Economic evaluation of trifluridine and tipiracil hydrochloride in the treatment of metastatic colorectal cancer in Greece
Abstract
Aim: To evaluate the cost–effectiveness of trifluridine and tipiracil hydrochloride (FTD/TPI) compared with best supportive care (BSC) or regorafenib for the treatment of patients with metastatic colorectal cancer who have been previously treated with or are not considered candidates for available therapies including fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapies, anti-VEGF agents and anti-EGFR agents in Greece. Methods: A partitioned survival model was locally adapted from a third-party payer perspective over a 10 year time horizon. Efficacy data and utility values were extracted from published studies. Resource consumption data were obtained from local experts using a questionnaire developed for the purpose of the study and was combined with unit costs obtained from official sources. All costs reflect the year 2017 in euros. Primary outcomes were patients’ life years (LYs), quality-adjusted life years (QALYs), total costs and incremental cost–effectiveness ratios (ICERs) per QALY and LYs gained. Results: Total life time cost per patient for FTD/TPI, BSC and regorafenib was estimated to be €10,087, €1,879 and €10,850, respectively. In terms of health outcomes, FTD/TPI was associated with 0.25 and 0.11 increment in LYs compared with BSC and regorafenib, respectively. Furthermore, FTD/TPI was associated with 0.17, and 0.07 increment in QALYs compared with BSC and regorafenib, resulting in ICERs of €32,759 per LY gained and €49,326 per QALY gained versus BSC. Moreover, FTD/TPI was a dominant alternative over regorafenib. Conclusion: The results indicate that FTD/TPI may represent a cost-effective treatment option compared with other alternative therapies as a third-line treatment of metastatic colorectal cancer in Greece.
In Europe, colorectal cancer (CRC) is the most frequently diagnosed cancer and the second leading cause of cancer death [1]. More specifically, CRC was responsible for 215,000 deaths in Europe in 2012 [1]. About 20–25% of patients with CRC have metastatic disease (mCRC) by the time of diagnosis, and up to 50% will develop metastases at some point [2]. Moreover, patients with mCRC have a poor prognosis with survival rate being estimated of 5–13% at 5 years [3].
Multiple treatments such as fluorouracil, oxaliplatin, irinotecan, bevacizumab, cetuximab and panitumumab have been approved over the last decade for the management of mCRC. However, there was no approved treatment available for patients who had experienced progression after these standard regimens [4].
Regorafenib was approved by the EMA in 2013 for the treatment of adult patients with mCRC who have been previously treated with, or are not considered candidates for, available therapies [4]. Clinical trial data from the placebo-controlled Phase III CORRECT study demonstrated an increase in median overall survival (OS) of 1.4 months (6.4 vs 5.0) for regorafenib (Hazard ratio [HR]: 0.77; 95% CI: 0.64–0.94; p = 0.0052) [4].
Recently, an oral agent that combines trifluridine and tipiracil hydrochloride (FTD/TPI), has been shown to be effective in the treatment of patients with mCRC, leading to a significant survival benefit that is similar to that of regorafenib, but with limited toxicity and is therefore a potential new option [5].
More specifically, FTD/TPI is indicated for treating adults with mCRC who have been previously treated with available therapies including fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapies, anti-VEGF agents, and anti-EGFR agents [6]. The Phase III RECOURSE trial [7] results showed a clinically meaningful increase in median OS of 2 months: 7.1 versus 5.3 for FTD/TPI and placebo, respectively (HR: 0.68; 95% CI: 0.58–0.81; p < 0.0001). Moreover, the Phase II trial [8] results showed an increase in median OS was 2.4 months: 9.0 versus 6.6 for FTD/TPI and placebo, respectively (HR: 0·56; 95% CI: 0·39–0·81; p = 0·0011).
Despite the aforementioned clinical findings, a question arises regarding the relative value for money of FTD/TPI compared with other alternative therapies given the healthcare costs challenges faced in Greece and in Europe generally. In this light the objective of the present study was to evaluate the cost–effectiveness of FTD/TPI compared with best supportive care (BSC), and regorafenib for the treatment of patients with mCRC who have been previously treated with, or are not considered candidates for available therapies including fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapies, anti-VEGF agents and anti-EGFR agents in Greece.
Methods
A partitioned survival model [9] was locally adapted to evaluate the cost–effectiveness of FTD/TPI compared with BSC and regorafenib for the treatment of patients with mCRC over a life-time horizon (10 years) in Greece. Primary outcomes were patients’ LYs, QALYs, total costs and incremental ICERs per QALY and LY gained. The analysis was conducted from a third-party payer perspective (National Healthcare Fund-EOPYY). An annual discounting of 3.5% was applied to both effectiveness and cost estimations as that is the standard practice in these studies in Greece [10–12].
Model structure
The partitioned survival model consists of three health states such as pre-progression, progressed disease and death as an absorbing state (Figure 1). Patients enter the model at the ‘pre-progression’ health state and remain in this until disease progression or death. Patient's transition from the ‘post-progression’ to the ‘pre-progression’ health state is not permitted. Patients can move to the ‘dead’ state from any other health state.

Patient population
The model considers adult patients who are being treated for mCRC and who have been treated previously with, or who are not considered candidates for fluoropyrimidine-, oxaliplatin- and irinotecan-based regimens, an anti-VEGF biological therapy, and an anti-EGFR therapy but who are well enough motivated to receive further treatments.
Clinical inputs
For the comparison of FTD/TPI versus BSC, the clinical inputs were obtained from a pooled analysis of Phase III RECOURSE clinical trial [7] and Phase II clinical trial (Yoshino et al. [8]). In particular, a meta-analysis was conducted pooling individual patient data, examining primarily OS and progression-free survival (PFS). The key assumption made was that, the trials being pooled were similar in all respects. The Phase III clinical trial (RECOURSE) and the Phase II clinical trial (Yoshino et al. [8]) were both multicenter, double-blind, 2:1 randomized, placebo-controlled trials to investigate the efficacy and safety of FTD/TPI. These clinical trials had similar designs, and patients in both trials had similar disease characteristics at baseline. Also, the pooled results mirrored the individual trials.
As regards the treatment comparison of FTD/TPI versus regorafenib, in absence of head to head clinical trial, an indirect statistical method proposed by Bucher et al. [13] was undertaken to estimate the relative efficacy of regorafenib over FTD/TPI in terms of OS and PFS. More specifically, HRs reported from the CORRECT clinical trial [4] for regorafenib versus BSC were combined with the HRs reported from the RECOURSE clinical trial [7] for FTD/TPI versus BSC. Further, these estimates have been used in the recent publication of the model [9].
Safety
Adverse events (AEs) were included in the model to account for the potential cost and quality-of-life burden of experiencing events while on treatment. The incidence rates of AEs for FTD/TPI, BSC and regorafenib were extracted from RECOURSE clinical trial [7] and CORRECT clinical trial [4], respectively.
Utility weights
Utility weights are a measure of a patient's preference of a particular health state and generally range from 0 to 1 where 1 corresponds to perfect health and 0 corresponds to death. The utility values used in the base-case analysis were taken from CORRECT clinical trial [4] (as the patients in this study had previously been treated for mCRC and were at the same disease stage). More specifically, the utility values applied in model were 0.73 in the pre-progression state for FTD/TPI and regorafenib and 0.74 for BSC. In post-progression state, utility value of 0.59 was considered for all the treatments.
Moreover, utility values from the CORRECT clinical trial [4] implied a small disutility (-0.01) for patients who have not yet progressed and are actively receiving treatment. This small disutility was considered in the model to account the potential decrement in quality of life associated with receiving active treatment with FTD/TPI or regorafenib. A disutility attributable to active treatment was used due to the lack of data available to inform AE-specific utility decrements (i.e., reductions in health utility due to the occurrence of AEs), and was assumed to be reasonable given the noninferior safety profile of FTD/TPI compared with regorafenib [9].
Cost & healthcare resource use
The economic evaluation was conducted from a third-party payer perspective and as such only healthcare costs reimbursed by the payer were considered. In particular, the cost inputs considered in the model include: monitoring cost, which split into progression-free and progressed disease health state cost per cycle, as well as end-of-life care cost, drug acquisition cost, AE cost and post-progression treatment cost.
To calculate all these costs with the exception of the drug acquisition cost, healthcare resource consumption as obtained from local experts (oncologists) using a questionnaire developed for the purpose of the study, was combined with unit costs obtained from official sources. All costs refer to the year 2017 (€).
Drug acquisition costs
The drug acquisition costs were calculated by combining the drug dose of each comparator, as obtained from summary of product characteristics and validated by local experts with the corresponding reimbursed drug cost.
More specifically, in case of FTD/TPI the recommended starting dose in adults is 35 mg/m2/dose administered orally twice daily on days 1–5 and days 8–12 of each 28-day cycle as long as benefit is observed or until unacceptable toxicity occurs. Moreover, the dosing of FTD/TPI was based on patient body surface area, and therefore, estimation of the body surface area distribution for patients with late-stage mCRC was taken from RECOURSE clinical trial [7]. As for regorafenib the dose of 160 mg (four tablets of 40 mg) taken once daily for 3 weeks followed by 1 week off therapy, was considered in the model. In this point, it should be mentioned that no drug acquisition cost for BSC was considered in the analysis (Table 1).
| Description | Unit costs (€) | Source | Ref. |
|---|---|---|---|
| Pre-progression costs | |||
| Drug acquisition cost (ex-factory price) | |||
| FTD/TPI 15 mg/TAB (pack of 20 TAB) | 585.57 | Price bulletin issued by the Ministry of Health (9 June 2017) | |
| FTD/TPI 15 mg/TAB (pack of 60 TAB) | 1,806.71 | Price bulletin issued by the Ministry of Health (9 June 2017) | |
| FTD/TPI 20 mg/TAB (pack of 20 TAB) | 802.99 | Price bulletin issued by the Ministry of Health (9 June 2017) | |
| FTD/TPI 20 mg/TAB (pack of 60 TAB) | 2,408.94 | Price bulletin issued by the Ministry of Health (9 June 2017) | |
| Regorafenib 40 mg/TAB (pack of 84 TAB) | 2,198.87 | Price bulletin issued by the Ministry of Health (9 June 2017) | |
| BSC | 0 | ||
| Monitoring cost per cycle | |||
| FTD/TPI-regorafenib | 82 | Local experts, official website of EOPYY and Government Gazette (Law B′2816/22 December 2015) | [14] |
| BSC | 82 | Local experts, official website of EOPYY and Government Gazette (Law B′2816/22 December 2015) | [14] |
| Post-progression costs | |||
| Monitoring cost per cycle | 55 | Local experts, official website of EOPYY and Government Gazette (Law B′2816/22 December 2015) | [14] |
| Subsequent treatment cost per patient | |||
| FTD/TPI | 245 | Local experts, drug price bulletin issued by the Ministry of Health on 9 June 2017 and the official website of EOPYY. | [14,15] |
| Regorafenib | 301 | ||
| BSC | 0 | ||
| End of life care cost | 684 | Local experts, official website of EOPYY, Government Gazette (Law A′ 262/16 December 2011 drug price bulletin [9 June 2017]) and DRG tariffs (Σ022x & ΣO3M) | [14,16] |
BSC: Best supportive care; DRG: Diagnosis-related groups; EOPYY: National Healthcare Fund; FTD-TPI: Trifluridine and tipiracil hydrochloride;
TAB: Tablet.
The reimbursed drug costs of FTD/TPI and regorafenib were calculated on the grounds of the ex-factory prices (Official Government Gazette, law 1907/15 July 2014), as they were published in the bulletin issued on 9 June 2017 by the Greek Ministry of Health [15] with the relevant discounts implemented by the corresponding legislation (Official Government Gazette, law 115/7 August 2017) (Table 1).
Monitoring cost
The monitoring cost is split into progression-free and progressed disease health state cost per week. The monitoring of patients as long as they are on the pre-progressed or progressed health state includes laboratory tests, diagnostic tests and physician visits. The resources were obtained from two local experts and were combined with the related unit costs obtained from Government Gazette (Law B′2816/22 December 2015 and law A′262/16 December 2011) and the official website of EOPYY (Table 1) [14]. Based on local experts’ advice, the monitoring cost in pre-progression state is not treatment related but state related.
Adverse events management cost
The cost of AEs management depends on the setting in which they are treated (i.e., inpatient or outpatient). The percentage of patients requiring hospitalization for AE management was provided by the local experts. Costs for treating and managing AE in the inpatient setting were obtained from the corresponding DRGs tariffs [16] issued by the Greek Ministry of Health. Costs related to the management of AEs in an outpatient setting were estimated by combining the resources consumed, as provided by local experts, with the corresponding unit costs obtained from the drug price bulletin issued on 9 June 2017 [15] in Government Gazette (Law B′2816/2212–2015, law A′262/16 December 2011) and the official website of EOPYY [14]. Finally, a weighted cost for the management of AEs was calculated. In the model, the calculated cost for each AE was combined with the incidence rate of each AE (Supplementary Table 1, Table 1).
Progression treatment cost
Following disease progression, patients may either be treated with another treatment or receive BSC. The proportion of patients distributed to the available treatments after disease progression was provided by local experts to reflect the most common clinical practice in Greece. More specifically, in the base-case analysis patients treated with FTD/TPI and regorafenib as a third-line treatment were deemed to move onto regorafenib and FTD/TPI, respectively or BSC. While, patients treated with BSC will not receive any other treatment.
This cost was applied as a lump sum for patients upon progression. The total costs of post-progression treatment include the drug acquisition costs of FTD/TPI and regorafenib (as these were mentioned in the pre-progression state), while the cost of BSC was estimated by combining the resources consumed, as provided by local experts, with the corresponding unit costs, as derived from the price bulletin issued by the Greek Ministry of Health (Table 1) [15].
End-of-life care cost
To reflect the fact that individuals incur additional resources shortly before death, all patients who die in the model, regardless the treatment option incur an additional resource use representing the ‘end-of-life’ care. The cost of the ‘end-of-life’ care depends on the setting in which this kind of care is provided in Greece (i.e., inpatient or outpatient). The percentage of patients requiring hospitalization for ‘end-of-life care’ was provided by local experts. The cost of inpatient ‘end-of-life’ care was obtained from the corresponding DRGs tariffs [16] issued by the Greek Ministry of Health. On the other hand, the cost of ‘end-of-life’ care provided in an outpatient setting was estimated by combining the resources consumed, as provided by local experts, with the corresponding unit costs obtained from the drug price bulletin issued by the Greek Ministry of Health (Table 1) [15].
Data analysis
The aforementioned approach and data were used to calculate mean estimates of life-time costs and QALYs for each comparator. The cost–effectiveness of FTD/TPI was evaluated by calculating the incremental cost per QALY gained (ICER). For a treatment to be considered cost-effective, a Willingness-to-pay (WTP) threshold of €51,000 per QALY was used in the current analysis. This is based on the WHO guidelines that state that a treatment should be considered cost-effective if the ICER is between 1 to 3 times the Gross domestic product (GDP) per capita of that country and a treatment is considered highly cost-effective at <1 times the GDP per capita [17]. The GDP per capita in Greece was estimated at €17,000 taken from the International monetary fund estimation of GDP per capita using current prices [18].
To assess the impact of the assumptions considered in the base-case analysis, one-way sensitivity analysis (OWSA) was undertaken to test the robustness of the results by varying individual parameters between low and high values. If CIs, or similar, have been reported these were used in the OWSA, otherwise, if the parameter uncertainty was unknown a standard 20% variation was used.
Probabilistic sensitivity analysis (PSA) assesses the stochastic parametric uncertainty, which is a technique that provides an estimate of the joint uncertainty of costs and effectiveness in the simulation by assigning probabilistic distributions to key input parameters, recursively resampling new values for each parameter from their respective distribution, and subsequently estimating the costs and effectiveness of each intervention based on the new values. This process is repeated multiple times to provide an estimate of the uncertainty surrounding the cost–effectiveness of interventions. Hence, simulation modeling was used to run 1000 analyses in order to be able to construct cost–effectiveness acceptability curves, which indicate the likelihood of the incremental cost per QALY to fall below specified thresholds.
In addition, different time horizons (8, 6 and 4 years) were tested and compared with base-case analysis.
Results
Deterministic results
The base case analysis showed that over a lifetime horizon (10 years), the total lifetime cost per patient for FTD/TPI, BSC and regorafenib was estimated to be €10,087, €1,879 and €10,850, respectively (Table 2).
| Breakdown cost (€) | FTD/TPI | BSC | Regorafenib |
|---|---|---|---|
| Drug costs | 7,200 | 0 | 8,171 |
| Post-progression costs | 242 | 0 | 297 |
| Monitoring cost | 784 | 551 | 705 |
| Adverse events cost | 1,201 | 660 | 1,013 |
| End-of-life cost | 661 | 668 | 664 |
| Total cost per patient | 10,087 | 1,879 | 10,850 |
| LY | 0.89 | 0.64 | 0.78 |
| QALYs | 0.57 | 0.40 | 0.50 |
| ICER per LY gained | 32,759 | Dominant | |
| ICER per QALY gained | 49,326 | Dominant |
BSC: Best supportive care; FTD/TPI: Trifluridine and tipiracil hydrochloride; ICER: Incremental cost–effectiveness ratio; LY: Life year; QALY: Quality-adjusted life year; SD: Standard deviation.
Dominant (improve outcomes in terms of LY and QALY with reduced total cost).
In terms of health outcomes, comparing FTD/TPI with BSC, the former was associated with 0.25 and 0.17 increment in LYs and QALYs respectively. When compared with regorafenib, FTD/TPI was associated with increases of 0.11 years and 0.07 QALYs, respectively (Table 2).
Based on these findings, treatment with FTD/TPI was estimated to be a dominant strategy when compared with regorafenib (improve outcomes with reduced costs) and cost-effective when compared with BSC (ICER: €49,326 per QALY gained) under the predetermined threshold of €51,000 per QALY gained (Table 2).
One-way sensitivity analysis
The results of OWSA for the comparison of FTD/TPI versus BSC indicated that the most influential parameters on the model were utility values assigned to the post-progression state for patients treated with BSC and FTD/TPI. Varying these parameters yielded ICERs ranging from €56,048 to €43,970. Other factor that impacted the results was the annual discount rate on outcome (QALYs) causing the ICER to range from €52,547 to €46,596 (Figure 2). As for the comparison of FTD/TPI versus regorafenib, the results of OWSA reported that the HR of PFS for regorafenib was the parameter with the greatest influence on the cost–effectiveness outcomes (Figure 3). Nevertheless, it should be stressed that, in the vast majority of sensitivity analyses, FTD/TPI remained a dominant strategy compared with regorafenib.
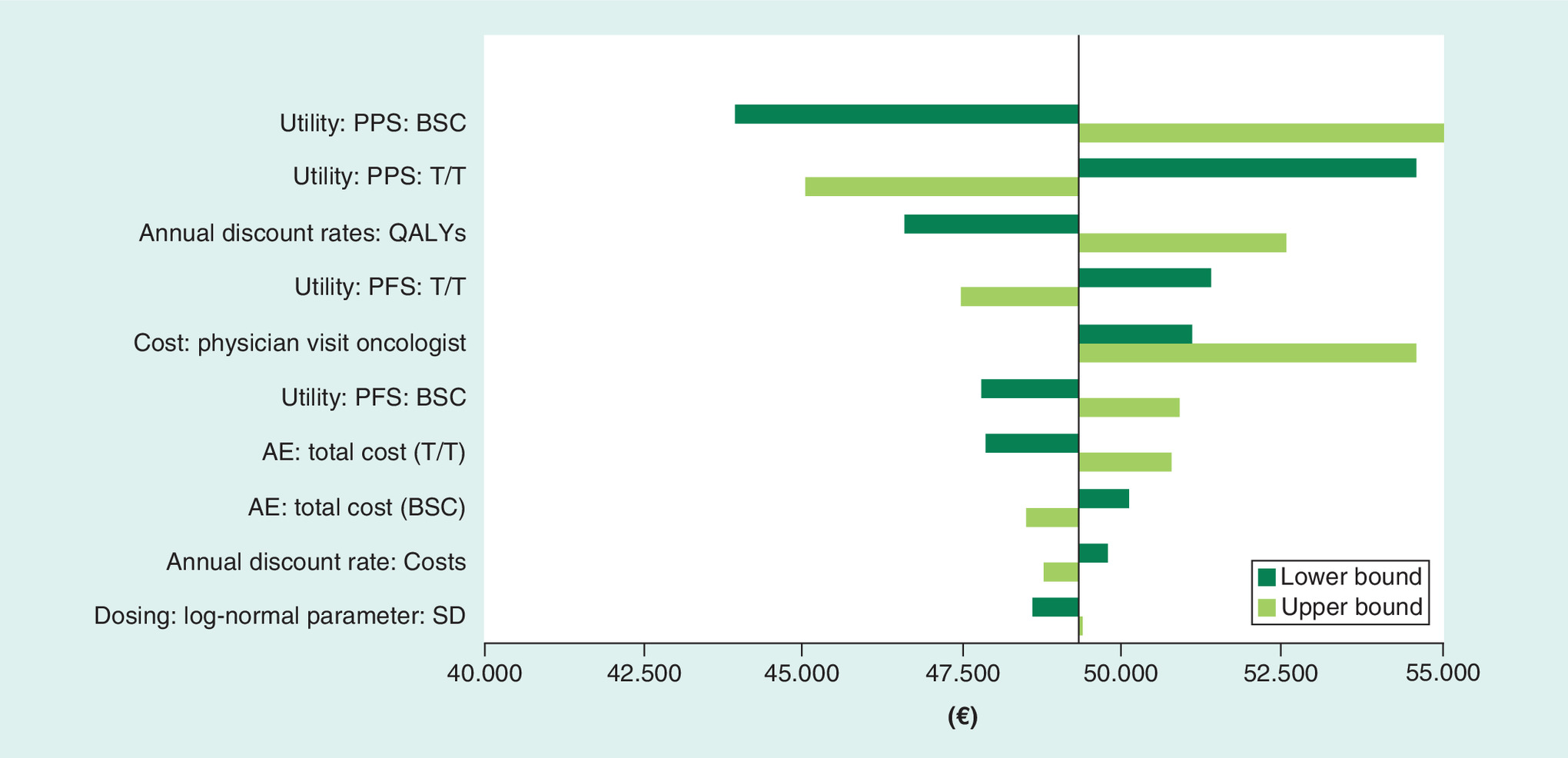
Figure 2. Tornado diagram of one-way sensitivity analysis: trifluridine and tipiracil hydrochloride versus best supportive care.
AE: Adverse event; BSC: Best supportive care; PFS: Progression-free survival; PPS: Post-progression state; QALY: Quality-adjusted life year.
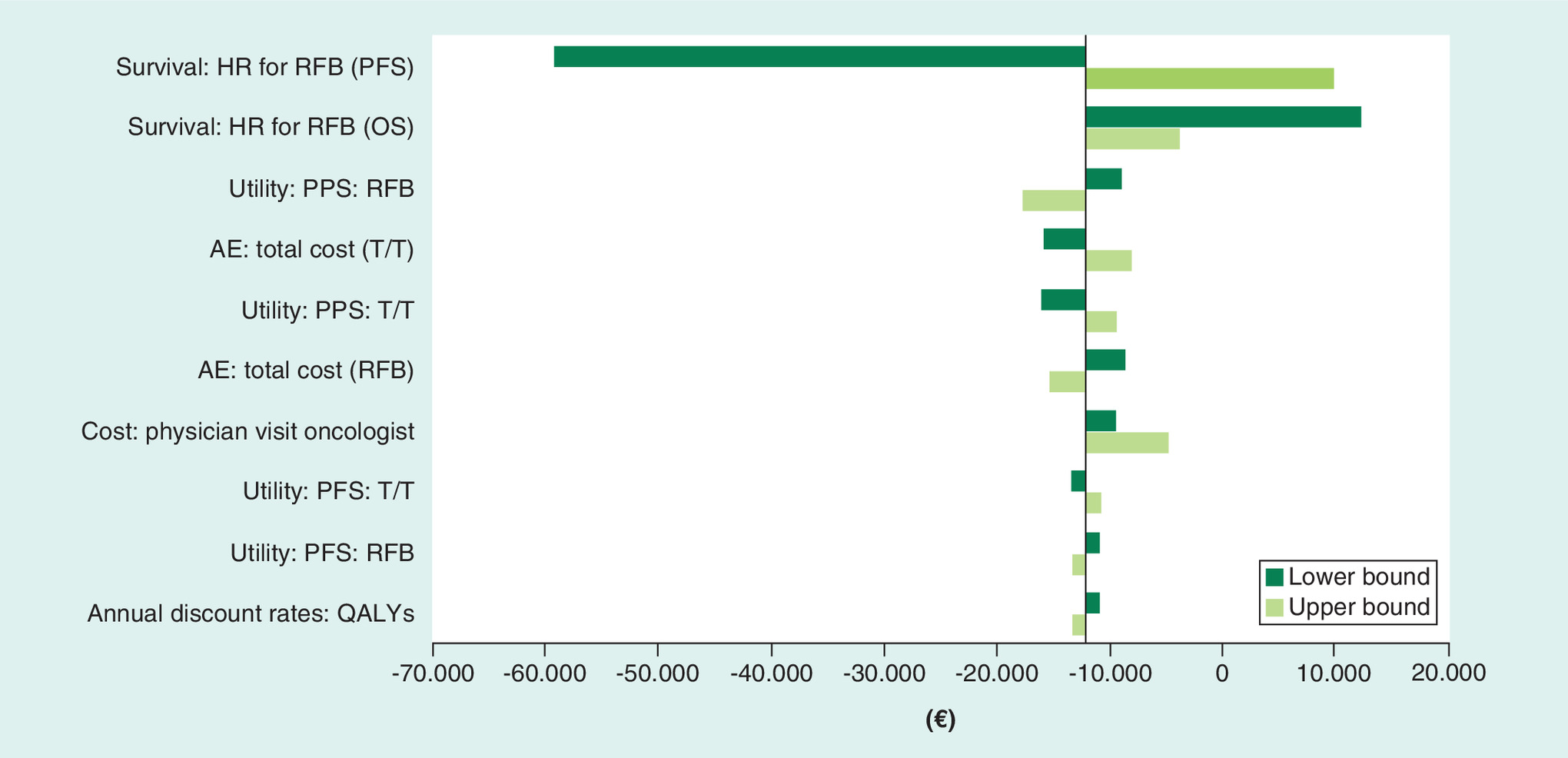
Figure 3. Tornado diagram of one-way sensitivity analysis: trifluridine and tipiracil hydrochloride versus regorafenib.
AE: Adverse event; HR: Hazard ratio; OS: Overall survival; PFS: Progression-free survival; PPS: Post-progression state; RFB: Regorafenib; FTD/TPI: Trifluridine and tipiracil hydrochloride.
Moreover, when model time horizon was set at 8, 6 and 4 years, the ICERs of FTD/TPI compared with BSC were €49,921, €51,028 and €53,029 respectively. As for the comparison of FTD/TPI versus regorafenib, although, different time horizons (8, 6 and 4 years) were considered in the model, FTD/TPI remained a dominant treatment option compared with regorafenib.
Probabilistic sensitivity analysis
The PSA confirmed the deterministic results. In particular, the analysis showed that at the predefined WTP of €51,000 per QALY gained, treatment with FTD/TPI had 45% and 89% (Figure 4) probability of being a cost-effective option compared with BSC and regorafenib, respectively.
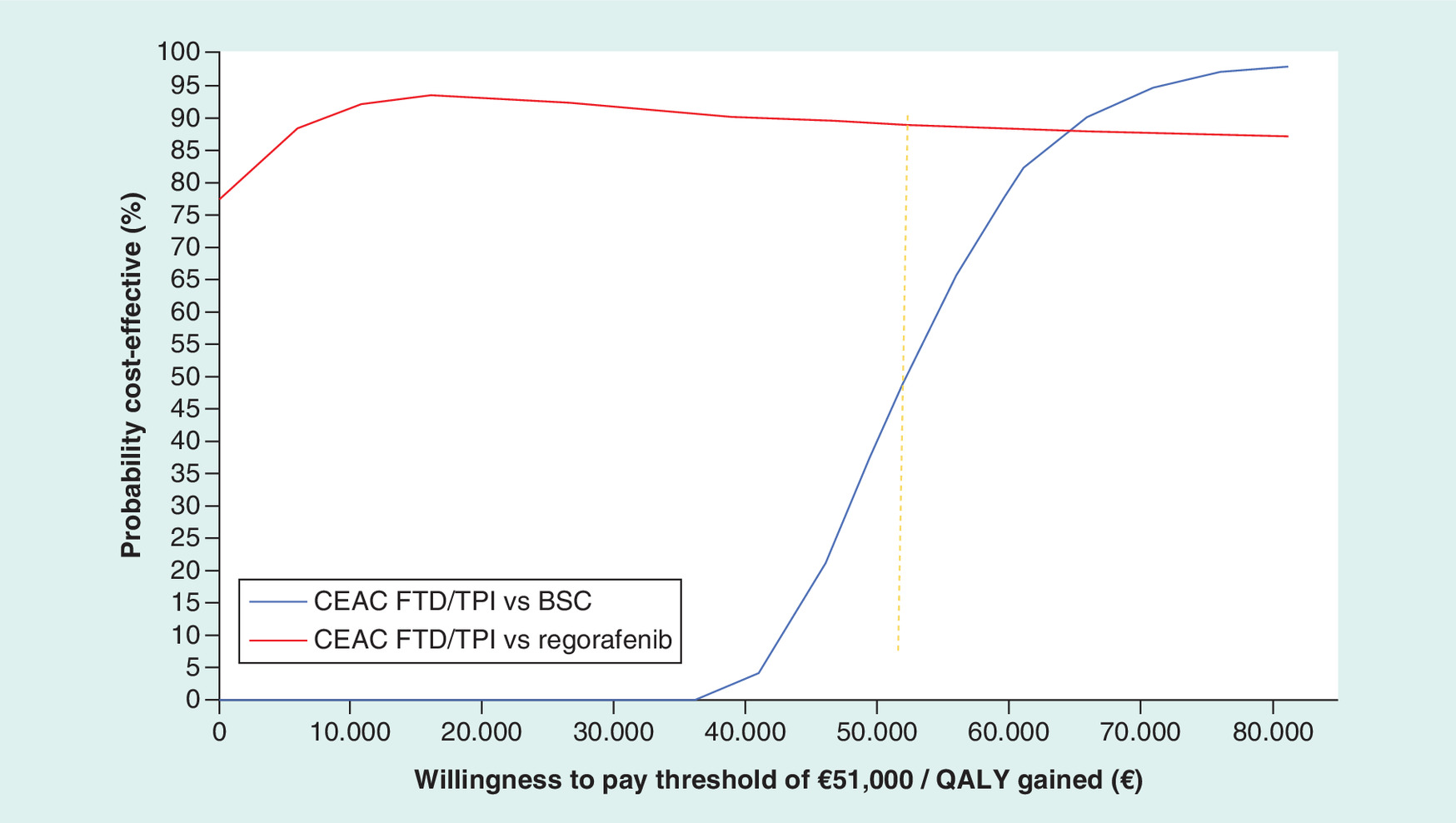
Figure 4. Cost–effectiveness acceptability curve of trifluridine and tipiracil hydrochloride versus comparators.
BSC: Best supportive care; CEAC: Cost–effectiveness acceptability curve; FTD/TPI: Trifluridine and tipiracil hydrochloride; QALY: Quality-adjusted life year.
Discussion
This economic evaluation suggests that FTD/TPI is a cost-effective treatment strategy even when it is compared with BSC, indicating that FTD/TPI represents a valuable treatment option for adult patients with mCRC who have been previously treated with, or are not considered candidates for, available therapies including fluoropyrimidine, oxaliplatin- and irinotecan-based chemotherapies, anti-VEGF agents, and anti-EGFR agents in Greece.
Over a lifetime horizon, the model showed that FTD/TPI is associated with health benefits in terms of life expectancy and quality-adjusted life expectancy over BSC and regorafenib. With respect to total cost, FTD/TPI was found to be associated with higher total cost compared with BSC and lower total cost compared with regorafenib. As such FTD/TPI may be a dominant treatment alternative over regorafenib, and cost-effective over BSC. These results are confirmed by OWSA and PSA indicating the robustness of the main results of our study.
Until the time of writing, not many published studies were found to evaluate the cost–effectiveness of FTD/TPI compared with alternative therapies in the treatment of patients with mCRC. However, it is important to mention, that our findings are in line with a recently published study [9] conducted in England and Wales. More specifically, study results indicated that FTD/TPI was a cost-effective treatment compared with BSC with an ICER of £51,194 per QALY gained and dominant option versus regorafenib.
Furthermore, a study [19] was conducted in Japan to compare the cost–effectiveness of regorafenib versus FTD/TPI. The annual direct cost related to the treatment with regorafenib or FTD/TPI was calculated. The median survival time (MST) as obtained from the CORRECT clinical trial [4] and the RECOURSE clinical trial [7] was used to evaluate the therapeutic efficacy of the regimens. The results of the study showed that the costs per patient for the regorafenib and the FTD/TPI regimen were ¥705,330 and ¥371,199, respectively, and the cost–effectiveness ratios were ¥110,208/MST and ¥52,282/MST, respectively. Hence, the FTD/TPI regimen was cost-effective compared with regorafenib regimen.
Several potential limitations to this cost–effectiveness study should be considered. First of all, in the present analysis it was assumed that the efficacy and utility data obtained from the published studies were applicable to the Greek healthcare setting. The use of these data may be challenged; however, given the absence of local data and the quality and validity of the respective study this choice was considered appropriate. Second, there was lack of direct clinical evidence for the comparison of FTD/TPI and regorafenib arms. In the absence of such a head-to-head clinical trial an indirect comparison was undertaken based on data reported by CORRECT [4] and RECOURSE [7] clinical trials. Both studies were placebo controlled, as such an indirect comparison is not expected to be biased. Nonetheless, indirect comparison is considered as a valid method as long as direct comparative trials are lacking. In addition, these clinical data were also considered in recent publication of the model [9].
Moreover, where needed, resource utilization was indicated by local experts, and experts’ consultation was sought to validate inputs considered in the model. This may raise concerns about the subjectivity of model inputs and leave space for challenging the study results. Nevertheless, a series of sensitivity analyses indicated that model outcomes are robust, since the main results remained unchanged in a wide range of parameter values.
Conclusion
To sum up, the derived ICER suggests that FTD/TPI was a cost-effective alternative compared with BSC and a dominant option compared with regorafenib, for the treatment of patients with mCRC who have had previous treatment with available therapies in Greece.
In Europe, colorectal cancer (CRC) is the most frequently diagnosed cancer and the second leading cause of cancer death.
About 20 to 25% of patients with CRC have metastatic disease (metastatic CRC [mCRC]) by the time of diagnosis, and up to 50% will develop metastases at some point.
The present study evaluates the cost–effectiveness of trifluridine and tipiracil hydrochloride (FTD/TPI) compared with best supportive care (BSC) or regorafenib for the treatment of patients with mCRC who have been previously treated with or are not considered candidates for available therapies in Greece.
A partitioned survival model was locally adapted to evaluate the cost–effectiveness of FTD/TPI compared with BSC and regorafenib for the treatment of patients with mCRC over a life-time horizon in Greece.
Efficacy data and utility values were extracted from published studies. Resource consumption data were obtained from local experts, using a questionnaire developed for the purpose of the study and was combined with unit costs obtained from official sources.
The results indicate that FTD/TPI was a cost-effective alternative compared with BSC, and a dominant option compared with regorafenib, for the treatment of patients with mCRC who have had previous treatment with available therapies in Greece.
Financial & competing interests disclosure
This study was funded by Servier Hellas. The study sponsor had no interference in the study design, data collection, data analysis or writing of the manuscript. N Maniadakis received speaker honoraria and research grants from Servier Hellas. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_file.docx)
- Download
- 21.07 KB
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur. J. Cancer 49(6), 1374–1403 (2013).
2.
Schmoll HJ, Van Cutsem E, Stein A et al. ESMO consensus guidelines for management of patients with colon and rectal cancer. a personalized approach to clinical decision making. Ann. Oncol. 23(10), 2479–2516 (2012).
3.
Chu E. An update on the current and emerging targeted agents in metastatic colorectal cancer. Clin. Colorectal Cancer 11(1), 1–13 (2012).
4.
Grothey A, Van Cutsem E, Sobrero A et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomized, placebo-controlled, Phase III trial. Lancet 381(9863), 303–312 (2013).
5.
Van Cutsem E, Cervantes A, Adam R et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 27(8), 1386–1422 (2016).
•• Guidelines for the management of patients with metastatic colorectal cancer.
6.
European Medicines Agency. Trifluridine/tipiracil (Lonsurf®) product information (2015). www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/003897/WC500206246.pdf.
7.
Mayer RJ, Van Cutsem E, Falcone A et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N. Engl. J. Med. 372(20), 1909–1919 (2015).
8.
Yoshino T1, Mizunuma N, Yamazaki K et al. TAS-102 monotherapy for pretreated metastatic colorectal cancer: a double-blind, randomized, placebo-controlled Phase II trial. Lancet Oncol. 13(10), 993–1001 (2012).
9.
Bullement A, Underhill S, Fougeray R, Hatswell AJ. Cost‐effectiveness of trifluridine/tipiracil for previously treated metastatic colorectal cancer in England and Wales. Clin. Colorectal Cancer 17(1), e143–e151 (2018).
10.
Kourlaba G, Rapti V, Alexopoulos A et al. Everolimus plus exemestane versus bevacizumab-based chemotherapy for second-line treatment of hormone receptor-positive metastatic breast cancer in Greece: an economic evaluation study. BMC Health Serv. Res. 15, 307 (2015).
11.
Maniadakis N, Kaitelidou D, Siskou O et al. Economic evaluation of treatment strategies for patients suffering acute myocardial infarction in Greece. Hellenic J. Cardiol. 46(3), 212–221 (2005).
12.
Gourzoulidis G, Kourlaba G, Kakisis J et al. Cost–effectiveness analysis of rivaroxaban for treatment of deep vein thrombosis and pulmonary embolism in Greece. Clin. Drug Investig. 37(9), 833–844 (2017).
13.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 50(6), 683–691 (1997).
14.
National Organisation for Healthcare Services Provision. Official web site of EOPYY. (2016). www.eopyy.gov.gr/Home/StartPage?a_HomePage=Index.
15.
Greek Ministry of Health. Drug price bulletin 2017. www.moh.gov.gr/articles/times-farmakwn/deltia-timwn.
16.
Greek Ministry of Health. Diagnostic related groups. www.yyka.gov.gr/articles/health/domes-kai-draseis-gia-thn-ygeia/kwdikopoihseis/709-kleista-enopoihmena-noshlia-1.
17.
Eichler HG, Kong SX, Gerth WC, Mavros P, Jönsson B. Use of cost–effectiveness analysis in health-care resource allocation decision-making: how are cost–effectiveness thresholds expected to emerge? Value Health 7(5), 518–528 (2004).
18.
International Monetary Fund. World economic outlook database. (2017). www.imf.org/external/pubs/ft/weo/2017/02/weodata/index.aspx.
19.
Kimura M, Usami E, Iwai M, Go M, Teramachi H, Yoshimura T. Comparison of cost–effectiveness of regorafenib and trifluridine/tipiracil combination tablet for treating advanced and recurrent colorectal cancer. Mol. Clin. Oncol. 5(5), 635–640 (2016).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 19 July 2018
Accepted: 20 November 2018
Published online: 14 December 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Economic evaluation of trifluridine and tipiracil hydrochloride in the treatment of metastatic colorectal cancer in Greece. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0076
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hwayoung Ahn, Kyungae Nam, Jaeyong Kim, Dong-Won Kang, Sun-Kyeong Park, A systematic review of cost-effectiveness studies of later-line treatments for refractory metastatic colorectal cancer, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2025.2603954, 26, 2, (161-169), (2025).
- Youwen Zhu, Kun Liu, Hong Zhu, TAS-102 with or without bevacizumab treatment for patients with metastatic colorectal cancer: a multi-country cost-effectiveness analysis, Therapeutic Advances in Gastroenterology, 10.1177/17562848241284998, 17, (2024).
- Jiayun Zhong, Yu Liu, Qian Fu, Dan Huang, Wenjun Gong, Jian Zou, Cost-Effectiveness Analysis of Regorafenib versus Other Third-Line Treatments for Metastatic Colorectal Cancer, Cancer Management and Research, 10.2147/CMAR.S464831, Volume 16, (593-602), (2024).
- André L. F. Azeredo-da-Silva, Victor Hugo F. de Jesus, Ion Agirrezabal, Victoria K. Brennan, Phuong L. Carion, Nathalie Amoury, Bruna M. Vetromilla, Bruna S. Zanotto, Suki Shergill, Patricia K. Ziegelmann, Selective Internal Radiation Therapy Using Y-90 Resin Microspheres for Metastatic Colorectal Cancer: An Updated Systematic Review and Network Meta-Analysis, Advances in Therapy, 10.1007/s12325-024-02800-5, 41, 4, (1606-1620), (2024).
- George Gourzoulidis, Oresteia Zisimopoulou, Andrianos Liavas, Charalampos Tzanetakos, Lorlatinib as a first-line treatment of adult patients with anaplastic lymphoma kinase-positive advanced non-small cell lung cancer: Α cost-effectiveness analysis in Greece, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2023.2288249, 24, 3, (375-385), (2023).
- Charalampos Tzanetakos, George Gourzoulidis, Does a Standard Cost-Effectiveness Threshold Exist? The Case of Greece, Value in Health Regional Issues, 10.1016/j.vhri.2023.02.006, 36, (18-26), (2023).
- George Gourzoulidis, Maria Koulentaki, Antonis Kattamis, Maria Bouzani, Chara Giatra, Vassiliki Chotzagiannoglou, Alexandra Beletsi, Georgia Kourlaba, Cost-Utility Analysis of Pegaspargase for the Treatment of Acute Lymphoblastic Leukemia in Greece, Clinical Drug Investigation, 10.1007/s40261-022-01207-w, 42, 11, (999-1008), (2022).
- Svetlana Babajanyan, Megan Pollack, Sarah Castelo, Abhishek Kavati, Tanios S Bekaii-Saab, Sequenced treatment after regorafenib and survival in metastatic colorectal cancer: a qualitative clinical review, Colorectal Cancer, 10.2217/crc-2022-0006, 10, 1, (2022).
- George Gourzoulidis, Oresteia Zisimopoulou, Nadia Boubouchairopoulou, Christina Michailidi, Chrissy Lowry, Charalampos Tzanetakos, Georgia Kourlaba, Cost-effectiveness Analysis of Lorlatinib in Patients Previously Treated with Anaplastic Lymphoma Kinase Inhibitors for Non-small Cell Lung Cancer in Greece, Journal of Health Economics and Outcomes Research, 10.36469/jheor.2022.32983, 9, 1, (50-57), (2022).
- George Gourzoulidis, Maria Koulentaki, Anna Koumarianou, Epaminondas Samadas, Nikolaos Androulakis, Spyridon Xynogalos, Pavlos Papakotoulas, Ioannis Boukovinas, Michalis Karamouzis, John Souglakos, Vasiliki Chotzagiannoglou, Alexandra Beletsi, Georgia Kourlaba, Cost-effectiveness of trifluridine/tipiracil as a third-line treatment of metastatic gastric cancer, including adenocarcinoma of the gastrohesophageal junction, among patients previously treated in Greece, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2021.1921576, 22, 2, (259-269), (2021).