Cost–effectiveness of standard utilization of zoledronic acid for bone metastases from advanced lung cancer in China
Abstract
Aim: To assess the cost–effectiveness of standard utilization of zoledronic acid (ZA) relative to real-world utilization of ZA for bone metastasis (BM) in Chinese patients with advanced lung cancer. Materials & methods: A decision analytic model was constructed to simulate health benefits and medical costs associated with standard and real-world utilization of ZA for BM in Chinese patients with advanced lung cancer. Results: Compared with real-world utilization of ZA, standard utilization of ZA reduced cumulative risk of skeletal-related events (45.7 vs 63.6%), increased quality-adjusted life years (0.673 vs 0.626 QALY) and saved cumulated medical costs (¥343,163 vs ¥376,943). Conclusion: Standard utilization of ZA dominated real-world utilization of ZA for BM in Chinese patients with advanced lung cancer from cost–effectiveness perspective.
In 2015, 733,300 new lung cancer cases and 610,200 lung cancer-related deaths were reported [1]. Lung cancer management is complicated when the disease becomes metastatic. The most prevalent lung cancer metastasis is bone metastasis (BM), which accounts for approximately 36% of metastatic lung cancer in China [2]. BM may precede skeletal-related events (SREs), which can double mortality risk [3]. Spinal cord compression, which is one of the typical SREs, may reduce the quality of life by 0.22–0.32, depending on the status of paralysis [4]. Additionally, SREs were reported to account for half of the medical costs associated with managing developed BM from lung cancer [5].
Bisphosphonates have been widely reimbursed for their superior effects and attractive cost–effectiveness in treating BM caused by advanced cancers [6,7]. Bisphosphonates are also listed for reimbursement to treat BM in China. However, standard treatment with bisphosphonates for BM in advanced lung cancer patients has been challengeable in some Chinese provinces where the public insurance plans only reimbursed medications prescribed in tertiary care hospital settings. Thus, the real-world utilization of bisphosphonates for BM in Chinese advanced lung cancer patients (average treatment rate: 44.6%; average treatment duration: 3.0 months) is far below the recommended lifetime standard treatment [8]. Thus, this study was designed as a cost–effectiveness analysis using zoledronic acid (ZA), the most prescribed bisphosphonate for BM in China, to address potential loss of health and economic benefits due to the underuse of bisphosphonate for BM in Chinese advanced lung cancer patients.
Materials & methods
This study was a cost–effectiveness analysis using a decision analytic model to assess the health benefits and medical costs associated with two scenarios for the utilization of ZA – standard utilization versus real-world utilization – for BM that developed from advanced lung cancer over a lifetime horizon from the perspective of Chinese healthcare payers.
Constructing decision analytic model
The constructed decision analytic model adapted a Markov model approach to simulate the risk of SREs and mortality associated with the two scenarios for the utilization of ZA (i.e., standard utilization and real-world utilization) in Chinese patients with BM developed from advanced lung cancer. According to the clinical practice guidelines, the standard utilization of ZA was defined as monthly intravenous administration of 4 mg of ZA during the model time horizon, which was set to lifetime. The real-world utilization of ZA was based on the observed treatment rate (44.6%) and treatment duration of bisphosphonates (3.0 months) in Chinese patients with BM and advanced lung cancer [8]. The constructed Markov model included three health states – BM only (without SRE), SRE and death – to simulate the risk of developing SRE from BM under the ZA treatment and the risk of mortality associated with BM only and SRE, respectively. The real-world utilization scenario stratified patients by ZA treatment status; then, the risks of having an SRE occur under ZA treatment and no ZA treatment were simulated, respectively. All Markov models were constructed with a 1-month cycle length to account for the rapid disease progression associated with advanced lung cancer. To follow the Chinese health economic evaluation guideline [9], the constructed decision analytic model discounted survival time, quality-adjusted life years (QALY) and medical costs at 3% per annum. The structure of the decision analytic model is illustrated in Figure 1.
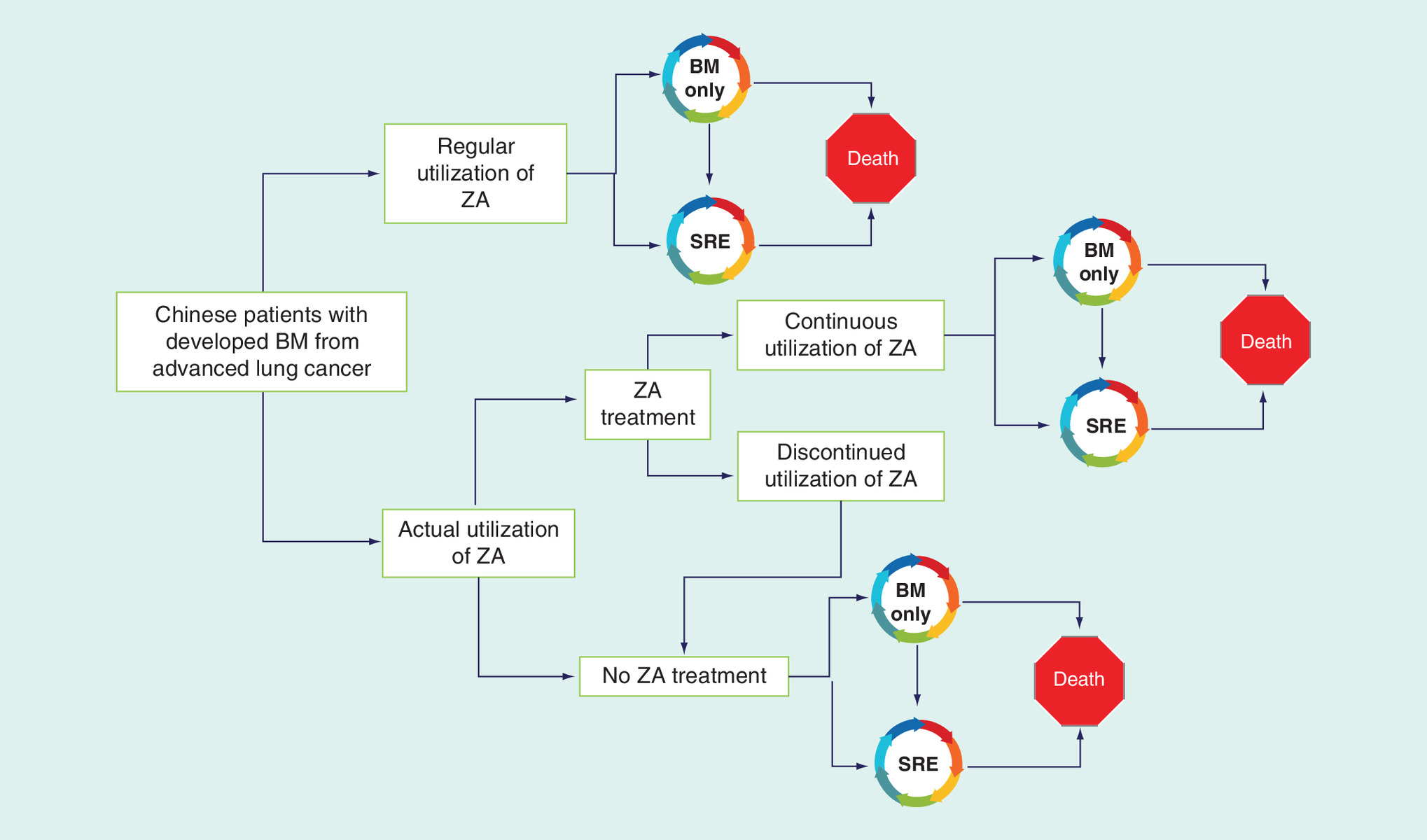
Figure 1. The structure of decision-making model assessing the cost–effectiveness of standard utilization of ZA relative to real-world utilization of ZA for developed bone metastasis from advanced lung cancer in Chinese patients.
BM: Bone metastasis; SRE: Skeletal-related event; ZA: Zoledronic acid.
Estimating model inputs
The literature search was conducted in both Chinese and English bibliographic databases to identify appropriate evidence to estimate monthly risk of SRE from BM under ZA (or no) treatment in patients with advanced lung cancer and the monthly risk of mortality associated with BM only as well as SRE in Chinese patients with advanced lung cancer. The monthly risks of SRE occurrence and mortality were estimated using a survival function formula with an exponential distribution (survival proportion = e-λt, where t is the follow-up time and λ is the hazard rate for the risk of SRE occurrence or mortality). Due to the lack of Chinese utility values associated with BM developed from advanced lung cancer, an empirical estimation of the utility was used [10]. The reported reduction of utility associated with the type of SRE relative to BM only and the reported distribution of SRE types in Chinese patients with developed BM from advanced lung cancer were used to estimate the model variables for utility [11,12]. This study identified a clinical cohort of advanced lung cancer patients with BM in a Chinese tertiary care cancer hospital from 1 January 2012 to 31 December 2015 to track their insurance claims records and estimate monthly medical costs associated with BM only and each SRE type. The estimated model variables are summarized in Table 1.
| Variables | Baseline | 95% CI | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Disease prognosis | ||||
| Median time-to-SRE associated with placebo (month) | 5.6 | 2.8 | 8.3 | |
| Median time-to-SRE associated with ZA (month) | 14 | 6.8 | 21.2 | |
| Median overall survival associated with BM only (month) | 11.7 | 10.6 | 12.8 | |
| Median overall survival associated with SRE (month) | 11 | 2.6 | 19.4 | |
| Monthly risk of SRE associated with placebo | 0.125 | 0.083 | 0.245 | |
| Monthly risk of SRE associated with ZA | 0.05 | 0.033 | 0.102 | |
| Monthly risk of mortality associated with BM only | 0.059 | 0.054 | 0.066 | |
| Monthly risk of mortality associated with SRE | 0.063 | 0.036 | 0.264 | |
| Distribution of SRE types (%) | ||||
| Bone pain | 58.0 | |||
| Bone fracture | 18.0 | |||
| Spinal compression | 35.4 | |||
| Hypercalcemia | 8.0 | |||
| Bone surgery | 22.0 | |||
| Utility | ||||
| BM only | 0.626 | 0.313 | 0.939 | |
| SRE | 0.445 | 0.222 | 0.667 | |
| Actual utilization of ZA | ||||
| Treatment rate (%) | 44.6 | |||
| Treatment duration (months) | 3.0 | |||
| Regular utilization of ZA | ||||
| Treatment rate (%) | 100 | |||
| Treatment duration (months) | 200 | |||
| Medical costs (¥, ¥1 = US$0.15) | ||||
| Unit price of ZA (Zometa, 4 mg) | ¥2,248 | |||
| BM only | ¥12,906 | ¥3,995 | ¥21,818 | |
| Weighted mean costs of SRE | ¥30,041 | ¥7,803 | ¥52,400 | |
BM: Bone metastasis; SRE: Skeletal-related event; ZA: Zoledronic acid.
Cost–effectiveness analysis
The constructed decision analytic model was used to perform the base-case analysis, one-way sensitivity analyses and a probabilistic sensitivity analysis (PSA) for the comparisons between the two ZA utilization scenarios – standard utilization versus real-world utilization – for the cumulated health benefits and medical costs over a lifetime horizon. The base-case analysis was conducted to estimate the point estimations of cumulated risk of SRE, survival time, QALY and lifetime medical costs associated with the two ZA utilization scenarios. The incremental cost–effectiveness ratio (ICER) per gained QALY was calculated using the ratio between the differences in cumulative medical costs and QALY associated with the two model scenarios. One-way sensitivity analyses were performed to assess the uncertainty associated with each model variable on the cost–effectiveness (indicated by ICER per gained QALY) by varying the model variable from the lower limit to the upper limit of its 95% CI or +/- 25% of its baseline value if their 95% CIs were lacking. A Monte Carlo simulation approach was used to perform the PSA by conducting 10,000 iterations under the gamma or beta distributions of model variables. The distribution of the 10,000 simulations of cost–effectiveness was used to identify the median and 95% credible interval of ICER per gained QALY.
This study used R statistical software to estimate the model variables from the identified literature evidence and estimate medical costs associated with BM only or SRE from the claims data. Microsoft Excel 2013 was used to construct the decision analytic model and conduct the cost–effectiveness analysis.
Results
The results of the conducted cost–effectiveness analysis in this study are reported as below for base-case analysis, one-way sensitivity analysis and PSA, respectively.
Base-case analysis
Based on the simulation of the newly developed SRE in each model cycle, the standard utilization of ZA scenario could reduce the lifetime cumulated risk of SRE by 17.9% (45.7 vs 63.6%) when compared with the real-world utilization scenario. The base-case analysis projected more gained QALY (0.673 vs 0.626 QALY) associated with the standard utilization scenario. Based on the illustrated curves for cumulated medical costs associated with health states over time in the model (Figure 2), the standard utilization scenario began costing less than real-world utilization scenario after 6 months simulation. The simulations of medical costs over lifetime model time horizon projected that the standard utilization scenario increased the cumulative medical costs for BM only (¥112,971 vs ¥79,354; difference ¥33,618, ¥1 = US$0.15 as of 14 November 2018) and drug acquisition costs of ZA (¥19,678 vs ¥4,701, difference ¥14,977) but saved more medical costs associated with SRE (¥210,514 vs ¥292,880, difference -¥82,366) over a lifetime horizon. Thus, the standard utilization scenario saved ¥33,771 in cumulated medical costs when compared with the real-world utilization scenario (¥ 343,163 vs ¥ 376,934). The standard utilization scenario dominated the real-world utilization scenario by gaining more health benefits and saving more cumulated medical costs in the base-case analysis. The point estimations of the cumulated health benefits and medical costs associated with the two model scenarios regarding the utilization of ZA for BM developed from advanced lung cancer in Chinese patients are summarized in Table 2.
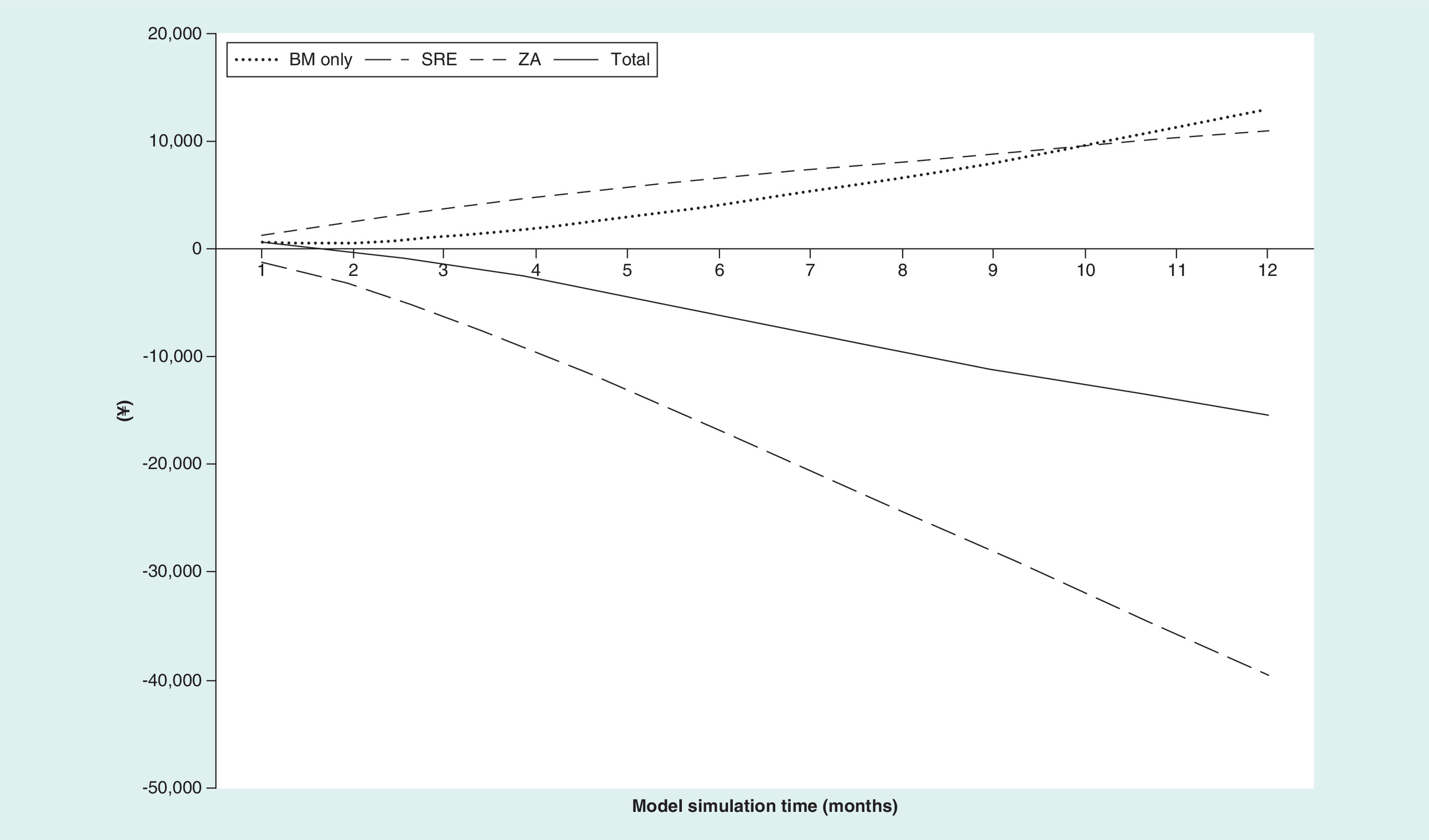
Figure 2. Simulations of cumulated medical costs associated with the two model scenarios for the utilization of zoledronic acid in Chinese patients with bone metastasis developed from advanced lung cancer.
BM: Bone metastasis; SRE: Skeletal-related event; ZA: Zoledronic acid.
| Model scenario | Regular utilization of ZA | Actual utilization of ZA | Difference |
|---|---|---|---|
| Cumulated health outcomes | |||
| – Risk of SRE | 45.7% | 63.6% | -17.9% |
| – Survival time (years) | 1.233 | 1.220 | 0.013 |
| – QALY | 0.673 | 0.626 | 0.047 |
| Cumulated medical costs | |||
| – Drug acquisition costs of ZA | ¥112,971 | ¥79,353 | ¥33,618 |
| – Medical costs associated with BM only | ¥210,514 | ¥292,880 | -¥82,366 |
| – Medical costs associated with SRE | ¥19,678 | ¥4,701 | ¥14,977 |
| – Total costs | ¥343,163 | ¥376,934 | -¥33,771 |
BM: Bone metastasis; QALY: Quality-adjusted life year; SRE: Skeletal-related event; ZA: Zoledronic acid.
One-way sensitivity analyses
One-way sensitivity analyses identified that the utility associated with BM only and the utility of SRE substantially drove up the ICER per gained QALY associated with the standard utilization scenario by ¥958,755 and ¥50,825,320, respectively, when these model values varied from the lower limit to the upper limit of their 95% CIs. Instead, the monthly risk of mortality associated with SRE, the monthly medical costs associated with SRE and the monthly medical costs associated with BM only reduced the ICER per gained QALY by ¥3,385,073, ¥2,603,536 and ¥1,321,895, respectively. The results of the one-way sensitivity analyses are illustrated in Figure 3. Additionally, increasing the ZA treatment rate from 25% and the ZA treatment duration from 6 months in the standard utilization scenario could allow the standard utilization scenario to cost less than the real-world utilization scenario.
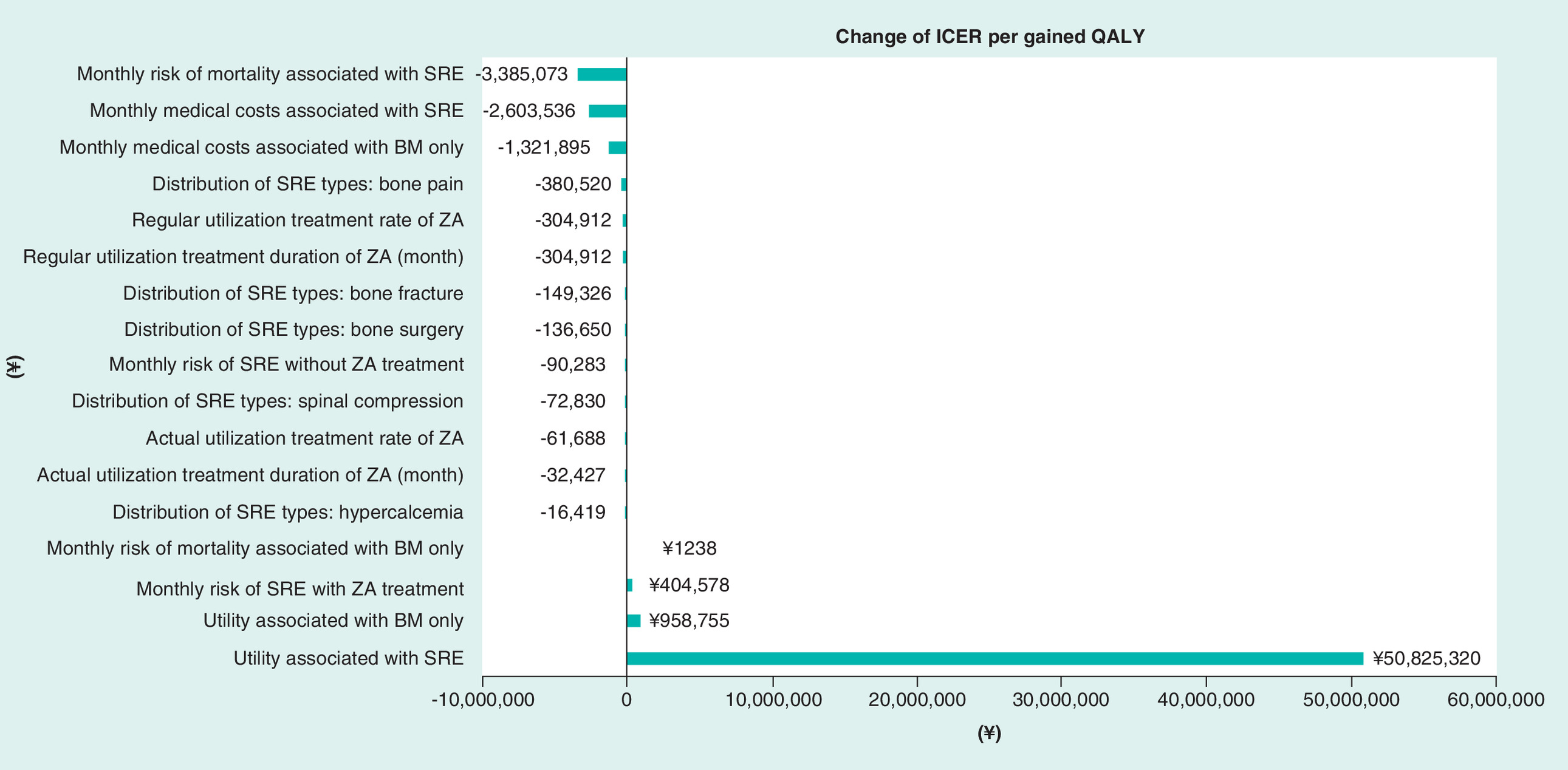
Figure 3. The results of one-way sensitivity analyses assessing the impact of uncertainty associated with model variables on the cost–effectiveness of standard utilization of zoledronic acid relative to real-world utilization of zoledronic acid in Chinese lung cancer patients with bone metastasis.
BM: Bone metastasis; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life years; SRE: Skeletal-related event; ZA: Zoledronic acid.
To further demonstrate the potential health and economic benefits associated with improving the utilization of ZA for developed BM from advanced lung cancer in Chinese patients, the one-way sensitivity analysis assessed the impact of increasing the treatment rate and treatment duration of ZA on the cumulated medical costs in the real-world utilization scenario. Increasing the treatment rate by 10% and the treatment duration by 1 month in the real-world utilization scenario could save ¥2219 and ¥828, respectively, in cumulated medical costs on average during the lifetime model simulation.
Probabilistic sensitivity analysis
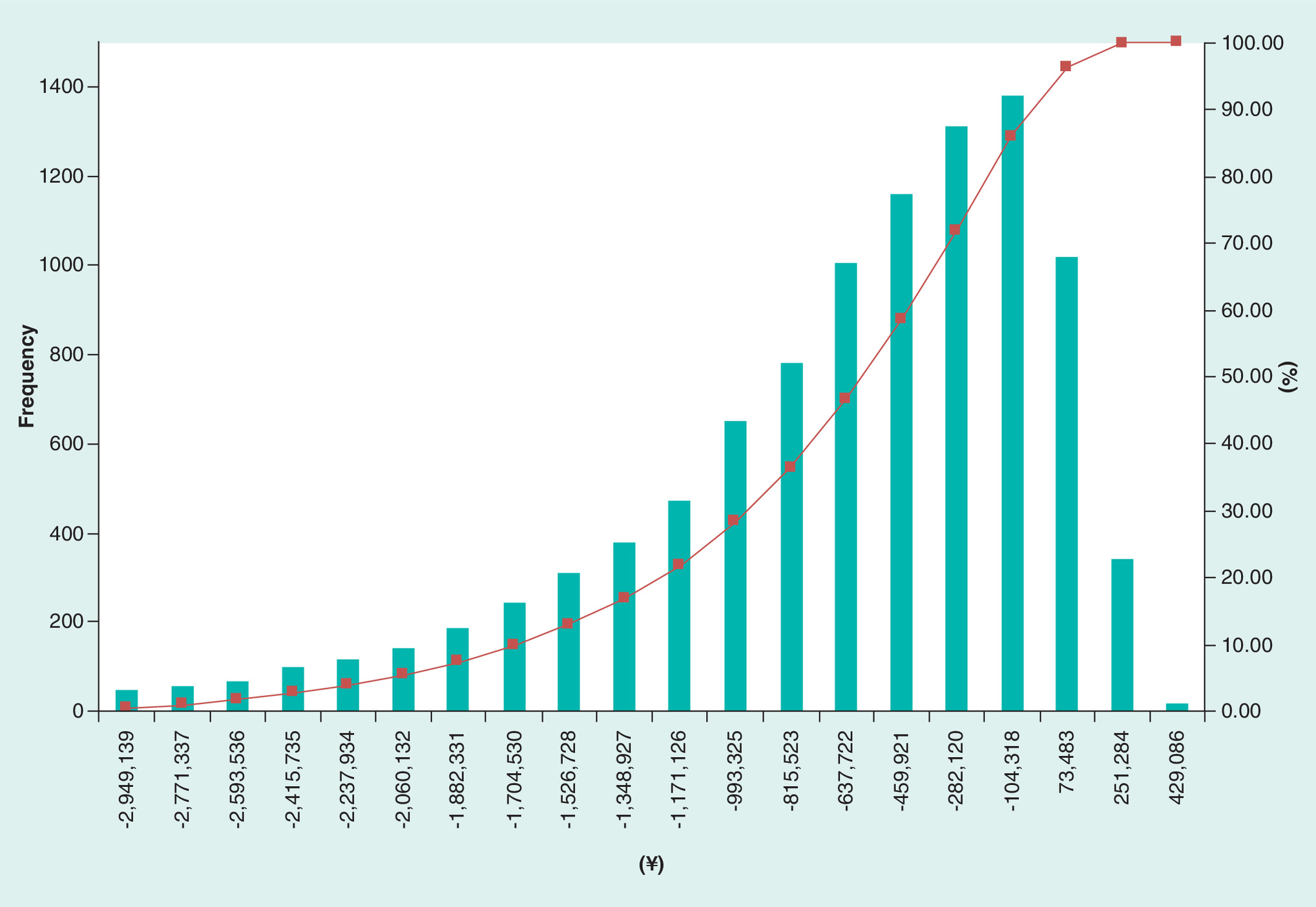
The generated ICER per gained QALY associated with the standard utilization scenario from the 10,000 simulations in the PSA were plotted to demonstrate the cost–effectiveness distribution (Figure 4). Based on the plotted cost–effectiveness distribution, the cost–effectiveness dominance of the standard utilization scenario was found in 92.8% of the 10,000 simulations. The identified median of the ICER per gained QALY associated with the standard utilization scenario relative to the real-world utilization scenario was -¥598,843 (95% credible interval: -¥2,918,636 to ¥102,492).
Discussion
The gained health benefits associated with standard utilization of ZA in our cost–effectiveness analysis was through the reduced risk of SRE, which substantially reduce quality of life. Even though studies that directly measure the quality of life associated with ZA treatment for BM in Chinese patients are lacking, ZA has been proven to effectively control bone pain [13], the symptom that affects over half of SRE patients [14] and substantially diminishes quality of life [15]. Additionally, other SRE types impair quality of life. For example, metastatic spinal cord compression can reduce patient quality of life by 47–68%, depending on the status of paralysis [4]. Bone surgery and bone fracture can also reduce quality of life by 6–15% [4].
The substantial impact of SREs on medical costs was the key factor driving the cost–effectiveness dominance of the standard utilization of ZA. Similar to the published cost studies in Western countries [5,16], the retrospective cost analysis in this study observed more than doubled medical costs associated with SREs when compared with the medical costs of BM without the occurrence of SREs. As expected, the reduced risk for SRE occurrence associated with the standard utilization scenario reduced the cumulated medical costs associated with SRE occurrence over the lifetime model simulation time. Furthermore, the reduced medical costs associated with SRE in the model scenario for standard utilization of ZA was sufficient to completely offset the increased medical costs due to increased survival time with BM only and increased drug acquisition costs associated with improved utilization of ZA. According to the base-case analysis, the standard utilization of ZA over the lifetime model time horizon could save over ¥33,000 per Chinese patient with BM developed from advanced lung cancer. The standard utilization of ZA could roughly save over 2 billion Chinese yuan per year in China according to the latest estimation for the annual incidence of lung cancer cases (733,300) [1].
Similar to other countries, reimbursement plays a crucial role in the treatment compliance associated with Chinese patients. Reimbursement support could be more important to Chinese patients with late lung cancer since a recent Chinese study found 100% poverty among the late lung cancer patients [17]. The reimbursement policy in some Chinese provinces is only applicable to ambulatory care. Thus, the lack of reimbursement support in outpatient settings could substantially reduce patient access to BM treatment and lead to the underuse of bisphosphonates for BM. Expanding reimbursement coverage to BM treatments in outpatient settings could produce a win-win result – that is, it could reduce the financial burden of both patients and healthcare payers according to our cost–effectiveness analysis. Some Chinese cities have expanded their reimbursement support to outpatient settings for the same purpose. For example, Beijing began reimbursing antiviral treatment for chronic hepatitis B in outpatient settings in order to improve patient compliance and reduce long-term liver-related morbidity and mortality. This new insurance policy has improved treatment compliance rates from 57.4 to 75.9% [18]. Thus, reimbursing BM treatments for patients with advanced lung cancer at outpatient settings should warrant future evaluation to confirm the saved medical costs associated with improved utilization of bisphosphonates.
Another potential solution to address the underuse of bisphosphonate in Chinese lung cancer patients is to monitor the blood concentration of bisphosphonate. Even though the main purpose of monitoring the concentration of bisphosphonate is to prevent bisphosphonate treatment toxicity, such as osteonecrosis of the jaw [19], the Chinese patients might benefit from the blood bisphosphonate concentration test that could be reimbursed at outpatient setting. For example, patients could seek the reimbursement of bisphosphonate treatment in hospital setting, once the low concentration of bisphosphonate is identified at outpatient setting.
There were several study limitations that could affect the generalizability of our cost–effectiveness analysis. Our study did not classify lung cancer by histology, and the published evidence for the treatment effects of ZA, the risk of developing SREs from BM and risk of mortality associated with BM and SREs were mainly based on patients with non-small-cell lung cancer, the predominant histological type of lung cancer in China. Additionally, the medical costs associated with BM and SREs were estimated from a clinical cohort managed in a regional cancer center hospital in the Liaoning province, which has a lower health budget than the national average. Thus, the cost variables in our cost–effectiveness model could be underestimated. However, these cost estimations were associated with the maximum internal validity through the full collection of medical claims data. Finally, our cost–effectiveness model did not account for the impact of new target therapy on the disease progression of advanced lung cancer. With slowed disease progression, both clinical and economic benefits associated with ZA treatment could be more promising.
Conclusion
This cost–effectiveness analysis indicated that the standard utilization of ZA could gain more health benefits but cost less than real-world utilization of ZA in Chinese patients with BM developed from advanced lung cancer. Thus, correcting the underuse of bisphosphonates through reimbursing BM management at outpatient settings could be an efficient solution to address unmet medical needs associated with Chinese patients with BM developed from advanced lung cancer.
What is already known about this subject?
Bisphosphonates have been recommended to treat bone metastasis (BM) in cancer patients for the prevention of skeletal-related events (SREs).
SREs significantly increase mortality, impair quality of life and increase health resources utilization.
Current hospitalization reimbursement policy in China leads to underuse of bisphosphonates in cancer patients with BM.
What are the new findings?
Standard utilization of zoledronic acid (ZA) could dominate the real-world utilization of ZA in Chinese lung cancer patients with BM by gaining more benefits and saving medical costs in the cost–effectiveness analysis.
The mortality and direct medical costs associated with SRE were the driving factors for the cost–effectiveness of standard utilization of ZA relative to the real-world utilization of ZA in Chinese lung cancer patients with BM.
The utilization of bisphosphonates for BM in the Chinese lung cancer patients under current hospitalization-based reimbursement policy was unlikely to fully prevent SRE.
Impact on clinical practice
Standard utilization of ZA for BM in lung cancer patients should be further encouraged as it could maximize health benefits and save direct medical costs.
Current hospitalization-based reimbursement policy should expanded to outpatient settings to improve the utilization of ZA in Chinese lung cancer patients with BM to address the medical needs regarding the prevention of SRE.
Financial & competing interests disclosure
This study was funded by Novartis, General Program of Natural Science Foundation of Liaoning Province (2015020464), Major Science and Technology Platform of Liaoning Higher Institution (no. 2916009), Science Research Foundation for Absorbed Talents Program of Liaoning Cancer Hospital and Special Project of Applied Technology of Population and Health by Shenyang Science and Technology Plan (no. 18-014-4-04). H Zhan and W Chen are the employees of Normin Health, a consulting firm receiving industry funds to conduct health outcomes and economics research. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval for all human or animal experimental investigations.
Author contributions
Z Yu, Y Cui, W Chen and H Liu formulated the research idea and developed the study protocol. Y Liu, Y Cui, R Ma and H Liu conducted the retrospective cost study for bone metastasis developed from advanced lung cancer in Chinese patients. H Zhan and W Chen developed the decision analytic model and conduct the cost–effectiveness analysis. Z Yu, W Chen and H Liu drafted the manuscript. All the authors participated the interpretation of study results. All the authors have critically reviewed the manuscript and approved the submission of this manuscript.
References
1.
Chen W, Zheng R, Peter D, Baade PD et al. Cancer Statistics in China, 2015. CA Cancer J. Clin. 66, 115–132 (2016).
2.
Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin. Cancer Res. 12, 6243s–6249s (2006).
3.
Cetin K, Christiansen CF, Jacobsen JB et al. Bone metastasis, skeletal-related events, and mortality in lung cancer patients: a Danish population-based cohort study. Lung Cancer 86(2), 247–254 (2014).
4.
Matza LS, Chung K, Van Brunt K et al. Health state utilities for skeletal-related events secondary to bone metastases. Eur. J. Health Econ. 15(1), 7–18 (2014).
5.
Decroisette C, Monnet I, Berard H et al. Epidemiology and treatment costs of bone metastases from lung cancer: a French prospective, observational, multicenter study (GFPC 0601). J. Thorac. Oncol. 6(3), 576–582 (2011).
6.
Peters S, Adjei AA, Gridelli C et al. Metastatic non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 23(Suppl. 7), vii56–64 (2012).
7.
Joshi AD, Carter JA, Botteman MF, Kaura S. Cost–effectiveness of zoledronic acid in the management of skeletal metastases in patients with lung cancer in France, Germany, Portugal, The Netherlands, and the United Kingdom. Clin. Ther. 33(3), 291–304 (2011).
8.
Utilization of bisphosphonates for bone metastasis in Chinese lung cancer and breast cancer patients. IMS market research (2013).
9.
China guidelines for pharmacoeconomic evaluations. www.ispor.org/PEguidelines/source/China-Guidelines-for-PharmacoeconomicEvaluations_2011_Chinese.pdf.
10.
Scott D, Andrew L, Mel W. Health state utility scores in advanced non-small cell lung cancer. Lung Cancer 62(3), 374 (2008).
11.
Hillner BE, Weeks JC, Desch CE et al. Pamidronate in prevention of bone complications in metastatic breast cancer: a cost–effectiveness analysis. J. Clin. Oncol. 18(1), 72 (2000).
12.
Yang Y, Ma Y, Jin S et al. A multicenter, retrospective epidemiologic survey of the clinical features and management of bone metastatic disease in China. Cancer 35(5), 40 (2016).
13.
Costa L, Major PP. Effect of bisphosphonates on pain and quality of life in patients with bone metastases. Nat. Clin. Pract. Oncol. 6(3), 163–174 (2009).
14.
Santini D, Barni S, Intagliata S et al. Natural history of non-small-cell lung cancer with bone metastases. Sci. Rep. UK 22(5), 18670 (2015).
15.
Gaze MN, Kelly CG, Kerr GR et al. Pain relief and quality of life following radiotherapy for bone metastases: a randomised trial of two fractionation schedules. Radiother. Oncol. 45(2), 109–116 (1997).
16.
Delea T, Langer C, McKiernan J et al. The cost of treatment of skeletal-related events in patients with bone metastases from lung cancer. Oncology 67(5-6), 390–396 (2004).
17.
Xiao S. The Impact of reimbursement on the financial burden of the lung cancer patients living in Wuhan city (Doctoral Dissertation). The Central China Technology University, Wuhan, China (2010).
18.
Qiu Q. Health economic evaluation of the new reimbursement policy on antiviral therapy for chronic hepatitis B in Beijing (Doctoral Dissertation). The Chinese Academy of Medical Sciences, Beijing, China (2015).
19.
Lo Faro AF, Giorgetti R, Busardò FP et al. Development and validation of a method using ultra performance liquid chromatography coupled to tandem mass spectrometry for determination of zoledronic acid concentration in human bone. J. Pharm. Biomed. Anal. 162, 286–290 (2019).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 16 November 2018
Accepted: 15 February 2019
Published online: 29 March 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of standard utilization of zoledronic acid for bone metastases from advanced lung cancer in China. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0127
Export citation
Select the citation format you wish to export for this article or chapter.