Depression, anxiety and stress severities in multiple sclerosis patients using injectable versus oral treatments
Abstract
Aim: Studies on multiple sclerosis in Saudi Arabia remain scant, particularly studies on the psychological aspects. This study measures severities of depression, anxiety and stress, and compares them to the used disease-modifying treatment. Materials & methods: Cross-sectional study using a phone questionnaire targeting 452 Saudi patients with relapsing-remitting multiple sclerosis following in King Khalid University Hospital, King Fahad Medical City or Security Forces Hospital. Results: From 235 patients, 149 used interferons, 58 used fingolimod and 28 used natalizumab. Depression scores were similar among all demographic and drug groups. Interferons versus fingolimod anxiety scores were significantly different (p = 0.035). Stress scores were within normal limits. Conclusion: Mild anxiety was higher among interferon users, which could be due to injection anxiety reasons.
First draft submitted: 28 November 2016; Accepted for publication: 27 February 2017; Published online: 12 July 2017
Multiple sclerosis (MS) is a chronic progressive inflammatory disease affecting the CNS, and most of its victims are young. It causes physical, cognitive and emotional deficits. Cognitive deficits can even be exaggerated by the presence of depression; therefore, they need accurate and timely evaluation. Depression and anxiety are reported to be common in MS patients [1–6].
Studies on MS in Saudi Arabia, and more so the psychological aspects of MS, remain scarce. The prevalence of MS in Saudi Arabia in 1998 was estimated to be 25/100,000 patients [7], with a rise noted in 2008 that reached 40/100,000 patients [8]. Saudi patients had a lower mean age of onset (25.9 years) when compared with non-Saudis (29.4 years) [9]. MS patients can be categorized according to their disease clinical course into: relapsing-remitting MS (RRMS), secondary-progressive MS, primary-progressive MS and progressive-relapsing MS. In 2014, progressive-relapsing MS has been eliminated from the classification and clinically isolated syndrome has been added [10]. RRMS is the most common disease course. Among Saudis, RRMS was the clinical course for 61% of the patients, progressive-relapsing was 20% and primary progressive was 19% [7,9].
Studies on MS and depression started around the 1950s with several studies suggesting that depression can reach up to a lifetime prevalence of 50% [11]. To our knowledge, there has been only one Saudi study on the psychological aspects of MS patients, which was published in 2015, the sample was of 25 hospitalized patients where six patients (25%) had moderate to severe anxiety or depression [12].
Internationally, a study from the United Arab Emirates published in 2015 by Alsaadi et al. found that among 80 patients who were seen in the MS clinics, 17.5% had depression and 20% had anxiety, while the remaining majority of the patients did not have depression or anxiety [13]. An Iranian study assessed the role of depression, anxiety, stress and fatigue in relation to MS patients’ quality of life; they found that depression, anxiety and fatigue were significantly negatively related to the physical aspects of lives of MS patients with anxiety being the strongest predictor – whereas in regard to the mental aspects, depression had the only significant negative role [14]. A large Canadian study found major depression to be higher in patients with MS than in people without MS (15.7 vs 7.4%) [15]. Anxiety disorders are also common in MS patients, with a lifetime prevalence of 35.7% and are often under-recognized and undertreated [16]. A randomized controlled trial on 121 patients with MS found that stress management therapy reduced the development of new MRI lesions [17]. However, the effect of stress on MS onset remained unclear according to a recent meta-analysis [18]. Pathogenesis of mood disorders in MS is not well understood and is rather multifactorial. It is also unclear whether depression and anxiety share the same mechanisms; depression has been found to possibly be an organic result of MS when compared with the more so psychosocial burden of disease that contributes to anxiety. Depression can be attributed to the direct inflammatory effects and demyelination in certain CNS structures, which are thought to have a relationship between neurophysiological disturbances and emotion [19–22]. There is also a possibility of depression and anxiety being drug-induced [23–25].
Currently, the treatment options for patients with RRMS have variable categories with different route options. Interferons, IFN-β, are three decades old and can be administered either intramuscularly or subcutaneously, natalizumab is given via intravenous infusion every 4 weeks and fingolimod is the oral medication.
The psychiatric impact of disease-modifying treatment (DMT) has been variable depending on the type of treatment being used. Interferon affective impacts have been controversial, with two randomized controlled trials finding no association between depression and interferon therapy. Nonetheless, because of its prevalence in MS patients, depression was recommended to be assessed regularly during the treatment course [26]. Fingolimod has shown to improve depression compared with a placebo at 6 months of treatment [27]. And in the TYNERGY trial, natalizumab showed to improve depression baseline but further independent studies have been recommended to confirm this finding [28,29].
To measure the dimensions of depression, anxiety and stress, Depression Anxiety and Stress Scale (DASS 21) was used. The aim of our study was to measure the severity of depression, anxiety and stress in Saudis with RRMS using the DASS 21, and then to compare scores among patients using interferon injections: Interferon beta-1b (Betaferon®; Bayer, Germany), Interferon beta-1a (Rebif®; Merck, Germany) and Avonex® (Biogen, MA, USA) versus patients on the oral treatment fingolimod (Gilenya™; Novartis, Switzerland) and versus patients taking the intravenous infusion natalizumab (Tysabri®, Biogen, MA, USA; see Table 1).
| Basic demographics | Values |
|---|---|
| All patients | |
| Total responses | 301 |
| Recently changed medication | 66 |
| Total included in comparative study | 235 |
| Age, mean (SD) | 34 (11) |
| BMI, mean (SD) | 26 (5) |
| Female gender, n (%) | 207 (69) |
| Marital status, n (%): | |
| – Single | 115 (38) |
| – Married | 171 (57) |
| – Others | 15 (5) |
| Education level, n (%): | |
| – Graduates | 165 (55) |
| – Nongraduates | 136 (45) |
| Interferons group (n = 149) | |
| Age, mean (SD) | 36 (12) |
| BMI, mean (SD) | 26 (5) |
| Female gender, n (%) | 95 (64) |
| Fingolimod group (n = 58) | |
| Age, mean (SD) | 31 (8) |
| BMI, mean (SD) | 25 (4) |
| Female gender, n (%) | 32 (55) |
| Natalizumab group (n = 28) | |
| Age, mean (SD) | 30 (8) |
| BMI, mean (SD) | 26 (6) |
| Female gender, n (%) | 20 (71) |
SD: Standard deviation.
Materials & methods
The research proposal of this cross-sectional study was approved by the Institutional Research Boards of three large participating hospitals in Riyadh, Saudi Arabia: King Khalid University Hospital, King Fahad Medical City and Security Forces Hospital.
Inclusion criteria include: age 18 years and above, diagnosis of RRMS and the use of a DMT. Patients who had a new MS attack in the last 4 weeks and patients who changed their DMT in the last 6 months were excluded. Patients were contacted by a phone call, were informed about the study and their consent was taken before proceeding with the phone questionnaire. The questionnaire contains demographic data, treatment history and the DASS-21 items. DASS 21 is a validated self-report questionnaire designed to measure the severity of a range of symptoms common to depression anxiety and stress [30]. This tool was designed to help in defining, understanding and measuring depression, anxiety and stress. DASS-21 scores will be interpreted as per tool instructions:
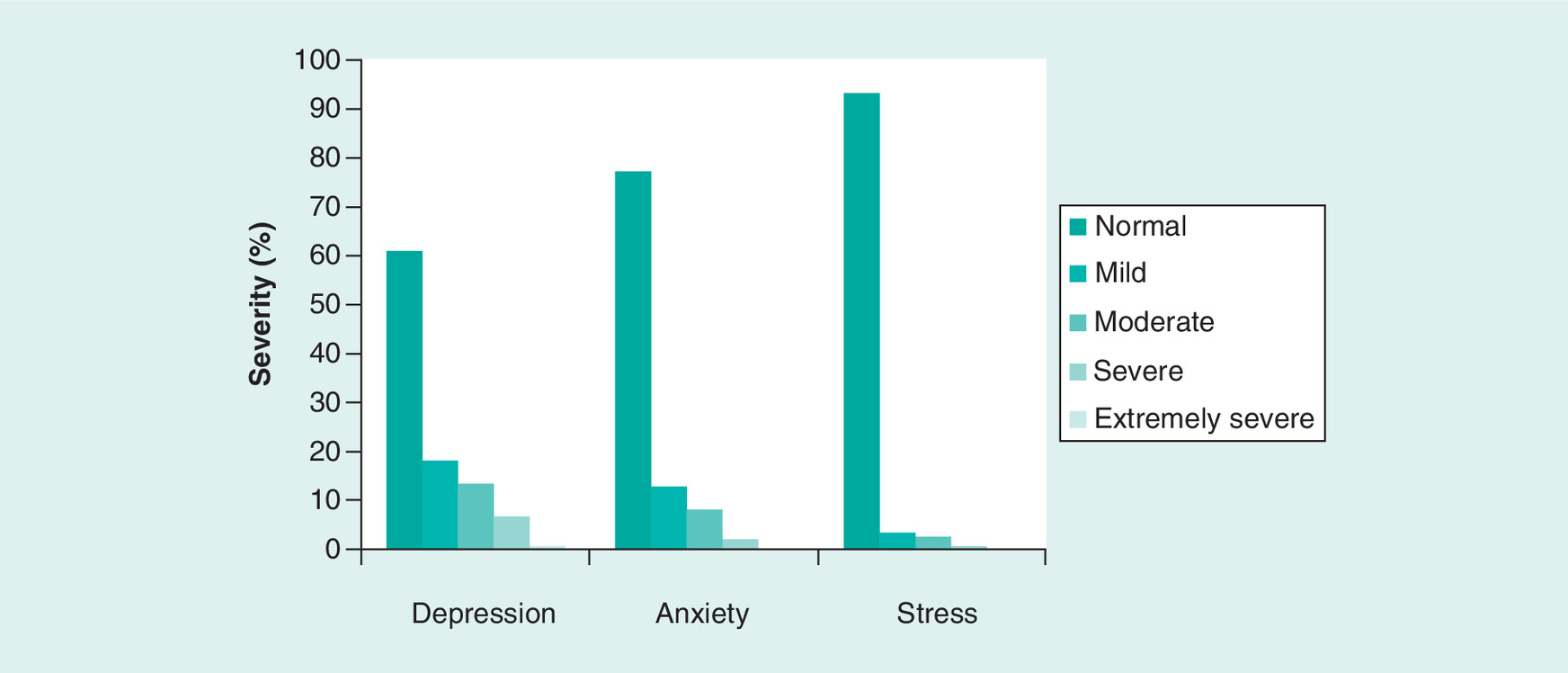
Depression interpretation scores: normal (0–4), mild (5–6), moderate (7–10), severe (11–13), extremely severe (14+).
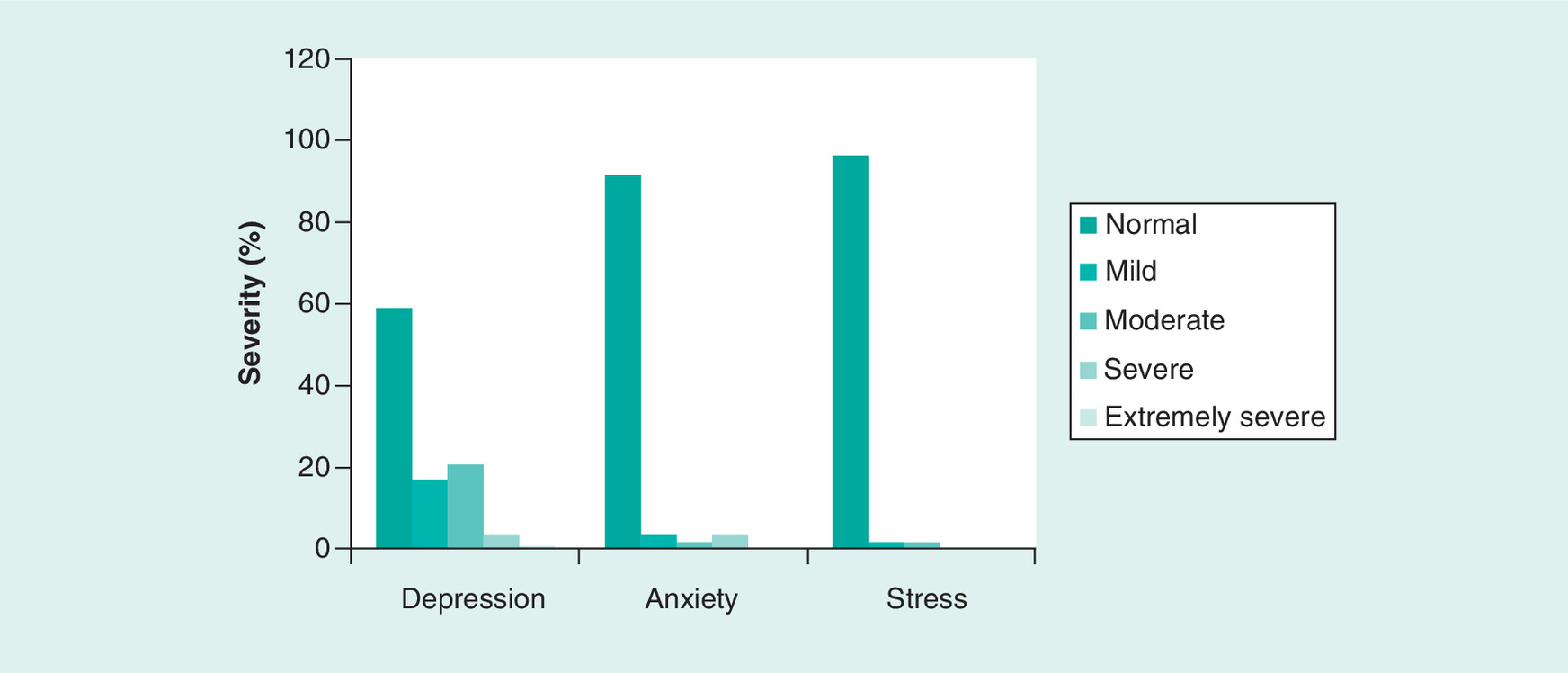
Anxiety interpretation scores: normal (0–3), mild (4–5), moderate (6–7), severe (8–9), extremely severe (10+).
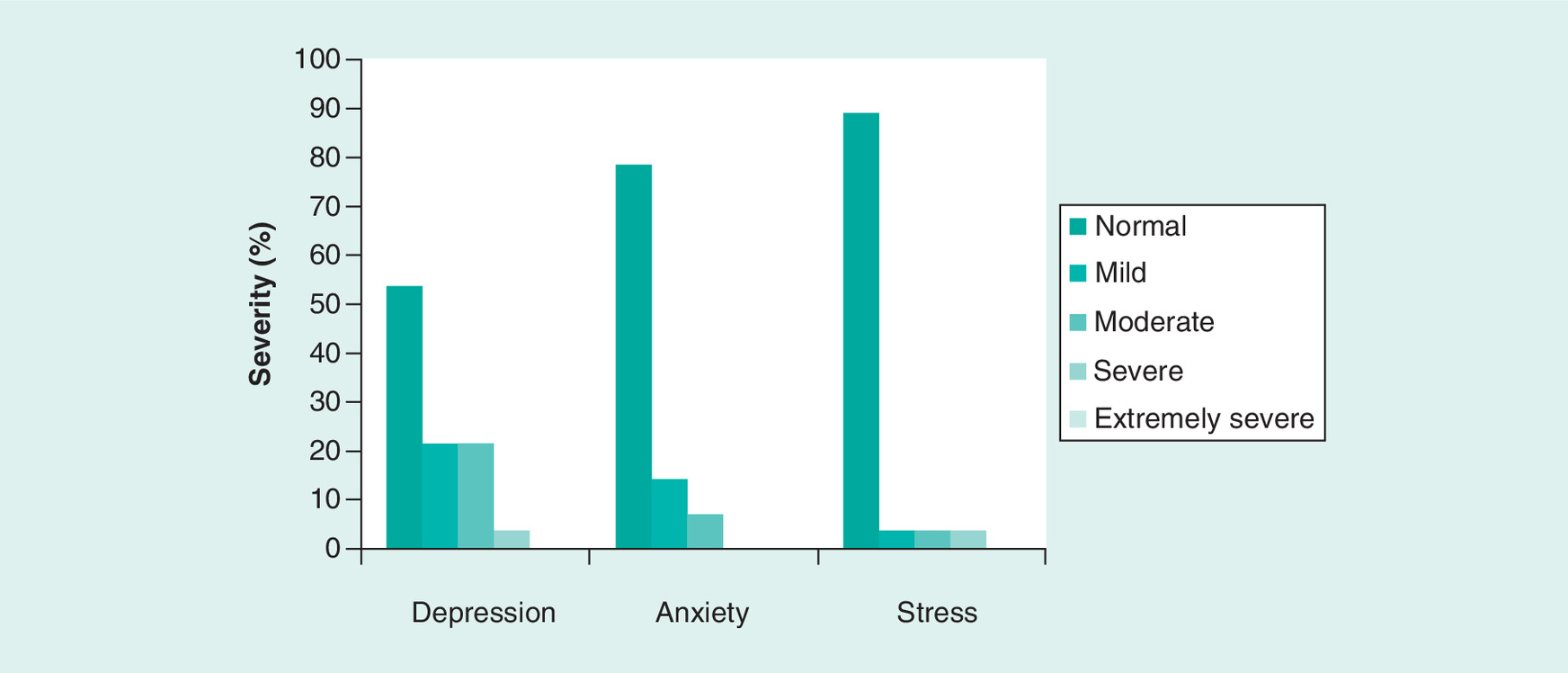
Stress interpretation scores: normal (0–7), mild (8–9), moderate (10–12), severe (13–16), extremely severe (17+).
Patient recruitment started in July 2013 and ended in June 2015. All patients who met the inclusion criteria were recruited without the need for randomization, and therefore had an equal chance of participation in the study. There was no control group of a normal population of matched age and gender in this cross-sectional study; however, there were three treatment groups to compare between.
Data analysis was performed using SPSS software, version 19 (NY, USA). Baseline characteristics were summarized by descriptive statistics (Table 1). Mean, percentages and standard deviation (SD) were calculated as per the study requirement. DASS scoring between groups was compared with analysis of variance (ANOVA) and simple unpaired t-test. All p ≤ 0.05 were considered as significant.
Results
The study targeted 452 RRMS patients who followed up at the participating clinics. Of these, 143 patients did not update their phone numbers at the clinics or did not answer the phone calls, and eight patients refused to participate. A total of 301 patients were recruited in this study. Out of which 235 patients were either on interferons, fingolimod or natalizumab medication, and 66 patients recently switched to other medications and have been excluded from the comparative DMT and DASS analyses. The response rate of the study was 66.6%. The mean age of 301 patients was 34.38 years (SD = 10.91). Of 301 patients, 68.77% were female, 38.21% were single, 56.81% were married and the remaining 4.98% were divorced or widowed. Education-wise, 54.82% were university graduates, and the rest were nongraduates. About half of the patients recruited (149 patients) were using one of the interferons with a mean age of 35.69 (SD ± 12.11) years, and 63.76% were female. A total of 58 patients were users of fingolimod with a mean age of 31.31 years (SD ± 7.82), and 55.17% of them were female. The natalizumab group had 28 patients with a mean age of 29.53 years (SD ± 8.25), and 71.42% of them were female. A total of 66 patients (22%) were recently switched from one treatment to another or were not compliant with any specific treatment (Table 1). There were no missing scores in the data collected.
In all patients, regardless of their medication type, the depression score average was 8.25 (SD ± 6.89), anxiety score was 3.30 (SD ± 3.83) and stress score was 3.85 (SD ± 5.73), thus suggesting depression was prominently associated with all drugs as compared with anxiety and stress. However, there was no statistically significant difference in DASS scores among all subjects when compared based on their age group or BMI (see Table 2). In gender-based comparison, we found stress scores to be higher in female patients 4.45 (SD ± 6.47) compared with males scores 2.23 (SD ± 4.39; p = 0.004). Since a stress score of 7 or less indicated a normal status, the statistical difference was not clinically significant (Table 2). Also, there was no statistically significant difference for depression or anxiety scores in males versus females.
| Variables | n | Mean score (SD) | ||
|---|---|---|---|---|
| Depression | Anxiety | Stress | ||
| Age (years): | ||||
| – All | 301 | 8 (7) | 3 (4) | 4 (6) |
| – 18–30 | 136 | 8 (7) | 3 (4) | 3 (5) |
| – 31–40 | 92 | 7 (7) | 4 (5) | 4 (7) |
| – 41–50 | 48 | 9 (7) | 3 (3) | 4 (6) |
| – >50 | 25 | 7 (7) | 2 (4) | 4 (6) |
| p-value | – | 0.31 | 0.09 | 0.84 |
| Gender: | ||||
| – Male | 94 | 8 (8) | 3 (4) | 2 (4) |
| – Female | 207 | 8 (7) | 4 (4) | 4 (6) |
| p-value | – | 0.32 | 0.28 | 0.00 |
| BMI: | ||||
| – <20 | 17 | 8 (7) | 6 (5) | 7 (10) |
| – 20–25 | 138 | 8 (7) | 4 (4) | 3 (5) |
| – 26–30 | 89 | 8 (7) | 3 (4) | 3 (6) |
| – >30 | 57 | 7 (6) | 3 (4) | 5 (6) |
| p-value | – | 0.89 | 0.09 | 0.06 |
SD: Standard deviation.
When we compared DASS scores among treatment groups (Table 3), we found no statistically significant difference in depression scores (p = 0.993, ANOVA), and no significance with anxiety scores (p = 0.086, ANOVA), stress scores were statistically but not clinically significant (p = 0.045, ANOVA). When using analysis of covariance (ANCOVA), we obtained almost the same p-values (i.e., results were nonsignificant). In the case of stress, homogeneity of regression was not justified and ANCOVA could not be performed. Age was divided into three groups: with the 18–30 age group, homogeneity of regression was observed and results were not significant. In the 31–40 age group, homogeneity of regression was observed and results were significant. In the 41–50 age group, homogeneity of regression was not justified and ANCOVA could not be performed. The above 50 age group only included two patients and ANCOVA could not be performed. An unpaired t-test evaluated if there was any significant effect between two medicine groups (Table 4). For anxiety, interferons versus fingolimod scores were significantly different (p = 0.035, t-test), interferons versus natalizumab and fingolimod versus natalizumab scores were not significantly different. For stress, fingolimod versus natalizumab scores were significantly different (p = 0.012, t-test), interferons versus fingolimod scores and interferons versus natalizumab scores were not significantly different.
| Medication | Mean score (SD) | ||
|---|---|---|---|
| Depression | Anxiety | Stress | |
| Interferons | 8 (7) | 4 (4) | 4 (6) |
| Fingolimod | 8 (7) | 3 (4) | 6 (7) |
| Natalizumab | 8 (7) | 3 (4) | 2 (4) |
| p-value | 0.99 | 0.09 | 0.05 |
SD: Standard deviation.
| Variable | Medication | p-value (unpaired t-test) |
|---|---|---|
| Depression | Interferons vs fingolimod | 0.957 |
| Interferons vs natalizumab | 0.933 | |
| Fingolimod vs natalizumab | 0.904 | |
| Anxiety | Interferons vs fingolimod | 0.035 |
| Interferons vs natalizumab | 0.296 | |
| Fingolimod vs natalizumab | 0.616 | |
| Stress | Interferons vs fingolimod | 0.137 |
| Interferons vs natalizumab | 0.110 | |
| Fingolimod vs natalizumab | 0.012 |
Discussion
Current medical literature has limited number of MS data coming from the Middle East, especially Saudi Arabia, and unfortunately we still do not have a Saudi MS registry. This study has a relatively generous sample size of Saudi patients with RRMS and an assessment of their mental health.
The results displayed some expected facts like MS being more prevalent in females, and the common coexisting emotional disorders. The study also showed that 38% of all MS patients were single, a much higher percentage than what was reported by the Saudi government statistics figure of 3.8% for women above age 30 years [31]. When it came to Education, 55% of Saudi MS patients had at least a university degree, which was close to the general figure in Saudi Arabia of 50% [31].
From Table 2, we see that the mean depression score for all subjects (8.25), a result that fits into moderate depression without significant difference between different age groups, gender, BMI or even treatment used. For anxiety, the mean score was (3.30) which fit into mild anxiety. The percentages of depression severities would be: 59.6% normal, 17% mild, 17% moderate, 6% severe and 0.4% extremely severe (Figure 1). Percentages for anxiety were: 80.4% normal, 10.2% mild, 7.2% moderate, 2.1% severe and none had extremely severe anxiety (Figure 2). And stress percentages were 93.6% normal, 3% mild, 2.6% moderate, 0.9% severe and none had extremely severe stress (Figure 3). We can compare our results to a recent smaller study on 24 Saudi patients, six patients (25%) had moderate-to-severe anxiety or depression by using the Hospital Anxiety and Depression Scale [12].
The anxiety severity scores did not significantly vary among different age groups, gender or BMI, but anxiety scores were higher in the group taking interferons (ANOVA) compared with natalizumab with statistical and clinical significance. The mechanism of the resultant anxiety is still unknown and can be related to interferon mechanism of action or related to injection pain and the way of receiving the drug. For stress scores, in general, they are small and within normal limits in different age groups, gender and BMI. ANOVA showed a statistical difference in stress scores between fingolimod and natalizumab; however, this difference does not seem clinically significant because the means of both groups were within the normal range for stress, and even when the SD was considered, the fingolimod group had mild stress with the highest range. Interferons scored similarly to the fingolimod group, natalizumab, on the other hand, did not display stress.
The limitations of this study could be addressed to the fact that the only tool used was the DASS 21; there was no parallel connection between the clinical scores with other investigations as brain imaging or serological markers. Correlations with radiological measures that reflect the severity of MS, and correlations between DASS 21, lesion localization and lesion volume would give more insight into depression and anxiety mechanisms and predictability. Another limitation is that DASS 21 can be influenced by the short-term depressive mood; therefore, it should be used in conjunction with a psychiatric assessment for mood disorders. Lastly, as this study is a cross-sectional one, the results represent an association of prevalence rather than temporal causation.
Conclusion
We can conclude from our study that RRMS in Saudi patients was associated with mild-to-moderate depression with no relation to a particular DMT. Mild anxiety, on the other hand, was more likely to be seen in those using interferon injections, which perhaps could be related to injection anxiety. These conclusions guide us to the fact that patients with RRMS do suffer from depression and may benefit from psychiatric support regardless of their depression degree or the DMT being used.
Future perspective
Newly released MS treatments can be included in future studies to give more insight about the relation of DMTs to levels of depression, anxiety, and stress. Also, involving the use of other illness related variables such as brain imaging might help correlate between signs of demyelination, lesion location and their relation to MS disability and psychologic manifestations versus drug related effects.
Multiple sclerosis (MS) is prevalent in Saudi Arabia and has a lower mean age of onset.
Relapsing-remitting MS is the most common phenotype in Saudi patients with MS.
Relapsing-remitting MS was associated with mild-to-moderate depression with no association to a particular disease-modifying treatment.
Anxiety was significantly higher in Interferon users compared with those on natalizumab.
Patients with MS could benefit from regular psychiatric evaluations regardless of the disease-modifying treatment they are using.
Acknowledgements
The authors thank G Murtaza, A Al-Qudimat and S Ezreqat for their statistical assistance. And they thank A AlQahtani, A AlRashed, A Alfaifi, A Al-Mohizea, B Al-Amr, E Albedaie, F Al-Turki, H Al-Sulimani, H Alkadhi, I AlFuraih, J Enani, K Alraddadi, L Al-Tawil, L AlFaraidi, L AlObaid, M Aleid, M Almarshad, M Alnafisah, M Sharefi, N Alnegheimish, NS Ahmed, N Alsalameh, RA Ohaly, R Alhifthi, R Al-Rakaf, R Algain, S Alrefaie, Y Al-Salloum and Z Alsawah for their help with data collection. The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding this work.
Financial & competing interests disclosure
This research is supported by the College of Medicine’s Research Center, Deanship of Scientific Research at King Saud University (No. RGP-1438-008). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Beiske AG, Svensson E, Sandanger I et al. Depression and anxiety amongst multiple sclerosis patients. Eur. J. Neurol. 15(3), 239–245 (2008).
2.
Dahl OP, Stordal E, Lydersen S, Midgard R. Anxiety and depression in multiple sclerosis. A comparative population-based study in Nord-Trondelag County, Norway. Mult. Scler. 15(12), 1495–1501 (2009).
3.
Jones KH, Ford DV, Jones PA et al. A large-scale study of anxiety and depression in people with multiple sclerosis: a survey via the web portal of the UK MS register. PLoS ONE 7(7), e41910 (2012).
4.
Wood B, Van Der Mei IA, Ponsonby AL et al. Prevalence and concurrence of anxiety, depression and fatigue over time in multiple sclerosis. Mult. Scler. 19(2), 217–224 (2013).
5.
Viner R, Fiest KM, Bulloch AG et al. Point prevalence and correlates of depression in a national community sample with multiple sclerosis. Gen. Hosp. Psychiatry 36(3), 352–354 (2014).
6.
De Cerqueira AC, Semionato De Andrade P, Godoy Barreiros JM, Teixeira AL, Nardi AE. Psychiatric disorders in patients with multiple sclerosis. Compr. Psychiatry 63, 10–14 (2015).
7.
Daif AK, Al-Rajeh S, Awada A et al. Pattern of presentation of multiple sclerosis in Saudi Arabia: analysis based on clinical and paraclinical features. Eur. Neurol. 39(3), 182–186 (1998).
• This was one of the first publications about multiple sclerosis (MS) in Saudi Arabia. It is an honor for us to publish our study with Abdulkader Daif, one of the leading names in MS management in Saudi Arabia.
8.
Bohlega S, Inshasi J, Al Tahan AR, Madani AB, Qahtani H, Rieckmann P. Multiple sclerosis in the Arabian Gulf countries: a consensus statement. J. Neurol. 260(12), 2959–2963 (2013).
9.
Heydarpour P, Khoshkish S, Abtahi S, Moradi-Lakeh M, Sahraian M. Multiple sclerosis epidemiology in Middle East and North Africa: a systematic review and meta-analysis. Neuroepidemiol. 44, 232–244 (2015).
• Interesting paper that compared epidemiology differences of multiple sclerosis in the Middle East.
10.
Lublin F. New multiple sclerosis phenotypic classification. Eur. Neurol. 72(Suppl. 1), 1–5 (2014).
11.
Siegert RJ, Abernethy DA. Depression in multiple sclerosis: a review. J. Neurol. Neurosurg. Psych. 76, 469–475 (2005).
12.
Alamri Y, Al-Busaidi IS. Multiple sclerosis in Saudi Arabia: anxiety, depression and suicidality. Psychiatry Res. 238, 24 (2016).
•• This was the first study that considered the psychological aspects of multiple sclerosis published from Saudi Arabia.
13.
Alsaadi T, El Hammasi K, Shahrour TM et al. Prevalence of depression and anxiety among patients with multiple sclerosis attending the MS clinic at Sheikh Khalifa Medical City, UAE: cross-sectional study. Mult. Scler. Int. 2015, 487159 (2015).
14.
Salehpoor G, Rezaei S, Hosseininezhad M. Quality of life in multiple sclerosis (MS) and role of fatigue, depression, anxiety, and stress: a bicenter study from north of Iran. Iran J. Nurs. Midwifery Res. 19(6), 593–599 (2014).
15.
Patten SB, Beck CA, Williams JV et al. Major depression in multiple sclerosis: a population-based perspective. Neurology 61, 1524–1527 (2003).
16.
Korostil M, Feinstein A. Anxiety disorders and their clinical correlates in multiple sclerosis patients. Mult. Scler. 13(1), 67–72 (2007).
17.
Mohr DC, Lovera J, Brown T et al. A randomized trial of stress management for the prevention of new brain lesions in MS. Neurol. 79(5), 412–419 (2012).
18.
Briones-Buixassa L, Milà R, Aragonès JM, Bufill E, Olaya B, Arrufat FX. Stress and multiple sclerosis: a systematic review considering potential moderating and mediating factors and methods of assessing stress. Health Psychol. Open 2(2), 2055102915612271 (2015).
19.
Pujol J, Bello J, Deus J, Marti-Vilalta JL, Capdevila A. Lesions in the left arcuate fasciculus region and depressive symptoms in multiple sclerosis. Neurology 49(4), 1105–1110 (1997).
20.
Bakshi R, Czarnecki D, Shaikh ZA et al. Brain MRI lesions and atrophy are related to depression in multiple sclerosis. Neuroreport 11(6), 1153–1158 (2000).
21.
Zorzon M, De Masi R, Nasuelli D et al. Depression and anxiety in multiple sclerosis. A clinical and MRI study in 95 subjects. J. Neurol. 248(5), 416–421 (2001).
22.
Feinstein A, Roy P, Lobaugh N, Feinstein K, O’Connor P, Black S. Structural brain abnormalities in multiple sclerosis patients with major depression. Neurology 62(4), 586–590 (2004).
23.
Jacobs LD, Beck RW, Simon JH et al. Intramuscular interferon beta-1a therapy initiated during a first demyelinating event in multiple sclerosis. CHAMPS Study Group. N. Engl. J. Med. 343(13), 898–904 (2000).
24.
Lana-Peixoto MA, Teixeira AL Jr, Haase VG. Interferon beta-1a-induced depression and suicidal ideation in multiple sclerosis. Arq. Neuropsiquiatr. 60(3-B), 721–724 (2002).
25.
Pandya R, Patten S. Depression in multiple sclerosis associated with interferon beta-1a (Rebif). Can. J. Psychiatry 47(7), 686 (2002).
26.
Chwastiak LA, Ehde DM. Psychiatric issues in multiple sclerosis. Psychiatr. Clin. North Am. 30(4), 803–817 (2007).
27.
Montalban X, Comi G, O’Connor P et al. Oral fingolimod (FTY720) in relapsing multiple sclerosis: impact on health-related quality of life in a Phase II study. Mult. Scler. 17(11), 1341–1350 (2011).
28.
Svenningsson A, Falk E, Celius EG et al. Natalizumab treatment reduces fatigue in multiple sclerosis. Results from the TYNERGY trial; a study in the real life setting. PLoS ONE 8(3), e58643 (2013).
29.
Hoepner R, Faissner S, Salmen A, Gold R, Chan A. Efficacy and side effects of natalizumab therapy in patients with multiple sclerosis. J. Cent. Nerv. Syst. Dis. 6, 41–49 (2014).
30.
Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br. J. Health Psychol. 44(Pt 2), 227–239 (2005).
31.
General Authority For Statistics: Kingdom of Saudi Arabia. www.stats.gov.sa/en/node
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 12 July 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Depression, anxiety and stress severities in multiple sclerosis patients using injectable versus oral treatments. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0087
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mariam Al-Ameri, Hanan Abu-Shaikh, Mohammad Mansour, Suha Al-Habahbeh, Feras Weshah, Wail Ennab, Ammena Y. Binsaleh, Sireen Abdul Rahim Shilbayeh, Omar Gammoh, Attention-Deficit Hyperactivity Disorder Symptoms in Adults Diagnosed with Multiple Sclerosis: Prevalence and Correlates, Journal of Clinical Medicine, 10.3390/jcm13133844, 13, 13, (3844), (2024).
- Sorour Khari, Marzieh Pazokian, Influence of religion and spirituality on the mental health of patients with multiple sclerosis, Journal of Spirituality in Mental Health, 10.1080/19349637.2023.2174920, 26, 2, (128-140), (2023).
- Duygu Özer, Elvan Emine Ata, Gül Dikeç, Serkan Demir, The relationship between stress, anxiety, and depression levels and pseudobulbar affect in patients with multiple sclerosis, Contemporary Nurse, 10.1080/10376178.2022.2107037, 58, 4, (317-329), (2022).
- Stella A Glasmacher, Patrick KA Kearns, Zackary Hassan, Peter Connick, Simone Tauber, Kathrin Reetz, Peter Foley, Siddharthan Chandran, The influence of disease-modifying therapy on hidden disability burden in people with newly diagnosed relapsing-remitting multiple sclerosis, Multiple Sclerosis and Related Disorders, 10.1016/j.msard.2022.103837, 63, (103837), (2022).
- Kerri A. Schoedel, Carine Kolly, Anne Gardin, Srikanth Neelakantham, Kasra Shakeri-Nejad, Abuse and dependence potential of sphingosine-1-phosphate (S1P) receptor modulators used in the treatment of multiple sclerosis: a review of literature and public data, Psychopharmacology, 10.1007/s00213-021-06011-6, 239, 1, (1-13), (2021).
- Ali Dehghani, Development and validation of the disease - specific problems questionnaire for patients with multiple sclerosis, BMC Neurology, 10.1186/s12883-021-02442-y, 21, 1, (2021).