Comparative effectiveness of surgery versus antibiotics in acute appendicitis: a systematic review
Abstract
Aim: To review outcomes of surgical and antibiotic management of acute appendicitis. Methods: 11 prospective studies comparing surgical versus antibiotic management of acute appendicitis over a 21-year period were reviewed. Results: Antibiotic management is successful in most cases of uncomplicated acute appendicitis. The need for crossover in management and recurrent appendicitis were low among all studies. For those patients who ultimately required surgery, no increased complications were observed. Conclusion: The decision to use antibiotics to treat acute appendicitis should be held to the same standards of diagnostic rigor as surgical management. Antibiotics may be safely recommended in patients with high surgical risk, such as the elderly or those with multiple comorbidities.
First draft submitted: 8 March 2017; Accepted for publication: 30 April 2017; Published online: 12 July 2017
Acute appendicitis is the most common urgent surgical diagnosis with an estimated lifetime incidence between 7 and 14% [1]. Within the USA, roughly 300,000 individuals undergo appendectomy annually [1,2]. Traditionally, it was thought that delayed time from presentation to surgery in patients with acute appendicitis led to an increased risk of perforation [1–3]. However, others have found no association between perforation and in-hospital time prior to surgery. Rather, perforation is more likely to be related to progression of disease in the prehospital interval, and is generally independent of in-hospital time [4]. In recent years, clinicians and researchers have challenged the notion that appendicitis must be managed surgically. Numerous studies have been conducted to evaluate the role of antibiotics in the management of acute appendicitis. Most of them have shown that appendectomy may not be necessary in the majority of patients with acute uncomplicated appendicitis [3,5–14].
This is an important consideration, because all the patients who undergo operations are subject to risks of potential intraoperative and postoperative complications, regardless of how ‘minor’ the operation may be. Although appendectomy carries a low 30-day mortality rate of 0.1% for laparoscopic appendectomy to 0.3% for open appendectomy [15], postoperative complications, such as abscess, hematoma/bleeding, wound infection and bowel injury, occur at a rate of 2–23% [7,16]. Approximately, 3% of appendectomy patients require admission for bowel obstruction within 10 years [7]. Moreover, some patients undergo ‘nontherapeutic’ operations when they are incorrectly diagnosed with appendicitis: these so-called ‘negative appendectomies’ (NA) have been estimated to occur in 15–30% [3–4,17] of appendectomies, though data conclusively show that modern diagnostic imaging capabilities can dramatically reduce the rate of misdiagnosis [17]. Patients at the greatest risk of bowel obstruction after appendectomy are those with perforated appendicitis, NA, advanced age and other comorbid conditions. Patients with NA were 5.4-times more likely to develop a bowel obstruction within a 30-year period in a study by Andersson [18], and NA has also been associated with longer length of stay (LOS), increased total hospital charges, higher case fatality rate and increased risk of postoperative infectious complications [19].
The first prospective study to evaluate the role of antibiotics as definitive management of acute appendicitis was conducted by Eriksson and Granström [8] between 1992 and 1994. Since that time, there have been numerous trials and observational studies designed to further investigate this question [3,5–14]. In USA, few prospective studies have been conducted to evaluate nonoperative management of acute appendicitis, and surgery is largely still considered the gold standard treatment for this condition. The aim of this review is to help clinicians and patients make informed and evidence-based decisions when considering an operative versus antibiotic therapy in acute appendicitis as well as to identify current gaps in relevant metrics that are important to providers and patients.
Methods
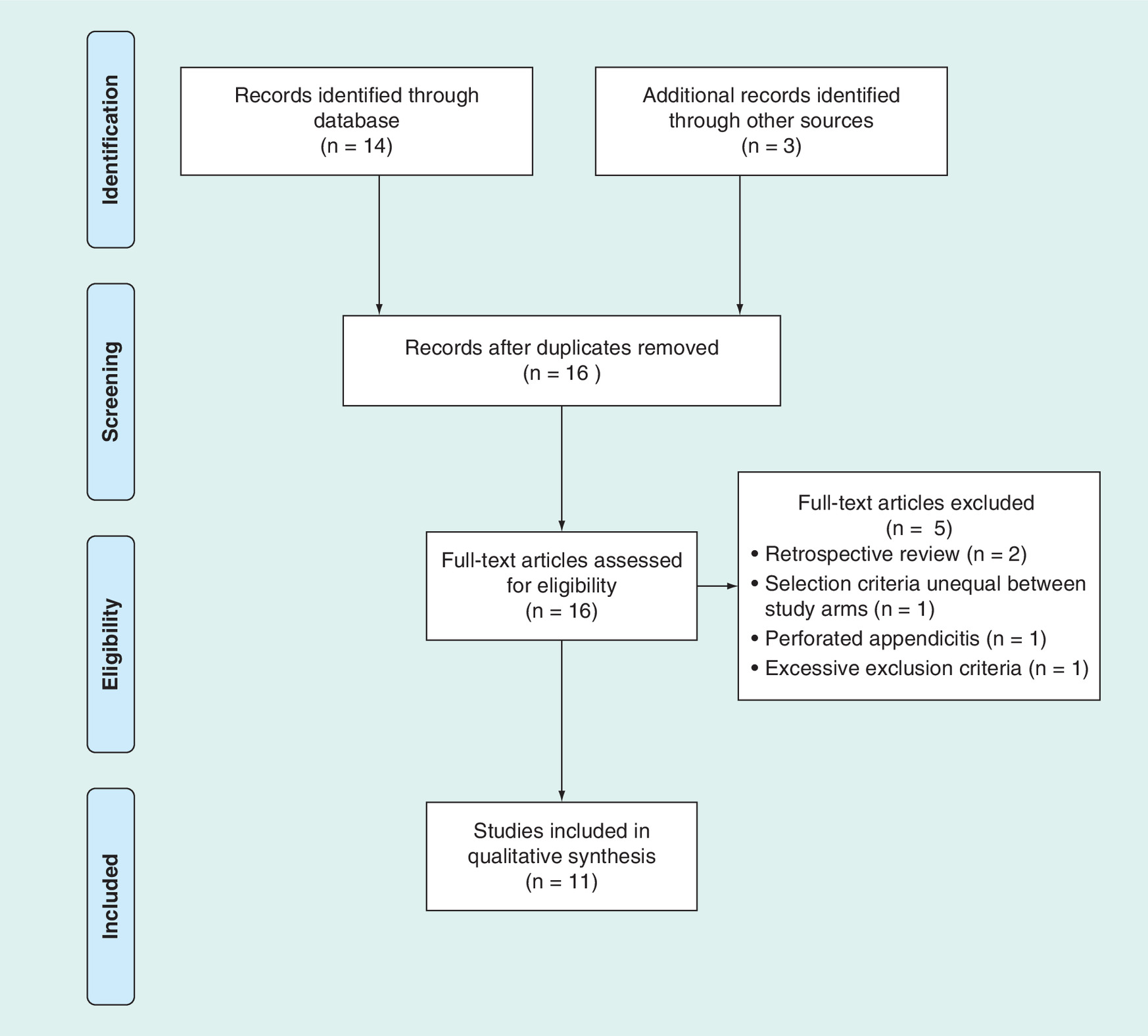
PubMed was used to conduct a review of all prospective studies and trials that compared operative and antibiotic management of acute appendicitis. Search terms included ‘appendectomy’, ‘appendicitis’, ‘antibiotic’ and ‘nonoperative’. Systematic reviews and meta-analyses were excluded although they were cross-referenced to identify additional studies that may have been missed during the initial search. The references included in the prospective studies were also cross-referenced to ensure that no pertinent studies were missed by the PubMed search strategy. The search was restricted to English-language studies. Our search strategy was developed and is presented in Figure 1 according to the PRISMA format [20].
Both pediatric and adult cohorts were eligible for inclusion. Additionally, enrollment criteria were required to be identical for surgical and antibiotic arms. For example, there was at least one study in which patients were included in the antibiotics arm if their diagnosis of appendicitis was not certain and those who were placed in the surgery arm were those with a more definitive diagnosis; this study was excluded from our review. Additionally, one study was excluded from our analysis due to overly stringent exclusion criteria that would not allow applicability to the general patient population.
Study characteristics and outcomes of interest were inclusion and exclusion criteria, antibiotic regimen, use of diagnostic imaging, use of laparoscopic approach, crossover from antibiotic to surgical management arm during index admission, appendicitis recurrence among antibiotic-managed subjects, final pathology, LOS, time away from work or school and complications. Cost ratios were used to compare surgery with antibiotic management without the need to convert currencies or account for inflation over a 21-year period.
Results
11 studies conducted from 1995 to 2016 were eligible for inclusion (Table 1). Study design varied among the selections; there were four randomized controlled trials, two prospective controlled trials, three nonrandomized controlled trials, one prospective observational study and one prospective patient choice study. Study population size ranged from 40 to 530. 40% were conducted as multicenter trials. Two studies included only pediatric patients [11,12] and one exclusively included men [9]. Seven studies were conducted in Europe, two in Asia and two in the USA (both included only pediatric patients).
| Study | Year | Type of study | Age group | Country | Number of patients | Imaging | Laparoscopic rate | Follow-up interval | Ref. | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author | Surgery | Antibiotics | Total | ||||||||
| Eriksson | 1995 | Prospective controlled | 18–75 | Sweden | 20 | 20 | 40 | Ultrasound | – | 1 year | [8] |
| Styrud | 2006 | Randomized controlled trial | 18–50 | Sweden | 124 | 128 | 252 | Not specified | 6% | 1 year | [9] |
| Hansson | 2009 | Prospective controlled | ≥18 | Sweden | 169† | 202† | 369 | Not required for diagnosis | – | 1 year | [6] |
| Turhan | 2009 | Nonrandomized clinical trial | Not specified | Turkey | 183 | 107 | 290 | Ultrasound/CT | 18.00% | 1 year | [5] |
| Malik | 2009 | Randomized controlled trial | 17–64 | India | 40 | 40 | 80 | Ultrasound | – | 1 year | [10] |
| Vons | 2011 | Randomized controlled trial | 18–68 | France | 120† | 123† | 243 | CT | 65.64% | 1 year | [7] |
| DiSaverio | 2014 | Single cohort, prospective observational | >14 | Italy | 0 | 159 | 159 | Ultrasound/CT | – | 2 years | [3] |
| Minneci | 2014 | Nonrandomized clinical trial | 7–17 | USA | 47 | 30 | 77 | Ultrasound/CT | 100% | 30 Days | [11] |
| Park | 2014 | Prospective nonrandomized | ≥18 | Republic of Korea | 159 | 119 | 278 | Ultrasound/CT | 98% | 30 Days | [14] |
| Salminen | 2015 | Randomized controlled trial | 18–60 | Finland | 273 | 257 | 530 | CT | 5.50% | 1 year | [13] |
| Minneci | 2016 | Prospective patient choice | 7–17 | USA | 65 | 37 | 102 | Ultrasound/CT | 100% | 1 year | [12] |
†Indicates intention to treat.
CT: Computed tomography.
Inclusion & exclusion criteria
To be included in this review, studies had to require the same diagnostic certainty for all the patients eligible for inclusion in either treatment arm. This should lead to similar rates of acute appendicitis, complicated appendicitis and misdiagnosis between operative and nonoperative groups [9]. All studies required basic history and physical exam findings to identify possible appendicitis. Lab values, including WBC and CRP were reported by most studies. The study design for Hansson et al. [6] included a deliberate attempt not to establish requirements for diagnosis; however, patient history, physical exam, laboratory tests and imaging results were used according to established clinical practice. The authors explained that they chose to not require imaging in the diagnostic criteria to reduce additional testing costs [6].
Exclusion criteria were not discussed in 27.3% of the reviewed studies [5,6,9]. The majority of studies excluded patients with peritonitis or suspicion of perforation [3,7–9,11–13]. Histories of chronic intermittent abdominal pain or inflammatory bowel disease were also exclusion criteria in five studies [3,7,11–13]. Recent antibiotic use [7] and allergy to study antibiotics [3,7,9] were also the exclusion criteria in some studies.
Diagnostic criteria
It is known that imaging can improve the diagnostic accuracy of acute appendicitis [8,9,17]. Improvements in diagnostic imaging technology quality and availability allow for improved preoperative diagnosis and characterization of the severity of appendicitis, which can direct patient care [11]. The choice of diagnostic imaging technique varied among studies and was not explicitly required in two studies [6,9]. For the remainder of the studies, ultrasound and/or computed tomography (CT) were used to confirm the diagnosis of appendicitis and to identify perforation, phlegmon or the presence of fecalith. CT scan was explicitly required by Vons et al. [7] and Salminen et al. [13] and was conducted after patient consent was obtained in the former. It is known that the use of CT scan reduces the number of NA [4,21,22]. However the number of patients imaged by each modality is not provided to allow us to evaluate a difference in imaging preference and its effect on outcomes [3,5,11,12,14].
The modified Alvarado score was used as a diagnostic criterion in two studies. However, one study did not specify a cut-off score [9] and the other used a cut-off score of 5, which is ‘equivocal for acute appendicitis’ [3]. The use of such a scoring system can help to guide the physicians in the identification of those with probable (score: 8–9) and highly probable (score: >9) acute appendicitis for treatment [23,24]. A study conducted by Farhnak and Talaei-Khoei [25] was excluded from our review because the Alvarado score was used to stratify patients into treatment arms. Patients with Alvarado score: 5–7 were treated with antibiotics and observation and those with score: 8–10 were surgically managed. While this might be a means of reducing the rate of NA, it does not ensure a high rate of diagnostic accuracy for the antibiotic group [25].
Treatment arms
Antibiotics regimens included one, two or three antibiotics. Duration of mandatory inpatient antibiotic management varied among studies from 0 to 2 days. The majority of protocols required a 1–2-day inpatient stay with intravenous antibiotics and transition to oral antibiotics prior to discharge [5,6,8,9,11–14]. Vons et al. [7] allowed patients to begin treatment with oral antibiotics if tolerated and DiSaverio et al. [3] discharged patients from the emergency department with oral antibiotics. Subjects were monitored as inpatients to observe failure of primary antibiotic therapy in 90.1% of studies [3,5–14]. Patients were discharged from the hospital when patients’ condition improved and oral antibiotics and diet were tolerated. Outpatient antibiotic regimens consisted of one to two antibiotics for total treatment duration of 4–10 days.
Patients within the operative management arms underwent surgery within 24 h of admission for all the studies. Use of laparoscopy ranged from 5.5 to 100% among studies that reported this operative modality [5,7,9,11–14]. Discrepancy in operative approach among studies likely relates both to difference in time periods and the countries in which the studies were conducted. Postoperative discharge criteria were not explicitly stated in the majority of studies evaluated.
Crossover
For the purpose of our review, we have defined crossover patients as those patients who were initially assigned to antibiotic management yet required surgery during the index admission (or in the case of discharge from the emergency department, within the first 5 days as was the definition for DiSaverio et al. [3]). Among the studies included in this review, crossover did not necessarily indicate early failure of antibiotic management, because crossover to surgery could occur for a variety of reasons (patient choice, surgeon discretion and misdiagnosis of disease severity on presentation, among others).
Crossover rates ranged from 5 to 47.5% (Table 2). While the majority of patients required crossover for failure to improve with antibiotic management, there were additional reasons for patients to change treatment arms within the index admission. Two studies cited patients’ desire for surgery as a reason for crossover [5,6]. The crossover rate from primary antibiotics management to primary surgical management for Hansson et al. [6] was the highest at 47.5%. Within this study, patients were allowed to change study arms on request. Among all the study patients, the authors reported that 30.3% of patients preferred a different treatment than what they were assigned; this included 12.9% of patients assigned to primary antibiotic management. Although the authors reported a primary failure rate of antibiotic therapy as 9.2%, they also noted that surgeons made the decision to crossover to surgery in 31.6% of patients originally randomized to antibiotics. Due to this ambiguity, we allocated these 31.6% of patients who underwent surgery during the index admission to the crossover group. One solution to the problem faced by Hansson et al. [6], is a prospective patient choice design [11,12]. Minneci et al. used this study design for both pilot and then a larger study in pediatric patients. Patient and family satisfaction was high among both surgical and antibiotic management groups in each study, which the authors attributed to the positive benefits of active patient involvement in decisions about their care [11,12].
| Study | Year | Crossover rate (during index admission) | Recurrent appendicitis | Time to recurrence mean (months, range) | Appendicitis on pathology | Postoperative complications | Percentage of patients successfully treated with antibiotics | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First author | Surgical group | Crossover group | Required surgery in follow-up | Overall | Surgery | Antibiotics | First episode | At follow-up | Ref. | ||||
| Eriksson | 1995 | 5% (1/20) | 36.8% (7/19) | 7 (3–12) | 85% (17/20) – 5% (1) perforated – 40% (8) phlegmonous – 40% (8) gangrenous | 100% (1/1) – 100% perforated | 100% (7/7) – 14.3% (1) perforated – 42.9% (6) phlegmonous | 89.3% (25/28) – 25% (7) perforated – 50% (14) phlegmonous – 28.6% (8) gangrenous | 10% (2/20) | 0% (0/8) | 95% (19/20) | 63.2% (12/19) | [8] |
| Styrud | 2006 | 11.7% (15/128) | 14.2% (16/113) | 4 (1–10) | 97% (120/124) – 4.8% (6) perforated – 0.8% (1) gangrenous | 93.3% (14/15) – 46.7% (7) perforated | 100% (16/16) – 31.3% (5) perforated | 96.8% (150/155) – 11.6% (18) perforated – 0.6% (1) gangrenous | 14% (17/124) | 12.9% (4/31) | 88.3% (113/128) | 85.8% (97/113) | [9] |
| Hansson | 2009 | 47.5% (96/202) | 14.2% (15/106) | – | 88.0% (220/250) – 20% (50) perforated – 51.2% (128) phlegmonous – 16.8% (42) gangrenous | (included in surgery group) | 100% (12/12) – 25% (3) perforated – 75% (8) phlegmonous – 8.3% (1) gangrenous | 89.7% (135/262) – 20.2% (53) perforated – 51.9% (136) phlegmonous – 16.4% gangrenous | 10.8% (18/167) | 16.2% (18/111) | 48.0% (97/202) | 79.0% (83/105) | [6] |
| Turhan | 2009 | 17.8% (19/107) | 10.2% (9/88) | – | Not reported – 18.6% (34) perforated | 100% (19/19) – 0 perforated | 100% (8/8) – 0 perforated | – | 4.4% (8/183) | 18.5% (5/27) | 82.2% (88/107) | 90.9% (80/88) | [5] |
| Malik | 2009 | – | 10% (4/40) | 8 (4–12) | 90% (36/40) – 5% (2) perforated – 30% (12) phlegmonous – 37.5% (15) gangrenous | – | – | – | 7.5% (3/40) | 0% (0/4) | – | 90% (36/40) | [10] |
| Vons | 2011 | – | 34.0% (36/106) | 4.2 (1.2–11.1) | Not reported – 17.5% (21) complicated | – | 88.9% (32/36) – 25% (9) complicated | – | – | – | – | 68% (81/120) | [7] |
| DiSaverio | 2014 | 11.9% (19/159; within 5 days) | 15.7 %(22/140) | – | Not applicable | 89.5% (17/19) | 75% (6/8) | 85.2% (23/27) | – | – | 88.1% (140/159) | 94.3% (132/140) | [3] |
| Minneci | 2014 | 6.7% (2/30) | 3.6% (1/28) | – | 95.7% (45/47) – 8.5% (4) perforated – 4.3% (2) gangrenous | 50% (1/2) – 0 perforated | 0% (0/1) | 92% (46/50) – 8% (4) perforated – 4% gangrenous | 10% (16/159) | – | 93.3% (28/30) | 96.4% (27/28) | [11] |
| Park | 2014 | – | 19.3% (23/119) | – | 95.6% (152/159) – 6.9% (11) complicated | Not reported | 80% (16/20) – 20% (4) complicated | 93.9% (168/179) – 8.4% (15) complicated | – | – | – | 83.2% (99/119) | [14] |
| Salminen | 2015 | 5.8% (15/257) | 22.7% (55/242) | 3.4 (2.3–4.5) | 99.3% (271/273) – 0.7% (2) perforated | 100% (15/15) – 46.7% (7) complicated | 90.9% (50/55) – 12.7% (7) complicated | 97.9% (336/343) – 4.7% (16) complicated | 20.5% (44/220) | 8.6% (6/70) | 94.2% (242/257) | 77.3% (187/242) | [13] |
| Minneci | 2016 | 5.5% (2/37) | 20% (7/35) | – | 93.8% (61/65) – 12.3% (8) complicated | – | not reported – 2.9% (1) complicated | – | 7.7% (5/65) | 0% (0/7) | 95.0% (35/37) | 80% (28/35) | [12] |
Length of stay
LOS is presented in Table 3. Many of the studies reported longer LOS for the antibiotic management arms. This was especially true among studies requiring two or more days of intravenous antibiotics with an early nothing by mouth (NPO) period [5,8–10,13]. LOS was shorter in studies with higher usage of laparoscopy and in fast-track antibiotic management, such as in DiSaverio et al. [3].
| Study | Year | Mean hospital LOS (SD) | Sick leave (SD) | Time off work/school (SD) | Ref. | |||
|---|---|---|---|---|---|---|---|---|
| First author | Surgery | Antibiotics | Surgery | Antibiotics | Surgery | Antibiotics | ||
| Eriksson | 1995 | 3.4 (1.9) | 3.1 (0.3) | – | – | – | – | [8] |
| Styrud | 2006 | 2.6 (1.2) | 3.0 (1.4) | 6.0 (4.4) | 5.3 (4.1) | 10.1 (7.6) | 8.0 (8.0) | [9] |
| Hansson | 2009 | 3 | 3 | 11 | 7 | – | – | [6] |
| Turhan | 2009 | 2.4 (1.4) | 3.14 (0.10) | – | – | – | – | [5] |
| Malik | 2009 | 1.2 (2.1) | 23.2 (0.3) | – | – | – | – | [10] |
| Vons | 2011 | 3.96 (4.87) | 3.04 (1.50) | – | – | – | – | [7] |
| DiSaverio | 2014 | NA | 0.4 | NA | 5.8 | – | – | [3] |
| Minneci | 2014 | 0.83 (median) | 1.58 (median) | – | – | 5 | 3 | [11] |
| Park | 2014 | 6.4 (1.7) | 3.4 (1.3) | – | – | – | – | [14] |
| Salminen | 2015 | 3.0 (median) | 3.0 (median) | 19 (median) | 7 (median) | – | – | [13] |
| Minneci | 2016 | 0.83 (median) | 1.54 (median) | – | – | – | – | [12] |
LOS presented as mean in days, unless noted otherwise(e.g., when noted as median). SD presented when available.
LOS: Length of stay; NA: Not Available; SD: Standard deviation.
Recurrence
Patients were followed on average for 1–2 years to assess for recurrence. Recurrence rates ranged from 3.6 to 36.8%, excluding those with immediate failure of antibiotic treatment requiring crossover to appendectomy (during index admission) and time to recurrence ranged from 3.4 to 8 months. Hansson et al. [6] did not report an overall recurrence rate, but did note that a third of recurrences occurred within 10 days of hospital discharge, and the remaining two-thirds between 3 and 16 months. The majority of patients with recurrence were managed operatively; however, some patients were successfully managed a second time with antibiotics [5–6,14]. Park et al. [14] and Hansson et al. [6] reported that 13–22.2% of patients with recurrent appendicitis were managed successfully with a second round of antibiotics. Turhan et al. [5,14] also reported that 22.2% of patients with recurrent appendicitis underwent medical treatment. One of these patients had a third recurrence, which was treated with appendectomy [5].
Pathology
Final pathology results were compared among the three groups: patients who underwent primary surgical management, patients who crossed over to surgery during the initial antibiotics phase and primary antibiotic patients with recurrent appendicitis. Among all groups who had surgery, appendicitis was found on pathology in 85.2–97.9% of patients (Table 2). Four studies did not report how many patients did not have appendicitis on final pathology. When reported, appendiceal inflammation documented on final pathology was present at higher rates in those who crossed over to surgery and those with recurrent appendicitis compared with those assigned to primary surgery management. Although many studies included ultrasound or CT for diagnosis, data correlating imaging modality and final pathology were not reported [3–5,11,12]. Accuracy of diagnosis was greatest in the study by Salminen et al. [13], which used CT as the required diagnostic imaging modality. In this study, patients in the surgery arm were correctly diagnosed 99.3% of time, crossover patients 100%, and antibiotic arm patients who later developed recurrence 90.9%. Vons et al. [7], which also used CT, did not report pathology of the surgical or crossover groups; however, diagnosis of appendicitis (based on pathology) for those with recurrent appendicitis was accurate in 88.9% [7]. When patients in these studies presented with recurrent abdominal pain, it was frequently presumed that they had recurrent appendicitis: however 10–11.1% of patients in the recurrence groups had NA. Use of diagnostic imaging was not reported among those with recurrent symptoms.
For those patients who underwent surgery in the study by Hansson et al. [6], efficacy of operative treatment was defined as either the correct pathology of appendicitis or another diagnosis requiring surgery. Among those who underwent surgery during the index admission, those in the surgery and crossover groups, 88% had pathology consistent with acute appendicitis and 1.2% had another diagnosis treatable by surgery, although the specific pathologies of the three patients in this category were not specified. For the purposes of our review, only diagnoses of acute appendicitis were considered efficacious.
Among all the included studies, the diagnoses of those without appendicitis included mesenteric adenitis [8,9], Campylobacter enteritis, terminal ileitis, ruptured ovarian cyst, pelvic inflammatory disease, Meckel’s diverticulum [9], granulomatous disease [11] and normal pathology [6,9].
Table 2 displays available data for rates of perforated appendicitis. Three studies presented data on complicated appendicitis, defined as presence of abscess, phlegmon or gangrene [3,12,14]. Rates were calculated using the number of patients with perforated or complicated appendicitis with respect to the number of patients undergoing surgery within a given group. Rates of perforated appendicitis ranged from 0.7 to 20% in the primary surgery group, 0–100% in the crossover group, and 0–31.3% in the recurrent appendicitis group. Eriksson and Granström [8] had one patient in the crossover group and the pathology of that patient was consistent with perforated appendicitis, giving a perforated appendicitis rate of 100%. This patient was noted to develop peritonitis during obligatory admission for antibiotics and was found to have appendiceal perforation on pathology [8]. It is not always possible to identify perforation on imaging, thus it is not known how many antibiotic-treated patients had perforated appendicitis at the time of randomization. Additionally, progression to perforation is a dynamic process and may occur between the time of imaging and randomization. Among the randomized controlled trials, the rates of perforated appendicitis should be equal between study arms. As more studies are conducted using modern diagnostic imaging tools, patients with significant perforation (i.e., not microperforations that are evident only on final pathology) may be identified prior to enrollment and not included. This will likely affect the rate of crossover in future studies as patients with clinically significant perforated appendicitis may not improve with antibiotics alone.
Complications
Rates of complications were calculated for patients assigned to surgical management and separately for those in the antibiotic group who required surgery (Table 2). Within the surgery group, complications occurred in 4.4–20.5% of cases versus 0–18.5% in the group of patients originally started on antibiotics but who crossed over to surgery. There was one death among all the study populations. The death occurred in a patient randomized to operative management and occurred on day 5 after surgery due to cardiomyopathy. The authors did not specify whether the patient’s heart disease decompensated secondary to perioperative stress [13]. Complications varied among studies, but were most commonly wound infections and intra-abdominal abscesses. Few patients required reoperations, and some of these were not complications, in particular two patients who required definitive operation for malignancy discovered at the initial surgery [5]. Complication rates for those with acute appendicitis on pathology versus those with not available (NA) were not reported.
Salminen et al. [13] and Hansson et al. [6] had the highest complication rates for surgery (20.5%) and antibiotic (16.2%) groups, respectively. Salminen et al. [13] reported a low laparoscopic surgery rate, which could explain the higher incidence of complications in this group. The authors noted in their discussion the majority of the morbidity within their surgery group was related to wound infections. They postulated that had their laparoscopic rates been higher, there would have been likely fewer complications [13]. Minneci et al. [12] reported a 100% laparoscopic rate and their rates of complication were 7.7%.
Other findings
Patients in the antibiotic group reported less pain than those in the surgery group and used less narcotics [8]. Lower pain scores were reported as early as 12 h [8]. Pain levels reported at 1 month were not different among groups [6,7]. Sick days and days of work/school missed were reported by few studies (Table 3). When presented, patients in the antibiotic group used less sick leave and spent less time away from school or work compared with patients undergoing predominantly open appendectomy [3,6,9,11,13].
Cost information was presented in five studies (Table 4). Primary admission costs were higher among those in the surgery group. As noted in the ‘Methods’ section, costs were compared as a ratio of surgery to antibiotics. Surgery ranged from 1.29- to 2.05-times more expensive than primary antibiotic management [3,5,6,12,14]. The cost ratio was highest for Hansson et al. [6], likely in part due to longer LOS for both arms due to including obligatory intravenous antibiotics for 24 h in the antibiotic group and recovery after open appendectomy in the surgery group. Cost of antibiotic management reported by DiSaverio et al. [3] was low due to outpatient antibiotic management of acute appendicitis [3]. The Comparing Outcomes of Drugs and Appendectomy Trial is a trial in active enrollment and is designed to evaluate the effectiveness of mostly outpatient antibiotic management of acute appendicitis in a setting where laparoscopic surgery is much more common than in the European trials [26]. As treatment practices move toward outpatient management with antibiotics and earlier discharge of surgically managed patients [27,28], costs of each arm will likely decrease.
| Study (year) | Mean cost of primary admission | Surgery/antibiotic-cost ratio | |
|---|---|---|---|
| First author | Surgery | Antibiotics | |
| Hansson (2009) | 36,900 SEK | 18,000 SEK | 2.05 |
| Turhan (2009) | 755 TL | 585 TL | 1.29 |
| DiSaverio (2014) | NA | €180 ($190.11) | – |
| Park (2014) | US$2207 | $1140 | 1.94 |
| Minneci (2016) | $4960 | $3641 | 1.36 |
Conclusion
In recent years, the treatment of numerous intra-abdominal pathologies has shifted from primary surgical management to primary medical therapy, with surgery reserved for those who fail to improve with medications alone. Medical or percutaneous management of intra-abdominal diseases, such as abscesses in Crohn’s disease, tubo-ovarian abscesses and acute diverticulitis, have been proven to be effective in these patients and minimal adverse effects are seen in patients who go on to require surgery [12]. Appendicitis may be added to this list in the future, but further data are necessary, particularly because the operation that definitively treats appendicitis is so much less morbid than, for example, Hartmann’s procedure for diverticulitis or salpingoophrectomy for a patient with tubo-ovarian abscess who might otherwise have her ovary spared.
Our review included 11 studies conducted over a 21-year period, demonstrating evolutions in protocols of care, diagnostic rigor and operative approach. One of the major limitations of this review is the heterogeneity of study designs, including patient inclusion, comparative metrics and measured outcomes. Despite this limitation, numerous themes can be extracted from a systematic review. Two temporal changes were especially evident: laparoscopy use increased in more recent studies (although international variation remains) and recent studies have required decreasing lengths of obligatory stay for antibiotic management.
The decision to use antibiotics to treat acute appendicitis should be held to the same standards of diagnostic rigor as surgical management. Antibiotics may be safely recommended in patients with high surgical risk, such as the elderly or those with multiple comorbidities [9]. However, antibiotics should not be used simply for patients with lower suspicion of acute appendicitis [9], as some studies had previously done [25]. Nonspecific management of equivocal appendicitis increases antibiotic exposure and subsequent risk of secondary healthcare associated infection in patients who may not require therapy and increase the societal risk of resistant bacterial strains [9]. Eriksson et al. evaluated the risk of secondary healthcare-associated infection as a result of antibiotic use; 39/40 patients were tested for Clostridium difficile infection in the follow-up period. Although none of the patients within this study tested positive for C. difficile, risk of secondary infection should be considered in all patients treated with antibiotics [8].
It is necessary to emphasize that the data reviewed here are for patients with uncomplicated appendicitis. Basic principles of general surgery and source control of intra-abdominal infection still apply: those with a consolidated abscess require source control (generally with percutaneous drain), severe phlegmon should generally be treated with intravenous antibiotics rather than immediate surgery, and those rare patients who present with signs/symptoms of diffuse peritonitis require an operation and intervention as dictated by the clinical findings.
In summary, these studies demonstrate that antibiotic management is successful in most cases of uncomplicated acute appendicitis. The need for crossover in management and rates of recurrent appendicitis were low among all the studies. Importantly, for those patients who ultimately required surgery, no increased complications were observed.
Future perspective
As the costs of each arm decrease, attention to patient-centered outcomes, including quality of life, pain control, satisfaction with care and time away from work/school, will likely become the key factors in patients’ decision-making processes [11]. The importance of informed consent in appendicitis management now requires not only the risks and benefits of surgery, but, for eligible patients, should also include the possibility of an antibiotics first approach including the risks of early failure and longer term recurrence, as well as the comparative risks and benefits of each therapeutic approach. Some patients are motivated to avoid surgery whenever possible. On the other hand, some patients and families may be unwilling to accept the risks of recurrent appendicitis with the attendant costs, missed school or work days, repeated imaging studies that use ionizing radiation and anxiety for each instance of nonsurgical abdominal discomfort [12]. Minneci et al. [12] found that patient and family satisfaction was high when given treatment choice. With increased emphasis on patient satisfaction in modern systems of healthcare delivery, patient choice – when appropriate – may become a major influence on the management of appendicitis. These data and data that are forthcoming will allow us to appropriately counsel patients on the comparative risks and benefits of each approach.
This is a review of 11 prospective studies comparing surgical and antibiotic management of acute appendicitis over a 21-year period.
Improvements in diagnostic imaging technology quality and availability allow for improved preoperative diagnosis and characterization of the severity of appendicitis, which can direct patient care.
Antibiotics regimens included one, two or three antibiotics. Duration of mandatory inpatient antibiotic management varied among studies from 0 to 2 days. Outpatient antibiotic regimens consisted of one to two antibiotics for total treatment duration of 4–10 days. Patients in surgical management arms were operated on within 24 h of admission.
We have defined crossover patients as those patients who were initially assigned to antibiotic management yet required surgery during the index admission. Crossover rates ranged from 5 to 47.5%.
Many of the studies reported longer lengths of stay for the antibiotic management arms.
Recurrence rates ranged from 3.6 to 36.8%, excluding those with immediate failure of antibiotic treatment requiring crossover to appendectomy.
Among all groups who had surgery, appendicitis was found on pathology in 85.2–97.9% of patients. Rates of perforated appendicitis ranged from 0.7 to 20% in the primary surgery group, 0–100% in the crossover group, and 0–31.3% in the recurrent appendicitis group.
Within the surgery group, postoperative complications occurred in 4.4–20.5% of cases versus 0–18.5% in the antibiotics group.
Primary admission costs were higher among those in the surgery group. Surgery ranged from 1.29 to 2.05-times more expensive than primary antibiotic management.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Flum DR. Acute appendicitis–appendectomy or the 'antibiotics first' strategy. N. Engl. J. Med. 372(20), 1937–1943 (2015).
2.
Ehlers AP, Talan DA, Moran GJ, Flum DR, Davidson GH. Evidence for an antibiotics first strategy for uncomplicated appendicitis in adults: a systematic review and gap analysis. JACS 222(3), 309–314 (2016).
3.
DiSaverio S, Sibilio A, Giorgini E, Biscardi A. The NOTA Study (Non Operative Treatment for Acute Appendicitis): prospective study on the efficacy and safety of antibiotics (amoxicillin and clavulanic acid) for treating patients with right lower quadrant pain and long-term follow-up of conservatively treated suspected appendicitis. Ann. Surg. 260, 109–117 (2014).
4.
Drake FT, Mottey NE, Farrokhi ET et al. Time to appendectomy and risk of perforation in acute appendicitis. JAMA Surg. 149(8), 837–844 (2014).
• Addresses a common oversimplification of the management of acute appendicitis. This manuscript describes appendiceal perforation as a prehospital phenomenon and not as an effect of in-hospital management.
5.
Turhan AN, Kaplan S, Kutukcu E, Yigitbas H, Hatipoglu S. Aygun E. Comparison of operative and non-operative management of acute appendicitis. Ulus. Travma Acil Cerrahi Derg. 15(5), 459–462 (2009).
6.
Hansson J, Korner U, Khorram-Manesh A, Solberg A, Lundholm K. Randomized clinical trial of antibiotic therapy versus appendicectomy as primary treatment of acute appendicitis in unselected patients. Br. J. Surg. 96, 473–481 (2009).
7.
Vons C, Barry C, Maitre S et al. Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomised controlled trial. Lancet 377, 1573–1579 (2011).
8.
Eriksson S, Granström L. Randomized controlled trial of appendicectomy versus antibiotic therapy for acute appendicitis. Br. J. Surg. 82, 166–169 (1995).
9.
Stryud J, Eriksson S, Nilsson I et al. Appendectomy versus antibiotic treatment in acute appendicitis. A prospective multicenter randomized controlled trial. World J. Surg. 30, 1033–1037 (2006).
10.
Malik AA, Bari S. Conservative management of acute appendicitis. J. Gastrointest. Surg. 13, 966–970 (2009).
11.
Minneci PC, Sulkowski JP, Nacion KM et al. Feasibility of a nonoperative management strategy for uncomplicated acute appendicitis in children. J. Am. Coll. Surg. 219(2), 272–279 (2014).
12.
Minneci PC, Mahida JB, Lodwick DL et al. Effectiveness of patient choice in nonoperative vs surgical management of pediatric uncomplicated acute appendicitis. JAMA Surg. 151(5), 408–415 (2016).
13.
Salminen P, Paajanen H, Rautio T et al. Antibiotic therapy vs appendectomy for treatment of uncomplicated acute appendicitis. JAMA 313(23), 2340–2348 (2015).
14.
Park HC, Kim MJ, Lee BH. The outcome of antibiotic therapy for uncomplicated appendicitis with diameters ≤ 10mm. Int. J. Surg. 12, 897–900 (2014).
15.
Page AJ, Pollock JD, Perez S, Davis SS, Lin E, Sweeney F. Laparoscopic versus open appendectomy: an analysis of outcomes in 17, 199 patients using ACS NSQIP. J. Gastrointest. Surg. 14, 1955–1962 (2010).
16.
Brugger L, Rosella L, Candinas D, Güller U. Improving outcomes after laparoscopic appendectomy: a population based, 12 year trend analysis of 7446 patients. Ann. Surg. 253, 309–313 (2011).
17.
Drake FT, Florence MG, Johnson MG et al. Progress in the diagnosis of appendicitis: a report from Washington State’s Surgical Care and Outcomes Assessment Program (SCOAP). Ann. Surg. 256(4), 586–594 (2012).
18.
Andersson REB. Small bowel obstruction after appendicectomy. Br. J. Surg. 88, 1387–1391 (2001).
19.
Flum DR, Koepsell T. The clinical and economic correlates of misdiagnosed appendicitis. Arch. Surg. 137, 799–804 (2002).
• Nationwide analysis detailing the clinical and financial costs of negative appendectomy, which is particularly relevant for patients with equivocal diagnosis of appendicitis.
20.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535 (2009).
21.
Coursey CA, Nelson RC, Patel MB et al. Making the diagnosis of acute appendicitis: do more preoperative CT scans mean fewer negative appendectomies? A 10-year study. Radiology 254(2), 260–268 (2010).
22.
Raja AS, Wright C, Sodickson AD et al. Negative appendectomy rate in the era of CT: an 18 year perspective. Radiology 256(2), 460–465 (2010).
23.
Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann. Emerg. Med. 15(5), 557–564 (1986).
24.
Kalan M, Talbot D, Cunliffe WJ, Rich AJ. Evaluation of the modified Alvarado score in the diagnosis of acute appendicitis: a prospective study. Ann. R. Coll. Surg. Engl. 76, 418–419 (1994).
25.
Farhnak M, Talei-Khoei M, Gorouhi F, Jalali A, Gorouhi F. The Alvarado score and antibiotics therapy as a corporate protocol versus conventional clinical management: randomized controlled pilot study of approach to acute appendicitis. Am. J. Emerg. Med. 25(7), 850–852 (2007).
26.
Flum DR. Comparing Outcomes of Drugs and Appendectomy (CODA). Patient-Centered Outcomes Research Institute. www.pcori.org/research-results/2015/comparing-outcomes-drugs-and-appendectomy-coda
27.
Cundy TP, Sierakowski K, Manna A, Cooper CM, Burgoyne LL, Khurana S. Fast-track surgery for uncomplicated appendicitis in children: a matched case-control study. ANZ J. Surg. 87(4), 271–276 (2016).
• With a recent focus on patient-centered outcomes, time to return to school is important in the management of acute appendicitis.
28.
Frazee RC, Abernathy SW, Davis M et al. Outpatient laparoscopic appendectomy should be the standard of care for uncomplicated appendicitis. J. Trauma Acute Care Surg. 76(1), 79–83 (2014).
• Similar to the paper by Cundy et al., fast-track appendectomy should be the standard of care for most patients with acute appendicitis.
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 12 July 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of surgery versus antibiotics in acute appendicitis: a systematic review. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0017
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Xinlin Chin, Sachini Mallika Arachchige, Jane L Orbell-Smith, Daniela Da Rocha, Anil Gandhi, Conservative Versus Surgical Management of Acute Appendicitis: A Systematic Review, Cureus, 10.7759/cureus.52697, (2024).
- Jian Li, Huan Liu, Shengbo Sun, Yanqiu Li, Weihua Tong, Prediction of Complex Acute Appendicitis Based on HGS-MSVM, IEEE Access, 10.1109/ACCESS.2023.3290473, 11, (84336-84345), (2023).
- Rubén Allende, Rodrigo Muñoz, Are antibiotics a safe and effective treatment for acute uncomplicated appendicitis?- First update, Medwave, 10.5867/medwave.2018.04.7229, 18, 04, (e7229-e7229), (2018).
- S. A. Sovtsov, A. G. Kriger, O. V. Pribytkova, A. V. Smirnov, Is medication possible for acute appendicitis?, Khirurgiya. Zhurnal im. N.I. Pirogova, 10.17116/hirurgia2018296-99, 2, (96), (2018).