Ticagrelor versus clopidogrel in East-Asian patients with acute coronary syndromes: a meta-analysis of randomized trials
Abstract
Aim: To determine whether ticagrelor or clopidogrel provides the best outcomes for East-Asian patients with acute coronary syndrome (ACS). Materials & methods: Identification and interrogation of electronic databases through 26 July 2016 revealed fully randomized and controlled trials wherein primary efficacy end points were major adverse cardiovascular events and all-cause death among East-Asian patients with ACS. Major bleeding and noncoronary artery bypass grafts major bleeding were primary safety end points. Results: Two studies met the inclusion criteria. Compared with clopidogrel, ticagrelor has no statistical difference in the end points of major adverse cardiovascular events (risk ratio [RR]: 1.08; 95% CI: 0.62–1.91; p = 0.7260), myocardial infarction (RR: 1.200; 95% CI: 0.64–2.24; p = 0.5669), stroke (RR: 1.11; 95% CI: 0.46–2.66; p = 0.8165), cardiovascular death (RR: 0.89; 95% CI: 0.48–1.65; p = 0.7150), or all-cause mortality (RR: 0.92; 95% CI: 0.43–1.96; p = 0.8252). When compared with clopidogrel, it was found that ticagrelor provoked marked increases in major bleeding (RR: 1.48; p = 0.0430) and noncoronary artery bypass grafts-associated major bleeding (RR: 1.62; p = 0.0454). Conclusion: Ticagrelor and clopidogrel displayed similar efficacies in ACS presenting patients from East Asia. Administration of ticagrelor also displays some side effects including an increased risk of major bleeding.
Rapid transitions of disease burden are currently progressing and observed throughout China. Major noncommunicable diseases have contributed to substantially greater number of lost years of life in 2013 as compared with 1990 and these diseases include ischemic cardiovascular disease (CVD), stroke and cancer [1]. In the Asia-Pacific region, acute coronary syndrome (ACS) is a leading cause of death [2]. According to the 2014 Chinese report on CVD, CVD-associated mortality is approximately 44.8% in rural areas and approximately 41.9% in urban areas [3]. An increasing trend in the incidence of ACS has been previously reported [3]. The sharp increase in the incidence of ischemic heart disease has resulted in an overutilization of percutaneous coronary intervention (PCI) and coronary catheterization. Using a combination of clopidogrel and aspirin as antiplatelet therapy has rapidly established itself as the cornerstone of the clinical management of ACS or in patients following PCI [4].
As a prodrug, clopidogrel requires two-step metabolism to modify its functional structure to the active form that serves to irreversibly block the platelet adenosine diphosphate (ADP) P2Y12 receptor. As a newly developed antiplatelet agent, ticagrelor noncompetitively blocks ADP-induced receptor signaling or ADP-binding due to its capacity to occupy the P2Y12 receptor [5,6]. In the multicenter Phase III PLATO trial, the clinical efficacy and toxicological safety profile were compared between ticagrelor and clopidogrel in patients that presented with ACS. Ticagrelor showed lower primary composite end points as compared with clopidogrel (9.8 vs 11.7%; p < 0.001), which included death due to CVD, stroke and myocardial infarction (MI). The results also showed that secondary end points had also markedly improved following therapy with ticagrelor [7,8], including MI (5.8 vs 6.9%; p = 0.05), death due to CVD (4.0 vs 5.1%; p = 0.001) and all-cause mortality (4.5 vs 5.9%; p < 0.001). The European Society of Cardiology and the American Heart Association/American College of Cardiology have updated their guidelines for the clinical management and therapy of patients with non-ST-elevated ACS and have done so by recommending ticagrelor administration as a key component of administered dual antiplatelet agents [9]. This is also a key therapeutic strategy that is recommended by cardiologists in East Asia [10]. However, an increasing body of data indicates that the East-Asian population that present with ACS or undergo PCI display highly variable risk profiles for bleeding and thrombophilia when compared with the Western population and a dissimilar platelet reactivity following PCI or ACS (the ‘East-Asian Paradox’) [11–13]. Therefore, East-Asian specific evidence is clearly warranted before firm decision is made to adopt the Western treatment strategies for P2Y12 inhibitors in East-Asian patients.
To replace the ‘one-guideline-fits-all races’ with ‘race-tailored antiplatelet therapy’ in the clinical management of ACS patients, we carried out a meta-analysis to examine with the overarching goal of determining the efficacy and safety of ticagrelor and clopidogrel in the East-Asian patients presenting with ACS.
Methods
Search strategy
This meta-analysis was conducted by following the methods that were previously described in the Cochrane Handbook and the preferred reporting items for systematic reviews and meta-analyses (PRISMA) [14]. Seven databases were independently searched by two investigators (B Wu and H Lin) until 26 July 2016 and included PubMed, Web of Science, EMBASE, The Cochrane Library, VIP, the Wanfang Database and the China National Knowledge Infrastructure (CNKI). Clinical trials were also searched at ClinicalTrials.gov and chictr.org.cn. The following provides an example of the search strategy used in our study: ‘clopidogrel’ AND (‘ticagrelor’ OR ‘AZD6140’) AND (‘acute coronary syndrome’ OR ‘unstable angina’ OR ‘myocardial infarction’ OR ‘percutaneous coronary intervention’) combined with ‘trial’. Furthermore, the reference list of eligible reports were cross-checked to the Google Scholar database to confirm that all appropriate studies were included. In addition, a manual search of all references extracted from the original studies was conducted in an attempt to identify additional published reports.
The current study represents a synthesis of a detailed analysis of the published data. Consequently, ethics committee approval was not needed for this study and was not sought.
Study selection
To obtain valid studies for this meta-analysis, the following preselected criteria were established: prospective randomized controlled trials (RCT); patients of East-Asian origin (including China, Taiwan, Macao, Hong Kong, South and North Korea, Japan, and Mongolia); clinical trials that compared ticagrelor with clopidogrel; follow-up time greater than or equal to 1 year [15]; and articles with available previously published data for at least one of the following outcome measures: major adverse cardiovascular event (MACE), MI, stroke, vascular death, all-cause death, major bleeding and major bleeding events that were associated with noncoronary artery bypass grafts (CABG). No specific restrictions involving language or publication year were applied. Irrelevant studies were excluded by scanning the titles and abstracts.
The exclusion criteria included the following: repetitive publications; analyses confined to specific subgroups of ACS population; reviews, case reports and case-only reports; studies of animal or cell cultures in vitro; and absence of ethical information.
Data extraction
All of the retrieved titles and abstracts for eligibility were inspected by two independent authors (i.e., H Lin and RG Tobe). Any disagreements and discrepancies in the analysis of the results were resolved by iteration and consensus. Duplicated reports, including those studies that used the same participant cohorts were excluded. The following information was obtained from every eligible report: name of the first author; publication year; country of origin; study design; number of participants; age of patients; completeness of the follow-up; and results of the clinical outcomes.
Quality assessment
The Jadad composite score was used for studying quality evaluation. This system scores a research article according to the descriptions of randomization (2 points), blinding (2 points) and attrition information (1 point). A score of ≥3 points suggests that the study was ‘high quality’; and a score of ≤2 points suggests that the study was of ‘low quality’ [16].
Data synthesis
All-cause death (death), MACEs, MI, death due to CVD, stroke, major bleeding and major bleeding that was associated with non-CABG were the primary outcomes. MACEs were referred to as a composite end point, including death due to CVD, stroke and MI [17]. The pooled relative risks (RRs) with 95% CI between ticagrelor and clopidogrel were calculated to establish the effect sizes using MetaXL version 5.3 statistical software (EpiGear International Pty Ltd, Wilston, Australia). We assessed heterogeneity among studies by Cochran's Q test and the I[2] statistic [18]. We indicated substantial and significant heterogeneity as follows: I[2] >50% and p < 0.05 [19]. We employed fixed-effect models in the case of low heterogeneity (I[2] <30%). Otherwise, we chose random effects models. Begg's tests examined publication bias [19,20]. An α value of p < 0.05 was deemed significant. All statistical tests were two-tailed. A funnel plot was created when the number of included reports was ≥10.
Results
Study selection
A total of 1265 literature citations were retrieved, including 941 potentially relevant studies (Figure 1). Of these, 119 publications were filtered to the final analysis for detailed evaluation by retrieving the full text. Finally, we included two articles in the meta-analysis.
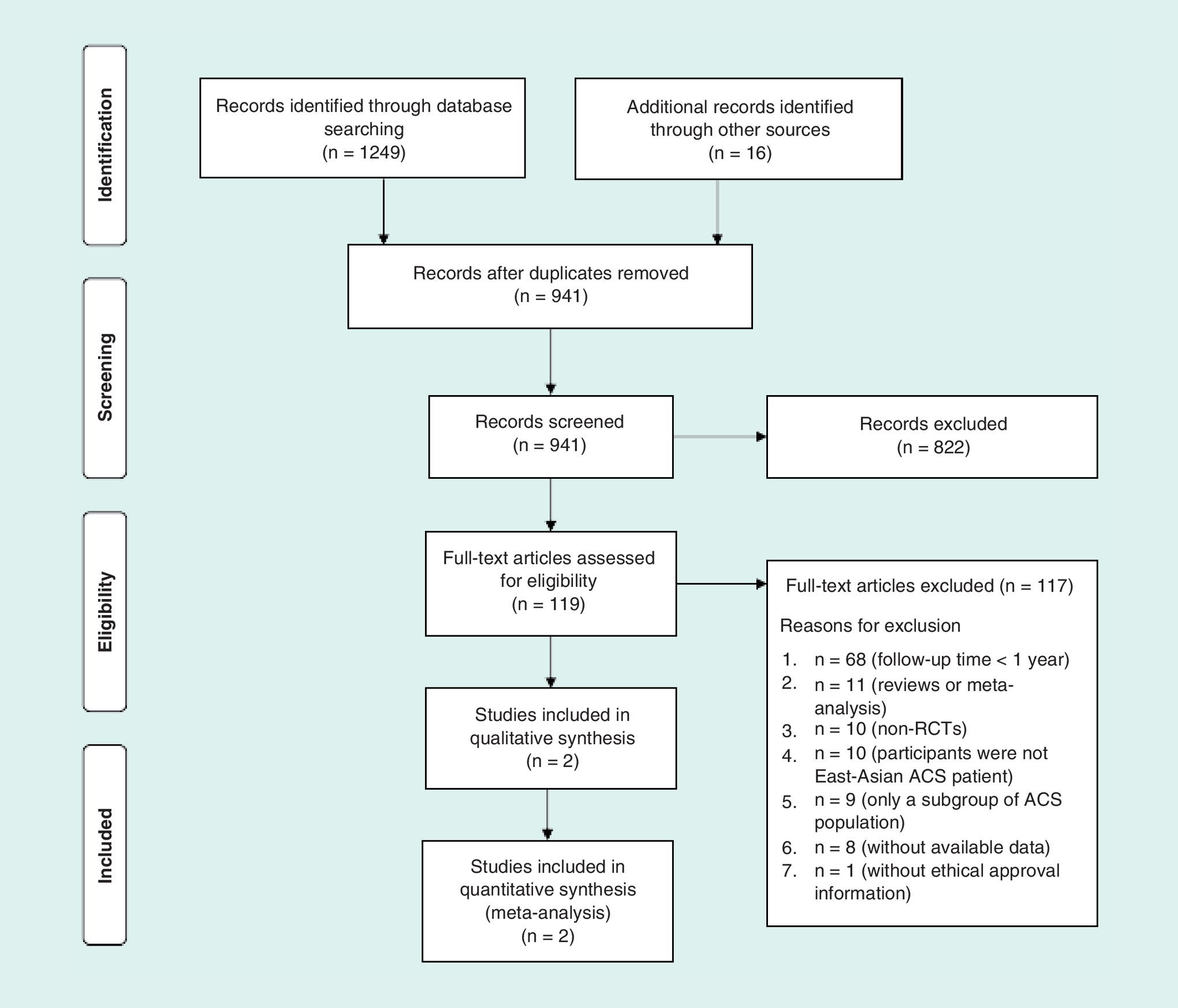
Figure 1. Flowchart outlining the study selection.
ACS: Acute coronary syndrome; RCT: Randomized controlled trial.
Study characteristics
Two RCT studies enrolled 1352 participants matching the inclusion criteria including 679 participants that were designated to the ticagrelor treatment group and 673 participants that were designated to the clopidogrel treatment group [21,22]. The characteristics of the included studies are shown in Table 1. No significant publication bias was indicated by Begg's test. The quality of the trials was high (Table 1).
| Variables | PLATO East Asia† | PHILO | |
|---|---|---|---|
| Trial design | Multicenter, randomized, controlled and double-blind trial | Multicenter, randomized, controlled and double-blind trial | |
| Sample size (n) | Study drug | 278 | 401 |
| Control drug | 273 | 400 | |
| Intervention in control group | Clopidogrel 300–600 mg loading dose and 75 mg b.i.d. daily | Clopidogrel 300 mg loading dose and 76 mg b.i.d. daily | |
| Intervention in study group | Ticagrelor 180 mg loading dose and 90 mg b.i.d. daily | Ticagrelor 180 mg loading dose and 91 mg b.i.d. daily | |
| Age (years) | Study drug | 60 | 67 |
| Control drug | 61 | 66 | |
| Female (%) | Study drug | 24.8 | 23.7 |
| Control drug | 27.8 | 23.3 | |
| ACS type (%) | |||
| Unstable angina | Study drug | 13.1 | 29.7 |
| Control drug | 16 | 27.3 | |
| Non-ST-segment elevation MI | Study drug | 38.1 | 16.5 |
| Control drug | 35.2 | 18.5 | |
| ST-segment elevation MI | Study drug | 45.6 | 51.1 |
| Control drug | 45.4 | 52.5 | |
| Medical and surgical history (%) | |||
| Angina pectoris | Study drug | 44.5 | 25.4 |
| Control drug | 45 | 27.5 | |
| MI | Study drug | 12 | 8.2 |
| Control drug | 17.7 | 7.8 | |
| Prior PCI | Study drug | 7.9 | 11.2 |
| Control drug | 7.9 | 10.5 | |
| Prior CABG | Study drug | 1.3 | 1.2 |
| Control drug | 2 | 0.3 | |
| Prior TIA | Study drug | 1.3 | 1.5 |
| Control drug | 2.2 | 2.8 | |
| Peripheral artery disease | Study drug | 0.7 | 3.2 |
| Control drug | 1.6 | 3.5 | |
| Chronic renal disease | Study drug | 4.4 | 4.5 |
| Control drug | 4.3 | 5 | |
| Diabetes mellitus | Study drug | 28.7 | 38.4 |
| Control drug | 30.1 | 31.1 | |
| Hypertension | Study drug | 60.2 | 76.1 |
| Control drug | 62.4 | 72.5 | |
| Dyslipidemia | Study drug | 31 | 78.3 |
| Control drug | 35.1 | 72.3 | |
| Ethnic group (%) | |||
| Chinese | Study drug | N/A | 4 |
| Control drug | N/A | 4.8 | |
| Japanese | Study drug | N/A | 90 |
| Control drug | N/A | 90 | |
| Korean | Study drug | N/A | 5.7 |
| Control drug | N/A | 5.3 | |
| Primary outcome | Composite of cardiovascular death, myocardial infarction and stroke | Composite of cardiovascular death, myocardial infarction and stroke | |
| Jadad score | 5 | 5 | |
†Data derived from the whole Asian cohort
ACS: Acute coronary syndrome; CABG: Coronary artery bypass graft; MI: Myocardial infarction; PCI: Percutaneous coronary intervention; TIA: Transient ischemic attack.
Meta-analysis
The risk of MACE (Figure 2) following treatment with ticagrelor was not statistically significant when compared with clopidogrel (8.69 vs 7.88%; RR: 1.08; 95% CI: 0.62–1.91; p = 0.7260). There was also no significant difference in MI (5.3 vs 4.3%; RR: 1.20; 95% CI: 0.64–2.24; p = 0.5669), stroke (1.62 vs 1.49%; RR: 1.11; 95% CI: 0.46–2.66; p = 0.8165) and death from CVD (2.80 vs 3.12%; RR: 0.89; 95% CI: 0.48–1.65; p = 0.7150), respectively (Figure 3). Similarly, the end point of all-cause mortality was not statistically different between ticagrelor and clopidogrel (2.94 vs 3.27%; RR: 0.92; 95% CI: 0.43–1.96; p = 0.8252). In addition, treatment with ticagrelor induced a significant increase in major bleeding (9.4 vs 6.3%; RR: 1.48; 95% CI: 1.01–2.16; p = 0.0430) and non-CABG related major bleeding (6.49 vs 4.01%; RR: 1.62; 95% CI: 1.01–2.60, p = 0.0454; Figure 4).
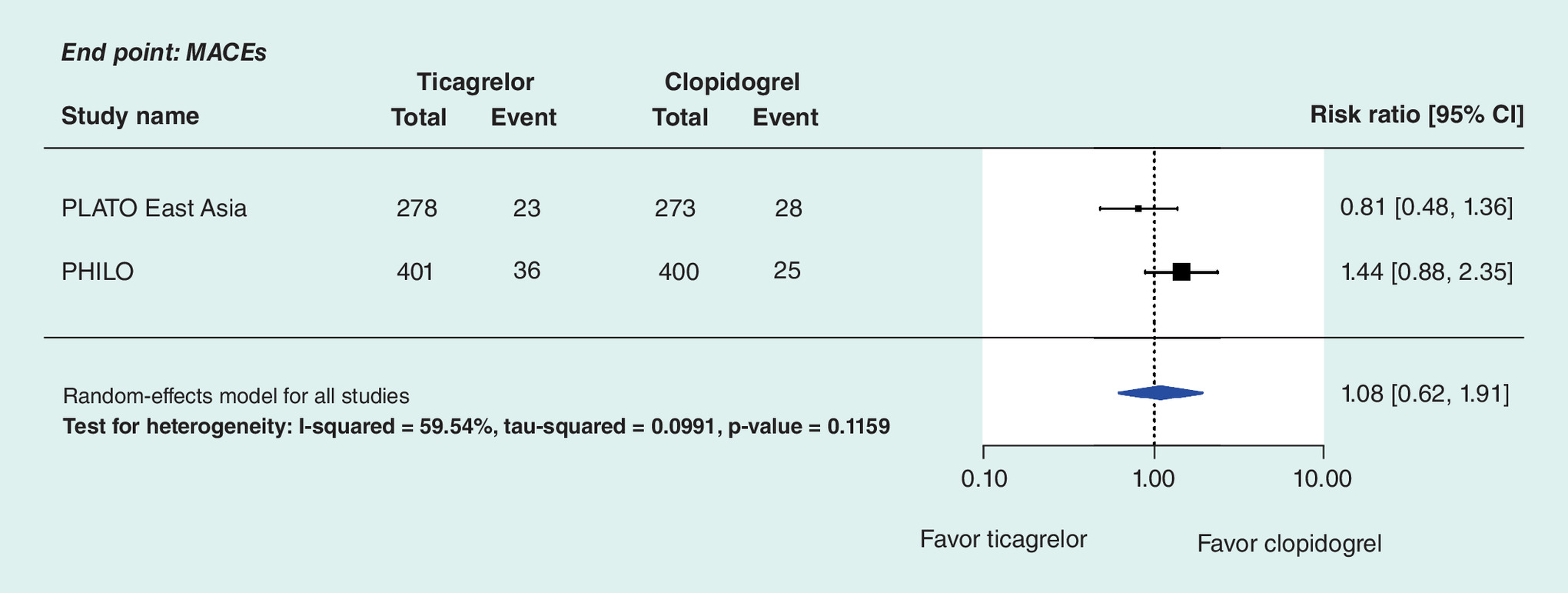
Figure 2. Forest plots of major adverse cardiovascular events in trials of ticagrelor as compared with clopidogrel in East-Asian patients with coronary artery disease.
MACE: Major adverse cardiovascular event.
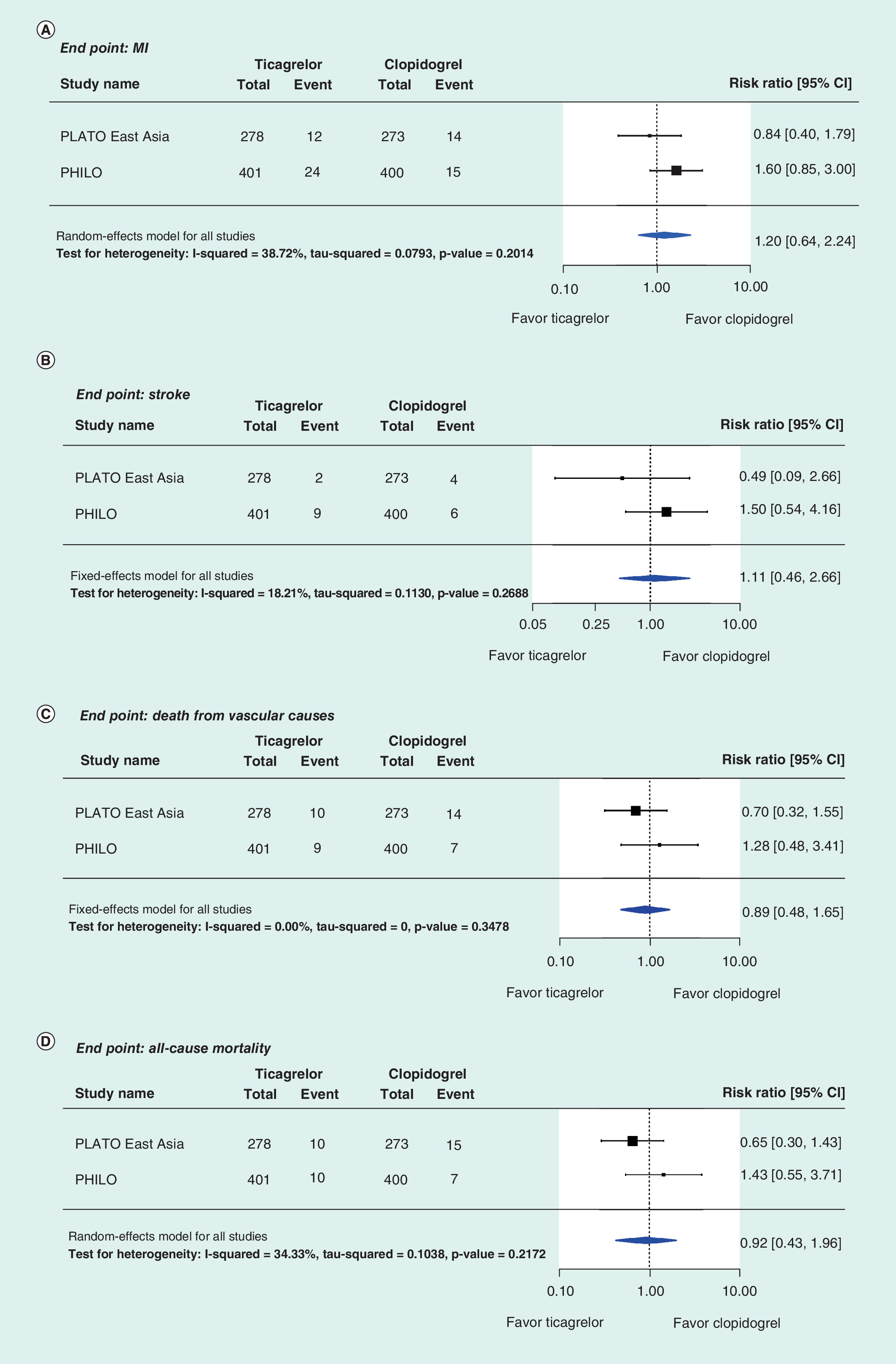
Figure 3. Results of clinical effectiveness.
Forest plots of (A) MI, (B) stroke, (C) death from vascular causes and (D) all-cause mortality in trials of ticagrelor versus clopidogrel in patients with coronary artery disease.
MI: Myocardial infarction.
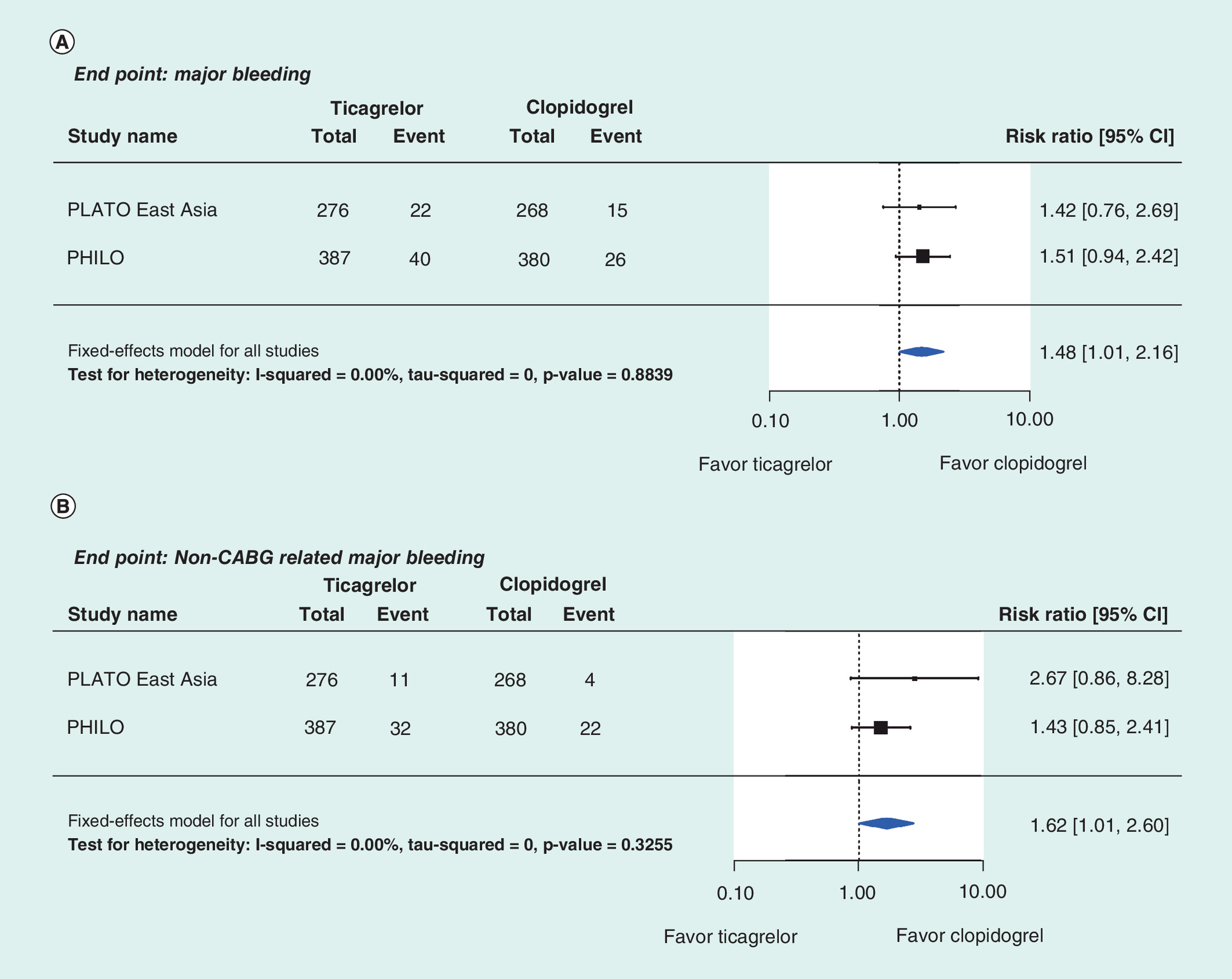
Figure 4. Results of clinical safety.
Forest plots of (A) major bleeding and (B) non-CABG-related major bleeding from vascular causes in trials of ticagrelor as compared with clopidogrel in patients presenting with coronary artery disease.
CABG: Coronary artery bypass graft.
Discussion
This meta-analysis extends prior analyses when considering the choice between ticagrelor and clopidogrel treatment in East-Asian populations that present with ACS. The pooled results from both selected trials representing more than 1400 patients improved the significance of the findings. As a validation design of the PLATO trial, the PHILO study enrolled patients from Japan, South Korea and Taiwan with the intent of exploring the consistency of the effects of ticagrelor in the PLATO study. Therefore, the meta-analysis findings have implications for treatment strategies in East-Asian populations presenting with ACS.
The results showed similar efficacy of MACE between the clopidogrel and the ticagrelor treatment group among East-Asian patients. We also found similar results or outcomes for MI, stroke, death from CVD and all-cause mortality. To our knowledge, the current meta-analysis is the first of its kind to establish the efficacy of ticagrelor when directly compared with clopidogrel in the setting of ACS, which was made possible by pooling the RCT data in East-Asian populations. Our finding was inconsistent when compared with other meta-analyses that showed outcomes with new oral antiplatelet treatment strategies with prasugrel or ticagrelor was associated with a notable decrease in mortality, MI and in-stent thrombosis in Western patients [23–26]. This discrepancy could be explained by the variation in the risk for thrombosis as a function of racial/ethnic diversity. Several studies have shown similar or lower risks of adverse ischemic outcomes or stent thrombosis after PCI in East-Asian patients as compared with Caucasians [27,28]. Based on the Texas (US) Heart Institute Research Database (THIRDBase) and the Coronary Revascularization Demonstrating Outcome (CREDO-Kyoto) registries, a recent study has found that Japanese patients manifested notably better survival outcomes than US patients after coronary revascularization when grouped by ethnicity (e.g., Hispanics: hazard ratio [HR]: 1.53; 95% CI: 1.22–1.93; Caucasians: HR: 1.56; 95% CI: 1.35–1.79; African–Americans: HR: 2.03; 95% CI: 1.62–2.56), except for Asian–Americans (HR: 0.84; 95% CI: 0.38–1.89) [29]. The genetic polymorphisms among ethnicities, which include prothrombin (G20210A) and factor V Leiden (G1691A) gene mutations, might partially account for this variation [30]. The different risk profiles for thrombosis in East-Asian patients as compared with Western patients might need to be demonstrated in the first instance to indicate a statistical difference with sufficient power between ticagrelor and clopidogrel. This is because the sample size of clinical trials conducted in East-Asian patients might need to be larger than in Western patients. Also, the outcomes might be different from those that have been found in Western patients.
The safety of P2Y12 inhibitors is a concern among clinicians and patients, especially with respect to major bleeding. Other meta-analyses found no significant increase in bleeding complications [23–26]. However, the populations included in those meta-analyses were mostly derived from the Western population. The current analysis focused on East-Asian patients. It showed that ticagrelor had a 48% increased risk of major bleeding events and a 62% increased risk of non-CABG major bleeding events when compared with clopidogrel, (p < 0.05), which is not in line with the above meta-analyses. Based on the Korea Acute Myocardial Infarction Registry, one recent report also found that ticagrelor did not decrease the risk of ischemic events, however, was associated with increased risk of bleeding complications in comparison with clopidogrel [31]. This difference could be explained by the propensity for bleeding between East-Asian and Caucasian populations. The threshold of antiplatelet therapy for Asian populations is two- to five-times higher than that found in the general US population because of a higher estimated incidence of hemorrhagic stroke following aspirin treatment (1.14 in the Japanese population vs 0.37 in the USA per 1000 person-years) [31]. The ACCEL-BLEED study tested the relationship between bleeding and platelet function in East-Asian patients undergoing PCI. This study showed that East Asians had a higher cut-off value of platelet reactivity that was associated with bleeding than previously reported in the general Western population [32].
Pharmacokinetic studies showed that active metabolite exposure rates in Asian patients were higher (nearly 20–30%) and pharmacodynamic responses were stronger than their Caucasian counterparts under conditions when the same oral doses of the new P2Y12 inhibitors were administered [33,34], which indicated a lower dose of ticagrelor might be reasonable in East-Asian patients presenting with ACS [12]. Currently, Japanese cardiologists have reduced the dose of clopidogrel to decrease the appearance of bleeding complications [12]. However, Chinese and South Korean physicians largely follow the ACC/AHA guidelines when managing their patients with ACS. The recommended doses of antiplatelet drugs are generally similar to those of the ACC/AHA. In East Asians, a rational dose of P2Y12 inhibitors should be explored due to their excessive inhibition of platelet function. An open-label trial showed that low-dose ticagrelor exhibited similar antiplatelet efficacy when compared with standard-dose ticagrelor in healthy Chinese volunteers [35], although this observation needs to be explored further to determine whether it could be applied to ACS patients.
The following describe the strengths of the current meta-analysis and include: comprehensive literature review; strict inclusion and exclusion criteria; specificity on East-Asian patients; the most up-to-date study; and robustness of the results. By pooling the clinical efficacy and safety end points, the potential utility of ticagrelor was adequately evaluated in East-Asian patients using ACS at the current time-point.
The limitations associated with this analysis includes the absence of individual data preventing an assessment of the association between individual variables and study outcomes. Further, only two studies with a relatively small sample size were included in our meta-analysis, which might have a potential impact on the detection of differences in adverse cardiovascular events that might be associated with ticagrelor and clopidogrel among East-Asian patients. Well-designed clinical trials are clearly needed. In view of the foregoing concerns described above, the conclusion described below should be treated with some caution.
Conclusion
The present meta-analysis showed that ticagrelor was related to a marked increase in major bleeding among East-Asian patients that presented with ACS when compared with clopidogrel. The efficacy of reducing the risk of major ischemic events was similar when comparing the effects of ticagrelor with clopidogrel.
Future perspective
The two antiplatelet agents and their treatment patterns should be carefully selected by carefully assessing the potential health benefits and toxicological safety profile of the agents. With further consideration of the relatively lower daily cost of clopidogrel as compared with ticagrelor, the preferred use of clopidogrel is strongly recommended for East-Asian patients that present with ACS. However, due to the limitation of current available data, especially high-quality studies among East-Asian population, further studies are needed to compare the efficacy and safety outcomes that might be associated with ticagrelor and clopidogrel in East-Asian populations. Appropriate doses of these drugs should also be further evaluated in high-quality dose-ranging studies.
Background
Antiplatelet therapy is the cornerstone of the clinical management of acute coronary syndrome. However, there is a paucity of East-Asian-specific evidence.
A meta-analysis was performed to summarize clinical study results for two antiplatelet agents, ticagrelor and clopidogrel in the East-Asian population.
Results
Systematic literature search (until 26 July 2016) yielded 1265 results; two studies were included for review.
Compared with clopidogrel, ticagrelor has no statistical difference in the end points of major adverse cardiovascular events (risk ratio [RR]: 1.08; 95% CI: 0.62–1.91; p = 0.7260), myocardial infarction (RR: 1.200; 95% CI: 0.64–2.24; p = 0.5669), stroke (RR: 1.11; 95% CI: 0.46–2.66, p = 0.8165), cardiovascular death (RR: 0.89; 95% CI: 0.48–1.65; p = 0.7150) or all-cause mortality (RR: 0.92; 95% CI: 0.43–1.96; p = 0.8252).
It was found that ticagrelor provoked marked increases in major bleeding (RR: 1.48; p = 0.0430) and noncoronary artery bypass grafts-associated major bleeding (RR: 1.62; p = 0.0454).
Conclusion
Results of this meta-analysis showed that ticagrelor and clopidogrel displayed similar efficacies in acute coronary syndrome presenting patients from East Asia. Administration of ticagrelor also displays some side effects including an increased risk of major bleeding.
Financial & competing interests disclosure
This study was supported by grants from the National Natural Science Foundation of China (NO. 71373160), and Shanghai Municipal Commission of Health and Family Planning (Evidence-based Public Health and Health Economics, NO. 15GWZK0901). The funding agencies had no role in the study design, data collection and analysis of the data, or the decision to publish. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Assistance with the writing and development of the manuscript was provided by MedSci and was funded by Sanofi China.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Zhou M, Wang H, Zhu J et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet 387(10015), 251–272 (2016).
2.
Chan MY, Du X, Eccleston D et al. Acute coronary syndrome in the Asia-Pacific region. Int. J. Cardiol. 202, 861–869 (2016).
3.
Deng M, Li H, Shi M et al. Prevalence of acute coronary heart disease among farmers in Panyu, Guangzhou: a 20 year population-based study. Zhonghua Xin Xue Guan Bing Za Zhi 42(3), 236–240 (2014).
4.
Cowley MJ, Kuritzky L. Developments in antiplatelet therapy for acute coronary syndromes and considerations for long-term management. Curr. Med. Res. Opin. 25(6), 1477–1490 (2009).
5.
Hochtl T, Sinnaeve PR, Adriaenssens T, Huber K. Oral antiplatelet therapy in acute coronary syndromes: update 2012. Eur. Heart. J. Acute Cardiovasc. Care 1(1), 79–86 (2012).
6.
Htun WW, Steinhubl SR. Ticagrelor: the first novel reversible P2Y(12) inhibitor. Expert Opin. Pharmacother. 14(2), 237–245 (2013).
7.
Wallentin L, Becker RC, Budaj A et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 361(11), 1045–1057 (2009).
8.
Cannon CP, Harrington RA, James S et al. Comparison of ticagrelor with clopidogrel in patients with a planned invasive strategy for acute coronary syndromes (PLATO): a randomised double-blind study. Lancet 375(9711), 283–293 (2010).
9.
Cayla G, Silvain J, Collet JP, Montalescot G. Updates and current recommendations for the management of patients with non-ST-elevation acute coronary syndromes: what it means for clinical practice. Am. J. Cardiol. 115(5 Suppl.), 10A–22A (2015).
10.
Chinese College of Cardiovascular Physician. Chinese expert consensus statement on clinical use of ticagrelor. Zhonghua Xin Xue Guan Bing Za Zhi 44(2), 112–120 (2016).
11.
Levine GN, Jeong YH, Goto S et al. Expert consensus document: World Heart Federation expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI. Nat. Rev. Cardiol. 11(10), 597–606 (2014).
•• This evidence based review described an ‘East-Asian paradox’ phenomenon in which, despite a higher level of platelet reactivity during clopidogrel treatment, East-Asian patients have a similar or lower rate of ischemic events after percutaneous coronary intervention compared with white patients, which also suggested that these evidences should be taken into consideration during the development of regional and national guidelines for East-Asian patients with acute coronary syndrome or undergoing percutaneous coronary intervention.
12.
Jeong YH. “East asian paradox”: challenge for the current antiplatelet strategy of “one-guideline-fits-all races” in acute coronary syndrome. Curr. Cardiol. Rep. 16(5), 485 (2014).
13.
Levine GN, Jeong YH, Goto S et al. World heart federation expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI. Glob. Heart 9(4), 457–467 (2014).
14.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6(7), e1000097 (2009).
15.
Bittl JA, Baber U, Bradley SM, Wijeysundera DN. duration of dual antiplatelet therapy: a systematic review for the 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation 134(10), e156–e178 (2016).
16.
Jadad AR, Moore RA, Carroll D et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control. Clin. Trials 17(1), 1–12 (1996).
17.
Bavishi C, Panwar S, Messerli FH, Bangalore S. Meta-analysis of comparison of the newer oral p2y12 inhibitors (prasugrel or ticagrelor) to clopidogrel in patients with non-st-elevation acute coronary syndrome. Am. J. Cardiol. 116(5), 809–817 (2015).
18.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 327(7414), 557–560 (2003).
19.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat. Med. 21(11), 1539–1558 (2002).
20.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 50(4), 1088–1101 (1994).
21.
Goto S, Huang CH, Park SJ, Emanuelsson H, Kimura T. Ticagrelor vs. clopidogrel in Japanese, Korean and Taiwanese patients with acute coronary syndrome – randomized, double-blind, phase III PHILO study. Circ. J. 79(11), 2452–2460 (2015).
22.
Kang HJ, Clare RM, Gao R et al. Ticagrelor versus clopidogrel in Asian patients with acute coronary syndrome: a retrospective analysis from the Platelet Inhibition and Patient Outcomes (PLATO) Trial. Am. Heart J. 169(6), 899–905 (2015).
23.
Navarese EP, Verdoia M, Schaffer A et al. Ischaemic and bleeding complications with new, compared with standard, ADP-antagonist regimens in acute coronary syndromes: a meta-analysis of randomized trials. QJM 104(7), 561–569 (2011).
24.
Verdoia M, Schaffer A, Barbieri L et al. Benefits from new ADP antagonists as compared with clopidogrel in patients with stable angina or acute coronary syndrome undergoing invasive management: a meta-analysis of randomized trials. J. Cardiovasc. Pharmacol. 63(4), 339–350 (2014).
25.
Bellemain-Appaix A, Brieger D, Beygui F et al. New P2Y12 inhibitors versus clopidogrel in percutaneous coronary intervention: a meta-analysis. J. Am. Coll. Cardiol. 56(19), 1542–1551 (2010).
26.
Gan XD, Wei BZ, Fang D et al. Efficacy and safety analysis of new P2Y12 inhibitors versus clopidogrel in patients with percutaneous coronary intervention: a meta-analysis. Curr. Med. Res. Opin. 31(12), 2313–2323 (2015).
27.
Kumar RS, Douglas PS, Peterson ED et al. Effect of race and ethnicity on outcomes with drug-eluting and bare metal stents: results in 423 965 patients in the linked National Cardiovascular Data Registry and centers for Medicare & Medicaid services payer databases. Circulation 127(13), 1395–1403 (2013).
• Evaluted the effect of race and ethnicity on outcomes with drug-eluting and bare metal stents in the linked National Cardiovascular Data Registry and centers for Medicare & Medicaid services payer databases.
28.
Sorich MJ, Rowland A, McKinnon RA, Wiese MD. CYP2C19 genotype has a greater effect on adverse cardiovascular outcomes following percutaneous coronary intervention and in Asian populations treated with clopidogrel: a meta-analysis. Circ. Cardiovasc. Genet. 7(6), 895–902 (2014).
29.
Inohara T, Kohsaka S, Goto M et al. Hypothesis of Long-term outcome after coronary revascularization in Japanese patients compared with multiethnic groups in the US. PLoS ONE 10(5), e128252 (2015).
30.
Ye Z, Liu EH, Higgins JP et al. Seven haemostatic gene polymorphisms in coronary disease: meta-analysis of 66,155 cases and 91,307 controls. Lancet 367(9511), 651–658 (2006).
31.
Morimoto T, Fukui T, Lee TH, Matsui K. Application of U.S. guidelines in other countries: aspirin for the primary prevention of cardiovascular events in Japan. Am. J. Med. 117(7), 459–468 (2004).
32.
Kwon TJ, Tantry US, Park Y et al. Influence of platelet reactivity on BARC classification in East Asian patients undergoing percutaneous coronary intervention. Results of the ACCEL-BLEED study. Thromb. Haemost. 115(5), 979–992 (2016).
33.
Guo LZ, Kim MH, Jin CD et al. Comparison of pharmacodynamics between low dose ticagrelor and clopidogrel after loading and maintenance doses in healthy Korean subjects. Platelets 26(6), 563–569 (2015).
34.
Small DS, Payne CD, Kothare P et al. Pharmacodynamics and pharmacokinetics of single doses of prasugrel 30 mg and clopidogrel 300 mg in healthy Chinese and white volunteers: an open-label trial. Clin. Ther. 32(2), 365–379 (2010).
35.
Li P, Gu Y, Yang Y et al. Low-dose ticagrelor yields an antiplatelet efficacy similar to that of standard-dose ticagrelor in healthy subjects: an open-label randomized controlled trial. Sci. Rep. 6, 31838 (2016).
• Low-dose ticagrelor achieved faster and higher inhibition of platelet functions in healthy Chinese subjects than did clopidogrel, with an antiplatelet efficacy similar to that of standard-dose ticagrelor.
Information & Authors
Information
Published In
Copyright
© 2017 Future Medicine Ltd.
History
Received: 21 September 2017
Accepted: 16 October 2017
Published online: 2 November 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Ticagrelor versus clopidogrel in East-Asian patients with acute coronary syndromes: a meta-analysis of randomized trials. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0074
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Abdur Rehman Khalid, Farooq Ahmad, Muhammad Ahrar Bin Naeem, Smak Ahmed, Muhammad Umar, Hassan Mehmood, Muhammad Kashif, Shazib Ali, Safety of Clopidogrel vs. Ticagrelor in Dual Antiplatelet Therapy Regimens for High-Bleeding Risk Acute Coronary Syndrome Patients: A Comprehensive Meta-analysis of Adverse Outcomes, High Blood Pressure & Cardiovascular Prevention, 10.1007/s40292-024-00635-3, 31, 2, (141-155), (2024).
- Yinxue Guo, Pingyu Ge, Ziju Li, Jingxia Xiao, Lirui Xie, Ticagrelor or Clopidogrel as Antiplatelet Agents in Patients with Chronic Kidney Disease and Cardiovascular Disease: A Meta-analysis, American Journal of Cardiovascular Drugs, 10.1007/s40256-023-00600-w, 23, 5, (533-546), (2023).
- Jingyuan Li, Qian Wang, Chunliu Wu, Xiaoyu Qu, Lei Zhang, Xiaofeng He, Sicong Ma, Miaohan Qiu, Xiaozeng Wang, Safety and Efficacy of Ticagrelor versus Clopidogrel in East Asian Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention Treated with Dual Antiplatelet Therapy: A Meta-Analysis of Randomized Controlled Trials, Cardiology, 10.1159/000530602, 148, 4, (363-373), (2023).
- Wenxing Peng, Yunnan Zhang, Xiaoxi Li, Yang Lin, Efficacy and Safety of Clopidogrel Versus Ticagrelor for Stabilized Patients With Acute Coronary Syndromes After Percutaneous Coronary Intervention: Results From a Real-World Registry in China, Journal of Cardiovascular Pharmacology, 10.1097/FJC.0000000000001381, 81, 2, (134-140), (2023).
- Yunxian Chen, Shaowen Tu, Zhixin Chen, Jue Xia, Baofeng Chen, Jinfeng Chen, Jiarong Liang, Xiangyang Liu, Liangqiu Tang, Ticagrelor versus Clopidogrel in Patients with Severe Renal Insufficiency Undergoing PCI for Acute Coronary Syndrome, Journal of Interventional Cardiology, 10.1155/2022/6476777, 2022, (1-9), (2022).
- Wenxing Peng, Yunnan Zhang, Yang Lin, Low-dose and standard-dose ticagrelor compared with clopidogrel in patients with acute coronary syndromes: A cohort study from china, Frontiers in Cardiovascular Medicine, 10.3389/fcvm.2022.937261, 9, (2022).
- Niklas Bergh, Anna Myredal, Per Nivedahl, Max Petzold, Sultan Zarin, Constanze Wartenberg, Susanna M. Wallerstedt, Efficacy and Safety of Clopidogrel Versus Ticagrelor as Part of Dual Antiplatelet Therapy in Acute Coronary Syndrome—A Systematic Review and Meta-analysis, Journal of Cardiovascular Pharmacology, 10.1097/FJC.0000000000001233, 79, 5, (620-631), (2022).
- Meijiao He, Yanxiang Zang, Danghui Sun, Jianqiang Li, Guangzhong Liu, Jing Shi, Yue Li, Ticagrelor versus clopidogrel in East Asian patients with acute coronary syndrome: A meta-analysis, Frigid Zone Medicine, 10.2478/fzm-2022-0004, 2, 1, (30-40), (2022).
- Jack WC Tan, Derek P Chew, Muhamad Ali SK Abdul Kader, Junya Ako, Vinay K Bahl, Mark Chan, Kyung Woo Park, Praveen Chandra, I-Chang Hsieh, Do Quang Huan, Sofian Johar, Dafsah Arifa Juzar, Byeong-Keuk Kim, Cheol Whan Lee, Michael Kang-Yin Lee, Yi-Heng Li, Wael Almahmeed, Eric Oliver Sison, Doreen Tan, Yu-Chen Wang, Shiuan Jong Yeh, Gilles Montalescot, 2020 Asian Pacific Society of Cardiology Consensus Recommendations on the Use of P2Y12 Receptor Antagonists in the Asia-Pacific Region, European Cardiology Review, 10.15420/ecr.2020.40, 16, (2021).
- Ji Heon Kim, Doreen Su-Yin Tan, Mark Yan Yee Chan, Cost-effectiveness of CYP2C19-guided antiplatelet therapy for acute coronary syndromes in Singapore, The Pharmacogenomics Journal, 10.1038/s41397-020-00204-6, 21, 2, (243-250), (2021).