Impact of initiating long-acting injectable antipsychotics on hospitalization in patients with bipolar I disorder
Abstract
Aim: To compare risk of hospitalization in patients with bipolar I disorder (BD-I) initiating long-acting injectable antipsychotics (LAIs). Materials & methods: Using Truven Health Analytics MarketScan® (Medicaid, Commercial and Medicare Supplemental) databases (2012–2016), patients (≥18 years) with BD-I with a LAI (aripiprazole once monthly [AOM 400], fluphenazine-LAI, haloperidol-LAI, risperidone-LAI and paliperidone-4-week-LAI) were identified. Results: The adjusted odds of having hospitalization were significantly higher in haloperidol-LAI (Odds ratio [95% CI]: 1.39 [1.03–1.87] all-cause; p = 0.029; 1.41 [1.03–1.93] psychiatric-specific; p = 0.032) and risperidone-LAI (1.54 [1.12–2.13]; p = 0.009; 1.68 [1.20–2.37]; p = 0.003) users versus AOM 400 users. Risks of hospitalization did not differ comparing fluphenazine-LAI and paliperidone-LAI users with AOM 400 users. Conclusion: AOM 400 may be more beneficial at reducing hospitalization rates in BD-I versus haloperidol-LAI and risperidone-LAI.
Bipolar disorder (BD) is a serious, chronic psychiatric disorder that places substantial economic burden on the US healthcare system. In 2015, patients with BD incurred US$200 billion in combined direct and indirect healthcare costs [1]. Hospitalization is one of the major drivers of healthcare costs, contributing to over a quarter of the total direct costs of treating patients with BD [1,2]. More than 75% of the BD population reports at least one psychiatric hospitalization in their lifetime [3]. Hospitalization has served as a proxy for relapse [4]. Preventing relapse is critical in successfully managing BD.
Atypical antipsychotics are increasingly used to treat patients with BD, either as monotherapy or as adjunctive therapy to mood stabilizers [2,5,6]. With administration schedules ranging from biweekly to every 3 months, long-acting injectable (LAI) formulations of antipsychotics offer several advantages over oral antipsychotics, such as not having to remember to take drugs daily, reducing the risk of unintentional or deliberate overdose and decreasing the number of required visits with a healthcare professional [7,8]. Patients with BD treated with LAIs are reported to have better medication adherence, a longer median time to medication discontinuation, less likely to discontinue their medication [6,9] and have reduced hospitalizations compared with those treated with oral antipsychotics [10].
There have been some head-to-head studies directly comparing one LAI versus another, but most focused on older LAIs, such as risperidone-LAI versus haloperidol-LAI [5], or paliperidone versus other older LAIs, and included patients with schizophrenia from clinical trials [11–13]. In the only observational study, we previously conducted comparing the effectiveness of aripiprazole once monthly (AOM 400) with other LAIs, it was found that AOM 400, one of the most recently approved LAI for maintenance monotherapy in adult patients with bipolar I disorder (BD-I), may be more effective than haloperidol- and risperidone-LAIs in reducing all-cause hospitalization [14]. However, in that study, we only included a small number of AOM 400 patients and did not have data on psychiatric hospitalization [14]. In the current study, we replicated the previous study design [14] and evaluated time to and risk of both all-cause and psychiatric hospitalization in a larger sample of patients with BD-I who were treated with different LAIs in the real-world setting.
Methods
Data source & study design
To identify patients with BD-I, administrative claims data from Truven Health Analytics MarketScan® Medicaid, Commercial and Medicare Supplemental databases were used. The MarketScan Medicaid claims database includes demographic and clinical information, inpatient and outpatient utilization data, and outpatient prescription data for 40 million Medicaid enrollees from multiple geographically dispersed states. The MarketScan Commercial database includes medical and pharmacy claims for nearly 62.9 million individuals and their dependents who are covered through employer-sponsored private health insurance plans. The MarketScan Medicare Supplemental database contains records on around 5.3 million retired employees and spouses older than 65 years who are enrolled in Medicare with supplemental Medigap insurance paid by their former employers.
The data used for the analyses covered from 1 January 2012 to 30 June 2016. All data were compliant with the Health Insurance Portability and Accountability Act (HIPAA) of 1996. As this study utilized deidentified administrative claims, neither informed content nor institutional review board approval were required.
Sample selection
Among patients having at least one inpatient or at least two outpatient claims for BD-I (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM]: 296.0x, 296.1x, 296.4x, 296.5x, 296.6x, 296.7x, 296.8x, except 296.82; ICD-10-CM code: F30.x, F31.x, except F31.81) at any time during the study period, five mutually exclusive LAI cohorts were established. These cohorts comprised patients with BD-I who initiated one of the following LAIs during the identification (ID) period (1 January 2013–30 June 2015): AOM 400, fluphenazine-LAI, haloperidol-LAI, paliperidone-LAI and risperidone-LAI. Among these, risperidone-LAI was the only LAI that carried an FDA-approved indication for the maintenance-treatment of BD-I in the USA during the study period. In addition, three currently marketed LAIs (olanzapine-LAI, aripiprazole lauroxil [Aristada®] and paliperidone palmitate 12 weeks [Invega Trinza®]) were not included in the study, due to having a small patient sample size. The index date was defined as the earliest occurrence (first date) of a claim for one of the LAI therapies of interest during the ID period. The LAI observed on the index date was defined as the index therapy. Use of nonindex LAI was allowed in the 1-year prior to the index date (baseline period), but patients were excluded if they had claims for index LAI therapies during the baseline period. To ensure patients had pre-existing mental illness, the first diagnosis of BD-I had to be before or on the index date. Patients were allowed to have other concomitant mental health diagnoses (e.g., schizophrenia, anxiety disorder or depression).
Patients were also required to be ≥18 years of age on the index date and have continuous health plan enrollment for the 12-month baseline period and at least 12 months after index date. Patients were followed for at least 1 year and until the end of enrollment or study end, whichever occurred first. Each patient was followed for a different period of time, with a minimum study period of 2 year (1 year before and 1 year after the index date) and a maximum of 4.5 years (1 year before and 3.5 years after the index date).
Patients were further excluded if they had a prescription claim for clozapine during the study period as clozapine is indicated for the treatment of severely ill patients with BD. In the Medicaid database, Medicare and Medicaid dual-eligible patients were also excluded, as these were patients who did not have pharmacy coverage, mental health coverage information or had capitated plans, as data for these patients may have been incomplete.
Study measures
Baseline measures
Baseline variables potentially related to illness severity were examined using data in the 1-year preindex period. These included: age, gender, insurance type (Commercial, Medicare Supplemental and Medicaid), Charlson comorbidity index [15,16], number of chronic conditions (Healthcare Cost and Utilization Project [HCUP]), somatic comorbidities (obesity, Type 2 diabetes mellitus), somatic medication use (antidiabetic, lipid-lowering and antihypertensive medications), psychiatric medication use (nonindex antipsychotics, antidepressants, antianxiety medications, sedatives or hypnotics and mood stabilizers) and any baseline hospitalization. The presence of claims for other psychiatric conditions was also evaluated (≥1 claim for schizophrenia, major depressive disorder, anxiety, personality disorder and substance abuse disorder).
Outcome measures
The outcome measures included in this study were rates of and time to first all-cause and psychiatric (with a primary diagnosis of any mental disorder [ICD-9-CM: 290.xx-311.xx; ICD-10-CM code: F01.xx-F99.xx]) hospitalization. Hospitalization rates were reported during the 1-year post-index period. The time to hospitalization was reported during the entire follow-up period.
Statistical analysis
Descriptive, unadjusted analyses were first performed to assess differences among the selected LAI cohorts across baseline covariates. Specifically, χ2 tests were used for categorical variables and a t-test or Wilcoxon rank-sum test was used for continuous variables, depending on the variable distributions. A logistic regression model was then used to estimate adjusted hospitalization rates (all-cause and psychiatric) across different LAIs during the 1-year post-index period, controlling for baseline covariates, including age groups, gender, insurance type, Charlson comorbidity index (modified), number of chronic conditions (HCUP), baseline psychiatric comorbidities (including schizophrenia, major depressive disorder, anxiety, personality disorder, substance abuse disorder), baseline obesity, baseline Type 2 diabetes mellitus, baseline hospitalization, and baseline psychiatric and somatic medication use. Kaplan–Meier curves and a Cox regression model were conducted to estimate time to and risks of hospitalization during the entire follow-up, adjusting for the baseline covariates mentioned above. All data transformations and statistical analysis were performed using SAS© version 9.4.
Results
Sample description
Of the 521,450 patients with BD-I identified from the MarketScan databases, 229,595 received at least one LAI in the ID period. Of these, 6700 started a new LAI in the ID period. After excluding those who did not have mono therapy, had use of clozapine and did not have at least one BD-I diagnosis prior to the index date, 4955 patients remained. A total of 2509 patients were further excluded for not meeting age and continuous health plan enrollment criteria; 54 for use of treatment with small sample size. A schematic diagram of patient disposition is shown in Figure 1. The final sample size consisted of 2392 patients with BD-I (Figure 1): 413 (17.3%) initiated AOM 400, 154 (6.4%) fluphenazine-LAI, 476 (19.9%) haloperidol-LAI, 1026 (42.9%) paliperidone-LAI and 323 (13.5%) risperidone-LAI.
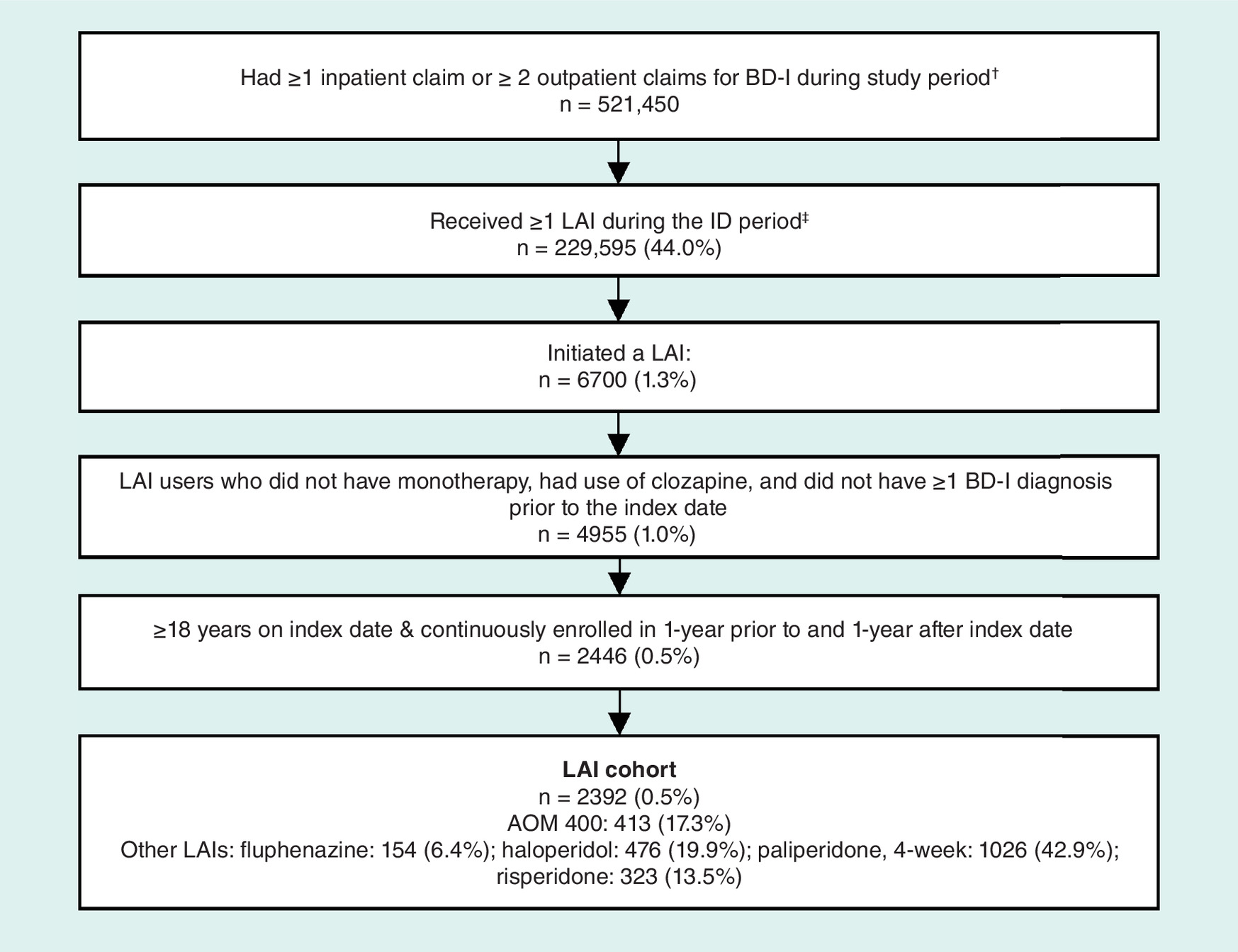
Figure 1. Patient identification.
†Study period is defined as 1 January 2012–30 June 2016.
‡Identification period is defined as 1 January 2013–30 June 2015.
AOM: Aripiprazole once monthly; BD-I: Bipolar I disorder; ID: Identification; LAI: Long-acting injectable antipsychotics.
Baseline characteristics
Table 1 shows patient characteristics at baseline. The mean (SD) age of the overall sample was 37.8 (14.5) years, 49.6% of patients were female and 76.6% were insured through Medicaid (Table 1).
| Baseline characteristics | AOM 400 n = 413; 17.3% | Fluphenazine n = 154; 6.4% | Haloperidol n = 476; 19.9% | Paliperidone n = 1026; 42.9% | Risperidone n = 323; 13.5% | All n = 2392 | p-value |
|---|---|---|---|---|---|---|---|
| Age in years, mean (SD) | 34.0 (12.9) | 44.4 (15.9) | 39.3 (14.6) | 37.0 (13.8) | 39.7 (16.1) | 37.8 (14.5) | <0.001 |
| Female, n (%) | 217 (52.5) | 82 (53.2) | 239 (50.2) | 479 (46.7) | 169 (52.3) | 1186 (49.6) | <0.149 |
| Insurance type, n (%): | <0.001 | ||||||
| –Medicaid | 301 (72.9) | 102 (66.2) | 382 (80.3) | 830 (80.9) | 217 (67.2) | 1832 (76.6) | |
| –Commercial | 107 (25.9) | 37 (24.0) | 71 (14.9) | 171 (16.7) | 87 (26.9) | 473 (19.8) | |
| –Medicare supplemental | 5 (1.2) | 15 (9.7) | 23 (4.8) | 25 (2.4) | 19 (5.9) | 87 (3.6) | |
| Charlson comorbidity index, mean (SD) | 1.1 (1.7) | 1.7 (2.1) | 1.4 (1.9) | 1.1 (1.7) | 1.3 (2.0) | 1.2 (1.8) | <0.001 |
| Number of chronic conditions | 4.0 (2.3) | 4.3 (2.2) | 4.3 (2.2) | 4.1 (2.3) | 4.0 (2.4) | 4.1 (2.3) | 0.237 |
| Any hospitalization, n (%) | 218 (52.8) | 99 (64.3) | 341 (71.6) | 676 (65.9) | 197 (61.0) | 1531 (64.0) | <0.001 |
| Use of any atypical and typical antipsychotics, n (%) | 369 (89.3) | 133 (86.4) | 432 (90.8) | 895 (87.2) | 290 (89.8) | 2119 (88.6) | 0.238 |
| Psychiatric medications, n (%) | 360 (87.2) | 127 (82.5) | 389 (81.7) | 850 (82.8) | 265 (82.0) | 1991 (83.2) | 0.210 |
| Somatic medications, n (%) | 200 (48.4) | 93 (60.4) | 240 (50.4) | 475 (46.3) | 160 (49.5) | 1168 (48.8) | 0.022 |
| Psychiatric comorbidities†, n (%) | 332 (80.4) | 121 (78.6) | 424 (89.1) | 886 (86.4) | 269 (83.3) | 2032 (84.9) | <0.001 |
| Somatic comorbidities‡, n (%) | 235 (56.9) | 106 (68.8) | 311 (65.3) | 583 (56.8) | 186 (57.6) | 1421 (59.4) | 0.002 |
†Major depressive disorder, anxiety, personality disorder, substance abuse disorders, schizophrenia.
‡Obesity, Type 2 diabetes mellitus.
AOM 400: Aripiprazole once monthly; SD: Standard deviation.
Baseline characteristics (age, insurance, comorbid illness and hospitalization rates) differed across LAIs. Compared with other LAI users with BD-I, AOM 400 users were statistically significantly younger and had lower hospitalization rates at baseline (p < 0.001 for all comparisons).
Unadjusted hospitalization rates & time to hospitalization
During the 1-year post-index follow-up period, the unadjusted all-cause and psychiatric hospitalization rates were highest among the other LAI users when compared with AOM 400 users: fluphenazine-LAI: 42.9% (all-cause), 35.1% (psychiatric); haloperidol-LAI: 47.5%, 38.4%; paliperidone-LAI: 38.6%, 32.1%; risperidone-LAI: 44.6%, 36.8%; AOM 400: 34.6%, 25.9% (p < 0.001 for all comparisons).
Considering the entire follow-up period, days to first all-cause and psychiatric hospitalization was significantly shorter for other LAI users than for AOM 400 (p < 0.05). It took 112 (all-cause) and 154 (psychiatric) days for 25% of fluphenazine-LAI, 89 and 133 days for haloperidol-LAI, 149 and 212 days for paliperidone-LAI, and 127 and 189 days for risperidone-LAI users to be hospitalized compared with 227 and 346 days for 25% of AOM 400 users (Figure 2A & 2B).
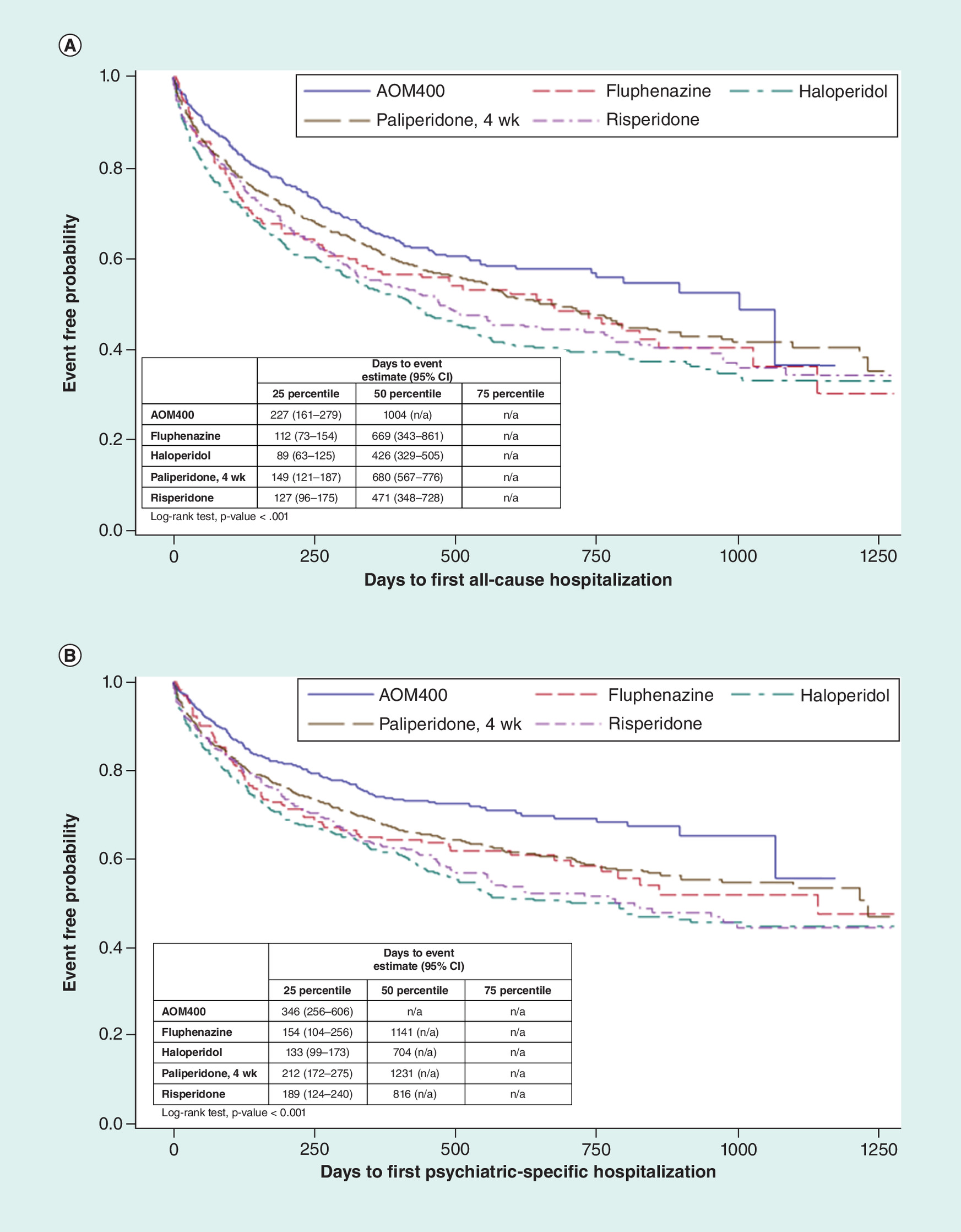
Figure 2. (A) Time to first all-cause hospitalization over the maximum of 3.5 years of follow-up. (B) Time to first psychiatric hospitalization over the maximum of 3.5 years of follow-up.
Based on Kaplan–Meier analysis; individual follow-up was a minimum of 1 year and a maximum of 3.5 years.
Adjusted hospitalization rates & risk of hospitalization
Adjusting for differences in baseline characteristics, the odds of both all-cause and psychiatric hospitalization during the 1-year post-index period were significantly higher in the haloperidol-LAI (Odds ratio [95% CI]: 1.39 [1.03–1.87] all-cause; p = 0.029; 1.41 [1.03–1.93] psychiatric-specific; p = 0.032) and risperidone-LAI (1.54 [1.12–2.13]); p = 0.009; 1.68 [1.20–2.37]; p = 0.003) cohorts compared with AOM 400 users (Figure 3). No statistically significant differences were observed in risk of hospitalizations comparing fluphenazine-LAI and paliperidone-LAI users with AOM 400 users (p > 0.05). Across LAIs, the lowest adjusted all-cause hospitalization rates were found in paliperidone-LAI (35.9%) and AOM 400 users (36.0%; p = 0.004). The lowest adjusted psychiatric hospitalization rate was in the AOM 400 cohort (25.7%; p = 0.013) followed by paliperidone-LAI (28.1%), haloperidol-LAI (32.8%), fluphenazine-LAI (33.1%) and risperidone-LAI (36.8%; Figure 4).
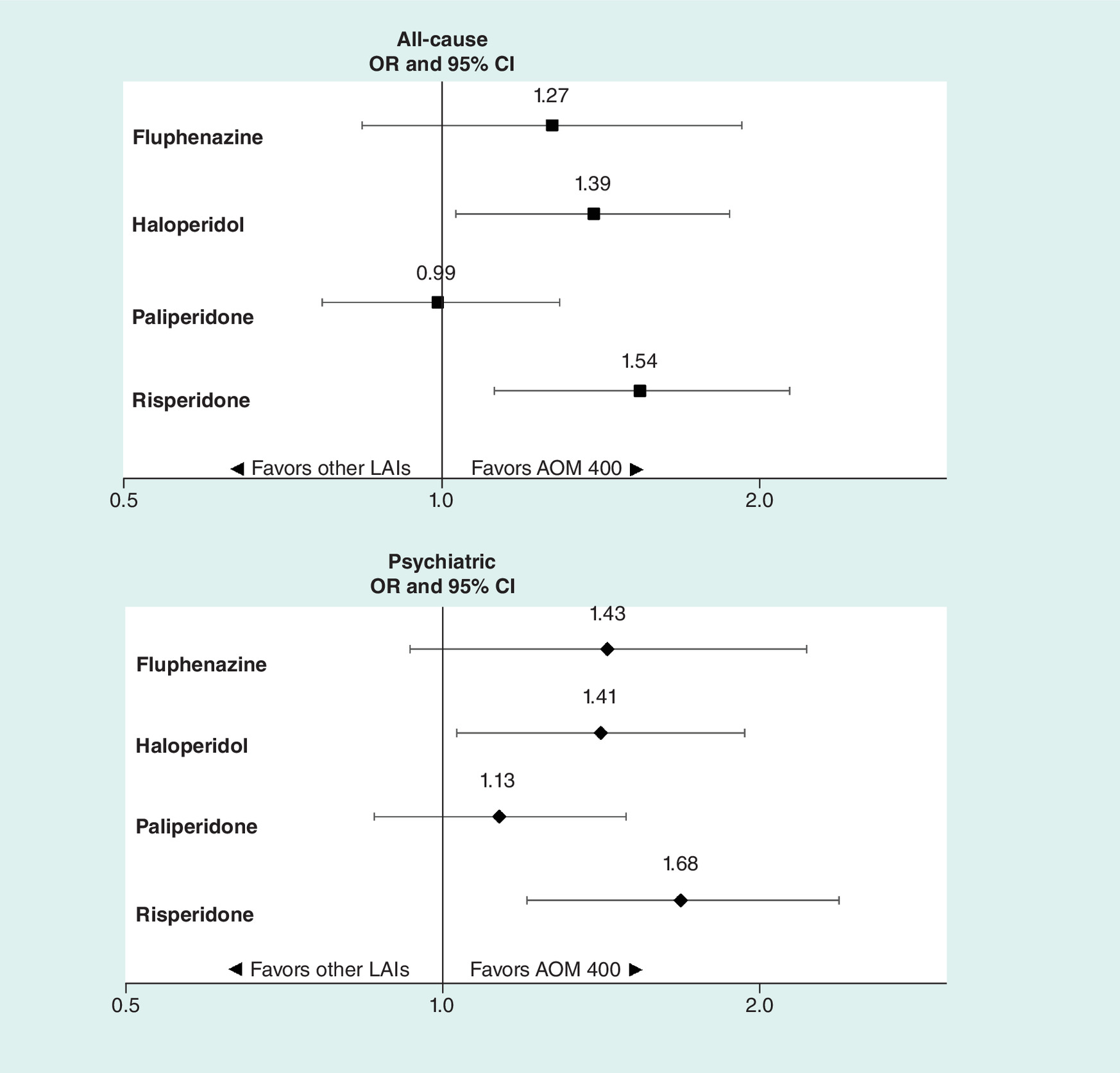
Figure 3. Risk of hospitalization during the 1-year follow-up.
Based on logistic regression analyses; all analyses adjusted by age group, gender, insurance type and the following baseline measures: Charlson comorbidity (modified), number of HCUP chronic conditions, psychiatric comorbidities (including schizophrenia, major depressive disorder, anxiety, personality disorder and substance abuse disorder), obesity, Type 2 diabetes mellitus, hospitalization, psychiatric medication use, somatic medication use, and nonindex antipsychotic.
AOM: Aripiprazole once monthly; CI: Confidence interval; LAI: Long-acting injectable antipsychotics; OR: Odds ratio.
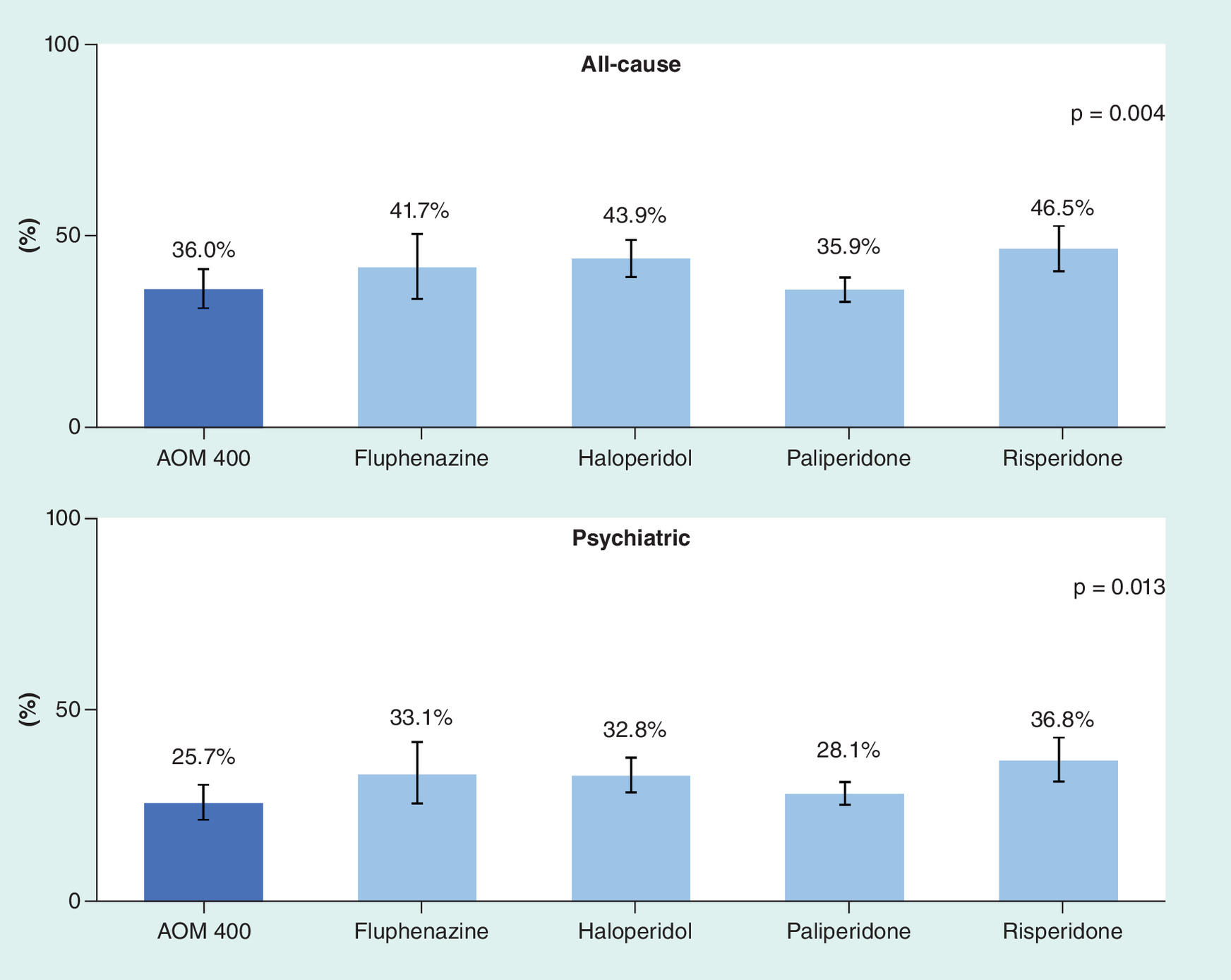
Figure 4. Adjusted rate of hospitalization during the 1-year follow-up.
Adjusted by age group, gender, insurance type and the following baseline measures: Charlson comorbidity (modified), number of HCUP chronic conditions, psychiatric comorbidities (including schizophrenia, major depressive disorder, anxiety, personality disorder and substance abuse disorder), obesity, Type 2 diabetes mellitus, hospitalization, psychiatric medication use, somatic medication use and nonindex antipsychotic.
AOM: Aripiprazole once monthly.
The risks of both all-cause and psychiatric hospitalization (over the entire follow-up period) were significantly higher in haloperidol-LAI (Hazard ratio [95% CI]: 1.40 [1.15–1.70] all-cause; p < 0.001; 1.54 [1.23–1.93] psychiatric; p < 0.001) and risperidone-LAI (1.37 [1.11–1.70] all-cause; p = 0.003; 1.68 [1.32–2.14] psychiatric; p < 0.001; Figure 5).
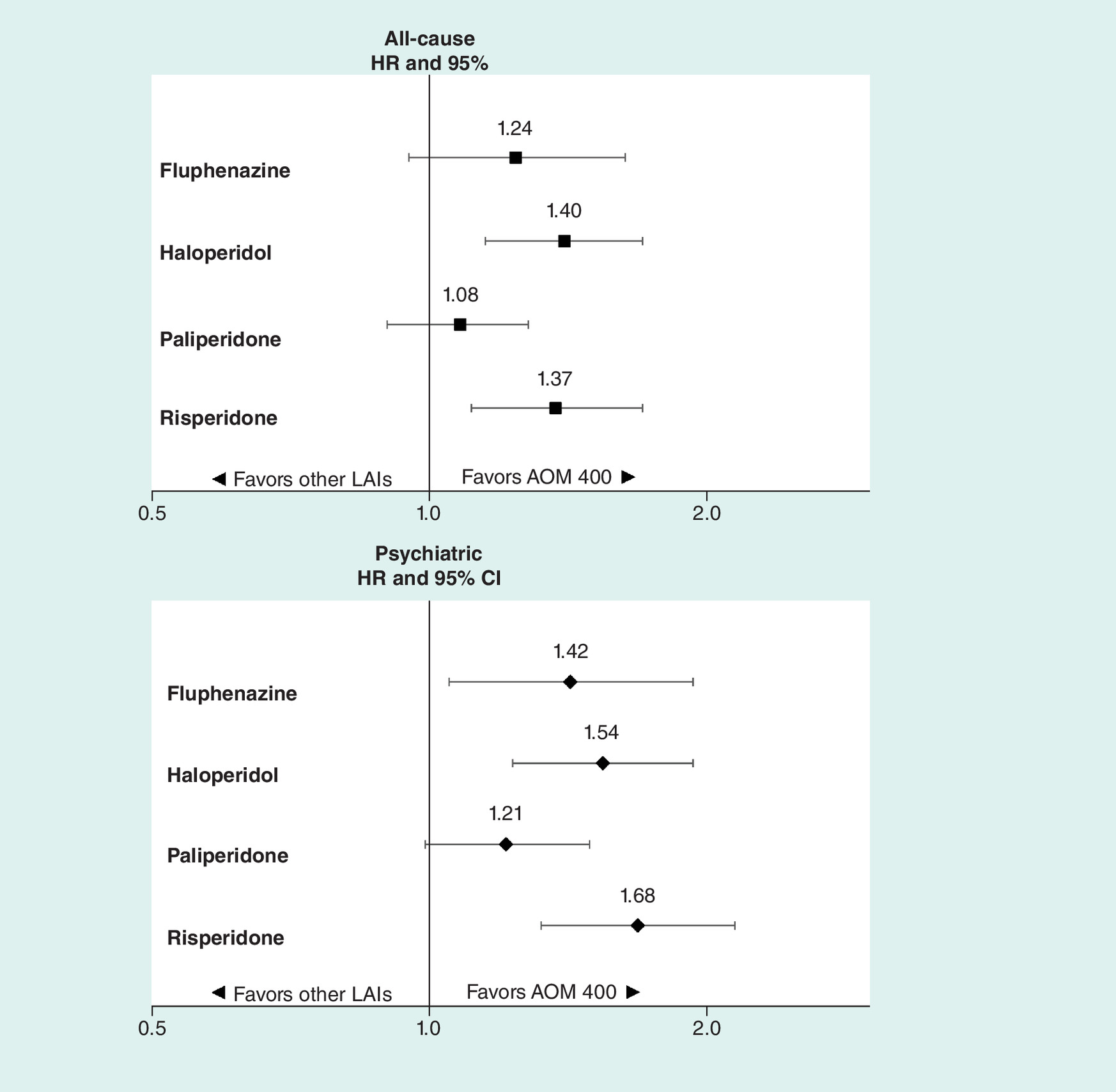
Figure 5. Risk of hospitalization over the maximum of 3.5 years of follow-up.
Based on Cox regression analyses; all analyses adjusted by age group, gender, insurance type and the following baseline measures: Charlson comorbidity (modified), number of HCUP chronic conditions, psychiatric comorbidities (including schizophrenia, major depressive disorder, anxiety, personality disorder and substance abuse disorder), obesity, Type 2 diabetes mellitus, hospitalization, psychiatric medication use, somatic medication use and nonindex antipsychotic. Individual follow-up was a minimum of 1 year and a maximum of 3.5 years.
AOM: Aripiprazole once monthly; CI: Confidence interval; HR: Hazard ratio; LAI: Long-acting injectable antipsychotics.
Discussion
This was a large retrospective study that examined risk of all-cause and psychiatric hospitalization among patients with BD-I who initiated different LAI treatments. We found AOM 400 was associated with lower rates of hospitalization than haloperidol- and risperidone-LAIs. Rates were approximately 37–68% lower for both all-cause and psychiatric hospitalizations, and the findings were consistent between 1 year after treatment initiation and over a mean of approximately 2 years of follow-up. The study included a wide variety of patient types and included commercially insured Medicare and Medicaid patients.
Hospitalization is one of the most expensive health outcomes in BD, and in research serves as a proxy for relapse [4]. If these findings are confirmed in prospective studies, it suggests patients treated with AOM 400 are dramatically less prone to relapse than initiators of haloperidol- and risperidone-LAIs. The observed reduction in hospitalization is of the same magnitude as is observed in studies comparing active treatment with mood stabilizer to placebo [17,18].
Given the potential benefit, it appears LAIs are underused [19,20]. LAIs are currently not considered the first-line treatment option for patients with BD-I [21]. LAIs are infrequently used for a first episode of psychosis [8], perhaps because physicians overestimate oral medication adherence or inaccurately assume patients prefer not to use LAIs. Other barriers to the usage of LAIs also exist, such as prior authorization policies [21], lack of treatment guidelines that include LAIs [10], and patients’ attitudes and healthcare providers’ (often mistaken) belief that patients fear injections [22]. Clinicians tend not to share the decision-making with their patients in discussions about the choice of treatment [22].
Most prior literature considered LAIs compared with orals in general and found the risk of all-cause and psychiatric rehospitalizations is approximately 30% lower in patients treated with LAIs compared with treatment with their oral counterparts [10]. However, data comparing the impact of selecting one LAI instead of another in BD is sparse. In one retrospective study, Patel and colleagues found paliperidone palmitate was not more effective than other cheaper LAI antipsychotics [23]. A study comparing paliperidone palmitate with AOM 400 found patients treated with AOM 400 had better health-related quality of life and were less likely to discontinue treatment than those treated with paliperidone palmitate [13]. The impact of AOM 400 versus other LAIs on time to and rates of hospitalization were not addressed in these studies.
This study has limitations. First, BD diagnosis was identified from health insurance claims, which are designed for reimbursement purposes and can contain errors. Additionally, this analysis only captured claims that were contained in the study databases. Information such as how long a patient has had BD-I, severity of BD and activities during hospitalization (e.g. transferring from a psychiatric ward to a nonpsychiatric ward) were not captured in our study. However, the large sample size and the inclusion of reliable measures of cost and utilization make health insurance claims data a valuable source of information. Second, the MarketScan Commercial database did not present information on race, which restricted us from including this potentially significant confounder in multivariate analysis. Third, compared with other LAI users with BD-I, AOM 400 users were statistically significantly younger and had lower hospitalization rates at baseline. Even though we adjusted for baseline differences, it is still possible that AOM 400 users were in early phases of their illness and thus better responders to treatments. This may be responsible for some advantages observed in the AOM 400. Fourth, the goal of the study was to examine time and rates of all-cause and psychiatric hospitalization associated with initiation of various LAIs, with an intent to treat basis. This study design, however, did not adjust for dosing or tolerability of, length of or adherence to, the treatment initiated. Additional research would need to be conducted to better understand the impact of these factors on outcome differences observed across the different LAI cohorts.
Conclusion
In this large real-world study, AOM 400 was associated with a greater reduction in both all-cause and psychiatric hospitalizations for patients with BD-I than haloperidol-LAI and risperidone-LAI. Continued development of LAIs and education on their use for both patients and clinicians, as well as integration into treatment guidelines, may help to reduce hospitalizations of patients with BD.
Bipolar disorder (BD) places a substantial burden on the US healthcare system with US$200 billion in direct and indirect healthcare costs associated with BD reported in 2015.
Hospitalization, a proxy for relapse, is one of the major drivers of BD healthcare costs.
Long-acting injectable antipsychotics (LAIs) have been associated with better medication adherence and reduced hospitalizations in patients with BD as compared with oral antipsychotic therapy.
Most studies that directly compare LAIs focus on older LAIs or included patients with schizophrenia.
This study expands on an earlier study conducted by the authors, which found that aripiprazole once monthly (AOM 400) may be more effective than haloperidol- and risperidone-LAI at reducing all-cause hospitalization in patients with bipolar I disorder (BD-I), by using a large sample size and evaluating time to and risk of both all-cause and psychiatric hospitalization.
Using 2012–2016 data from the Truven Health Analytics MarketScan® (Medicaid, Commercial and Medicare Supplemental) databases, 2392 patients with BD-I initiating an LAI of interest were included in the final sample: 413 (17.3%) initiated AOM 400, 154 (6.4%) fluphenazine-LAI, 476 (19.9%) haloperidol-LAI, 1,026 (42.9%) paliperidone-LAI and 323 (13.5%) risperidone-LAI.
In multivariate analyses adjusting for baseline differences, AOM 400 was associated with a greater reduction in both all-cause and psychiatric hospitalizations for patients with BD-I than haloperidol-LAI and risperidone-LAI.
The lowest adjusted psychiatric hospitalization rate was in the AOM 400 cohort.
Continued development and integration of LAIs as an effective treatment option may help to reduce hospitalizations of patients with BD-I.
Authors’ contributions
All authors were equally involved in the design of the study. E Chang conducted the statistical analyses and all authors contributed equally in the interpretation of results and writing of the manuscript.
Financial & competing interests disclosure
Funding for the study was received from Otsuka Pharmaceutical Development and Commercialization, Inc. and Lundbeck. MS Broder, E Chang and T Yan are employees of PHAR, LLC, which was paid by Otsuka and Lundbeck to perform the research described in this manuscript. M Greene is an employee of Ostuka Pharmaceutical Development & Commercialization, Inc. M Touya is an employee of Lundbeck. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest
1.
Cloutier M, Greene M, Guerin A, Touya M, Wu E. The economic burden of bipolar I disorder in the USA in 2015. J. Affect. Disord. 226, 45–51 (2017).
• Study reported the most recent healthcare costs in the USA associated with bipolar disorder, highlighting the burden associated with the disease.
2.
Bergeson JG, Kalsekar I, Jing Y, You M, Forbes RA, Hebden T. Medical care costs and hospitalization in patients with bipolar disorder treated with atypical antipsychotics. Am. Health Drug Benefits 5(6), 379–386 (2012).
3.
Kim E, You M, Pikalov A, Van-Tran Q, Jing Y. One-year risk of psychiatric hospitalization and associated treatment costs in bipolar disorder treated with atypical antipsychotics: a retrospective claims database analysis. BMC Psych. 11, 6 (2011).
• Study compared psychiatric hospitalization and associated costs in commercially insured patients with bipolar disorder being treated with various antipsychotics.
4.
Olivares JM, Sermon J, Hemels M, Schreiner A. Definitions and drivers of relapse in patients with schizophrenia: a systematic literature review. Ann. Gen. Psych. 12(1), 32 (2013).
• Review provided rationale for using hospitalization as a proxy for relapse.
5.
Wu C-S, Hsieh MH, Tang C-H, Chang C-J. Comparative effectiveness of long-acting injectable risperidone versus long-acting injectable first-generation antipsychotics in bipolar disorder. J. Affect. Disord. 197, 189–195 (2016).
6.
Greene M, Yan T, Chang E, Hartry A, Touya M, Broder MS. Medication adherence and discontinuation of long-acting injectable versus oral antipsychotics in patients with schizophrenia or bipolar disorder. J. Med. Econ. 21(2), 127–134 (2018).
• Real-world study reported that patients with schizophrenia or bipolar disorder, who initiated therapy with long-acting injectable antipsychotics, had better medication adherence and lower risk of discontinuation than those who changed to a different oral antipsychotic.
7.
Sacchetti E, Grunze H, Leucht S, Vita A. Long-acting injection antipsychotic medications in the management of schizophrenia. Evid. Based Psychiatr. Care 1, 27–36 (2015).
8.
Meyer JM. Converting oral to long-acting injectable antipsychotics: a guide for the perplexed. CNS Spectr. 22(S1), 14–28 (2017).
9.
Pilon D, Tandon N, Lafeuille M-H et al. Treatment patterns, health care resource utilization, and spending in medicaid beneficiaries initiating second-generation long-acting injectable agents versus oral atypical antipsychotics. Clin. Ther. 39(10), 1972.e2–1985.e2 (2017).
•Study focused on a Medicaid population of patients with schizophrenia and indicated better adherence and persistence associated with second-generation long-acting injectable therapies versus oral atypical antipsychotics.
10.
Lähteenvuo M, Tanskanen A, Taipale H et al. Real-world effectiveness of pharmacologic treatments for the prevention of rehospitalization in a Finnish nationwide cohort of patients with bipolar disorder. JAMA Psych. 75(4), 347 (2018).
• Comparing long-acting injectable antipsychotics with the oral counterpart, this Finnish study found that long-acting injectable antipsychotics were the most effective antipsychotics in patients with bipolar disorder.
11.
Pandina G, Lane R, Gopal S et al. A double-blind study of paliperidone palmitate and risperidone long-acting injectable in adults with schizophrenia. Prog. Neuropsychopharmacol. Biol. Psych. 35(1), 218–226 (2011).
12.
Li H, Rui Q, Ning X, Xu H, Gu N. A comparative study of paliperidone palmitate and risperidone long-acting injectable therapy in schizophrenia. Prog. Neuropsychopharmacol. Biol. Psych. 35(4), 1002–1008 (2011).
13.
Naber D, Hansen K, Forray C et al. Qualify: a randomized head-to-head study of aripiprazole once-monthly and paliperidone palmitate in the treatment of schizophrenia. Schizophr. Res. 168(1–2), 498–504 (2015).
14.
Yan T, Greene M, Chang E, Hartry A, Touya M, Broder MS. All-cause hospitalization and associated costs in patients with schizophrenia or bipolar disorder initiating long-acting injectable antipsychotics. Curr. Med. Res. Opin. 34(1), 41–47 (2018).
• In this head-to-head comparison that included recently approved long-acting injectables, aripiprazole once monthly was more effective than haloperidol- and risperidone-long-acting injectable antipsychotics in reducing all-cause hospitalization.
15.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40(5), 373–383 (1987).
16.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45(6), 613–619 (1992).
17.
Geddes JR, Burgess S, Hawton K, Jamison K, Goodwin GM. Long-term lithium therapy for bipolar disorder: systematic review and meta-analysis of randomized controlled trials. Am. J. Psychiatry. 161(2), 217–222 (2004).
18.
Solomon DA, Keitner GI, Miller IW, Shea MT, Keller MB. Course of illness and maintenance treatments for patients with bipolar disorder. J. Clin. Psych. 56(1), 5–13 (1995).
19.
Kane JM, Kim E, Kan HJ et al. Comparative utility of aripiprazole and haloperidol in schizophrenia: post hoc analysis of two 52-week, randomized, controlled trials. Appl. Health Econ. Health Pol. 7(2), 109–119 (2009).
20.
Koola MM, Wehring HJ, Kelly DL. The Potential role of long-acting injectable antipsychotics in people with schizophrenia and comorbid substance use. J. Dual Diagn. 8(1), 50–61 (2012).
21.
Jackson JW, Fulchino L, Rogers J et al. ‘Impact of drug-reimbursement policies on prescribing: a case-study of a newly marketed long-acting injectable antipsychotic among relapsed schizophrenia patients’. Pharmacoepidemiol. Drug Saf. 27(1), 95–104 (2018).
22.
Cahling L, Berntsson A, Bröms G, Öhrmalm L. Perceptions and knowledge of antipsychotics among mental health professionals and patients. BJPsych Bull. 41(05), 254–259 (2017).
• Article highlighted potential reasons for underutilization of long-acting injectable antipsychotics.
23.
Patel R, Chesney E, Taylor M, Taylor D, McGuire P. Is paliperidone palmitate more effective than other long-acting injectable antipsychotics? Psychol. Med. 48(10), 1616–1623 (2018).
Information & Authors
Information
Published In
Copyright
© 2018 Otsuka Pharmaceuticals.
History
Received: 11 July 2018
Accepted: 2 August 2018
Published online: 21 August 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact of initiating long-acting injectable antipsychotics on hospitalization in patients with bipolar I disorder. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0068
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Juan Antonio García‐Carmona, Joshua Barnett, María Pilar Campos‐Navarro, Katie Mason, Jorge Simal‐Aguado, Sofia Pappa, A Multicentre, 4‐Year Mirror‐Image Study Comparing the Effectiveness of Long‐Acting Injectable Antipsychotics in the Treatment of Bipolar Disorder: Results From the LAICO Study , Bipolar Disorders, 10.1111/bdi.70080, 28, 1, (2026).
- Chun Lin, Yueh-Pin Lin, Seon-Cheol Park, Ok-Jin Jang, Tian-Mei Si, Yu-Tao Xiang, Huang-Li Lin, Afzal Javed, M.Nasar Sayeed Khan, Sandeep Grover, Roy Abraham Kallivayali, Kok Yoon Chee, Takahiro A. Kato, Pornjira Pariwatcharakul, Margarita Maramis, Lakmi Seneviratne, Kang Sim, Wai Kwong Tang, Tin Oo, Norman Sartorius, Chay-Hoon Tan, undefined Mian-Yoon, Naotaka Shinfuku, Shih-Ku Lin, Long-acting injectable antipsychotic use in patients with bipolar disorder: Findings from the REAP-BD study, Asian Journal of Psychiatry, 10.1016/j.ajp.2024.104338, 103, (104338), (2025).
- Laura Orsolini, Sofia Pacini Biagiotti, Lorenzo Maria Martino, Umberto Volpe, A case report of LAI two injection start in a 16-year-old adolescent with severe manic episode and comorbid cannabinoid use disorder, Asian Journal of Psychiatry, 10.1016/j.ajp.2024.103992, 94, (103992), (2024).
- Christie Teigland, Iman Mohammadi, Barnabie C. Agatep, Dusica Hadzi Boskovic, Martha Sajatovic, Relationship between social determinants of health and hospitalizations and costs among patients with bipolar disorder 1, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2024.30.1.72, 30, 1, (72-85), (2024).
- Joshua Caballero, Jianing Xu, Daniel B. Hall, Xianyan Chen, Henry N. Young, Racial and ethnic differences in patterns of use and discontinuation of long-acting injectable antipsychotics using Medicaid claims data, Mental Health Clinician, 10.9740/mhc.2023.08.183, 13, 4, (183-189), (2023).
- Heidi C. Waters, Maelys Touya, Soon Nan Wee, Michelle Ng, Simran Thadani, Subina Surendran, Miguel Rentería, A. John Rush, Rashmi Patel, Joydeep Sarkar, Heather M. Fitzgerald, Xue Han, Psychiatric healthcare resource utilization following initiation of aripiprazole once-monthly: a retrospective real-world study, Current Medical Research and Opinion, 10.1080/03007995.2022.2148461, 39, 2, (299-306), (2022).
- R. Medinas, R. Caetano, A. Quintão, F. Azevedo, C. Laginhas, P.0407 Follow-up study on long‐acting injectable antipsychotics on bipolar disorder at a portuguese inpatient psychiatric unit (Hospital Egas Moniz), European Neuropsychopharmacology, 10.1016/j.euroneuro.2021.10.380, 53, (S295), (2021).
- Ivana Clark, Phoebe Wallman, Victoria Cornelius, David Taylor, Factors predicting relapse and treatment discontinuation with paliperidone 3-monthly long-acting injection: A 2-year naturalistic follow-up study, European Psychiatry, 10.1192/j.eurpsy.2021.2243, 64, 1, (2021).
- Ching-Hua Lin, Hung-Yu Chan, Chun-Chi Hsu, Feng-Chua Chen, Time to rehospitalization in patients with bipolar mania discharged on long-acting injectable or oral antipsychotics, Journal of Affective Disorders, 10.1016/j.jad.2020.10.023, 279, (292-298), (2021).
- Ali Metehan Caliskan, Saliha Calisir, Sila Caliskan, Mehmet Arslan, Ikbal Inanli, Ibrahim Eren, Impact of initiating long-acting injectable paliperidone palmitate on relapse and hospitalization in patients with bipolar I disorder: A mirror image retrospective study, Asian Journal of Psychiatry, 10.1016/j.ajp.2020.102457, 54, (102457), (2020).