A stakeholder-informed randomized, controlled comparative effectiveness study of an order prescribing intervention to improve colony stimulating factor use for cancer patients receiving myelosuppressive chemotherapy: the TrACER study
Abstract
Colony stimulating factors (CSF) are widely prescribed to avoid febrile neutropenia (FN) among cancer patients receiving chemotherapy, but studies show their use is often not consistent with practice guidelines. In addition, there is limited high quality evidence assessing benefits and harms of primary prophylactic-CSF (PP-CSF) in the setting of chemotherapy that poses an intermediate risk of FN. To address these issues, with funding from the Patient Centered Outcomes Research Institute (PCORI) and the National Cancer Institute's Community Oncology Research Program, SWOG is sponsoring a prospective, cluster randomized controlled pragmatic trial of an automated order entry protocol for PP-CSF among patients with breast, lung and colorectal cancer receiving myelosuppressive chemotherapy, with a nested randomized controlled trial of PP-CSF for patients receiving intermediate risk chemotherapy. Primary outcomes include adherence to practice guidelines, overall rates of FN and rates of FN among persons receiving intermediate risk chemotherapy. The study, the first pragmatic trial in the National Cancer Institute's cancer cooperative clinical trials network, will provide critical evidence to inform physician and patient decision-making around PP-CSF use and practice policies regarding automated orders in cancer components.
First draft submitted: 17 January 2017; Accepted for publication: 21 April 2017; Published online: 7 July 2017
Complications during chemotherapy are a major source of morbidity, mortality and cost for cancer patients. Among the nearly 600,000 US patients who will be diagnosed with breast, colorectal or lung cancer in 2016 [1], nearly half will be offered chemotherapy. Many of these therapies have a risk of neutropenic complications including febrile neutropenia (FN). Patients with FN are typically hospitalized, and nearly 8% of those hospitalized for FN die [2]. Colony-stimulating factors (CSFs) can be used to maintain the white blood cell count, and are commonly used to reduce the risk of FN, as well as its severity and duration.
Oncology practice guidelines recommend prophylactic administration of CSFs with the first chemotherapy cycle – termed primary prophylactic-CSF (PP-CSF) use – for chemotherapy regimens that carry a high risk of causing FN in patients who receive them (high risk is defined as >20% chance of developing FN). Further, the guidelines state to consider PP-CSF for patients receiving chemotherapy with an intermediate risk (10–20%) of FN and not use PP-CSF for patients receiving chemotherapy with low-risk (<10%) of FN [3,4]. Although practice guidelines for PP-CSF have been available for nearly two decades, multiple studies show that between 55 and 95% of PP-CSF prescribing is inconsistent with them [3–11]. These studies show both underuse for high-risk regimens (where PP-CSF is recommended) and overuse of PP-CSF for low-risk chemotherapy (where PP-CSF is not recommended). A contributor to PP-CSF prescribing variability is the limited high quality evidence assessing the effectiveness of PP-CSF for patients receiving intermediate-risk chemotherapy regimens. Pivotal trials evaluating the effectiveness of PP-CSF in reducing FN are more than two decades old [12,13], and few studies have evaluated their effectiveness among patients with solid tumors receiving modern chemotherapy, the majority of which are considered intermediate risk regimens.
To address these questions, we designed a pragmatic, prospective, randomized controlled trial to address two important unmet needs for PP-CSF prescribing: first, whether a guideline-informed standing order for administering PP-CSF could improve prescribing and reduce the incidence of FN when compared with usual care, and second, for patients receiving intermediate risk chemotherapy, to determine the impact of PP-CSF on FN. In addition to these primary objectives, the study has several secondary objectives focused on the impact of the intervention on patient-centered outcomes; for example, health-related quality of life, knowledge of the benefits and risks of CSF, adherence to chemotherapy, adverse events such as emergency department visits and hospitalizations, and survival.
Because CSF prescribing is influenced by patients, health insurance policies and practice guidelines, an important feature of our study was its intent to inform the design with key stakeholders from these communities. In this paper, we describe and discuss the design features of the TrACER study (A pragmatic Trial Assessing CSF prescribing Effectiveness and Risk), a prospective, cluster randomized pragmatic trial designed to improve PP-CSF prescribing and improve the evidence base supporting its effectiveness and use.
Methods
Setting
TrACER was developed in response to the Patient Centered Outcomes Research Institute's (PCORI's) Large Pragmatic Trials initiative [14]. The study is being conducted by SWOG through the National Cancer Institute (NCI) Community Oncology Research Program (NCORP) network [15] in components funded to sponsor Cancer Care Delivery Research (CCDR) studies. The NCORP sites include community hospitals and physicians funded by a peer-reviewed cooperative agreement to participate in NCI-sponsored cancer treatment, prevention and control trials. The NCORP component network includes 34 community sites, 12 minority/underserved community sites (bases comprised of institutions with a 30% or greater minority cancer patient population) and seven research bases. A component may be a single institution or a hospital with several satellite components, or a grouping of institutions, hospitals and components. Within the NCORP network of 842 components and subcomponents are 1565 NCORP investigators representing all oncology specialties who actively recruit patients into cancer prevention, treatment and control studies.
Within the NCORP network are more than 200 components funded for CCDR. CCDR encompasses a multidisciplinary field of scientific investigation. It examines how social factors, financing systems, organizational structures and processes, health technologies, and healthcare provider and individual behaviors affect cancer outcomes, access to and quality of care, cancer care costs, and the health and well-being of cancer patients and survivors [16].
Trial objectives
This study has three intertwined primary objectives: to determine the impact of the PP-CSF order entry system on PP-CSF prescribing; overall rates of FN for patients receiving myelosuppressive chemotherapy within 6 months of registration; and the rate of FN among intermediate risk patients within 6 months of registration. In addition to a standing order PP-CSF intervention arm and a control (usual care) arm, the study also includes a cohort arm, an observational study of component sites with existing PP-CSF order entry systems, and thus ineligible for randomization. The objective for the cohort study is to compare patterns of PP-CSF prescribing and outcomes in component sites with existing (and variable) PP-CSF order entry systems to the PP-CSF order entry system implemented in the intervention arm of the trial. Box 1 lists all primary and secondary objectives of the TrACER study.
Trial design
This trial compares the effectiveness of a guideline-based, standing order PP-CSF intervention to usual care. The unit of randomization for this study is an NCORP CCDR component site, as described above where all hospitals or clinics operating as part of that component share the same electronic medical record (EMR). CCDR component sites that have not yet adopted a PP-CSF ordering system used for high, intermediate and low risk regimens are eligible for randomization to either the intervention or control (usual care) arm. The intervention consists of standing orders for administering PP-CSF within 24–48 h following the first cycle of chemotherapy, based on the myelosuppressive risk of each chemotherapy regimen, as specified by the National Comprehensive Cancer Network Guidelines; in cases where National Comprehensive Cancer Network Guidelines do not assign FN risk for a regimen, information from the package labels of the chemotherapy regimens were used to determine risk. In the usual care arm, PP-CSF prescribing will remain as currently prescribed by the oncologists and their component staff (no change to standing orders). Component sites which already have existing CSF order entry systems are assigned to a nonrandomized observational cohort arm. All patients at participating components will be subject to the PP-CSF use care as determined by component assignment (usual care, intervention or cohort); physician discretion will determine the actual care received by patients. Only consented patients registered to the study will participate in the data collection. Figure 1 provides an overview of the trial design.
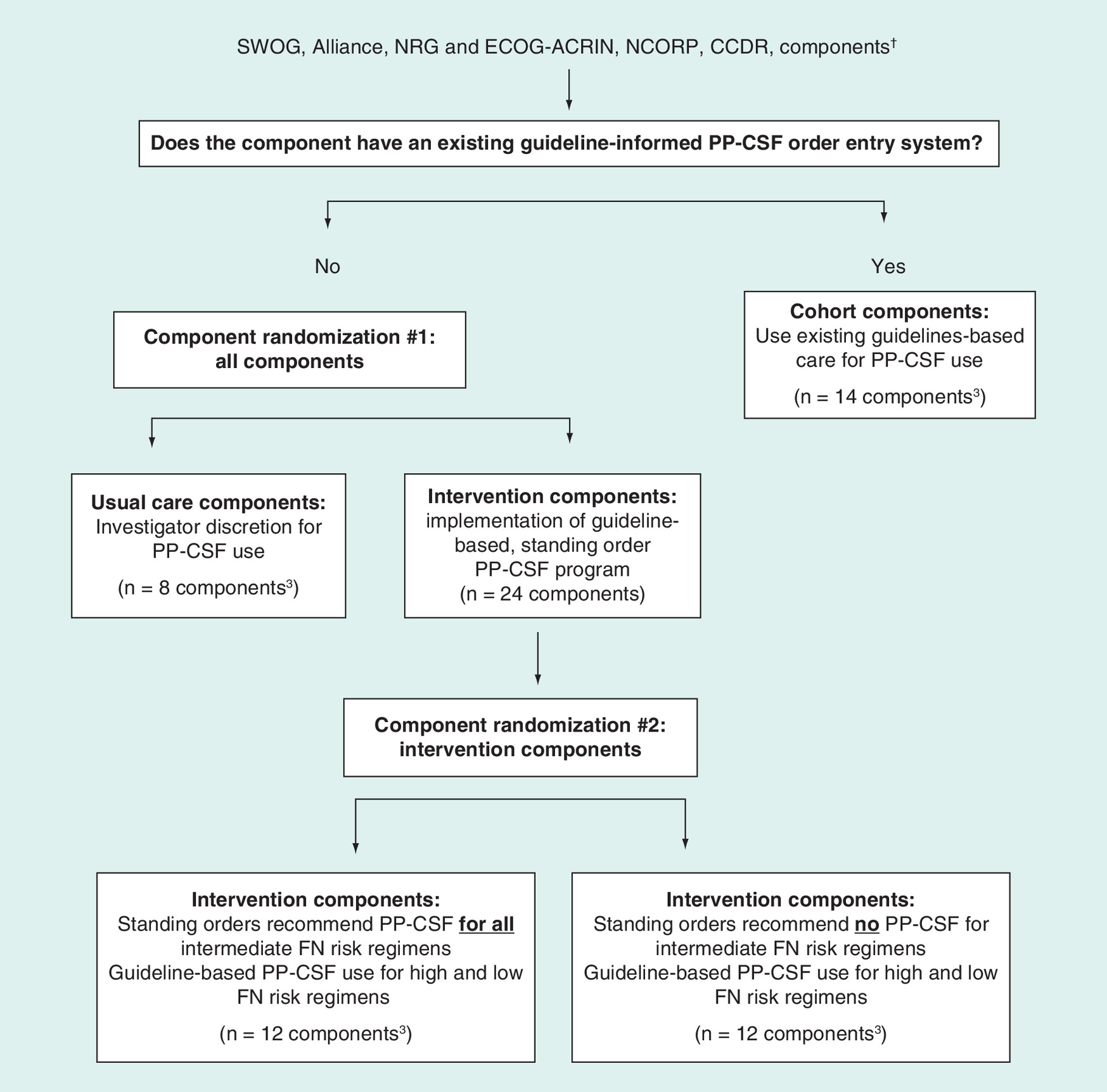
Figure 1. Study overview and randomization scheme.
†See text for a description of National Cancer Institute Community Oncology Research Program components.
CCDR: Cancer Care Delivery Research; FN: Febrile neutropenia; NCORP: National Cancer Institute Community Oncology Research Program; PP-CSF: Primary prophylactic-colony stimulating factor.
To maximize recruitment efficiency, very low volume components (chemotherapy administered to less than 60 [total] breast, lung or colorectal cancer patients annually) are excluded. Components are randomly assigned into the intervention or usual care group using a 3:1 randomization scheme.
Among component sites randomized to the intervention group in the primary randomization, a secondary component-level randomization (1:1) is performed to evaluate the effectiveness of PP-CSF among patients receiving intermediate risk chemotherapy. In the first intervention group, the standing orders for all intermediate risk chemotherapy regimens will include PP-CSF. The second intervention group will have standing orders that do not include PP-CSF with intermediate risk chemotherapy regimens.
Inclusion & exclusion criteria: components & patients
The inclusion and exclusion criteria are minimally restrictive to reflect the pragmatic nature of the trial design (Box 2).
Intervention: automated standing CSF order entry
To implement the automated PP-CSF order entry system across a variety of EMR platforms, the research team staff includes persons with expertise in biomedical informatics to help sites modify their platforms to allow for both medical orders and extraction of relevant data. The team will engage component EMR technical staff to implement the protocol-based PP-CSF orders, and physicians, nurses and pharmacists, to assure feasibility and accuracy of order changes (Box 3).
The protocol PP-CSF orders will be customized to the capabilities of each component, taking into account the procedures by which chemotherapy orders are administered by the staff and how chemotherapy is given to participants. Physician, nurse, pharmacy and information technology leaders at participating components will be asked to help develop an implementation blueprint within each component as part of the rollout of the intervention. To facilitate the analysis and implementation at local sites we provide basic requirements, as well as screenshots of examples for new order sets in commonly used EMR systems upon request.
Hypotheses & sample size considerations
Funding considerations allowed for a maximum of 32 components in the randomized trial, which we allocated as 24 intervention components and eight usual care components to achieve sufficient power. The number of patients per component was calculated to ensure ≥80% power for the three primary objectives. Because FN events are less common among intermediate risk patients, we estimated sample size using a two-step approach. First, we calculated the sample size required to test the hypothesis that PP-CSF would result in a 50% reduction in FN rate among intermediate risk patients, based on prior studies in other FN risk groups [17]. Based on an expected baseline FN rate of 15% among persons receiving intermediate risk chemotherapy [5–6,18–22] and for α = 0.05, among the 24 components in the intervention group, 12 will be randomized to all intermediate risk chemotherapy patients being assigned PP-CSF, and 12 will be randomized to no intermediate risk patients receiving PP-CSF. Assuming that among patients receiving chemotherapy at each component, the proportion of high, intermediate and low risk patients is 30, 50 and 20%, respectively, a total of 90 breast, lung or colorectal cancer patients are needed per component to test the hypothesis [7,8].
Second, we hypothesize that patients receiving high and intermediate risk chemotherapy in intervention components will experience FN rates that are 50% lower than patients receiving high and intermediate risk chemotherapy in usual care components. Assuming a baseline FN risk of 25% among patients receiving high risk chemotherapy, a 3:1 randomization scheme (eight components randomized to usual care and 24 components randomized to intervention) will provide 90% power for testing this hypothesis. Finally, our sample size results in 80% power to detect the following changes in PP-CSF prescribing rates as a result of the order entry intervention: a reduction from 17 to 7% among low risk patients and an increase from 40 to 75% among high-risk patients [8]. The trial will thus include a total of 2980 eligible patients in the randomized study: 2160 in the intervention arm; 720 in the usual care arm. We will allow for 10% additional accrual to account for ineligible patients, and for dropout and death (not due to FN) that may occur earlier than 6 months after registration.
Intraclass correlation coefficient (ICC): The above calculations account for a possible reduction in power due to correlation among patients at the same component. An ICC of zero corresponds to randomization of individuals rather than components; ICC >0 indicates correlation among patient outcomes within a component. We estimated the ICC for FN in the SWOG adjuvant breast cancer study S0221, which had 262 components with 2666 patients [23]. The ICC for that study was estimated to be 0.01; we used 0.02 to protect against underestimation.
The parallel observational cohort study will include 14 components with existing PP-CSF order entry systems (720 eligible patients, about 52 eligible patients per component).
Analysis plan
Intent-to-treat
Randomization is at the component level and outcomes are measured at the patient level. There may be nonadherence to the assigned treatment (intervention or usual care) at the component or patient level. The primary analysis will be based on an intent-to-treat analysis, which analyzes patients and components according to the arms to which they were randomly assigned. As a sensitivity analysis, we will account for nonadherence and conduct an as-treated analysis. In order to understand any differences between results from the intent-to-treat and as-treated analyses and to assess the extent to which noncompliant components and patients may have biased results, we will compare their characteristics to those of all other components and patients in the analysis.
Analysis for primary aims
Since patients are nested within components, this structure will be accounted for by using mixed effects regression models including a random effect for component. Among high risk and low risk patients, separate mixed effects logistic models will be fit to assess the effect of the intervention on PP-CSF use. A mixed effects logistic model will also be used to assess the impact of the intervention on FN occurrence within 6 months from registration. In all analyses, there will be adjustment for component-level characteristics and patient-level clinical and demographic characteristics.
Subgroup analysis
We will assess the magnitude of intervention effect across subgroups. We will use interaction tests and a forest plot to display the heterogeneity in intervention effects across subgroups. Subgroup analyses will be performed for each cancer type, level of FN risk (low, intermediate, high), and the following variables: race (African–American, White, other), age (categorized as <50, 50–59, 60–69, 70–79, 80+ years), noncancer comorbidity performance status (Zubrod) and stage of cancer at enrollment (distant, local, regional) [6,9,11,18–23].
Interim analysis
Early termination of part of the secondary trial (e.g., a single arm) in intermediate risk patients may occur due to demonstrated efficacy or futility of PP-CSF in an interim analysis of FN incidence. Two interim analyses will be conducted when 360 patients and 650 patients in the intermediate risk group at intervention components have complete outcome information; these sample sizes correspond to 50 and 75% accrued information. We will use O'Brien–Fleming stopping rules, which employ conservative criteria for termination [24]. The trial will be monitored by the SWOG Data Safety Monitoring Committee, with respect to accrual, adverse events, and interim and final analyses.
External stakeholder advisory group involvement in trial design
A key component of patient-centered outcomes research is the integration of perspectives from external stakeholders who represent constituencies that will be affected by research findings into the trial design process [4]. We assembled an external stakeholder advisory group (ESAG), chaired by two members of the study team (SD Sullivan and GH Lyman) to advise on trial design, implementation and dissemination. The ESAG includes representatives from patient advocacy groups, clinicians, health insurers, test manufacturers, regulators and policy-makers (Figure 2).
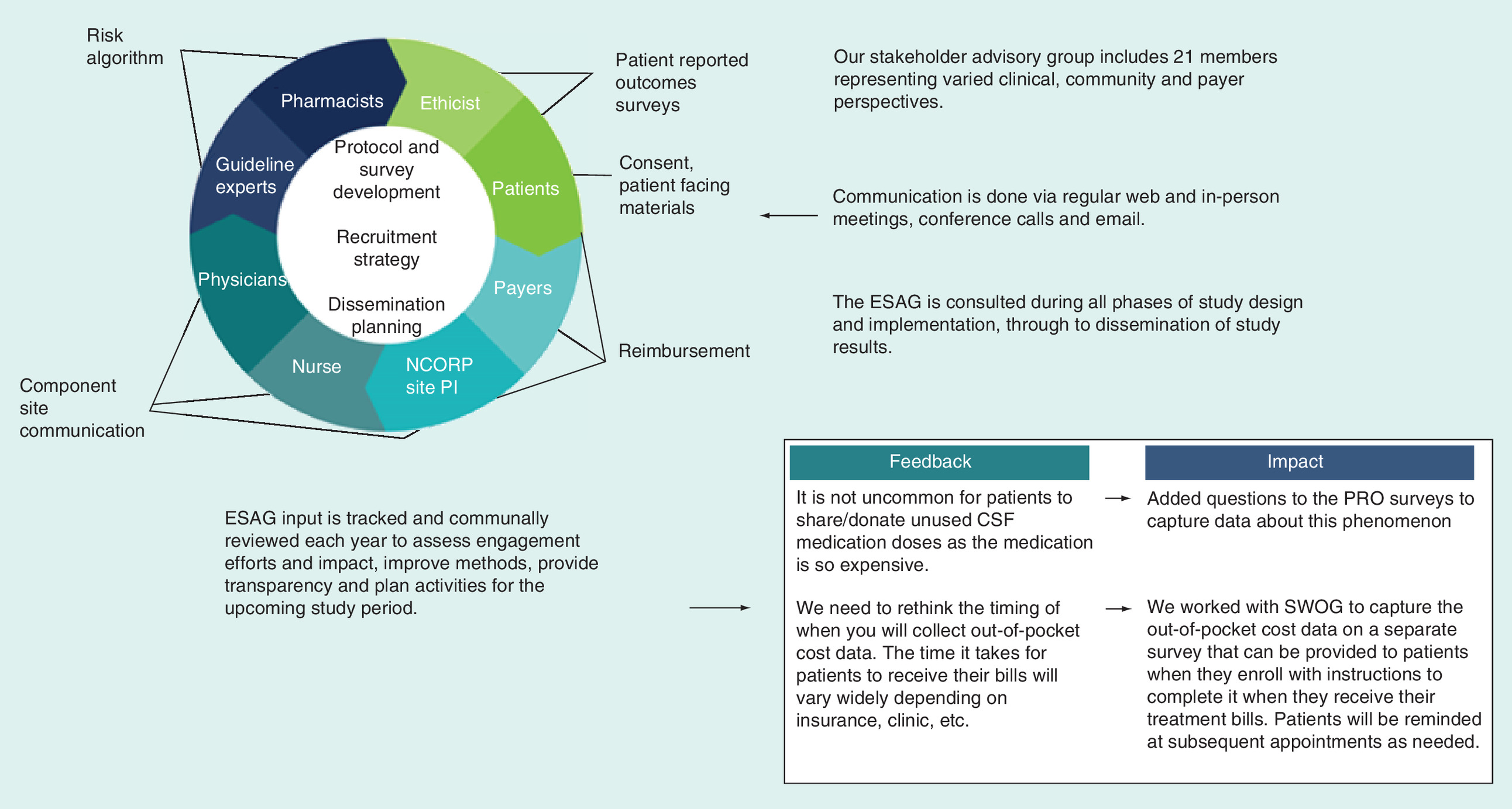
Figure 2. External stakeholder advisory group member representation and study engagement.
CSF: Colony stimulating factor; ESAG: External stakeholder advisory group; PRO: Patient-reported outcomes.
Engagement with the ESAG started from the point of writing the grant proposal. The ESAG provided input and feedback on formulation of the research questions, reviewing the intervention, study design, setting, patient populations, recruitment procedures and end points for the study, as well as reviewing the intervention to help determine relevance to patients, feasibility and potential impact.
The ESAG was convened at separate webinars for orientation to the goals of the trial, introduced to the study team and each other, provided an overview of the proposed engagement plan, and given an opportunity to comment on their proposed role in the study. The group was asked to help refine the research questions and outcomes to be relevant to patients, payers and other stakeholders. In addition, members with experience were asked to share their knowledge about PP-CSF prescribing, the prevalence of over- and underuse, risks of treatments and potential challenges to support of the dissemination of trial findings, such as language to frame the context for a research study that may result in less use of a treatment in certain patient populations. ESAG feedback was used to revise, refine and strengthen the study design.
Discussion
Prospective randomized controlled trials provide the highest quality evidence to address questions of comparative benefit and safety. For questions that can be addressed effectively with pragmatic trial methods, an infrastructure must be available to generate credible, representative information as quickly, efficiently and inexpensively as possible. In response to PCORI's Large Pragmatic Trials initiative, the TrACER study was designed to address two fundamental issues for PP-CSF prescribing: lack of adherence to long-published practice guidelines for use of PP-CSF for patients receiving myelosuppressive chemotherapy; and limited evidence regarding the effectiveness of PP-CSF among patients receiving chemotherapy with an intermediate FN risk. The combination of PCORI's approach to stakeholder-informed research design and the NCI's NCORP infrastructure offers a compelling combination for addressing critical needs in oncology such as PP-CSF prescribing in a timely fashion with a high evidence standard.
The TrACER trial represents several ‘firsts’: the first pragmatic trial in an NCI cancer cooperative group setting, the first cluster-randomized trial in SWOG and the first wave of large pragmatic trials funded by PCORI. TrACER also provides an avenue for collaboration between the NCI and PCORI in a way that leverages both organizations’ resources, in this case to address a major issue for cancer care delivery research as well as an area of clinical uncertainty. In an era of constrained budgets for research, pragmatic trials hold promise as a lower cost alternative to address important questions in these areas.
The TrACER study concept proposal was approved by SWOG on 19 August 2014. PCORI initiated the study contract on September 1st 2015 following approval for funding in February 2015. The NCI protocol was approved on February 16th 2016 and the study was activated on October 7th 2016. In November 2016 the first component site randomized to the intervention arm completed the process to modify their EMR to include protocol-indicated standing orders. The first patient was registered on October 26th 2016. Planned patient enrollment is expected to continue through March 2019, with primary analysis scheduled for completion on July 31st 2020.
Primary objectives
To compare the use of primary prophylactic-colony stimulating factor (PP-CSF) according to recommended clinical practice guidelines among patients registered at intervention components versus usual care components.
To compare the rate of febrile neutropenia (FN) among patients registered at intervention components versus those providing usual care.
To compare the rate of FN among intermediate risk patients registered at intervention components by component treatment assignment (administer PP-CSF to intermediate risk patients vs not).
Secondary objectives
To compare the rate of FN among low-risk patients registered at intervention components versus those providing usual care.
To compare the FN-related health-related quality of life (HRQL) among low-risk patients registered at intervention components versus usual care components.
To compare patient adherence to PP-CSF prescribing among patients registered at intervention components versus usual care components.
To compare patient knowledge of the indications for, efficacy of, and side effects associated with PP-CSF between the initiation and conclusion of the first cycle of myelosuppressive systemic therapy among patients registered at intervention components versus usual care components.
To compare the proportion of patients completing the initial systemic therapy regimen at planned duration and at planned dose intensity among patients registered at intervention components versus usual care components.
To compare antibiotic use both as prophylaxis and as treatment for FN among patients registered at intervention components versus usual care components.
To compare the rate of FN-related emergency department visits and hospitalizations among intermediate risk patients registered to intervention components by component treatment assignment (administer PP-CSF to intermediate risk patients vs not).
To compare the FN-related HRQL among intermediate risk patients registered to intervention components by component treatment assignment (administer PP-CSF to intermediate risk patients vs not).
To compare overall survival among intermediate risk patients registered to intervention components by component treatment assignment (administer PP-CSF to intermediate risk patients vs not).
Additional objectives
To characterize and descriptively report the differences among cohort components and the intervention and usual care components, according to the end points outlined in Section 10.0.
To evaluate the time to invasive recurrence in nonmetastatic patients by component treatment assignment.
Component site eligibility
Minority-Underserved National Cancer Institute Community Oncology Research Program Cancer Care Delivery Research (MU-NCORP CCDR) oncology component sites. A component is a NCORP designated unit comprised of a single institution or a hospital with satellite clinics, or a grouping of institutions, hospitals and clinics.
At least 60 breast, non-small-cell lung and colorectal cancer patients (total) received chemotherapy in 2015.
Technically and logistically feasible to modify the existing clinic order entry system to include the protocol-indicated order set and system notes for colony stimulating factor (CSF).
Component site is willing to undergo secondary randomization to include/exclude CSF standing orders for intermediate risk regimens.
Patient eligibility
Disease-related criteria:
Patients must have a current diagnosis of breast cancer, non-small-cell lung cancer or colorectal cancer. Cancer may be metastatic or nonmetastatic.
Prior/concurrent therapy criteria:
Patients must be planning to receive one of the study-allowed regimens as their initial treatment for their current diagnosis.
Patients must be registered prior to their first cycle of systemic therapy (chemotherapy, immunotherapy, biologic therapy or combination regimens) for this diagnosis. If patient has had any prior systemic therapy for another malignancy, patient must not have had any systemic therapy in the 180 days just prior to registration.
Patients must not have any known contraindication to CSFs prior to registration, including prior hypersensitivity to Escherichia coli-derived proteins, filgrastim, pegfilgrastim or Tbo-filgrastim.
Clinical criteria
Patient must be at least 18 years of age.
Patients must be able to understand and provide information for the patient-completed study forms in either English or Spanish.
Patients may have had a prior malignancy.
Patients must not be participating or plan to participate in other clinical trials that involve investigational systemic cancer treatments or investigational uses of CSF.
Regulatory criteria
Patients must be informed of the investigational nature of this study and must sign and give written informed consent in accordance with institutional and federal guidelines.
As a part of the OPEN registration process the treating institution's identity is provided in order to ensure that the current (within 365 days) date of institutional review board approval for this study has been entered in the system.
Step 1: Discovery & planning
Component site establishes a local project implementation team including specialists such as clinical analysts, order set developers, and clinical pharmacists.
A Trial assessing CSF prescribing Effectiveness and Risk (TrACER) research team works with the local team to map out the local processes for modifying the order sets. Component site is asked to complete a clinic characterization survey to help the research team understand the characteristics of the existing electronic medical record and specific technical and environmental challenges.
Key local implementation contacts and stakeholders are identified and consulted by the project team. Early questions and concerns are addressed.
Step 2: Establish intervention blueprint
Verify which clinical systems need to be modified (e.g., EPIC, Cerner, Allscripts).
Work with local analyst, clinical pharmacist and other key staff to confirm clinical requirements and the impact of the protocol-indicated changes.
Work with local analyst and IT staff to determine technical requirements.
Design build specifications.
Step 3: Analyst mock-up & testing: central review & approval of changes
Changes are made by local project implementation team or a technical consultant provided by the research team.
Changes are piloted in ‘off line’ mode and revised as needed.
Local project implementation team submits a completed implementation form and screenshots of the build to the research team for review.
The research team change-control board reviews the component site build documentation and approves the changes or recommends additional revisions that must be made before the site can implement the changes in a live clinic environment.
Step 4: Implement changes in production clinical systems environment
Protocol-indicated standing orders are in active use.
Local project implementation team monitors for issues, reporting to research team if questions or issues arise.
Systems are modified as appropriate based on feedback and issues encountered during the run-in.
Multiple studies show that between 55 and 95% of primary prophylactic colony-stimulating factor (PP-CSF) prescribing is inconsistent with established clinical guidelines. A contributor to the variability of CSF prescribing is limited high quality evidence assessing the effectiveness of PP-CSF for patients receiving intermediate risk chemotherapy regimens.
Trial Assessing CSF Prescribing Effectiveness and Risk (TrACER) is a pragmatic, prospective, randomized controlled trial to address two important unmet needs for PP-CSF prescribing: first, whether a guideline-informed standing order for administering PP-CSF could improve prescribing and reduce the incidence of febrile neutropenia when compared with usual care, and second, for patients receiving intermediate risk chemotherapy, to determine the impact of PP-CSF on febrile neutropenia.
The study uses a cluster randomized design. The unit of randomization is an National Cancer Institute Community Oncology Research Program designated Cancer Care Delivery component site. All hospitals or clinics operating as part of a component site share the same electronic medical record.
There are four study arms. Component sites with existing CSF order entry systems are assigned to a nonrandomized observational cohort arm (study group 1). Component sites with no existing CSF order entry system are randomized into one of three arms – one usual care arm and two intervention arms. In the usual care arm (study group 2), PP-CSF prescribing will remain as currently configured by the oncologists and their component staff. In the intervention arms, components will alter their electronic medical record to standing orders for PP-CSF based on the myelosuppressive risk of each chemotherapy regimen, as specified by the National Comprehensive Cancer Network guidelines. In study group 3, all patients receiving intermediate risk regimens will have standing orders to receive CSF. In study group 4, patients receiving intermediate risk chemotherapy regimens will not have standing orders for CSF.
14 components are participating in the cohort study. 32 components are participating in the randomized trial: 24 intervention components and eight usual care components. The number of patients per component was calculated to ensure ≥80% power for the three primary objectives.
As a key component for patient-centered outcomes research, an External Stakeholder Advisory Group had advised the investigator team on trial design, implementation and dissemination. The group includes representatives from patient advocacy groups, clinicians, health insurers, test manufacturers, regulators and policy-makers.
The TrACER trial represents the first pragmatic trial in an NCI cancer cooperative group setting, the first cluster-randomized trial in SWOG, and the first wave of large pragmatic trials funded by Patient Centered Outcomes Research Institute.
Acknowledgements
The authors thank K Arnold for helpful comments on a previous version of this manuscript.
Disclaimers
The content of this manuscript is solely the responsibility of the authors and does not necessarily reflect the views or policies of the National Cancer Institute, nor does mention of trade names, commercial products, or organizations imply endorsement by the US Government. The views presented in this work are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute, its Board of Governors or Methodology Committee.
Financial & competing interests disclosure
Research reported in this manuscript was partially funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (PCS-1402-09988) and through the National Cancer Institute (5U10 CA180819-03 and 5UG1CA189974). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest
1.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J. Clin. 66(1), 7–30 (2016).
2.
Kuderer NM, Dale DC, Crawford J, Cosler LE, Lyman GH. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer 106(10), 2258–2266 (2006).
• Study done to better define mortality, length of stay, cost and risk factors associated with mortality and prolonged hospitalization in cancer patients with febrile neutropenia (FN).
3.
Smith TJ, Bohlke K, Lyman GH et al. Recommendations for the use of WBC growth factors: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 33(28), 3199–3212 (2015).
4.
National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Myeloid Growth Factors (2016). www.nccn.org/professionals/physician_gls/PDF/myeloid_growth.pdf.
5.
Aapro MS, Bohlius J, Cameron DA et al. 2010 update of EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphoproliferative disorders and solid tumours. Eur. J. Cancer 47(1), 8–32 (2011).
6.
Potosky AL, Malin JL, Kim B et al. Use of colony-stimulating factors with chemotherapy: opportunities for cost savings and improved outcomes. J. Natl Cancer Inst. 103(12), 979–982 (2011).
• Study evaluating colony stimulating factor (CSF) use in a multiregional population-based cohort of lung and colorectal cancer patient showing findings that suggest policies to decrease CSF use in patients at lower or intermediate risk of febrile neutropenia may yield substantial cost savings without compromising patient outcomes.
7.
Ramsey SD, Mccune JS, Blough DK et al. Colony-stimulating factor prescribing patterns in patients receiving chemotherapy for cancer. Am. J. Manag. Care 16(9), 678–686 (2010).
8.
Crawford J, Dale DC, Kuderer NM et al. Risk and timing of neutropenic events in adult cancer patients receiving chemotherapy: the results of a prospective nationwide study of oncology practice. J. Natl Compr. Canc. Netw. 6(2), 109–118 (2008).
• This study was done to describe the relationship between the occurrence and timing of neutropenic events and chemotherapy treatment and concluded that improved methods of pretreatment assessment of patient risk factors for neutropenia are needed.
9.
Schnipper LE, Smith TJ, Raghavan D et al. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: the top five list for oncology. J. Clin. Oncol. 30(14), 1715–1724 (2012).
• American Society of Clinical Oncology identifies as “don't use white cell stimulating factors for primary prevention of FN (febrile neutropenia) for patients with less than 20% risk for this complication” as one of its top five categories of tests, procedures and/or treatments whose common use and clinical value are not supported by available evidence.
10.
National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Breast Cancer (2016). www.nccn.org/professionals/physician_gls/PDF/breast.pdf.
11.
National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Non-small Cell Lung Cancer (2016). www.nccn.org/professionals/physician_gls/PDF/nscl.pdf.
12.
Crawford J, Ozer H, Stoller R et al. Reduction by granulocyte colony-stimulating factor of fever and neutropenia induced by chemotherapy in patients with small-cell lung cancer. N. Eng. J. Med. 325(3), 164–170 (1991).
• Granulocyte colony-stimulating factor as an adjunct to chemotherapy in patients with small-cell cancer of the lung led to reductions in the incidence of febrile neutropenia, in the incidence and duration of grade IV neutropenia and reduced the total number of days of treatment with IV antibiotics and hospitalization.
13.
Pettengell R, Gurney H, Radford JA et al. Granulocyte colony-stimulating factor to prevent dose-limiting neutropenia in non-Hodgkin's lymphoma: a randomized controlled trial. Blood 80(6), 1430–1436 (1992).
14.
Patient-Centered Outcomes Research Institute. Funding Announcement: Improving Methods for Conducting Patient-Centered Outcomes Research (2014). www.pcori.org/sites/default/files/PCORI-PFA-2014-Spring-PFA-Improving-Methods.pdf.
15.
NCORP: NCI Community Oncology Research Program. https://ncorp.cancer.gov/.
16.
National Cancer Institute Community Oncology Research Program. Research Areas (2016). https://ncorp.cancer.gov/research/.
17.
Kuderer NM, Dale DC, Crawford J, Lyman GH. Impact of primary prophylaxis with granulocyte colony-stimulating factor on febrile neutropenia and mortality in adult cancer patients receiving chemotherapy: a systematic review. J. Clin. Oncol. 25(21), 3158–3167 (2007).
18.
Mccune JS, Sullivan SD, Blough DK et al. Colony-stimulating factor use and impact on febrile neutropenia among patients with newly diagnosed breast, colorectal, or non-small cell lung cancer who were receiving chemotherapy. Pharmacotherapy 32(1), 7–19 (2012).
• This retrospective study to determine the impact of primary prophylactic colony-stimulating factor (PP-CSF) use on febrile neutropenia in a patient population receiving contemporary chemotherapy regimens to treat breast, colorectal or non-small-cell lung cancer showed the need for further research studies to evaluate if guideline-directed prescribing of PP-CSFs can improve clinical outcomes.
19.
Morrison VA, Wong M, Hershman D, Campos LT, Ding B, Malin J. Observational study of the prevalence of febrile neutropenia in patients who received filgrastim or pegfilgrastim associated with 3–4-week chemotherapy regimens in community oncology practices. J. Manag. Care Pharm. 13(4), 337–348 (2007).
20.
Kuderer NM, Lyman GH. Personalized medicine and cancer supportive care: appropriate use of colony-stimulating factor support of chemotherapy. J. Natl Cancer Inst. 103(12), 910–913 (2011).
21.
Smith K, Wray L, Klein-Cabral M et al. Ethnic disparities in adjuvant chemotherapy for breast cancer are not caused by excess toxicity in black patients. Clin. Breast Cancer 6(3), 260–266 (2005).
22.
Lyman GH, Kuderer NM, Crawford J et al. Predicting individual risk of neutropenic complications in patients receiving cancer chemotherapy. Cancer 117(9), 1917–1927 (2011).
23.
Zirpoli GR, Brennan PM, Hong CC et al. Supplement use during an intergroup clinical trial for breast cancer (S0221). Breast Cancer Res. Treat. 137(3), 903–913 (2013).
24.
O'Brien PC, Fleming TR. A multiple testing procedure for clinical trials. Biometrics 35(3), 549–556 (1979).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 7 July 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A stakeholder-informed randomized, controlled comparative effectiveness study of an order prescribing intervention to improve colony stimulating factor use for cancer patients receiving myelosuppressive chemotherapy: the TrACER study. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0005
Export citation
Select the citation format you wish to export for this article or chapter.