Randomized comparative efficacy and safety study of intermittent simvastatin versus fenofibrate in hemodialysis
Abstract
Aim: Compare the safety and efficacy of intermittent fenofibrate versus simvastatin in chronic hemodialysis patients. Patients & methods: Sixty patients received either fenofibrate 100 mg or simvastatin 20 mg after their dialysis session (parallel study). The safety and efficacy of drugs on lipid profile, oxidized low-density lipoprotein (Ox-LDL), glutathione peroxidase and C-reactive protein were compared before and after 16-week treatment. Results: After treatment, significant increase in glutathione peroxidase, significant decrease in total cholesterol, triglycerides, low density lipoprotein (LDL) and ox-LDL (p < 0.05) and no significant changes in C-reactive protein (p > 0.05) were observed in both groups. Both drugs were well tolerated with no serious side effects reported by the patients. Conclusion: Both drugs have comparable efficacy and safety when used as intermittent low dose regimen in hemodialysis. Larger studies with longer follow-up periods are needed to confirm our new findings.
First draft submitted: 25 October 2016; Accepted for publication: 23 February 2017; Published online: 19 June 2017
Cardiovascular disease (CVD) is the main cause of morbidity and mortality among hemodialysis (HD) patients (stage 5 chronic kidney disease [CKD]). It is responsible for approximately 50% of the observed mortality associated with CKD [1]. Moreover, the mortality rate from CVD and the prevalence of premature accelerated atherosclerosis are dramatically higher than that of the general population [2]. Thus, they are considered as a high risk group for CVD as reported by National Kidney Foundation in 1998 [3]. This can be attributed to the presence of complex interplay between traditional and nontraditional risk factors that are present exclusively in uremic patients [4]. Dyslipidemia, a traditional risk factor, together with oxidative stress and inflammation, nontraditional risk factors, are implicated in the pathogenesis of accelerated premature atherosclerosis in HD patients and represent new targets for therapeutic intervention [5]. Both statins and fibrates have beneficial effects in treating dyslipidemia via their effect on the lipid profile, oxidative stress and inflammation [6].
In HD, simvastatin was reported to significantly lower total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), the atherogenic small dense LDL and to a lesser extent triglycerides (TG) levels [7]. Moreover, added improvements of oxidative stress and inflammatory states were also observed in CKD patients. These effects were detected after prolonged use or with high doses [8–12]. Interestingly, Yigit et al. [13] had shown that the continuous use of simvastatin in hypercholesterolemic patients has the same tolerability and efficacy as intermittent use (only on dialysis days).
Fenofibrate has also been used for treating dyslipidemia due to its effective reduction of serum TGs and increase in serum high-density lipoprotein cholesterol (HDL-C) levels [14]. Besides the lipid lowering effect, fenofibrate also exerts antioxidant effect [15]. However, clinical evidence supporting this effect in HD patients is scarce. Only one study successfully explained the effect of fenofibrate on aminothiols for 4 weeks only. Makwoka et al. [14] demonstrated that intermittent low dose fenofibrate resulted in shifting aminothiol balance to a less pro-oxidative pattern compared with placebo without significant changes in the inflammatory marker, C-reactive protein (CRP). Nevertheless, the use of fenofibrate in HD is limited due to the accumulation of metabolites and increased potential for side effects, such as increased serum creatinine levels and higher risk of rhabdomyolysis. These side effects were observed only when fenofibrate is given in doses comparable to those used in patients with normal glomerular filtration rate or in combination with statins [16,17]. Current guidelines limiting the use of fibrates may be too restrictive, especially that long-term fenofibrate use was found safe and effective among 9000 diabetic patients with moderate renal impairment in the Fenofibrate Intervention and Event Lowering in Diabetes trial [18]. Moreover, Makwoka et al. [14] demonstrated that fenofibrate can be used safely in HD patients [14].
Furthermore, HD patients have to comply with a very difficult treatment regimen such as fluid restriction, diet and the use of medications with adjusted doses. Thus, an intermittent regimen allowing lower dosing frequency may theoretically result in better compliance, reduced cost and lower risk of adverse events [2,13].
There is a lack of clinical trials comparing the efficacy and safety of simvastatin versus the cheaper fenofibrate using intermittent regimen in HD. Thus, this study was conducted to compare the efficacy and safety of an intermittent low dose fenofibrate versus simvastatin together with evaluation of patients’ compliance. Our screening panel included lipid profile, inflammatory markers and oxidative stress markers.
Patients & methods
Study design
This was a 16-week, multicenter, prospective, randomized, parallel study from October 2013 till January 2016 [19]. Patients were recruited from Kasr Al-Aini Center for Kidney Disease and Dialysis, King Fahd Dialysis Unit, the dialysis unit in the New Kasr Al Aini Teaching hospital, Cairo University teaching hospitals and the two dialysis units present in Ahmed Maher Teaching hospital, Cairo, Egypt.
Patients & study protocol
Patients aged >18 years, males or females, at least 12 months on chronic HD therapy with three dialysis sessions per week and diagnosed with hyperlipidemia ([TC] >200 mg/dl or [LDL-C] >130 mg/dl and [TGs] >150 mg/dl) were included in the study. Only newly diagnosed hyperlipidemic patients or those who did not use any fibrates or statins 6 months prior to the study were included.
Patients were excluded from the study if they were treated with immunosuppressants or steroids, intolerant to fibrates or statins previously or if they had any of the following conditions: hypothyroidism, uncontrolled hypertension, gall bladder disease, active liver disease (unexplained persistent increase in liver enzymes, ALT and AST > two-times the upper limit of normal ULN), muscle toxicity (CK > two-times ULN), history of myocardial infarction or coronary bypass surgery in last 3 months.
Serum levels of TC and TGs were screened for all patients available in the study centers that the researchers had access to. Eligible patients were randomly assigned to receive either fenofibrate 100 mg (group 1) or simvastatin 20 mg (group 2) three-times a week after the dialysis session with a 1:1 allocation. They were stratified by dialysis session timing using permuted blocks of randomly varied sizes. Before the study, all other chronically used medications were checked for any possible interactions with the medications under study and with lipid levels.
All blood samples were obtained after the patients had fasted for 12 h. Blood samples were withdrawn immediately prior to dialysis after the vascular access cannulation. HD for all patients consisted of a 4-h dialysis session three-times per week, with a blood flow of 250–300 ml/min and bicarbonate dialysate flow of 500–800 ml/min. Dialyzer surfaces were chosen according to the patient’s body surface area. In all cases, Haidylena® micro-undulated Polysulfone-based hollow fiber hemodialyzers (Haidylena for Advanced Medical Industries, 6th October City, Egypt) were used. The hemodialyzers used were either PS 130 (low flux dialyzer) or Platinum HPS (high performance series) to provide effective surface of 1.3 and 1.7 m2 respectively. The Kt/V index, which represents fractional urea clearance for adequacy of dialysis, for each session was >1.2 according to the current guidelines set for HD adequacy [20].
Safety & efficacy measurements
At baseline, careful history of the recruited patients including demographic characteristics, physical examination, comorbidities, medication history, familial history and social history was documented. Moreover, the following parameters were measured: blood pressure, body height, body weight and interdialytic weight gain (IDWG). The IDWG (the difference between the current predialysis weight and the preceding postdialytic weight) were recorded during 12 consecutive dialysis sessions. Then, the mean IDWG was calculated to be used for statistical analysis. The IDWG% was expressed as a proportion of the current patient’s dry weight [21,22]. Efficacy outcomes included serum oxidized LDL (ox-LDL), glutathione peroxidase (GSH-Px), CRP, TC, TGs, HDL-C and LDL-C (calculated using Friedewald’s formula [LDL = TC – [TG/5 + HDL]]). Safety outcomes included; urea, creatinine, ALT, AST, albumin, hemoglobin, CK and electrolytes (sodium, potassium, calcium and phosphorous) levels. All were measured at baseline, every month and till the end of the study period. However, ox-LDL, GSH-Px and CRP measurements were measured at baseline and after 16 weeks only.
Patients were interviewed monthly and questioned about any side effects and any signs or symptoms of muscle toxicity. Patients would be withdrawn if a serious adverse event occurred. In addition, the percentage of the compliance was calculated for each patient using tablet-count method [23] every month till the end of the study to ensure compliance throughout the study.
At each monthly visit, two blood samples were withdrawn from each patient for serum preparation and hemoglobin level determination. Serum concentrations of urea, creatinine, calcium and phosphorous were analyzed using Erba XL 100™ automated clinical chemistry analyzer (Mannheim, Germany), using kits from ERBA® diagnostics (Mannheim, Germany). While TC, TGs, HDL-C, CRP, CK, ALT, AST, albumin, sodium and potassium were analyzed using (STAT LAB SZSL60 - SPECTRUM) by kits provided from spectrum diagnostic® (Hannover, Germany). Serum ox-LDL and GSH-Px were analyzed by ELISA reader (Biotek-ELx808™, Winooski, VT 05404, USA) using kits provided from Glory Science Co., Ltd (Del Rio, TX 78840, USA).
Statistical analysis
All continuous variables were tested for normality using Shapiro–Wilk test. Demographic continuous data were expressed as mean ± standard deviation. Non-normally distributed continuous data were expressed as median, interquartile range (IQR). Categorical data were expressed as frequency and/or percentages. Fisher’s exact test was used for qualitative variables, Mann–Whitney U test or independent samples t-test for intergroup comparison; and Wilcoxon signed-rank test or Friedman’s test for within group data comparison. Following Friedman’s test, post hoc analysis with multiple pairwise comparisons using Wilcoxon signed-rank test was conducted with a Bonferroni correction applied resulting in significant level set at (p < 0.005). In addition, post-treatment values of each efficacy outcomes between fenofibrate and simvastatin groups were compared with analysis of covariance (ANCOVA) model using respective baseline values as a covariate. Statistical significance was defined as p < 0.05. Statistical analysis was performed using the Statistical Package for the Social Sciences software package version 20.
Results
The serum levels of TC and TGs were screened for 402 HD patients attending the study centers of whom 60 patients were eligible for the study. This was the maximum number of eligible patients that could be recruited in the dialysis centers that the researchers had access to. Group 1 (n = 30) received fenofibrate 100 mg capsules and group 2 (n = 30) received simvastatin 20 mg tablets three-times per week for 16 weeks. All recruited patients were anuric with residual diuresis <50 ml/day. Using interaction checker, the coadministered medications were found to neither affect the medications under study nor the lipid profile of the patients. From the recruited 60 patients, one patient from fenofibrate group and two from simvastatin group, died after 8 weeks of therapy. Comorbidities including hypertension, diabetes, hepatic viral infections (hepatitis C and hepatitis B), and hematological, neurological, cardiovascular and gastrointestinal problems were nonsignificantly different among both groups (p > 0.05). Patients in both groups were comparable with respect to age, gender, height, weight, BMI, time on HD, IDWG and their biochemical parameters (Table 1).
| Parameter | Fenofibrate group (group 1; n = 30) | Simvastatin group (group 2; n = 30) | p-value* |
|---|---|---|---|
| Age, mean ± SD (years) | 48.8 ± 11.55 | 51.83 ± 11.01 | 0.302† |
| Gender, No. of males (%) | 12 (40%) | 15 (50%) | 0.604‡ |
| Weight, mean ± SD (kg) | 72.9 ± 13.89 | 72.2 ± 16.71 | 0.861† |
| IDWG, median (IQR; %) | 3.18 (1.99–4.82) | 3.56 (2.11–4.29) | 0.888§ |
| BMI, mean ± SD (kg/m2) | 25.03 ± 4.03 | 25.02 ± 5 | 0.997† |
| Duration on HD, median (IQR; years) | 3 (2–10) | 3 (2–6.5) | 0.877§ |
| SBP, mean ± SD (mmHg) | 132 ± 17.89 | 130.67 ± 23.03 | 0.803† |
| DBP, mean ± SD (mmHg) | 81 ± 11.25 | 82.67 ± 10.48 | 0.555† |
| Urea, median (IQR; mg/dl) | 142.5 (75.25–172) | 113 (36–156) | 0.133§ |
| Creatinine, median (IQR; mg/dl) | 9.65 (8.25–11.8) | 10 (7.6–12) | 0.950§ |
| ALT, median (IQR; U/l) | 25.5 (20.25–32.25) | 30.88 (27.89–35.34) | 0.088§ |
| AST, median (IQR; U/l) | 25.5 (21.75–34.75) | 27.63 (23.95–35.88) | 0.203§ |
| Albumin, median (IQR; g/dl) | 3.91 (3.58–4.08) | 3.77 (3.35–4.21) | 0.894§ |
| CK, median (IQR; U/l) | 105.5 (70–138) | 118 (81.5–145.5) | 0.333§ |
| Hb, median (IQR; g/dl) | 9.7 (8.8–11.9) | 10.05 (7.87–10.57) | 0.270§ |
Data are represented as median, IQR or mean ± SD.
*Level of significance p < 0.05.
†Independent samples t-test at p < 0.05.
‡Fisher Exact test at p < 0.05.
§Mann–Whitney U test at p < 0.05.
DBP: Diastolic blood pressure; Hb: Hemoglobin; HD: Hemodialysis; IDWG: Interdialytic weight gain; IQR: Interquartile range; SD: Standard deviation; SBP: Systolic blood pressure.
Monitoring safety parameters, only one patient reported diarrhea upon starting fenofibrate but it ceased with continued use. None of the patients complained of muscle pain, weakness, or elevation of serum CK, ALT or AST more than three-times ULN. In group 1, only one patient showed increase in ALT (from 42 to 101 U/l) and AST (from 33 to 98 U/l) more than two-times ULN at the end of the study. Sodium, potassium, ALT and CK levels in fenofibrate group and sodium levels in simvastatin group remained within the normal range despite the observed significant difference (p > 0.05, Friedman’s test). During the whole study period, patients in both groups were comparable with respect to serum levels of urea, creatinine, ALT, AST and phosphorous (p > 0.05; Mann–Whitney U test). However, significant differences were observed in the second month serum levels of sodium (p = 0.011), potassium (p = 0.003) and calcium (p = 0.014) and in the first month of serum CK levels (p = 0.014; Table 2). However, none of these safety measurements differed significantly between both groups by the end of the study period (p > 0.05).
| Parameters | Fenofibrate group (group 1) | Simvastatin group (group 2) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 30 | n = 29 | p-value† | n = 30 | n = 28 | p-value† | |||||||
| Baseline | 1st month | 2nd month | 3rd month | 4th month | Baseline | 1st month | 2nd month | 3rd month | 4th month | |||
| Urea (IQR; mg/dl) | 142.5 (75.25 –172) | 141.5 (58.25–189.25) | 144 (70–193) | 146 (100.5–178.5) | 104 (59–179.5) | 0.599 | 114.5 (38.75–159) | 111 (71.6–162.5) | 119 (60–144) | 126 (109.5–167.5) | 122 (68–161) | 0.790 |
| Creatinine (IQR; mg/dl) | 9.65 (8.25–11.8) | 9.65 (8.2–11.17) | 9 (8–10.9) | 9.2 (7.97–10.25) | 8.8 (8.35–9.8) | 0.593 | 9.75 (7.6–11.85) | 9.9 (7.8–12) | 8.8 (6.7–11.5) | 9.2 (7.45–11.3) | 9.8 (7.9–12.3) | 0.556 |
| ALT (IQR; U/l) | 25.5 (21.75–34.75) | 29.5 (19.75–37) | 28 (23–37.5) | 37 (25 – 41) | 37 (28–44) | 0.004† | 27 (24–36) | 29 (24–36) | 27 (24–39) | 27 (20–39) | 29 (24.5–40) | 0.862 |
| AST (IQR; U/l) | 25.5 (20.25–32.44) | 29.5 (18–40) | 32 (25.75–36) | 30 (23.5–36) | 33 (25–37) | 0.219 | 30.88 (27.89–35.34) | 30 (23–41) | 35 (28–41) | 32 (22.5–41) | 31 (26.5–40) | 0.475 |
| Albumin (IQR; g/dl) | 3.9 (3.58–4.08) | 4.01 (3.85–4.2) | 3.79 (3.49–4.23) | 3.66 (3.28–4.09) | 3.81 (3.5–4.25) | 0.324 | 3.82 (3.36–4.17) | 3.89 (3.59–4.09) | 3.9 (3.16–4.15) | 3.72 (3.18–4.01) | 4 (3.68–4.23) | 0.541 |
| CK (IQR; U/l) | 105.5 (70–138) | 90‡ (72.75–130) | 99.5 (73.75–117.25) | 107 (89–140) | 112 (100–136.5) | 0.047† | 118 (81.5–145.5) | 132 (90.25–166) | 103 (79.5–125.75) | 118 (93–141.5) | 110 (88.75–136.75) | 0.323 |
| Hb (IQR; g/dl) | 9.7 (8.8–11.9) | 9.4 (8.45–11.17) | 10.05 (8.92–11.72) | 10.45 (9.3–11.85) | 10 (9.15–11.4) | 0.084 | 10.05 (7.87–10.57) | 9.9 (8.6–11) | 9.3 (7.7–11.4) | 10 (8.5 – 11) | 10.15 (9–11.47) | 0.361 |
| SBP (IQR; mmHg) | 130 (120–150) | 130 (110–140) | 135 (110–140) | 130 (110–150) | 130 (110–140) | 0.453 | 130 (120–140) | 130 (120–140) | 130 (117.5–140) | 130 (120–140) | 130 (130–140) | 0.472 |
| DBP (IQR; mmHg) | 80 (70–90) | 80 (77.5–90) | 80 (77.5–90) | 80 (70–90) | 80‡ (70–90) | 0.330 | 85 (77.5–90) | 80 (80–90) | 80 (70–90) | 80 (80–90) | 90 (80–90) | 0.104 |
| IDWG (IQR; %) | 3.18 (1.99–4.82) | 3.25 (2.37–4.18) | 3.3 (2.36–4.46) | 2.99 (1.97–4.46) | 2.86 (2.22–4.62) | 0.934 | 3.56 (2.11–4.29) | 3.24 (2.07–4.2) | 3.23 (1.88–3.7) | 2.87 (2–3.9) | 2.36 (1.76–3.75) | 0.184 |
| Sodium (IQR; mEq/l) | 148 (140.5–166.25) | 143 (139.75–150) | 151‡ (144.75–153.25) | 143 (137–150) | 146 (140.5–151.5) | 0.013† | 147 (140.25–151) | 140.5 (137–144.25) | 146.5 (138–150.25) | 147 (139.5–151.75) | 142 (138–147.5) | 0.025† |
| Potassium (IQR; mmol/l) | 4.64 (3.98–5.11) | 4.28 (3.89–4.96) | 4.89‡ (4.36–5.31) | 4.93 (4.53–5.3) | 4.88 (4.06–5.13) | 0.021† | 4.65 (4.01–5.32) | 4.52 (3.88–5.03) | 4.2 (3.8–4.9) | 4.66 (4.11–5.06) | 4.68 (4.22–5.01) | 0.609 |
| Calcium (IQR; mg/dl) | 8.45 (7.98–9.04) | 8.1 (7.83–8.85) | 8.83‡ (8.19–9.05) | 8.8 (8.07–9.25) | 8.32 (7.81–9.22) | 0.311 | 8.07 (7.8–8.77) | 8.41 (7.67–8.8) | 8.15 (7.62–8.68) | 8.42 (7.82–8.84) | 8.3 (7.82–8.79) | 0.230 |
| Phosphorus (IQR; mg/dl) | 4.45 (3.43–5) | 4.59 (3.27–5.52) | 4.55 (3.5–5.8) | 4 (3.59–5.05) | 4.9 (3.56–5.8) | 0.606 | 4.39 (3.66–5.32) | 4.5 (3.7–5.4) | 4.23 (3.44–5.2) | 4.7 (3.59–5.5) | 4.52 (3.41–5.4) | 0.613 |
†p < 0.05: Significant within the groups (Friedman’s test).
‡p < 0.05: Significant between the two groups (Mann–Whitney U test).
DBP: Diastolic blood pressure; Hb: Hemoglobin; IDWG: Interdialytic weight gain; IQR: Interquartile range; SBP: Systolic blood pressure.
After 16 weeks, within group comparison revealed significant decrease in serum ox-LDL, TC, TGs and LDL-C as well as significant increase in GSH-Px following the administration of both fenofibrate and simvastatin (p < 0.05). However, no significant differences were observed in the changes of these parameters between both groups (p > 0.05, Mann–Whitney U test) during the whole study period. Moreover, significant difference was observed in HDL-C level 2 months following administration (p = 0.013, Mann–Whitney U test) where the fenofibrate group showed higher levels than that observed in the simvastatin group. Following the administration of both fenofibrate and simvastatin, no significant changes in serum CRP levels in both groups were observed (p > 0.05, Wilcoxon signed-rank test). However, simvastatin group showed significantly lower CRP level than fenofibrate at the end of the study (p = 0.025, Mann–Whitney U test). Before conducting the multivariable adjusted, baseline-controlled ANCOVA, the data of the primary outcomes were non-normally distributed. Thus, a log transformation of the data has been done to be able to conduct ANCOVA. No significant differences were observed between patients in the effect on ox-LDL (p = 0.683), GSH-Px (p = 0.37), TC (p = 0.834), TGs (p = 0.576), LDL-C (p = 0.563) and HDL-C (p = 0.466) after fenofibrate and simvastatin administrations taking into account the baseline concentrations of these parameters as covariates. CRP was the only variable the have changed differently under the effect of the two drugs (p = 0.025) confirming conventional statistical analysis results that simvastatin treatment was associated with significantly lower CRP levels compared with fenofibrate. The changes in the efficacy outcomes between the two treatment groups after 16 weeks are shown in Figure 1 & Tables 3 & 4.
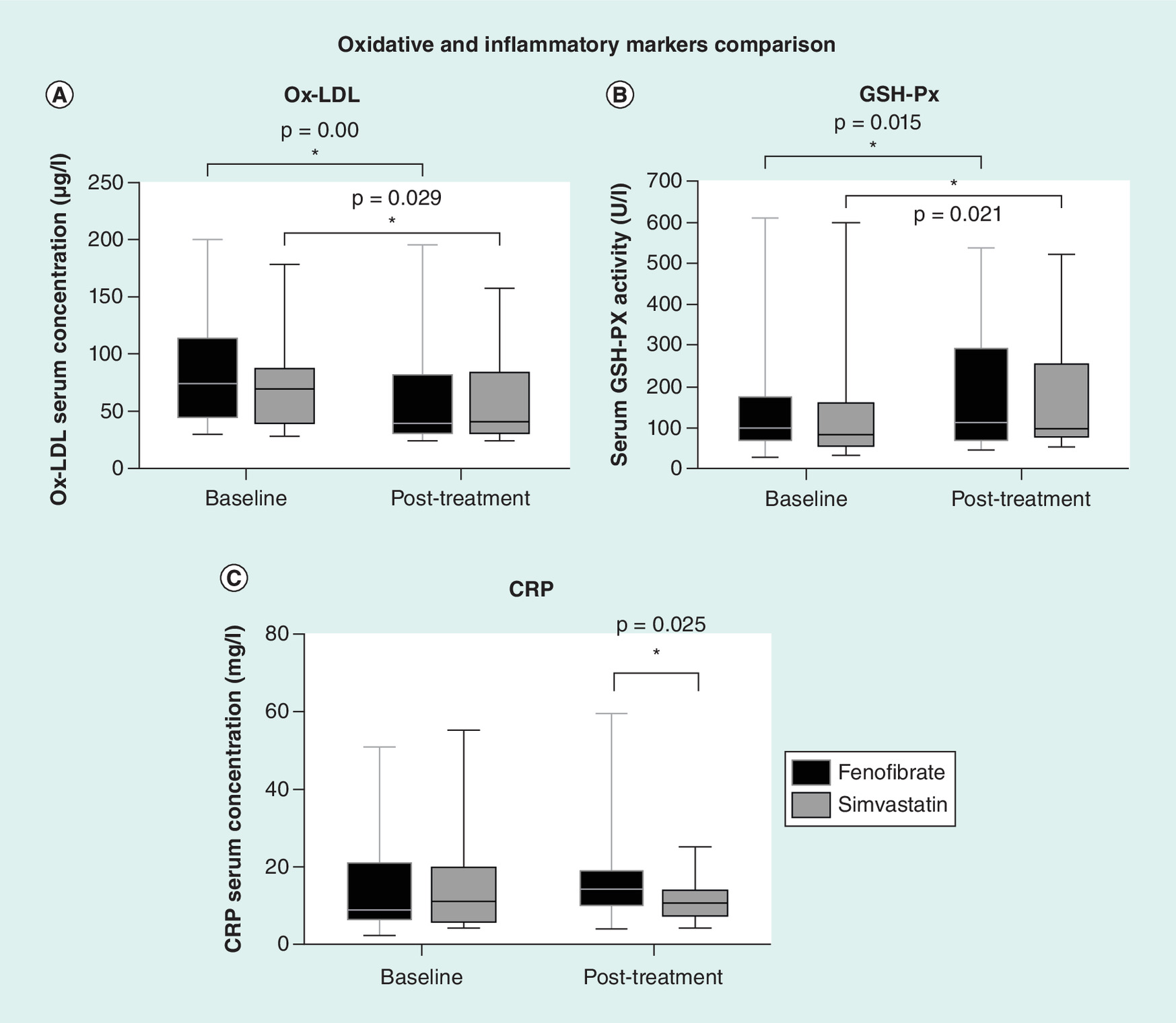
Figure 1. Comparison of the changes in the oxidative stress and inflammatory marker levels.
(A) Effect on oxidized low-density lipoprotein levels. (B) Effect on the antioxidant glutathione peroxidase marker levels. (C) Effect on inflammatory C-reactive protein marker levels.
CRP: C-reactive protein; GSH-Px: Glutathione peroxidase; Ox-LDL: Oxidized low-density lipoprotein.
| Parameters | Fenofibrate group (group 1) | Simvastatin group (group 2) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 30 | n = 29 | p-value† | n = 30 | n = 28 | p-value† | |||||||
| Baseline | 1st month | 2nd month | 3rd month | 4th month | Baseline | 1st month | 2nd month | 3rd month | 4th month | |||
| TC (IQR; mg/dl) | 245.5 (210.33–270.25) | 207.5 (187.75–252.5) | 197 (177.23–219.78) | 181 (162–196) | 184 (164.5–194) | 0.000† | 257 (224–286) | 204 (183–235) | 193 (165–224) | 182 (160–211) | 183 (164–203.5) | 0.000† |
| LDL-C (IQR; mg/dl) | 157.59 (114.59–183.95) | 131.29 (102.07–155.63) | 114.05 (97.14–140.88) | 105.09 (78.49–122.38) | 105.64 (80.73–124.63) | 0.000† | 166.22 (140.4–200.8) | 130.38 (105.75–157.98) | 120.3 (95.46–133.66) | 103.5 (82.55–122.3) | 113.25 (85.93–127.71) | 0.000† |
| HDL-C (IQR; mg/dl) | 42.46 (35.75–51.89) | 53.92 (41.66–66.98) | 53.92‡ (41.66–66.98) | 48.71 (35.21–63.84) | 43.89 (33.13–64.12) | 0.027† | 46.09 (31.92–61.18) | 52.38 (36.1–63.72) | 41.42 (32.48–53.31) | 44.67 (35.01–58.63) | 46.36 (36.56–52.72) | 0.206 |
| TGs (IQR; mg/dl) | 234.5 (202.42–287.47) | 172.5 (131.75–185.75) | 151.5 (98.25–182.75) | 137 (112.5–177) | 139 (114–180) | 0.000† | 198 (188–248) | 176 (110–196) | 158 (121–195) | 155 (117.5–198.5) | 139 (108–183) | 0.000† |
†p < 0.05: Significant within the groups (Friedman’s test).
‡p < 0.05: Significant between the two groups (Mann–Whitney U test).
HDL-C: High-density lipoprotein cholesterol; IQR: Interquartile range; LDL-C: Low-density lipoprotein cholesterol; TC: Total cholesterol; TGs: Triglycerides.
| Parameters | Fenofibrate group | Simvastatin group | p-value† |
|---|---|---|---|
| Change (%) | Change (%) | ||
| Ox-LDL (μg/l) | -17.96 | -13.26 | 0.257 |
| GSH-Px (U/l) | 32.01 | 35.40 | 0.473 |
| CRP (mg/l) | 33.33 | -21.82 | 0.109 |
| TC (mg/dl) | -25.79 | -30.34 | 0.191 |
| TGs (mg/dl) | -44.86 | -26.82 | 0.114 |
| LDL-C (mg/dl) | -32.81 | -38.52 | 0.278 |
| HDL-C (mg/dl) | -2.03 | -11.04 | 0.299 |
†Data are presented as median.
Mann–Whitney U test at p < 0.05.
HDL-C: High-density lipoprotein cholesterol; LDL-C: Low-density lipoprotein cholesterol; Ox-LDL: Oxidized low-density lipoprotein cholesterol; TC: Total cholesterol; TGs: Triglycerides.
In order to ensure that the patients were taking the medications properly as prescribed, patient compliance was assessed. The percentage compliance was calculated for each patient every month till the end of the study. Significant increase in compliance in both fenofibrate group from 93 to 99% (p = 0.022, Friedman’s test) and simvastatin group from 94 to 99% (p = 0.002, Friedman’s test) was observed at the end of the study.
Discussion
Major trials evaluating the role of dyslipidemia treatment in primary and secondary prevention of CVD in HD are lacking [24]. To the best of our knowledge, this is the first trial to compare the efficacy and safety of fenofibrate versus simvastatin in HD patients using intermittent low dose regimen. In assessing the efficacy and safety using this regimen, both drugs have favorable safety profile in dialysis patients and resulted in improved oxidative stress status and significant lipid-lowering effect.
Increased oxidative stress is a characteristic nontraditional risk factor in HD patients that results in accelerated progression of atherosclerosis. This is confirmed by the finding of reduced activity of the antioxidant GSH-Px enzyme with subsequent progressive increase in lipid peroxidation (increased the atherogenic ox-LDL), evidence of endothelial injury and increased atherosclerosis risk among HD patients [12,25]. In our study, both simvastatin and fenofibrate were associated with significantly increased activity of GSH-Px and reduced ox-LDL levels. These effects were comparable between the two treatment groups. This is in agreement with previous studies where the antioxidant effect of simvastatin was either attributed to lowering in the ox-LDL level [12], malondialdehyde level, a lipid peroxidation index [9] or increasing GSH-Px enzyme activity by increasing serum selenium concentration which is a component of catalytic sites of GSH-Px [11]. On the other hand, there is a lack of studies confirming the antioxidant effect of fenofibrate in HD patients except one study which reported that the intermittent reduced dose of fenofibrate resulted in a less pro-oxidative pattern of the aminothiol redox status [14]. Unlike our results, Dummer et al. [26] and Dogra et al. [27] reported that statins and fibrates caused nonsignificant effects on oxidative stress markers in CKD patients when used for 8 and 6 weeks, respectively. This may be attributed to the shorter courses of treatment used compared with our study. Thus, we can conclude that the antioxidant effect of both drugs is possibly observed on prolonged use only.
In our study, all patients had elevated level of CRP confirming that HD patients have higher degree of inflammation; making them ideal candidates to study the efficacy of drugs on inflammatory markers especially CRP [8,10]. Although simvastatin group showed significantly lower CRP level than fenofibrate at the end of the study, there were nonsignificant changes in CRP along the study period in both groups. These nonsignificant changes might be attributed to the short study period. Kirmizis et al. [8] showed that simvastatin (10 mg/day) resulted in significant reduction of CRP only after 6 months, but not after 3 months of treatment. Dummer et al. [26] reported that the 8-week use of 20 mg simvastatin resulted in nonsignificant effect on CRP. van den Akker et al. [12] also showed nonsignificant change in CRP after 18 weeks in accordance with our study. However, treating HD patients with higher doses or longer courses of statins resulted in significant reduction of CRP level, thus supporting the anti-inflammatory effect of statins in HD patients [8,10,11,28,29]. On the other hand, Makowka et al. [14] found out that 4-week use of fenofibrate did not produce significant change in CRP in accordance with our study. The lack of studies evaluating the anti-inflammatory effect of fibrates and comparing them with statins in dialysis patients increases the need for more prospective randomized trials involving large number of patients.
When dealing with HD patients, two main concerns have to be taken into consideration. First, the adverse events of simvastatin, namely myopathy and increased liver transaminases, are often dose related [30]. However, when simvastatin is used in doses not exceeding 20 mg, no significant difference in adverse events (including patients’ symptoms, increased hepatic enzymes and elevated CK) was observed [7,13]. Moreover, Yigit et al. [13] reported that intermittent simvastatin administered only on dialysis days can be used as an alternative to the continuous therapy with similar efficacy and tolerability in hypercholesterolemic HD patients. Second, HD patients are more prone to the toxic effect of fenofibrate because it is eliminated mainly through kidney and poorly dialyzed [6]. However, Makowka et al. [14] have found that the safety profile of fenofibrate (100 mg administered on dialysis days) was satisfactory with no significant adverse events being experienced in HD patients. Therefore, this study was conducted for 16 weeks using low dose therapy and limiting the administration of the drugs to dialysis days only (intermittent regimen) considering the above safety concerns.
In our study, none of the patients in both groups had any complaints of muscle pain, weakness, or elevation of serum CK, ALT or AST more than three-times ULN. This may be due to the fact that we excluded the patients who were intolerant or used any fibrates or statins 6 months prior to the study. Thus, the simultaneous use of fibrates and statins with its associated highest risk of rhabdomyolysis was avoided [16]. Moreover, both drugs were administered only on dialysis days and in low dose regimen guaranteeing minimum toxicity [13,14]. Despite the significant rise in serum ALT in fenofibrate group, the serum levels remained within the normal ranges except for only one patient who experienced increase in ALT and AST more than two-times ULN at the end of the study.
At each monthly visit, patients were asked whether they took their drug regularly, prescriptions were refilled, tablets were counted and percentage compliance were calculated. There was a significant increase in compliance in both fenofibrate and simvastatin group to reach 99% by the end of the study. Explaining the treatment benefits to the patients and taking into consideration any of their complaints in the monthly visit might have contributed to the improved compliance during the study. In accordance with our study, Yigit et al. [13] showed that a high rate of compliance (93.3%) was observed in the intermittent simvastatin group. Moreover, Makowka et al. [14] ensured good compliance by administering intermittent fenofibrate in the dialysis centers.
The main limitation of this study was the small sample size due to difficulty in recruiting patients, only 60 out of 402 patients were found to comply with the study criteria, in addition to limited resources prohibiting the recruitment of more patients. Thus, this might have masked any differences existing between the two treatments and lead to decreasing the statistical power. However, the comparison in this small study has not been done before and therefore opens the door for further large-scale research. The limited resources also gave rise to other limitations which were the lack of placebo control group and inability to administer the medications for longer period with long term follow-up of clinical end points such as CVD development and mortality.
Conclusion
In summary, we found out that both the drugs had comparable efficacy and safety when used as intermittent low dose regimen in HD patients. Satisfactory safety profile and improved lipid profile and oxidative stress status are the main outcomes for both simvastatin and fenofibrate in HD in this study. Moreover, patients might have benefited from the use of intermittent low dose regimen in minimizing the drug related adverse events. However, these results need to be confirmed by larger studies with longer follow-up periods to ensure that the effects of both drugs will be sustained with favorable effect on CVD development and mortality rates.
In this study we compared the tolerability of intermittent low dose fenofibrate versus simvastatin in hemodialysis patients and their effects on lipid profile, oxidative stress and inflammation.
Patients & methods
Patients were recruited from five dialysis centers in Egypt (multicenter study).
Eligible patients were randomly assigned to receive either fenofibrate 100 mg (group 1) or simvastatin 20 mg (group 2) three-times a week after the dialysis session with a 1:1 allocation (block randomization).
The effect of drugs on lipid profile, oxidized low-density lipoprotein, glutathione peroxidase and C-reactive protein were compared before and after 16-week treatment.
For safety; serum urea, creatinine, ALT, AST, albumin, hemoglobin, CK and electrolytes (sodium, potassium, calcium and phosphorous) levels were monthly measured.
Results
After 16 weeks, the median reduction in total cholesterol, triglycerides, low-density lipoprotein cholesterol and oxidized low-density lipoprotein cholesterol was 25.79, 44.86, 32.8 and 17% respectively in group 1 as compared with 30.34, 26.8, 38.52 and 13% in group 2. Moreover, glutathione peroxidase increased significantly by 32.01 and 35.4% in group 1 and 2, respectively (p < 0.05). There was no significant difference in C-reactive protein in both groups (p > 0.05).
Both drugs were well tolerated during the study with no serious side effects being experienced.
Conclusion
Fenofibrate has comparable efficacy and reliability as simvastatin when used in low dose intermittent regimen in hemodialysis patients.
Satisfactory safety profile, decreased oxidants, increased antioxidant markers and favorable lipid profile are the main outcomes for both simvastatin and fenofibrate when used in hemodialysis.
Larger studies with longer follow-up periods are needed to confirm our new findings.
Acknowledgements
The authors acknowledge the efforts made by the nursing staff in the dialysis units in Kasr Al Aini, New Kasr Al Aini and Ahmed Maher Teaching Hospitals, Cairo, Egypt.
Financial & competing interests disclosure
Funding was received from Faculty of Pharmacy, Cairo University, Egypt. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of the Faculty of Pharmacy, Cairo University.
Informed consent was obtained from all individual participants included in the study.
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Saran R, Li Y, Robinson B et al. US Renal Data System 2015 annual data report: epidemiology of kidney disease in the United States. Am. J. Kidney Dis. 67(3 Suppl. 1), S219–S226 (2016).
2.
Prichard SS. Impact of dyslipidemia in end-stage renal disease. J. Am. Soc. Nephrol. 14(9 Suppl. 4), S315–S320 (2003).
3.
Levey AS, Beto JA, Coronado BE et al. Controlling the epidemic of cardiovascular disease in chronic renal disease: what do we know? What do we need to learn? Where do we go from here? National Kidney Foundation Task Force on cardiovascular disease. Am. J. Kidney Dis. 32(5), 853–906 (1998).
4.
Sarnak MJ, Levey AS, Schoolwerth AC et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Hypertension 42(5), 1050–1065 (2003).
5.
Modaresi A, Nafar M, Sahraei Z. Oxidative stress in chronic kidney disease. Iran J. Kidney Dis. 9(3), 165–179 (2015).
6.
Moutzouri E, Kei A, Elisaf MS, Milionis HJ. Management of dyslipidemias with fibrates, alone and in combination with statins: role of delayed-release fenofibric acid. Vasc. Health Risk Manag. 6, 525–539 (2010).
7.
Shurraw S, Tonelli M. Statins for treatment of dyslipidemia in chronic kidney disease. Perit. Dial. Int. 26(5), 523–539 (2006).
8.
Kirmizis D, Papagianni A, Dogrammatzi F et al. Effects of simvastatin on markers of inflammation, oxidative stress and endothelial cell apoptosis in patients on chronic hemodialysis. J. Atheroscler. Thromb. 17(12), 1256–1265 (2010).
9.
Nishikawa O, Mune M, Miyano M et al. Effect of simvastatin on the lipid profile of hemodialysis patients. Kidney Int. Suppl. 71, S219–S221 (1999).
10.
Shahbazian H, Atrian A, Yazdanpanah L, Lashkarara GR, Zafar Mohtashami A. Anti-inflammatory effect of simvastatin in hemodialysis patients. Jundishapur. J. Nat. Pharm. Prod. 10(1), e17962 (2015).
11.
Taccone-Gallucci M, Noce A, Bertucci P et al. Chronic treatment with statins increases the availability of selenium in the antioxidant defence systems of hemodialysis patients. J. Trace Elem. Med. Biol. 24(1), 27–30 (2010).
12.
van den Akker JM, Bredie SJ, Diepenveen SH, van Tits LJ, Stalenhoef AF, van Leusen R. Atorvastatin and simvastatin in patients on hemodialysis: effects on lipoproteins, C-reactive protein and in vivo oxidized LDL. J. Nephrol. 16(2), 238–244 (2003).
13.
Yigit F, Muderrisoglu H, Guz G et al. Comparison of intermittent with continuous simvastatin treatment in hypercholesterolemic patients with end stage renal failure. Jpn Heart J. 45(6), 959–968 (2004).
•• Compares the efficacy of intermittent versus continuous therapy of simvastatin in hemodialysis.
14.
Makowka A, Dryja P, Chwatko G, Bald E, Nowicki M. Treatment of chronic hemodialysis patients with low-dose fenofibrate effectively reduces plasma lipids and affects plasma redox status. Lipids Health Dis. 11, 47 (2012).
•• Studies the efficacy and safety of intermittent fenofibrate versus placebo in hemodialysis patients.
15.
Tkáč I, Molčányiová A, Javorský M, Kozárová M. Fenofibrate treatment reduces circulating conjugated diene level and increases glutathione peroxidase activity. Pharmacol. Res. 53(3), 261–264 (2006).
16.
Wu J, Song Y, Li H, Chen J. Rhabdomyolysis associated with fibrate therapy: review of 76 published cases and a new case report. Eur. J. Clin. Pharmacol. 65(12), 1169–1174 (2009).
17.
Ansquer J-C, Dalton RN, Caussé E, Crimet D, Le Malicot K, Foucher C. Effect of fenofibrate on kidney function: a 6-week randomized crossover trial in healthy people. Am. J. Kidney Dis. 51(6), 904–913 (2008).
18.
Ting R-D, Keech AC, Drury PL et al. Benefits and safety of long-term fenofibrate therapy in people with type 2 diabetes and renal impairment the FIELD study. Diabetes Care 35(2), 218–225 (2012).
19.
Clinical Trials Database: NCT02886299. https://clinicaltrials.gov/ct2/show/NCT02886299
20.
Hemodialysis Adequacy 2006 Work Group. Clinical practice guidelines for hemodyalisis adequacy – update 2006. Am. J. Kidney Dis. 48(1 Suppl. 1), S2–S90 (2006).
21.
Lopez-Gomez JM, Villaverde M, Jofre R, Rodriguez-Benitez P, Perez-Garcia R. Interdialytic weight gain as a marker of blood pressure, nutrition, and survival in hemodialysis patients. Kidney Int. Suppl. 67(Suppl. 93), S63–S68 (2005).
22.
Yang SC, Chiang CK, Hsu SP, Hung KY. Relationship between interdialytic weight gain and nutritional markers in younger and older hemodialysis patients. J. Ren. Nutr. 18(2), 210–222 (2008).
23.
Boudes P. Drug compliance in therapeutic trials: a review. Control. Clin. Trials 19(3), 257–268 (1998).
24.
Omran J, Al-Dadah A, Dellsperger KC. Dyslipidemia in patients with chronic and end-stage kidney disease. Cardiorenal Med. 3(3), 165–177 (2013).
25.
Ahmadpoor P, Eftekhar E, Nourooz-Zadeh J, Servat H, Makhdoomi K, Ghafari A. Glutathione, glutathione-related enzymes, and total antioxidant capacity in patients on maintenance dialysis. Iran J. Kidney Dis. 3(1), 22–27 (2009).
26.
Dummer CD, Thome’ FS, Zingano B, Lindoso A, Veronese FV. Acute effect of simvastatin on inflammation and oxidative stress in chronic kidney disease. J. Nephrol. 21(6), 900–908 (2008).
27.
Dogra G, Irish A, Chan D, Watts G. A randomized trial of the effect of statin and fibrate therapy on arterial function in CKD. Am. J. Kidney Dis. 49(6), 776–785 (2007).
28.
Chang JW, Yang WS, Min WK, Lee SK, Park JS, Kim SB. Effects of simvastatin on high-sensitivity C-reactive protein and serum albumin in hemodialysis patients. Am. J. Kidney Dis. 39(6), 1213–1217 (2002).
29.
Vernaglione L, Cristofano C, Muscogiuri P, Chimienti S. Does atorvastatin influence serum C-reactive protein levels in patients on long-term hemodialysis? Am. J. Kidney Dis. 43(3), 471–478 (2004).
30.
Harper CR, Jacobson TA. Managing dyslipidemia in chronic kidney disease. J. Am. Coll. Cardiol. 51(25), 2375–2384 (2008).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 19 June 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Randomized comparative efficacy and safety study of intermittent simvastatin versus fenofibrate in hemodialysis. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0076
Export citation
Select the citation format you wish to export for this article or chapter.