Real-world effectiveness of palonosetron-based antiemetic regimens: preventing chemotherapy-induced nausea and vomiting
Abstract
Aim: To evaluate real-world effectiveness of guideline-recommended palonosetron-containing antiemetic regimens in patients receiving highly (HEC) or moderately emetogenic (MEC) chemotherapy. Patients & methods: This retrospective analysis used records of adults receiving first-line chemotherapy and a three-drug palonosetron-containing antiemetic regimen for HEC or palonosetron-containing antiemetic regimen for MEC (carboplatin). Results: A total of 1587 records were evaluated. For HEC and MEC, respectively, chemotherapy-induced nausea and vomiting (CINV) occurred in 40 versus 44% of patient cycles (p = 0.01), and unscheduled iv. antiemetics in 41 versus 35% (p < 0.05). A total of 48% of HEC patients versus 42% of MEC patients had CINV-related clinic visits (p = 0.05). Conclusion: Palonosetron-containing antiemetic regimens may provide insufficient CINV control. Alternative regimens may improve patient quality of life and reduce healthcare resource utilization.
In patients with cancer, uncontrolled or poorly controlled chemotherapy-induced nausea and vomiting (CINV) has negative effects on their health and quality of life [1–3], may lead to chemotherapy delays or discontinuations [4] and increases healthcare costs [3,5]. In the absence of antiemetic prophylaxis, highly emetogenic chemotherapy (HEC) induces CINV in more than 90% of patients, and moderately emetogenic chemotherapy (MEC) induces CINV in 30–90% of patients [6–8]. Common iv. regimens classified as highly emetogenic include cisplatin-containing regimens and regimens including any combination of doxorubicin and cyclophosphamide (AC) [6,9,10]. Intravenous (iv.) carboplatin is now classified as highly emetogenic if the area under the concentration–time curve (AUC) is 4 mg/ml or greater [6,9].
Antiemetic guidelines from the American Society of Clinical Oncology (ASCO), the Multinational Association of Supportive Care in Cancer and European Society of Medical Oncology (MASCC/ESMO) and the National Comprehensive Cancer Network (NCCN) recommend various antiemetic regimens for the prevention of CINV associated with HEC and MEC; these include a combination of a 5-hydroxytryptamine type 3 (5-HT3) receptor antagonist (RA), a neurokinin 1 (NK-1) RA and dexamethasone, with or without olanzapine, for patients scheduled to receive HEC [6,9,10] and a two-drug regimen of a 5-HT3 RA plus dexamethasone for patients scheduled to receive MEC [6,9,11]. The NCCN guidelines recommend the addition of olanzapine to this regimen as another option for patients receiving MEC, and the addition of an NK-1 RA in patients with additional risk factors for CINV [6]. The MASCC/ESMO guidelines also recommend a three-drug regimen of a 5-HT3 RA, an NK-1 RA and dexamethasone for patients receiving carboplatin, similar to the ASCO and NCCN guidelines, but do not specify the emetogenicity of carboplatin by the AUC [11].
Several 5-HT3 RAs are available for use in antiemetic regimens, including granisetron, ondansetron and palonosetron. Granisetron is available in iv., oral, transdermal and sc. formulations [12–15], ondansetron in iv. and oral formulations [16,17], and palonosetron in iv. and oral formulations [18,19]. Intravenous palonosetron is indicated for the prevention of CINV in both acute (within 24 h of chemotherapy administration) and delayed (more than 24 h after chemotherapy) phases following MEC, but only in the acute phase following HEC [18].
Despite the availability of effective antiemetics and comprehensive antiemetic guidelines, CINV has been reported to occur in up to 61% of patients receiving antiemetic therapy, with nausea being experienced more frequently than vomiting, and delayed CINV occurring more frequently than acute CINV [2,5,20–22]. The effects of poorly controlled CINV on healthcare resource utilization (HCRU; such as physician visits, emergency room [ER] visits and hospitalizations) are considerable, increasing the overall public health burden of cancer and its treatment [2,3,5,23,24].
Because findings from clinical trials investigating CINV control with antiemetic agents may not reflect real-world experience, we conducted a retrospective study to evaluate the real-world effectiveness of guideline-recommended palonosetron-containing antiemetic regimens in patients receiving selected HEC and MEC treatments.
Patients & methods
Study design
This was a retrospective longitudinal database analysis of third-party payer claims containing longitudinal medical (outpatient and inpatient) and pharmacy claims data, including patients covered by employer-sponsored and government insurance programs (Medicare, Medicare Advantage and Medicaid). Selected patients were aged 18 years or older with a diagnosis of any solid tumor (presence of at least one nondiagnostic medical claim with an International Classification of Diseases, Ninth Revision [ICD-9] code of 140–151.x, 153.x, 156–157.x, 159.xx, 162.x, 164.x, 170.x, 172.x, 174–176.x, 179, 180–189.x, 193 or 195.x) and had initiated first-line treatment with a HEC regimen (anthracycline ± cyclophosphamide, or cisplatin) or carboplatin between 1 January 2012 and 31 December 2014. The data cutoff was 31 December 2015. Patients were required to have completed first-line chemotherapy, as evidenced by a discontinuation of therapy (gap of >90 days), or to have switched to a subsequent treatment regimen. Cycles were approximated based on the dates of claims for the infusion of chemotherapy. Patients must have been treated with a three-drug antiemetic regimen comprising palonosetron – an NK-1 RA – and dexamethasone if they had received HEC, and with a palonosetron-containing antiemetic regimen if they had received carboplatin; they also must have had data available for the full first line of therapy treatment period, including time for claims maturation. All claims had been fully adjudicated by the time of data access. Patients were excluded if they had been participating in any interventional clinical trial, received benzodiazepines within 7 days of starting chemotherapy and antiemetics, received radiation therapy -7 to +6 days from the first day of the chemotherapy cycle, or if records were not available in the database for 1 month prior to the first dose of chemotherapy. As the research involved the de-identified Health Insurance Portability and Accountability Act of 1996 (HIPAA)-compliant database, no institutional review board approval was necessary.
Objectives
The objectives of the study were to assess the following over cycle 1 and across all cycles of the selected HEC and MEC regimens by patient and by patient cycle: nausea and vomiting events, HCRU, rescue medication use, changes in prophylactic antiemetic regimens and antiemetic efficacy. In addition, the study compared differences in these parameters between patients receiving HEC and MEC.
Assessments
Nausea and vomiting events were recorded at any time during each chemotherapy cycle, regardless of whether they occurred during the acute or delayed phase of CINV. Events were assessed by ICD-9 codes [25]. Data were included in the analysis if the ICD-9 codes used in the claims database were consistent with symptoms or outcomes related to CINV, as assessed by the treating physician (Table 1). Any code or combination of codes occurring on chemotherapy cycle day 1 was considered one event; if a code was identified on a subsequent day, that was defined as a separate CINV event. ICD-9 codes were used, as they designate the diagnosis for which a service was performed (whereas Current Procedural Technology [CPT] codes indicate a claim for a service provided). Thus, nausea and vomiting events were defined using diagnoses only, so as not to identify services that might have been delivered for other diagnoses (e.g., a hydration service administered for diarrhea).
| ICD-9 code | Definition |
|---|---|
| 787.03 | Vomiting alone |
| 263.9 | Protein calorie malnutrition, unspecified |
| 276.1 | Hypo-osmolality |
| 458.0 | Orthostatic hypotension |
| 458.9 | Hypotension, unspecified |
| 536.2 | Persistent vomiting |
| 780.2 | Syncope and collapse |
| 783.0 | Anorexia |
| 275.42 | Hypercalcemia |
| 276.50 | Volume depletion, unspecified |
| 276.51 | Dehydration |
| 530.19 | Esophagitis, other |
| 530.81 | Esophageal reflux |
| 560.39 | Impaction intestine, other |
| 564.00 | Unspecified constipation |
| 564.09 | Constipation, other |
| 780.79 | Malaise/fatigue, other |
| 787.01 | Nausea with vomiting |
| 787.02 | Nausea alone |
| 276.5x | Volume depletion |
| 276.xx | Disorders of fluid and electrolyte and acid base balance |
CINV: Chemotherapy-induced nausea and vomiting; ICD-9: International Classification of Diseases, ninth revision.
Data from Centers for Disease Control and Prevention [25].
The duration of the first line of therapy was measured as the time from the start of the first line of therapy until the start of the second line of therapy. The time to discontinuation of the first line of therapy was measured as the time from the start of the first line of therapy to the last injection date for the first line of therapy prior to the patient receiving the next line of therapy.
HCRU associated with CINV events was determined by the numbers of all-cause (scheduled or unscheduled) and CINV-related physician clinic visits, ER visits and hospitalizations by cycle for cycle 1 and across all cycles.
Scheduled prophylactic antiemetic regimen changes (i.e., deliberate changes to a prophylactic antiemetic regimen to be administered) were determined by cycle for cycle 1 and across all cycles. Rescue medication use (i.e., addition of an unscheduled antiemetic), calculated from day 2 of chemotherapy onward by cycle for cycle 1 and across all cycles, was assessed by a claim for any antiemetic drug not already prescribed from the date after chemotherapy treatment to the end of the CINV episode during each chemotherapy cycle.
Antiemetic efficacy was determined by the absence of a CINV event over cycle 1 and across all cycles. A CINV event was defined as any event listed in the ICD-9 codes (e.g., nausea, vomiting or dehydration), and the administration of an unscheduled iv. antiemetic. An unscheduled iv. antiemetic was defined as any antiemetic that was not prescribed prior to chemotherapy and that started on chemotherapy day 2 or later.
Data were collected and analyzed for the duration of the first-line chemotherapy regimen. Other collected data included follow-up time from diagnosis, duration of first-line chemotherapy, time from start of first-line chemotherapy to discontinuation, time from diagnosis to first-line chemotherapy discontinuation and number of chemotherapy treatment cycles. The duration of chemotherapy was defined as day 1 of each chemotherapy cycle to day -1 of the next cycle. Assessments were done for all cycles and for cycle 1 only.
Statistical methods
Patient baseline demographics and treatment characteristics were analyzed using descriptive statistics. Categorical variables were tabulated as frequency and percentage. Continuous variables were calculated as mean (standard deviation [SD]) and median (range). χ2 and Fisher’s exact tests were conducted to determine differences in CINV events and HCRU between HEC and MEC regimens. This is a retrospective study; the comparisons presented are for trends and/or informative purposes only. All ‘significance’ results should be qualified as such. There is no scientific basis for statistical significance claims between retrospective groups.
Results
Patients & treatments
In total, 1587 patient records met the inclusion criteria, 1299 of whom received HEC (AC, n = 1247; cisplatin, n = 52), and 288 of whom received MEC (carboplatin) (Figure 1). The analysis population was mainly women (91%), the mean age of patients at the time of their first line of chemotherapy was 54.8 years, and most patients (79%) had breast cancer (Table 2). The mean comorbidity index was 1.0 for all patients at diagnosis, and 1.9 at the start of the first line of chemotherapy. Most patients had commercial medical insurance plans (53%).
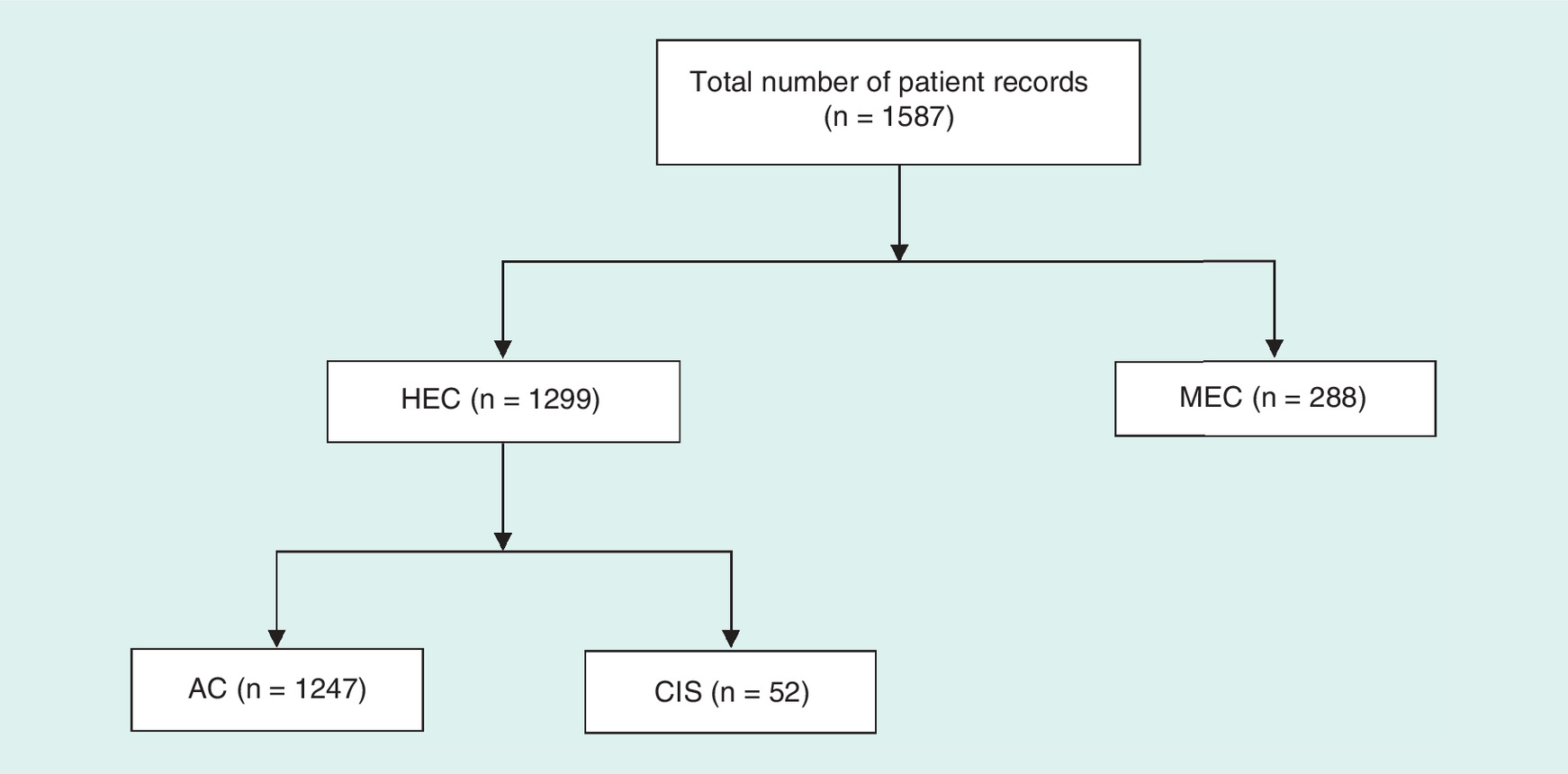
Figure 1. Patient disposition.
AC: Doxorubicin + cyclophosphamide-containing regimen; CIS: Cisplatin-containing regimen; HEC: Highly emetogenic chemotherapy; MEC: Moderately emetogenic chemotherapy.
| Demographics | HEC (AC) n = 1247 | HEC (CIS) n = 52 | HEC all n = 1299 | MEC (CARBO) n = 288 | Total n = 1587 |
|---|---|---|---|---|---|
| Age, years, mean (SD) | |||||
| At diagnosis | 52.7 (10.9) | 58.5 (11.7) | 53.0 (11.0) | 61.8 (15.4) | 54.6 (12.4) |
| At start of first LOT | 53.0 (10.9) | 58.7 (11.9) | 53.2 (11.0) | 62.1 (15.5) | 54.8 (12.4) |
| Sex, % | |||||
| Female | 99 | 38 | 97 | 67 | 91 |
| Male | 1 | 62 | 3 | 33 | 9 |
| Race, % | |||||
| White | 17 | 29 | 17 | 29 | 19 |
| African American | 8 | 13 | 8 | 2 | 7 |
| Asian or Pacific Islander | 1 | 2 | 1 | 2 | 1 |
| Other | 21 | 13 | 21 | 10 | 19 |
| Unknown | 53 | 42 | 53 | 56 | 54 |
| Cancer type, % | |||||
| Breast | 99 | 3 | 96 | 5 | 79 |
| Lung | 1 | 4 | 0 | 17 | 3 |
| Head and neck | 0 | 60 | 3 | 3 | 3 |
| Ovarian | 0 | 13 | 0 | 31 | 6 |
| Cervical | 0 | 8 | 0 | 2 | 1 |
| Endometrial | 0 | 0 | 0 | 18 | 3 |
| Other | 0 | 12 | 1 | 24 | 5 |
| Comorbidity index, mean (SD) | |||||
| At diagnosis | 0.7 (1.6) | 2.5 (2.8) | 0.8 (1.7) | 2.0 (2.5) | 1.0 (2.0) |
| At start of first LOT | 1.5 (2.3) | 3.2 (2.8) | 1.6 (2.4) | 3.3 (2.7) | 1.9 (2.5) |
| Age-adjusted comorbidity index, mean (SD) | |||||
| At diagnosis | 2.6 (2.1) | 4.9 (3.3) | 2.7 (2.2) | 4.7 (3.1) | 3.0 (2.4) |
| At start of first LOT | 3.3 (2.6) | 5.7 (3.2) | 3.4 (2.7) | 5.9 (3.3) | 3.9 (2.9) |
| Payer type, % of patients | |||||
| Commercial | 60 | 33 | 59 | 28 | 53 |
| Medicaid | 17 | 21 | 17 | 17 | 17 |
| Medicare | 16 | 31 | 17 | 48 | 23 |
| Other | 6 | 15 | 7 | 7 | 7 |
| Region, % of patients | |||||
| Midwest | 29 | 15 | 29 | 19 | 27 |
| Northeast | 27 | 33 | 27 | 27 | 27 |
| South | 23 | 40 | 24 | 29 | 25 |
| West | 18 | 10 | 18 | 20 | 18 |
| Unknown | 2 | 2 | 2 | 5 | 3 |
AC: Doxorubicin + cyclophosphamide-containing regimen; CARBO: Carboplatin-containing regimen; CIS: Cisplatin-containing regimen; HEC: Highly emetogenic chemotherapy; LOT: Line of therapy; MEC: Moderately emetogenic chemotherapy; SD: Standard deviation.
The most common first line of chemotherapy in the overall analysis population was an AC-containing regimen (79%), and the mean duration of first-line chemotherapy (time from start of first-line therapy until start of second-line therapy) was 10.8 months, although the duration of first-line chemotherapy was longer in the HEC group (12.3 months) than in the MEC group (4.1 months). The mean time to discontinuation of first-line chemotherapy over cycles 1–4 was 6.9 months. The mean number of treatment cycles overall was 3.5, with a median of 4 (range 1–16). For the HEC and MEC groups, the median (range) numbers of chemotherapy cycles administered were 4 (1–10) and 3 (1–16), respectively. Chemotherapy regimens, durations of therapy and mean number of cycles by HEC and MEC subgroups are shown in Table 3.
| HEC (AC) n = 1247 | HEC (CIS) n = 52 | HEC all n = 1299 | MEC (CARBO) n = 288 | Total n = 1587 | |
|---|---|---|---|---|---|
| Follow-up time from diagnosis, months, mean (SD) | 19.5 (13.5) | 13.3 (15.1) | 19.2 (13.6) | 12.5 (11.9) | 18.0 (13.6) |
| Time to discontinuation from diagnosis, months, mean (SD) | 9.8 (9.7) | 7.2 (12.6) | 9.7 (9.9) | 7.6 (9.5) | 9.3 (9.8) |
| Duration of first LOT,† months, mean (SD) | 12.6 (12.1) | 4.4 (8.7) | 12.3 (12.0) | 4.1 (6.5) | 10.8 (11.7) |
| Time to discontinuation of first LOT for cycles 1–4, months,‡ mean (SD) | 7.6 (8.4) | 4.4 (7.3) | 7.4 (8.4) | 4.4 (6.4) | 6.9 (8.1) |
| Number of chemotherapy treatment cycles, mean (SD) | 3.5 (0.9) | 2.3 (1.9) | 3.5 (1.1) | 3.6 (2.8) | 3.5 (1.5) |
| Chemotherapy regimen, % | |||||
| – Monotherapy | 0 | 100 | 4 | 100 | 21 |
| – Combination therapy | 100 | 0 | 96 | 0 | 79 |
| First chemotherapy LOT, n (%) | |||||
| – AC | 1240 (99) | 0 | 1240 (95) | 0 | 1240 (78) |
| – Epirubicin + cyclophosphamide | 7 (1) | 0 | 7 (1) | 0 | 7 (<1) |
| – CIS | 0 | 52 (100) | 52 (4) | 0 | 52 (3) |
| – CARBO | 0 | 0 | 0 | 288 (100) | 288 (18) |
†Duration of first LOT was measured as the time from the start of the first LOT until the start of the second LOT.
‡Time to discontinuation was measured as time from start of the first LOT to the last injection date for the first LOT prior to the patient receiving the next LOT.
AC: Doxorubicin + cyclophosphamide-containing regimen; CARBO: Carboplatin-containing regimen; CIS: Cisplatin-containing regimen; HEC: Highly emetogenic chemotherapy; LOT: Line of therapy; MEC: Moderately emetogenic chemotherapy; SD: Standard deviation.
Table 4 shows antiemetic regimens administered during the first line of chemotherapy, overall and by HEC and MEC subgroups. In the HEC group, the most common prophylactic antiemetic regimen (in 92% of patients) was an iv. NK-1 RA plus palonosetron plus dexamethasone; in the MEC group, the most common antiemetic regimen (in 52% of patients) was palonosetron plus dexamethasone.
| Chemotherapy regimen, n (%) | HEC (AC) n = 1247 | HEC (CIS) n = 52 | HEC all n = 1299 | MEC (CARBO) n = 288 | Total n = 1587 |
|---|---|---|---|---|---|
| iv. NK-1 RA + ondansetron + palonosetron + DEX | 0 | 0 | 0 | 11 (4) | 0 |
| iv. NK-1 RA + palonosetron + DEX | 1143 (92) | 49 (94) | 1192 (92) | 64 (22) | 1256 (79) |
| iv. NK-1 RA + palonosetron + DEX + PO NK-1 RA | 0 | 0 | 0 | 0 | 0 |
| Ondansetron + palonosetron + DEX | 0 | 0 | 0 | 25 (9) | 25 (2) |
| Palonosetron + DEX | 0 | 0 | 0 | 149 (52) | 149 (9) |
| Palonosetron + DEX + PO NK-1 RA | 104 (8) | 3 (6) | 105 (7) | 0 | 105 (6) |
| iv. NK-1 RA + palonosetron | 0 | 0 | 0 | 4 (1) | 4 (<1) |
| Ondansetron + palonosetron | 0 | 0 | 0 | 6 (2) | 6 (<1) |
| Granisetron + palonosetron + DEX | 0 | 0 | 2 (<1) | 0 | 2 (<1) |
| iv. NK-1 RA + ondansetron + DEX | 0 | 0 | 0 | 0 | 11 (1) |
| Palonosetron | 0 | 0 | 0 | 29 (10) | 29 (2) |
AC: Doxorubicin + cyclophosphamide-containing regimen; CARBO: Carboplatin-containing regimen; CIS: Cisplatin-containing regimen; DEX: Dexamethasone; HEC: Highly emetogenic chemotherapy; iv.: Intravenous; MEC: Moderately emetogenic chemotherapy; NK-1 RA: Neurokinin 1 receptor antagonist; PO: Oral.
CINV events
The frequency of CINV events across all cycles by patient and by patient cycle for HEC and MEC groups is shown in Figure 2. There was a significant difference between HEC and MEC groups for CINV events by patient cycle, with CINV events in 40% of HEC cycles and 44% of MEC cycles (p = 0.01). At the patient level, there was no significant difference in the proportion of patients experiencing CINV events between the HEC (51%) and MEC (52%) groups.
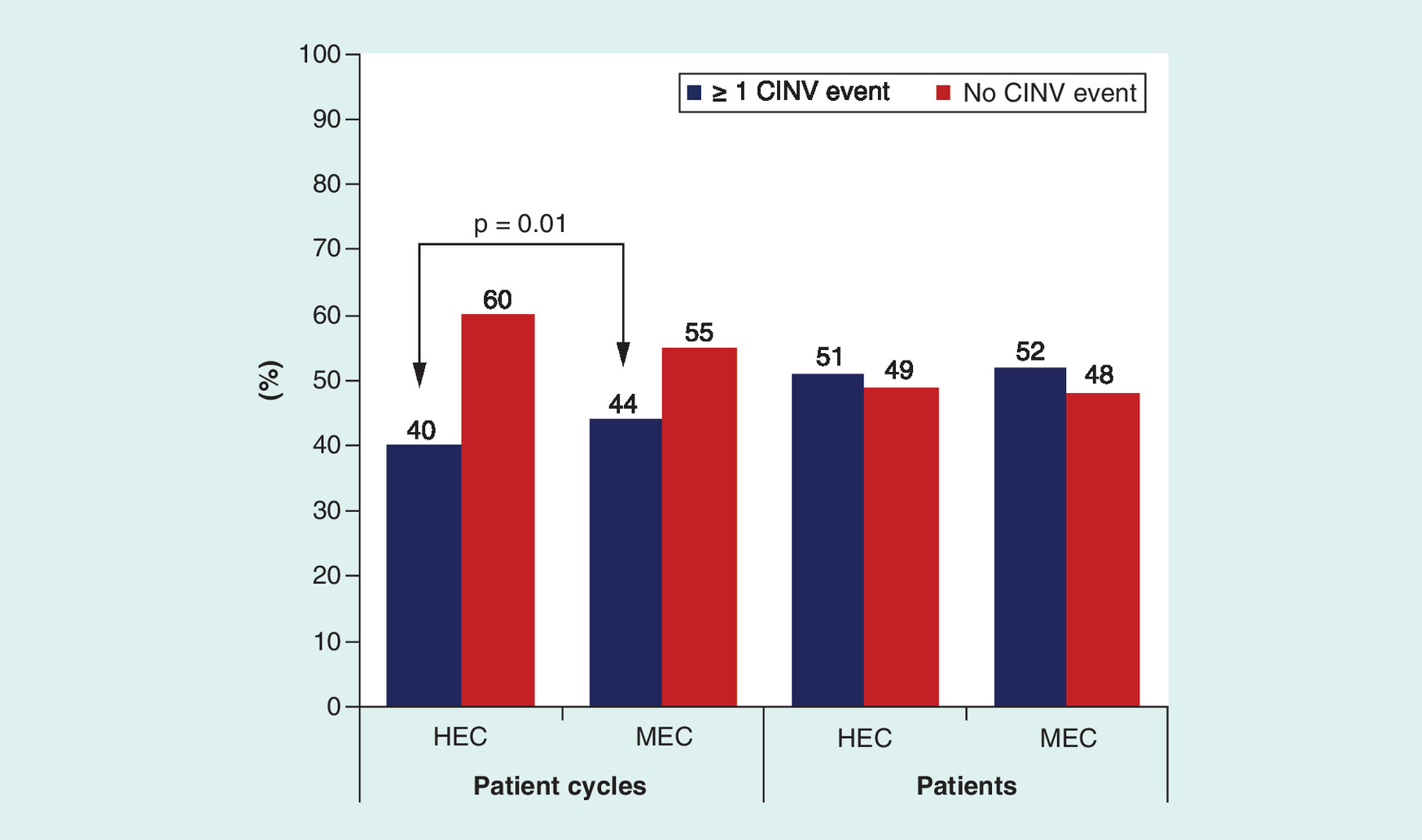
Figure 2. Chemotherapy-induced nausea and vomiting events in highly and moderately emetogenic chemotherapy groups across all chemotherapy cycles.
There was a significant difference between the HEC and MEC groups for CINV events by patient cycle (p = 0.01).
CINV: Chemotherapy-induced nausea and vomiting; HEC: Highly emetogenic chemotherapy; MEC: Moderately emetogenic chemotherapy.
In cycle 1 only, a significantly lower proportion of patients had CINV events in the HEC group than in the MEC group at the patient level (39 vs 45%; p = 0.04).
Healthcare resource utilization
Across all cycles at the patient cycle level, there was no difference in the frequency of clinic visits for any reason between HEC (97%) and MEC (96%) groups. Across all cycles at the patient level, the majority of patients had clinic visits for any reason, but the proportion was higher among patients receiving HEC than among patients receiving MEC (99 vs 97%, respectively; p = 0.01). Clinic visits due to CINV were not significantly different at the patient cycle level between HEC (38%) and MEC (40%) groups, but significantly more patients receiving HEC than MEC (48 vs 42%, respectively; p = 0.05) had a CINV-related clinic visit (Figure 3).

Figure 3. Clinic visits due to chemotherapy-induced nausea and vomiting in highly and moderately emetogenic chemotherapy groups across all chemotherapy cycles.
There was a significant difference between the HEC and MEC groups for the proportion of patients who had clinic visits due to CINV (p = 0.05).
CINV: Chemotherapy-induced nausea and vomiting; HEC: Highly emetogenic chemotherapy; MEC: Moderately emetogenic chemotherapy.
The proportions of patients with ER visits for any cause and for CINV were low overall. However, across all cycles, significantly more patient cycles in the HEC group had an ER visit for any cause compared with the MEC group (8 vs 5%; p = 0.05), although there was no significant difference between HEC (13%) and MEC (14%) groups in any-cause ER visits at the patient level. For ER visits due to CINV, there was no significant difference between HEC and MEC groups at the patient cycle level or at the patient level (Figure 4).
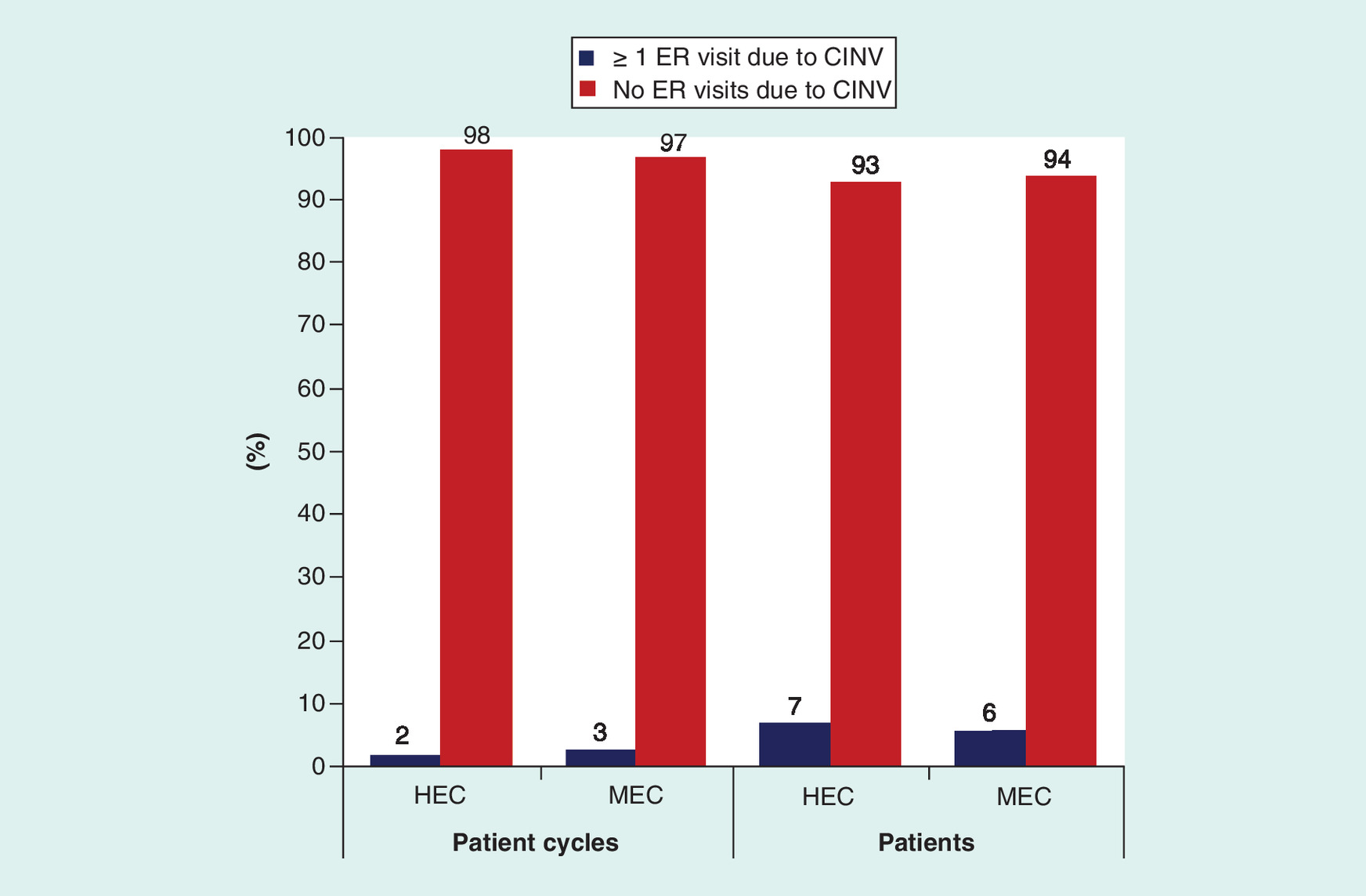
Figure 4. Emergency room visits due to chemotherapy-induced nausea and vomiting in highly and moderately emetogenic groups across all chemotherapy cycles.
CINV: Chemotherapy-induced nausea and vomiting; ER: Emergency room; HEC: Highly emetogenic chemotherapy; MEC: Moderately emetogenic chemotherapy.
The proportions of hospitalizations for any reason and for CINV were low overall. There were no differences at the patient cycle or patient level between HEC and MEC groups in the frequency of hospitalizations for any cause or due to CINV across all cycles (Figure 5).

Figure 5. Hospitalizations due to chemotherapy-induced nausea and vomiting in highly and moderately emetogenic groups across all chemotherapy cycles.
CINV: Chemotherapy-induced nausea and vomiting; HEC: Highly emetogenic chemotherapy; MEC: Moderately emetogenic chemotherapy.
For cycle 1 only, clinic visits for any reason (scheduled or unscheduled) were significantly higher in the HEC group than in the MEC group (98 vs 95%; p = 0.01), but there was no difference in the proportion of patients with CINV-related clinic visits between the HEC and MEC groups (37 vs 40%, respectively).
The frequency of ER visits in cycle 1 was low overall. There was no difference between HEC and MEC groups in the percentage of patients with at least 1 ER visit for any reason (7 vs 8%, respectively) and for CINV (3 vs 4%, respectively).
The incidence of hospitalization during cycle 1 was low. A lower proportion of patients in the HEC group than in the MEC group had hospitalizations for any reason (2 vs 5%; p < 0.01) and because of CINV (1 vs 3%, respectively; p < 0.01).
Antiemetic regimen changes
Antiemetic regimen changes were recorded as either unscheduled changes, in other words, a new ‘rescue’ medication administered in the clinic from day 2 after chemotherapy administration and in addition to the prescribed antiemetic regimen, or a scheduled (deliberate) change to the prescribed prophylactic antiemetic regimen.
Across all cycles, significantly more patient cycles in the HEC group than in the MEC group had unscheduled iv. antiemetic regimen changes (41 vs 35%, respectively; p < 0.05). A similar result was also found at the patient level for all cycles (39 vs 27%, respectively; p < 0.05) (Figure 6A). Moreover, in cycle 1 only, a significantly higher proportion of patients in the HEC group than in the MEC group had unscheduled iv. antiemetic regimen changes (39 vs 27%, respectively; p < 0.01).
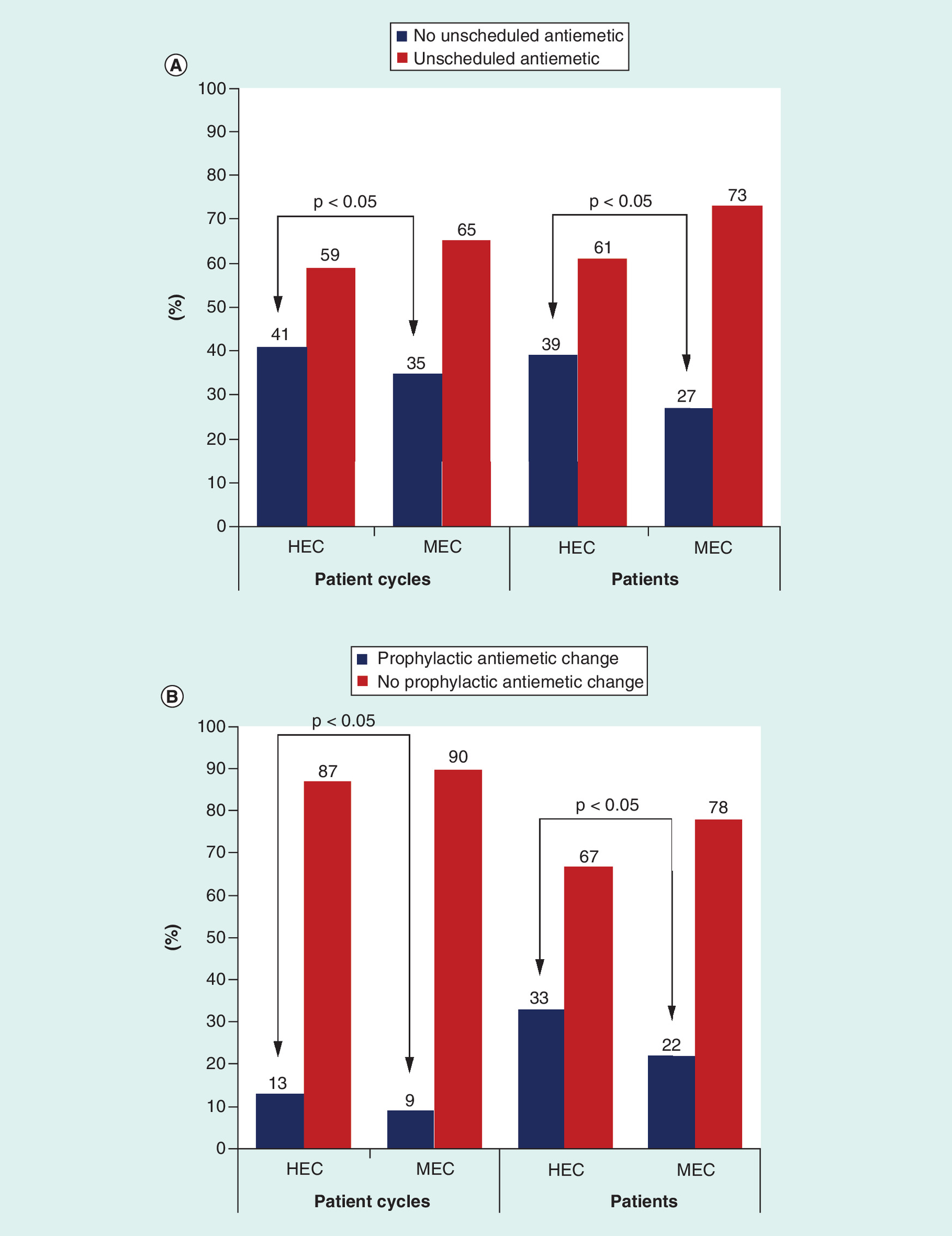
Figure 6. Unscheduled (rescue medication use) and prophylactic antiemetic regimen changes in highly and moderately emetogenic group across all chemotherapy cycles.
(A) Unscheduled antiemetic regimen changes. (B) Prophylactic antiemetic regimen changes. There were significant differences between the HEC and MEC groups in unscheduled iv. antiemetic regimen changes and in deliberate changes in prescribed prophylactic antiemetic regimens by patient cycle and by patient (p = 0.05 in each case).
HEC: Highly emetogenic chemotherapy; MEC: Moderately emetogenic chemotherapy.
Regarding deliberate changes to the prophylactic antiemetic regimens prescribed, there were significantly more changes for the HEC versus MEC groups over all the cycles at the patient cycle level (13 vs 9%, respectively; p < 0.05) and at the patient level (33 vs 22%, respectively; p < 0.05) (Figure 6B).
Antiemetic efficacy
Across all cycles, antiemetic efficacy was significantly higher in the HEC group than in the MEC group at the patient cycle level (40 vs 35%; p = 0.01) and at the patient level (38 vs 27%, respectively; p < 0.05). Findings for cycle 1 only were similar; antiemetic efficacy was significantly higher in the HEC group compared with the MEC group (38% of patients vs 27%, respectively; p < 0.01).
Discussion
The objectives of this retrospective claims database analysis were to assess CINV events, HCRU, rescue medication use, changes in prophylactic antiemetic regimens and antiemetic efficacy for cycle 1 and across all cycles of selected HEC (AC-containing or cisplatin-containing) or MEC (carboplatin-containing) regimens. Most of the 1587 patients in the analysis were women, and the majority had breast cancer.
Prescribed prophylactic antiemetic regimens reflected the emetogenicity of the chemotherapy administered. A three-drug antiemetic regimen of an iv. NK-1 RA plus palonosetron plus dexamethasone was prescribed for almost all patients receiving HEC (92%), consistent with the three-drug regimen of an NK-1 RA, 5-HT3 RA and dexamethasone recommended by major antiemetic guidelines [6,9,10]. For patients receiving MEC, the antiemetic regimens were more diverse, with approximately half of patients being prescribed a two-drug regimen of palonosetron plus dexamethasone (consistent with antiemetic guidelines for MEC) [6,9,11] and 22% receiving a three-drug regimen of a 5-HT3 RA, an NK-1 RA and dexamethasone (consistent with NCCN guidelines for patients with additional risk factors for CINV [6], and with MASCC/ESMO guidelines for carboplatin-containing regimens) [11]. Because this analysis included patient records up to 2015, and the only iv. NK-1 RA available at that time was aprepitant (as the prodrug fosaprepitant), it can be assumed that all 92% patients in the HEC group and all 27% of patients in the MEC (carboplatin) group who had received an iv. NK-1 RA had received aprepitant. Most of the 7% of patients in the HEC group who had received an oral NK-1 RA were likely to have received oral aprepitant, which was approved in 2003. Oral rolapitant was not approved until September 2015, and other NK-1 RAs or formulations were not approved until after the cutoff date for the patient records analyzed. Consequently, it is reasonable to attribute differences in the efficacy of the antiemetic regimens administered in this analysis to the 5-HT3 RA, rather than to the NK-1 RA.
Approximately half of patients reported CINV events in both the HEC and MEC groups over all cycles while receiving antiemetic therapy. Thus, even though the majority of patients in the HEC group had a recommended three-drug antiemetic regimen of palonosetron plus an NK-1 RA plus dexamethasone and most patients in the MEC group had two-drug or three-drug prophylactic antiemetic regimens, CINV prophylaxis was insufficient. Antiemetic efficacy data also support the poor control of CINV, with only about a third of patients in the HEC and MEC groups achieving antiemetic efficacy over all cycles.
HCRU was measured by the proportion of CINV-related clinic visits, ER visits and hospitalizations. Approximately a third to one-half of patients and patient cycles had CINV-related clinic visits across all cycles, occurring in a higher percentage of patients in the HEC than in the MEC group, as might be expected. Although ER visits and hospitalizations related to CINV were infrequent, a small proportion of patients (<10%) had ER visits or were hospitalized in the HEC and MEC groups, despite prophylactic antiemetic therapy. The use of unscheduled antiemetics (rescue medication), another measure of resource utilization, reflected the findings of poor CINV control, as approximately a third of patients reported rescue medication use.
In this analysis of real-world data, 61% of patients receiving HEC had no CINV event in cycle 1 and a third had no CINV event and no unscheduled iv. antiemetic when receiving a palonosetron-containing three-drug antiemetic regimen. These findings are consistent with data from two prospective observational studies of the antiemetic efficacy of palonosetron-containing three-drug antiemetic regimens in real-world settings. In the INSPIRE study of adherence to consensus antiemetic guidelines in US community oncology practices, 94% of patients received a palonosetron-containing regimen. For patients undergoing HEC who received guideline-consistent CINV prophylaxis (a three-drug regimen according to the NCCN guidelines at the time), antiemetic efficacy (no CINV, defined as no emesis and no clinically significant nausea) was reported in 49% of patients [26]. In another study of a guideline-consistent palonosetron-containing three-drug regimen for patients receiving HEC at oncology research centers, the overall complete response (CR) rate (no emetic episodes and no use of rescue medication for CINV) for cycle 1 was 32% [27]. In contrast, in a Phase III clinical trial in which palonosetron was used in a three-drug regimen with an NK-1 RA and dexamethasone in patients receiving HEC, 73% of patients achieved a CR over 0–120 h after chemotherapy [28]. The definitions of antiemetic efficacy differed across these studies, as some included nausea and other CINV-related events, making comparisons across studies difficult, and patient nonadherence to their prescribed antiemetic therapy and/or their inability to tolerate oral medications may have contributed to the lower efficacy of prophylactic antiemetic regimens in the real-world setting [29]. However, together these data suggest that a palonosetron-containing three-drug antiemetic regimen may not be providing sufficient antiemetic control for many patients undergoing HEC.
Consequently, alternative antiemetic regimens may be necessary to improve CINV control in patients receiving HEC or carboplatin in the outpatient setting. In 2017, an extended-release sc. formulation of the 5-HT3 RA granisetron (granisetron extended-release sc. injection [GERSC]; Sustol®) was approved, in combination with other antiemetics, for the prevention of acute and delayed CINV associated with MEC or AC-based HEC chemotherapy [15]. GERSC uses a patented Biochronomer® technology, comprising a viscous bioerodible polymer and 2% granisetron, permitting slow, controlled release of therapeutic concentrations of granisetron for 5 days or more following a single sc. injection [30,31]. In two large Phase III trials in patients with cancer, GERSC provided effective CINV control in both acute and delayed phases in patients receiving MEC or HEC [32–34]. More recently, an iv. formulation of the fixed-dose netupitant and palonosetron combination (Akynzeo®) was approved, in combination with dexamethasone, for the prevention of acute and delayed nausea and vomiting associated with HEC [35], based on bioequivalence with the oral fixed-dose formulation. In a Phase III trial in patients receiving AC chemotherapy (classified as MEC at the time the study was conducted), this combination of netupitant/palonosetron and dexamethasone (a three-drug antiemetic regimen) was superior to a two-drug antiemetic regimen of palonosetron plus dexamethasone in preventing CINV (no emesis and no rescue medication) over 5 days [36]. Both of these newer agents provide alternative options for the 5-HT3 RA component of prophylactic antiemetic regimens.
In current antiemetic guidelines, there is no preferred 5-HT3 RA in the HEC setting [6,9,10]. In the MEC setting, only the NCCN guidelines recommend GERSC or palonosetron as preferred 5-HT3 RAs in the absence of an NK-1 RA [6]. The ASCO and NCCN antiemetic guidelines were recently updated to include a four-drug regimen as an option in the HEC setting, with the addition of olanzapine to the three-drug regimen of a 5-HT3 RA plus an NK-1 RA plus dexamethasone [6,9]. This four-drug regimen has demonstrated significantly better nausea control compared with the three-drug regimen, suggesting that this regimen may be a preferred option for patients in whom nausea is a particular challenge [37].
The current retrospective analysis has some limitations, including the known issues with evaluating retrospective claims databases and the fact that CINV events were determined only based on ICD-9 codes and CPT codes. Furthermore, the definition of antiemetic efficacy used here was no CINV events and no rescue medication, which differs from the CR end point of no emesis and no rescue medication used in most clinical trials. The doses of oral rescue medication administered were not assessed. No patient-reported outcomes were evaluated. In addition, the patient population was primarily women, and female sex is a known risk factor for CINV [20,38]. The data analyzed were from patients who initiated first-line chemotherapy between 2012 and 2014, and antiemetic guidelines have been updated several times since that period. However, patients included in our analysis who received HEC (82% of the population) had to have received a three-drug antiemetic regimen comprising palonosetron, an NK-1 RA, and dexamethasone, which is a recommended antiemetic regimen according to current guidelines [6,9,10]. At the time of treatment, all carboplatin regimens were categorized as MEC, whereas certain carboplatin regimens are now categorized as HEC or requiring a three-drug antiemetic prophylactic regimen [6,9,10]. Thus, some patients in the carboplatin group may not have received antiemetic prophylaxis that is consistent with the most recent antiemetic guidelines, but considering the cancer types of these patients, it is likely that their carboplatin-containing regimen was moderately emetogenic. Nevertheless, real-world evidence on the use and antiemetic efficacy of palonosetron-containing antiemetic regimens is essential to understand the differences between findings from clinical trials, conducted in a controlled setting, and experiences in the clinic.
In conclusion, findings from this retrospective study of real-world data show that CINV control was inadequate with palonosetron-containing antiemetic regimens in patients receiving HEC or MEC (carboplatin), suggesting that alternative antiemetic regimens should be considered to improve patient quality of life and reduce HCRU.
The effects of poorly controlled chemotherapy-induced nausea and vomiting (CINV) on healthcare resource utilization (HCRU), such as physician visits, emergency room (ER) visits and hospitalizations, are considerable, increasing the overall public health burden of cancer and its treatment.
Antiemetic guidelines recommend a combination of a 5-hydroxytryptamine type 3 (5-HT3) receptor antagonist (e.g., palonosetron), a neurokinin 1 receptor antagonist and dexamethasone, with or without olanzapine, for patients scheduled to receive highly emetogenic chemotherapy (HEC).
Because findings from clinical trials investigating CINV control with antiemetics may not reflect real-world experience, we conducted a retrospective study to evaluate the real-world effectiveness of guideline-recommended palonosetron-containing antiemetic regimens in patients receiving HEC or moderately emetogenic chemotherapy (MEC).
Records from 1587 patients were assessed, most of which were from women with breast cancer who were receiving anthracycline- and cyclophosphamide-containing chemotherapy regimens.
CINV events were significantly more common in HEC patient cycles than in MEC patient cycles (40 vs 44%, respectively; p = 0.01).
Significantly more patients receiving HEC than MEC (48 vs 42%, respectively; p = 0.05) had a CINV-related clinic visit, but the proportions of ER visits and hospitalizations were low for each chemotherapy group.
Significantly more patient cycles in the HEC group than in the MEC group had unscheduled iv. antiemetic regimen changes (41 vs 35%, respectively; p < 0.05).
Antiemetic efficacy (absence of a CINV event) was significantly higher in the HEC group than in the MEC group at the patient cycle level (40 vs 35%; p = 0.01).
These data suggest that a palonosetron-containing three-drug antiemetic regimen may not provide sufficient antiemetic control for many patients undergoing HEC, and alternative antiemetic regimens may be necessary to improve CINV control in patients receiving HEC or carboplatin-containing regimens in the outpatient setting.
Financial & competing interests disclosure
Research support was provided by Heron Therapeutics, Inc., San Diego, CA, USA. LS Schwartzberg has been a consultant/advisor for Helsinn, Heron, Merck and Tesaro, and received research funding from Helsinn. SM Marks has stock ownership in Amgen, BMS and Merck, and received honoraria from Integra Connect. NY Gabrail received honoraria from AbbVie, Heron, J&J, Mateon and Taiho; is consultant/advisor for AbbVie, Bayer, Heron, J&J, and Taiho; and a member of speaker bureau for Heron, J&J and Taiho; and received research funding from AbbVie, Acerta, Amgen, Bayer, BMS, Celgene, Gilead, Halozyme, Incyte, J&J, Sanofi and Taiho. RB Geller has employment in Heron and stock ownership in Amgen, Gilead and Heron. J Kish has employment and stock ownership in Cardinal Health. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was provided by YE Yarker of SciStrategy Communications, Conshohocken, PA, USA, and funded by Heron Therapeutics, Inc., San Diego, CA, USA.
Ethical conduct of research
This was a retrospective longitudinal analysis from a de-identified HIPAA-compliant claims database, so no institutional review board approval was necessary.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Cohen L, de Moor CA, Eisenberg P, Ming EE, Hu H. Chemotherapy-induced nausea and vomiting: incidence and impact on patient quality of life at community oncology settings. Support. Care Cancer 15(5), 497–503 (2007).
2.
Haiderali A, Menditto L, Good M, Teitelbaum A, Wegner J. Impact on daily functioning and indirect/direct costs associated with chemotherapy-induced nausea and vomiting (CINV) in a U.S. population. Support. Care Cancer 19(6), 843–851 (2011).
3.
Sommariva S, Pongiglione B, Tarricone R. Impact of chemotherapy-induced nausea and vomiting on health-related quality of life and resource utilization: a systematic review. Crit. Rev. Oncol. Hematol. 99, 13–36 (2016).
•• Systematic review of the effects of chemotherapy-induced nausea and vomiting (CINV) on quality of life and resource utilization.
4.
Van Laar ES, Desai JM, Jatoi A. Professional educational needs for chemotherapy-induced nausea and vomiting (CINV): multinational survey results from 2388 health care providers. Support. Care Cancer 23(1), 151–157 (2015).
5.
Schwartzberg L, Harrow B, Lal LS, Radtchenko J, Lyman GH. Resource utilization for chemotherapy-induced nausea and vomiting events in patients with solid tumors treated with antiemetic regimens. Am. Health Drug Benefits 8(5), 273–282 (2015).
6.
NCCN. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Antiemesis–v1.2019 (2019). www.nccn.org/professionals/physician_gls/default.aspx
• National Comprehensive Cancer Network antiemesis guidelines for the prevention of CINV.
7.
Hesketh PJ, Kris MG, Grunberg SM et al. Proposal for classifying the acute emetogenicity of cancer chemotherapy. J. Clin. Oncol. 15(1), 103–109 (1997).
8.
Grunberg SM, Warr D, Gralla RJ et al. Evaluation of new antiemetic agents and definition of antineoplastic agent emetogenicity – state of the art. Support. Care Cancer 19(Suppl. 1), S43–S47 (2011).
9.
Hesketh PJ, Kris MG, Basch E et al. Antiemetics: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 13(12), 825–830 (2017).
• American Society of Clinical Oncology antiemesis guidelines for the prevention of CINV.
10.
Herrstedt J, Roila F, Warr D et al. 2016 Updated MASCC/ESMO consensus recommendations: prevention of nausea and vomiting following high emetic risk chemotherapy. Support. Care Cancer 25(1), 277–288 (2017).
• Multinational Association of Supportive Care in Cancer and European Society of Medical Oncology (MASCC/ESMO) antiemesis guidelines for the prevention of CINV following highly emetogenic chemotherapy (HEC).
11.
Roila F, Warr D, Hesketh PJ et al. 2016 updated MASCC/ESMO consensus recommendations: prevention of nausea and vomiting following moderately emetogenic chemotherapy. Support. Care Cancer 25(1), 289–294 (2017).
• MASCC/ESMO guidelines for the prevention of CINV following moderately emetogenic chemotherapy (MEC).
12.
Kytril (granisetron hydrochloride) injection, for intravenous use [prescribing information]. Genentech, Inc., South San Francisco, CA, USA (2011).
13.
Kytril (granisetron hydrochloride) tablets, oral solution [prescribing information]. Roche Pharmaceuticals, Nutley, NJ, USA (2010).
14.
Sancuso (granisetron transdermal system) [prescribing information]. Kyowa Kirin, Inc., Bedminster, NJ, USA (2017).
15.
Sustol (granisetron) extended-release injection, for subcutaneous use [prescribing information]. Heron Therapeutics, Redwood City, CA, USA (2017).
16.
Zofran (ondansetron hydrochloride) injection, for intravenous or intramuscular use [prescribing information]. GlaxoSmithKline, Research Triangle Park, NC, USA (2017).
17.
Zofran (ondansetron hydrochloride) tablets, orally disintegrating tablets, oral solution [prescribing information]. Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA.(2017).
18.
Aloxi (palonosetron HCl) injection for intravenous use [prescribing information]. Eisai Inc., Woodcliff Lake, NJ, USA (2015).
19.
Aloxi (palonosetron HCl) capsules [prescribing information]. Eisai, Inc., Woodcliff Lake, NJ, USA (2014).
20.
Hilarius DL, Kloeg PH, van der Wall E, van den Heuvel JJ, Gundy CM, Aaronson NK. Chemotherapy-induced nausea and vomiting in daily clinical practice: a community hospital-based study. Support. Care Cancer 20(1), 107–117 (2012).
21.
Bloechl-Daum B, Deuson RR, Mavros P, Hansen M, Herrstedt J. Delayed nausea and vomiting continue to reduce patients’ quality of life after highly and moderately emetogenic chemotherapy despite antiemetic treatment. J. Clin. Oncol. 24(27), 4472–4478 (2006).
22.
Escobar Y, Cajaraville G, Virizuela JA et al. Incidence of chemotherapy-induced nausea and vomiting with moderately emetogenic chemotherapy: ADVICE (Actual Data of Vomiting Incidence by Chemotherapy Evaluation) study. Support. Care Cancer 23(9), 2833–2840 (2015).
23.
Burke TA, Wisniewski T, Ernst FR. Resource utilization and costs associated with chemotherapy-induced nausea and vomiting (CINV) following highly or moderately emetogenic chemotherapy administered in the US outpatient hospital setting. Support. Care Cancer 19(1), 131–140 (2011).
•• Retrospective study of the effects of CINV on resource utilization in patients receiving HEC or MEC.
24.
Shih TYC, Xu Y, Elting LS. Costs of uncontrolled chemotherapy-induced nausea and vomiting among working-age cancer patients receiving highly or moderately emetogenic chemotherapy. Cancer 110(3), 678–685 (2007).
25.
Centers for Disease Control and Prevention, National Center for Health Statistics. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9). www.cdc.gov/nchs/icd/icd9cm.htm
26.
Gilmore JW, Peacock NW, Gu A et al. Antiemetic guideline consistency and incidence of chemotherapy-induced nausea and vomiting in US community oncology practice: INSPIRE Study. J. Oncol. Pract. 10(1), 68–74 (2014).
27.
Geller RB, McLaughlin T, McLeod K et al. Real-world effectiveness of palonosetron within a three-drug regimen to prevent chemotherapy induced nausea and vomiting (CINV) following highly emetogenic chemotherapy (HEC). J. Clin. Oncol. 34(Suppl.), Abstract e18231 (2016).
28.
Navari RM, Gray SE, Kerr AC. Olanzapine versus aprepitant for the prevention of chemotherapy-induced nausea and vomiting: a randomized Phase III trial. J. Support. Oncol. 9(5), 188–195 (2011).
29.
Kraut L, Fauser AA. Anti-emetics for cancer chemotherapy-induced emesis: potential of alternative delivery systems. Drugs 61(11), 1553–1562 (2001).
30.
Ottoboni T, Gelder MS, O'Boyle E. Biochronomer technology and the development of APF530, a sustained release formulation of granisetron. J. Exp. Pharmacol. 6, 15–21 (2014).
31.
Gabrail N, Yanagihara R, Spaczynski M et al. Pharmacokinetics, safety, and efficacy of APF530 (extended-release granisetron) in patients receiving moderately or highly emetogenic chemotherapy: results of two Phase II trials. Cancer Manag. Res. 7, 83–92 (2015).
32.
Raftopoulos H, Boccia R, Cooper W, O'Boyle E, Gralla RJ. Slow-release granisetron (APF530) versus palonosetron for chemotherapy-induced nausea/vomiting: analysis by American Society of Clinical Oncology emetogenicity criteria. Future Oncol. 11(18), 1–11 (2015).
33.
Raftopoulos H, Cooper W, O'Boyle E, Gabrail N, Boccia R, Gralla RJ. Comparison of an extended-release formulation of granisetron (APF530) versus palonosetron for the prevention of chemotherapy-induced nausea and vomiting associated with moderately or highly emetogenic chemotherapy: results of a prospective, randomized, double-blind, noninferiority Phase III trial. Support. Care Cancer 23(3), 723–732 (2015).
34.
Schnadig ID, Agajanian R, Dakhil SR et al. APF530 (granisetron inj extended-release) in a three-drug regimen for delayed CINV in highly emetogenic chemotherapy. Future Oncol. 12(12), 1469–1481 (2016).
35.
Akynzeo (netupitant and palonosetron) injection, for intravenous use [prescribing information]. Helsinn Therapeutics, Inc., Iselin, NJ, USA (2018).
36.
Aapro M, Rugo H, Rossi G et al. A randomized Phase III study evaluating the efficacy and safety of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy. Ann. Oncol. 25(7), 1328–1333 (2014).
37.
Navari RM, Qin R, Ruddy KJ et al. Olanzapine for the prevention of chemotherapy-induced nausea and vomiting. N. Engl. J. Med. 375(2), 134–142 (2016).
38.
Pirri C, Katris P, Trotter J, Bayliss E, Bennett R, Drummond P. Risk factors at pretreatment predicting treatment-induced nausea and vomiting in Australian cancer patients: a prospective, longitudinal, observational study. Support. Care Cancer 19(10), 1549–1563 (2011).
Information & Authors
Information
Published In
Copyright
© 2019 Lee S Schwartzberg, MD, FACP.
History
Received: 1 October 2018
Accepted: 23 April 2019
Published online: 9 May 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world effectiveness of palonosetron-based antiemetic regimens: preventing chemotherapy-induced nausea and vomiting. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0104
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Soumya Simhadri, Sowmya Dayyala, Anjani Devi Musinipally, Lavanya Guram, Mamatha Madavi, Ramakrishna Kancha, Krishna Chaitanya Puligundla, Generic Netupitant Plus Palonosetron and Dexamethasone for Prophylaxis of Chemotherapy-Induced Nausea and Vomiting (CINV) in Cancer Patients Receiving Highly or Moderately Emetogenic Chemotherapy: A Retrospective Study, South Asian Journal of Cancer, 10.1055/s-0044-1786001, 14, 02, (213-217), (2024).
- Matti Aapro, Karin Jordan, Florian Scotté, Luigi Celio, Meinolf Karthaus, Eric Roeland, Netupitant-palonosetron (NEPA) for Preventing Chemotherapy-induced Nausea and Vomiting: From Clinical Trials to Daily Practice, Current Cancer Drug Targets, 10.2174/1568009622666220513094352, 22, 10, (806-824), (2022).
- Keerthi Rapolu, Uday Kiran Uppada, Ramen Sinha, A. V. S. S. Subramanya Kumar, Efficacy of palonosetron in the management of postoperative nausea vomiting in oral and maxillofacial surgery, National Journal of Maxillofacial Surgery, 10.4103/njms.NJMS_346_21, 13, 2, (283-288), (2022).
- Shilpa Sunil Khanna, Muqthadir Siddiqui Mohammed Abdul, Urooj Fatima, Harshitha Garlapati, Mohd Abdul Qayyum, Sunil Kumar Gulia, Role of general anesthetic agents in postoperative nausea and vomiting, National Journal of Maxillofacial Surgery, 10.4103/njms.NJMS_146_20, 13, 2, (190-194), (2022).
- Yuko Watanabe, Yoshitaka Saito, Takashi Mitamura, Yoh Takekuma, Mitsuru Sugawara, Adding aprepitant to palonosetron does not decrease carboplatin-induced nausea and vomiting in patients with gynecologic cancer, Journal of Pharmaceutical Health Care and Sciences, 10.1186/s40780-021-00204-z, 7, 1, (2021).
- Jörg Schilling, Christian M. Kurbacher, Claus Hanusch, Steffi Busch, Martin Holländer, Janine Kreiss-Sender, Daniela Rezek, Elisa Flahaut, Meinolf Karthaus, Quality of Life Effects of an Oral Fixed Combination of Netupitant and Palonosetron in Chemotherapy-Induced Nausea and Vomiting Prevention: Real-World Evidence in Patients with Breast Cancer Receiving Anthracycline-Cyclophosphamide-Based Chemotherapy, Breast Care, 10.1159/000514891, 17, 2, (130-136), (2021).
- Matti Aapro, Florian Scotté, Yolanda Escobar, Luigi Celio, Richard Berman, Alessandra Franceschetti, Danielle Bell, Karin Jordan, Practice Patterns for Prevention of Chemotherapy-Induced Nausea and Vomiting and Antiemetic Guideline Adherence Based on Real-World Prescribing Data, The Oncologist, 10.1002/onco.13716, 26, 6, (e1073-e1082), (2021).