Comparison between porous tantalum metal implants and autograft in anterior cervical discectomy and fusion: a meta-analysis
Abstract
Aim: The objective of this study was to systematically compare the safety and efficacy of porous tantalum metal (TM) implants and autograft in single-level anterior cervical discectomy and fusion. Methods: Potential academic articles were acquired from the Cochrane Library, Medline, PubMed, Embase, Science Direct and other databases. The time range used was from the inception of the electronic databases to March 2018. Gray studies were identified from the references of included literature reports. STATA version 11.0 (Stata Corporation, TX, USA) was used to analyze the pooled data. Results: Four randomized, controlled trials (RCTs) were identified according to the retrieval process. There were significant differences in operation time (mean difference [MD]: -28.846, 95% confidence interval [CI: -47.087, -10.604], p = 0.002) and satisfaction rate (odds ratio [OR]: 2.196, 95% CI: [1.061–4. 546]; p = 0.034). However, no significant difference was detected in blood loss (MD: -73.606, 95% CI: [-217.720, 70.509], p = 0.317), hospital stay (MD: -0.512, 95% CI [-1.082, 0.058]; p = 0.079), fusion rate (OR: 0.497, 95% CI [0.079, 3.115]; p = 0.455), visual analog scale (MD: -0.310, 95% CI [-0.433, -0.186]; p < 0.001) or complication rate (risk difference [RD]: -0.140, 95% CI: [-0.378, 0.099]; p = 0.251). Conclusion: Porous TM implants are equally as effective and safe as autograft in anterior cervical discectomy and fusion processes. In addition, porous TM implants could reduce operation time and improve clinical satisfaction significantly.
The overwhelming majority of radiculopathy and myelopathy are caused by degenerative cervical spine disease that may necessitate surgery [1]. Every year, more than 100,000 surgeries are performed to treat degenerative cervical spine disease in the USA, and the number of surgeries have doubled in the past decade [2,3]. Anterior cervical discectomy and fusion (ACDF) is a surgical process that can restore the segmental intervertebral space height through fusion [4,5]. Currently, ACDF has become the most common surgical procedure for cervical degenerative diseases [6]. Although the fusion rate of the autologous bone graft is up to 83–97%, there is significant morbidity (pain, vascular injury, numbness and sensory abnormalities, pelvic ring fracture or iliac bone fracture, infection, etc.) associated with iliac crest graft harvest [7]. The incidence of iliac crest graft harvest is ∼5–20% [8]. Therefore, metal materials have gradually become necessary for bone grafting because of their unique advantages. It has been shown that tantalum metal (TM) implants are useful in obtaining fusion and improving patient outcomes in the lumbar spine [9]. An experiment in pigs demonstrates that using a porous metal cage could achieve higher interface healing and more reliable fusion [10]. Although the TM implant has a theoretical advantage in spinal surgery, there is a lack of large-sample, multicenter, randomized controlled clinical studies. This study aims to systematically compare the effect of porous TM implants and autograft in ACDF through meta-analysis.
Materials & methods
Literature & search strategy
Electronic databases, including Cochrane Library, Medline, PubMed, Embase and ScienceDirect were queried to identify publications of randomized controlled trials (RCTs) and retrospective controlled studies (RCS) exploring the effect of porous TM implants or autograft in ACDF from the inception of the electronic databases to March 2018. Structured search strategies were used in combination according to Boolean logic: porous metal implant; TM, autograft and cervical spondylopathy, degenerative cervical spine disease. In addition, the research on the appraisal reference list was manually reviewed for other potential trials that should be included. The process was iterated until no further articles could be determined. The meta-analysis was based on acknowledged PRISMA guidelines (the Prioritized Reported Items for Systematic review and Meta-Analysis).
Inclusion & exclusion criteria
If the article met the following criteria in accordance with PICOS, the article was considered to be included in the current meta-analysis: population: patients with degenerative cervical spondylopathy; intervention: patients who received ACDF; comparison intervention: porous TM implant or autograft; outcome measures: one or more of the following outcomes were reported: operation time, visual analog scale (VAS), satisfaction rate, hospital stay, fusion rate, blood loss and complication rate; study design: RCTs or non-RCTs reported in full-text English-language articles. Exclusion criteria: in vitro and animal experiments, and meeting abstracts were excluded; multiple segmental surgery.
Data extraction & outcome measures
Two of the reviewers independently extracted data from the included studies. The following essential information was captured: first author name, nationality, publication year, device, sample size, study design, follow-up and outcomes. Other relevant data such as patient characteristics and literature quality evaluation were also extracted from individual studies. The extracted data: median, range and size of the trial, and mean difference (MD) and standard deviation (SD) were input into the designed standardized table. When there were differences in opinion, another author had the final decision. The outcome measures included the VAS, satisfaction rate, hospital stay, fusion rate, complications and blood loss. Complications included dysphagia, hoarseness, infection, cerebral fluid leakage, reoperation, donor-site-related complications, graft-related complications and hardware-related complications.
Quality assessment & statistical analysis
The Cochrane Collaboration's tool for assessing risk of bias and the methodological index for nonrandomized studies (MINORS) were used to evaluate the quality of the included studies. The literature quality evaluation was conducted separately by two reviewers. Consensus was reached through consultation for divergence. We used STATA version 11.0 (Stata Corporation, TX, USA) for statistical analyses. When I2 > 50%, we considered that the data had apparent heterogeneity, and we conducted a meta-analysis using a random-effects model according to the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0). Otherwise, the fixed-effect model was performed. The results of continuous outcomes (operation time, hospital stay, blood loss, VAS), were expressed as the mean difference (MD) with 95% confidence intervals (CIs). For discontinuous variable outcomes (satisfaction rate, fusion rate, complication rate), a risk difference (RD), odds ratio (OR) or relative risk (RR) with 95% CI was applied for the assessment.
Results
Search results
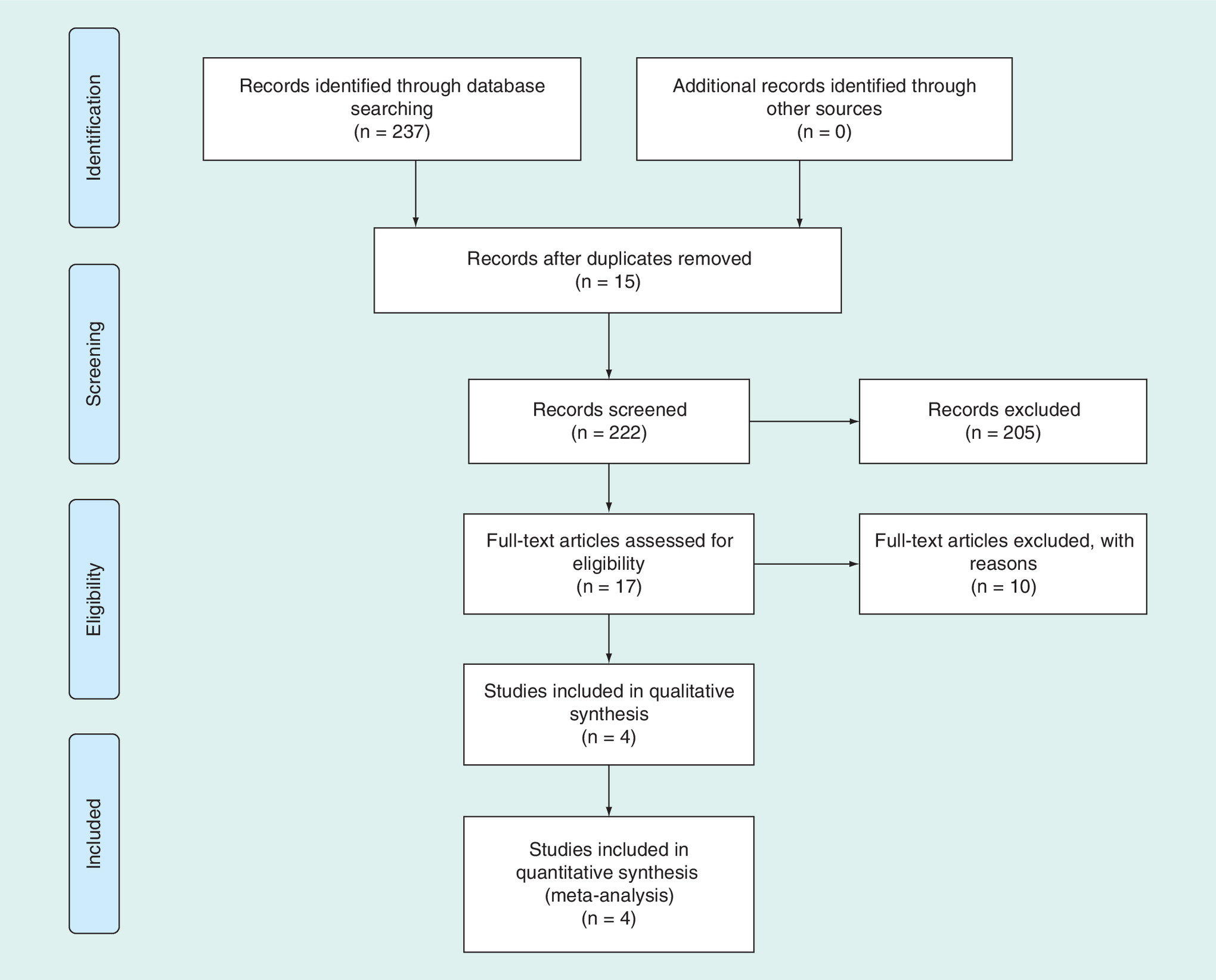
The selection process is illustrated in Figure 1; the original database search (Cochrane Library, Medline, PubMed, Embase, ScienceDirect) yielded 237 records. Of these, 220 were excluded for various reasons (unavailable data, case reports, reviews and irrelevant articles, duplication). The full text of the remaining 17 articles was reviewed. Four RCTs [11–14] were included after reading the whole text according to the inclusion and exclusion criteria, with a total of 204 patients included in the present meta-analysis.
Risk of bias assessment
The Cochrane Collaboration's tool was used to evaluate the quality of the included RCTs. Details are presented in Table 2.
| Studies | Country | Simple size TM/AUTO | Age TM/AUTO | Type | Follow-up | Device | Outcome |
|---|---|---|---|---|---|---|---|
| Lofgren 2010 | Sweden | 40/40 | 48/49 | RCT | 24 months | Trabecular Metal 100 | 1, 2, 3, 4, 5, 7 |
| Wigfiled 2003 | Britain | 17/7 | 50.8/62.7 | RCT | 24 months | Novus block and ring | 2, 3, 4, 5, 6, 7 |
| Kasliwal 2013 | America | 28/11 | 45.6/44.9 | RCT | 24 months | Trabecular Metal 100 | 1, 2, 4, 5, 6, 7 |
| Fernandez 2008 | Spain | 28/33 | 47.5/49.3 | RCT | 24 months | Trabecular Metal 100 | 1, 2, 3, 4, 5, 6, 7 |
| Operation level | Fusion standard | ||||||
| Single-level | Visual evaluation of the A–P and lateral views in forced flexion/extension of the cervical spine | ||||||
| Single-level | Less than 48 sagittal angulation between flexion and extension radiographs at the operated level, and the absence of radiolucency extending over more than 50% of the implant/endplate interface | ||||||
| Single-level | Angulation (<2 degrees) or the alteration of interspinous process distance (<2 mm) | ||||||
| Single-level | Bony bridging around the implant and/or <2° of variation of Cobb's angle on F/E radiographs or <2 mm of variation in the interspinous distance, in the absence of periimplant radiolucency | ||||||
TM: Tantalum; AUTO: Autograft. 1. Visual analog scale (VAS), 2. Complication rate, 3. Satisfaction rate, 4. Fusion rate, 5. Operation time, 5. Blood loss, 7. Hospital stay.
| Risk of bias assessment | Fernandez 2008 | Lofgren 2010 | Wigfiled 2003 | Kasliwal 2013 |
|---|---|---|---|---|
| Random sequence generation | Low | Low | Low | Low |
| Allocation concealment | Unclear | Unclear | Low | Unclear |
| Blinding of participants and personnel | Low | High | High | High |
| Blinding of outcome assessment | Low | Unclear | Unclear | High |
| Incomplete outcome data addressed | Low | Low | Unclear | Unclear |
| Selective reporting | Low | Low | Low | Low |
| Free of other bias | Low | Low | Low | Low |
WMD: Weighted mean difference.
Study characteristics
Demographic characteristics and details concerning the literature type of the included studies are summarized in Table 1. The studies included in the meta-analysis were conducted in four countries (Sweden, the USA, Britain and Spain) from 2003 to 2013, and involved 204 patients (113 patients treated with porous TM implants and 91 patients were treated with autograft).
Outcomes of meta-analysis
Operation time
The comparison of operation time between the two groups was conducted among four of the included studies. The results of the random-effects show that there were significant differences between patients treated with porous TM implants and autograft (heterogeneity p = 0.000; I2 = 88.1%; MD: -28.846; 95% CI: -47.087 to -10.604; p = 0.02; Figure 2).
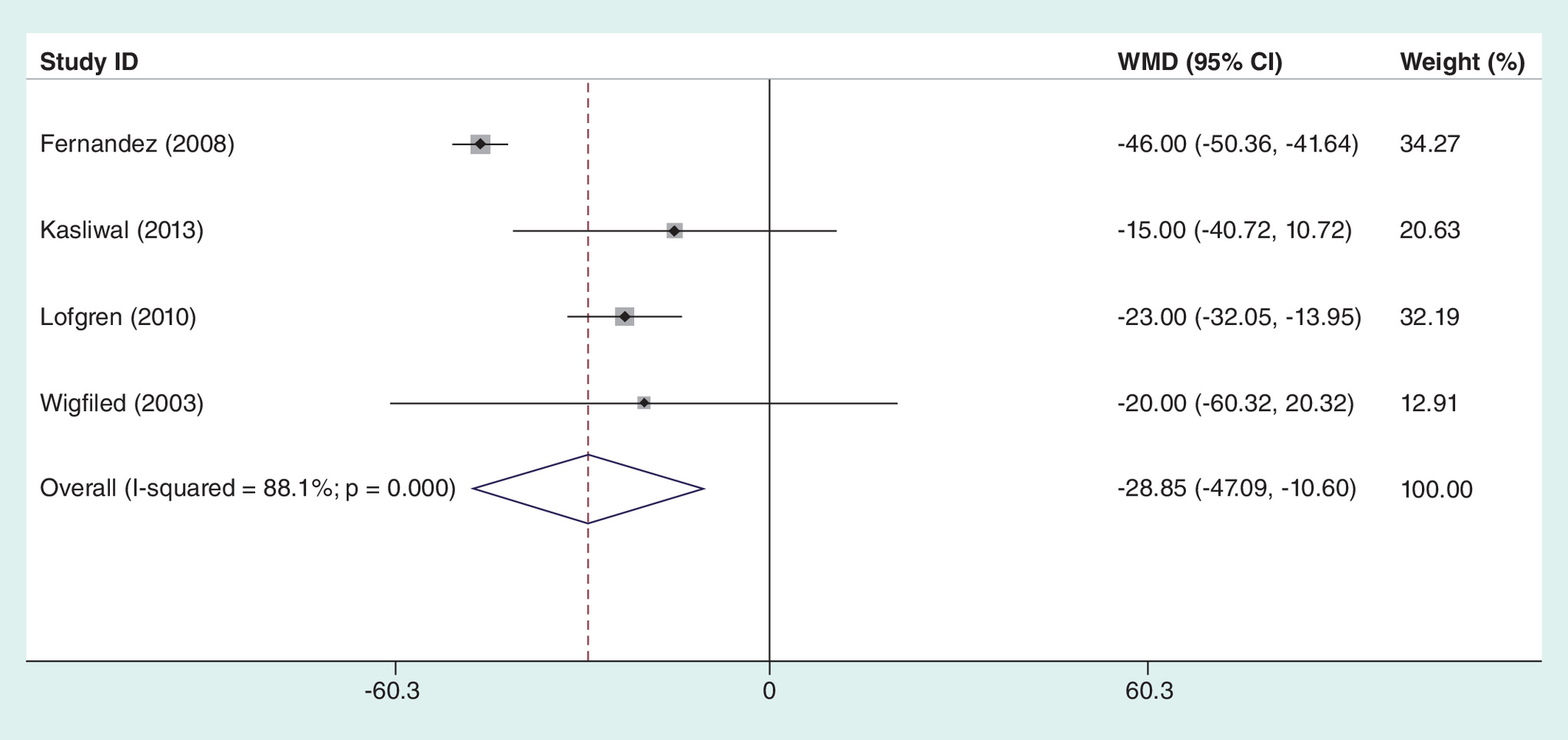
Figure 2. Forest plot diagram showing the operation time.
WMD: Weighted mean difference.
Visual analog scale
Three articles have been published on the visual analog scale (VAS). There is no heterogeneity in the statistical results of the pooled literature (I2: 0.0%; p = 0.710). The result of the fixed effect model showed that porous TM implants have an advantage on autograft for VAS (MD: -0.310; 95% CI: -0.433 to -0.186; p < 0.001; Figure 3). However, the extreme range of 95% CI and the value of MD may not reflect the actual clinical meaning.
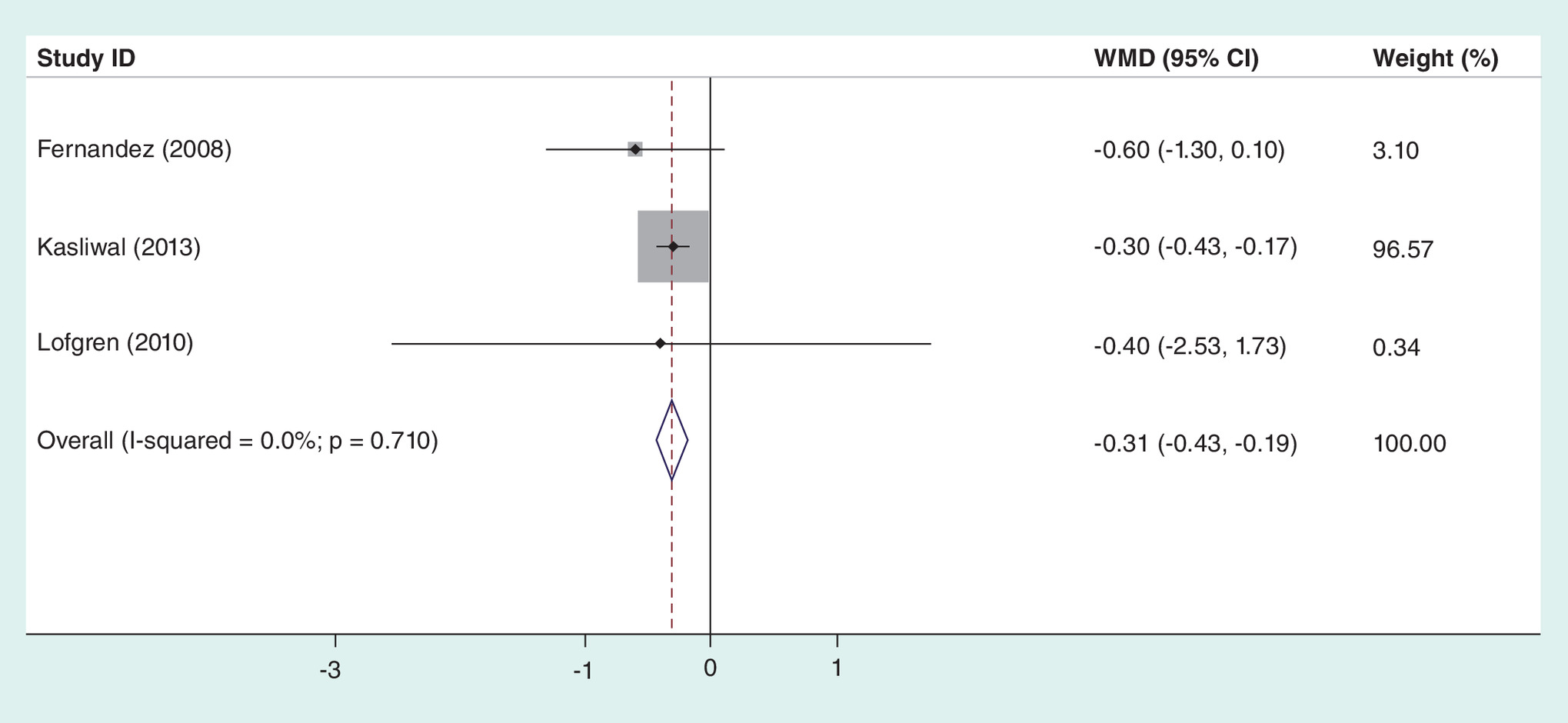
Figure 3. Forest plot diagram showing the visual analog scale.
WMD: Weighted mean difference.
Satisfaction rate
Three publications reported the satisfaction rate among 165 patients. A fixed-effects model was used. The results also showed that the patients who were treated with porous TM implants could reach a higher satisfaction (heterogeneity p = 0.895; I2: 0.0%; OR: 2.196; 95% CI: 1.061–4.546; p = 0.034; Figure 4).
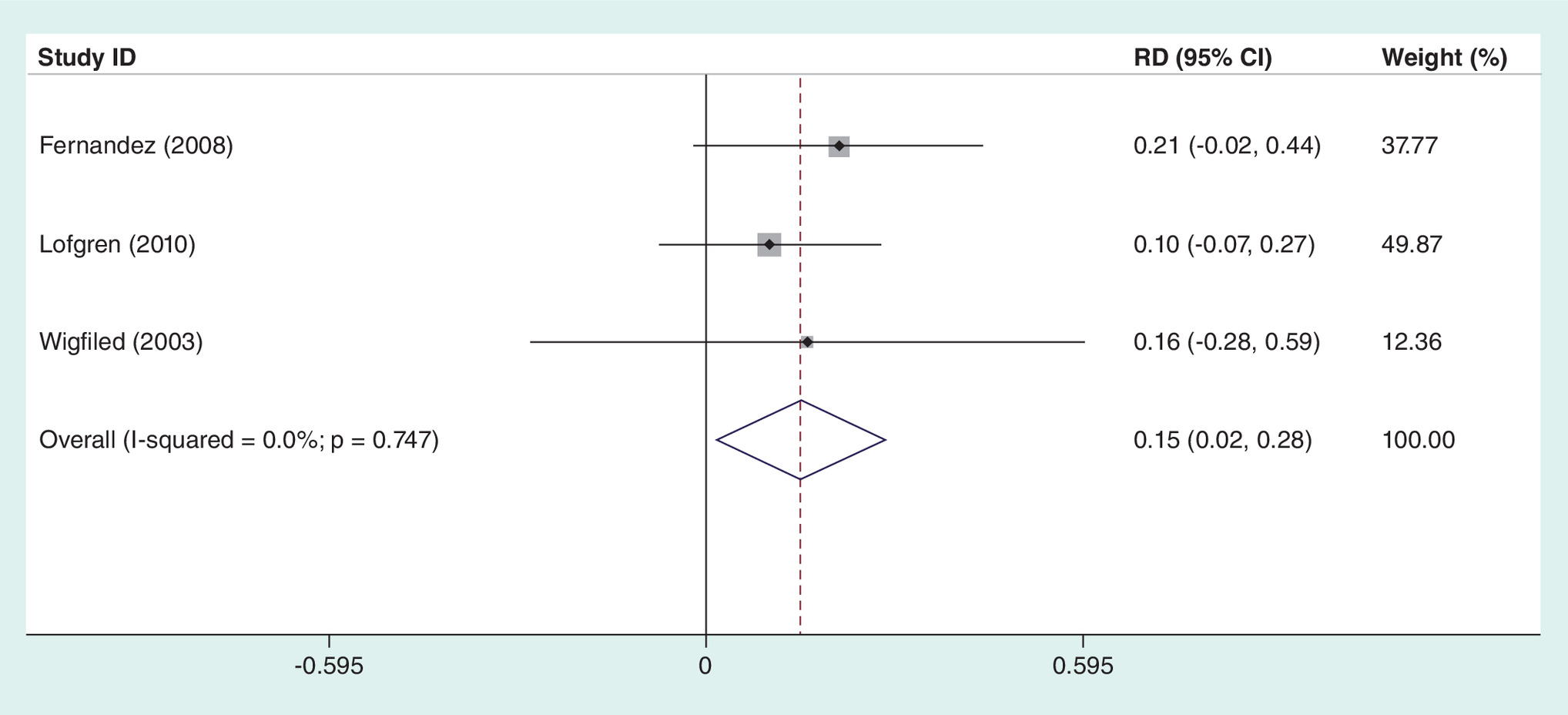
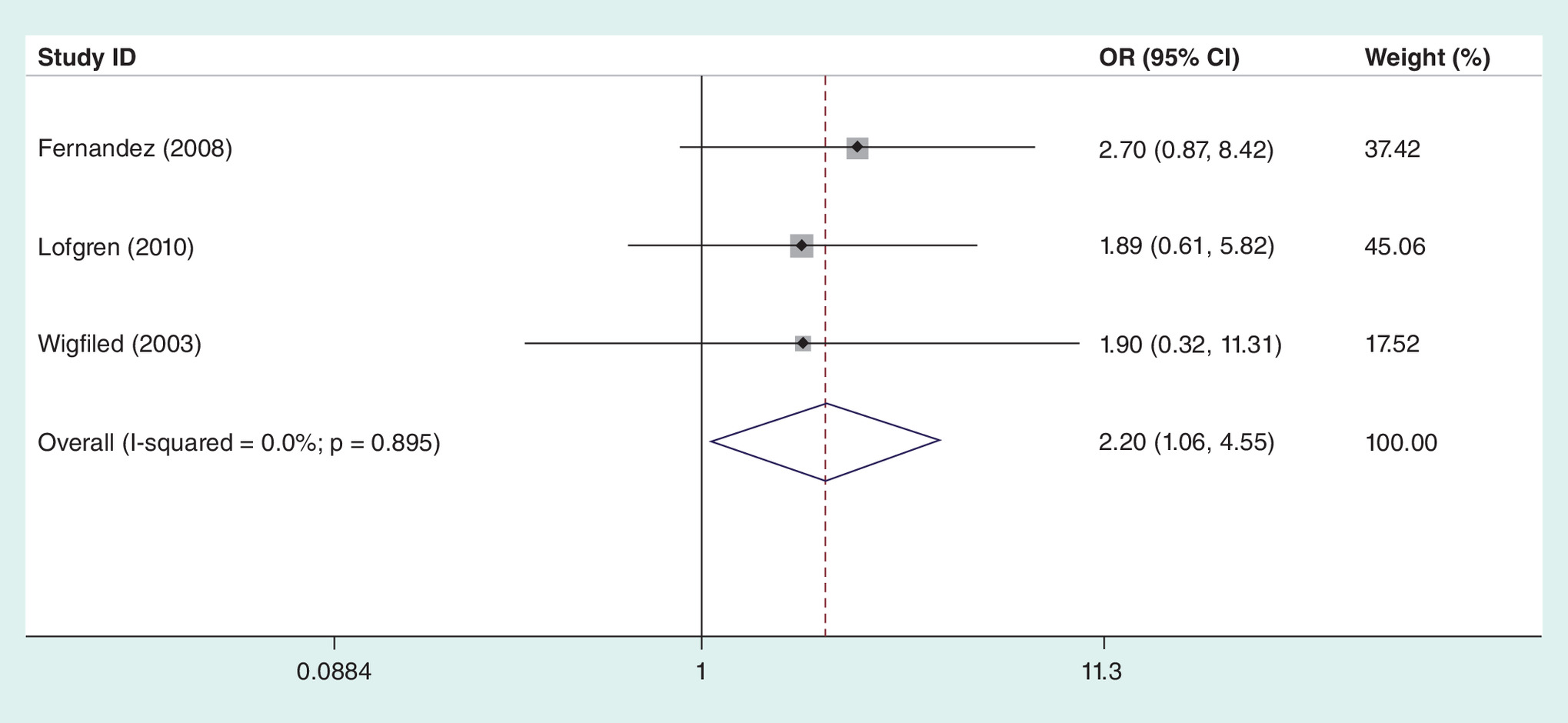
Figure 4. Forest plot diagram showing the satisfaction rate.
OR: Odds ratio; RD: Risk difference.
Hospital stays
Figure 5 shows hospital stay results. In four publications, 113 and 91 patients were enrolled in the TM group, respectively. A random-effects model was used. There was no significant difference between the two groups (heterogeneity p = 0.001; I2: 81.0%; MD: -0.512; 95% CI: -1.082–0.058; p = 0.097).
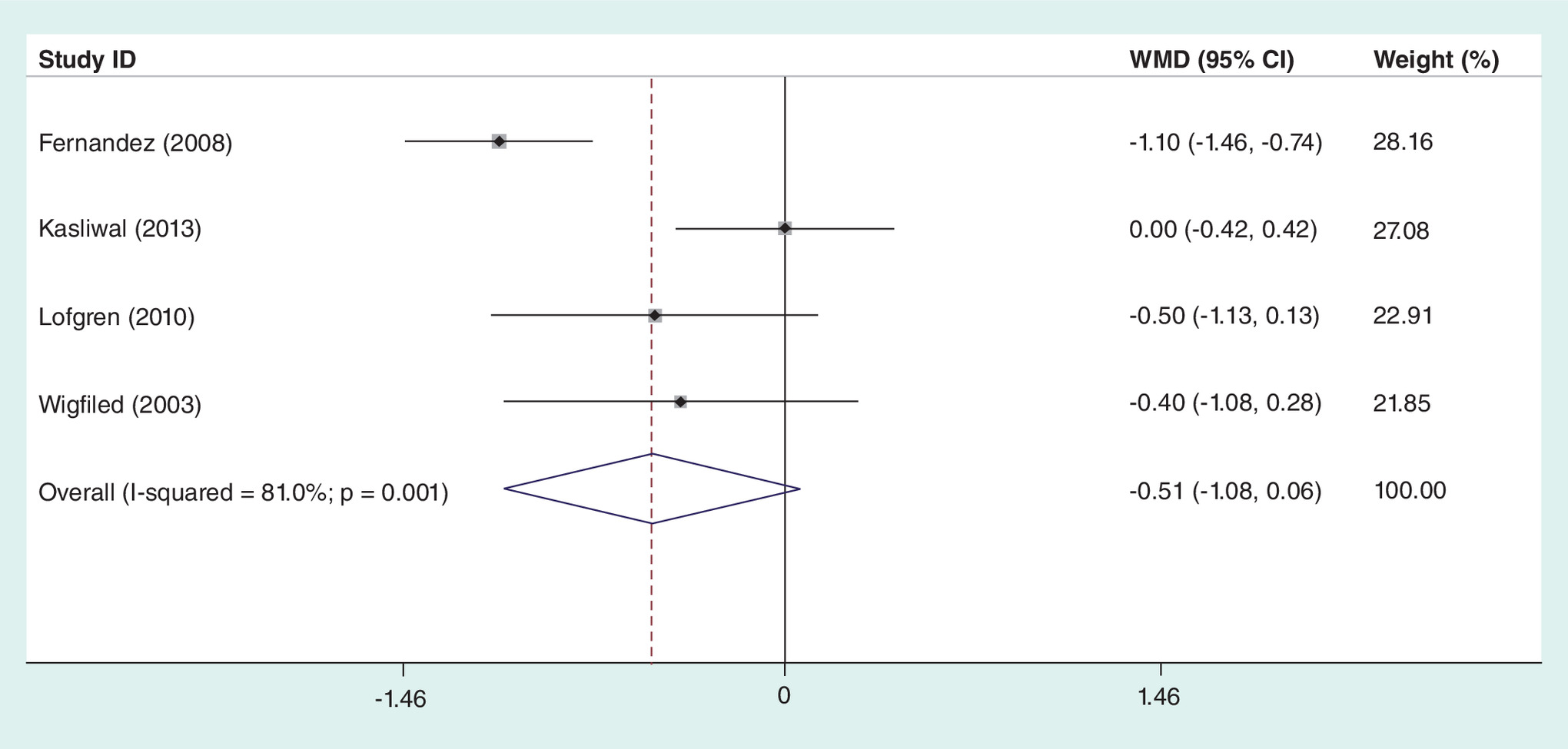
Figure 5. Forest plot diagram showing the hospital stay.
WMD: Weighted mean difference.
Fusion rate
Two authors counted the fusion among 204 patients. In total, 80 patients meet the fusion criterion in the TM group, and 81 patients in the control group. The random-effects model was selected. The results of the meta-analysis showed that there was no significant difference between the two groups (heterogeneity p = 0.019; I2: 70.0%; OR: 0.497; 95% CI: 0.079–3.141; p = 0.455; Figure 6).
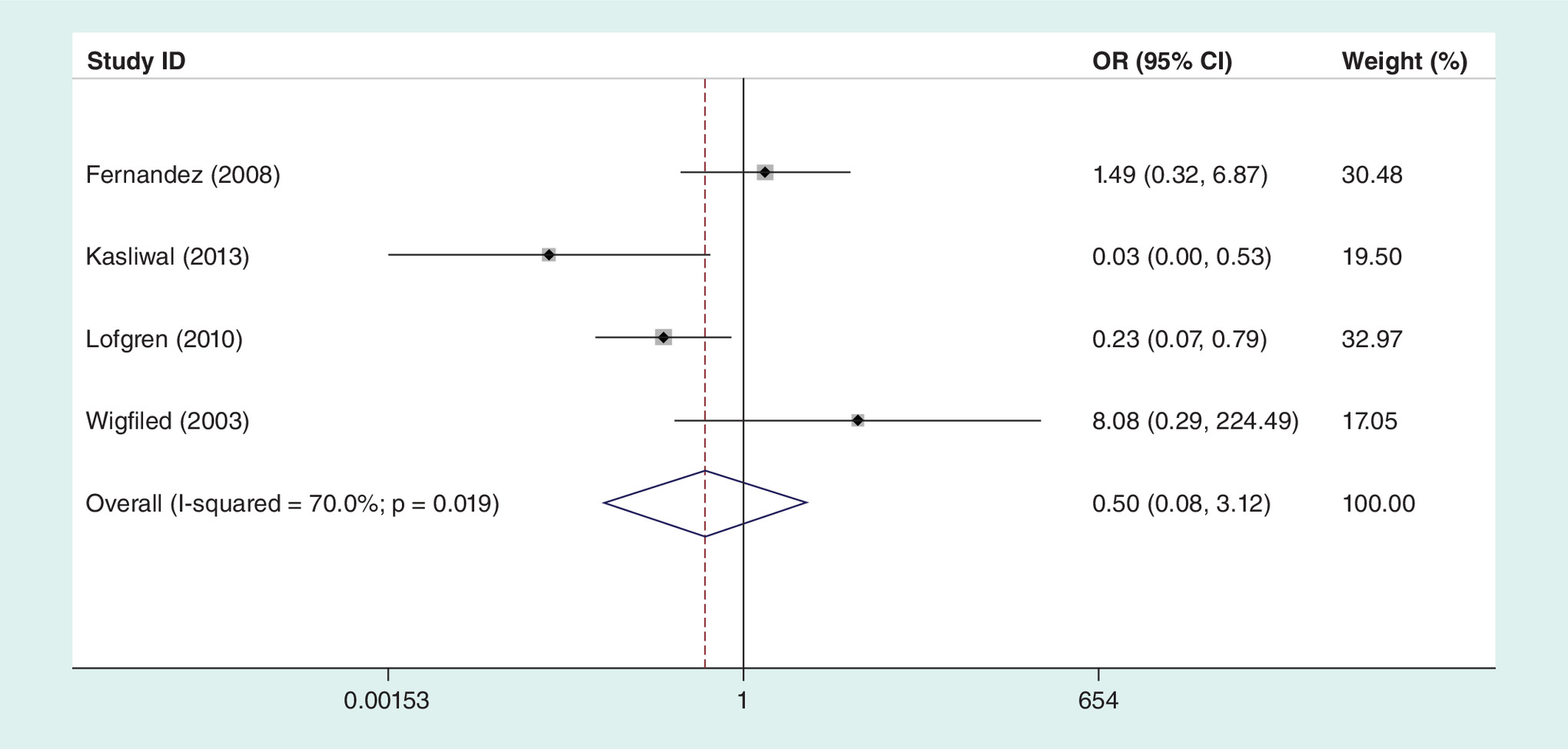
Figure 6. Forest plot diagram showing the fusion rate.
OR: Odds ratio.
Complications
Complications, including dysphagia, hoarseness, infection, cerebral fluid leakage, reoperation, donor-site-related complications, graft-related complications and hardware-related complications, were evaluated in the four studies. No significant differences were observed between the two groups (RD: -0.140, 95% CI: -0.378 to 0.099; p = 0.251; Figure 7) with obvious heterogeneity (heterogeneity p = 0.000; I2: 83.6%), a random-effects model was used.
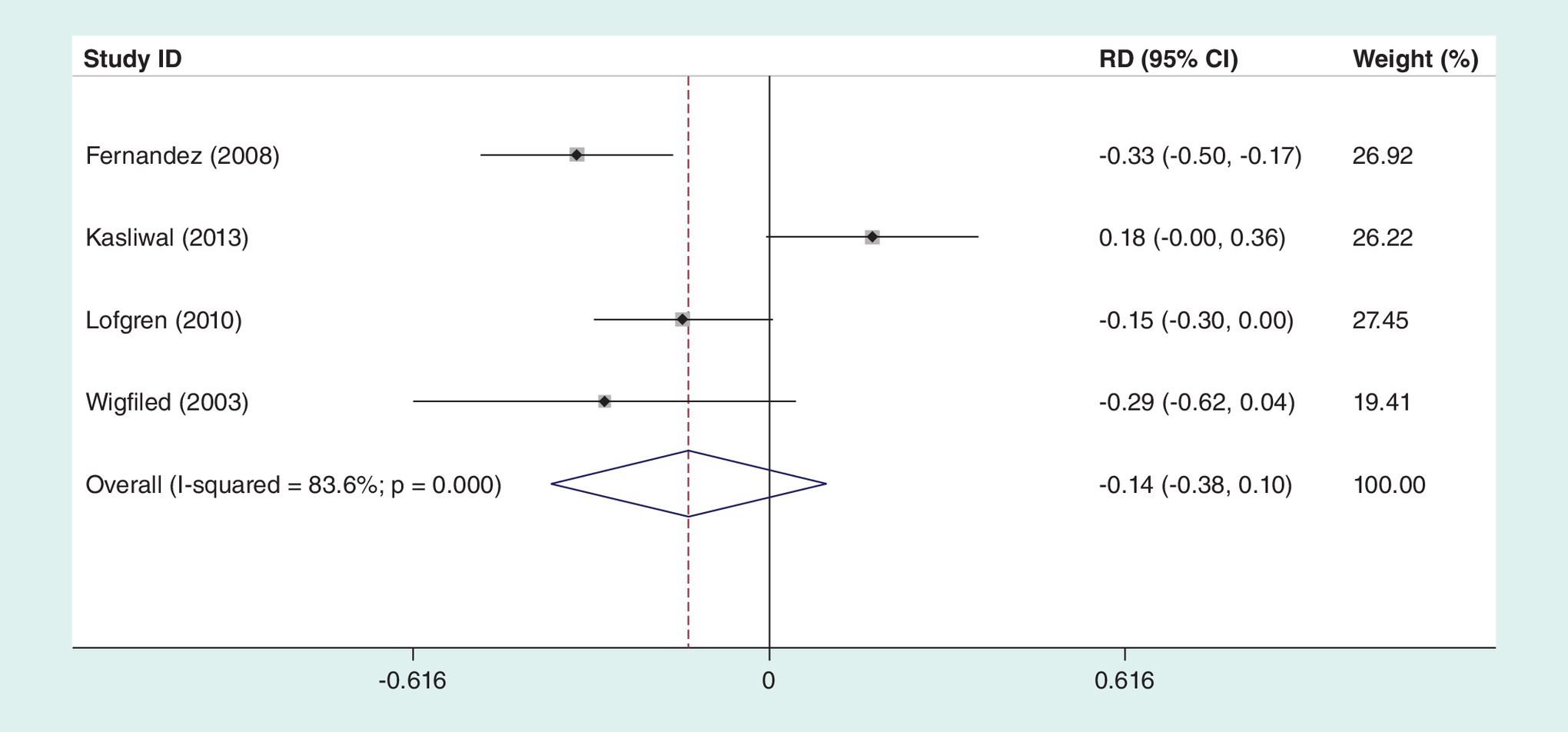
Figure 7. Forest plot diagram showing the complications.
RD: Risk difference.
Blood loss
Blood loss was reported in three of the included studies. A random-effects model was performed with obvious heterogeneity. There were no significant differences in the two groups (MD: -73.606; 95% CI: -217.720 to 70.509; p = 0.317; Figure 8).
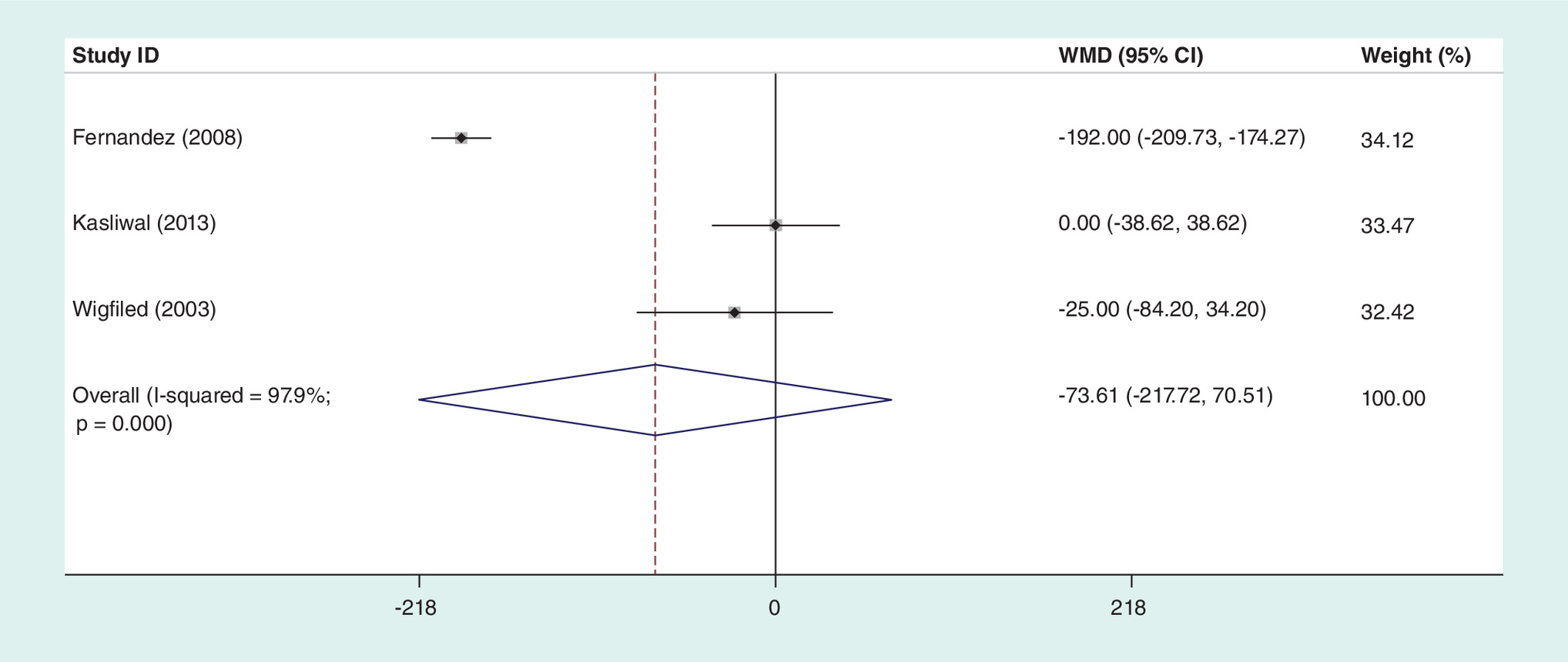
Figure 8. Forest plot diagram showing the blood loss.
WMD: Weighted mean difference.
Discussion
ACDF is a surgical approach for patients suffering from nerve compression due to degenerative cervical spine disease that is unresponsive to conservative therapy [15]. Autologous bone graft has long been the gold standard in spinal fusion surgery for its osteogenicity, osteoconductivity and osteoinductivity, but it is still associated with issues of bone resorption and graft subsidence [16–18]. Porous metal implants are a new generation of fusion materials for spinal surgery [19,20]. Metal implants with a porous structure of Ti6Al4V facilitated bone ingrowth and maintained the stability of cervical spine in a sheep model [21]. Wu et al. observed that porous metal implants are equipped with superior bone growth and stability to polyetheretherketone (PEEK) [22]. TM as a new spinal implant with the following advantages: it has a range of Young's modulus similar to cancellous bone (0.1–1.7 GPa) leading to a decrease of stress shielding at bone/implant interfaces [23]. The surface roughness of the tantalum implant ensures the improvement of the initial stability with additional external support [24]. The porous structure of new materials could significantly change the ability of bone to penetrate. The stiffness and strength of porous metal could be changed from cancellous bone (80% porosity) to cortical bone (50%) by adjusting porosity. Three included studies used the Trabecular 100 Metal TM products of the American Zimmer company, and one study used the Novus block and ring tantalum products of the American Medtronic company. The process principle and microspore structure of the two products are the same, and the porosity is mainly controlled between 60 and 65%. Blanco shows that bone marrow mesenchymal stem cells could grow well and maintain bioactivity in the TM environment [25]. Meanwhile, Cattrysse believes that patients with TM implants for ACDF have a significant advantage over the iliac crest graft harvest group with the standard Smith–Robinson surgical procedure [26]. This study also shows that TM implants could provide multiple effects on restoring the height of the vertebral body, promoting the fusion of adjacent endplates and maintaining intervertebral stability [26].
Although the result of the present meta-analysis shows that there was no statistical difference between the fusion rates of porous tantalum implants and autograft, we think there is cause for concern regarding the conclusion that tantalum implants fuse as well as autograft. In the forest plot of the meta-analysis regarding fusion rate, two studies show a significant result of fusion failure in the tantalum groups (Kasliwal [13] and Lofgren [11]), compared with the other two studies which demonstrate no significant differences in the fusion rates. In an included RCT by Fernandez et al. [12], the efficacy of tantalum implants was found to be equivalent to autograft in terms of achieving good radiologic and clinical outcome. A finding duplicated in Winfield's study [13]. However, the study was terminated early because of concerns regarding radiologic nonunion at 6-month follow-up radiographs in the tantalum treatment group. By contrast, the number of patients fused with tantalum was markedly less than in the autograft group in a recently published multicenter prospective RCT by Kasliwal et al. [14] (38%<100%). It is noteworthy that there are only 11 participants in the autograft group. It can be difficult to assess bony fusion when the material under investigation does not permit visualization of the formation of bridging trabeculae due to its dense radioopaque nature. We compared the different criteria for fusion in the included studies and found that less stringent fusion standards (allowing more motion) naturally increased the fusion rate, as illustrated by other literature [27]. Zoega [28] even found that none of the patients had fusion with porous tantalum implant devices through a sensitive method for detecting motion-radiostereometric analysis at the 2-year follow-up. Furthermore, we observed that the anterior plate-assisted porous tantalum implant contributes to initial stability and a higher fusion rate [10,29]. Clarification of stopping criteria in relation to outcome measures and criteria for fusion should be considered in randomized trials of spinal surgical techniques and implants.
The operation time was also discussed in the included studies. Lofgren [11] believed that the operation time was shorter in the porous metal implant group compared with the autograft group, which was similar to an RCT reported by Fernandez [12]. Our findings are consistent with their research. In the present meta-analysis, the TM group could reduce operation time. The reason for more time in the autograft group is that it takes extra time to perform the iliac crest resection.
Autogenous bone graft needs to remove cancellous bone from the iliac crest. This operation may cause pain, infection, hematoma and other complications, and prolonged hospitalization [30]. Porous TM implants could avoid the occurrence of the above issue. The complications of porous TM implants are mainly manifested in implant-related complications. In the included study, only five device fragmentations were observed in the TM implant group. Two had transient hoarseness. And one of them also had swallowing disturbances. Concerning the results of the meta-analysis, there is no statistical difference in the incidence of overall complications.
At least 75–80% of the patients consider that the effect of ACDF was satisfactory in alleviating pain, and improving function and neurological restitution [7,31,32]. An RCT conducted by Fernandez [12] showed that the satisfaction rate in the TM group was 82.2 and 69.7% in the control group. Our meta-analysis demonstrates that the patients who were treated with a TM implant could have higher postoperative satisfaction (77.6% > 65%). We consider that the lower number of donor site complications in the tantalum group could lead to better results.
Three included studies have reported the VAS at the follow-up period. Fernandez [12] reported that VAS score respectively improved to 4.1 for TM and 4.7 for the control group at 2 years follow-up, which is similar to the research of Lofgren [11]. Although the result of our research demonstrated that there were significant differences in VAS, the extreme range of 95% CI and the value of MD may not reflect the actual clinical meaning. Beside, due to the small sample size, we could not clarify whether tantalum has a more significant advantage on VAS.
The results of our meta-analysis indicate that there were significant differences in operation time and satisfaction. However, no significant difference was detected in blood loss, hospital stay and fusion rate VAS and complication rate. This study has the following limitations: there are fewer relevant studies of porous TM implants for ACDF, mostly in single-center studies with small sample sizes. Different criteria for fusion in studies bias the results of the combined effect.
Conclusion
Porous TM implants are equally as effective and safe as autograft in ACDF. In addition, the porous TM implants could reduce operation time and improve clinical satisfaction significantly.
Anterior cervical discectomy and fusion (ACDF) has become the most common surgical procedure for cervical degenerative diseases.
Although the fusion rate of the autologous bone graft is up to 83–97%, there is significant morbidity associated with iliac crest graft harvest.
It has been shown that tantalum metal (TM) implants are useful in obtaining fusion and improving patient outcomes in the lumbar spine.
Although TM implants have a theoretical advantage in spinal surgery, there is a lack of large sample, multicenter, randomized controlled clinical studies.
There were significant differences in operation time and satisfaction rate.
No significant difference was detected in blood loss, hospital stay, fusion rate, visual analog scale or complication rate.
Porous TM implants are equally as effective and safe as autograft in ACDF processes.
In addition, porous TM implants could reduce operation time and improve clinical satisfaction significantly.
Author contributions
W-Q Hu, Q-F Li conceived of the design of the study. N Li, W-Q Xin and P Tian performed and collected the data and contributed to the design of the study. W-Q Hu and N Li prepared and revised the manuscript. All authors read and approved the final content of the manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
1.
Cepoiu-Martin M, Faris P, Lorenzetti D, Prefontaine E, Noseworthy T, Sutherland L. Artificial cervical disc arthroplasty: a systematic review. Spine 36(25), E1623–E1633 (2011).
2.
Patil PG, Turner DA, Pietrobon R. National trends in surgical procedures for degenerative cervical spine disease: 1990–2000. Neurosurgery 57(4), 753–758; discussion 753–758 (2005).
3.
Wang MC, Chan L, Maiman DJ, Kreuter W, Deyo RA. Complications and mortality associated with cervical spine surgery for degenerative disease in the United States. Spine 32(3), 342–347 (2007).
4.
Smith GW, Robinson RA. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J. Bone Joint Surg. Am. 40-A(3), 607–624 (1958).
5.
Hacker RJ, Cauthen JC, Gilbert TJ, Griffith SL. A prospective randomized multicenter clinical evaluation of an anterior cervical fusion cage. Spine 25(20), 2646–2654; discussion 2655 (2000).
6.
Kani KK, Chew FS. Anterior cervical discectomy and fusion: review and update for radiologists. Skeletal Radiol. 47(1), 7–17 (2018).
7.
Peolsson A, Vavruch L, Hedlund R. Long-term randomised comparison between a carbon fibre cage and the Cloward procedure in the cervical spine. Eur. Spine J. 16(2), 173–178 (2007).
8.
Banwart JC, Asher MA, Hassanein RS. Iliac crest bone graft harvest donor site morbidity. A statistical evaluation. Spine 20(9), 1055–1060 (1995).
9.
Hanc M, Fokter SK, Vogrin M, Molicnik A, Recnik G. Porous tantalum in spinal surgery: an overview. Eur. J. Orthop. Surg. Traumatol. 26(1), 1–7 (2016).
10.
Zou X, Li H, Teng X et al. Pedicle screw fixation enhances anterior lumbar interbody fusion with porous tantalum cages: an experimental study in pigs. Spine 30(14), E392–E399 (2005).
11.
Lofgren H, Engquist M, Hoffmann P, Sigstedt B, Vavruch L. Clinical and radiological evaluation of Trabecular Metal and the Smith–Robinson technique in anterior cervical fusion for degenerative disease: a prospective, randomized, controlled study with 2-year follow-up. Eur. Spine J. 19(3), 464–473 (2010).
12.
Fernandez-Fairen M, Sala P, Dufoo M Jr, Ballester J, Murcia A, Merzthal L. Anterior cervical fusion with tantalum implant: a prospective randomized controlled study. Spine 33(5), 465–472 (2008).
13.
Wigfield C, Robertson J, Gill S, Nelson R. Clinical experience with porous tantalum cervical interbody implants in a prospective randomized controlled trial. Brit. J. Neurosurg. 17(5), 418–425 (2003).
14.
Kasliwal MK, Baskin DS, Traynelis VC. Failure of porous tantalum cervical interbody fusion devices: two-year results from a prospective, randomized, multicenter clinical study. J. Spinal Disord. Tech. 26(5), 239–245 (2013).
15.
Jagannathan J, Shaffrey CI, Oskouian RJ et al. Radiographic and clinical outcomes following single-level anterior cervical discectomy and allograft fusion without plate placement or cervical collar. J. Neurosurg. Spine 8(5), 420–428 (2008).
16.
Chau AM, Mobbs RJ. Bone graft substitutes in anterior cervical discectomy and fusion. Eur. Spine J. 18(4), 449–464 (2009).
17.
Deutsch H, Haid R, Rodts G Jr, Mummaneni PV. The decision-making process: allograft versus autograft. Neurosurgery 60(1 Suppl. 1), S98–S102 (2007).
18.
van Limbeek J, Jacobs WC, Anderson PG, Pavlov PW. A systematic literature review to identify the best method for a single level anterior cervical interbody fusion. Eur. Spine J. 9(2), 129–136 (2000).
19.
Murr LE, Gaytan SM, Martinez E, Medina F, Wicker RB. Next generation orthopaedic implants by additive manufacturing using electron beam melting. Int. J. Biomater. 2012, 245727 (2012).
20.
Murr LE, Gaytan SM, Medina F et al. Next-generation biomedical implants using additive manufacturing of complex, cellular and functional mesh arrays. Philos. Trans. A Math. Phys. Eng. Sci. 368(1917), 1999–2032 (2010).
21.
Yang J, Cai H, Lv J et al. In vivo study of a self-stabilizing artificial vertebral body fabricated by electron beam melting. Spine 39(8), E486–E492 (2014).
22.
Wu SH, Li Y, Zhang YQ et al. Porous titanium-6 aluminum-4 vanadium cage has better osseointegration and less micromotion than a poly-ether-ether-ketone cage in sheep vertebral fusion. Artificial Org. 37(12), E191–E201 (2013).
23.
Black J. Biological performance of tantalum. Clin. Mat. 16(3), 167–173 (1994).
24.
Bobyn JD, Stackpool GJ, Hacking SA, Tanzer M, Krygier JJ. Characteristics of bone ingrowth and interface mechanics of a new porous tantalum biomaterial. J. Bone Joint Surg. Br. 81(5), 907–914 (1999).
25.
Blanco JF, Sanchez-Guijo FM, Carrancio S, Muntion S, Garcia-Brinon J, del Canizo MC. Titanium and tantalum as mesenchymal stem cell scaffolds for spinal fusion: an in vitro comparative study. Eur. Spine J. 20(Suppl. 3), 353–360 (2011).
26.
Cattrysse E, Moens M, Schaillee E, D'Haens J, Van Roy P. Changed cervical kinematics after fusion surgery. Eur. Spine J. 21(7), 1353–1359 (2012).
27.
Fassett DR, Apfelbaum RI, Hipp JA. Comparison of fusion assessment techniques: computer-assisted versus manual measurements. J. Neurosurg. Spine 8(6), 544–547 (2008).
28.
Zoega B, Karrholm J, Lind B. Outcome scores in degenerative cervical disc surgery. Eur. Spine J. 9(2), 137–143 (2000).
29.
Shimamoto N, Cunningham BW, Dmitriev AE, Minami A, McAfee PC. Biomechanical evaluation of stand-alone interbody fusion cages in the cervical spine. Spine 26(19), E432–E436 (2001).
30.
Vavruch L, Hedlund R, Javid D, Leszniewski W, Shalabi A. A prospective randomized comparison between the cloward procedure and a carbon fiber cage in the cervical spine: a clinical and radiologic study. Spine 27(16), 1694–1701 (2002).
31.
Cauthen JC, Kinard RE, Vogler JB et al. Outcome analysis of noninstrumented anterior cervical discectomy and interbody fusion in 348 patients. Spine 23(2), 188–192 (1998).
32.
Ryu SI, Mitchell M, Kim DH. A prospective randomized study comparing a cervical carbon fiber cage to the Smith–Robinson technique with allograft and plating: up to 24 months follow-up. Eur. Spine J. 15(2), 157–164 (2006).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 9 October 2018
Accepted: 12 January 2019
Published online: 25 March 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparison between porous tantalum metal implants and autograft in anterior cervical discectomy and fusion: a meta-analysis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0107
Export citation
Select the citation format you wish to export for this article or chapter.