Comparative effectiveness of a human fibroblast-derived dermal substitute and a viable cryopreserved placental membrane for the treatment of diabetic foot ulcers
Publication: Journal of Comparative Effectiveness Research
Abstract
Objective: To compare a human fibroblast-derived dermal substitute (HFDS) to a viable cryopreserved placental membrane (vCPM) for use in diabetic foot ulcers (DFUs). Methods: An electronic medical record database of 1622 refractory DFUs with areas 1–40 cm2 was analyzed. Results: Cox estimates of wound closure for HFDS (1444 wounds) were significantly greater (p = 0.0002) by weeks 12 (31 vs 21%), 24 (55 vs 39%) and 36 (68 vs 51%) compared with vCPM (178 wounds). HFDS reduced the median time to wound closure by 55% compared with vCPM, (20 vs 36 weeks, p = 0.0002). HFDS also increased the probability of wound closure by 60% (hazard ratio = 1.60 [95% confidence interval, (1.25, 2.06)], p = 0.0002). Conclusion: HFDS improved time and frequency of wound closure in DFUs versus vCPM.
Twenty million patients have been diagnosed with diabetes in the USA, and approximately 25% of these patients develop a diabetic foot ulcer (DFU) [1,2]. The incidence of DFUs has been reported to be up to 8% of diabetes patients annually [3,4]. DFUs are associated with prolonged hospitalizations, increased risk of infections, cellulitis, osteomyelitis, sepsis and amputations [5–7]. The risk of amputation for patients with foot infections has been shown to be over 150-times greater than for those without foot infections [8]. The 5-year mortality rate for amputated patients is approximately 50%. Patients that have undergone an amputation have a greater 5-year mortality rate than those patients diagnosed with the most commonly occurring cancers [9]. DFUs impose a significant financial burden on US payers at an estimated annual direct medical cost of up to $13 billion [9].
Standard wound management for DFUs consists of debridement, infection control, use of dressings and offloading. However, up to 70% of DFUs do not respond to standard care [10]. The Wound Healing Society guidelines recommend the use of standard care therapy for an initial period of 4 weeks, at which time, if a wound size reduction of at least 50% is not observed, then intervention with advanced therapies, including skin substitutes, is recommended to achieve complete wound closure (CWC) and reduce the risk of complications [11].
More than 50 skin substitute products are available for treating wounds. They have been categorized based on whether they are acellular or cellular, derived from human or animal tissue and the methods/extent of processing. Human fibroblast-derived dermal substitute (HFDS; Dermagraft; Organogenesis Inc., MA, USA) and viable cryopreserved placental membrane (vCPM; Grafix; Osiris Therapeutics Inc., MD, USA) have been used for the treatment of DFUs. HFDS was approved by the US FDA as a wound treatment for DFUs via the premarket approval process. Pivotal randomized controlled trials (RCTs) were required to demonstrate efficacy and safety to support the indication for use [12]. Additional RCTs have been conducted with HFDS both prior to and after the FDA approval [13–18]. Manufacturing of HFDS is compliant with the American Association of Tissue Banking standards, Good Tissue Practice and Good Manufacturing Practice requirements. vCPM is classified as a human cells, tissues and cellular, and tissue-based product (HCT/P). vCPM is considered by FDA guidelines as a wound covering. Prospective RCTs have been performed with vCPM without a requirement for FDA premarket review of clinical outcomes. FDA regulates the manufacturing process for vCPM for compliance with Good Tissue Practice and Good Manufacturing Practice. While no FDA premarket evaluation was required for vCPM as an HCT/P, vCPM has been evaluated in clinical studies for publication [19–22].
Many skin substitute products are available for the treatment of chronic wounds, yet real-world comparative effectiveness research CER studies that involve large numbers of wound care facilities and large numbers of patients are relatively lacking for this treatment class. However, information regarding clinical outcomes in real-world, physician practice settings is required to determine the concordance between RCT data collected under rigorous, more restrictive conditions required by protocols and data from CER studies that reflect current practice conditions. Such data are becoming increasingly important in the US healthcare environment, which today is driven by outcomes and cost efficiencies.
HFDS is a wound treatment that was FDA-approved for the treatment of DFUs in 2001. It is a bioengineered living cellular construct containing metabolically active fibroblasts obtained from human newborn foreskin tissue. The fibroblasts are seeded on a bioabsorbable polyglactin mesh scaffold, and are known to produce human collagen, extracellular matrix (ECM) proteins, cytokines and growth factors [23]. The efficacy of HFDS is supported by a large scale, multicenter RCT which showed that treatment with HFDS resulted in a significantly greater percentage of healed ulcers compared with standard care therapy [12]. HFDS is cryopreserved and thawed prior to use. vCPM is a HCT/P, a placental tissue allograft having endogenous growth factors in a native amniotic matrix containing collagen, and various cell types including epithelial cells, fibroblasts and mesenchymal stem cells [24,25]. HFDS and vCPM are different in composition and cell populations; however, both products are cryopreserved and are stored at -80°C [26,27].
HFDS has not been compared with vCPM in CER studies. Effective treatment, established in CER studies, is the extent to which a treatment intervention produces its intended effect in real-world care conditions. RCTs with positive results, on the other hand, provide evidence of efficacious treatment in controlled, highly constrained conditions that are optimal for obtaining favorable results [28,29]. Assessing if efficacy reported from the results of RCTs can be translated to everyday, clinical wound care settings (effectiveness) will provide additional evidence to examine existing treatment algorithms.
The objective of this study was to evaluate the comparative effectiveness of HFDS compared with vCPM for the treatment of DFUs in real-world settings using data over a 5-year period from a large wound care specific electronic medical record (EMR) database (WoundExpert, Net Health, PA, USA) that is utilized by approximately 20,000 physicians in over 1000 wound care facilities across the USA.
Methods
Study design
This study is a retrospective analysis to compare the effectiveness of HFDS and vCPM for the treatment of DFUs using de-identified EMRs from wound care facilities across the USA in a 5-year period. The primary analyses were frequency of CWC evaluated up to 36 months and median time to CWC. Wound areas (cm2) were calculated from wound measurements of length and width. CWC was defined as full epithelialization of the wound with the absence of drainage. Epithelialization was defined as a layer of epithelium visible on the wound surface.
Patients
Patients eligible for inclusion were those documented as receiving at least one treatment of either HFDS or vCPM on a DFU located on the foot, heel, toes, metatarsal heads or other anatomical structures below the ankle determined to be of diabetic wound etiology. Included baseline wound areas were 1–40 cm2 with an ulcer duration of at least 1 month prior to first treatment with HFDS or vCPM. To assure analyses were restricted to refractory DFUs, wounds needed to have closed no more than 50% within the 4 weeks prior to first treatment with HFDS or vCPM. Wounds without baseline or follow-up area measurements were excluded as well as those where the date of HFDS or vCPM treatment was unknown. Wounds were also excluded if they received either HFDS or vCPM within 28 days of the first treatment with HFDS or, alternatively, if they received HFDS or vCPM within 28 days of the first treatment with vCPM. Censoring occurred for nonhealed wounds at their last visit with an area measurement. Patients were also censored at the visit where an alternate skin substitute product was applied (Apligraf, Oasis, Epifix, Primatrix, Theraskin, Graftjacket). Other adjunctive treatments such as hyperbaric oxygen (HBO2) or negative pressure wound therapy (NPWT) were allowed.
Data collection
Data were obtained from the WoundExpert EMR, which was de-identified consistent with the terms and conditions of the Health Insurance Portability and Accountability Act of 1996. Net Health (PA, USA) provided all treatment records for any patient receiving at least one application of HFDS or vCPM in a 5-year period between July 2013 and July 2018 from 242 centers with contracted agreements for the transfer of de-identified data for research purposes. Treatment records included patient baseline demographics, baseline wound characteristics such as age (years, ≤89 per HIPAA), sex, race, wound location, wound size and duration, and other wound-specific information recorded at each visit including area measurements and treatments.
Statistical analyses
Descriptive data were expressed as mean (standard deviation [SD]) and median for continuous variables and n (%) for categorical variables. The level of p < 0.05 was established for the purpose of defining statistical significance. Baseline patient, wound and treatment characteristics were compared between treatment groups in the following manner: normal theory variables used the two-sample t-test, other continuous variables used the Mann–Whitney–Wilcoxon test and categorical variables used the Chi-square test. The primary analysis comparing incidence of and median time to CWC were determined by Kaplan-Meier analysis with a two-tailed log–rank test. Averages for the treatment group were applied for missing data. The hazard ratio (HR) along with its 95% confidence interval (CI) and p-value were based on a Cox proportional hazards regression model with terms for treatment group and baseline wound area as a continuous variable.
Results
In 242 wound care facilities across the USA over a 5-year period, a total of 1498 patients with 1622 refractory DFUs, as defined by failure to have >50% reduction in size in the 4 weeks prior to treatment with surface areas between 1 and 40 cm2, were analyzed for CWC. Cox model-derived estimates of CWC for HFDS (1321 patients having 1444 wounds) were compared with vCPM (177 patients having 178 wounds).
There were no significant differences in baseline patient demographics and wound characteristics between the two treatment groups, except for number of wounds per patient and baseline ulcer duration (Tables 1 & 2). The majority of patients was male (68.1%) and Caucasian (75.8%) The median BMI was 32 (body mass index in kg/m2), and the median age was 62 years. At the first treatment application, the median wound area was 7.23 cm2 in the HFDS group and 6.43 cm2 in the vCPM group with the majority of ulcers being located at the foot. The median wound duration was 4.63 months in the HFDS group and 6.13 months in the vCPM groups.
| Patient characteristic | HFDS (n = 1321) | vCPM (n = 177) | p-value |
|---|---|---|---|
| Age (years), n – Mean ± SD – Median | 1317 62.0 ± 12.4 62.0 | 177 62.0 ± 12.0 62.0 | 0.915 |
| Sex, n (%) – Female – Male | 1305 427 (32.7) 878 (67.3) | 176 45 (25.6) 131 (74.4) | 0.056 |
| Body mass index (kg/m2), n – Mean ± SD – Median | 923 33.22 ± 8.11 32.06 | 159 32.27 ± 7.49 31.71 | 0.189 |
| Number of wounds per patient, n – Mean ± SD – Median | 1321 1.49 ± 1.01 1.0 | 177 1.24 ± 0.89 1.0 | <0.001 |
| Single/multiple wounds per patient, n (%) – Single wound – Multiple wounds | 1321 946 (71.6) 375 (28.4) | 177 151 (85.3) 026 (14.7) | <0.001 |
HFDS: Human fibroblast-derived dermal substitute; SD: Standard deviation; vCPM: Viable cryopreserved placental membrane.
| Wound characteristic | HFDS (n = 1444) | vCPM (n = 178) | p-value |
|---|---|---|---|
| Wound area (cm2), n – Mean ± SD – Median | 1444 7.23 ± 7.74 4.00 | 178 6.43 ± 6.73 3.60 | 0.557 |
| Wound duration (months), n – Mean ± SD – Median | 1153 8.97 ± 14.96 4.63 | 124 11.54 ± 19.30 6.13 | 0.011 |
| Wound depth (mm), n – Mean ± SD – Median | 1424 4.0 ± 5.9 2.0 | 178 4.5 ± 4.59 3.0 | 0.892 |
| Wound location, n (%) – Foot – Heel – Toes – Metatarsal heads – Other | 1444 785 (54.4) 367 (25.4) 179 (12.4) 97 (6.7) 16 (1.1) | 178 93 (52.2) 49 (25.7) 21 (11.8) 13 (7.3) 2 (1.1) | 0.970 |
HFDS: Human fibroblast-derived dermal substitute; SD: Standard deviation; vCPM: Viable cryopreserved placental membrane.
The average number of treatment applications used in the HFDS-treated wounds was 4.91 versus 4.63 for vCPM-treated wounds (Table 3). A total of 17.2% of HFDS patients received a single application, and 82.8% received multiple applications. 24.2% of vCPM patients received a single application and 75.8% received multiple applications. For patients receiving multiple applications, the median interval between applications was 9.0 days for both groups. Treatment with HBO2 or NPWT in both the pretreatment phase (28 days prior to initial treatment) and treatment phase (day 0 to last follow-up visit) of the study occurred at rates of <24% for HBO and <4% for NPWT (Table 3).
| Treatment Characteristic | HFDS (n = 1444) | vCPM (n = 178) | p-value |
|---|---|---|---|
| Number of treatment applications – Mean ± SD – Median | 1444 4.91 ± 3.33 4.0 | 178 4.63 ± 3.87 3.50 | 0.015 |
| Interval between application (days), n – Mean ± SD – Median | 1196 13.8 ± 15.4 9.0 | 135 14.0 ± 17.9 9.0 | 0.791 |
| Single/multiple applications, n (% patients) – Single – Multiple | 1444 248 (17.2%) 1196 (82.8%) | 178 43 (24.2%) 135 (75.8%) | 0.053 |
| Other treatments, n (% patients) HBO2 – Day -28 to day 0 – Day 0 to last follow-up visit NPWT – Day -28 to day 0 – Day 0 to last follow-up visit | 1321 269 (20.4) 320 (24.2) 45 (3.4) 39 (3.0) | 177 21 (11.9) 25 (14.1) 0 (0.0) 0 (0.0) | 0.007 0.003 0.013 0.021 |
HBO2: Hyperbaric oxygen; HFDS: Human fibroblast-derived dermal substitute; NPWT: Negative pressure wound therapy; SD: Standard deviation; vCPM: Viable cryopreserved placental membrane.
Cox Proportional Hazards Regression adjusted data calculating time to CWC and frequency of CWC was performed using all available data up to 36 months. The Cox regression model included terms for treatment, and baseline wound area as covariates. The analysis showed HFDS treatment significantly accelerated the median time to CWC by 55%, achieving the end point 16 weeks sooner when compared with the vCPM-treated patients (20 weeks for HFDS vs 36 weeks for vCPM, p = 0.0002; Figure 1). The estimated frequency of CWC for HFDS compared with vCPM was significantly improved at every timepoint throughout the study. HFDS demonstrated superiority in achieving CWC compared with vCPM at weeks 12 (31 vs 26%), 24 (50 vs 41%) and 36 (61 vs 46%), respectively (p = 0.0002; Figure 2). HFDS treatment significantly increased the probability of wound healing by 60% compared with vCPM treatment showing an HR = 1.60 (95% CI: 1.25, 2.06; p = 0.0002).
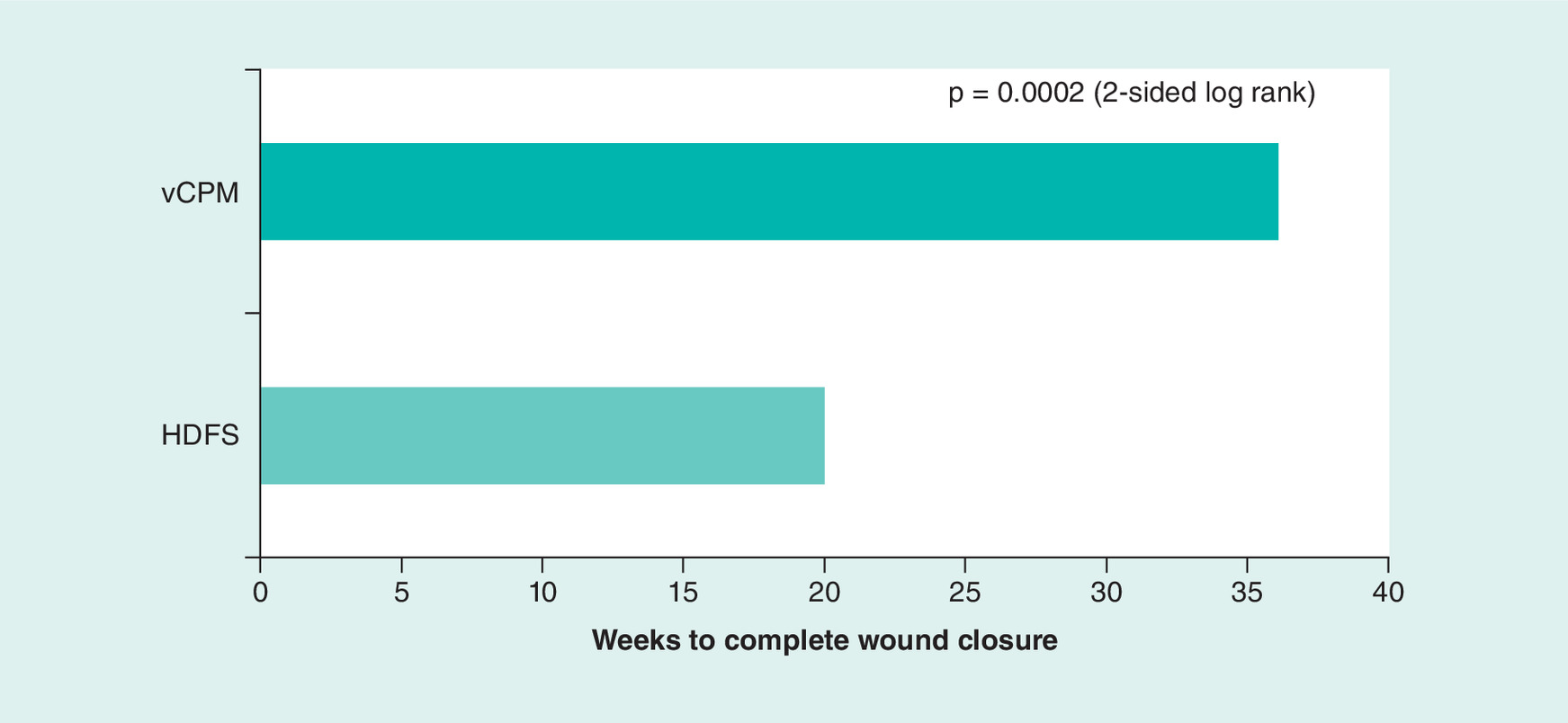
Figure 1. Median time to complete wound closure.
HFDS: Human fibroblast-derived dermal substitute; vCPM: Viable cryopreserved placental membrane.
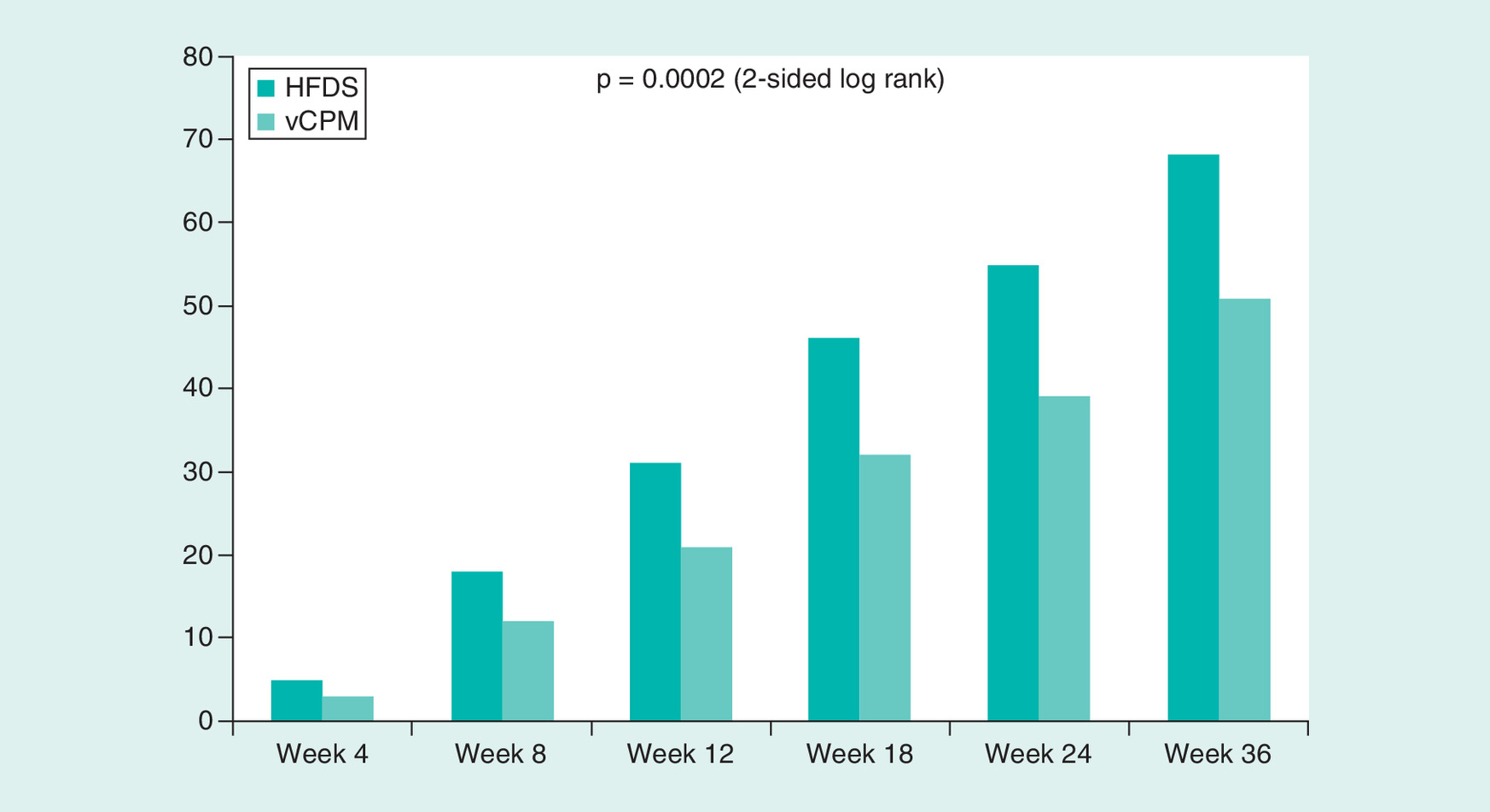
Figure 2. Frequency of complete wound closure.
HFDS: Human fibroblast-derived dermal substitute; vCPM: Viable cryopreserved placental membrane.
There were no significant differences between treatment groups in wound related adverse events (AEs) or serious adverse events (SAEs). All AEs were spontaneously reported by the wound care facility.
Discussion
To our knowledge, this is the first comparative effectiveness study to evaluate HFDS and vCPM for the treatment of DFUs. We found that use of HFDS closed significantly more DFUs and in less time compared with vCPM. Overall, HFDS increased the probability of healing by 60% compared with vCPM.
CER is defined by the practical goal of informing healthcare decisions through comparisons of credible, alternative interventions in a representative study population. The Institute of Medicine (2009) issued findings to set priorities for national CER standards that would support better decision making about interventions in healthcare [30]. The report highlighted the need to perform comparisons of interventions among patients in typical patient care settings and to focus resources on promising approaches [31]. Nevertheless, there are relatively few CER studies and fewer CER studies in the field of wound care to provide real-word data to help guide wound care clinicians.
CER studies differ from traditional efficacy trials. Efficacy trials are typically RCTs designed to prove that a product works. They are designed to operate under a highly controlled environment to optimize the probability of showing a difference between the investigational treatment and a comparator [29]. Inclusion and exclusion criteria are developed to select for homogenous populations that may not represent the entire patient population that suffers from the medical disorder under study. Protocol restrictions in RCTs which may maximize the likelihood of demonstrating study efficacy may also make trial results less than optimal for predicting real-world effectiveness. Products that demonstrate efficacy in RCTs may perform differently in routine clinical practice where variations in patient comorbidities, concomitant medications, compliance with treatment regimens, adjunctive therapies and other unexpected factors can significantly impact the net benefits of a chosen therapy [32,33]. In contrast, CER studies are designed to evaluate the real-world applicability of a product and a comparator that reflect a much more generalizable and diverse range of patients. When results are consistent between RCTs and CER studies, the evidence is generally considered strong [34,35].
The effectiveness results for HFDS in the current EMR analysis demonstrated superiority and supported the efficacy results from its pivotal RCT in DFUs [12]. In the pivotal trial, Marston et al. reported that 30% of ulcers treated with HFDS plus standard care healed at the end of 12 weeks. In the current analysis, 31% of ulcers healed at 12 weeks with HFDS treatment. In contrast, the effectiveness results for vCPM were somewhat different from its published prospective clinical study [19,21,22]. In the reported RCT multicenter study to treat DFUs, vCPM plus standard care therapy was found to heal 62% of wounds by 12 weeks. This is much higher than that reported in the current CER analysis, which found a healing rate of 21% at 12 weeks with vCPM.
For the primary effectiveness end points, HFDS was found to be more effective and accelerated CWC when compared with vCPM. Possible explanations include differences in the manufacturing processes, cell populations present in the two products, chemokine profiles/concentrations and percentage recovery of viable cells delivered to the site of the wound. HFDS is a bioengineered dermal substitute containing high concentrations of living human fibroblasts whereas vCPM contains collagen, ECM proteins, trophoblasts and other mesenchymal stem cells. Fibroblasts play a critically important role in the wound healing process, being present from the late inflammatory phase through full epithelialization and remodeling [23,36–38]. Within several days of injury, fibroblasts migrate into wound sites to synthesize and deposit collagen and ECM proteins which ultimately serve as the scaffold and provide the tensile strength for angiogenesis. Fibroblasts also secrete a variety of cytokines and growth factors in the normal wound healing process. However, the fibroblasts of patients with diabetes may be phenotypically altered and impaired [23]. Evidence suggests that fibroblasts isolated from DFUs are senescent, having been shown to have a decreased proliferative response to growth factors [39]. The fibroblasts in HFDS have been shown to produce human collagen, various ECM proteins and a wide variety of cytokines and growth factors, including PDGF-A, KGF and VEGF [16]. Thus, whereas vCPM may provide extracellular collagen-rich matrix proteins, a unique profile of cytokines, a scaffold to support the healing process and a complex array of cellular components, it may be that in addition to providing structure and mechanical support HFDS improves and accelerates healing by delivering healthy living fibroblasts in high concentrations that actively produce and elaborate essential bioactive proteins to the wound bed.
This study is among a series of retrospective analyses [40,41] that assessed comparative effectiveness between skin substitutes using the WoundExpert EMR database. One study involved the treatment of DFUs and compared another living cellular versus a nonviable skin substitute [42]. The other study was specific to the treatment of venous leg ulcers [41]. In Kirsner et al., the effectiveness of a bioengineered living cellular construct (BLCC; Apligraf; Organogenesis Inc., MA, USA) was compared with dehydrated human amniotic allograft (dHACM; Epifix; MiMedx Group Inc., GA, USA) [40]. Like HFDS, BLCC is approved as a wound treatment. It is comprised of living human neonatal keratinocytes and fibroblasts in an ECM. dHACM is a collagenous covering with no living cells and is derived from donated human placenta. The analysis found that the skin substitute containing living human cells was more effective in healing DFUs than the nonviable comparator. At 12 weeks, the frequency of wound closure with BLCC was 48 versus 28% with dHACM. At 24 weeks, the proportions of wound closure were 72 versus 47%, respectively. In addition, BLCC treatment significantly improved the median time to DFU wound closure by 49% (13.3 weeks vs 26 weeks). These results are comparable to the results reported in this current study with HFDS. Notably, the analysis done in this study included more HFDS-treated patients (n = 1321) and vCPM-treated patients (n = 177) than the number of BLCC-treated patients (n = 155) and dHACM-treated patients (n = 63) in the Kirsner et al. study [40].
Healing of DFUs is impacted by patients' comorbidities. Peripheral neuropathy and/or peripheral arterial disease act as risk factors associated with nonhealing. DFUs can be categorized as purely neuropathic, purely ischemic, or a combination of the two, neuroischemic [43,44]. The estimated prevalence of each is 35, 15 and 50%, respectively [45]. In this study, multiple ulcers per patient were reported at a greater rate in the HFDS group (28.4%) compared with the vCPM group (14.7%); p < 0.001. Using national databases (2006–2012); 443 HFDS-treated DFU patients showed a prevalence of peripheral arterial disease of 64.8% [9,46]. Using real-world data from a recent CER study, 360 vCPM-treated DFU patients showed a prevalence of peripheral artery disease of 11.4% [47]. These data are consistent with the demonstrated effectiveness of HFDS on hard to heal DFUs.
While the EMR database in this study did not capture costs related to wound care and outcomes, the significant differences in incidence and time to healing in this study suggest potential cost savings with HFDS. DFUs comprise a costly burden to the medical health system, owing to the substantial costs and resource use related to care, including home health, prescription drugs, physician office visits, emergency department visits and hospitalizations. Compared with non-DFU controls, the average annual incremental cost of treating a patient with DFU is approximately $14,000 USD [9]. The potential cost savings may be even greater if one were to compare against standard care therapy alone. In a recent economic outcome analysis which evaluated Medicare administrative claims data, patients with DFUs who received HFDS had fewer lower limb amputations (-22%), fewer emergency department visits (-25%) and fewer days hospitalized when compared with matched conventional care counterparts (-42%) [48]. Consequently, this translated to a nearly $7000 USD lower per-patient average healthcare costs during the 18-month follow-up. Although patients treated with HFDS incurred greater costs of direct treatment and greater intensity of physician office services, these costs were offset by reductions in lower-limb amputations and other resource use, especially inpatient services. In a post-hoc analysis of the pivotal trial AE data, the incidence of ulcer-related amputation or bone resection was significantly lower in patients who received HFDS versus conventional care (5.5 vs 12.6%, respectively; p = 0.031) [14].
The limitations of this study include those inherent to retrospective data collection and analyses. The Net Health database was not designed specifically for research purposes, and as such, there may be missing data. The database provides consistent and reliably filled out data on patient characteristics, wound areas over time, other clinically meaningful wound and treatment characteristics making this database ideal for assessing CWC outcomes. However, completion of patient-level medical history data such as comorbidities, prior surgeries or concomitant medications varied across centers making analyses of certain subgroups difficult. Specifics regarding the off-loading techniques, methods of debridement, or use of other standard care therapies may not have been completely captured. Safety-related outcomes or AEs were captured by spontaneous AE reporting and not by active data collection. All safety-related outcomes (AEs, SAEs), ulcer recurrence and amputations were difficult to be coded and analyzed. This is a limitation of this study and study design. Emergency room visits, hospitalizations and patient-reported outcomes were not able to be reported given the coded data available. Lastly, given the lack of randomization, there is a possibility of bias in selection of patients for HFDS or vCPM at participating centers. However, given the number of wounds and centers providing information for the analysis, it is less likely that a uniform bias was present affecting study results.
It should be noted that the purpose of this CER did not include drawing any clinically meaningful conclusions regarding any individual patient subgroup. Such analyses would have required larger patient numbers in the subgroup of interest. It is important to draw attention to the fact that the use of adjunctive therapies was permitted in this CER study, and that the study was designed with the objective of capturing real-world treatment practices and long-term clinical outcomes. Because the purpose of the study was not to examine the effectiveness of HBO2 or NPWT for example, the study was not properly powered to examine effects of these adjunctive therapies. Nevertheless, given clinical thinking that HBO2 and NPWT may improve healing outcomes, exploratory Cox analyses were performed that adjusted for HBO2 and NPWT as covariates. These adjusted analyses showed that neither HBO2 nor NPWT had significant effects on CWC end points reported in this CER study. Future prospective RCTs are recommended to provide more systematic opportunities to perform subgroup analyses and specific analyses of the effectiveness of various adjunctive therapies to treat DFUs.
Conclusion
These real-world data showed that HFDS compared with vCPM significantly improved the probability, speed and the incidence of complete wound closure in DFUs. These results are comparable to and further support the efficacy data from the pivotal RCT for HFDS. These data provide additional information to inform treatment algorithms for the management of DFUs.
•
This was the first comparative effectiveness research study that compares the clinical outcomes of a human fibroblast-derived dermal substitute (HFDS) and a viable cryopreserved placental membrane (vCPM) for the treatment of diabetic foot ulcers (DFUs) in a real-world setting.
•
Treatment with HFDS significantly improved the incidence and speed of DFU wound closure compared with vCPM.
•
The incidence of wound closure was superior with HFDS versus vCPM at weeks 12 (31 vs 26%), 24 (50 vs 41%) and 36 (61 vs 46%), respectively (p = 0.0002).
•
HFDS demonstrated accelerated time to wound closure of 55%, a 16-week improvement compared with vCPM.
•
HFDS showed a 60% greater probability of wound closure when compared with vCPM.
•
Improvements in the probability, speed and the incidence of wound closure in DFUs treated with HFDS confirm clinical effectiveness and support potential cost saving benefits.
•
Comparative effectiveness research is defined by the practical goal of informing healthcare decisions through comparisons of credible, alternative interventions in a representative study population.
•
Comparative effectiveness research studies of real-world data provide meaningful information to inform treatment algorithms for the management DFUs.
Financial & competing interests disclosure
This study was funded by Organogenesis, Inc. ML Sabolinski, serves as managing member of Sabolinski LLC., MA, USA. ML Sabolinski serves as a consultant for Organogenesis Inc. JV Capotuto is a pediatric endocrinologist and co-founder of RestorixHealth. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
De-identified patient data released to Organogenesis, Inc. were consistent with the terms and conditions of Net Health's client contracts and the requirements of the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Net Health was not involved in the analysis, interpretation or reporting of the data.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: •• of considerable interest
1.
American Diabetes Association AD. Economic costs of diabetes in the U.S. in 2012. Diabetes Care 36(4), 1033–1046 (2013).
2.
Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA 293(2), 217–228 (2005).
3.
Margolis DJ, Malay DS, Hoffstad OJ et al. Incidence of diabetic foot ulcer and lower extremity amputation among Medicare beneficiaries, 2006 to 2008: Data Points #2 (2011). http://www.ncbi.nlm.nih.gov/pubmed/22049565
4.
Margolis DJ, Malay DS, Hoffstad OJ et al. Prevalence of diabetes, diabetic foot ulcer, and lower extremity amputation among Medicare beneficiaries, 2006 to 2008: Data Points #1 (2011). http://www.ncbi.nlm.nih.gov/pubmed/22049561
5.
Frykberg RG, Zgonis T, Armstrong DG et al. Diabetic Foot Disorders: A Clinical Practice Guideline (2006 revision) (2006). https://www.acfas.org/uploadedFiles/Healthcare_Community/Education_and_Publications/Clinical_Practice_Guidelines/Introduction.pdf
6.
Gordois A, Scuffham P, Shearer A, Oglesby A, Tobian JA. The health care costs of diabetic peripheral neuropathy in the US. Diabetes Care 26(6), 1790–1795 (2003).
7.
Armstrong DG, Wrobel J, Robbins JM. Guest Editorial: are diabetes-related wounds and amputations worse than cancer? Int. Wound J. 4(4), 286–287 (2007).
8.
Lavery LA, Armstrong DG, Wunderlich RP, Mohler MJ, Wendel CS, Lipsky BA. Risk factors for foot infections in individuals with diabetes. Diabetes Care 29(6), 1288–1293 (2006).
9.
Rice JB, Desai U, Cummings AKG, Birnbaum HG, Skornicki M, Parsons NB. Burden of diabetic foot ulcers for medicare and private insurers. Diabetes Care 37(3), 651–658 (2014).
10.
Margolis DJ, Kantor J, Berlin JA. Healing of diabetic neuropathic foot ulcers receiving standard treatment. A meta-analysis. Diabetes Care 22(5), 692–695 (1999).
11.
Lavery LA, Davis KE, Berriman SJ et al. WHS guidelines update: diabetic foot ulcer treatment guidelines. Wound Repair Regen. 24(1), 112–26 (2016).
12.
Marston WA, Hanft J, Norwood P, Pollak R, Dermagraft Diabetic Foot Ulcer Study Group. The efficacy and safety of Dermagraft in improving the healing of chronic diabetic foot ulcers: results of a prospective randomized trial. Diabetes Care 26(6), 1701–1705 (2003).
•• Landmark study of the treatment of diabetic foot ulcers (DFUs) with a bioengineered living human fibroblast derived substitute (HFDS) versus Standard of Care (SOC).
13.
Gentzkow GD, Iwasaki SD, Hershon KS et al. Use of dermagraft, a cultured human dermis, to treat diabetic foot ulcers. Diabetes Care 19(4), 350–354 (1996).
14.
Frykberg RG, Marston WA, Cardinal M. The incidence of lower-extremity amputation and bone resection in diabetic foot ulcer patients treated with a human fibroblast-derived dermal substitute. Adv. Skin Wound Care 28(1), 17–20 (2015).
15.
Genzkow GD, Jensen JL, Pollak RA et al. Improved healing of diabetic foot ulcers after grafting with a living human dermal replacement. Wounds 11, 77–84 (1999).
16.
Roberts C, Mansbridge J. The scientific basis and differentiating features of Dermagraft. Can. J. Plast. Surg. 10(Suppl. A), 6A–13A (2002).
17.
Naughton G, Mansbridge J, Gentzkow G. A metabolically active human dermal replacement for the treatment of diabetic foot ulcers. Artif. Organs 21(11), 1203–1210 (2008).
18.
Harding K, Sumner M, Cardinal M. A prospective, multicentre, randomised controlled study of human fibroblast-derived dermal substitute (Dermagraft) in patients with venous leg ulcers. Int. Wound J. 10(2), 132–137 (2013).
19.
Raspovic KM, Wukich DK, Naiman DQ et al. Effectiveness of viable cryopreserved placental membranes for management of diabetic foot ulcers in a real world setting. Wound Repair Regen. 26(2), 213–220 (2018).
20.
Johnson EL, Marshall JT, Michael GM. A comparative outcomes analysis evaluating clinical effectiveness in two different human placental membrane products for wound management. Wound Repair Regen. 25(1), 145–149 (2017).
21.
Ananian CE, Dhillon YS, Van Gils CC et al. A multicenter, randomized, single-blind trial comparing the efficacy of viable cryopreserved placental membrane to human fibroblast-derived dermal substitute for the treatment of chronic diabetic foot ulcers. Wound Repair Regen. 26(3), 274–283 (2018).
22.
Lavery LA, Fulmer J, Shebetka KA et al. The efficacy and safety of Grafix® for the treatment of chronic diabetic foot ulcers: results of a multi-centre, controlled, randomised, blinded, clinical trial. Int. Wound J. 11(5), 554–560 (2014).
23.
Falanga V. Wound healing and its impairment in the diabetic foot. Lancet (London, England) 366(9498), 1736–1743 (2005).
24.
Niknejad H, Peirovi H, Jorjani M, Ahmadiani A, Ghanavi J, Seifalian AM. Properties of the amniotic membrane for potential use in tissue engineering. Eur. Cell. Mater. 15, 88–99 (2008).
25.
Maxson S, Lopez EA, Yoo D, Danilkovitch-Miagkova A, Leroux MA. Concise review: role of mesenchymal stem cells in wound repair. Stem Cells Transl. Med. 1(2), 142–149 (2012).
26.
Dermagraft® Directions For Use. http://www.dermagraft.com/home/wp-content/uploads/sites/1/Dermagraft_Directions_for_Use.pdf
27.
Gibbons GW. Grafix®, a cryopreserved placental membrane, for the treatment of chronic/stalled wounds. Adv. Wound Care 4(9), 534–544 (2015).
28.
Berger ML, Mamdani M, Atkins D, Johnson ML. Good research practices for comparative effectiveness research: defining, reporting and interpreting nonrandomized studies of treatment effects using secondary data sources: the ISPOR Good Research Practices for Retrospective Database Analysis Task Force Report–Part I. Value Health 12(8), 1044–1052 (2009).
29.
Eaglstein WH, Kirsner RS. Expectations for comparative effectiveness and efficacy research. JAMA Dermatol. 149(1), 18 (2013).
30.
Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research. National Academies Press, DC, USA. http://www.nap.edu/catalog/12648
31.
Sox HC, Greenfield S. Comparative effectiveness research: a report from the Institute of Medicine. Ann. Intern. Med. 151(3), 203–205 (2009).
32.
Berger ML, Mamdani M, Atkins D, Johnson ML. Good research practices for comparative effectiveness research: defining, reporting and interpreting nonrandomized studies of treatment effects using secondary data sources: the ISPOR Good Research Practices for Retrospective Database Analysis Task Force Report–Part I. Value Health 12(8), 1044–1052 (2009).
33.
Velentgas P, Dreyer NA, Nourjah P, Smith SR, Torchia MM. Developing a Protocol for Observational Comparative Effectiveness Research: A User's Guide . Agency for Healthcare Research and Quality, USA. http://www.ncbi.nlm.nih.gov/pubmed/23469377
34.
Wound Care HER, Net Health (2018). https://www.nethealth.com/products/wound-care/woundexpert-software-wound-care-ehr/
35.
Velentgas P, Dreyer NA, Nourjah P, Smith SR, Torchia MM. Developing a Protocol for Observational Comparative Effectiveness Research: A User's Guide . Agency for Healthcare Research and Quality, USA. http://www.ncbi.nlm.nih.gov/pubmed/23469377
36.
Hunt TK, Hopf H, Hussain Z. Physiology of wound healing. Adv. Skin Wound Care 13(2 Suppl.), 6–11 (2000).
37.
Bainbridge P. Wound healing and the role of fibroblasts. J. Wound Care 22(8), 407–412 (2013).
38.
Broughton G, Janis JE, Attinger CE. The basic science of wound healing. Plast. Reconstr. Surg. 117(7 Suppl.), 12S–34S (2006).
39.
Loots MA, Lamme EN, Zeegelaar J, Mekkes JR, Bos JD, Middelkoop E. Differences in cellular infiltrate and extracellular matrix of chronic diabetic and venous ulcers versus acute wounds. J. Invest. Dermatol. 111(5), 850–857 (1998).
40.
Kirsner RS, Sabolinski ML, Parsons NB, Skornicki M, Marston WA. Comparative effectiveness of a bioengineered living cellular construct vs. a dehydrated human amniotic membrane allograft for the treatment of diabetic foot ulcers in a real world setting. Wound Repair Regen. 23(5), 737–744 (2015).
41.
Marston WA, Sabolinski ML, Parsons NB, Kirsner RS. Comparative effectiveness of a bilayered living cellular construct and a porcine collagen wound dressing in the treatment of venous leg ulcers. Wound Repair Regen. 22(3), 334–340 (2014).
42.
Kirsner RS, Sabolinski ML, Parsons NB, Skornicki M, Marston WA. Comparative effectiveness of a bioengineered living cellular construct vs. a dehydrated human amniotic membrane allograft for the treatment of diabetic foot ulcers in a real world setting. Wound Repair Regen. 23(5), 737–744 (2015).
•• Provides Comparative Effectiveness Research study data for the treatment of DFUs with a bioengineered living cellular technology versus Standard of Care (SOC).
43.
Armstrong DG, Lavery LA, Harkless LB. Validation of a diabetic wound classification system: the contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care 21(5), 855–859 (1998).
44.
Amin N, Doupis J. Diabetic foot disease: from the evaluation of the “foot at risk” to the novel diabetic ulcer treatment modalities. World J. Diabetes. 7(7), 153–164 (2016).
45.
Armstrong DG, Cohen K, Courric S, Bharara M, Marston W. Diabetic foot ulcers and vascular insufficiency: our population has changed, but our methods have not. J. Diabetes Sci. Technol. 5(6), 1591–1595 (2011).
46.
Rice JB, Desai U, Ristovska L et al. Economic outcomes among Medicare patients receiving bioengineered cellular technologies for treatment of diabetic foot ulcers. J. Med. Econ. 18(8), 586–595 (2015).
•• Provides a detailed analysis of the costs of treating nonhealed diabetic foot ulcers.
47.
Raspovic KM, Wukich DK, Naiman DQ et al. Effectiveness of viable cryopreserved placental membranes for management of diabetic foot ulcers in a real world setting. Wound Repair Regen. 26(2), 213–220 (2018).
48.
Rice JB, Desai U, Ristovska L et al. Economic outcomes among Medicare patients receiving bioengineered cellular technologies for treatment of diabetic foot ulcers. J. Med. Econ. 18(8), 586–595 (2015).
Information & Authors
Information
Published In
Pages: 1229 - 1238
PubMed: 31407588
Copyright
© 2019 Michael L Sabolinski.
History
Received: 2 January 2019
Accepted: 29 July 2019
Published online: 13 August 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of a human fibroblast-derived dermal substitute and a viable cryopreserved placental membrane for the treatment of diabetic foot ulcers. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0001
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ying Zhou, Hongbo Yu, Lingfeng Yin, Yudong Fang, Qintong Yang, Zhe Liu, Lei Xu, A combination of compound phellodendron liquid and infrared irradiation in patients with diabetic foot, Journal of Radiation Research and Applied Sciences, 10.1016/j.jrras.2025.102001, 18, 4, (102001), (2025).
- Poonam Tapsale, Vishal Kadam, Onkar Lande, Madan S. Hardikar, Nitin Chaudhari, A prospective observational study on management approaches for non-healing ulcers in dermatology: From conventional to advanced modalities., undefined, 10.51168/sjhrafrica.v6i9.2149, (2025).
- Michael L Sabolinski, Tad Archambault, Real-world data analysis of bilayered living cellular construct and fetal bovine collagen dressing treatment for pressure injuries: a comparative effectiveness study, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0109, 13, 4, (2024).
- Boram Kim, EunAh Lee, Cryopreservation of engineered tissues and organoids, Organoid, 10.51335/organoid.2023.3.e15, 3, (e15), (2023).
- Francisca Sousa Lima, Maria Girlane Sousa Albuquerque Brandão, Dara Cesario Oliveira, Aline de Oliveira Ramalho, Anne Fayma Lopes Chaves, Thiago Moura de Araújo, Vivian Saraiva Veras, UTILIZAÇÃO DA PLACENTA HUMANA NA CICATRIZAÇÃO DE ÚLCERAS NOS PÉS DE PESSOAS COM DIABETES: REVISÃO INTEGRATIVA, ESTIMA, Brazilian Journal of Enterostomal Therapy, 10.30886/estima.v20.1238_PT, (2022).
- Francisca Sousa Lima, Maria Girlane Sousa Albuquerque Brandão, Dara Cesario Oliveira, Aline de Oliveira Ramalho, Anne Fayma Lopes Chaves, Thiago Moura de Araújo, Vivian Saraiva Veras, USE OF THE HUMAN PLACENTA IN THE HEALING OF FOOT ULCERS IN PEOPLE WITH DIABETES: INTEGRATIVE REVIEW, ESTIMA, Brazilian Journal of Enterostomal Therapy, 10.30886/estima.v20.1238_IN, (2022).
- Steven L. Stuto, Crystal L. Ramanujam, Thomas Zgonis, Soft Tissue and Osseous Substitutes for the Diabetic Foot, Clinics in Podiatric Medicine and Surgery, 10.1016/j.cpm.2021.11.006, 39, 2, (343-350), (2022).
- Meilang Xue, Ruilong Zhao, Lyn March, Christopher Jackson, Dermal Fibroblast Heterogeneity and Its Contribution to the Skin Repair and Regeneration, Advances in Wound Care, 10.1089/wound.2020.1287, 11, 2, (87-107), (2021).
- Irina Arutyunyan, Andrey Elchaninov, Gennady Sukhikh, Timur Fatkhudinov, Cryopreservation of Tissue-Engineered Scaffold-Based Constructs: from Concept to Reality, Stem Cell Reviews and Reports, 10.1007/s12015-021-10299-4, 18, 4, (1234-1252), (2021).
- Davide Vincenzo Verdolino, Helen A. Thomason, Andrea Fotticchia, Sarah Cartmell, Wound dressings: curbing inflammation in chronic wound healing, Emerging Topics in Life Sciences, 10.1042/ETLS20200346, 5, 4, (523-537), (2021).