The cost–effectiveness of blue-light therapy in the treatment of mild-to-moderate psoriasis
Abstract
Aim: To investigate the cost–effectiveness of blue-light therapy versus a two-compound formulation (TCF) (Dovobet® gel [calcipotriol and betamethasone]) in mild-to-moderate psoriasis. Methods: A Markov model was applied to describe the course of disease among Dutch patients with a Psoriasis Area and Severity Index (PASI) score ≤ 10 over a 52-week time horizon. Patients received either 12-week blue-light therapy or two 4-week treatments with TCF. Patients, experiencing no PASI reduction after either therapy, were assumed to receive 12-week ultraviolet B phototherapy. Results: There was no significant difference in PASI reduction between two interventions (71 vs 72%). However, blue-light therapy was associated with a cost savings of EU€248. Conclusion: Treatment of mild-to-moderate chronic plaque psoriasis using blue-light therapy may be more cost-effective than TCF.
First draft submitted: 20 January 2017; Accepted for publication: 24 March 2017; Published online: 28 April 2017
Combination therapy of vitamin D analogs and betamethasone appears to be the most efficacious treatment option in mild-to-moderate psoriasis [1]. Moreover, studies have reported that this option is also cost-effective than alternative therapies in most cases [2–5]. A two-compound formulation (TCF) product containing 50 μg calcipotriol and 0.5 mg betamethasone per gram (Dovobet® [made by LEO Pharma, Denmark]) [6] is a topical therapy often used by Dutch dermatologists to treat psoriasis vulgaris. While it is offered in two forms (gel and ointment), the gel form appears to offer advantages over the ointment form, including better patient compliance, better treatment adherence and better cost–effectiveness [7]. However, dermatologists who have tried topical therapy for mild-to-moderate psoriatic patients see that it has insufficient effect and may switch to ultraviolet B (UVB) phototherapy, which is generally offered on an outpatient basis but can be used at home [8].
A new alternative to treat mild-to-moderate psoriasis is ultraviolet (UV)-free blue-light therapy, which has both photobiological/chemical and thermal effects on the body [9]. Its immunomodulatory effects could be responsible for the clinical efficacy in chronic plaque psoriasis. A portable medical device is currently available that can produce blue light and be used to treat mild-to-moderate psoriasis on the trunk and limbs [10]. Its portability means that patients can use it at home and whenever they like. The aim of this study was to determine the cost–effectiveness of blue-light therapy (BlueControl® [10]) versus TCF in the first-line treatment of Dutch patients with mild-to-moderate psoriasis vulgaris seen by dermatologists.
Materials & methods
A decision analytic Markov model was developed to estimate the costs and clinical outcomes of blue-light therapy and Dovobet gel over a 52-week time horizon (Figure 1). The target population comprised patients eligible for both topical therapy and blue-light therapy, and who were referred to dermatologists. Effectiveness data from previously published randomized controlled trials (RCTs) and cost–effectiveness analyses were used to construct the model [4,8,9]. Total costs and clinical outcomes were assessed over a 52-week time horizon with a 4-week cycle length.
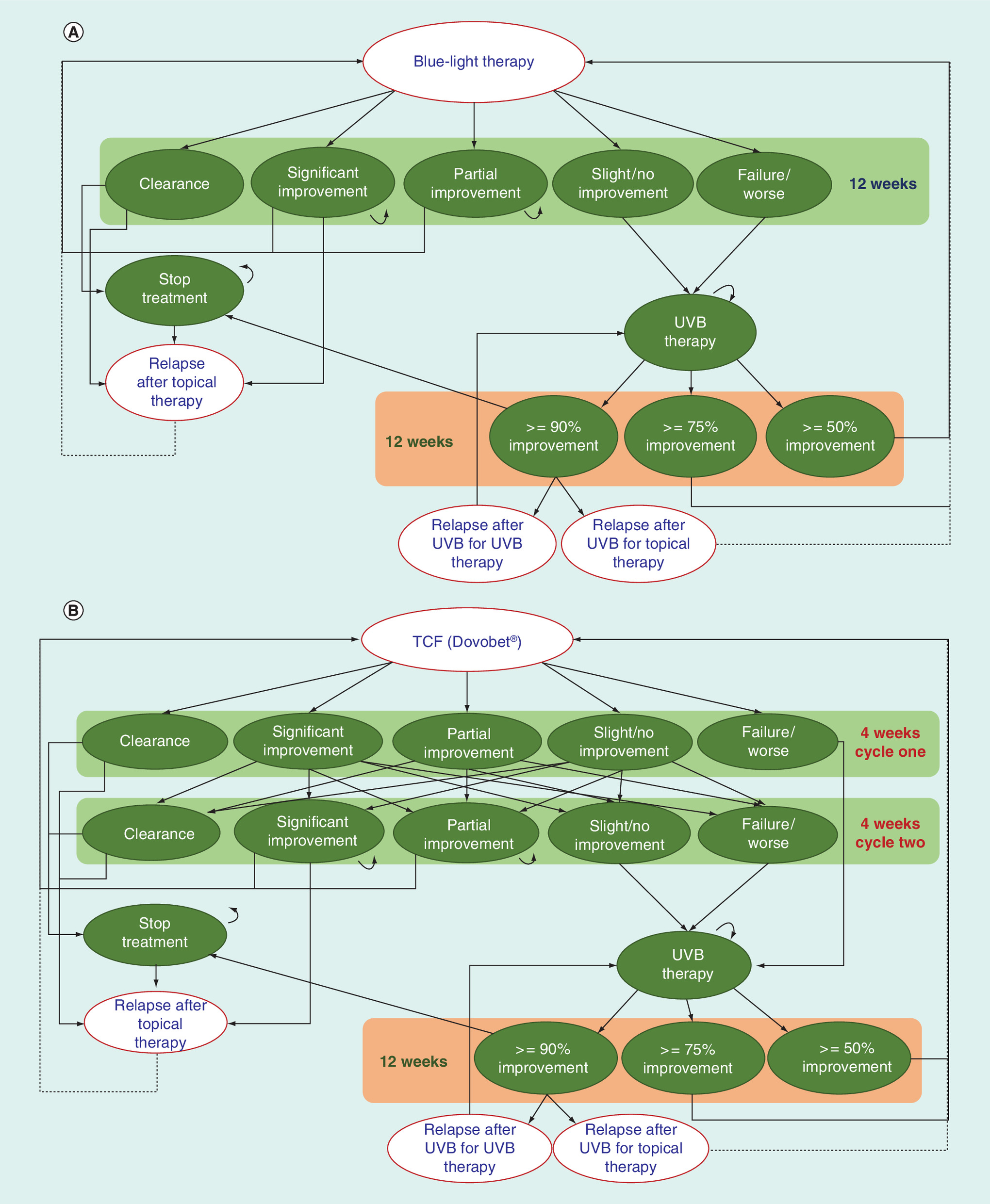
Figure 1. Schematic diagram of the model structure.
(A) Model structure for blue-light therapy and UVB and (B) model structure for two-compound formulation (TCF [Dovobet®]) and UVB.
TCF: Two-compound formulation; UVB: Ultraviolet B.
Treatment approaches
As Figure 1 shows, in first-line therapy, two treatments were compared: blue-light therapy, used once-daily for 12 weeks, and TCF (containing calcipotriol and betamethasone), used once-daily for two 4-week periods. After completion of these regimens, patients were categorized into five categories: clearance, significant improvement, partial improvement, no improvement or no change and worsening. In both arms, patients with clearance discontinued therapy until they experienced a recurrence. In contrast, those who showed significant or partial improvement continued therapy. Patients with no improvement and worsening were given second-line therapy. Patients who relapsed after first-line therapy received the same therapy (blue light or TCF) that they had received before.
Treatment outcomes following second-line therapy (12 weeks of UVB phototherapy in both treatment strategies) were as follows: 90% and more improvement (90 UVB), 75–90% improvement (75 UVB), 50–75% improvement (50 UVB) and less than 50% improvement (<50 UVB) [8]. Patients with 90% and more improvement suspended treatment until the lesions relapsed. Patients with 50–90% improvement were considered candidates for topical therapy; the initial state when starting topical therapy was the significant improvement health state (for patients with 75 UVB) and the partial improvement health state (for patients with 50 UVB). Patients who experienced less than 50% improvement were assumed to receive third-line therapy; this possibility was excluded in this study since it was assumed that the frequency of mild-to-moderate psoriasis patients receiving third-line therapy within the first 52-week period would be low. All patients who experienced a recurrence after UVB phototherapy based on their psoriasis status were given topical therapy or UVB phototherapy.
Transition probabilities
The transition probabilities used in the analyses are shown in Table 1. The probabilities of moving between different health states for TCF arm were obtained from a previous cost–effectiveness study [4]. However, we used their transition probabilities for TCF only in the first 4-week cycle since the patients in their study switched to calcipotriol therapy as a second-line treatment in the next 4-week cycle. The results of a double-blind RCT were used to estimate the transition probabilities for blue-light therapy [9] while the PLUTO study, a single-blind RCT performed in The Netherlands [8], was used to estimate the transition probabilities for UVB phototherapy.
Estimates of the chance and time of onset of relapse were based on an observational study of patients who received TCF for an 8-week period [11]. Due to lack of data, we assumed that the chance and time of onset of relapse for blue-light therapy were equal to those for TCF. Finally, a randomized, observer-blinded trial [12] was used to obtain the chance of dual management (topical therapy or further UVB phototherapy) after recurrence following UVB phototherapy.
Clinical outcomes
The primary clinical outcome was the Psoriasis Area and Severity Index (PASI) and the range in values used was 0 (no lesions) to 10 (the severest degree for mild-to-moderate chronic plaque psoriasis). The secondary outcome was disease-controlled days (DCDs), defined as the number of days that patients experienced 75% or more reduction in PASI.
Table 1 also shows the PASI and body surface area (BSA) values used in the analyses, most of which were based on Langley et al. [14]. Patients experiencing clearance were considered to have a PASI of 0.01 while patients who experienced worsening were considered to have a PASI that was equal to the ‘baseline’ PASI score. A similar approach was used for the outcomes following UVB phototherapy: 90% or more improvement (90 UVB) was matched with the value for ‘clearance', 75–90% improvement (75 UVB) was equated with ‘significant improvement’, 50–75% (50 UVB) was equated with ‘partial improvement’ and <50% improvement (<50 UVB) was equated with ‘slight/no-improvement'.
Patients who experienced a recurrence after topical therapy or UVB phototherapy and were candidates for further topical therapy were assumed to have a health state that was equal to the partial improvement state. Similarly, patients who relapsed after UVB therapy and were candidates for further UVB phototherapy were assumed to start in the ‘slight/no-improvement’ health state.
Costs
Costs were assessed using a societal perspective, as recommended in the Dutch pharmacoeconomic guidelines [18]. However, only direct treatment costs were examined. That is, no differences in indirect costs and productivity costs were expected since the two treatment strategies (blue light/UVB and TCF/UVB) involve therapies for home use. Use of TCF was determined by the BSA affected by the psoriasis. Total BSA was estimated from the PASI using the following formula: PASI = 4.3 + 47 × BSA [13]. However, the range of BSA was limited to 0–12, which is associated with a PASI score of less than 10, since our study focused only on patients with mild-to-moderate psoriasis. The average baseline BSA was estimated using information found in Langley et al. [11]. The TCF treatment dose per BSA was estimated using the maximum dose per week (100 g) and the maximum possible BSA (30%) [19] for management of psoriasis, which would be 13.2 g/BSA per 4 weeks. The price of TCF per tube (EU€45.56/60 g) and delivery costs at treatment start and every 8 weeks thereafter were obtained from the Dutch National Health Care Institute [15] website (Table 1).
The cost of blue-light therapy was fixed at EU€36.00 per 4-week period and the cost of electricity necessary to use the device was a fixed rate of EU€0.0043 per treatment (provided by Philips Light & Health). When combined with the total 12-week period of use, this meant a total cost of EU€184.19.
The costs of UVB phototherapy were based on costs from the PLUTO study [8] and adjusted for inflation to February 2017 costs (Statistics Netherlands) [16].
The costs of dermatologist visits, including the number of visits and the average duration per visit, were assumed to be equal in both arms and therefore excluded from the analyses. The costs of side effects were also excluded because of their low incidence from TCF use (even after 52 weeks of use) [19] and because studies of blue-light therapy have not observed any side effects [9].
Assumptions
Besides the assumptions described above, other assumptions were needed to conduct this study. First of all, we assumed that all patients who experience a relapse received more therapy, where the type of therapy (topical therapy or UVB) was based on their PASI. It was assumed that TCF and blue-light therapy would be just as efficacious in treating recurrence as they were in treating the initial problem with psoriasis. Finally, the variation in time to relapse onset was assumed to be ± 10 days around the mean because of lack of information [11].
Statistical analysis
Statistical analysis was performed to estimate the costs and health outcomes of TCF and blue-light therapy and validate the results of the model. All analyses were conducted using Microsoft Excel 2013.
The influence of the values of input parameters on the cost-effectiveness of blue-light therapy was examined using deterministic sensitivity analysis.
A probabilistic sensitivity analysis was performed to estimate the overall uncertainty in the differences in costs and effectiveness of blue-light therapy versus TCF [20,21]. Probability distributions were determined for each input parameter using published values wherever possible. The beta distribution was used for binomial variables, the Dirichlet distribution for multinomial variables, the log-normal distribution for costs and the beta distribution was used for outcomes and utility weights. The number of iterations used in the Markov Chain Monte Carlo simulation was determined by the number needed to derive stable estimates of the results (10,000 times).
Model validation
Internal validation was performed to assess how well the model’s results for PASI reduction of TCF, blue light and UVB corresponded with the data used to create the model. External validation involved comparing our results with the results of other studies not used in our analyses. As part of this validation, we compared our estimates of PASI reduction over the 52-week time horizon with the published results of a RCT [19] and also used t-tests to assess the differences between the two sets of results.
Results
Over a 52-week time horizon, there was a small nonsignificant difference in PASI reduction of 1% (95% CI: -7%–3%) between blue-light therapy and TCF (71 vs 72%) (Table 2). The analyses also showed that blue-light therapy resulted in 79 (95% CI: -105, -42) fewer DCDs than TCF (120 vs 199 days). However, blue-light therapy resulted in lower costs (-EU€248; 95% CI: -437–92) compared with TCF (EU€638 vs EU€886).
The cost-effectiveness of blue-light therapy is calculated by dividing the difference in costs by the difference in effectiveness. However, blue-light therapy leads to lower overall costs (-EU€248) and a slight decrease in effectiveness (1%, PASI), which makes interpretation difficult. A simpler interpretation can be obtained if we reverse the comparison to TCF versus blue-light therapy, where we would conclude that TCF use leads to a cost increase (EU€248) and a small gain in PASI improvement (1%) when compared with blue-light therapy. If the cost increase is divided by the effectiveness difference, the resulting ratio of EU€36,754 is interpretable as the extra costs to achieve a 100% improvement in PASI over a 1-year period. A similar calculation can be done using DCD: dividing the cost increases (EU€248) by the gain in DCDs (79) yields the extra cost to gain one extra DCD, which is EU€3.17 (or EU€1158 to gain one extra disease-controlled year).
One-way sensitivity analyses (Figure 2A) revealed that the input parameters with the greatest effect on the cost–effectiveness of blue-light therapy were the PASI value achieved after partial improvement, the probability of relapse in both arms and the baseline PASI. Figure 2B shows the results of the probabilistic sensitivity analysis on the cost–effectiveness plane, where effectiveness is based on PASI improvement. The variation in the location of the dots reflects the degree of uncertainty regarding the differences in costs and effectiveness between blue-light therapy and TCF. Dots to the right of the Y-axis indicate that blue-light therapy is more effective than TCF, while dots above the X-axis indicate that blue-light therapy leads to more costs than TCF. In this figure, most of the dots lie below the X-axis, indicating a high probability that blue-light therapy will reduce costs. In contrast, there are about as many dots to the left of the Y-axis as there are to the right of the Y-axis, which indicate that there is essentially no difference in effectiveness between the two therapies (as shown in Table 2). The cost–effectiveness acceptability curve [22] (Figure 2C) shows the probability that blue-light therapy is cost-effective compared with TCF at various levels of willingness to pay to achieve 100% PASI improvement for 1 year. Overall, there is a 50% chance that blue-light therapy is more cost-effective than TCF, although its chance of being cost-effective increases to almost 77% at lower willingness to pay thresholds.
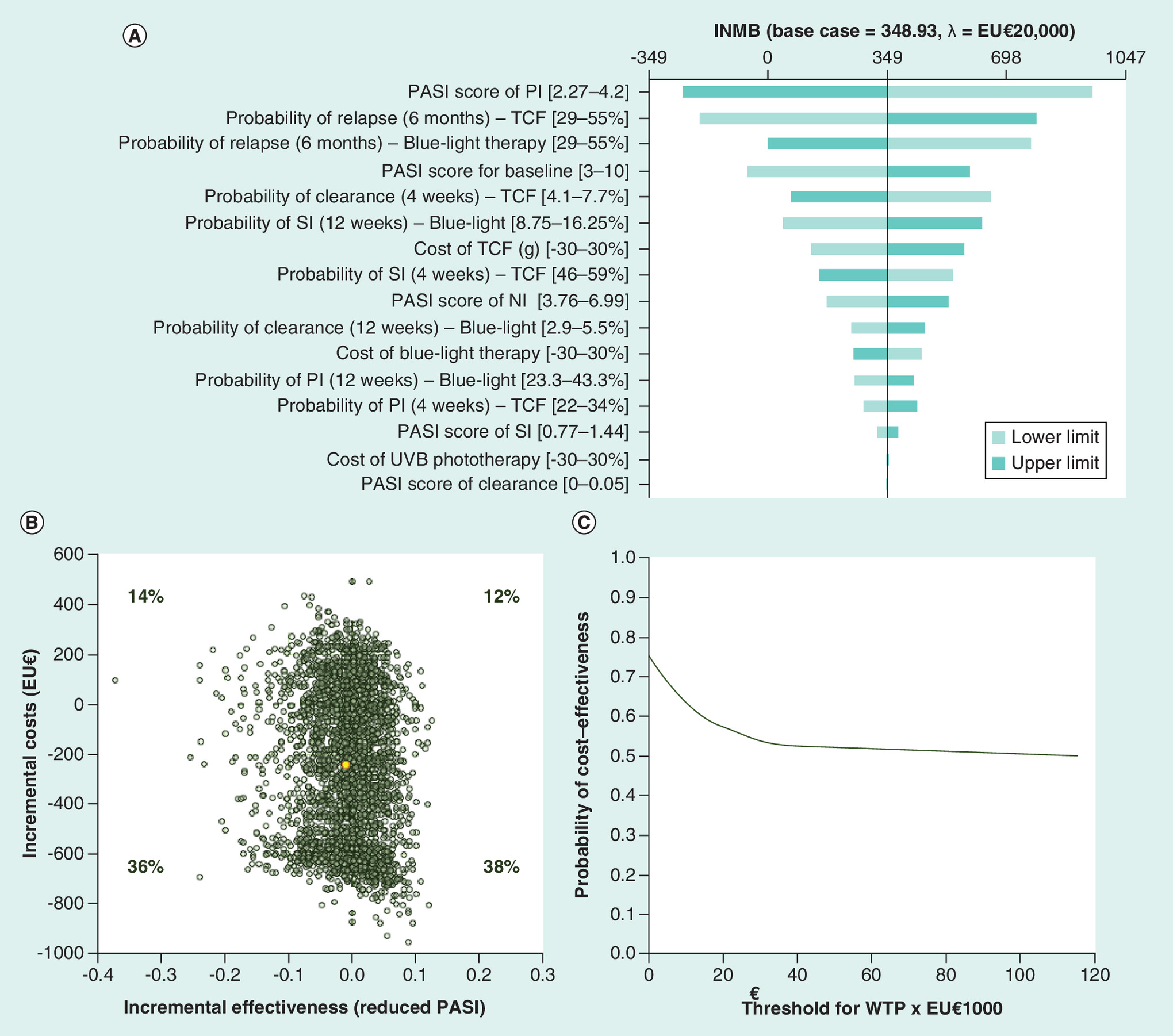
Figure 2. The results of cost-effectiveness analysis.
(A) The results of one-way deterministic sensitivity analysis. (B) Scatterplot showing the uncertainty regarding the differences in costs and effectiveness (PASI reduction) between blue-light therapy and TCF. (C) The probability of blue-light therapy being cost-effective versus TCF using a cost–effectiveness acceptability curve.
INMB: Incremental net monetary benefit. The probability of cost–effectiveness of blue-light therapy versus TCF using a cost–effectiveness acceptability curve; M: Month; NI: No improvement; PASI: Psoriasis Area and Severity Index; PI: Partial improvement; SI: Significant improvement; TCF: Two-compound formulation; W: Week; WTP: Willingness-to-pay.
Validation of the results
The internal validation results for the three treatments (blue light, TCF and UVB) revealed no significant differences between our results and the results of the studies used to perform our analyses (Table 3). Validation was only possible for the first treatment period for each type of treatment since the treatment of first and second lines could not be assessed due to lack of information.
External model validation for TCF using different end points and treatment durations revealed that our results at 4 and 8 weeks were generally higher than the results from other studies, suggesting that we might have overestimated the effectiveness of TCF (Table 3). Our results over the 52-week time horizon were comparable with the results of Kragballe et al. [26]. Since Kragballe reported the efficacy of interventions using the physician’s global assessment (PGA), we converted our PASI results to PGA using the formula PGA = (PASI - 0.0344)/1.0251 [27]. There was no significant difference (p = 0.477) between our results and Kragballe’s results over the entire 52-week period.
Discussion
Many Dutch patients with mild-to-moderate psoriasis currently receive semi-liquid dosage forms (ointment or gel) of different monotherapies or combination therapies as a first-line therapy. Blue-light therapy represents a new option to these types of treatment and our study suggests that blue-light therapy followed by UVB is cost-effective versus TCF followed by UVB since it is similar in effectiveness but could reduce total costs over a 52-week period.
To our knowledge, this is the first study to compare the cost–effectiveness of a medical device with medication in mild-to-moderate psoriasis management across two consecutive treatment lines. The results of this study can help to raise discussion about the potential of using UV-free blue-light therapy in mild-to-moderate psoriasis. While various therapies could have been used as a ‘comparator’ therapy for this study of blue-light therapy, we selected TCF as the ‘comparator’ therapy since previous studies have suggested that the combination of vitamin D and corticosteroids like TCF are more cost-effective than other topical therapies [4,5,11]. In addition, patients have shown better compliance to the gel form than to other forms [7]. Therefore, the use of a different therapy in our study would have resulted in more favorable outcomes for blue-light therapy than the results reported here.
Cost–effectiveness is one criterion used in assessing the value of one treatment versus another. We found that TCF increases costs and slightly increases PASI reduction. The resulting cost–effectiveness ratio of EU€21,082 is interpretable as the extra cost to gain 1 year of 100% PASI reduction. However, this finding is difficult to determine since the most common type of effectiveness outcome used in cost–effectiveness analyses is quality-adjusted life-years (QALYs). This problem can be solved by transforming the ratio into the incremental cost per QALY gained. One study found that the quality of life (QoL) of patients with mild-to-moderate psoriasis patients is 0.74 ± 0.23 [28]. If we assume that patients have that QoL when they start therapy but improve to a ‘normal’ QoL if they experience a 100% PASI reduction (where normal means the QoL seen in the Dutch general population, or 0.869 ± 0.170 [29]), then this would be a gain in QoL of 0.13. However, this QoL gain is actually hypothetical since the actual difference in PASI improvement that we found in this study was just 1%; this small PASI improvement translates into a QoL gain that is 1% of 0.13, or 0.0013. When this value is combined with the cost increase of EU€248 over a period of 1 year, this would mean that the extra cost to gain one QALY is EU€191,013, which is much higher than any existing cost–effectiveness thresholds. For example, the highest threshold suggested for use in The Netherlands has been EU€80,000 [30], which has been suggested only if the disease is severe; the threshold for mild disease is much lower (EU€20,000) [30]. Note that this higher ICER of EU€191,013/QALY actually means that TCF is not cost-effective when compared with blue-light therapy, which is cheaper but less effective. In other words, based on this estimate, TCF is not cost-effective versus blue-light therapy.
Effectiveness and cost-effectiveness are not the only two factors to consider when comparing the values of different treatments. For example, patient preferences can also play a role when selecting a treatment for a particular patient. Eastman et al. showed that treatments which improve patient compliance can also help to improve treatment adherence [31] and most recently Alinia et al. showed that patient adherence attenuates in long-term care with topical therapy in mild-to-moderate psoriasis [32]. In addition, patient preferences can be seen as a criterion in its own right. Although no information is available regarding patient preferences between a semiliquid drug dosage form and a medical device in psoriatic patients, blue-light therapy has a high rate of patient acceptance [9], suggesting that some patients may prefer to use it instead of a drug. Since our study suggests that blue-light therapy may be similar in effectiveness but potentially cost-saving compared with TCF, this may mean that patient preferences can be a deciding factor in determining which treatment is the most appropriate one for an individual patient.
The findings of our study only relate to patients who are eligible for both blue-light therapy and TCF. Therefore, the results do not extend to patients whose psoriasis is found in parts of the body like elbows or the scalp where the blue-light emitting device cannot be used.
Our study has some limitations worth noting. First, the number of patients included in the RCT of blue-light therapy was small, which resulted in uncertainty about its effectiveness compared with TCF. Nevertheless, our findings suggest that there is a 50% chance that blue-light therapy is more cost-effective than TCF. Second, since there have been no trials comparing blue-light therapy with TCF directly, we used a modeling approach to compare their cost-effectiveness. However, we conducted several validation analyses to ensure that the model produced valid results; in particular, the external validation process meant comparing our results with the results from studies that were not directly used to make the model. Third, since the RCT of blue-light therapy did not examine the long-term outcomes of blue-light therapy, assumptions were needed about the long-term results and the chance of long-term failure. Fourth, other assumptions were necessary to perform the analysis due to lack of data. However, sensitivity analysis showed that these assumptions did not substantially affect the cost–effectiveness results. Last, we could not use the Dermatology Life Quality Index due to lack of information. Instead, we used the PASI as our primary effectiveness outcome, which is a commonly used tool for effectiveness in both clinical trials [27] and cost–effectiveness analyses [3–4,23,33–34].
Conclusion
Treatment of mild-to-moderate psoriasis with blue-light therapy appears to be as cost-effective as TCF. Specifically, our results suggest that blue-light therapy could be just as effective as TCF but cheaper than TCF as a first-line treatment, which could help to reduce overall healthcare costs without jeopardizing effectiveness. However, blue-light therapy cannot be considered as a definite alternative for TCF but rather as a new treatment alternative for certain types of patients with mild-to-moderate psoriasis. The small differences in effectiveness seen to date might mean that patient preference and clinician judgment can be the deciding parameters when it comes to choosing which treatment is best for an individual patient. Further studies would help to reduce the uncertainty about the effectiveness and cost–effectiveness of blue-light therapy versus alternative treatments like TCF. These studies should investigate the long-term efficacy, safety and costs of blue-light therapy versus alternative treatments as well as examine patient preferences.
| Parameter | Base-case estimate | Standard error | Distribution | Distribution parameters | Source | Ref. |
|---|---|---|---|---|---|---|
| Transition probabilities | ||||||
| TCF (4 weeks): | ||||||
| – Clearance | 5.9% | – | – | α1 = 14 | Augustin et al. | [4] |
| – Significant improvement | 52.5% | – | – | α2 = 126 | Augustin et al. | |
| – Partial improvement | 27.7% | – | – | α3 = 67 | Augustin et al. | |
| – Slight improvement/no change | 13% | – | Dirichlet | α4 = 31 | Augustin et al. | |
| – Failure/worse | 0.9% | – | – | α5 = 2 | Augustin et al. | |
| – Time to relapse (median) | 63 days | – | Log-normal | μ = 4.14, s = 0.08 | Langley et al. | [11] |
| – Probability of relapse 6 months after starting Dovobet® | 42% | – | Beta | α = 28, β = 39 | Langley et al. | |
| Blue-light therapy (12 weeks) | ||||||
| Clearance | 4.2% | – | Beta | α = 1, β = 23 | Pfaff et al. | [9] |
| Significant improvement | 12.5% | – | Beta | α = 3, β = 21 | ||
| Partial improvement | 33.3% | – | Beta | α = 8, β = 16 | ||
| Slight improvement/no change | 29.2% | – | Beta | α = 7, β = 17 | ||
| Failure/worse | 20.8% | – | Beta | α = 5, β = 19 | ||
| Time to relapse | Same as Dovobet | – | – | – | Assumption | |
| Probability of relapse 6 months after starting Dovobet | Same as Dovobet | – | – | – | Assumption | |
| UVB phototherapy (12 weeks) | ||||||
| ≥90% improvement | 19.0% | – | Beta | α = 16, β = 68 | PLUTO study | [8] |
| ≥75% to <90% improvement | 22.6% | – | Beta | α = 19, β = 65 | PLUTO study | |
| ≥50% to <75% improvement | 31.0% | – | Beta | α = 26, β = 58 | PLUTO study | |
| Probability of relapse 6 months after starting UVB | 72.5% | – | Beta | α = 85, β = 78 | Cameron et al. | [12] |
| Probability of relapse 12 months after starting UVB | 31.0% | – | Beta | α = 35, β = 28 | Cameron et al. | |
| Clinical outcomes and utilities | ||||||
| PASI: | ||||||
| – Baseline | 8.53 | 1.02 | Log-normal | – | Langley et al. and Henseler et al. | [11,13] |
| – Clearance | 0.01 | 0.01 | Log-normal | – | Langley et al. and Henseler et al. | |
| – Significant improvement | 1.11 | 1.02 | Log-normal | – | Langley et al. | [14] |
| – Partial improvement | 3.24 | 1.02 | Log-normal | – | Langley et al. | |
| – Slight/no improvement | 5.37 | 1.02 | Log-normal | – | Langley et al. | |
| Body surface area | ||||||
| Baseline involved (%) | 9.0 | 7.70 | Log-normal | – | Langley et al. | [11] |
| Costs (EU€) | ||||||
| Blue-light therapy | 36.00 | – | Fixed | – | Philips Light & Health | |
| Energy cost per treatment | 0.0043 | – | Fixed | – | Philips Light & Health | |
| TCF† | 90.89 | 70.48 | Log-normal | – | medicijnkosten.nl | [15] |
| Delivery cost – 1st week | 12.00 | – | Fixed | – | medicijnkosten.nl | |
| Delivery cost every 8 weeks | 6.00 | – | Fixed | – | medicijnkosten.nl | |
| UVB therapy | 125.50 | 64.76 | Log-normal | – | PLUTO study, Statistics Netherlands | [16,17] |
†Costs of TCF were estimated using body surface area involved (%).
PASI: Psoriasis Area and Severity Index; TCF: Two-compound formulation; UVB: Ultraviolet B.
| Interventions | Clinical outcomes and costs | Mean | SD | Range (95% CI) | Incremental cost–effectiveness ratio |
|---|---|---|---|---|---|
| Blue-light therapy and UVB | Improvement in local PASI (%) | 71 | 9 | 50–85 | – |
| DCDs (days) | 120 | 27 | 73–178 | ||
| Cost (EU€) | 638 | 147 | 448–1005 | ||
| TCF and UVB | Improvement in local PASI (%) | 72 | 6 | 57–82 | – |
| DCDs (days) | 199 | 11 | 178–220 | ||
| Cost (EU€) | 886 | 314 | 356–1442 | ||
| Difference | Improvement in local PASI (%) | -1% | – | -7–3 | 36,754 |
| DCDs (days) | -79 | – | -105, -42 | 3.17 | |
| Cost (EU€) | -248 | – | -437–92 | – |
DCD: Disease-controlled day; PASI: Psoriasis Area and Severity Index; SD: Standard deviation; TCF: Two-compound formulation; UVB: Ultraviolet B.
| Treatment duration | Study (year) | NPs | Clearance (%) | ≥75% PASI reduction (%) | ≥50% PASI reduction (%) | Mean % reduction in PASI | Ref. | |
|---|---|---|---|---|---|---|---|---|
| Internal validation | Blue-light therapy | |||||||
| 4 weeks | Pfaff et al. (2015) | 24 | NR | NR | NR | 38 | [9] | |
| Model | n/a | 3 | 14 | 40 | 37 | |||
| 12 weeks | Pfaff et al. (2015) | 24 | 4 | 17 | 50 | 46 | [9] | |
| Model | n/a | 4 | 17 | 51 | 45 | |||
| TCF | ||||||||
| 4 weeks | Augustin et al. (2007) | 249 | 6 | 58 | 87 | 74 | [4] | |
| Model | n/a | 6 | 58 | 87 | 74 | |||
| UVB therapy | ||||||||
| 14.1 weeks | PLUTO (2009) | 84 | 19 | 42 | 73 | 70 | [8] | |
| 12 weeks | Model | n/a | 18 | 40 | 72 | 68 | ||
| External validation | ||||||||
| TCF 4 weeks | Kaufmann (2002) | 490 | NR | 56 | NR | 71 | [23] | |
| Ortonne (2004) | 249 | NR | 58 | NR | 65 | [24] | ||
| Peeters (2005) | 249 | NR | 47 | NR | NR | [3] | ||
| Langley (2011)† | 183 | 19 | 21 | 62 | 54 | [11] | ||
| Model | n/a | 6 | 69 | 87 | 74 | |||
| TCF 8 weeks | Fleming(2010) | 162 | NR | NR | NR | 55 | [25] | |
| Langley (2011)† | 183 | 41 | 33 | 68 | 59 | [11] | ||
| Model | n/a | 23 | 47 | 73 | 71 | |||
| TCF 52 weeks | Kragballe(2006)† | 212 | 38 | NR | 88 | 79 | [26] | |
| Model | n/a | 33 | 67 | 89 | 77 | |||
†Converted from physician’s global assessment to PASI (Physician’s global assessment = [PASI - 0.0344]/1.0251).
n/a: Not applicable; NP: Number of patient, NR: Not reported; PASI: Psoriasis Area and Severity Index; TCF: Two-compound formulation; UVB: Ultraviolet B.
Mild-to-moderate chronic plaque psoriasis is often treated using various medications or combinations of medications.
Blue-light therapy, produced by a portable medical device suitable for home use, represents an alternative way to treat this disease.
The aim of this study was to investigate cost-effectiveness of blue-light therapy versus Dovobet® gel (calcipotriol and betamethasone dipropionate), a two-compound formulation (TCF), in mild-to-moderate chronic plaque psoriasis.
A Markov model was used to describe the course of disease among Dutch patients with a Psoriasis Area and Severity Index (PASI) score ≤10 over a 52-week time horizon.
Effectiveness outcomes were percentage reduction in PASI and disease-controlled days. Costs were calculated using updated results of previous studies and other sources.
Our results showed that there was no significant difference in PASI reduction between blue-light therapy and TCF (71 vs 72%) (difference: 1%; 95% CI: -7–3%).
Blue-light therapy was associated with a cost-savings of EU€248 (95% CI: -EU€437–EU€92) since its total costs were EU€638 vs EU€886 for TCF.
Consequently, treatment of mild-to-moderate chronic plaque psoriasis using blue-light therapy may be more cost-effective than TCF.
Author contributions
A Ansaripour and WR Redekop had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. A Ansaripour, HB Thio, R Maessen and WK Redekop did study concept and design. A Ansaripour, HB Thio and WK Redekop performed acquisition, analysis and interpretation of data. A Ansaripour drafted the manuscript. WK Redekop and HB Thio performed critical revision of the manuscript for important intellectual content. A Ansaripour performed the statistical analysis. WK Redekop supervised the study.
Acknowledgements
We thank W de Kort (Department of Dermatology, Amphia Hospital, Breda, The Netherlands) for his help in providing information about routine practice regarding psoriasis management in The Netherlands.
Financial & competing interests disclosure
This study was funded by Philips Light & Health in Eindhoven, The Netherlands. The funder had no influence on the design, interpretation of data, writing of the report and the decision to submit the article for publication. Funding was obtained from the Institute for Medical Technology Assessment, Institute of Health Policy & Management, Erasmus University Rotterdam. R Maessen is an official employee at Philips Lighting in Eindhoven, The Netherlands. Other authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Mason AR, Mason J, Cork M, Dooley G, Edwards G. Topical treatments for chronic plaque psoriasis CD. Cochrane Database Syst. Rev. (2), CD005028 (2009).
• This Cochrane review systematically evaluated studies of the efficacy of different topical treatments for chronic plaque psoriasis.
2.
Douglas WS, Poulin Y, Decroix J et al. A new calcipotriol/betamethasone formulation with rapid onset of action was superior to monotherapy with betamethasone dipropionate or calcipotriol in psoriasis vulgaris. Acta Derm. Venereol. 82(2), 131–135 (2002).
3.
Peeters P, Ortonne JP, Sitbon R, Guignard E. Cost-effectiveness of once-daily treatment with calcipotriol/betamethasone dipropionate followed by calcipotriol alone compared with tacalcitol in the treatment of psoriasis vulgaris. Dermatology 211, 139–145 (2005).
4.
Augustin M, Peeters P, Radtke M, Moehling U, Lapp C. Cost-effectiveness model of topical treatment of mild to moderate psoriasis vulgaris in Germany. A comparison of calcipotriol/betamethasone (Daivobet/Dovobet/Taclonex) once daily and a morning/evening non-fix combination of calcipotriol and betamethasone. Dermatology 215, 219–228 (2007).
•• Describes a cost–effectiveness analysis of topical therapies (a fix combination of calcipotriol and betamethasone compared with a nonfix calcipotriol/betamethasone combination as first-line treatment options) with a time horizon of 48 weeks in patients with mild-to-moderate psoriasis.
5.
Augustin M, Radtke M, van Engen A, Ruedig C, Lapp C, Moehling U. Pharmacoeconomic model of topical treatment options of mild to moderate psoriasis vulgaris in Germany. J. Dtsch. Dermatol. Ges. 7(4), 329–338 (2009).
6.
Dovobet leaflet: information for the user (2015). www.leo-pharma.nl/Admin/Public/DWSDownload.aspx?File=%2fFiles%2fFiler%2fBijsluiters%2fDovobet+gel+-+SmPC++03-Oct-2013.pdf
7.
Colombo GL, Di Matteo S, Bruno G, Girolomoni G, Vena GA. Calcipotriol and betamethasone dipropionate in the treatment of mild-to-moderate psoriasis: a cost-effectiveness analysis of the ointment versus gel formulation. Clinicoecon. Outcomes Res. 4, 261–268 (2012).
8.
Koek MBG, Buskens E, van Weelden H, Steegmans PHA, Bruijnzeel-Koomen CAFM, Sigurdsson V. Home versus outpatient ultraviolet B phototherapy for mild to severe psoriasis: pragmatic multicentre randomised controlled non-inferiority trial (PLUTO study). BMJ 338(7704), 1181–1186 (2009).
•• Evaluated the effectiveness and quality of life of home UVB phototherapy versus conventional outpatient UVB phototherapy.
9.
Pfaff S, Liebmann J, Born M, Merk HF, von Felbert V. Prospective randomized long-term study on the efficacy and safety of UV-free blue light for treating mild psoriasis vulgaris. Dermatology 231, 24–34 (2015).
•• Evaluated the safety and efficacy of long-term UV-free blue-light therapy at home for mild psoriasis.
10.
Philips launches BlueControl, the world’s first wearable blue LED light therapy device to treat skin disease psoriasis vulgaris. www.newscenter.philips.com/main/standard/news/press/2014/20140930-philips-launches-bluecontrol.wpd#.VqtnGvkrKHs
11.
Langley RGB, Gupta A, Papp K, Wexler D, Østerdal ML, Ćurčić D. Calcipotriol plus betamethasone dipropionate gel compared with tacalcitol ointment and the gel vehicle alone in patients with psoriasis vulgaris: a randomized, controlled clinical trial. Dermatology 222, 148–156 (2011).
12.
Cameron H, Dawe RS, Yule S, Murphy J, Ibbotson SH, Ferguson J. A randomized, observer-blinded trial of twice vs. three times weekly narrowband ultraviolet B phototherapy for chronic plaque psoriasis. Br. J. Dermatol. 147(5), 973–978 (2002).
13.
Henseler T, Schmitt-Rau K. A comparison between BSA, PASI, PLASI and SAPASI as measures of disease severity and improvement by therapy in patients with psoriasis. Int. J. Dermatol. 47(10), 1019–1023 (2008).
14.
Langley RGB, Feldman SR, Nyirady J, van DK, Papavassilis C. The 5-point Investigator’s Global Assessment (IGA) Scale: a modified tool for evaluating plaque psoriasis severity in clinical trials. J. Dermatol. Treat. 26(1), 23–31 (2015).
15.
Zorginstituut Nederland (2017). www.medicijnkosten.nl/stap3.asp?modus=2&zoek=dovobet&art=3234821
16.
17.
Koek MBG, Sigurdsson V, van Weelden H, Steegmans PHA, Bruijnzeel-Koomen CAFM, Buskens E. Cost effectiveness of home ultraviolet B phototherapy for psoriasis: economic evaluation of a randomised controlled trial (PLUTO study). BMJ 340, c1490 (2010).
18.
Nederland Zorginstituut. Guideline for conducting economic evaluations in healthcare (2017). https://english.zorginstituutnederland.nl/binaries/zinl-eng/documents/reports/2016/06/16/guideline-for-economic-evaluations-in-healthcare/Guideline+for+economic+evaluations+in+healthcare.pdf
19.
Kragballe K, Austad J, Barnes L et al. A 52-week randomized safety study of a calcipotriol/betamethasone dipropionate two-compound product (Dovobet/Daivobet/Taclonex) in the treatment of psoriasis vulgaris. Br. J. Dermatol. 154(6), 1155–1160 (2006).
20.
Briggs A, Sculpher M, Buxton M. Uncertainty in the economic evaluation of health care technologies: the role of sensitivity analysis. Health Econ. 3(2), 95–104 (1994).
21.
Halpern EF, Weinstein MC, Hunink MGM, Gazelle GS. Representing both first- and second-order uncertainties by Monte Carlo simulation for groups of patients. Medical Decision Making 20(3), 314–322 (2000).
22.
Fenwick E, Byford S. A guide to cost-effectiveness acceptability curves. Brit. J. Psych. 187(2), 106–108 (2005).
23.
Kaufmann R, Bibby AJ, Bissonnette R et al. A new calcipotriol/betamethasone dipropionate formulation (Daivobet) is an effective once-daily treatment for psoriasis vulgaris. Dermatology 205(4), 389–393 (2002).
24.
Ortonne J, Kaufmann R, Lecha M, Goodfield M. Efficacy of treatment with calcipotriol/betamethasone dipropionate followed by calcipotriol alone compared with tacalcitol for the treatment of psoriasis vulgaris: a randomised, double-blind trial. Dermatology 209, 308–313 (2004).
25.
Fleming C, Ganslandt C, Guenther L et al. Calcipotriol plus betamethasone dipropionate gel compared with its active components in the same vehicle and the vehicle alone in the treatment of psoriasis vulgaris: a randomised, parallel group, double-blind, exploratory study. Eur. J. Dermatol. 20(4), 465–471 (2010).
26.
Kragballe K, Austad J, Barnes L et al. Efficacy results of a 52-week, randomised, double-blind, safety study of a calcipotriol/betamethasone dipropionate two-compound product (Daivobet/Dovobet/Taclonex) in the treatment of psoriasis vulgaris. Dermatology 213, 319–326 (2006).
• Evaluated the clinical efficacy of two different treatment regimens involving the two-compound product (Dovobet®) over a 52-week period.
27.
Robinson A, Kardos M, Kimball AB. Physician Global Assessment (PGA) and Psoriasis Area and Severity Index (PASI): why do both? A systematic analysis of randomized controlled trials of biologic agents for moderate to severe plaque psoriasis. J. Am. Acad. Dermatol. 66(3), 369–375 (2012).
28.
Kontochristopoulos G, Kouris A, Chantzaras A, Petridis A, Yfantopoulos J. Improvement of health-related quality of life and adherence to treatment with calcipotriol-betamethasone dipropionate gel in patients with psoriasis vulgaris. An. Bras. Dermatol. 91(2), 160–166 (2015).
29.
Versteegh MM, Vermeulen KM, Evers SM, de Wit GA, Prenger R, Stolk EA. Dutch tariff for the five-level version of EQ-5D. Value Health 19(4), 343–352 (2016).
• Provides a report on the EQ-5D-5L valuation study in The Netherlands and an algorithm that can be used to attach values to all 3125 health states for use in economic evaluations.
30.
Zwaap J, Knies S, van der Meijden C, Staal P, van der Heiden L. Cost-Effectiveness in Practice. National Healthcare Institute, Diemen, The Netherlands (2015).
31.
Eastman WJ, Malahias SF, Delconte JF, DiBenedetti D. Assessing attributes of topical vehicles for the treatment of acne, atopic dermatitis, and plaque psoriasis. Cutis 94(1), 46–53 (2014).
32.
Alinia H, Moradi Tuchayi S, Smith JA et al. Long-term adherence to topical psoriasis treatment can be abysmal: a one-year randomized intervention study using objective electronic adherence monitoring. Br. J. Dermatol. 176(3), 555–837 (2016).
33.
Augustin M, Radtke M, van Engen A, Ruedig C, Lapp C, Moehling U. Pharmacoeconomic model of topical treatment options of mild to moderate psoriasis vulgaris in Germany. J. Dtsch. Dermatol. Ges. 7(4), 329–338 (2009).
34.
Affleck AG, Bottomley JM, Auland M, Jackson P, Ryttov J. Cost effectiveness of the two-compound formulation calcipotriol and betamethasone dipropionate gel in the treatment of scalp psoriasis in Scotland. Curr. Med. Res. Opin. 27(1), 269–284 (2011).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 28 April 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The cost–effectiveness of blue-light therapy in the treatment of mild-to-moderate psoriasis. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0007
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Aleksandra Werner, Anna Erkiert-Polguj, Elzbieta Budzisz, The two faces of blue light: From treating inflammation to causing oxidative stress in the skin, Biomedicine & Pharmacotherapy, 10.1016/j.biopha.2025.118442, 191, (118442), (2025).
- Pimsiri Ngowwatana, Naruepon Kampa, Somphong Hoisang, Suvaluk Seesupa, Duangdaow Khunbutsri, Saikam Chaimongkol, Preenun Jitasombuti, Supranee Jitpean, Thanikul Srithunyarat, Chalermkwan Nonthakotr, Nitaya Boonbal, Piyasak Wipoosak, Duangdaun Kaenkangploo, Selective bactericidal efficacy of 465-nm blue light phototherapy against standard and canine wound pathogens: An in vitro evaluation, Veterinary World, 10.14202/vetworld.2025.2064-2071, (2064-2071), (2025).
- Chen Fengchao, Zhang Siya, Yan Tongtong, Wang Hongquan, Li Jie, Wang Qiang, Subhan Danish, Li Kun, The enhanced cytotoxicity on breast cancer cells by Tanshinone I-induced photodynamic effect, Scientific Reports, 10.1038/s41598-023-43456-5, 13, 1, (2023).
- Shae D. Morgan, Deborah Yoder-Himes, Douglas Jackson, John Naber, Rachel Berry, Elizabeth Cash, Swapna Chandran, Thomas Roussel, Bactericidal effects of high-energy visible light on common otitis media pathogens, Journal of Applied Microbiology, 10.1111/jam.15366, 132, 3, (1856-1865), (2022).
- Li Juan, Wei Diandian, Wang Jianfeng, Li Ning, Fan Yuchen, Li Na, Zhao Sijie, Li Kun, Sun Fengyuan, Efficient Anticancer Effect on Choroidal Melanoma Cells Induced by Tanshinone IIA Photosensitization, Photochemistry and Photobiology, 10.1111/php.13399, 97, 4, (841-850), (2021).
- Giovanni Cannarozzo, Steven Paul Nisticò, Keyvan Nouri, Mario Sannino, Giovanni Cannarozzo, Steven Paul Nisticò, Keyvan Nouri, Mario Sannino, Blue Light Therapy, Atlas of Lasers and Lights in Dermatology, 10.1007/978-3-030-31232-9_16, (81-86), (2020).