Familial clustering of atrial fibrillation and comparative longitudinal outcomes of familial and non-familial atrial fibrillation
Abstract
Several studies have suggested that family history of atrial fibrillation (AF) is an important risk factor for AF, with several specific genetic regions now implicated through Genome Wide Association Studies. In addition, familial AF is associated with earlier age of onset and affects patients with fewer comorbid conditions than their non-familial counterparts. While those with familial AF have worse symptoms, all-cause mortality and risk of thromboembolic complications are similar among familial and non-familial AF patients.
First draft submitted: 2 December 2016; Accepted for publication: 16 January 2017; Published online: 9 May 2017
Atrial fibrillation (AF) is the most common sustained arrhythmia in clinical practice [1]. Its incidence and prevalence are increasing, and in 2010 an estimated 20.9 million males and 12.6 million females were diagnosed with AF globally [2]. AF is associated with up to fivefold increased risk of thromboembolic complications [1,3–4]. This risk is reduced through treatment with antithrombotic agents, but still remains increased in comparison with those without AF [5]. Even though many risk factors for AF have been identified (e.g., advancing age, sex [male], valvular heart disease, obesity, hypertension, alcohol abuse, and heart failure), the exact pathophysiology of AF remains unknown [6–12]. Although, certain genetic factors have been linked to AF it is still uncertain to what degree a family history of AF influences both the risk of AF and subsequent outcomes.
Familial AF
In 1997, Brugada et al. screened the human genome and performed a genetic-linkage analysis in members from a large family in which AF segregated as an autosomal dominant disease. They found the disease locus for this familial form of AF to be located at chromosome 10q22-q24 [13]. Since then, several studies have identified multiple genetic regions to correlate with lone AF and AF in general [14–34]. These monogenic variants of AF are associated with large effect sizes, but the genetic variants are rare [12]. Since 2007, several large Genome Wide Association Studies (GWAS) have identified genomic regions associated with AF [35–38]. These studies compare allele and genotype frequencies of specific single nucleotide polymorphisms in AF patients and individuals without AF and identify genomic variants associated with AF. In these studies, the recognized genomic regions are more common, but have lower effect sizes than the monogenic variants of AF [12]. Since 2007, regions located on chromosomes 4q25, 16q22 and 1q21 [35–38] have been identified, and in a meta-analysis Shoemaker et al. furthermore found the chromosome 4q25 SNP rs2200733 to be significantly associated with recurrence of AF after catheter ablation for AF [39].
Recently epidemiological studies examining the magnitude of heritability in AF [40–46] have found a familial aggregation of AF and suggested a family history of AF to be an important risk factor for the development of AF. The acknowledgement of a familial form of AF should lead to considerations regarding the potential differences in the disease course in familial and non-familial AF and ultimately whether the two patient groups would benefit from different treatment strategies.
Familial clustering of AF in a nationwide cohort
In a previous study, we estimated the incidence of AF among first-degree family members to patients diagnosed with AF in the period from 1978 to 2012. We used Danish registries and thereby constructed a nationwide cohort of individuals. We sought to clarify whether a family history of AF independently and incrementally contributed to the longitudinal risk of developing AF. The study found a significantly increased risk of AF among first-degree family members to AF patients compared with the general population with the highest incidence of AF among individuals with a sibling diagnosed with AF (rate ratio of AF compared with the general population: 5.20; 95% CI: 4.61–5.85). Furthermore, this increased risk of AF seemed to be age-dependent, with higher risk of AF among those whose AF-proband was diagnosed before the age of 50 years (Figure 1) [46]. These findings were in accordance with previous studies. In 2004, Fox et al. reported an increased risk of AF among children with a parent diagnosed with AF. As in our study, this risk increased with younger age of AF diagnosis in the proband [40,46]. In 2010, Lubitz et al. reported the risk of AF in first-degree relatives to AF patients in The Framingham Heart Study, a large prospective population-based cohort study. Again, an increased risk of AF was seen in relatives to AF patients and this risk was furthermore inversely related to the age at which the first-degree family member developed AF [41]. In 2012, a Danish nationwide cohort study by Øyen et al. investigated the risk of developing lone AF before the age of 60 years when a first-degree family member was diagnosed with lone AF. The study found a family history of lone AF to be associated with a substantial risk of lone AF in first-degree family members, and again the highest risk of AF was found to be associated with young age at AF onset in the proband [45]. The mechanisms behind the increased risk of AF in family members to AF patients can possibly include genetic as well as lifestyle factors aggregated in families. The consistent findings of an increasing risk of AF to be inversely related to the age at which the proband developed AF support a genetic predisposition to AF. This is further supported by a study from 2006 by Arnar et al. that found an exponential decline in the risk of AF in relatives to AF patients by degree of relatedness [43].
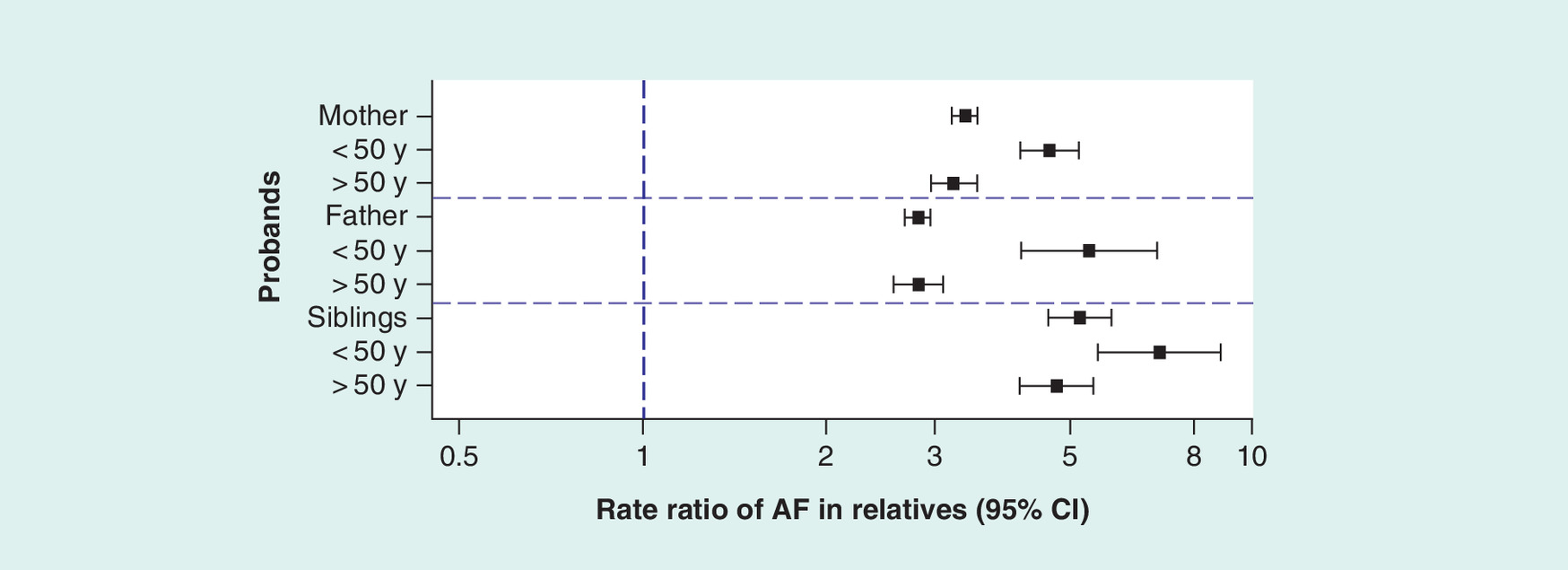
Figure 1. Adjusted rate ratios of atrial fibrillation among relatives to atrial fibrillation-probands compared with the general population.
Associated relatives were defined as first-degree family members to AF patients.
AF: Atrial fibrillation; y: Years.
Reproduced with permission from [46].
Disease course in familial AF
Using a prospective multicenter outpatient database, the Outcomes Registry for Better Informed Treatment of AF (ORBIT-AF), including approximately 10,000, mostly Caucasian AF patients [47], we addressed potential differences in patient characteristics and disease course in familial and non-familial AF patients. Familial AF was defined as AF in an individual with a first-degree family member diagnosed with AF. In this study, 14.8% of the AF patients reported a family history of AF. These patients were diagnosed with AF in a younger age (median age 65 years, IQR 63–79 vs 70 years, IQR 61–77; p < 0.01) and fewer were male (55.2 vs 58.1%; p = 0.04) than in the non-familial AF group. Regarding other risk factors for developing AF, patients with familial AF in general had a higher BMI than patients with non-familial AF (median BMI 29.9 [IQR 26–35] vs 29.0 [IQR 25–34]; p < 0.01), they were less likely to suffer from heart valve disease compared with non-familial AF patients (22.2 vs 25.9%; p < 0.01) while no differences existed regarding prevalence of heart failure (32.4 vs 30.1%; p = 0.25) and hypertension (81.8 vs 83.1%; p = 0.22) at AF diagnosis among familial and non-familial AF patients. In general, the familial AF patients had less comorbid illness (chronic obstructive pulmonary disease, prior stroke or transient ischemic attack [TIA], heart failure, ischemic heart disease), and suffered from more disabling symptoms (measured by the European Hear Association Score of AF [EHRA-score]) than those without a family history of AF. This difference remained in an analysis matching the familial AF patients with non-familial AF patients upon age and gender. This has to our knowledge never been described before and the mechanism behind remains unknown. The EHRA-score is a subjective scale, and a possible explanation for more enabling symptoms in the familial AF group could be increased awareness of the symptoms among those with a family history of the disease. It is also possible that some genetic forms of AF differ from AF in general, and may have more enabling symptoms.
We also compared the familial and the non-familial AF patients in terms of their longitudinal adjusted risk of AF progression (paroxysmal AF to persistent AF, or paroxysmal/persistent AF to permanent AF), stroke or non-CNS embolism or TIA, all cause hospitalization, and all-cause death. This study had a median follow-up time of 24 months and during this time we found no differences in the risk of these four outcomes in patients with familial AF compared with those with non-familial AF (Table 1) [47].
Because of the limited follow-up time of this study, we conducted a new study to compare the long-term risk of death and thromboembolic complications in familial and non-familial AF patients. As in the first study estimating the risk of AF among first-degree family members to AF patients, we used the Danish nationwide registries. We identified all AF patients in Denmark diagnosed with AF in the period from 1995 to 2012 who had a parent or a sibling diagnosed with AF prior to their own diagnosis. These were defined as familial AF patients, and were subsequently matched upon age, gender and year of AF diagnosis with non-familial AF patients, defined as AF patients without a family history of AF. The two patient groups were followed for a median time of 40 months (IQR 17–78 months) and their risk of all-cause death and thromboembolic events were compared. In concordance with our previous work the familial AF patients of this study were younger at their AF debut than AF patients in general (median age 50 years, IQR 43–54 years) and in the age, gender, and year matched population of familial and non-familial AF patients, the familial AF patients suffered from less comorbid illness (alcohol abuse, diabetes, ischemic heart disease, peptic ulcer, peripheral vascular disease or a prior shock/sepsis). No differences existed in prevalence of hypertension and heart failure among familial and non-familial AF patients (27.1 vs 26.1%; p = 0.29 and 16.0 vs 16.0%; p = 1.00, respectively) while fewer patients with familial AF than non-familial AF had a diagnosis of alcohol abuse (1.9 vs 2.7%, p = 0.03). As was the case in our study from the ORBIT-AF database [47] we found no differences in the longitudinal risk of death and thromboembolic complications in familial and non-familial AF patients (Figure 2) [48]. These studies presented here are to our knowledge the first examining the course of familial AF including long-term outcomes. They add important new knowledge regarding to which degree a family history of AF is a risk factor for developing AF and also for the subsequent risk of adverse outcome.

Figure 2. Incidence rates and adjusted hazard ratios of long-term outcomes according to family history of atrial fibrillation.
Inherited genes or inherited lifestyle?
In spite of plenty of genetic studies identifying specific and rare monogenic versions of AF, GWAS studies presenting common genomic variants associated with AF, and epidemiological studies finding a family history of AF to be an important risk factor for AF, we still do not know to what degree these findings are linked. The genetic studies do not say anything about the incidence of genetically inherited AF while the epidemiological studies are lacking information about causation. The proportion of AF patients who had a family history of AF was almost 15% in the study from the ORBIT-AF registry [47]. So the question is whether only a few or all 15% of these patients were genetically predisposed to AF or whether they developed AF because of other genetically inherited comorbidities (e.g., hypertension) associated with AF or due to shared AF risk factors among close family members. In the epidemiological studies, familial AF was diagnosed at a younger age and with less concomitant comorbidities than non-familial AF. In our previous work, no differences existed among familial and non-familial AF patients regarding prevalence of hypertension and heart failure [47,48]. In the ORBIT-AF registry, the familial AF group consisted of significantly fewer male patients than in the non-familial AF group, and patients with familial AF suffered from less heart valve disease than patients with non-familial AF [47]. In the Danish registries, significantly fewer patients with familial AF suffered from alcohol abuse compared with the non-familial AF patients [48]. All of these factors increase the risk of getting AF [12], and the fact that patients with familial AF had lower or the same prevalence of these risk factors points in the direction of a genetic explanation to familial AF. On the other hand, being overweight is also a well-known risk factor for AF, and in the ORBIT-AF registry, the familial AF patients had a significantly higher BMI than the non-familial AF patients (no data on BMI were available in the Danish registries) [47]. In 2010, Christophersen et al. examined the risk of AF in twins whose twin sibling was diagnosed with AF. By using biometrical models they suggested that more than half of AF cases are due to genetic additive effects [42]. Obesity may, therefore, contribute to the increased risk of AF among individuals with a family history of AF.
It seems like the clinician should be aware of a familial predisposition to AF but also keep other risk factors for AF in mind when consulting AF patients with a family history of AF. At last, it is important to keep in mind that the majority of the reviewed studies were conducted on primarily Caucasian patients, and the results should be interpreted with caution with regard to other human races.
Treatment of familial AF: should it differ from general guidelines?
In this paper, we have reviewed our previous work regarding familial AF. The data originate from a US prospective multicenter outpatient database (ORBIT-AF) with a median age of the familial AF population on 65 years and from retrospective nationwide registries from Denmark with a median age of the familial AF patients at 50 years. The studies, therefore, cover a wide range of AF patients and thromboembolic risk.
Our study of familial AF in the ORBIT-AF registry found familial AF patients to suffer from more symptoms than non-familial AF patients, but when looking at longitudinal outcomes as AF progression, all-cause hospitalizations, thromboembolic complications, and all-cause mortality no differences were found between the two groups of patients [47]. This was confirmed in our latest work, where no long-term differences were found in terms of risk of death and thromboembolic complications in familial versus non-familial AF patients [48]. So, the latest research comparing familial and non-familial AF patients in terms of their long-term complications does not indicate a need for differentiation of the antithrombotic treatment according to family history of AF. More aggressive antiarrhythmic therapy and rhythm control may be beneficial in familial AF patients because of their more disabling symptoms. Regarding catheter ablation of AF, the study by Shoemaker et al. found patients with chromosome 4q25 SNP rs2200733 to be more likely to have recurrence of AF within a time period of 12 months from the catheter ablation [39]. This may suggest personalized selection of patients for catheter ablation including genetic tests, but more research in this point of area is definitely needed.
Future perspective
The majority of AF patients develop the disease without any family history of AF, probably because of lifestyle factors and comorbid illness predisposing to AF. The acknowledgement of a familial form of AF has led to considerations whether familial and non-familial AF actually differs in disease course and in the long-term risk of complications. When looking at familial AF as a whole in population science studies we found no differences in important long-term end points in familial and non-familial AF patients. This indicates that a family history of AF in itself does not influence on the course of AF but it still remains unknown whether AF patients with specific genetic susceptibility loci for AF are clinically different. However, for both familial and non-familial AF, treatment and preventive strategies are underused and even in the anticoagulated patients the thromboembolic risk remains higher than in the general population. Studies looking into and comparing patients with the specific genomic regions associated with AF found in GWAS studies with respect to disease course and long-term outcomes of death and thromboembolic complications would be highly relevant.
| Outcome | No family history of AF: events (events per 100 patient-years) | Family history of: events (events per 100 patient-years) | Unadjusted HR (95% CI) for family history of AF | p-value | Adjusted HR (95% CI) for family history AF‡ | p-value |
|---|---|---|---|---|---|---|
| First AF progression | 1346 (14.74) | 239 (14.48) | 0.99 (0.84,1.15) | 0.8537 | 0.98 (0.85,1.14) | 0.8420 |
| First stroke or non-CNS embolism or TIA | 259 (1.63) | 39 (1.36) | 0.83 (0.59,1.17) | 0.2827 | 0.95 (0.67,1.34) | 0.7643 |
| All-cause first hospitalization | 3970 (34.78) | 686 (33.30) | 0.96 (0.88,1.04) | 0.3331 | 1.03 (0.94,1.12) | 0.5331 |
| All-cause death | 891 (5.53) | 128 (4.42) | 0.82 (0.68,0.99) | 0.0388 | 1.05 90.86,1.27) | 0.6454 |
†First AF progression was defined as either progression of AF at baseline from paroxysmal to persistent, from persistent to permanent or from paroxysmal to permanent.
‡Adjustments:
• First AF progression: most recent 12 lead ECG – atrial fibrillation or atrial flutter, heart rate, congestive heart failure, age at baseline, degree of left atrial enlargement, prior cardioversions, race, sinus node dysfunction/sick sinus syndrome, anemia, and type of AF at baseline.
• First stroke or non-CNS embolism or TIA: dialysis, AF type, peripheral vascular disease, AV Node/HIS bundle ablation, weight, hypertension, age at baseline, and history of stroke or TIA.
• First hospitalization (all-cause): age at baseline, BMI, weight, osteoporosis, height, prior PCI, cancer, obstructive sleep apnea, anemia, frailty, insurance status, history of CAD, principal investigator/site specialty, prior antiarrhythmic drug use, peripheral vascular disease, functional status, heart rate, diabetes, hematocrit, eGFR, COPD, diastolic blood pressure, EHRA score, and congestive heart failure.
• All-cause death: level of education, current AF management status, cognitive impairment/dementia, hyperlipidemia, eGFR, degree of left atrial enlargement, cancer, diastolic blood pressure, intraventricular conduction, frailty, height, heart rate, hematocrit, diabetes, smoking, systolic blood pressure, COPD, BMI, sex, congestive heart failure, age, and functional status.
AF: Atrial fibrillation; CAD: Coronary artery disease; COPD: Chronic obstructive pulmonary disease; eGFR: Estimated glomerular filtration rate; EHRA: European Heart Association Score of AF; ECG: Electrocardiography; HR: Hazard ratio; PCI: Percutaneous coronary intervention; TIA: Transient ischemic attack.
Data taken with permission from [47].
Familial atrial fibrillation
Three genomic regions have been associated with atrial fibrillation (AF).
AF accumulates in families and the risk of AF is substantially increased in individuals with first-degree family members diagnosed with AF.
Familial clustering of AF in a nationwide cohort
The younger the age at which the proband develops AF, the higher the risk of AF in the first-degree family members.
Disease course in familial AF
Familial AF patients develop the disease in a younger age than non-familial AF patients and with less comorbid illnesses.
Familial AF patients suffer from more disabling symptoms than age and gender matched non-familial AF patients.
Familial AF patients seem to have the same risk of all-cause mortality and thromboembolism as non-familial AF patients when accounting for age, gender, and comorbidities.
Inherited genes or inherited lifestyle?
Familial AF may be caused by a combination of genetic susceptibility and lifestyle factors.
Treatment of familial AF: should it differ from general guidelines?
Apparently, no differences have been found in long-term complications of familial and non-familial AF. Therefore, and at this point, there is no indication for differentiation in antithrombotic treatment for familial and non-familial AF patients.
More aggressive antiarrhythmic therapy and rhythm control may be indicated in familial AF patients.
Future perspective
Research regarding disease course and long-term outcomes in AF patients with different genomic regions associated with AF is warranted.
Financial & competing interests disclosure
JB Olesen: received speaker fees from Bristol-Myers Squibb and Boehringer Ingelheim, and funding for research from Bristol-Myers Squibb and The Capital Region of Denmark, Foundation for Health Research; ED Peterson: reports grants and personal fees from Janssen, personal fees from Boehringer Ingelheim, personal fees from Bayer, personal fees from Sanofi, personal fees from Astra Zeneca, personal fees from Merck, outside the submitted work; GH Gislason: reports grants from AstraZeneca, grants from Bristol-Myers Squibb, grants from Bayer, grants from Boehringer Ingelheim, outside the submitted work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Fuster V, Rydén LE, Cannom DS et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation – a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to revise the 2001 guidelines for the management of patients with atrial fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation 114(7), e257–e354 (2006).
2.
Chugh SS, Havmoeller R, Narayanan K et al. Worldwide epidemiology of atrial fibrillation: a global burden of disease 2010 study. Circulation 129(8), 837–847 (2014).
3.
Stewart S, Hart CL, Hole DJ, McMurray JJV. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am. J. Med. 113(5), 359–364 (2002).
4.
Krahn AD, Manfreda J, Tate RB, Mathewson FAL, Cuddy TE. The natural history of atrial fibrillation: incidence, risk factors, and prognosis in the manitoba follow-up study. Am. J. Med. 98(5), 476–484 (1995).
5.
Albertsen IE, Rasmussen LH, Overvad TF, Graungaard T, Larsen TB, Lip GYH. Risk of stroke or systemic embolism in atrial fibrillation patients treated with warfarin a systematic review and meta-analysis. Stroke 44(5), 1329–1336 (2013).
6.
Wang TJ, Parise H, Levy D et al. Obesity and the risk of new-onset atrial fibrillation. JAMA 292(20), 2471–2477 (2004).
7.
Frost L, Hune LJ, Vestergaard P. Overweight and obesity as risk factors for atrial fibrillation or flutter: the Danish Diet, Cancer, and Health Study. Am. J. Med. 118(5), 489–495 (2005).
8.
Djoussé L, Levy D, Benjamin EJ et al. Long-term alcohol consumption and the risk of atrial fibrillation in the Framingham Study. Am. J. Cardiol. 93(6), 710–713 (2004).
9.
Luong C, Barnes ME, Tsang TSM. Atrial fibrillation and heart failure: cause or effect? Curr. Heart Fail. Rep. 11(4), 463–470 (2014).
10.
Psaty BM, Manolio TA, Kuller LH et al. Incidence of and risk factors for atrial fibrillation in older adults. Circulation 96(7), 2455–2461 (1997).
11.
Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am. J. Cardiol. 82(8A), N2–N9 (1998).
12.
Hayashi K, Tada H, Yamagishi M. The genetics of atrial fibrillation. Curr. Opin. Cardiol. 32(1), 10–16 (2017).
13.
Brugada R, Tapscott T, Czernuszewicz GZ et al. Identification of a genetic locus for familial atrial fibrillation. N. Engl. J. Med. 336(13), 905–911 (1997).
• A seminal paper, being the first to identify a genetic loci associated with atrial fibrillation (AF).
14.
Chen Y-H, Xu S-J, Bendahhou S et al. KCNQ1 gain-of-function mutation in familial atrial fibrillation. Science 299(5604), 251–254 (2003).
15.
Ellinor PT, Shin JT, Moore RK, Yoerger DM, MacRae CA. Locus for atrial fibrillation maps to chromosome 6q14–16. Circulation 107(23), 2880–2883 (2003).
16.
Lai L-P, Su M-J, Yeh H-M et al. Association of the human minK gene 38G allele with atrial fibrillation: evidence of possible genetic control on the pathogenesis of atrial fibrillation. Am. Heart J. 144(3), 485–490 (2002).
17.
Sinner MF, Tucker NR, Lunetta KL et al. Integrating genetic, transcriptional, and functional analyses to identify 5 novel genes for atrial fibrillation. Circulation 130(15), 1225–1235 (2014).
18.
Ellinor PT, Lunetta KL, Glazer NL et al. Common variants in KCNN3 are associated with lone atrial fibrillation. Nat. Genet. 42(3), 240–244 (2010).
19.
Benjamin EJ, Rice KM, Arking DE et al. Variants in ZFHX3 are associated with atrial fibrillation in individuals of European ancestry. Nat. Genet. 41(8), 879–881 (2009).
20.
Das S, Makino S, Melman YF et al. Mutation in the S3 segment of KCNQ1 results in familial lone atrial fibrillation. Heart Rhythm 6(8), 1146–1153 (2009).
21.
Otway R, Vandenberg JI, Guo G et al. Stretch-sensitive KCNQ1 mutation a link between genetic and environmental factors in the pathogenesis of atrial fibrillation? J. Am. Coll. Cardiol. 49(5), 578–586 (2007).
22.
Lundby A, Ravn LS, Svendsen JH, Olesen S-P, Schmitt N. KCNQ1 mutation Q147R is associated with atrial fibrillation and prolonged QT interval. Heart Rhythm 4(12), 1532–1541 (2007).
23.
Yang Y, Xia M, Jin Q et al. Identification of a KCNE2 gain-of-function mutation in patients with familial atrial fibrillation. Am. J. Hum. Genet. 75(5), 899–905 (2004).
24.
Xia M, Jin Q, Bendahhou S et al. A Kir2.1 gain-of-function mutation underlies familial atrial fibrillation. Biochem. Biophys. Res. Commun. 332(4), 1012–1019 (2005).
25.
Ravn LS, Aizawa Y, Pollevick GD et al. Gain of function in IKs secondary to a mutation in KCNE5 associated with atrial fibrillation. Heart Rhythm 5(3), 427–435 (2008).
26.
Olson TM, Alekseev AE, Liu XK et al. Kv1.5 channelopathy due to KCNA5 loss-of-function mutation causes human atrial fibrillation. Hum. Mol. Genet. 15(14), 2185–2191 (2006).
27.
Yang T, Yang P, Roden DM, Darbar D. Novel KCNA5 mutation implicates tyrosine kinase signaling in human atrial fibrillation. Heart Rhythm 7(9), 1246–1252 (2010).
28.
Darbar D, Kannankeril PJ, Donahue BS et al. Cardiac sodium channel (SCN5A) variants associated with atrial fibrillation. Circulation 117(15), 1927–1935 (2008).
29.
Ellinor PT, Nam EG, Shea MA, Milan DJ, Ruskin JN, MacRae CA. Cardiac sodium channel mutation in atrial fibrillation. Heart Rhythm 5(1), 99–105 (2008).
30.
Thibodeau IL, Xu J, Li Q et al. Paradigm of genetic mosaicism and lone atrial fibrillation: physiological characterization of a connexin 43-deletion mutant identified from atrial tissue. Circulation 122(3), 236–244 (2010).
31.
Yang Y-Q, Liu X, Zhang X-L et al. Novel connexin40 missense mutations in patients with familial atrial fibrillation. Europace 12(10), 1421–1427 (2010).
32.
Makiyama T, Akao M, Shizuta S et al. A novel SCN5A gain-of-function mutation M1875T associated with familial atrial fibrillation. J. Am. Coll. Cardiol. 52(16), 1326–1334 (2008).
33.
Li Q, Huang H, Liu G et al. Gain-of-function mutation of Nav1.5 in atrial fibrillation enhances cellular excitability and lowers the threshold for action potential firing. Biochem. Biophys. Res. Commun. 380(1), 132–137 (2009).
34.
Roberts JD, Gollob MH. A contemporary review on the genetic basis of atrial fibrillation. Methodist DeBakey Cardiovasc. J. 10(1), 18–24 (2014).
35.
Kiliszek M, Franaszczyk M, Kozluk E et al. Association between variants on chromosome 4q25, 16q22 and 1q21 and atrial fibrillation in the Polish population. PLoS ONE 6(7), e21790 (2011).
36.
Gudbjartsson DF, Arnar DO, Helgadottir A et al. Variants conferring risk of atrial fibrillation on chromosome 4q25. Nature 448(7151), 353–357 (2007).
37.
Gudbjartsson DF, Holm H, Gretarsdottir S et al. A sequence variant in ZFHX3 on 16q22 associates with atrial fibrillation and ischemic stroke. Nat. Genet. 41(8), 876–878 (2009).
38.
Ellinor PT, Lunetta KL, Albert CM et al. Meta-analysis identifies six new susceptibility loci for atrial fibrillation. Nat. Genet. 44(6), 670–675 (2012).
• A meta-analysis of the large genome-wide association studies previously performed.
39.
Shoemaker MB, Bollmann A, Lubitz SA et al. Common genetic variants and response to atrial fibrillation ablation. Circ. Arrhythm. Electrophysiol. 8(2), 296–302 (2015).
40.
Fox CS, Parise H, D’Agostino RB Sr et al. Parental atrial fibrillation as a risk factor for atrial fibrillation in offspring. J. Am. Med. Assoc. 291(23), 2851–2855 (2004).
• One of the important familial AF papers, which found an increased risk of AF among offspring to AF patients.
41.
Lubitz SA, Yin X, Fontes JD et al. Association between familial atrial fibrillation and risk of new-onset atrial fibrillation. J. Am. Med. Assoc. 304(20), 2263–2269 (2010).
• One of the important familial AF papers, which found an increased risk of AF among offspring to AF patients.
42.
Christophersen IE, Ravn LS, Budtz-Joergensen E et al. Familial aggregation of atrial fibrillation – a study in Danish twins. Circ. Arrhythm. Electrophysiol. 2(4), 378–383 (2009).
43.
Arnar DO, Thorvaldsson S, Manolio TA et al. Familial aggregation of atrial fibrillation in Iceland. Eur. Heart J. 27(6), 708–712 (2006).
44.
Ellinor PT, Yoerger DM, Ruskin JN, MacRae CA. Familial aggregation in lone atrial fibrillation. Hum. Genet. 118(2), 179–184 (2005).
45.
Øyen N, Ranthe MF, Carstensen L et al. Familial aggregation of lone atrial fibrillation in young persons. J. Am. Coll. Cardiol. 60(10), 917–921 (2012).
46.
Gundlund A, Christiansen MN, Hansen ML et al. Familial clustering and subsequent incidence of atrial fibrillation among first-degree relatives in Denmark. Europace 18(5), 658–664 (2016).
•• One of our previous works, and one of the main papers in this review.
47.
Gundlund A, Fosbøl EL, Kim S et al. Family history of atrial fibrillation is associated with earlier-onset and more symptomatic atrial fibrillation: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) registry. Am. Heart J. 175, 28–35 (2016).
•• One of our previous works, and one of the main papers in this review.
48.
Gundlund A, Olesen JB, Staerk L et al. Outcomes associated with familial versus nonfamilial atrial fibrillation: a matched nationwide cohort study. J. Am. Heart Assoc. 5(11), e003836 (2016).
•• One of our previous works, and one of the main papers in this review.
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 9 May 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Familial clustering of atrial fibrillation and comparative longitudinal outcomes of familial and non-familial atrial fibrillation. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0088
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Iurii Titarenko, The Role of Digital Health Technology in Personalized Allergy Therapy, SSP Modern Pharmacy and Medicine, 10.53933/wv26wm48, 6, 1, (102), (2026).
- Iulia Cristina Marginean, Sergiu Marian Cazacu, Cristina Maria Marginean, Mihaela Popescu, George Alexandru Iacob, Marian Sorin Popescu, Cristin Constantin Vere, When Atrial Fibrillation Meets Alcoholic Liver Cirrhosis: Can Direct Oral Anticoagulants Bridge the Therapeutic Gap?, Biomedicines, 10.3390/biomedicines14030531, 14, 3, (531), (2026).
- Kyung‐Yeon Lee, So‐Ryoung Lee, Eue‐Keun Choi, JungMin Choi, Hyo‐Jeong Ahn, Soonil Kwon, Kyung‐Do Han, Seil Oh, Gregory Y. H. Lip, Cardiovascular benefits of early rhythm control and healthy lifestyle in young atrial fibrillation, European Journal of Clinical Investigation, 10.1111/eci.70018, 55, 6, (2025).
- Juqian Zhang, Søren Paaske Johnsen, Yutao Guo, Gregory Y.H. Lip, Epidemiology of Atrial Fibrillation, Cardiac Electrophysiology Clinics, 10.1016/j.ccep.2020.10.010, 13, 1, (1-23), (2021).
- Daniele Pastori, Danilo Menichelli, Gregory Y.H. Lip, Angela Sciacqua, Francesco Violi, Pasquale Pignatelli, Mirella Saliola, Marco Antonio Casciaro, Greta Rende, Tommasa Vicario, Francesco Del Sole, Tommaso Bucci, Family History of Atrial Fibrillation and Risk of Cardiovascular Events, Circulation: Arrhythmia and Electrophysiology, 10.1161/CIRCEP.120.008477, 13, 9, (2020).