Indirect treatment comparison of valbenazine and deutetrabenazine efficacy and safety in tardive dyskinesia
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Utilize the Bucher indirect treatment comparison (ITC) method to compare valbenazine and deutetrabenazine efficacy using clinical trial data. Methods: Outcomes included mean change from baseline in Abnormal Involuntary Movement Scale (AIMS) total score, AIMS response (≥50% improvement), clinical global impression of change response (score ≤2) and safety outcomes. Data were pooled by trial and dose; outcomes were analyzed at multiple time points. Results: ITC of AIMS score improvement significantly favored valbenazine 80 mg/day at 6 weeks versus deutetrabenazine 36 mg/day at 8 weeks, while valbenazine 40 mg/day was statistically similar to all doses of deutetrabenazine at all time points. No significant differences between drugs were found in AIMS and clinical global impression of change responses and safety outcomes. Conclusion: In this ITC of pooled trial data, valbenazine was generally favorable over deutetrabenazine, although dose titration and equivalency should be considered when interpreting results.
Tardive dyskinesia (TD), an often irreversible and disabling movement disorder characterized by involuntary choreic or athetoid movements in the face/mouth, neck/trunk and/or extremities, is associated with prolonged exposure to antipsychotics and other dopamine receptor blocking agents [1–6]. Risk factors predictive of TD development (other than dopamine receptor blocking agent exposure) include older age, presence of diabetes mellitus and occurrence of acute dystonic reactions or drug-induced parkinsonism [5,7–10].
Since the introduction of second-generation antipsychotics (SGAs) in the 1980s, the expanding use of these drugs as mood stabilizers, adjunctive treatment for refractory depression, anti-anxiety agents and treatments for other conditions (e.g., agitation in dementia, disruptive behavior in pediatric patients) has contributed to a greater than threefold increase in prescriptions over 10 years [5,11]. Although preclinical data suggested that SGAs would be associated with a greatly reduced risk of TD [5], a recent meta-analysis of 41 studies estimated the global prevalence of TD to be 30% with first-generation antipsychotics and 21% with SGAs. In other words, even with the development of SGAs, the risk of developing TD is still substantial [12].
Until recently, in the absence of any US FDA approved treatments for TD, off-label medications such as tetrabenazine, a vesicular monoamine transporter 2 (VMAT2) inhibitor developed in the 1950s, were often prescribed to treat patients with this indication but with little evidence of efficacy [3,13]. Tetrabenazine is approved in the USA for the treatment of chorea associated with Huntington’s disease and has been used off-label to manage TD; however, there is limited evidence for tetrabenazine efficacy in TD due to a lack of randomized controlled trials (RCTs) [13,14]. In April 2017, however, a novel and highly selective VMAT2 inhibitor, valbenazine, was approved by the FDA for treating adults with TD. Approval of a second VMAT2 inhibitor, deutetrabenazine, a deuterated form of tetrabenazine, followed later that year [15,16]. While the underlying pathophysiology of TD is not yet fully understood, the identification of these treatments resulted, at least in part, from early data supporting the hypothesis that TD was the result of D2 receptor hypersensitivity related to chronic reduction of dopaminergic neurotransmission [6,17].
The approvals of valbenazine and deutetrabenazine were based on improvements in TD symptoms that were demonstrated in randomized, double-blind, placebo-controlled clinical trials [18–21]. In the studies, both drugs showed significant reduction in TD severity by 6 weeks (valbenazine) and 12 weeks (deutetrabenazine). In addition, a systematic review and meta-analysis of both agents in RCTs of TD concluded that both demonstrated efficacy compared with placebo in acute and long-term settings [22]. Although of great interest in evaluating treatment options, a direct comparison of the efficacy of valbenazine and deutetrabenazine could not be made due to the lack of head-to-head trials [22]. In the absence of studies that directly assess the relative efficacy of two treatments, methodologies have been developed to allow the indirect comparisons of treatment effects in RCTs [23]. Among these is the Bucher method, which allows an indirect treatment comparison (ITC) using a single common comparator. In previous studies, it has provided the closest correlation when compared with results from head-to-head comparative trials [24,25].
The present analysis utilized the Bucher ITC method to compare efficacy and safety outcomes for valbenazine and deutetrabenazine in patients with TD using RCT data obtained by a systematic literature review. Tetrabenazine was not included in the ITC due to lack of RCTs in TD [14].
Methods
Literature search & studies identified
To identify published, randomized, placebo-controlled studies of valbenazine and deutetrabenazine in TD, a search was conducted of PubMed and Embase on 29 August 2018 with the terms valbenazine [Title/Abstract] OR NBI 98854 [Title/Abstract] OR deutetrabenazine [Title/Abstract] OR SD 809 [Title/Abstract]. No restrictions were placed on date or language. Titles and/or abstracts were screened and excluded if they were duplicates, reviews, non-TD, pharmacokinetic/pharmacodynamic, or safety only. Of the 254 citations that were initially identified (Figure 1), 215 were excluded. The remaining 39 full text or conference abstracts were screened for eligibility, leaving two valbenazine studies (KINECT 2 [NCT01733121] [21] and KINECT 3 [NCT02274558] [20]) and two deutetrabenazine studies (ARM-TD [NCT02195700] [19] and AIM-TD [NCT02291861] [18,26]).
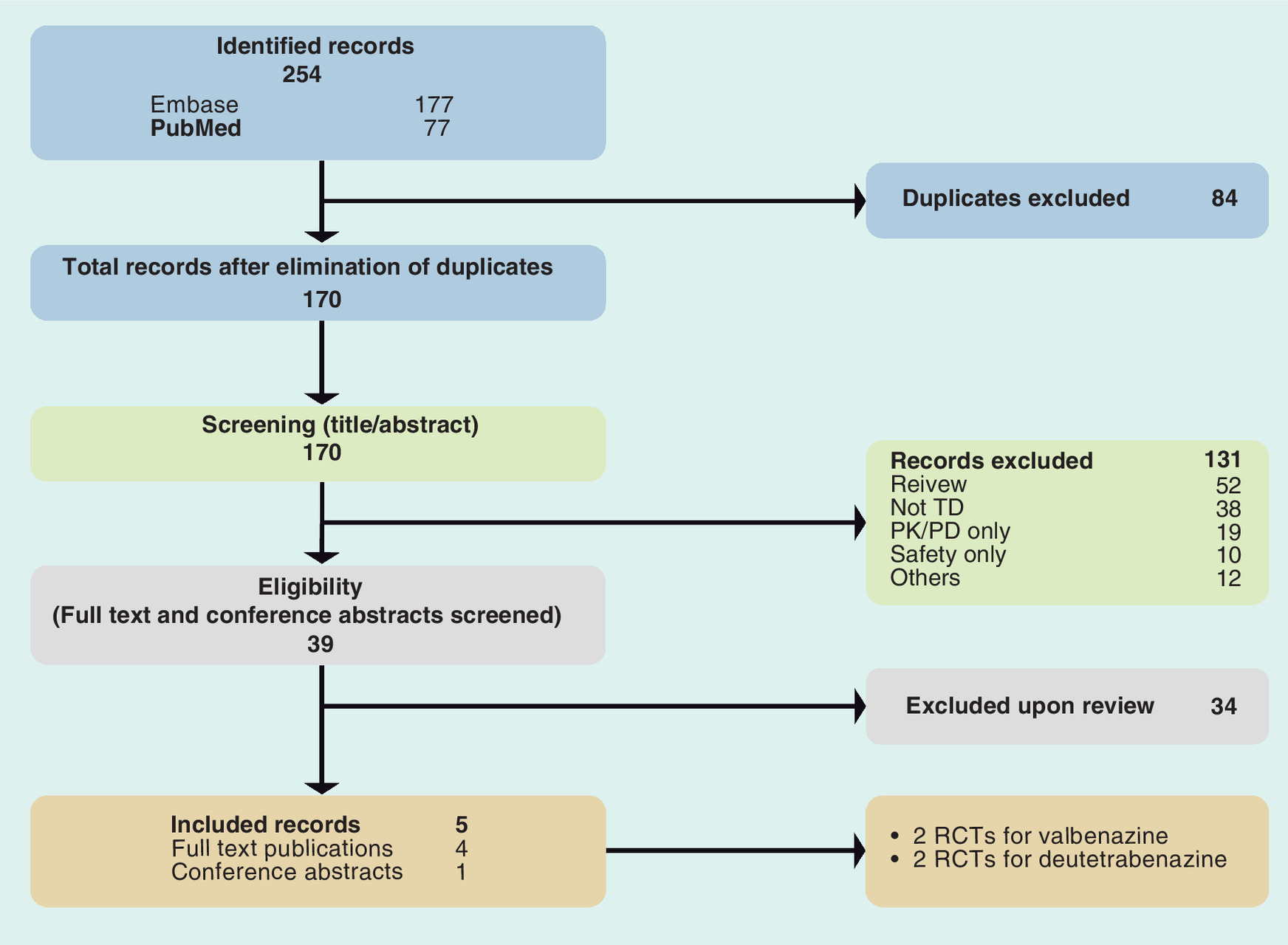
Figure 1. PRISMA flowchart of study selection process.
PK/PD: Pharmacokinetic/pharmacodynamic; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT: Randomized controlled trial; TD: Tardive dyskinesia.
Overall, the valbenazine and deutetrabenazine studies were similar in study design (Table 1). All four were randomized, placebo-controlled and double-blinded. Two were flexible-dose in design (KINECT 2, once-daily valbenazine 25–75 mg; ARM-TD, twice-daily deutetrabenazine 12–48 mg [19,21]), and two were fixed-dose (KINECT 3, once-daily valbenazine 40 or 80 mg; AIM-TD, twice-daily deutetrabenazine 12, 24 and 36 mg [18,20]). The primary efficacy outcome for the studies was mean change from baseline (CFB) in Abnormal Involuntary Movement Scale (AIMS) total score (sum of items 1–7) [27], which was assessed in all four studies by blinded central video raters who were experts in movement disorders. Additional outcomes included AIMS response (≥50% total score improvement from baseline) and clinical global impression of change (CGIC) response (score of 1 ‘very much improved’ or 2 ‘much improved’) [27]. Safety outcomes included treatment-emergent adverse events (TEAEs), serious adverse events (SAEs) and discontinuations due to TEAEs.
| Study (Duration) | Treatment groups, dosage† (n) | Key eligibility criteria | Efficacy outcomes | Ref. |
|---|---|---|---|---|
| Valbenazine | ||||
| KINECT 2 (6 weeks) | VBZ 25–75 (45) PBO (44) | • Drug-induced TD for ≥3 months • Moderate to severe dyskinesia (as qualitatively assessed) ‡ • Stable psychiatric status • Stable doses of psychiatric medications allowed • Concomitant anticholinergics allowed | AIMS total CFB AIMS 50% response CGIC response | [21] |
| KINECT 3 (6 weeks) | VBZ 40 (52) VBZ 80 (61) PBO (66) | • Drug-induced TD for ≥3 months • Moderate to severe dyskinesia (as qualitatively assessed) ‡ • Stable psychiatric status • Stable doses of psychiatric medications allowed • Concomitant anticholinergics allowed | AIMS total CFB AIMS 50% response CGIC response | [20] |
| Deutetrabenazine | ||||
| ARM-TD (12 weeks) | DTBZ 12–48 (48) PBO (49) | • TD diagnosis • AIMS total score ≥6 § • DRBA exposure ≥3 months (≥1 month if ≥60 years) • Stable doses of psychiatric medications allowed • Strong anticholinergics not allowed | AIMS total CFB AIMS 50% response¶ CGIC response | [19,26] |
| AIM-TD (12 weeks) | DTBZ 12 (60) DTBZ 24 (49) DTBZ 36 (55) PBO (58) | • TD diagnosis • AIMS total score ≥6 § • DRBA exposure ≥3 months (≥1 month if ≥60 years) • Stable doses of psychiatric medications allowed • Strong anticholinergics not allowed | AIMS total CFB AIMS 50% response CGIC response | [18] |
†
Dosages reported in total mg/day (valbenazine was given once daily and deutetrabenazine was given twice daily).
‡
Based on qualitative assessment of screening video by external reviewer.
§
Investigator-assessed at both screening and baseline and confirmed by blinded central video rater.
¶
Reported in Jimenez-Shahed et al. [26].
Bold font indicates differences between studies.
AIMS: Abnormal Involuntary Movement Scale; CFB: Change from baseline; CGIC: Clinical global impression of change; DRBA: Dopamine receptor blocking agent; DTBZ: Deutetrabenazine; PBO: Placebo; TD: Tardive dyskinesia; VBZ: Valbenazine.
Among the notable differences in study design were titration schedule and treatment duration. The flexible dose studies had longer escalation periods of 4 weeks (KINECT 2) and 6 weeks (ARM-TD), while the fixed-dose studies had shorter titration periods of 1 week (KINECT 3) and 4 weeks (AIM-TD) (Figure 2). The valbenazine trials were 6 weeks in duration, and the deutetrabenazine trials were 12 weeks. In addition, participants in the deutetrabenazine studies were required to have an AIMS total score ≥6 at baseline, while the valbenazine studies required participants to have moderate to severe dyskinesia at screening (based on qualitative assessment by an external reviewer). Finally, the valbenazine studies allowed concomitant anticholinergics, but the deutetrabenazine studies did not allow use of strong anticholinergics (e.g., trihexyphenidyl, benztropine, orphenadrine, procyclidine or biperiden).
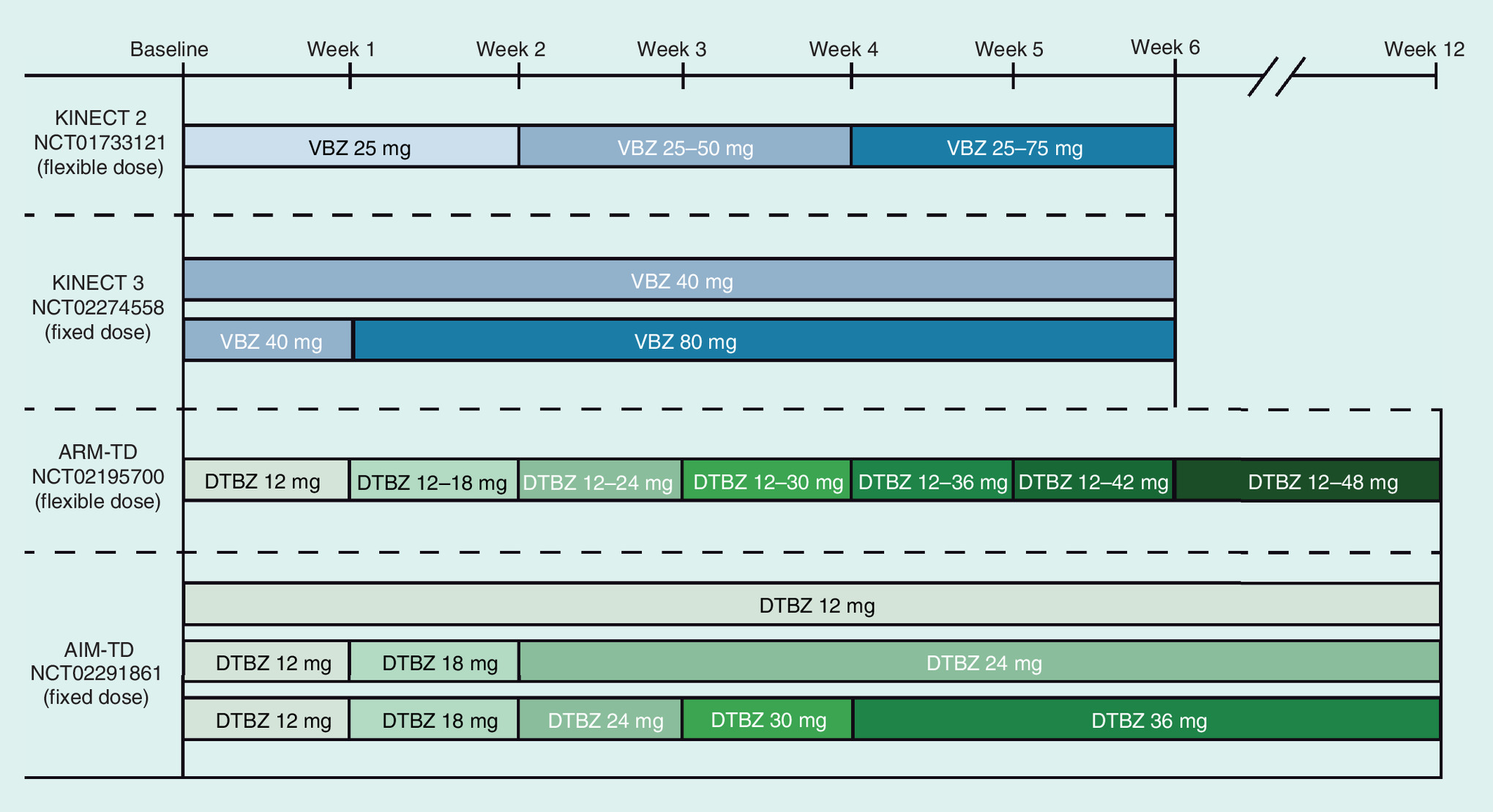
Figure 2. Titration schedules of valbenazine and deutetrabenazine studies.
DTBZ: Deutetrabenazine; VBZ: Valbenazine.
Data extraction & risk of bias assessment
Clinically relevant data on study characteristics (i.e., sample size, treatment duration and dosages), patient characteristics (i.e., age, sex and diagnosis) and efficacy data were extracted from the published valbenazine and deutetrabenazine studies and a 2016 deutetrabenazine poster [18–21,26]. The quality of the four studies identified in the search had previously been assessed and reported using the Cochrane tool for assessing risk of bias [22,28]. Risk of bias due to adequate sequence generation, allocation concealment, blinding (participant and personnel), blinding (outcome assessment), addressing of incomplete outcome data, freedom from selective reporting, freedom from other bias and summary bias assessment were judged to be low for all four trials.
ITC
The ITC was conducted by the method of Bucher et al., the preferred methodology for such comparisons [24]. This method allows for comparison of treatment effects for drugs A and B based on a comparison of observed effects for A versus C (placebo) and B versus C, with the log of the effect size for A versus B equal to the difference of log effect size measures for A versus C and B versus C.
Efficacy outcomes analyzed were mean CFB in AIMS total score (sum of items 1–7) [27], AIMS response (≥50% total score improvement) and CGIC response (score ≤2 [rating of ‘very much improved’ or ‘much improved’]). Data for valbenazine and deutetrabenazine were compared by trial and dose; outcomes were analyzed at multiple time points. Pooled AIMS score changes for valbenazine at 6 weeks (the duration of the valbenazine studies) were compared with pooled deutetrabenazine AIMS score changes at 12 weeks (the duration of the deutetrabenazine studies). Due to the difference in efficacy assessment time points between the valbenazine and deutetrabenazine trials, pooled AIMS scores assessments were compared at similar time points for valbenazine and deutetrabenazine by extracting AIMS scores at earlier time points from the deutetrabenazine publications using a plot digitizer. Valbenazine 6-week assessments were compared with 6 and 9 weeks for ARM-TD and 8 weeks for AIM-TD (6-week scores were not reported in AIM-TD). For AIMS and CGIC response analyses, however, no data were reported before week 12 for deutetrabenazine; therefore, response analyses were only conducted for valbenazine at 6 weeks versus deutetrabenazine at 12 weeks. Also, since efficacy was not demonstrated for the lowest dose of deutetrabenazine (12 mg) in AIM-TD, an additional (and more conservative) analysis of AIMS mean score change was conducted in which the 12 mg dose was excluded from the pooled deutetrabenazine dataset.
Safety outcomes analyzed were TEAEs, SAEs and discontinuations due to TEAEs. Data for valbenazine and deutetrabenazine were compared by trial and dose for valbenazine (6 weeks) versus deutetrabenazine (12 weeks).
The inverse variance method was used for pooling low and high doses in the fixed-dose studies (KINECT 3 and AIM-TD) and for estimation of overall AIMS CFB. For AIMS and CGIC response rates, odds rations (ORs) with 95% confidence interval (CI) were estimated using the Mantel–Haenszel test [29]. For ARM-TD, AIMS 50% response was estimated from a figure in Jimenez-Shahed et al. [26]. Inter-study heterogeneity was assessed with Cochran’s Q test. For safety outcomes, ORs with 95% CI were estimated using Fisher’s exact test.
Results
Baseline demographics for the four trials were generally similar (Table 2), but there was a slightly lower proportion of females in the valbenazine studies (KINECT 2, 43.0%; KINECT 3, 45.8%) than the deutetrabenazine studies (ARM-TD, 52.1%; AIM-TD, 55%) and a smaller proportion of white patients in the valbenazine studies (KINECT 2, 63.0%; KINECT 3, 56.4%) than the deutetrabenazine studies (ARM-TD, 69.2%; AIM-TD, 79%). Finally, mean baseline AIMS scores were slightly lower in KINECT 2 (8.0) than in KINECT 3 (10.0) or ARM-TD (9.6).
| Study | Age, mean (SD) | Females, n (%) | White, n (%) | AIMS score, mean (SD) | Schizophrenia/schizoaffective disorder, n (%) | Ref. |
|---|---|---|---|---|---|---|
| Valbenazine | ||||||
| KINECT 2 Placebo Valbenazine All | 55.6 (9.8) 56.7 (10.8) 56.2 (10.3) | 22 (44.9) 21 (41.2) 43 (43.0) | 30 (61.2) 33 (64.7) 63 (63.0) | 7.9 (4.5) 8.0 (3.5) 8.0 (4.0) | 30 (61.2) 28 (54.9) 58 (58.0) | [21] |
| KINECT 3 Placebo Valbenazine 40 mg Valbenazine 80 mg All | 57.0 (10.5) 55.3 (8.5) 56.0 (10.1) 56.1 (9.7) | 34 (44.7) 30 (41.7) 40 (50.6) 104 (45.8) | 43 (56.6) 41 (56.9) 44 (55.7) 128 (56.4) | 9.9 (4.3) 9.7 (4.1) 10.4 (3.6) 10.0 (4.0) | 50 (65.8) 48 (66.7) 52 (65.8) 150 (66.1) | [20] |
| Deutetrabenazine | ||||||
| ARM-TD Placebo Deutetrabenazine All | 53.3 (10.6) 55.9 (9.8) 54.6 (10.3) | 32 (54.2) 29 (50.0) 61 (52.1) | 44 (74.6) 37 (63.8) 81 (69.2) | 9.6 (3.8) 9.6 (4.1) 9.6 (3.9) | 40 (67.8) 40 (69.0) 80 (68.4) | [19] |
| AIM-TD Placebo Deutetrabenazine 12 mg Deutetrabenazine 24 mg Deutetrabenazine 36 mg All | 54.6 (12.1) 57.0 (10.0) 55.6 (11.3) 58.3 (11.6) 56.4 (11.3) | 37 (51) 42 (57) 41 (56) 42 (57) 162 (55) | 59 (82) 58 (78) 54 (74) 61 (82) 232 (79) | 9.5 (2.7)† 9.6 (2.4)† 9.4 (2.9)† 10.1 (3.2)† NR† | 42 (58.3) 40 (54.1) 49 (67.1) 44 (59.5) 175 (59.7) | [18] |
†
Based on the efficacy population. All other results based on safety populations.
AIMS: Abnormal Involuntary Movement Scale; NR: Not reported; SD: Standard deviation.
ITC
Differences between AIMS CFB for valbenazine and deutetrabenazine by dosage group and time point are shown in Figure 3. Compared with AIMS CFB for valbenazine 40 mg at 6 weeks, AIMS CFB for deutetrabenazine 24 mg and 36 mg at 8 or 12 weeks were generally similar. AIMS CFB for valbenazine 80 mg at 6 weeks, however, were more favorable than those for deutetrabenazine 24 or 36 mg at 8 or 12 weeks, with a statistically significant (p < 0.05) improvement for valbenazine 80 mg at 6 weeks compared with 36 mg deutetrabenazine at 8 weeks (-1.57; 95% CI: -3.12 to -0.21).
Indirect comparison by individual trials are shown in Figure 4. In all of these individual trial comparisons, differences in AIMS CFB favored valbenazine. This difference reached statistical significance for KINECT 3 pooled (40 and 80 mg) at 6 weeks versus AIM-TD pooled (12, 24 and 36 mg) at 8 weeks (-1.29; 95% CI: -2.49 to -0.09; p < 0.05).
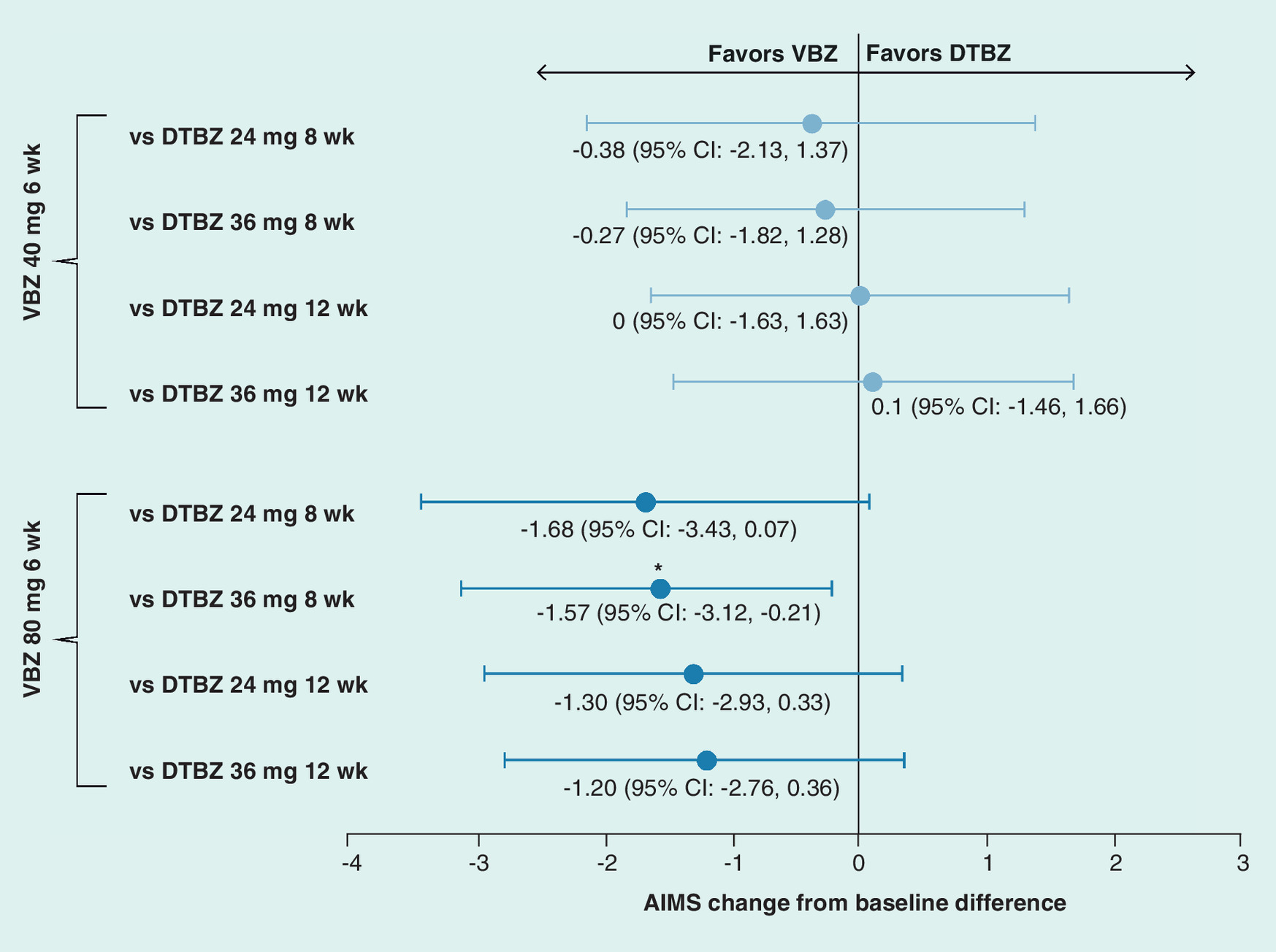
Figure 3. Differences in valbenazine and deutetrabenazine Abnormal Involuntary Movement Scale score changes and 95% CIs by dosage.
*Statistical significance (p < 0.05).
AIMS: Abnormal Involuntary Movement Scale; DTBZ: Deutetrabenazine; VBZ: Valbenazine.
ITCs using pooled data for all valbenazine and deutetrabenazine trials are shown in Figure 5. Regardless of the time point analyzed for pooled deutetrabenazine trials, and independent of whether or not data for the lowest and least effective (based on CFB in mean AIMS score) dose (12 mg) of deutetrabenazine was included, the reductions in AIMS scores favored the pooled valbenazine trials. Differences in effects were statistically significant (p < 0.05) for comparisons of the 6-week valbenazine time point versus the 6/8- or 9/8-week deutetrabenazine time point, but not for the 6-week valbenazine versus 12-week deutetrabenazine time point comparison.
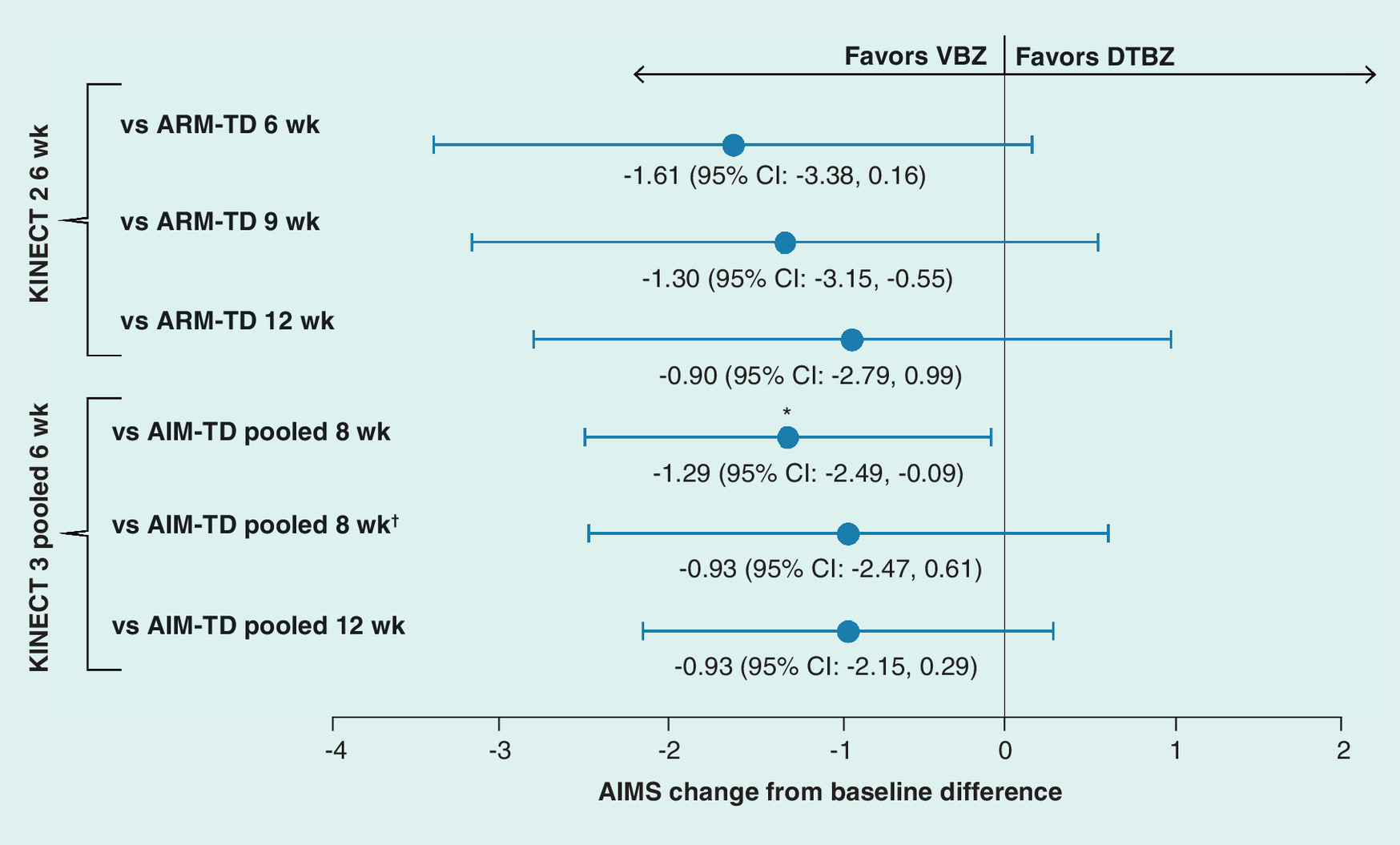
Figure 4. Differences in valbenazine and deutetrabenazine Abnormal Involuntary Movement Scale score changes and 95% CIs by trial.
†Without 12 mg arm.
*Statistical significance (p < 0.05).
AIMS: Abnormal Involuntary Movement Scale; DTBZ: Deutetrabenazine; VBZ: Valbenazine.

Figure 5. Differences in valbenazine and deutetrabenazine Abnormal Involuntary Movement Scale score changes and 95% CIs for pooled trials.
†Without 12 mg arm.
*Statistical significance (p < 0.05).
AIMS: Abnormal Involuntary Movement Scale; DTBZ: Deutetrabenazine; VBZ: Valbenazine.
ITC analyses of valbenazine (6 weeks) and deutetrabenazine (12 weeks) by the ORs for AIMS response (≥50% total score improvement from baseline) and CGIC response (score ≤2) are shown in Table 3. The ORs for AIMS response favored valbenazine over deutetrabenazine in individual trial comparisons. In dosage comparisons, deutetrabenazine 24 and 36 mg were slightly favored compared with valbenazine 40 mg, but valbenazine 80 mg was favored compared with deutetrabenazine 24 and 36 mg. For the overall pooled valbenazine 6 week versus pooled deutetrabenazine 12-week comparison, valbenazine was favored (OR: 2.3; 95% CI: 0.91–5.81). In no cases, however, were the differences statistically significant.
| Valbenazine group (n) | Deutetrabenazine group (n) | OR (95% CI) |
|---|---|---|
| AIMS response (≥50% total score improvement) | ||
| Individual trial comparison | ||
| KINECT 2 (45) | ARM-TD (48) | 2.91 (0.74–11.44) |
| KINECT 3 (133) | AIM-TD (164) | 1.94 (0.55–6.82) |
| Dosage comparison | ||
| KINECT 3 40 mg (63) | AIM-TD 24 mg (49) | 0.85 (0.21–3.50) |
| KINECT 3 40 mg (63) | AIM-TD 36 mg (55) | 0.93 (0.23–3.79) |
| KINECT 3 80 mg (70) | AIM-TD 24 mg (49) | 1.81 (0.46–7.17) |
| KINECT 3 80 mg (70) | AIM-TD 36 mg (55) | 1.98 (0.50–7.77) |
| Pooled comparison | ||
| KINECT 2/3 (178) | ARM-TD/AIM-TD (212) | 2.30 (0.91–5.81) |
| CGIC response (score ≤2 at end point) | ||
| Individual trial comparison | ||
| KINECT 2 (45) | ARM-TD (48) | 5.16 (1.4–19.04)† |
| KINECT 3 (113) | AIM-TD (164) | 1.14 (0.43–3.03) |
| Dosage comparison | ||
| KINECT 3 40 mg (52) | AIM-TD 24 mg (49) | 0.79 (0.25–2.51) |
| KINECT 3 40 mg (52) | AIM-TD 36 mg (55) | 0.97 (0.31–3.08) |
| KINECT 3 80 mg (61) | AIM-TD 24 mg (49) | 0.78 (0.25–2.44) |
| KINECT 3 80 mg (61) | AIM-TD 36 mg (55) | 0.97 (0.31–3.0) |
| Pooled comparison | ||
| KINECT 2/3 (158) | ARM-TD/AIM-TD (212) | 2.34 (0.45–12.12) |
†
Statistical significance (p < 0.05).
AIMS: Abnormal Involuntary Movement Scale; CGIC: Clinical global impression of change; OR: Odds ratio.
The ORs for CGIC response rates in the individual trials and overall pooled comparisons favored valbenazine 6 weeks versus deutetrabenazine 12 weeks. ORs for CGIC response in dosage comparisons of deutetrabenazine (24 or 36 mg) versus valbenazine (40 or 80 mg) slightly favored deutetrabenazine. None of these differences reached statistical significance, except for the individual trial comparison of KINECT 2 versus ARM-TD, which significantly favored valbenazine (OR: 5.16; 95% CI: 1.4–19.0; p < 0.05).
None of the ORs for individual trial, pooled dosage or overall pooled comparisons of TEAEs, SAEs and discontinuations due to TEAEs of valbenazine 6 weeks versus deutetrabenazine 12 weeks reached statistical significance (Table 4). Incidences of SAEs and TEAE discontinuations were low in all four studies, which is reflected in the wide CIs for the ORs. Two individual trial comparisons were not feasible due to zero SAEs and TEAE discontinuation events reported in KINECT 2.
| Valbenazine group (n) | Deutetrabenazine group (n) | OR (95% CI) |
|---|---|---|
| TEAEs | ||
| Individual trial comparison | ||
| KINECT 2 (51) | ARM-TD (58) | 1.17 (0.35–3.90) |
| KINECT 3 (151) | AIM-TD (221) | 1.68 (0.68–4.10) |
| Dosage comparison | ||
| KINECT 3 40 mg (72) | AIM-TD 24 mg (73) | 1.78 (0.56–5.64) |
| KINECT 3 40 mg (72) | AIM-TD 36 mg (74) | 0.98 (0.33–2.88) |
| KINECT 3 80 mg (79) | AIM-TD 24 mg (73) | 2.70 (0.86–8.45) |
| KINECT 3 80 mg (79) | AIM-TD 36 mg (74) | 1.49 (0.52–4.31) |
| Pooled comparison | ||
| KINECT 2/3 (202) | ARM-TD/AIM-TD (279) | 1.78 (0.90–3.51) |
| SAEs | ||
| Individual trial comparison | ||
| KINECT 2 (51) | ARM-TD (58) | NA† |
| KINECT 3 (151) | AIM-TD (221) | 1.77 (0.68–4.10) |
| Dosage comparison | ||
| KINECT 3 40 mg (72) | AIM-TD 24 mg (73) | 0.94 (0.08–10.82) |
| KINECT 3 40 mg (72) | AIM-TD 36 mg (74) | 1.47 (0.12–18.95) |
| KINECT 3 80 mg (79) | AIM-TD 24 mg (73) | 1.31 (0.13–13.37) |
| KINECT 3 80 mg (79) | AIM-TD 36 mg (74) | 2.06 (0.18–23.53) |
| Pooled comparison | ||
| KINECT 2/3 (202) | ARM-TD/AIM-TD (279) | 0.88 (0.14–5.56) |
| Discontinuations due to TEAEs | ||
| Individual trial comparison | ||
| KINECT 2 (51) | ARM-TD (58) | NA† |
| KINECT 3 (151) | AIM-TD (221) | 0.77 (0.07–8.52) |
| Dosage comparison | ||
| KINECT 3 40 mg (72) | AIM-TD 24 mg (73) | 1.07 (0.05–25.31) |
| KINECT 3 40 mg (72) | AIM-TD 36 mg (74) | 0.72 (0.04–13.23) |
| KINECT 3 80 mg (79) | AIM-TD 24 mg (73) | 1.23 (0.06–27.52) |
| KINECT 3 80 mg (79) | AIM-TD 36 mg (74) | 0.82 (0.05–14.32) |
| Pooled comparison | ||
| KINECT 2/3 (202) | ARM-TD/AIM-TD (279) | 1.20 (0.17–8.59) |
†
Indirect treatment comparisons were not feasible because there were no SAEs or discontinuations leading to TEAEs in KINECT 2.
NA: Not applicable; OR: Odds ratio; SAE: Serious adverse event; TEAE: Treatment-emergent adverse event.
Discussion
While the pivotal RCTs of valbenazine and deutetrabenazine showed significant improvements for both drugs compared with placebo [18–21], there have been no comparative trials assessing the relative efficacy of these approved TD medications. In the absence of such head-to-head data, other methodological approaches (e.g., meta-analyses, indirect comparisons) can provide useful tools for informing treatment choices [23]. In this study, an ITC of valbenazine versus deutetrabenazine efficacy and safety outcomes from the RCTs was conducted using the Bucher method.
In comparisons of AIMS score changes by dose, valbenazine 40 mg/day at 6 weeks was similar to deutetrabenazine 24 and 36 mg/day at 8 and 12 weeks. Valbenazine 80 mg/day had more favorable AIMS scores than both doses of deutetrabenazine at 8 and 12 weeks, with statistical significance reached versus 36 mg/day at 8 weeks. Comparison of AIMS score changes by individual trial favored valbenazine, with statistical significance achieved for the KINECT 3 (6 weeks) versus AIM-TD (8 weeks) AIMS CFB. In the overall pooled ITC analysis, valbenazine AIMS score improvements at 6 weeks were favored compared with deutetrabenazine scores at 6/8, 9/8 and 12 weeks (even in the more conservative analysis in which the 12-mg dose of deutetrabenazine was excluded for lack of demonstrated efficacy). This difference reached statistical significance when compared with the extrapolated earlier deutetrabenazine time points (6/8 and 9/8 weeks), which are more comparable with the valbenazine study durations.
None of the pooled ITCs of the secondary end points of AIMS and CGIC response or safety outcomes of TEAEs, SAEs and discontinuation due to TEAEs reaching statistical significance.
The following limitations of this ITC analysis should be considered. As noted by Bucher, the strength of inference from indirect comparisons is limited [24]. Inter-trial variability in baseline populations, treatment duration and titration schedules can affect results. Despite notable differences in inclusion and exclusion criteria (e.g., symptom severity at baseline and concomitant medications), baseline characteristics were similar among the trials. To account for the potential differences in treatment durations and titration schedules in the ITC analysis, multiple comparisons were conducted at different time points by extracting AIMS scores from the deutetrabenazine publications at multiple time points (including earlier time points similar to the duration of the valbenazine trials).
The titration periods were generally longer in the deutetrabenazine trials: a clinically efficacious dose (≥24 mg/day) was not reached until week 3, compared with valbenazine trials in which patients started at an efficacious dose (≥40 mg/day) or achieved by week 2. However, starting doses in all the studies were within the dosing range indicated in each drug’s product label (12 mg/day for deutetrabenazine and 40 mg/day for valbenazine), with the exception of KINECT 2 in which a therapeutic dose (50 mg/day) was reached after 2 weeks [15,16]. Moreover, valbenazine was favored over deutetrabenazine when comparing the valbenazine 6-week AIMS score changes to the deutetrabenazine 8/9-week score changes, when patients in the deutetrabenazine trials had been receiving a clinically efficacious dose for a similar duration to those in the valbenazine trials, despite the slower titration.
The favorable improvement of valbenazine at earlier time points found in this study may be due in part to its unique characteristics, including a pharmacokinetic profile (e.g., apparent half-life of 15–22 h) that allows for once-daily dosing and a titration schedule that achieves a therapeutic dose (40 mg/day) at initiation and the maximum recommended dose (80 mg/day) within 1 week of initiation [15,30,31]. In contrast, deutetrabenazine has a half-life of 9–10 h and requires twice-daily dosing, with titration by weekly 6-mg increments as tolerated to a therapeutic dose of 12–48 mg/day [16,30]. Many patients may require at least 36 mg/day for efficacy, as indicated by the mean daily doses reported in ARM-TD, which were 38.8 mg at the end of titration and 38.3 mg at end of treatment [19].
While the ITC of safety outcomes showed similar tolerability for both drugs, the shorter duration for valbenazine versus deutetrabenazine studies may have affected results (comparisons at earlier time points for deutetrabenazine were not possible, as safety data were reported only for the 12-week trial duration). In addition, sample sizes were very small for reported SAEs and discontinuation due to TEAEs, which was reflected by the large CIs.
As with any statistical method, results will depend on sample size, which is limited in this analysis to the four available RCTs. Finally, there was no analysis of long-term data, as this study focused by design on efficacy outcomes in well-controlled trials, which were shorter in duration.
When making treatment decisions for patients with TD, clinicians must consider the many factors that contribute to treatment success, such as the efficacy, safety, tolerability and timing of dosing. In this ITC, the efficacy of valbenazine 80 mg/day was statistically favorable to deutetrabenazine 36 mg/day at earlier time points, while valbenazine 40 mg/day was statistically similar to all doses of deutetrabenazine at all time points. No significant differences were found in safety profiles of valbenazine versus deutetrabenazine. Based on this analysis, valbenazine 80 mg/day may be more efficacious in improving TD symptoms than deutetrabenazine when compared at equal timeframes.
Future perspective
The availability of the first-approved treatments for TD, valbenazine and deutetrabenazine, has revolutionized the treatment of this debilitating and often irreversible disorder. As we strive to provide better care and improved quality of life for patients with TD, there are many important areas for future research. There is a pressing need to increase awareness of TD and to create standards to guide screening, diagnosis and treatment. Future research is needed to better understand the comparative safety of approved TD treatments and the impact of these medications on patient function and quality of life. In addition, more work is needed on the fundamental questions of the neurobiology of TD, such as the potential for prevention and reversibility, risk factors and the potential benefit of earlier introduction of VMAT2 inhibitors to delay onset or progression of TD.
•
Valbenazine and deutetrabenazine, the first-approved treatments available for adults with tardive dyskinesia (TD), have demonstrated efficacy to significantly improve TD symptoms in randomized controlled trials.
•
In the absence of head-to-head data comparing the relative efficacy of the two drugs, indirect treatment comparison can provide useful tools for informing treatment choices for TD.
•
A Bucher indirect treatment comparison was conducted to compare efficacy and safety of valbenazine and deutetrabenazine using pooled data from randomized controlled trial studies.
•
Abnormal Involuntary Movement Scale (AIMS) change from baseline in pooled comparisons by dose favored valbenazine 80 mg/day versus deutetrabenazine 24 and 36 mg/day at 8 and 12 weeks (statistically significant versus 36 mg/day at 8 weeks); valbenazine 40 mg/day was similar to both deutetrabenazine doses at both time points.
•
AIMS change from baseline in individual trial and overall pooled comparisons favored valbenazine at 6 weeks versus deutetrabenazine at 6/8, 9/8 and 12 weeks; this reached statistical significance at the earlier time points (6/8 and 9/8 weeks).
•
There were no significant differences in individual trial and pooled comparisons of AIMS and clinical global impression of change responses, and no significant differences in safety outcomes.
•
Based on this analysis, valbenazine 80 mg/day may be more efficacious in improving TD symptoms than deutetrabenazine when compared at equal timeframes.
Author contributions
All authors contributed to the preparation of this manuscript, approved this version for publication and met the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. S Aggarwal, M Serbin and C Yonan contributed to study design, interpretation of data and manuscript preparation and review. S Aggarwal performed the ITC analysis.
Acknowledgments
S Kumar of Novel Health Strategies (Washington, DC) assisted S Aggarwal with data extraction and risk of bias assessment for the analysis.
Financial & competing interests disclosure
S Aggarwal is Principal of Novel Health Strategies, which was contracted by Neurocrine Biosciences, Inc. (CA, USA) to conduct this analysis. M Serbin and C Yonan are employed by Neurocrine Biosciences, Inc., and own shares in the company. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing and editorial assistance were provided by Prescott Medical Communications Group (IL, USA), with support from Neurocrine Biosciences, Inc.
Ethical disclosure
This study was noninterventional in nature and did not include primary data collection; therefore institutional review board approval was not required. Secondary data used in this study were taken from previously published randomized controlled trials, which were approved by the institutional review boards of the participating sites, with informed consent from participants.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
American Psychiatric Association. Medication Induced Movement Disorders and Other Adverse Effects of Medication (5th Edition). American Psychiatric Publishing, Washington, DC, USA, 709–714 (2013).
2.
Caroff SN, Davis VG, Miller DD et al. Treatment outcomes of patients with tardive dyskinesia and chronic schizophrenia. J. Clin. Psychiatry 72(3), 295–303 (2011).
3.
Rana AQ, Chaudry ZM, Blanchet PJ. New and emerging treatments for symptomatic tardive dyskinesia. Drug Design Dev. Ther. 7, 1329–1340 (2013).
4.
Vijayakumar D, Jankovic J. Drug-induced dyskinesia, part 2: treatment of tardive dyskinesia. Drugs 76(7), 779–787 (2016).
5.
Cloud LJ, Zutshi D, Factor SA. Tardive dyskinesia: therapeutic options for an increasingly common disorder. Neurotherapeutics 11(1), 166–176 (2014).
• Comprehensive review of tardive dyskinesia (TD).
6.
Scorr LM, Factor SA. VMAT2 inhibitors for the treatment of tardive dyskinesia. J. Neurol. Sci. 389, 43–47 (2018).
7.
Tenback DE, Van Harten PN. Epidemiology and risk factors for (tardive) dyskinesia. Int. Rev. Neurobiol. 98, 211–230 (2011).
8.
Woerner MG, Alvir JM, Saltz BL, Lieberman JA, Kane JM. Prospective study of tardive dyskinesia in the elderly: rates and risk factors. Am. J. Psychiatry 155(11), 1521–1528 (1998).
9.
Woerner MG, Saltz BL, Kane JM, Lieberman JA, Alvir JM. Diabetes and development of tardive dyskinesia. Am. J. Psychiatry 150(6), 966–968 (1993).
10.
Yassa R, Nastase C, Dupont D, Thibeau M. Tardive dyskinesia in elderly psychiatric patients: a 5-year study. Am. J. Psychiatry 149(9), 1206–1211 (1992).
11.
Olfson M, Blanco C, Liu SM, Wang S, Correll CU. National trends in the office-based treatment of children, adolescents, and adults with antipsychotics. Arch. Gen. Psychiatry 69(12), 1247–1256 (2012).
12.
Carbon M, Hsieh CH, Kane JM, Correll CU. Tardive dyskinesia prevalence in the period of second-generation antipsychotic use: a meta-analysis. J. Clin. Psychiatry 78(3), e264–e278 (2017).
• Recent meta-analylsis of antipsychotic clinical trials that estimates TD prevalence.
13.
Bhidayasiri R, Jitkritsadakul O, Friedman JH, Fahn S. Updating the recommendations for treatment of tardive syndromes: a systematic review of new evidence and practical treatment algorithm. J. Neurol. Sci. 389, 67–75 (2018).
14.
Caroff SN, Aggarwal S, Yonan C. Treatment of tardive dyskinesia with tetrabenazine or valbenazine: a systematic review. J. Comp. Eff. Res. 7(2), 135–148 (2018).
15.
Ingrezza, prescribing information. Neurocrine Biosciences, Inc., San Diego, CA, USA (2017).
16.
Austedo, prescribing information. Teva Pharmaceuticals USA, Inc., North Wales, PA, USA (2017).
17.
Hauser RA, Truong D. Tardive dyskinesia: out of the shadows. J. Neurol. Sci. 389, 1–3 (2018).
18.
Anderson KE, Stamler D, Davis MD et al. Deutetrabenazine for treatment of involuntary movements in patients with tardive dyskinesia (AIM-TD): a double-blind, randomised, placebo-controlled, Phase III trial. Lancet Psych. 4(8), 595–604 (2017).
•• Pivotal clinical trial of deutetrabenazine in TD.
19.
Fernandez HH, Factor SA, Hauser RA et al. Randomized controlled trial of deutetrabenazine for tardive dyskinesia: the ARM-TD study. Neurology 88(21), 2003–2010 (2017).
•• Pivotal clinical trial of deutetrabenazine in TD.
20.
Hauser RA, Factor SA, Marder SR et al. KINECT 3: a Phase III randomized, double-blind, placebo-controlled trial of valbenazine for tardive dyskinesia. Am. J. Psychiatry 174(5), 476–484 (2017).
•• Pivotal clinical trial of valbenazine in TD.
21.
O’Brien CF, Jimenez R, Hauser RA et al. NBI-98854, a selective monoamine transport inhibitor for the treatment of tardive dyskinesia: a randomized, double-blind, placebo-controlled study. Mov. Disord. 30(12), 1681–1687 (2015).
•• Pivotal clinical trial of valbenazine in TD.
22.
Solmi M, Pigato G, Kane JM, Correll CU. Treatment of tardive dyskinesia with VMAT-2 inhibitors: a systematic review and meta-analysis of randomized controlled trials. Drug Design Dev. Ther. 12, 1215–1238 (2018).
• Review and meta-analysis of valbenazine and deutetrebenazine trials.
23.
Edwards SJ, Clarke MJ, Wordsworth S, Borrill J. Indirect comparisons of treatments based on systematic reviews of randomised controlled trials. Int. J. Clin. Pract. 63(6), 841–854 (2009).
24.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 50(6), 683–691 (1997).
•• Description of indirect treatment comparison method.
25.
Song F, Altman DG, Glenny AM, Deeks JJ. Validity of indirect comparison for estimating efficacy of competing interventions: empirical evidence from published meta-analyses. BMJ 326(7387), 472 (2003).
26.
Jimenez-Shahed J, Factor SA, Ondo WG. Deutetrabenazine is associated with an improvement in involuntary movements in patients with tardive dyskinesia (TD) as seen by the high proportion of responders to treatment in the ARM-TD study. Poster Presentation 208. 29th US Psychiatric and Mental Health Congress. TX, USA, 21–24 October 2016.
27.
Guy W. ECDEU Assessment Manual for Psychopharmacology. US Dept. of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs, MD, USA (1976).
28.
Higgins JP, Altman DG, Gotzsche PC et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
29.
Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl Cancer Inst. 22(4), 719–748 (1959).
30.
Harriott ND, Williams JP, Smith EB, Bozigian HP, Grigoriadis DE. VMAT2 inhibitors and the path to ingrezza (valbenazine). Prog. Med. Chem. 57(1), 87–111 (2018).
31.
Luo R, Bozigian H, Jimenez R, Loewen G, O’Brien CF. Single dose and repeat once-daily dose safety, tolerability and pharmacokinetics of valbenazine in healthy male subjects. Psychopharmacol. Bull. 47(3), 44–52 (2017).
Information & Authors
Information
Published In
Pages: 1077 - 1088
PubMed: 31464152
Copyright
© 2019 Yonan et al. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 20 May 2019
Accepted: 29 July 2019
Published online: 29 August 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Indirect treatment comparison of valbenazine and deutetrabenazine efficacy and safety in tardive dyskinesia. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0059
Export citation
Select the citation format you wish to export for this article or chapter.