Comparison between minimally invasive plate osteosynthesis and open plating for proximal humeral fractures: a meta-analysis
Abstract
Aim: We conducted this meta-analysis for comparing the efficacy and safety in proximal humeral fractures by treatment minimally invasive plate osteosynthesis and open plating. Methods: The potential academic literature were identified from the Cochrane Library, Springer, PubMed, Embase and ScienceDirect. Pooled data were analyzed by RevMan 5.1. Results: Seven studies marched with the inclusion criteria. Meta-analysis showed the significant differences in terms of blood loss, operative time, length of hospital stays and constant score between two groups. No significant differences were found in time to union, the union rate and complications. Conclusion: Minimally invasive plate osteosynthesis in proximal humeral fractures provided significantly shorter operative times, length of hospital stays, less blood loss and better clinical outcomes without increasing complications.
The proximal humeral fracture (PHF) is a common fracture in the extremities and account for approximately 4–5% of all adult fractures [1]. The morbidity and severity of PHF is increasing year by year due to an increased number of older patients with osteoporotic fractures [2]. Nonsurgical treatment and surgical treatment are used to treat these fractures [3]. Surgical treatment, including external fixation, plating, intramedullary fixation and shoulder arthroplasty, has been reported to be associated with earlier resumption of daily activity and good clinical outcomes [4–6]. Of these, open reduction and internal fixation (ORIF) is the most commonly used technique for the majority of fractures and has been considered to be the gold standard surgical treatment [7,8]. However, ORIF inevitably exposes the fracture region and strip periosteum [9,10] and reveals complications such as postoperative infection, nonunion, nerve injury and hardware removal.
Minimally invasive plate osteosynthesis (MIPO) is popular for its advantages of reserving and avoiding extensive soft tissue dissection [11–13]. Thus, MIPO provides more favorable conditions for fracture healing by preserving local fracture biology. To date, several researches had been reported that compared MIPO with ORIF in the treatment of PHF. The methodological flaws in the published literature include poor study designs, small sample sizes and variable outcomes, although a meta-analyses has been published to discuss comparisons of MIPO with ORIF in the treatment of PHF [14]. However, this literature had a few limitations, such as language bias, lacking updated studies published in recent years and some errors in counting the characteristics of included studies. Therefore, it is necessary to conduct a large sample meta-analysis from randomized controlled trials (RCTs) and non-RCT studies to compare the efficacy and safety of MIPO with ORIF in the treatment with PHF.
Methods
Search strategy
The literature searches were performed in Cochrane Library, Springer, PubMed, Embase and ScienceDirect from 1966 to March 2018. Secondary sources were identified from studies cited in the references of retrieved articles. No studies were excluded based on language. The key search terms applied were ‘humeral fracture’, ‘plate’, ‘open’ and ‘minimally invasive’ in combination with the Boolean operators AND or OR.
Inclusion criteria
The following criteria were considered eligible as including studies: patients with proximal humeral fractures; intervention: treated with MIPO; control: treated with ORIF; outcome measures, one or more of the following outcomes were reported: operative time, blood loss, union time, function score, perioperative outcomes and complications and study design: RCT and non-RCT.
Exclusion criteria
We excluded studies that were: studies without controlled groups; unavailable full-text versions; unavailable outcomes data and pathological fractures or multiple fractures.
Selection criteria
Data were extracted from the included studies by two independent researchers. We contacted the corresponding author for additional information in case of the study with an incomplete data. The following information was extracted: the first author's name, publication year, interventions, outcome measures, sample size and comparable baselines. Other relevant parameters were also extracted from the individual studies.
Quality assessment
The methodological index for non-randomized studies form was used to assess non-RCT [15]. Quality assessment for the RCTs was conducted according to a modification of the generic evaluation tool described in the Cochrane Handbook for systematic review of interventions [16]. A third reviewer resolved disagreements.
Data extraction
The data were extracted from the included trials by two independently researchers. In cases of incomplete data, the corresponding author of the study was contacted for additional information. The following information was extracted: the first author's name, publication year, interventions, outcome measures, sample size and comparable baselines.
Data analysis & statistical methods
The RevMan 5.1 (The Cochrane Collaboration, Oxford, UK) were used for data analysis. The mean difference (MD) and 95% confidence intervals (CIs) were determined for continuing outcomes. The dichotomous data were calculated by the risk difference and 95% CIs. The heterogeneity was estimated by I2 based on the standard chi-square test. When I2 < 50% and p > 0.1, no significant heterogeneity existed, and a fixed-effects model was used for the data analyzing while a random-effects model was used when I2 > 50% and p < 0.1. Subgroup analysis was performed to investigate the sources of heterogeneity.
Results
Search results
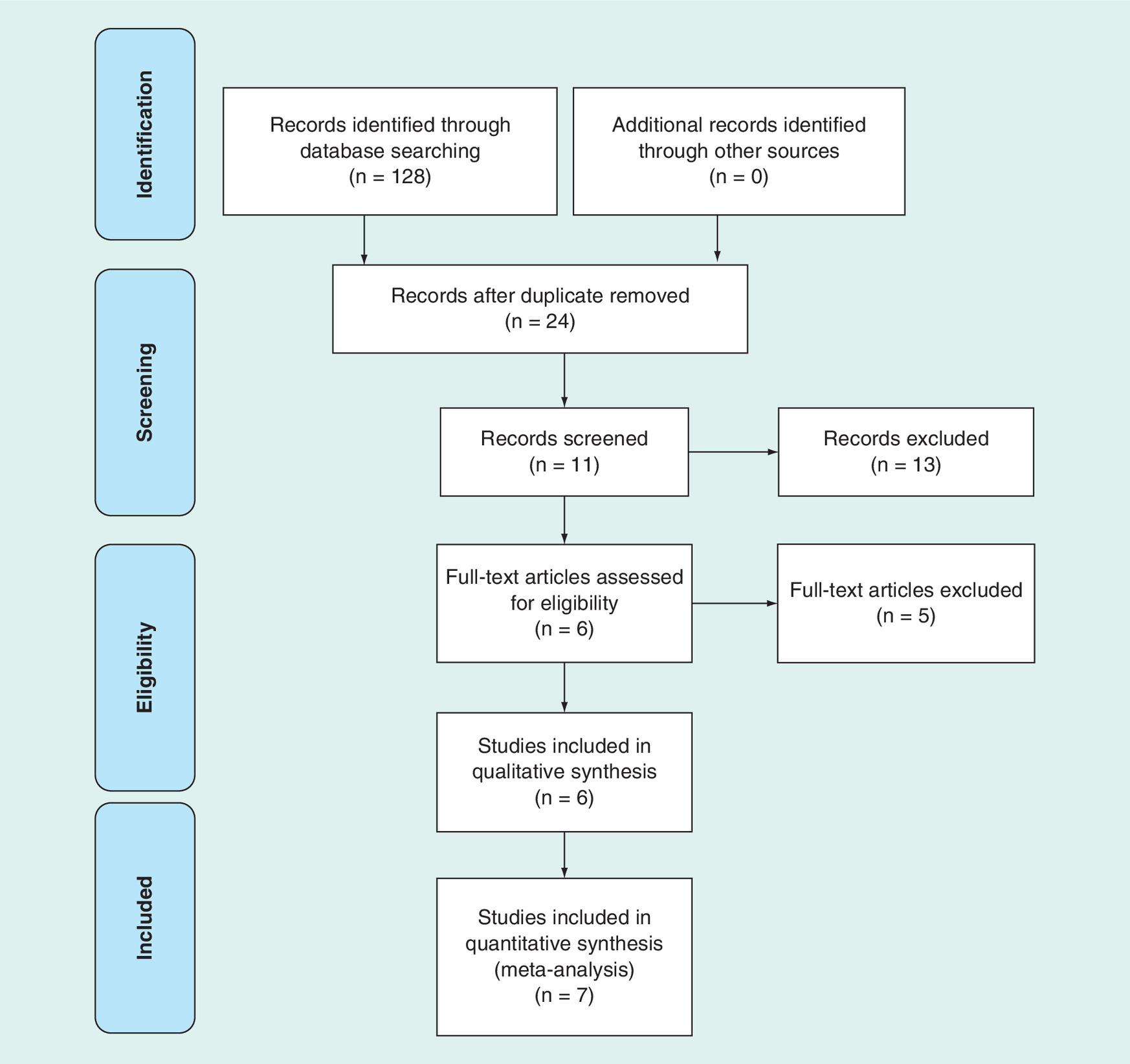
The search strategy identified 158 citations as potentially relevant literature reports. By screening titles and abstracts, 151 references were excluded due to the eligibility criteria. No additional studies were obtained after the reference review. Ultimately, one RCT and six non-RCTs were eligible for data extraction and meta-analysis [9,10,17–21]. A flow chart of the studies recruited in our review was shown in Figure 1.
Risk of bias assessment
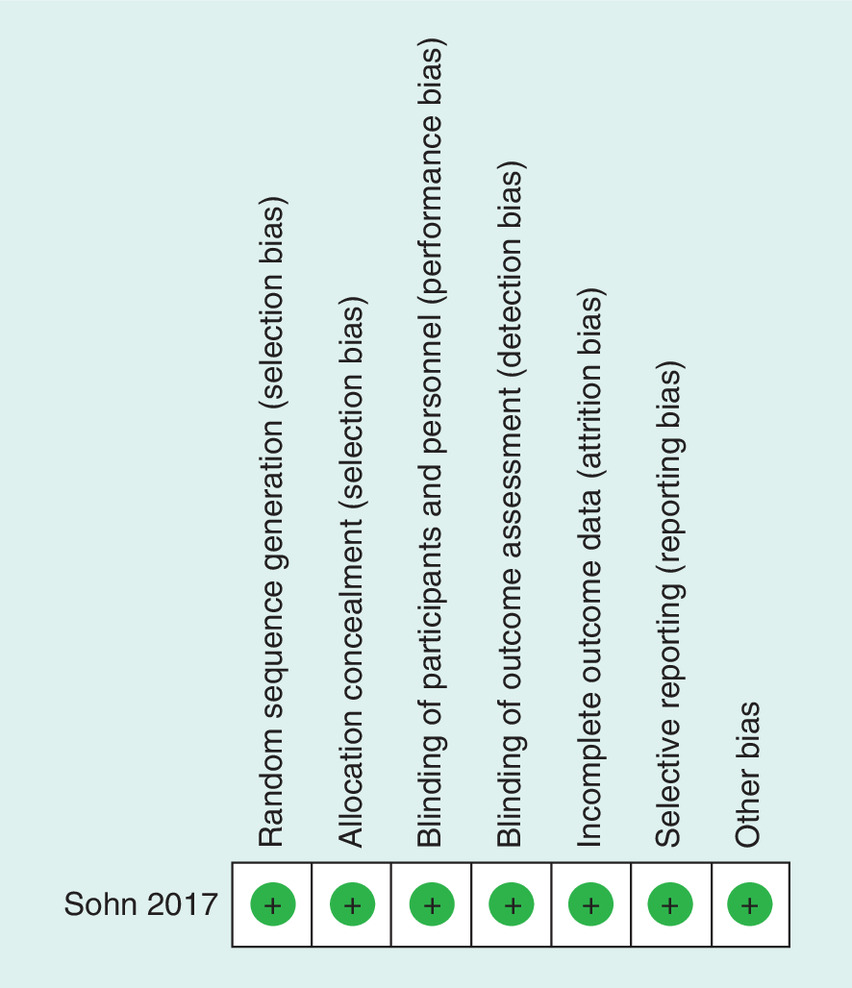
A summary of the methodological assessment results is presented in Figure 2. All the seven parameters showed low risks of bias of RCT. The methodological index for non-randomized studies scores of non-RCTs were 16–20. A summary of the methodological assessment results is presented in Table 2.
| Study (year) | Group | Simple size | Age (Y) | Gender (M/F) | Fracture classification (two/three/four) | Follow-up months | Refs. |
|---|---|---|---|---|---|---|---|
| Chiewchantanakit (2015) | MIPO ORIF | 12 16 | 51.9 62.2 | 4/8 8/8 | 8/4/0 6/10/0 | NS NS | [17] |
| Lin (2014) | MIPO ORIF | 43 43 | 63 61 | 16/27 12/31 | 10/24/9 9/22/12 | 12 12 | [18] |
| Liu (2015) | MIPO ORIF | 39 52 | 60.2 61.7 | 17/22 25/27 | 15/18/6 18/25/9 | 24 24 | [9] |
| Liu (2016) | MIPO ORIF | 33 42 | 50.3 52.1 | 12/21 16/26 | 22/11/0 25/17/0 | 14.2 14.2 | [19] |
| Röderer (2011) | MIPO ORIF | 46 61 | 67.6 65 | 13/33 19/42 | NS NS | 12 12 | [20] |
| Sohn (2017) | MIPO ORIF | 45 45 | 61 62.6 | NS NS | 17/21/7 18/23/4 | 14.3 15 | [10] |
| Zhao (2017) | MIPO ORIF | 17 19 | 64.0 64.3 | 9/8 12/7 | 8/9/0 7/12/0 | 10 10 | [21] |
F: Female; M: Male; MIPO: Minimally invasive plate osteosynthesis; NS: Not stated; ORIF: Open reduction and internal fixation; Y: Year.
| Quality assessment for nonrandomized trials | Chiewchantanakit (2015) [17] | Lin (2014) [18] | Liu (2015) [9] | Liu (2016) [19] | Röderer (2011) [20] | Zhao (2017) [21] |
|---|---|---|---|---|---|---|
| A clearly stated aim | 2 | 2 | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 2 | 2 | 2 | 2 | 2 | 2 |
| Prospective data collection | 0 | 0 | 0 | 0 | 0 | 0 |
| End points appropriate to the aim of the study | 2 | 2 | 2 | 2 | 2 | 2 |
| Unbiased assessment of the study end point | 2 | 2 | 2 | 2 | 2 | 2 |
| A follow-up period appropriate to the aims of study | 2 | 2 | 2 | 2 | 2 | 2 |
| Less than 5 % loss to follow-up | 2 | 0 | 2 | 2 | 2 | 2 |
| Prospective calculation of the sample size | 0 | 0 | 0 | 0 | 0 | 0 |
| An adequate control group | 2 | 2 | 2 | 2 | 2 | 2 |
| Contemporary groups | 2 | 0 | 2 | 2 | 2 | 2 |
| Baseline equivalence of groups | 2 | 2 | 2 | 2 | 2 | 2 |
| Adequate statistical analyses | 2 | 2 | 2 | 2 | 2 | 2 |
| Total score | 20 | 16 | 20 | 20 | 20 | 20 |
Study characteristics
The characteristics of the included studies are shown in Table 1. There was no significant difference between demographic variables in the study. The studies’ sample sizes ranged from 28 to 107 shoulders.
Outcomes of meta-analysis
Operative time
Operative time was shown in seven articles [9,10,17–21]. A random-effects model was performed with obvious heterogeneity (I2 = 88%; p < 0.00001). Operative time in the MIPO group was significantly lower than in the ORIF group (MD = -15.58; 95% CI: -23.44 to -7.73; p = 0.0001; Table 3).
| Outcome | Studies | Groups (MIPO/ORIF) | Overall effect | Heterogeneity | |||
|---|---|---|---|---|---|---|---|
| Effect estimate | 95% CI | p-value | I2(%) | p-value | |||
| Operative time | 7 | 235/278 | -15.58 | -23.44; -7.73 | 0.0001 | 88 | <0.00001 |
| Blood loss | 6 | 190/233 | -77.95 | -151.01; -4.89 | 0.04 | 98 | <0.00001 |
| Time to union | 3 | 74/80 | -0.94 | -5.58; 3.70 | 0.69 | 91 | <0.0001 |
| Union rate | 4 | 132/156 | 0.00 | -0.04; 0.05 | 0.83 | 12 | 0.33 |
| Length of hospital stay | 3 | 101/120 | -1.05 | -1.71; -0.39 | 0.002 | 6 | 0.35 |
| Constant score | |||||||
| 3 months | 2 | 82/95 | 4.47 | 1.95; 7.00 | 0.005 | 0 | 0.68 |
| 6 months | 2 | 82/95 | 4.07 | 1.52; 6.63 | 0.002 | 0 | 0.55 |
| 12 months | 4 | 132/156 | 2.14 | 1.20; 3.08 | 0.00001 | 0 | 0.54 |
| Complications | |||||||
| Avascular necrosis | 4 | 163/200 | -0.01 | -0.05; 0.03 | 048 | 32 | 0.22 |
| Impingement | 3 | 134/149 | -0.01 | -0.05; 0.04 | 0.82 | 0 | 0.83 |
| Screw perforation | 3 | 134/149 | 0.01 | -0.05; 0.08 | 0.72 | 0 | 0.51 |
| Implant loosening | 3 | 130/158 | 0.01 | -0.06; 0.07 | 0.83 | 0 | 0.71 |
| Nerve injury | 4 | 111/130 | 0.01 | -0.03; 0.04 | 0.65 | 0 | 0.94 |
| Delayed union | 2 | 85/113 | -0.01 | -0.04; 0.03 | 0.76 | 0 | 0.53 |
| Infection | 3 | 96/122 | -0.01 | -0.06; 0.04 | 0.69 | 0 | 0.73 |
| Stiff shoulder | 2 | 91/106 | -0.01 | -0.08; 0.06 | 0.87 | 57 | 0.13 |
| Varus collapse | 2 | 88/88 | 0.00 | -0.06; 0.06 | 1.00 | 0 | 0.39 |
CI: Confidence interval; MIPO: Minimally invasive plate osteosynthesis; ORIF: Open reduction and internal fixation.
Blood loss
Time to union
Union rate
Length of hospital stay
Postoperative functional assessment
Constant score at postoperative 3 months were provided in two studies [9,18]. A fixed-effects model was performed without heterogeneity (I2 = 0%; p = 0.68). Constant score at postoperative 3 months in the MIPO group was significantly higher than that in the ORIF group (MD = 4.47; 95% CI: 1.95–7.00; p = 0.005; Table 3). Constant score at postoperative 6 months was provided in two studies [9,18]. A fixed-effects model was performed without heterogeneity (I2 = 0%; p = 0.55). Constant score at postoperative 6 months in the MIPO group was significantly higher than that in the ORIF group (MD = 4.07; 95% CI: 1.52–6.63; p = 0.002; Table 3). Constant scores at postoperative 12 months were reported in four included studies [9,18,19,21]. A fixed-effects model was performed without heterogeneity (I2 = 0%; p = 0.54). Constant score at postoperative 12 months in the MIPO group was significantly higher than in the ORIF group (MD = 2.14; 95% CI: 1.20–3.08; p = 0.00001; Table 3).
Complications
Complications were reported in all six included studies. A fixed-effects model was performed without heterogeneity. No significant difference between the two groups regarding all complications, such as avascular necrosis of humerus head, impingement, screw perforation, implant loosening, nerve injury, delayed union, infection, stiff shoulder and varus collapse (Table 3).
Discussion
Plate fixation has been regarded as an effective treatment for PHF. ORIF and MIPO are two different plate fixation procedures [22]. In the present meta-analysis, we pooled the most recent evidence from both RCTs and non-RCTs and provided the most reliable evidence. This meta-analysis illustrated that, compared with ORIF, MIPO could decrease operative time, blood loss, length of hospital stays and show more effective recovery of shoulder joint function in the treatment of PHF. Based on the results, MIPO is a safe technique with no significant postoperative complications.
Technically, the MIPO technique avoids directly exposing the fracture site to preserve the enveloped soft tissue around the fracture site [23]. Liu et al. [19] reported that MIPO in PHF requires a shorter length of incision than ORIF during the surgery (6.74 vs 16.82 cm). In the present meta-analysis, pooled results indicated that MIPO decrease operative time, blood loss and length of hospital stay. The small incision contributed to the significantly reduced operative time and blood loss.
Several surgeons believed that the MIPO technique maintains the periosteal circulation and potentially accelerates the fracture union process [9,10]. Chiewchantanakit et al. [17] reported that MIPO offers a shorter time to union than ORIF in PHF (12 vs 20 weeks). Pooled results indicated that no significant differences in time to union (p = 0.71) and union rate (p = 0.82) were found between the MIPO and ORIF groups. These may be due to the small sample size of included studies, including simple fractures or better protection of blood supply during ORIF.
Shoulder postoperative function is another element in determining the effectiveness of MIPO in PHF. Different scoring systems were used to assess shoulder function. The Constant score is a clinician-assessed score that has been used extensively in the literature to record patient outcomes following shoulder surgery. The pooled result found MIPO provides a better constant score at postoperative 3, 6 and 12 months (p = 0.005; p = 0.002 and p = 0.004, respectively). Liu et al. reported that constant score and the disabilities of arm, shoulder and hand questionnaire score at postoperative 24 months were not significantly different. The better postoperative function score indicated good rehabilitation.
Malreduction screw perforation or nerve injury may occur because fracture reduction was indirect in the MIPO technique. Complications with MIPO also lead to orthopedic surgeons’ concern. The pooled results showed no significant differences in impingement, screw perforation, implant loosening, nerve injury, infection, stiff shoulder and varus collapse between the two groups. Although the MIPO technique preserves periosteal blood supply without directly exposing the fracture area, pooled result show that MIPO did not decrease the incidence of avascular necrosis of the humeral head in short-term follow-up. The incidence of avascular necrosis of the humeral head may increase in patients with middle- or long-term follow-up.
There are several limitations should be listed: only one RCT was included, which weakened our power to draw a definitively confirming conclusion; the sample sizes were small in most studies; according to the limited number of included studies, the source of heterogeneity could not be determined. We could not perform subgroup analysis in this meta-analysis, and the follow-up period is relatively short and might underestimate the complications.
Conclusion
MIPO in PHF provided significantly shorter operative times, blood loss and length of hospital stay. The MIPO technique had better clinical outcomes compared with ORIF without increasing complications. Further studies that include larger sample sizes, and more detailed clinical data with a longer follow-up time are required to confirm our conclusion.
Minimally invasive plate osteosynthesis (MIPO) is popular for its advantages of reserving and avoiding extensive soft tissue dissection in fracture healing.
A meta-analysis was conducted to compare the efficacy and safety of MIPO with open reduction and internal fixation in the treatment with proximal humeral fracture.
Systematic Cochrane Library, Springer, PubMed, Embase, and ScienceDirect searches (January 1966–March 2018) yielded 158 results; 7 studies were included for review.
Meta-analyses were conducted using a fixed-effects or random model that reported risk difference or mean differences and 95% credible intervals.
MIPO had the lower operative time (MD = -17.33; 95% CI: -27.22 to -7.45; p = 0.0006), blood loss (MD = -90.87; 95% CI: -167.24 to -14.49; p = 0.02), and length of hospital stay (MD = -1.05; 95% CI: -1.71 to -0.39; p = 0.002), and higher constant score than open reduction and internal fixation.
Results for union, union rate and complications were similar across comparators.
MIPO in proximal humeral fractures provided significantly shorter operative times, length of hospital stay and less blood loss.
MIPO technique had better clinical outcomes compared with open plating without increasing complications.
Acknowledgements
The authors thank the authors of all included studies.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
1.
Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury 37(8), 691–697 (2006).
2.
Kannus P, Palvanen M, Niemi S, Sievanen H, Parkkari J. Rate of proximal humeral fractures in older Finnish women between 1970 and 2007. Bone 44(4), 656–659 (2009).
3.
Handoll HH, Brorson S. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev (11), CD000434 (2015).
4.
Chen L, Xing F, Xiang Z. Effectiveness and safety of interventions for treating adults with displaced proximal humeral fracture: a network meta-analysis and systematic review. PLoS ONE 11(11), e0166801 (2016).
5.
Wang G, Mao Z, Zhang L et al. Meta-analysis of locking plate versus intramedullary nail for treatment of proximal humeral fractures. J. Orthop. Surg. Res. 10, 122 (2015).
6.
Dai J, Chai Y, Wang C, Wen G. Meta-analysis comparing locking plate fixation with hemiarthroplasty for complex proximal humeral fractures. Eur. J. Orthop. Surg. Traumatol. 24(3), 305–313 (2014).
7.
Helmy N, Hintermann B. New trends in the treatment of proximal humerus fractures. Clin. Orthop. Relat. Res. 442, 100–108 (2006).
8.
Wijgman AJ, Roolker W, Patt TW, Raaymakers EL, Marti RK. Open reduction and internal fixation of three and four-part fractures of the proximal part of the humerus. J. Bone Joint Surg. Am. 84-A(11), 1919–1925 (2002).
9.
Liu K, Liu PC, Liu R, Wu X. Advantage of minimally invasive lateral approach relative to conventional deltopectoral approach for treatment of proximal humerus fractures. Med. Sci. Monit. 21, 496–504 (2015).
10.
Sohn HS, Jeon YS, Lee J, Shin SJ. Clinical comparison between open plating and minimally invasive plate osteosynthesis for displaced proximal humeral fractures: a prospective randomized controlled trial. Injury 48(6), 1175–1182 (2017).
11.
Ortmaier R, Filzmaier V, Hitzl W et al. Comparison between minimally invasive, percutaneous osteosynthesis and locking plate osteosynthesis in 3-and 4-part proximal humerus fractures. BMC Musculoskelet. Disord. 16, 297 (2015).
12.
Bogner R, Ortmaier R, Moroder P et al. Minimally invasive treatment of displaced proximal humeralractures in patients older than 70 years using the Humerus block. Biomed. Res. Int. (2016) (Epub ahead of print).
13.
Aguado HJ, Mingo J, Torres M, Alvarez-Ramos A, Martin-Ferrero MA. Minimally invasive polyaxial locking plate osteosynthesis for 3–4 part proximal humeral fractures: our institutional experience. Injury 47(Suppl. 3), S22–S28 (2016).
14.
Zhao W, Zhang Y, Johansson D, Chen X, Zheng F, Li L. Comparison of minimally invasive percutaneous plate osteosynthesis and open reduction internal fixation on proximal humeral fracture in elder patients: a systematic review and meta-analysis. Biomed. Res. Int. (2017).
15.
Handoll HH, Gillespie WJ, Gillespie LD, Madhok R. The Cochrane collaboration: a leading role in producing reliable evidence to inform healthcare decisions in musculoskeletal trauma and disorders. Indian J. Orthop. 42(3), 247–251 (2008).
16.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J. Surg. 73(9), 712–716 (2003).
17.
Chiewchantanakit S, Tangsripong P. Locking plate fixation of proximal humeral fracture: minimally invasive vs. standard delto-pectoral approach. J. Med. Assoc. Thai. 98(2), 196–200 (2015).
18.
Lin T, Xiao B, Ma X, Fu D, Yang S. Minimally invasive plate osteosynthesis with a locking compression plate is superior to open reduction and internal fixation in the management of the proximal humerus fractures. BMC Musculoskelet. Disord. 15, 206 (2014).
19.
Liu YW, Wei XE, Kuang Y et al. Open vs. closed reduction combined with minimally invasive plate osteosynthesis in humeral fractures. Minim. Invasive Ther. Allied Technol. 25(4), 215–221 (2016).
20.
Roderer G, Erhardt J, Kuster M et al. Second generation locked plating of proximal humerus fractures: a prospective multicenter observational study. Int. Orthop. 35(3), 425–432 (2011).
21.
Zhao L, Yang P, Zhu L, Chen AM. Minimal invasive percutaneous plate osteosynthesis (MIPPO) through deltoid-pectoralis approach for the treatment of elderly proximal humeral fractures. BMC Musculoskelet. Disord. 18(1), 187 (2017).
22.
Wild JR, Demers A, French R et al. Functional outcomes for surgically treated 3- and 4-part proximal humerus fractures. Orthopedics 34(10), e629–6e33 (2011).
23.
Gonc U, Atabek M, Teker K, Tanriover A. Minimally invasive plate osteosynthesis with PHILOS plate for proximal humerus fractures. Acta Orthop. Traumatol. Turc. 51(1), 17–22 (2017).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 3 May 2018
Accepted: 4 July 2018
Published online: 1 October 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparison between minimally invasive plate osteosynthesis and open plating for proximal humeral fractures: a meta-analysis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0042
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Meisam Jafari Kafiabadi, Saber Barazandeh Rad, Farsad Biglari, Mehrdad Sadighi, Amir Sabaghzadeh, Babak Toloue Ghamari, Adel Ebrahimpour, Combination of MIPO and WALANT procedure versus ORIF and general anesthesia in midshaft clavicle fracture: a prospective comparative cohort study, European Journal of Orthopaedic Surgery & Traumatology, 10.1007/s00590-025-04555-3, 35, 1, (2025).
- Helen HG Handoll, Joanne Elliott, Theis M Thillemann, Patricia Aluko, Stig Brorson, Interventions for treating proximal humeral fractures in adults, Cochrane Database of Systematic Reviews, 10.1002/14651858.CD000434.pub5, 2022, 6, (2022).
- Wardah Rafaqat, Tashfeen Ahmad, Muhammad Talal Ibrahim, Sudhesh Kumar, Eric M. Bluman, Khalid S. Khan, Is minimally invasive orthopedic surgery safer than open? A systematic review of systematic reviews, International Journal of Surgery, 10.1016/j.ijsu.2022.106616, 101, (106616), (2022).
- Feilong Li, Xuqiang Liu, Fuqiang Wang, Zhiping Gu, Qianyuan Tao, Cong Yao, Xuwen Luo, Tao Nie, Comparison between minimally invasive plate osteosynthesis and open reduction-internal fixation for proximal humeral fractures: a meta-analysis based on 1050 individuals, BMC Musculoskeletal Disorders, 10.1186/s12891-019-2936-y, 20, 1, (2019).