Experience with developing antibiotic stewardship programs in Serbia: potential model for other Balkan countries?
Abstract
Aim: Antimicrobial resistance and inappropriate use of antibiotics in children are important issues. Consequently, there is a need to develop comprehensive stewardship programs even in hospitals with limited resources starting with children's hospitals. Methods: Retrospective observational analysis of antimicrobial utilization and resistance patterns over 5 years in a tertiary care children's hospital in Serbia. Results: Cumulative antimicrobial resistance decreased but was still high, with high cumulative resistance rates among the most widely used antibiotics in the hospital. Total antibiotic use decreased from 2010 to 2014 although there was still high prescribing of reserved antibiotics. Conclusion: Concerns with inappropriate use and high resistance rates among some antibiotics used in the hospital are being used to develop guidance on future antibiotic use in this hospital, building on the recently introduced antibiotic stewardship program, as well as encourage other hospitals in Serbia to review their policies.
There are concerns with increasing resistance to antibiotics through their inappropriate use, leading to increased morbidity, mortality and costs [1–5]. The costs of antibiotic resistance in Europe were estimated at €1.5 billion in 2007, now reaching €9 billion per year or higher [6,7], with costs also increasing with the use of newer more expensive antibiotics to treat resistant organisms [2,8]. As a result, the monitoring of antimicrobial resistance (AMR), antibacterial use and the establishment of infection control programs, including the development of antibiotic stewardship (AS) programs in hospitals, are seen as increasingly necessary to reduce resistance development and conserve existing antibiotics [9–15]. As part of this, antibiotic prescribing in children is of primary concern to reduce future morbidity and mortality. This includes both access to antibiotics, which can be a concern in some countries, as well as appropriate use [2,3,7].
In Serbia, antimicrobial use policies within hospitals are principally based on administrative measures and restrictions. In 2005, the concept of reserving antibiotics was implemented within the reimbursed hospital drug list, List B. This has resulted in regulations regarding their use including countersigning by specialists and an evaluation of the microbiological outcomes [16,17]. Under exceptional circumstances, hospitals can use an antibiotic which is not on the positive list [18]. Currently, restricted antibiotics include the carbapenems, linezolid, vancomycin, piperacillin–tazobactam, teicoplanin, colistin and ceftriaxone. In addition, in 2013, the Ministry of Health requested that every hospital in Serbia should establish an antibiotic committee to instigate AMR monitoring and reporting as well as give professional advice for the rational use of antibiotics [19]. However, there were limited resources to implement such measures.
Despite these initiatives, data regarding antibiotic use and AMR patterns among children in hospitals in Serbia are currently very limited. This is not helped by the fact that antibiotic prescriptions and microbiology test results are often recorded on separate pieces of paper by different departments. As a result, making correlations between the two datasets is challenging. This will potentially compromise the implementation of activities such as surveillance of antibiotic utilization and/or AMR patterns.
Consequently, we sought to combine these two datasets within a leading children's hospital in Serbia to guide future empiric use as part of antimicrobial stewardship programs. Our assumption was that if we found concerns in a leading children's hospital in Serbia, there will be a high likelihood of similar concerns among other hospitals in Serbia where children are being treated as well as more widely within Serbia.
Materials & methods
A retrospective drug utilization (DU) and surveillance study was conducted among the pediatric and pediatric surgery clinics (125 beds) of a tertiary care institution in Serbia, the Clinical Centre Kragujevac hospital, which overall has 1274 beds. The number of beds available for children (patients aged 0–18 years) did not significantly change during the study period, with the number of bed days oscillating between 28,576 and 36,171 per year in the pediatric wards.
In the first part of the study, we undertook an analysis combining antimicrobial utilization data with cumulative resistance in 2010 versus 2014.
Antibiotic utilization data were measured using the Anatomical Therapeutic Chemical Classification (ATC)/defined daily dose (DDD) methodology, with DDDs typically accepted for recording medicine use for comparative purposes [20–24]. We are aware that DDDs are normally assigned based on their use in adults, and for medicines approved for use in children, dose recommendations will differ based on children's age and body weight. In addition, many medicines used in children are typically not approved for such use, and documentation regarding dosing regimens are generally unavailable. Consequently, the WHO International Working Group for Drug Statistics Methodology concluded that pediatric DDDs are impossible to assign, and prescribed daily dosages and indications in pediatric population should be used if available [25]. However, if this is difficult, the Working Group suggested that DDDs should be used as a measuring tool for overall comparisons [25].
Antibiotic dispensing data were collected from the hospital pharmacy on all antibiotics prescribed for systemic use among children from 2010 to 2014. In order to concentrate on the most prescribed antibiotics, the data on their utilization were limited to those antibiotics which comprised 90% of the total utilization expressed in DDDs/100 patient days [23,26,27]. At the same time, we followed the percentages of bacterial isolates resistant and susceptible to the same antibiotics that were used in the study site. Utilization and resistance rates were combined. Cumulative resistance rates were calculated for those microbes naturally susceptible to each antibiotic from those antibiotics comprising 90% of the total antibiotic utilization as a percentage of resistant, intermediate or susceptible strains from the total number of strains analyzed. Resistant and intermediate strain data were subsequently combined. This is part of ongoing antimicrobial stewardship programs in the hospital.
We are aware that AS programs do differ in their content from hospital to hospital, and from country to country, to reduce infections and colonization with antibiotic-resistant bacteria within hospitals [15,28,29]. We are also aware that there are limited data available on their implementation and effectiveness among pediatric patients [30]. In the Clinical Center Kragujevac, AS was composed of the following elements: establishing a drug and therapeutics committee; issuing antibiotic prescribing policies and hospital formularies via the drug and therapeutics committee; biannual analysis of resistance patterns among the isolates from the central intensive care unit (ICU) and its distribution to all clinicians; preauthorization of reserve antibiotics dispensing by a clinical pharmacology specialist; issuing local guidelines for antibiotic prophylaxis and empiric treatment; and consulting clinical pharmacologists and infectious diseases specialists when prescribing antibiotics to complex patients. The AS was fully implemented in this hospital at the beginning of 2014, and is ongoing.
Data on AMR were obtained from hospital microbiological laboratory. This included more than 90,000 uniform Excel files from 2010 to 2014 containing information, for instance, regarding the clinic/ward where the specimens were collected and in which material, for example, sputum, blood or liquor, which bacteria were isolated, what antibiotics were used to test potential bacteria resistance and what the results were. Using Excel macros, data involving children were extracted for each year. The data were subsequently filtered to improve the understanding in tables and graphs. Duplicate samples with the same isolates from the same patients were taken into account as one sample.
We included only species with at least ≥30 isolates tested. Under certain circumstances, when we did not have ≥30 isolates, we combined the isolates form two consecutive years into the calculations [27]. All sources of potential microbes, including pus, sputum, wounds, blood and urine, were analyzed together since we wished to represent the total volume of resistant pathogens circulating in the hospital. Microbiology reports define resistant, intermediate or sensitive strains according to the Clinical and Laboratory Standard Institute (CLSI) standards [31]. Antimicrobial susceptibility systems employed by the microbiology department have not changed through the years.
The costs per DDD were also calculated to help with future guidance. Cost data was recorded in local currency (RSD) to avoid problems with currency conversions. This included developments in the procurement system, including centralized procurement, to help reduce costs [32].
In the second part of the study, we looked at AMR patterns in more detail for five consecutive years to determine specific cumulative resistance and utilization rates for the predominant bacterial population to provide future guidance. For these microbes, cumulative resistance rates were calculated for the most used antibiotics from the antibiotic panel used in the sensitivity tests with the same methodology described above.
Data from clinical and surgical units included in the study are provided in one group as the first step of introducing a new surveillance system in hospital settings with limited resources. This methodology can be further modified by the type of medical specialty (medical vs surgical, ICU and non-ICU) since the nature of any surveillance system is to disentangle the epidemiology of antibiotic use and define areas at risk of antibiotic misuse.
Results
Antibiotic utilization data
Figure 1 documents the utilization and resistance profile for antibiotics for systemic use (ATC J01) in the pediatric and pediatric surgery clinics of Clinical Center Kragujevac in 2010.
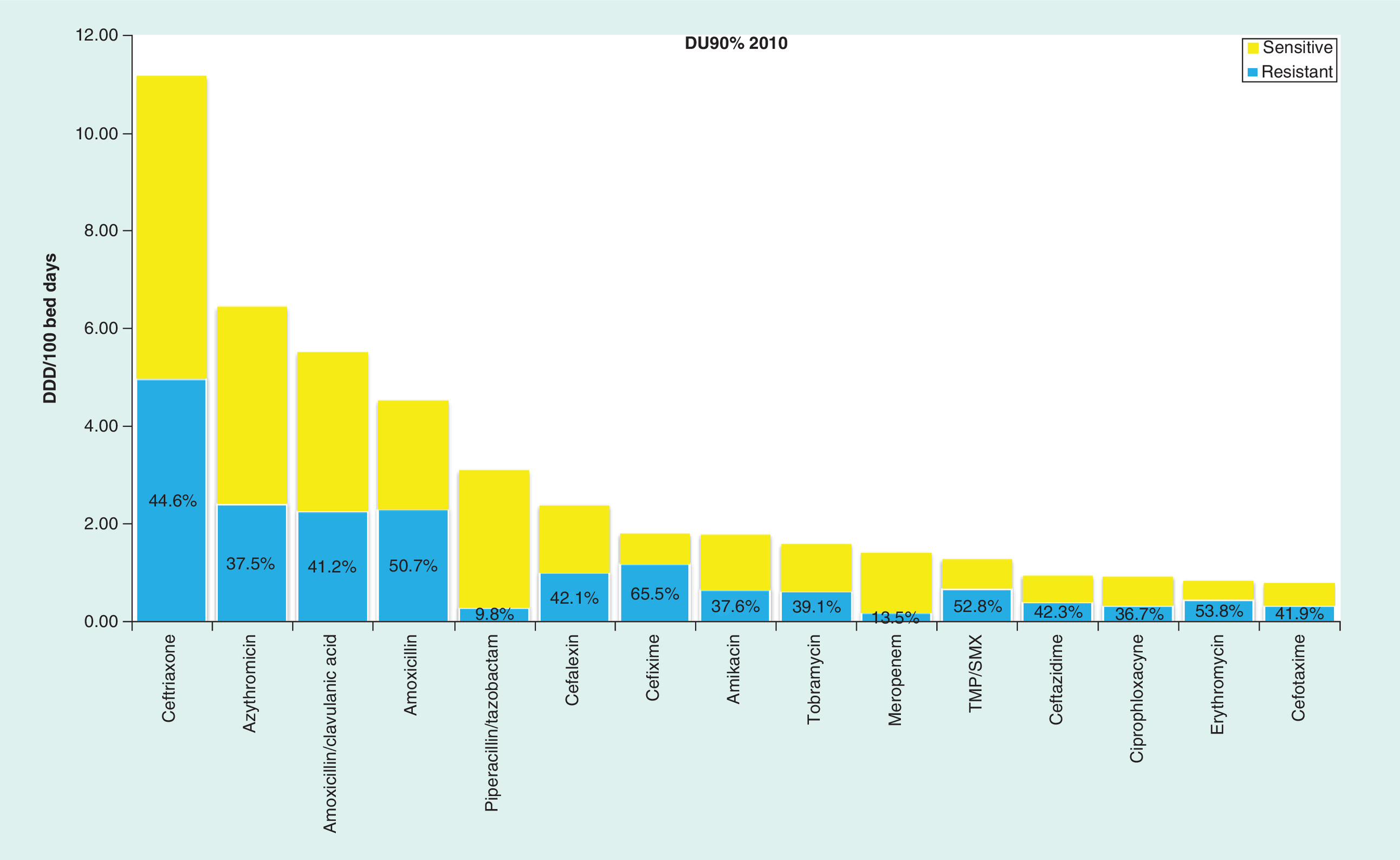
Figure 1. Drug utilization 90%-cumulative resistance profile in 2010.
DDD: Defined daily dose; DU: Drug utilization.
In 2010, antibiotics outside DU90% included ampicillin, benzylpenicillin, phenoxymethylpenicillin, benzylpenicillin procaine, chloramphenicol, cefazolin, cefuroxime, cefprozil, cefepime, imipenem/cilastatin, clarithromycin, clindamycin, gentamicin, vancomycin, teicoplanin, colistin and metronidazole. Supplementary Table 1 documents the 15 antibiotics ranked in order of the number of DDDs corresponding to 90% of their use in 2010 as well as percentage resistance.
Figure 2 documents antibiotics for systemic use (ATC J01) as well as resistance profiles in pediatric and pediatric surgery clinics of Clinical Center Kragujevac in 2014.
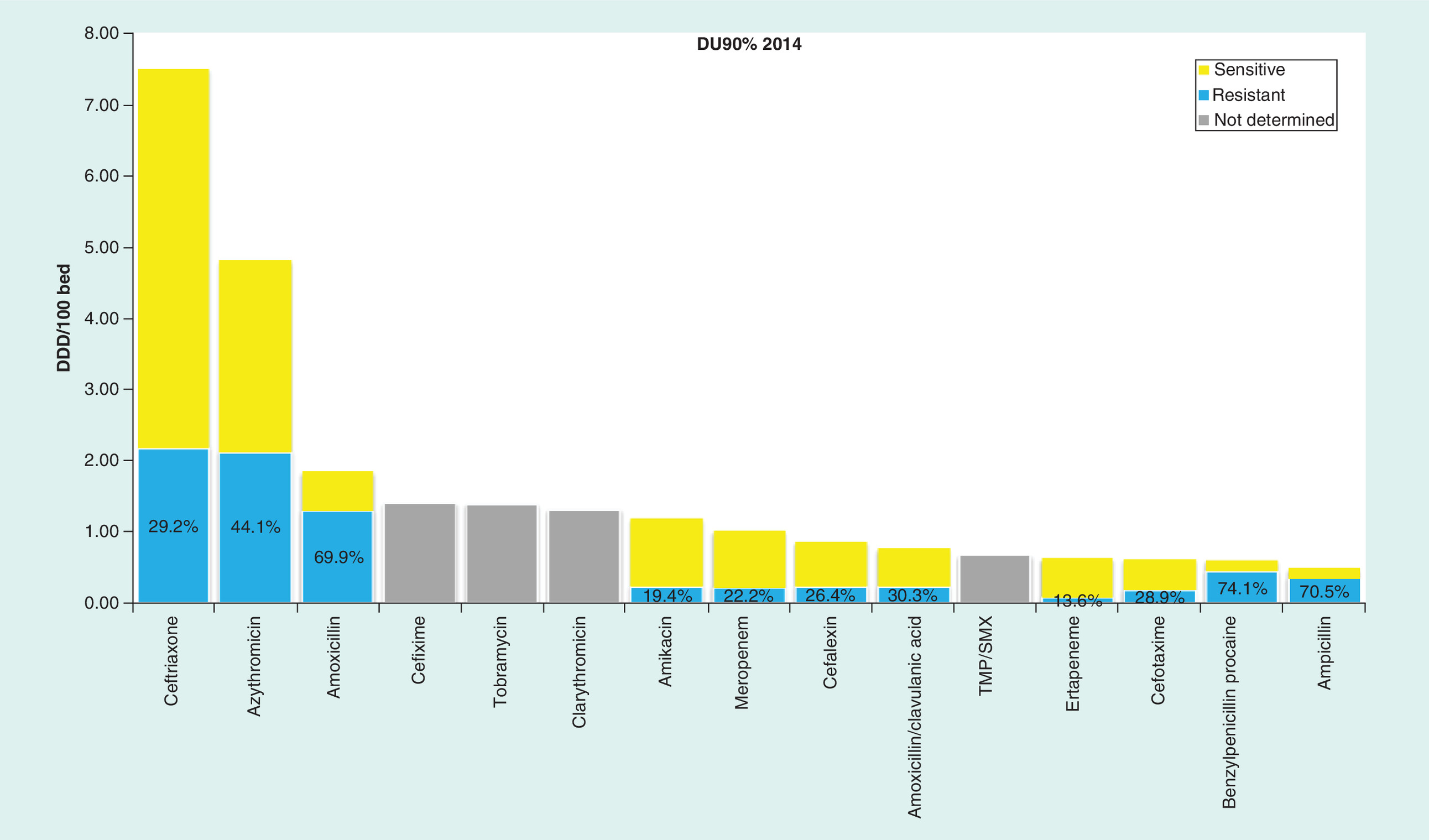
Figure 2. Drug utilization 90%-cumulative resistance profile in 2014.
DDD: Defined daily dose; DU: Drug utilization.
In 2014, antibiotics outside DU90% included chloramphenicol, ampicillin–sulbactam, piperacillin–tazobactam, cefazolin, cefprozil, ceftazidime, imipenem/cilastatin, erythromycin, clindamycin, gentamicin, ofloxacin, ciprophloxacin, vancomycin, teicoplanin, colistin and metronidazole. Supplementary Table 2 documents the 15 antibiotics ranked in order of the number of DDDs corresponding to 90% of the use in 2014.
From the antibiotic DU90% profile for 2010 versus 2014, total antimicrobial use among children in the hospital was 49.4 and 27.8 DDDs/100 bed days in 2010 versus 2014 (Supplementary Tables 1 & 2). There were limited changes in the patterns of antibiotic use comparing 2010 with 2014. The utilization of reserve antibiotics from the reimbursement drug list was approximately 30% of the total consumption within the DU90% segment, with high utilization of ceftriaxone and low utilization of the other restricted antibiotics. Cumulative resistance rates generally decreased with a slight increase of resistance to azithromycin (from 37.5 to 44.1%, 2010 vs 2014, calculated by dividing the number of resistant isolates by the total number of isolates). However, there was high cumulative resistance to benzyl penicillin, amoxicillin and ampicillin as the antibiotic panel used in sensitivity tests for Staphylococcus aureus, the most common isolated bacteria, included these antibiotics and almost all S. aureus tested were 100% resistant. No data on resistance patterns were available for 4 out of the 15 most commonly used antibiotics in 2014, while all were available in 2010. These were cefixime, tobramycin, clarithromycin and TMP–SMX. Finally, the total costs per DDD typically decreased during the study period.
Specific cumulative resistance & utilization rates for predominant bacterial population
The number of the assays performed for the pediatric and pediatric surgery clinics was comparable across the years, for example, 4516 in 2010, 5268 in 2011, 4441 in 2012, 5217 in 2013 and 6871 in 2014.
The most identified isolated organisms in the pediatric and pediatric surgery clinics in Clinical Center Kragujevac in 2014 were S. aureus (36%), Streptococcus pneumoniae (20%) and Escherichia coli (13%).
As methicillin resistance is the CLSI-recommended surrogate for all beta lactams, we report just the extent of methicillin-resistant S. aureus. This reflected a general downward trend from 13.3% in 2010 to 3.8% in 2011, 0% in 2012, 6.7% in 2013 and 0.5% in 2014. Oxacillin is currently not available in Serbia, just cloxacillin. However, the antibiotic panel used in sensitivity tests for S. aureus does not contain routine testing for cloxacillin. In addition, cefpodoxime is not currently tested, with cefpodoxime known to have good activity among major respiratory pathogens [36]
Figures 3–5 provide further details of the most common bacteria and the most common AMR patterns. Streptococcus pneumoniae isolates used to create the antibiogram reflected complicated and refractory infections since S. pneumoniae is not routinely cultured in uncomplicated otitis media or pneumonia (Figure 3).
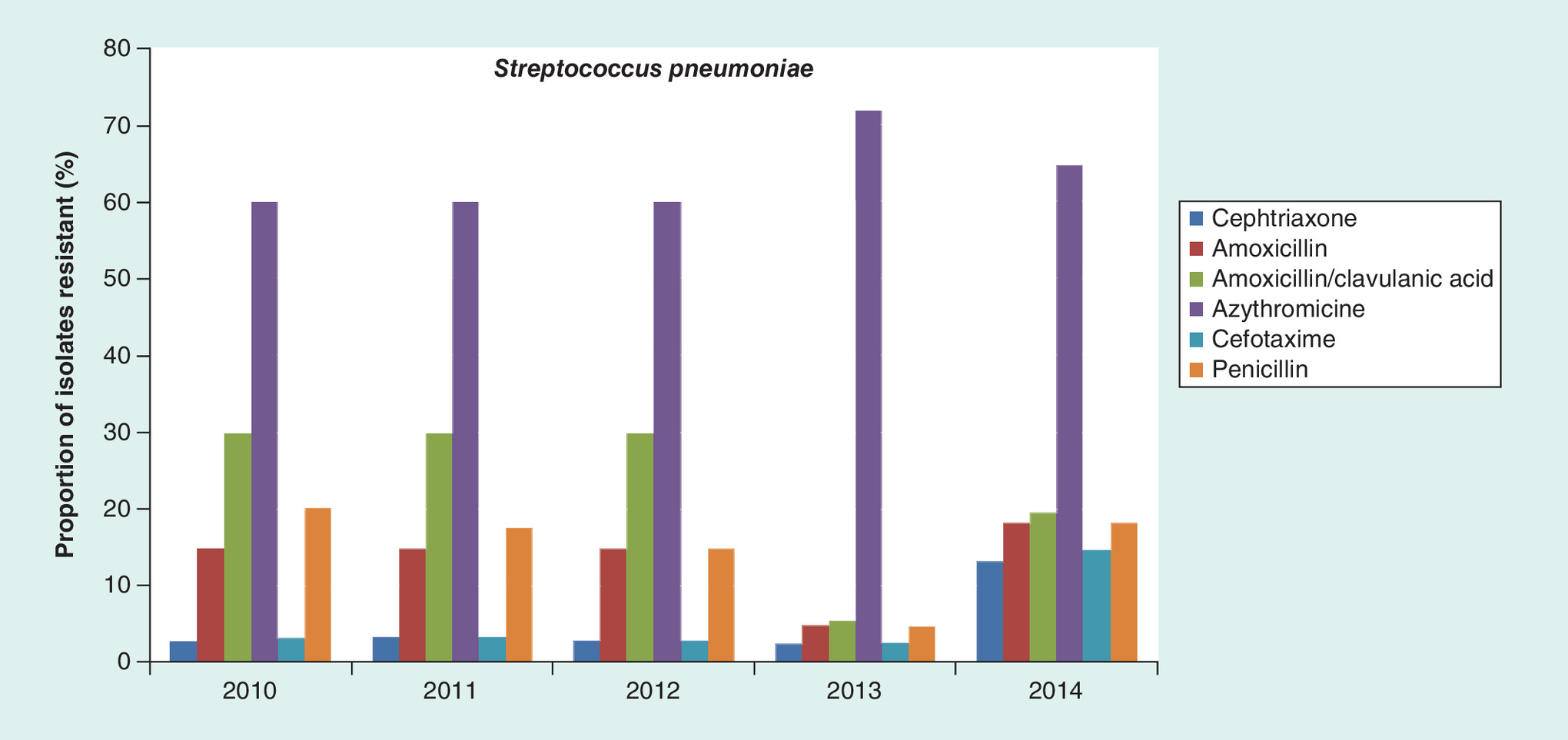
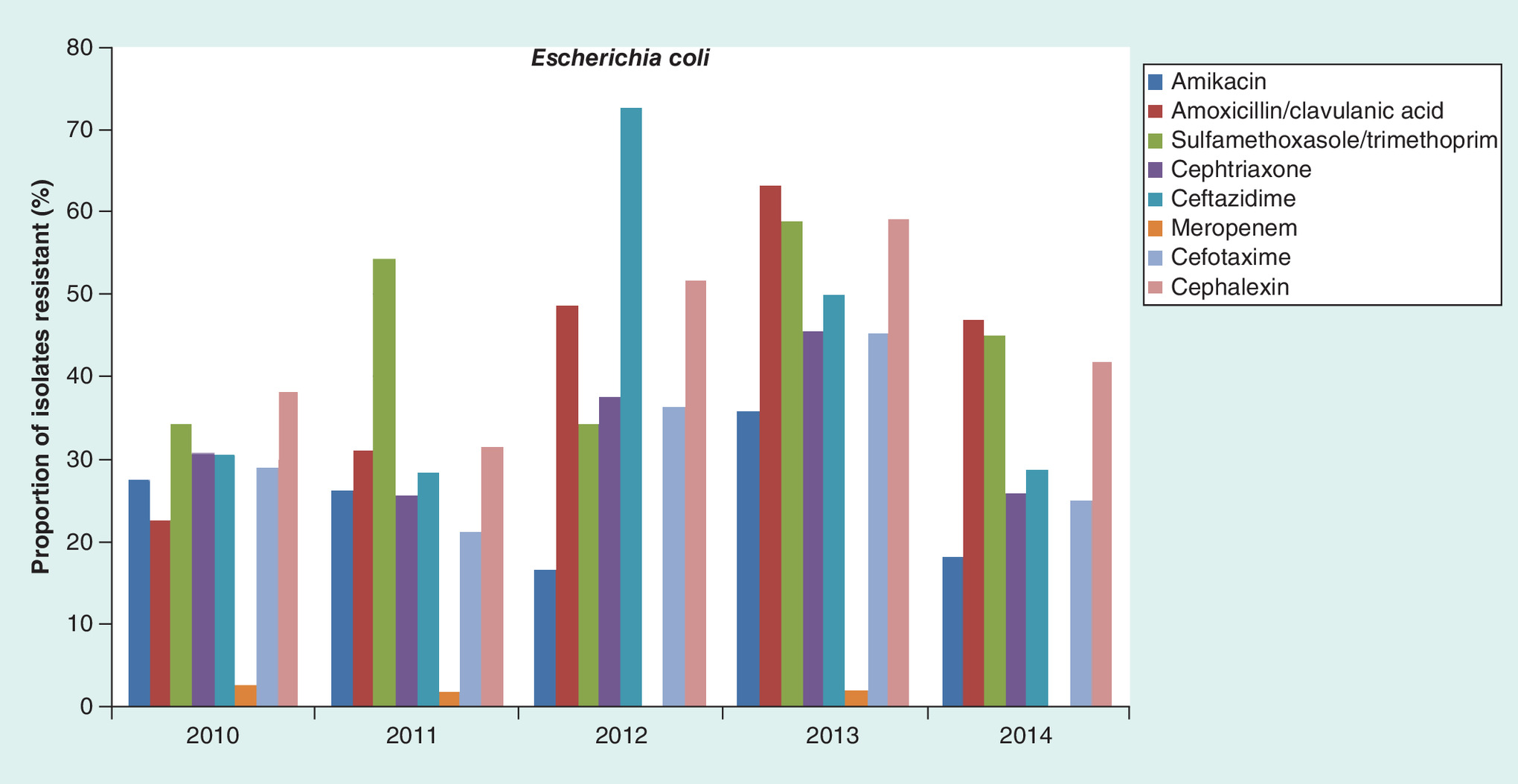
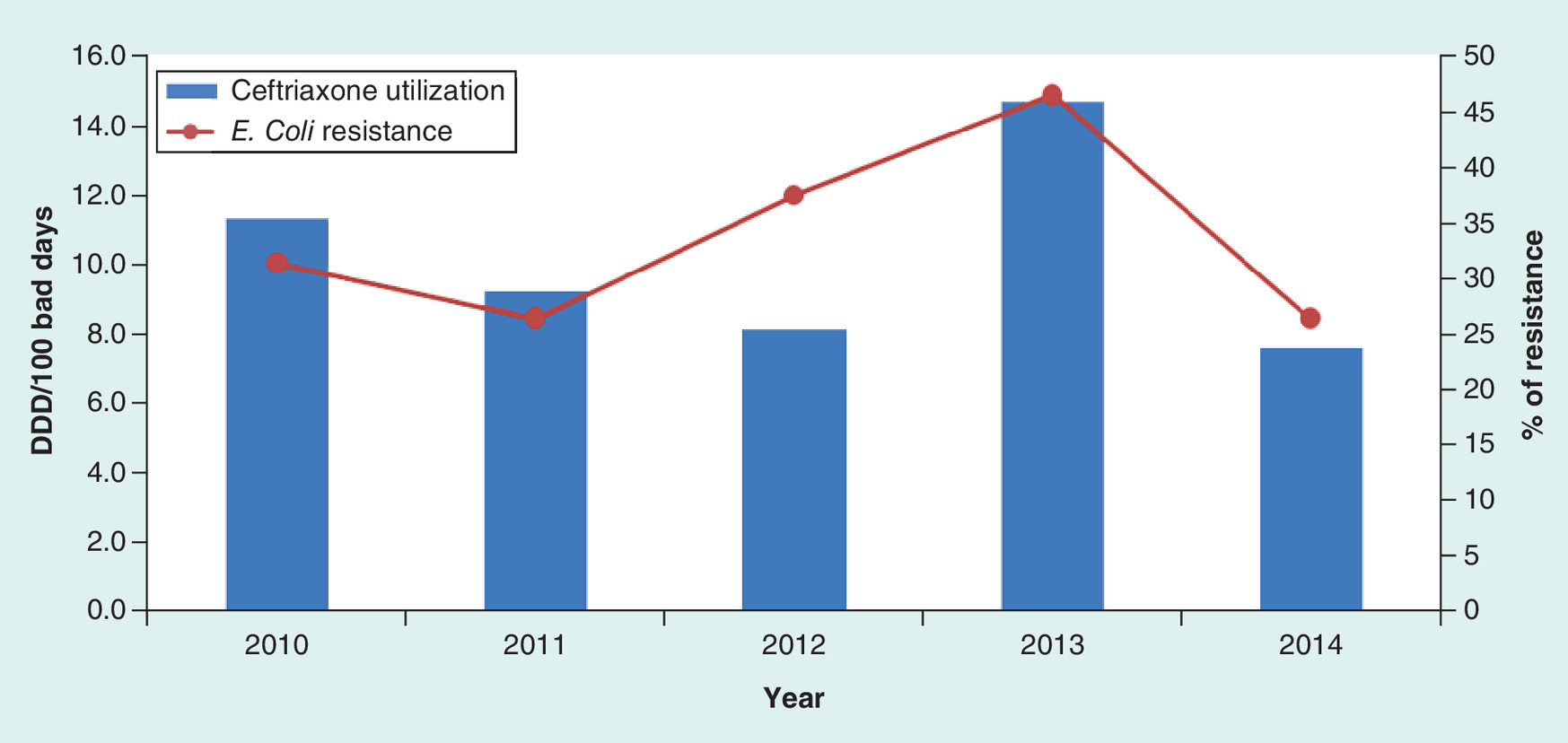
Figure 5. Trend analysis of ceftriaxone utilization and resistance pattern for Escherichia coli.
DDD: Defined daily dose.
The percentage of isolates that conferred resistance to amoxicillin and amoxicillin–clavulanic acid decreased from 30% in 2010 to 20% in 2014, and for ampicillin from 17 to 15%, respectively. The percentage of isolates that conferred resistance to ceftriaxone and cefotaxime increased to 13 and 15% in 2014 from 3% in 2010, respectively (Figure 3).
Regarding the most used antimicrobials tested, the proportion of erythromycin resistance varied from 40% in 2010/2011 to 51% in 2014. Erythromycin susceptibility predicts azithromycin susceptibility to S. pneumoniae. Clindamycin resistance varied from 55% in 2010/2011 to 59% in 2014. All isolates with exception of one were susceptible to vancomycin in 2014 (0.5%). Overall, 18% of S. pneumoniae at KC Kragujevac were resistant to penicillins.
According to CLSI recommended standards, CNS breakpoints were used for S. pneumoniae isolated from cerebrospinal fluid. During the study period, there were three isolates and all were susceptible to ceftriaxone and one was resistant to penicillin. Resistance to azithromycin was high throughout the study period (Figure 3). However, there is no obvious association between the extent of azithromycin use and antibiotic resistance patterns for S. pneumoniae.
Figure 4 shows the trend in resistance rate of E.coli to amikacin, amoxicillin–clavulanic acid, TMP–SMX, ceftriaxone, ceftazidime, cefotaxime, cephalexin and meropenem. The results of resistance rates for the other tested antimicrobials in 2014 were 66% for ampicillin, 55% for gentamicin, 52% for cefuroxime, 15% for cefepime, 7% ofloxacin, 5% nitrofurantoin and 0% for imipenem and ertapenem.
Extended-spectrum beta-lactamases (ESBL)-rates were estimated based on susceptibility to third-generation cephalosporins, such as ceftazidime. The rate of ESBL-producing E. coli did not appreciably change during the study period although there appeared to be a downward trend, that is, 30% in 2010 and 28% in 2014, respectively.
Cefazolin is a first-generation parenteral cephalosporin and an important choice for the treatment of acute urinary tract infection; however, its susceptibility is currently not routinely tested in the hospital. However, even for the cephalosporins that are routinely used in susceptibility tests, it is not possible to make a straightforward decision whether their use was justified and therefore whether they contributed to the observed resistance patterns. For example, without an insight in diagnoses of the patients, we could not decide about the relation between ceftriaxone and resistance rate shown in the Figure 5.
Cost data
The total costs per DDD typically decreased during the study period (Supplementary Tables 1 & 2). For example, the cost of ceftriaxone fell from 856 RSD/DDD in 2010 to 128 RSD/DDD in 2014, meropenem from 4475 in 2010 to 1970 RSD/DDD in 2014, and cefixime from 193 in 2010 to 134 RSD/DDD in 2014 (Table 1).
| No. | ATC | INN | Cost (RSD)/DDD |
|---|---|---|---|
| 1 | J01DH03 | Ertapenem | 5098 |
| 2 | J01GB01 | Tobramycin | 3993 |
| 3 | J01DH02 | Meropenem | 1970 |
| 4 | J01DD01 | Cefotaxime | 510 |
| 5 | J01GB06 | Amikacin | 436 |
| 6 | J01CA01 | Ampicillin | 254 |
| 7 | J01EE01 | Sulfamethoxazole and trimethoprim | 163 |
| 8 | J01DD08 | Cefixime | 134 |
| 9 | J01DD04 | Ceftriaxone | 128 |
| 10 | J01CR02 | Amoxicillin and enzyme inhibitor | 61 |
| 11 | J01FA10 | Azithromycin | 56 |
| 12 | J01DB01 | Cefalexin | 53 |
| 13 | J01CE30 | Benzylpenicillin procaine | 51 |
| 14 | J01FA09 | Clarithromycin | 32 |
| 15 | J01CA04 | Amoxicillin | 19 |
ATC: Anatomical therapeutic chemical; DDD: Defined daily dose; INN: International nonproprietary name.
Discussion
Developing effective antibiotic policies in hospitals depends on the surveillance of current resistance patterns, coupled with an understanding of current antibiotic utilization patterns, to guide empiric use while sensitivity analyses are being undertaken. Hence, it should become mandatory for hospitals to establish efficient surveillance systems along with monitoring current antibiotic utilization to improve their appropriate use. This can be helped by instigating measures, such as the WHONET Software program, to monitor local resistance patterns; however, we believe only one hospital in Serbia is currently using this program [37].
From the antibiotic DU90% profile in 2010 versus 2014, we can conclude that the cumulative antimicrobial resistance is similar and relatively high (Figures 1 & 2 & Supplementary Tables 1 & 2), with high cumulative resistance rates among the most widely used antibiotics from 2010.
Overall, total antibiotic use decreased appreciably from 2010 to 2014 (Supplementary Tables 1 & 2); however, there was high prescribing of the reserved antibiotic ceftriaxone. In addition, sensitivity tests were not available for 4 out of the 15 most commonly used antibiotics in 2014, pointing to a lack of integration between microbiology and routine clinical care in the hospital. We will now be reviewing this within the hospital to develop policies to improve future prescribing, and this will be part of future studies. This can also act as an exemplar for other hospitals in Serbia to improve future antibiotic prescribing.
One of the main findings of this study is the high resistance of S. pneumoniae to azithromycin (Figure 3). This maybe because there has been high total antibiotic consumption in Serbia versus other European countries in recent years [38]. In addition, antibiotic use among children in primary care in Serbia has been extremely high, with frequent prescribing for indications with little or no benefit from antibiotics such as upper respiratory tract infections [27]. This is important since previous antibiotic exposure in primary care is related to high antibiotic resistance in hospitals [39].
The debate continues in literature with regard to the impact of macrolide resistance on the outcome of pneumococcal pneumonia. Antibiotic-resistant strains increase the severity of illness and make it more difficult to treat these infections effectively. Several cases of macrolide treatment failure have been documented in the literature [40,41], and with high levels of macrolide resistance in this children's hospital, we believe these antibiotics should not be routinely used as empiric therapy of S. pneumoniae while AMR rates remain high. Probable reason for the increase in the resistance rate of azithromycin and amoxicillin in 2014, despite a decrease in their intrahospital use, is the extensive and unjustified prescribing of these antibiotics in primary care. On the other hand, the antibiotics used only in hospitals, such as ceftriaxone, had decreased both in usage and resistance rates. The main promoter of resistance to antibiotics is likely inappropriate use of these antibiotics in ambulatory care especially for wrong indications, which include potential viral infections, and this should be placed in focus in future interventions within the healthcare system in Serbia and other countries. A reasonable alternative to macrolides may be levofloxacin, which is already being used for the treatment of community-acquired pneumonia in children in clinical trials [42,43]. Although quinolones may have adverse effects on the cartilage of great joints in children, recent studies with long-term follow-up showed that this risk was overestimated and its use in hospitalized children with such serious infections as community-acquired pneumonia is justified [44]. Consequently, we have begun implementing this recommendation in this children's hospital, alongside educational and other measures, to reduce inappropriate macrolide use, and will be following this up in future studies to further guide prescribing in this and other similar hospitals in Serbia.
Additionally, the Ministry of Health in Serbia is now planning to introduce in a national immunization program – the pneumococcal conjugate vaccine – in all infants and young children. This may also be critical in reducing nasopharyngeal carriage and limiting the dissemination of drug-resistant strains [45–47]. We will also be monitoring this impact in the future.
Ramos et al. showed that the prevalence of resistance is country specific and reflects differences in the availability and consumption of antibiotics. In countries with a long tradition of surveillance programs such as Australia, Slovakia and Sweden, there have been reductions in the prescription and use of antibiotics [48]. In our study, ESBL-rate E. coli decreased with decreased antibiotic consumption in 2010 versus 2014; however, this was still high at 28% in 2014. For an antibiotic to be considered as first-line empirical treatment for urinary tract infections, resistance should not exceed 20% in the most likely infecting strains [49,50]. According to these criteria, all third generation cephalosporins used in our hospital are currently above this with reported resistance rates from 25 to 28% (Figure 5). The use of antimicrobials for which the uropathogen has shown resistance can lead to serious consequences [51], particularly for patients with pyelonephritis. Consequently, in this situation, healthcare providers should consider empiric treatment with carbapenem or amikacin or another agent found to be consistently active on the basis of the local antibiogram. This policy has again already been introduced into our hospital, and again we will be monitoring the situation to provide guidance to others.
Encouragingly, the rate of methicillin-resistant S. aureus among the pediatric population in KC Kragujevac is relatively low compared with reports from other countries [52], and it should be kept this way through the continuous monitoring of local S. aureus susceptibility patterns.
Since cloxacillin must be administered frequently (i.e., four-times daily in children), and cloxacillin is sometimes associated with severe phlebitis, cefazolin is a reasonable substitute for the empiric management of bacteremia with methicillin-sensitive S. aureus. With such high levels of resistance in our hospital, clindamycin should only be used for infections caused by methicillin-sensitive S. aureus if the sensitivity of an isolate was confirmed, and the D-test for erythromycin-induced resistance was negative. Such recommendations have also now been introduced in our hospital.
In recent years, the costs of antibiotics have been falling. This can be partially explained by a reform in the procurement system for hospital medicines in Serbia. Until 2013, Serbia had a system whereby each hospital procured their own medicines individually, choosing their own suppliers and brands for medicines to address particular diseases. Rather than competing on price, suppliers typically competed on the level of ‘rebate’ offered to a hospital to increase the monies available to the hospital to purchase other goods and services. These rebates were often as much as a third of the total purchase price. The new procurement system was introduced in 2014 to address this leading to central procurement and an appreciable drop in prices such as prices for ceftriaxone (Table 1) [32].
We acknowledge that there are typically a low number of tissue specimens analyzed in Serbian hospital, which may have influenced interpretation of the results. General limitations of DDDs are common for all aggregated data, exacerbated in the case of pediatric patients. This together with and the limitations of the aggregate microbiology data are described by Goryachkina et al. [26]. Calculations of costs and DU in children based on adult DDDs can also not be used for estimates of prevalence, so the only aspects we could follow were time trends and comparisons between the groups. Despite these limitations, we believe our findings are robust and are already influencing prescribing in this hospital and wider.
Conclusion & recommendations
Overall, we believe our findings show that increased local efforts to enhance surveillance for AMR are necessary to inform treatment decisions, especially empiric use. The approach to local infection control should be multifaceted and should include microbiology and utilization assessments together with measures to improve local hygiene such as improved hand-hygiene in wards [53–56]. The development of pro-active AS programs is a way forward [13–15,29,57–61] as well as consulting microbiologists and clinical pharmacologists when prescribing antibiotics for complex clinical cases [62]. Furthermore, joint efforts should be made to enhance appropriate antibiotic prescribing and dispensing in all primary, secondary and tertiary care settings in Serbia which treat children. This again will be the subject of future research projects together with increasing efforts in Serbia to reduce the illegal purchase of antibiotics in Serbia [38] as well as improve physician education surrounding antibiotic use.
Finally, we hope this original research in Serbia has implications for other central and eastern European countries struggling to enhance their appropriate use of antibiotics.
The appropriate use of antibiotics especially in children is of growing importance given the extent of antibiotic resistance across countries including Serbia and the lack of new antibiotics.
Knowledge of current antibiotic utilization patterns coupled with knowledge regarding current resistance rates is essential to improve the empiric use of antibiotics and reduce future antimicrobial resistance rates across sectors including hospitals.
Effective antibiotic guidance can be developed by combining an analysis of antibiotic utilization and resistance patterns even in countries with limited resources, and lead to changes in the future empiric use of antibiotics and subsequent changes in resistance rates.
Reserving antibiotics through formal guidelines can help control their use, especially if prior authorization schemes are in place in hospitals. However, this needs to be followed up with education and other initiatives to improve future use.
Appropriate use of antibiotics coupled with changes in pricing policies can appreciably reduce their costs benefitting all key stakeholder groups.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Acknowledgements
All authors have been active participants in the research. We would like to thank R Kuzmanovic for IT support regarding microbial resistance data.
Financial & competing interests disclosure
The write-up of the paper was in part supported by a grant from the Karolinska. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
File (suppl_tables.docx)
- Download
- 96.93 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Her Majesty's Government. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. www.jpiamr.eu/wp-content/uploads/2014/12/AMR-Review-Paper-Tackling-a-crisis-for-the-health-and-wealth-of-nations_1–2.pdf
2.
Rezal RS, Hassali MA, Alrasheedy AA et al. Physicians’ knowledge, perceptions and behaviour towards antibiotic prescribing: a systematic review of the literature. Expert Rev. Anti-Infect. Ther. 13(5), 665–680 (2015).
• Good review paper discussing physicians’ knowledge and attitudes toward antibiotics.
3.
Laxminarayan R, Matsoso P, Pant S et al. Access to effective antimicrobials: a worldwide challenge. Lancet 387(10014), 168–175 (2016).
4.
Loeffler JM, Garbino J, Lew D et al. Antibiotic consumption, bacterial resistance and their correlation in a Swiss university hospital and its adult intensive care units. Scand. J. Infect. Dis. 35(11–12), 843–850 (2003).
5.
Frank U, Kleissle EM, Daschner FD et al. Multicentre study of antimicrobial resistance and antibiotic consumption among 6780 patients with bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 25(12), 815–817 (2006).
6.
Gandra S, Barter DM, Laxminarayan R. Economic burden of antibiotic resistance: how much do we really know? Clin. Microbiol. Infect. 20(10), 973–980 (2014).
7.
Oxford J, Kozlov R. Antibiotic resistance – a call to arms for primary healthcare providers. Int. J. Clin. Pract. Suppl. 180, 1–3 (2013).
8.
Laxminarayan R, Heymann DL. Challenges of drug resistance in the developing world. Brit. Med. J. 344, e1567 (2012).
9.
Earnshaw S, Mendez A, Monnet DL et al. Global collaboration to encourage prudent antibiotic use. Lancet Infect. Dis. 13(12), 1003–1004 (2013).
10.
Ganguly NK, Arora NK, Chandy SJ et al. Rationalizing antibiotic use to limit antibiotic resistance in India. Indian J. Med. Res. 134, 281–294 (2011).
11.
Laxminarayan R, Duse A, Wattal C et al. Antibiotic resistance – the need for global solutions. Lancet Infect. Dis. 13(12), 1057–1098 (2013).
12.
GRIPP. The Global Respiratory Infection Partnership. www.grip-initiative.org/about-the-partnership/partnerships-mission/the-grip-declaration/
13.
Baur D, Gladstone BP, Burkert F et al. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect. Dis. 17(9), 990–1001 (2017).
• Good paper outlining the impact of a recent antibiotic stewardship program.
14.
Hulscher M, Prins JM. Antibiotic stewardship: does it work in hospital practice? A review of the evidence base. Clin. Microbiol. Infect. 23(11), 799–805 (2017).
• Good paper outlining antibiotic stwardship programs in practice in hospitals.
15.
Dyar OJ, Huttner B, Schouten J, Pulcini C. What is antimicrobial stewardship? Clin. Microbiol. Infect. 23(11), 793–798 (2017).
16.
Official Gazette of the Republic of Serbia. Rulebook of the criteria, manner and procedure for listing/delisting of reimbursement medicines in/from the list of medicines prescribed and dispensed under the compulsory health insurance coverage. No: 65/15, 71/15, 104/15.
17.
Official Gazette of the Republic of Serbia. Rulebook of the criteria, manner and procedure for listing/delisting of reimbursement medicines in/from the list of medicines prescribed and dispensed under the compulsory health insurance coverage. Nos: 24/16, 57/16, 61/16.
18.
Official Gazette of the Republic Serbia, No 12/2016.
19.
Official Gazette of the Republic Serbia, No 101/13.
20.
WHO Collaborating Centre for Drug statistics Methodology. Guidelines for ATC classification and DDD assignment (2015). www.whocc.no/filearchive/publications/2015_guidelines.pdf
21.
Versporten A, Bolokhovets G, Ghazaryan L et al. Antibiotic use in eastern Europe: a cross-national database study in coordination with the WHO Regional Office for Europe. Lancet Infect. Dis. 14(5), 381–387 (2014).
22.
Furst J, Cizman M, Mrak J et al. The influence of a sustained multifaceted approach to improve antibiotic prescribing in Slovenia during the past decade: findings and implications. Expert Rev. Anti-Infect. Ther. 13(2), 279–289 (2015).
23.
Bergman U, Risinggard H, Vlahovic-Palcevski V, Ericsson O. Use of antibiotics at hospitals in Stockholm: a benchmarking project using internet. Pharmacoepidemiol. Drug Saf. 13(7), 465–471 (2004).
24.
Vlahovic-Palcevski V, Gantumur M, Radosevic N et al. Coping with changes in the defined daily dose in a longitudinal drug consumption database. Pharmacy World Sci. 32(2), 125–129 (2010).
25.
WHO Collaborating Centre for Drug Statistics Methodology, Guidelines for ATC classification and DDD assignment 2016. Oslo, Norway (2016). www.whocc.no/filearchive/publications/2017_guidelines_web.pdf
26.
Goryachkina K, Babak S, Burbello A et al. Quality use of medicines: a new method of combining antibiotic consumption and sensitivity data-application in a Russian hospital. Pharmacoepidemiol. Drug Saf. 17, 636–644 (2008).
•• Good paper outlining a new methodology to review utilization patterns alongside resistance patterns to guide future care.
27.
Bozic B. Use of antibiotics in paediatric primary care settings in Serbia. Arch. Dis. Child. 100(10), 966–999 (2015).
•• Landmark paper in Serbia discussing antibiotic use in this important patient population.
28.
Cox JA, Vlieghe E, Mendelson M et al. Antibiotic stewardship in low-and middle-income countries: ‘same, but different’?Clin. Microbiol. Infect. 23(11), 812–818 (2017).
29.
Pulcini C. Antibiotic stewardship: update and perspectives. Clin. Microbiol. Infect. 23(11), 791–792 (2017).
30.
Araujo da Silva AR, Albernaz de Almeida Dias DC, Marques AF et al. The role of antimicrobial stewardship programmes in children: a systematic review. J. Hosp. Infect. (2017) (Epub ahead of print).
31.
Clinical and Laboratory Standards Institute. Performance standards for antimicrobial disk susceptibility tests. Document M2-A9. Wayne, PA: CLSI; 20010.
32.
33.
Chitnis A, Wang R, Sun SX et al. Impact of initiation of asenapine on patterns of utilization and cost of healthcare resources associated with the treatment of bipolar I disorder. J. Med. Econ. 18(11), 863–870 (2015).
34.
Godman B, Petzold M, Bennett K et al. Can authorities appreciably enhance the prescribing of oral generic risperidone to conserve resources?: Findings from across Europe and their implications. BMC Med. 12, 98 (2014).
35.
Moon JC, Godman B, Petzold M et al. Different initiatives across Europe to enhance losartan utilization post generics: impact and implications. Front. Pharmacol. 5, 219 (2014).
36.
Schito GC, Georgopoulos A, Prieto J. Antibacterial activity of oral antibiotics against community-acquired respiratory pathogens from three European countries. J. Antimicrob. Chemother. 50(Suppl.), 7–11 (2002).
37.
38.
Kalaba M, Bajcetic M, Sipetic T et al. High rate of self purchasing of oral antibiotics in Serbia: implications for future policies. PPRI Vienna (2011). http://whocc.goeg.at/Downloads/Conference2011/PraesentationenPPRIKonferenz/general_PPRI%20conference%202011%20Abstract%20book.pdf
39.
Costelloe C, Metcalfe C, Lovering A et al. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. Brit. Med. J. 340, c2096 (2010).
•• Interesting paper discussing prescribing and resistance patterns in ambulatory care.
40.
Musher D, Dowell M, Shortridge VD et al. Emergence of macrolide resistance during treatment of pneumococcal pneumonia. N. Engl. J. Med. 346, 630–631 (2002).
41.
Van Kerkhoven D, Peetermans WE, Verbsit L, Verhaegen J. Breakthrough pneumococcal becteraemia in patients treated with clarithromycin or oral β-lactams. J. Antimicrob. Chemother. 51, 691–696 (2003).
42.
Bradley JS, Arguedas A, Blumer JL et al. Comparative study of levofloxacin in the treatment of children with community-acquired pneumonia. Pediatr. Infect. Dis. J. 26(10), 868–878 (2007).
43.
Kabra SK, Lodha R, Pandey RM. Antibiotics for community-acquired pneumonia in children. Cochrane Database Syst. Rev. (3), CD004874 (2010).
44.
Bradley JS, Kauffman RE, Balis DA et al. Assessment of musculoskeletal toxicity 5 years after therapy with levofloxacin. Pediatrics 134(1), E146–E153 (2014).
45.
Escola, Kilpi T, Palmu A et al. Efficacy of a pneumococcal conjugate vaccine against otitis media. N. Engl. J. Med. 344, 403–409 (2001).
46.
Mbelle N, Huebner RE, Wasas AD et al. Immunogenicity and impact on nasopharyngeal carriage of nonvalent pneumococcal conjugate vaccine. J. Infect. Dis. 180, 1171–1176 (1999).
47.
Black S, Shinefield H, Fireman D. Efficacy, safety and immunogenocity of heptavalent pneumococcal conjugate vaccine in children. Pediatr. Infect. Dis. J. 19, 187–115 (2000).
48.
Ramos NL, Dzung DT, Stopsack K et al. Characterisation of uropathogenic Escherichia coli from children with urinary tract infections in different countries. Eur. J. Clin. Microbial. Infect. Dis. 30, 1587–1593 (2011).
•• Landmark paper in this population to provide guidance on future care.
49.
Gupta K, Hooton TM, Naber KG et al. Infectious Diseases Society of America European Society for Microbiology and Infectious Diseases. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 52, E103–E120 (2011).
50.
Bryce A, Hay AJ, Lane I et al. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: systematic review and meta-analysis. Brit. Med. J. 352, i939 (2016).
51.
Lee S, Song Y, Cho SH, Kwon KT. Impact of extended-spectrum beta-lactamase on acute pyelonephritis treated with empirical ceftriaxone. Microb. Drug Resist. 20, 39–44 (2014).
• Well-conducted research discussing empiric use of ceftriaxone in this patient population.
52.
Herigon JC, Hersh AL, Gerber JS et al. Antibiotic management of Staphylococcus aureus infections in US Children's hospitals, 1999–2008. Pediatrics 125(6), e1294–e1300 (2010).
53.
Freeman J, Dawson L, Jowitt D et al. The impact of the Hand Hygiene New Zealand programme on hand hygiene practices in New Zealand's public hospitals. NZ Med. J. 129, 67–76 (2016).
54.
Hansen S, Zingg W, Ahmad R et al. Organization of infection control in European hospitals. J. Hosp. Infect. 91, 338–345 (2015).
55.
Storr JA, Engineer C, Allan V. Save lives: clean your hands: a WHO patient safety initiative for 2009. World Hosp. Health Serv. 45, 23–25 (2009).
56.
Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 5, 229–241 (2014).
57.
Viale P, Tumietto F, Giannella M et al. Impact of a hospital-wide multifaceted programme for reducing carbapenem-resistant Enterobacteriaceae infections in a large teaching hospital in northern Italy. Clin. Microbiol. Infect. 21, 242–247 (2015).
58.
Rocha-Pereira N, Lafferty N, Nathwani D. Educating healthcare professionals in antimicrobial stewardship: can online-learning solutions help? J. Antimicrob. Chemother. 70, 3175–3177 (2015).
59.
Zhang YZ, Singh S. Antibiotic stewardship programmes in intensive care units: why, how, and where are they leading us. World J. Crit. Care Med. 4, 13–28 (2015).
60.
Pollack LA, Srinivasan A. Core elements of hospital antibiotic stewardship programs from the Centers for Disease Control and Prevention. Clin. Infect. Dis. 59(Suppl. 3), S97–S100 (2014).
61.
Goff DA, Mendelson M. Antibiotic stewardship hits a home run for patients. Lancet Infect. Dis. 17(9), 892–893 (2017).
62.
Jankovic SM, Milovanovic D, RuzicZecevic D et al. Consulting clinical pharmacologist about treatment of inpatients in a tertiary hospital in Serbia. Eur. J. Clin. Pharmacol. 72(12), 1541–1543 (2016).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 21 July 2017
Accepted: 26 October 2017
Published online: 21 February 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Experience with developing antibiotic stewardship programs in Serbia: potential model for other Balkan countries?. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0055
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Indrė Trečiokienė, ClaudiaGarciaSerpa Osorio‐de‐Castro, Aggregate‐level drug utilization analyses, Drug Utilization Research, 10.1002/9781119911685.ch14, (148-157), (2024).
- Ummara Altaf, Zikria Saleem, Muhammad Akhtar, Waleed Altowayan, Abdulmajeed Alqasoumi, Mohammed Alshammari, Abdul Haseeb, Fahad Raees, Mohammad Imam, Narjis Batool, Muhammad Akhtar, Brian Godman, Using Culture Sensitivity Reports to Optimize Antimicrobial Therapy: Findings and Implications of Antimicrobial Stewardship Activity in a Hospital in Pakistan, Medicina, 10.3390/medicina59071237, 59, 7, (1237), (2023).
- Yara-Natalie Abo, Bridget Freyne, Diana Kululanga, Penelope A. Bryant, The Impact of Antimicrobial Stewardship in Children in Low- and Middle-income Countries, Pediatric Infectious Disease Journal, 10.1097/INF.0000000000003317, 41, 3S, (S10-S17), (2022).
- PP Skosana, N Schellack, B Godman, A Kurdi, M Bennie, D Kruger, JC Meyer, A point prevalence survey of antimicrobial utilisation patterns and quality indices amongst hospitals in South Africa; findings and implications, Expert Review of Anti-infective Therapy, 10.1080/14787210.2021.1898946, 19, 10, (1353-1366), (2021).
- Zorana Kovacevic, Bojan Blagojevic, Jelena Suran, Olga Horvat, Mapping knowledge and comprehension of antimicrobial stewardship and biosecurity among veterinary students, PLOS ONE, 10.1371/journal.pone.0235866, 15, 8, (e0235866), (2020).
- Olga Horvat, Ana Tomas, Milica Paut Kusturica, Dragica Bukumiric, Bojan Blagojevic, Zorana Kovacevic, Serbian students’ knowledge, attitudes and behaviour towards antibiotic use: is there room for improvement?, International Journal of Public Health, 10.1007/s00038-020-01448-6, 65, 8, (1257-1267), (2020).
- Zikria Saleem, Mohamed Azmi Hassali, Brian Godman, Ann Versporten, Furqan Khurshid Hashmi, Hamid Saeed, Fahad Saleem, Muhammad Salman, Inayat Ur Rehman, Tahir Mehmood Khan, Point prevalence surveys of antimicrobial use: a systematic review and the implications, Expert Review of Anti-infective Therapy, 10.1080/14787210.2020.1767593, 18, 9, (897-910), (2020).
- Radmila Popović, Zdenko Tomić, Ana Tomas, Nada Anđelić, Sanja Vicković, Gordana Jovanović, Dragica Bukumirić, Olga Horvat, Ana Sabo, Five-year surveillance and correlation of antibiotic consumption and resistance of Gram-negative bacteria at an intensive care unit in Serbia, Journal of Chemotherapy, 10.1080/1120009X.2020.1755588, 32, 6, (294-303), (2020).
- Jane Robertson, Kotoji Iwamoto, Iris Hoxha, Lilit Ghazaryan, Vafa Abilova, Ana Cvijanovic, Halina Pyshnik, Marina Darakhvelidze, Larissa Makalkina, Arianit Jakupi, Aigul Dzhakubekova, Angela Carp, Lidija Cizmovic, Svetlana Rachina, Vesela Radonjic, Salomudin Yusufi, Mesil Aksoy, Muhabbat Ibragimova, Brian Godman, Hans Kluge, Hanne Bak Pedersen, Antimicrobial Medicines Consumption in Eastern Europeand Central Asia – An Updated Cross-National Study and Assessment of QuantitativeMetrics for Policy Action, Frontiers in Pharmacology, 10.3389/fphar.2018.01156, 9, (2019).