-436), (2024).
- Josep Comín Colet, Antoni Sicras Mainar, Joel Salazar-Mendiguchía, María Isabel del Campo Alonso, Ainara Echeto, David Vilanova Larena, Olga Delgado Sánchez, Influence of the COVID-19 pandemic on patients receiving oral anticoagulants for the treatment of non-valvular atrial fibrillation, IJC Heart & Vasculature, 10.1016/j.ijcha.2024.101358, 51, (101358), (2024).
- Josep Comín Colet, Antoni Sicras Mainar, Joel Salazar-Mendiguchía, María Isabel del Campo Alonso, Ainara Echeto, David Vilanova Larena, Olga Delgado Sánchez, Healthcare resources and costs associated with nonvalvular atrial fibrillation in Spain: apixaban versus acenocoumarol, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0007, 12, 8, (2023).
- E. Rodilla, M.I. Orts-Martínez, M.A. Sanz-Caballer, M.T. Gimeno-Brosel, M.J. Arilla-Morel, I. Navarro-Gonzalo, I. Castillo-Valero, I. Salvador-Mercader, A. Carral-Tatay, Patterns and outcomes of switching direct oral anticoagulants in non-valvular atrial fibrillation: A real-world experience from Spain, Revista Clínica Española (English Edition), 10.1016/j.rceng.2023.04.005, 223, 6, (340-349), (2023).
- E. Rodilla, M.I. Orts-Martínez, M.Á. Sanz-Caballer, M.T. Gimeno-Brosel, M.J. Arilla-Morel, I. Navarro-Gonzalo, I. Castillo-Valero, I. Salvador-Mercader, A. Carral-Tatay, Patrones y resultados del cambio de anticoagulantes orales directos en la fibrilación auricular no valvular: experiencia en la práctica clínica en España, Revista Clínica Española, 10.1016/j.rce.2023.03.007, 223, 6, (340-349), (2023).