Efficacy and safety of APT198K for the treatment of infantile colic: a pilot study
Abstract
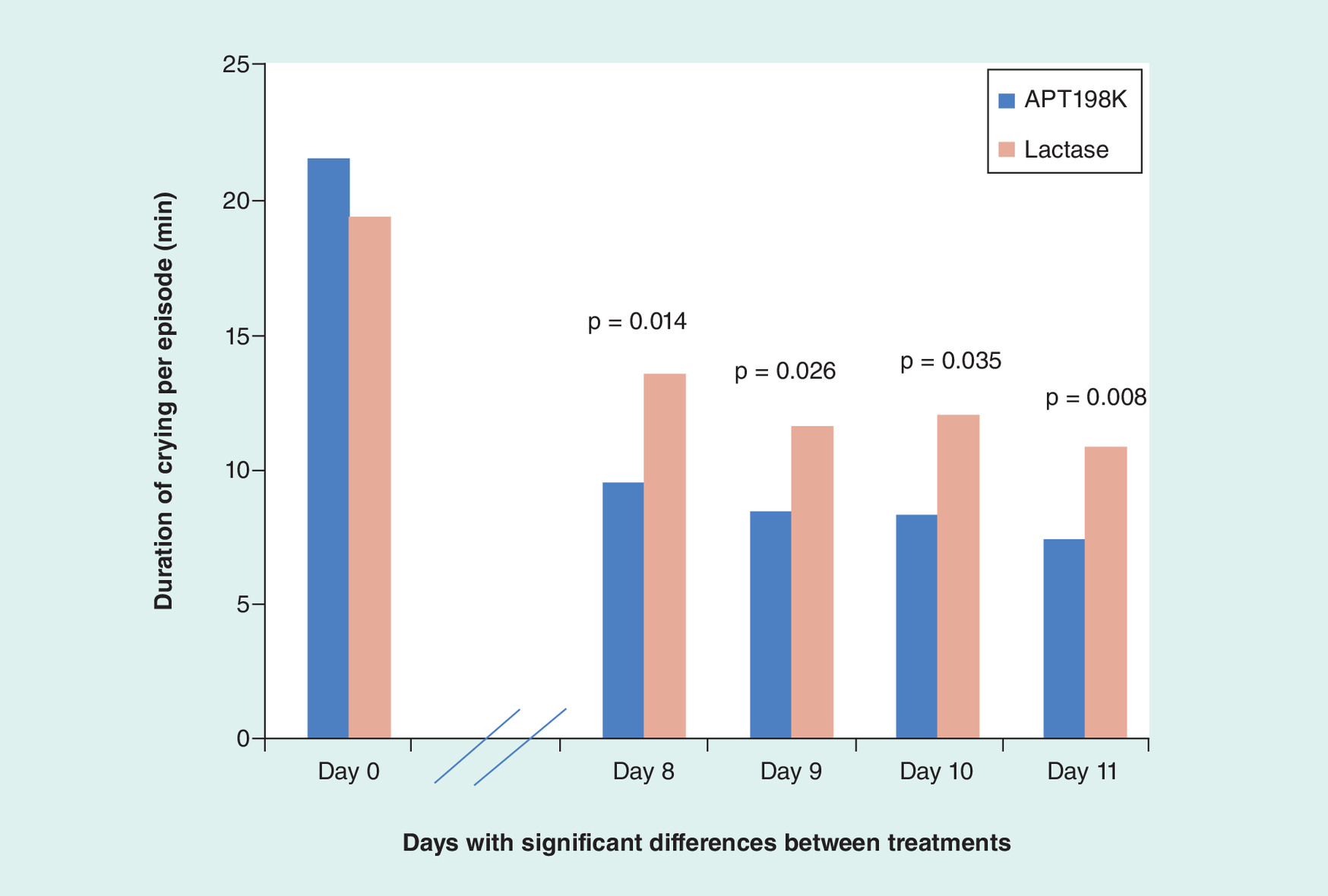
Aim: Comparing efficacy and safety of APT198K (xyloglucan plus heat-killed Lactobacillus reuteri SGL01 and Bifidobacterium brevis SGB01) versus a lactase dietary supplement as first-line treatment of infantile colic. Methods: Randomized, multicenter, open-label, parallel group, active-controlled study, in 46 infants aged 3–16 weeks with infantile colic, receiving APT198K or a lactase dietary supplement for 10 days. Results: Number and duration of crying episodes decreased significantly versus baseline in both groups. On day 8, the mean duration of crying per episode was significantly shorter in the APT198K group compared with the lactase group (9.14 ± 5.34 vs 13.22 ± 5.29 min; p = 0.014) and remained so up to day 11. Conclusion: APT198K decreased the mean duration per crying episode significantly more than a lactase dietary supplement in infants with colic. Further evaluation in larger studies is warranted. Clinical trial registry: EudraCT number 2014-002860-334; https://eudract.ema.europa.eu.

First draft submitted: 24 August 2016; Accepted for publication: 22 November 2016; Published online: 24 January 2017
Infantile colic affects approximately 20% of infants [1] and is one of the most common reasons that parents seek medical advice for babies under 4 months of age [2]. According to Rome IV criteria, infantile colic is defined for research purposes as episodes of inconsolable/unsoothable crying confirmed as lasting more than 3 h per day, on at least 3 out of 7 days [3].
Colic typically begins within the first few weeks of life and resolves before 5 months of age [3,4]. Crying is prolonged, often high-pitched, and tends to occur in the afternoon or evening [3,4]. It is generally accompanied by facial flushing and grimacing, as well as postural changes including clenched fists, flexing of the legs up to the abdomen and arching of the back [3–5]. Abdominal distension and increased gas may also be present [3].
The cause of infantile colic is not known, although gastrointestinal, neurodevelopmental and psychosocial factors have been suggested [4,5]. Consequently, a range of treatments has been suggested [2,6,7]. However, evidence supporting most of these is limited and there is currently no consensus on the optimal approach to the management of the disorder [7].
One therapeutic approach is to administer products containing microbial organisms, either live bacteria (probiotics) or heat-killed bacteria. Infants with colic have low levels of lactobacilli and increased levels of gas-forming coliform bacteria in their intestines [8,9], and there is evidence that probiotics, such as Lactobacillus reuteri DSM 17938 may reduce crying time in mainly breastfed babies with infantile colic [10]. Moreover, beneficial gastrointestinal effects can also be achieved with dead microbes, which produce a similar immunomodulatory effect and anti-inflammatory response within the gastrointestinal mucosa to live microbes [11,12]. Another approach to treatment is to administer exogenous lactase, based on the theory that infants with colic may have transient lactose intolerance [13,14]. There is some evidence that oral lactase can reduce crying time in certain infants with colic [13].
APT198K (provided by Novintethical Pharma SA, Switzerland) is a combined medical device class IIa that is indicated for the treatment of the causes of meteorism, which may be associated with colic. It contains xyloglucan 0.6 g/10 ml, which forms a mechanical barrier over the wall of the gastrointestinal tract, as well as the probiotics L. reuteri SGL01 100 × 109 colony-forming units (CFU)/g and Bifidobacterium brevis SGB01 100 × 109 CFU/g. The aim of this study was to compare the efficacy and safety of APT198K with that of a dietary supplement (Colief®, Crosscare Limited, Ireland) containing lactase 0.40 g (minimum 45,000 ONPGU/g) when used as first-line treatment for infantile colic in neonates and infants.
Methods
Study population
The study included breast and/or formula-fed neonates and infants of both genders, aged between 3 and 16 weeks, who had symptoms of infantile colic (defined as paroxysms of excessive crying in an otherwise healthy baby lasting more than 3 h per day, occurring on more than 3 days in any week and for at least 3 weeks) [15]. The babies had to be developmentally normal for their age, with no organic disease and with normal findings on physical examination. Patients were excluded if they were receiving any other treatment for infantile colic, were allergic to any of the study treatment ingredients, had undergone recent surgery, or had any serious medical condition or need for hospitalization.
Study design & procedures
This was a multicenter, randomized, open-label, parallel group, active-controlled study conducted at medical centers and pediatric hospitals in Romania between October 2014 and January 2015. The study, conducted in accordance with ICH Good Clinical Practice and the principles expressed in the Declaration of Helsinki, was approved by the relevant Independent Ethics Committee. Informed consent was obtained from each patient's legal representative prior to enrollment.
Patients were randomized to receive oral treatment with either APT198K (xyloglucan 0.6 g/ml plus heat-killed L. reuteri SGL01 100 × 109 CFU/g and B. brevis SGB01 100 × 109 CFU/g) or a dietary supplement containing lactase 0.40 g (minimum 45,000 ONPGU/g) (Colief® Infant Drops; hereafter referred to as lactase) for 10 days. APT198K was administered at a dose of 10 drops twice daily. Lactase was administered according to the relevant label (4 drops per milk feed if breastfeeding or bottle-feeding with newly made formula or 2 drops per feed if bottle-feeding using preprepared formula). Randomization was based on a randomization list prepared by a pseudorandom number generator. The randomization list contained 46 randomization positions, allocated between APT198K and lactase in a 1:1 ratio. Each study site received a sub-list of randomization positions from the master list. When a subject was enrolled, the first available randomization position/code from the sub-list was assigned to that subject.
Study visits took place at baseline, day 6 and day 11 (the day after the final treatment day), and included assessments of demographics and medical history (baseline only), weight and length, signs and symptoms associated with infantile colic, and adverse events. The babies’ mothers/caregivers completed daily diaries, recording details of crying episodes and evaluating the evolution of signs and symptoms over time using a 7-point Likert scale (where 1 = very much worse, 2 = much worse, 3 = somewhat worse, 4 = same condition, 5 = somewhat better, 6 = much better, 7 = very much better). The clinical status at baseline was based on symptoms during the 24 h prior to the baseline visit.
Efficacy outcome measures included crying (duration of each crying episode, total daily duration of crying, number of crying episodes per day), bowel symptoms (including bloating and flatulence), tension of the abdominal muscles, facial flushing and postural changes (including curled-up legs or clenched fists). Safety was assessed through the evaluation of adverse events.
Statistical methods
The study sample size was based on the duration of crying. Published literature suggested that the mean duration of crying during an episode was 17.3 min in active-treatment groups and 47.5 min in placebo groups, with a standard deviation (SD) of 28.5 min [16]. For a reduction of 50% in crying duration with active treatment compared with placebo, and assuming 80% power and an error alpha of 5%, it was calculated that 23 subjects per group were needed. Focus was placed on duration of crying per episode as it provides a specific variable to measure. Total crying time is affected by the duration of each episode.
Study variables were analyzed using descriptive statistical methods, to provide mean and SD for continuous variables, and absolute and relative frequency counts for categorical variables. Exploratory statistical tests were performed to determine whether there were differences in crying duration and other variables between groups (using the t-test, Mann–Whitney U test, Chi square test or Wilcoxon's test, as appropriate). Differences in group scores were compared between groups using analysis of variance.
Results
A total of 46 patients were randomized in the study – 23 in each group (Figure 1). All subjects were included in the analysis. There were no clinically significant differences between the groups in terms of demographics and general characteristics at baseline (Table 1). Just over half of the study population was female. The mean ± SD age of the overall population was 45 ± 28 days. The APT198K group had a slightly lower mean age (41 days) than the lactase group (49 days) but this was not considered clinically relevant (and would only be of benefit for the lactase group as they were 1 week older and colic spontaneously decreases with age).
Crying
The mean ± SD duration of crying per episode decreased in both the APT198K and lactase groups during treatment, with a statistically significant reduction versus baseline apparent as early as day 1 (p = 0.033 for both groups combined). The mean ± SD duration was significantly shorter in the APT198K group compared with the lactase group on day 8, -9, -10 and -11 (Figure 2 & Table 2).
The total duration of crying per day and the total number of crying episodes per day decreased from baseline in both groups, with no significant between-group differences evident (Table 2).
Bowel symptoms
There was a significantly greater improvement in bowel symptoms (bloating and flatulence) on day 6 versus baseline in the APT198K group compared with the lactase group, as indicated by a higher mean Likert scale score (p = 0.005) (Table 3). APT198K was also superior to lactase in terms of the improvement seen on day 11 versus baseline (p = 0.038) (Table 3).
When comparing mean ± SD changes in bowel symptoms with the previous 24-h period, significantly greater improvements were seen with APT198K compared with lactase on day 1 (4.3 ± 0.55 vs 4.0 ± 0.30; p = 0.028), day 4 (5.35 ± 0.93 vs 4.57 ± 0.59; p = 0.002), day 5 (5.52 ± 0.89 vs 4.87 ± 0.62; p = 0.006) and day 6 (5.70 ± 0.82 vs 5.13 ± 0.81; p = 0.024).
Abdominal muscle tension
Based on Likert scale scores, a significantly greater reduction in the tension of the abdominal muscles versus baseline was observed on day 6 in the APT198K group compared with the lactase group (p = 0.004), but not on day 11 (Table 3).
Compared with the previous 24-h period, significantly greater mean ± SD improvements in abdominal muscle tension were seen with APT198K compared with lactase on day 4 (Likert scale score 5.48 ± 0.84 vs 4.78 ± 0.51; p = 0.002), day 5 (5.57 ± 1.03 vs 4.91 ± 0.59; p = 0.013) and day 6 (5.70 ± 0.82 vs 5.13 ± 0.81; p = 0.024).
Facial flushing
A significantly greater reduction in facial flushing versus baseline was observed in the APT198K group compared with the lactase group on day 6 (p < 0.05), but not on day 11 (Table 3).
Compared with the previous 24-h period, significantly greater mean ± SD improvements in facial flushing were seen with APT198K compared with lactase on day 4 (Likert scale score 5.26 ± 1.01 vs 4.61 ± 0.65; p = 0.013), day 5 (5.48 ± 1.08 vs 4.78 ± 0.60; p = 0.011) and day 6 (5.74 ± 1.05 vs 5.00 ± 0.79; p = 0.01).
Postural changes
Postural changes (including curled-up legs and clenched fists) were reduced significantly versus baseline in the APT198K group compared with the lactase group on both day 6 (p < 0.05) and day 11 (p = 0.012) (Table 3).
Compared with the previous 24-h period, significantly greater mean ± SD improvements in postural changes were seen with APT198K versus lactase on day 5 (Likert scale score 5.74 ± 1.05 vs 4.96 ± 0.47; p = 0.003) and day 6 (5.96 ± 0.92 vs 5.17 ± 0.77; p = 0.003).
Adverse events
Overall, both treatments appeared to be generally well tolerated. The only minor adverse event reported was vomiting (lasting 2 min) in a baby receiving APT198K.
Discussion
The results of this study suggest that APT198K is more effective than a lactase dietary supplement for the management of infantile colic.
Although infantile colic is a self-limiting disorder that usually resolves by around 4 months of age [4], it is distressing and stressful for parents [17,18]. A key aspect of the management of the condition is to provide reassurance and support to the parents [2,4]; however, they are often keen to explore additional therapeutic options [2]. There is currently no consensus about the best approach for infantile colic, and the level of evidence for many of the available options is weak [2,7]. No pharmacological agents have shown definitive efficacy, and some are associated with adverse effects [2]. A range of dietary interventions have been tried, although the quality of the supporting evidence varies [2,7,19]. Additional well-designed trials are needed to confirm the most effective interventions for infantile colic, and the current study adds to this body of evidence.
Both APT198K and lactase were effective at reducing the number and duration of crying episodes compared with baseline, but from day 8 of treatment onward APT198K provided a significantly greater reduction in the mean duration of crying episodes compared with lactase. In addition, APT198K provided significantly greater improvements in terms of bloating/flatulence, abdominal muscle tension, facial flushing and postural changes when day 6 of treatment was compared with baseline. This remained the case for bowel symptoms and postural changes at the end of the treatment period. When individual 24-h periods were compared, APT198K provided significantly greater improvements than lactase from day 1 for bowel symptoms, day 4 for abdominal muscle tension and facial flushing, and day 5 for postural changes, although these differences did not continue beyond day 6 of treatment. Both treatments were well tolerated, with just one patient, in the APT198K group, experiencing an adverse event (vomiting).
APT198K contains a combination of xyloglucan and heat-killed bacteria. Studies suggest that the gut microbiota is disturbed in infants with colic [10,20–23]. In particular, these babies appear to have reduced levels of lactobacilli and increased levels of coliform bacteria [9,10]. Probiotics (products containing live bacteria) promote microbial diversity and may reduce levels of gas-forming coliform bacteria [24,25], and it has been shown that enhancing the levels of certain bacteria, such as L. reuteri DSM 17938 can reduce infant distress [10]. Clinical trials of probiotics in infantile colic have produced variable results [26,27], but a recent meta-analysis of six trials concluded that L. reuteri DSM 17938 may reduce crying time in infants with colic [10]. APT198K contains heat-killed L. reuteri SGL01 and B. brevis SGB01. Beneficial biological responses can be achieved with either probiotics or products containing dead bacteria [11,12]. Both live and dead microbes exert immunomodulatory effects and induce an anti-inflammatory response within the gastrointestinal mucosa, while live bacteria also modify the gastrointestinal microflora [11,12]. The administration of live microbes may be associated with safety concerns in some patients, and products containing dead microbes could be a safer alternative which provides similar benefits [11,12]. Moreover, products containing dead bacteria have advantages over probiotics in terms of the ease of production and storage. The other component of APT198K, xyloglucan, is a water-soluble, polysaccharide hemicellulose extracted from the tamarind tree (Tamarindus indica) [28,29]. It is not broken down by digestive enzymes and passes through the gastrointestinal tract, forming a protective film over the mucosa, which helps improve the function of the intestinal barrier [29].
The comparator used in the study was a lactase dietary supplement that is indicated for the treatment of transient lactose intolerance in infants with colic [11]. Transient lactose intolerance is recognized as a possible causative factor in some infants with colic [11,14]. Although clinical studies have produced mixed results [11,30–32], the largest trial found that pretreating feeds with lactase reduced median crying time and breath hydrogen (an indirect biomarker of hypolactasia) significantly compared with placebo, and a reduction of more than 45% in both parameters was achieved in 26% of participants [11]. Although not all experts recommend its use in infantile colic [19], some guidance suggests it as a possible treatment option [33].
The main limitations of the study were the open design and the small sample size. An open-label design was used in order to facilitate enrollment of an adequate number of participants in a reasonable timescale, by ensuring parents could know what therapy their child was being given at any time. Larger studies using a double-blind design would be helpful to confirm the effect of APT198K in infantile colic. Another limitation was the use of lactase as the active comparator, because it is likely that this enzyme would only be effective in infants whose colic was associated with temporary lactose intolerance, and it is not known what proportion of the study population had this. Since APT198K contains heat-killed bacteria, studies comparing it with other heat-killed bacterial products and with probiotics would be helpful in the future. In addition, follow-up assessments to check for relapse were not undertaken.
Conclusion
The results of this study suggest that in infants with colic, APT198K may decrease the mean duration per crying episode to a greater extent than seen with a lactase dietary supplement and that it is well tolerated. Further evaluation in larger studies is warranted.
| Variable | APT198K (n = 23) | Lactase (n = 23) |
|---|---|---|
| Gender (male/female), n | 11/12 | 10/13 |
| Age (days): | ||
| – Mean ± standard deviation | 41.04 ± 27.29 | 48.87 ± 28.83 |
| – Median (range) | 31.0 (14–104) | 42.0 (14–98) |
| Apgar score: | ||
| – Mean ± standard deviation | 9.17 ± 0.77 | 8.91 ± 0.79 |
| – Median (range) | 9.0 (8–10) | 9.0 (7–10) |
| Weight (kg): | ||
| – Mean ± standard deviation | 4.21 ± 1.08 | 4.24 ± 1.13 |
| – Median (range) | 4.0 (2.9–6.8) | 4.2 (2.7–6.9) |
| Length (cm): | ||
| – Mean ± standard deviation | 53.87 ± 2.71 | 53.74 ± 4.24 |
| – Median (range) | 54.0 (49–61) | 53.0 (46–63) |
| Variable and timing of assessment | APT198K (n = 23) | Lactase (n = 23) |
|---|---|---|
| Duration of crying per episode (min) | ||
| Baseline: | ||
| – Mean ± SD | 21.17 ± 10.27 | 19.00 ± 9.43 |
| – Median (range) | 20.0 (5–40) | 18.0 (5–40) |
| Day 6: | ||
| – Mean ± SD | 11.41 ± 6.14 | 14.04 ± 4.98 |
| – Median (range) | 10 (2–24) | 15 (3–30) |
| Day 11: | ||
| – Mean ± SD | 7.05 ± 4.17* | 10.48 ± 4.01 |
| – Median (range) | 5 (2–18) | 10 (3–17) |
| Total duration of crying per day (min) | ||
| Baseline: | ||
| – Mean ± SD | 113.35 ± 76.39 | 98.61 ± 56.28 |
| – Median (range) | 90.00 (25–320) | 80.00 (35–240) |
| Day 6: | ||
| – Mean ± SD | 48.64 ± 65.06 | 57.52 ± 37.23 |
| – Median (range) | 29.50 (8–145) | 60 (1–9) |
| Day 11: | ||
| – Mean ± SD | 22.62 ± 23.71 | 33.13 ± 24.24 |
| – Median (range) | 11 (3–72) | 30 (5–77) |
| Number of crying episodes per day | ||
| Baseline: | ||
| – Mean ± SD | 5.26 ± 1.42 | 5.48 ± 1.56 |
| – Median (range) | 5 (3–8) | 5 (3–9) |
| Day 6: | ||
| – Mean ± SD | 5.59 ± 6.19 | 4.22 ± 2.35 |
| – Median (range) | 3.50 (1–6) | 4 (1–9) |
| Day 11: | ||
| – Mean ± SD | 2.81 ± 1.53 | 2.96 ± 1.63 |
| – Median (range) | 2.50 (1–5) | 3 (1–7) |
Values are mean ± SD.
*p = 0.008 vs lactase group.
SD: Standard deviation.
| Variable and timing of assessment | APT198K (n = 23) | Lactase (n = 23) | p-value for difference between groups |
|---|---|---|---|
| Bowel symptoms (bloating, flatulence) | |||
| Day 6: | 0.005 | ||
| – Mean ± SD | 5.87 ± 0.54 | 4.96 ± 0.47 | |
| – Median (range) | 6.00 (5, 7) | 5.00 (4, 6) | |
| Day 11: | 0.038 | ||
| – Mean ± SD | 6.39 ± 0.78 | 5.91 ± 0.73 | |
| – Median (range) | 7.00 (4, 7) | 6.00 (4, 7) | |
| Abdominal muscle tension | |||
| Day 6: | 0.004 | ||
| – Mean ± SD | 5.70 ± 0.82 | 5.04 ± 0.63 | |
| – Median (range) | 1 (0, 1) | 1 (0, 1) | |
| Day 11: | 0.081 | ||
| – Mean ± SD | 6.47 ± 0.43 | 5.76 ± 0.55 | |
| – Mean ± SD | 1 (0, 1) | 1 (0, 1) | |
| Facial flushing | |||
| Day 6: | <0.05 | ||
| – Mean ± SD | 5.83 ± 0.77 | 5.00 ± 0.60 | |
| – Median (range) | 1 (0, 1) | 1 (0, 1) | |
| Day 11: | 0.980 | ||
| – Mean ± SD | 6.32 ± 0.42 | 5.69 ± 0.39 | |
| – Median (range) | 1 (0, 1) | 1 (0, 1) | |
| Posture changes (curled-up legs, clenched fists) | |||
| Day 6: | <0.05 | ||
| – Mean ± SD | 6.00 ± 0.73 | 5.13 ± 0.45 | |
| – Median (range) | 1 (0, 1) | 1 (0, 1) | |
| Day 11: | 0.012 | ||
| – Mean ± SD | 6.48 ± 0.94 | 5.78 ± 0.85 | |
| – Median (range) | 1 (0, 1) | 1 (0, 1) | |
Data presented are mean ± SD scores for a 7-point Likert scale where 1 = very much worse, 2 = much worse, 3 = somewhat worse, 4 = same condition, 5 = somewhat better, 6 = much better, 7 = very much better. A higher mean score indicates a greater improvement.
SD: Standard deviation.
Infantile colic is a common reason for parents seeking medical advice for young infants.
The cause of infantile colic is not known, but possible factors include disturbed gut microbiota and/or transient lactose intolerance.
Probiotics and lactase are used as treatments.
APT198K (xyloglucan plus heat-killed Lactobacillus reuteri SGL01 and Bifidobacterium brevis SGB01) decreases intestinal meteorism, which may be associated with colic.
APT198K was more effective than a lactase dietary supplement for the treatment of infantile colic, and was well tolerated.
APT198K may provide a treatment option for infantile colic.
Authors’ contributions
All authors have contributed significantly to conception, design and execution of the study. All authors have participated in drafting, reviewing, and/or revising the manuscript and have approved its submission.
Financial & competing interests disclosure
Y Vandenplas has participated as a clinical investigator, and/or advisory board member, and/or consultant, and/or speaker for Abbott Nutrition, Aspen, Biogaia, Biocodex, Danone, Hero, Nestle Nutrition Institute, Nutricia, Mead Johnson Nutrition, Merck, Orafti, Phacobel, Rontis, Sari Husada, United Pharmaceuticals, Wyeth and Yakult. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors thank Content Ed Net for providing editorial assistance in the preparation of this article, with funding from Noventure SL, Barcelona, Spain.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Vandenplas Y, Abkari A, Bellaiche M et al. Prevalence and health outcomes of functional gastrointestinal symptoms in infants from birth to 12 months of age. J. Pediatr. Gastroenterol. Nutr. 61(5), 531–537 (2015).
• Provides an estimation of the worldwide prevalence of infantile colic.
2.
Bellaiche M, Levy M, Jung C. Treatments for infant colic. J. Pediatr. Gastroenterol. Nutr. 57(Suppl. 1), S27–S30 (2013).
3.
Benninga MA, Nurko S, Faure C et al. Childhood functional gastrointestinal disorders: neonate/toddler. Gastroenterology 150, 1443–1455 (2016).
4.
Roberts DM, Ostapchuk M, O'Brien JG. Infantile colic. Am. Fam. Physician 70(4), 735–740 (2004).
5.
Savino F, Ceratto S, De Marco A, di Montezemolo LC. Looking for new treatments of infantile colic. Ital. J. Pediatr. 40, 53 (2014).
• Overview of treatment options for infantile colic.
6.
Harb T, Matsuyama M, David M, Hill R. Infant colic – what works: a systematic review of interventions for breastfed infants. J. Pediatr. Gastroenterol. Nutr. 62(5), 668–686 (2016).
7.
Caffarelli C, Santamaria F, Cesari S et al. Advances in pediatrics in 2014: current practices and challenges in allergy, gastroenterology, infectious diseases, neonatology, nutrition, oncology and respiratory tract illnesses. Ital. J. Pediatr. 41, 84 (2015).
8.
Pärtty A, Kalliomäki M, Endo A, Salminen S, Isolauri E. Compositional development of Bifidobacterium and Lactobacillus microbiota is linked with crying and fussing in early infancy. PLoS ONE 7(3), e32495 (2012).
9.
Savino F, Cordisco L, Tarasco V, Calabrese R, Palumeri E, Matteuzzi D. Molecular identification of coliform bacteria from colicky breastfed infants. Acta Paediatr. 98(10), 1582–1588 (2009).
10.
Xu M, Wang J, Wang N, Sun F, Wang L, Liu XH. The efficacy and safety of the probiotic bacterium Lactobacillus reuteri DSM 17938 for infantile colic: a meta-analysis of randomized controlled trials. PLoS ONE 10(10), e0141445 (2015).
• Meta-analysis of the effect of one strain of Lactobacillus reuteri in the treatment of infantile colic.
11.
Kataria J, Li N, Wynn JL, Neu J. Probiotic microbes: do they need to be alive to be beneficial? Nutr. Rev. 67(9), 546–550 (2009).
12.
Adams CA. The probiotic paradox: live and dead cells are biological response modifiers. Nutr. Res. Rev. 23(1), 37–46 (2010).
• Review of the biological responses seen with probiotics containing dead cells.
13.
Kanabar D, Randhawa M, Clayton P. Improvement of symptoms in infant colic following reduction of lactose load with lactase. J. Hum. Nutr. Diet 14(5), 359–363 (2001).
• One of the larger studies of lactase treatment for infantile colic, showing that a subset of patients responded well.
14.
Miller JJ, McVeagh P, Fleet GH, Petocz P, Brand JC. Breath hydrogen excretion in infants with colic. Arch. Dis. Child. 64(5), 725–729 (1989).
15.
Wessel MA, Cobb JC, Jackson EB, Harris GS, Detwiler AC. Paroxysmal fussing in infancy, sometimes called colic. Pediatrics 14(5), 421–435 (1954).
16.
Cohen-Silver J, Ratnapalan S. Management of infantile colic: a review. Clin. Pediatr. (Phila.) 48(1), 14–17 (2009).
17.
Radesky JS, Zuckerman B, Silverstein M et al. Inconsolable infant crying and maternal postpartum depressive symptoms. Pediatrics 131(6), e1857–e1864 (2013).
18.
Abacı FB, Gökçe S, Tuygun N, Karacan CD, Őner Ő. Psychosocial status and quality of life in mothers of infants with colic. Turk. J. Pediatr. 55(4), 391–395 (2013).
19.
Critch J. Infantile colic: is there a role for dietary interventions? Paediatr. Child Health 16(1), 47–49 (2011).
20.
de Weerth C, Fuentes S, Puylaert P, de Vos WM. Intestinal microbiota of infants with colic: development and specific signatures. Pediatrics 131(2), e550–e558 (2013).
21.
Savino F, Bailo E, Oggero R et al. Bacterial counts of intestinal Lactobacillus species in infants with colic. Pediatr. Allergy Immunol. 16(1), 72–75 (2005).
22.
Rhoads JM, Fatheree NY, Norori J et al. Altered fecal microflora and increased fecal calprotectin in infants with colic. J. Pediatr. 155(6), 823–828.e1 (2009).
23.
Lehtonen L, Korvenranta H, Eerola E. Intestinal microflora in colicky and noncolicky infants: bacterial cultures and gas-liquid chromatography. J. Pediatr. Gastroenterol. Nutr. 19(3), 310–314 (1994).
24.
Simone M, Gozzoli C, Quartieri A et al. The probiotic Bifidobacterium breve B632 inhibited the growth of Enterobacteriaceae within colicky infant microbiota cultures. Biomed. Res. Int. 2014, 301053 (2014).
25.
Savino F, Cordisco L, Tarasco V et al. Antagonistic effect of Lactobacillus strains against gas-producing coliforms isolated from colicky infants. BMC Microbiol. 11, 157 (2011).
26.
Chau K, Lau E, Greenberg S et al. Probiotics for infantile colic: a randomized, double-blind, placebo-controlled trial investigating Lactobacillus reuteri DSM 17938. J. Pediatr. 166(1), 74–78 (2015).
27.
Sung V, Hiscock H, Tang ML et al. Treating infant colic with the probiotic Lactobacillus reuteri: double blind, placebo controlled randomised trial. BMJ 348, g2107 (2014).
28.
Bueno L, Theodorou V, Sekkal S. Xyloglucan: a new agent to protect the intestinal mucosa and to prevent bacterially-mediated alteration of tight junction permeability [Abstract P1675]. Presented at: United European Gastroenterology Week. Vienna, Austria, 18–22 October 2014.
29.
Gnessi L, Bacarea V, Marusteri M, Picqué N. Xyloglucan for the treatment of acute diarrhea: results of a randomized, controlled, open-label, parallel group, multicentre, national clinical trial. BMC Gastroenterol. 15(1), 153 (2015).
30.
Ståhlberg MR, Savilahti E. Infantile colic and feeding. Arch. Dis. Child. 61(12), 1232–1233 (1986).
31.
Miller JJ, McVeagh P, Fleet GH, Petocz P, Brand JC. Effect of yeast lactase enzyme on “colic” in infants fed human milk. J. Pediatr. 117(2 Pt 1), 261–263 (1990).
32.
Kearney PJ, Malone AJ, Hayes T, Cole M, Hyland M. A trial of lactase in the management of infant colic. J. Hum. Nutr. Dietet. 11(4), 281–285 (1998).
33.
National Institute for Health and Care Excellence (NICE). Clinical knowledge summaries: colic – infantile (November 2014). http://cks.nice.org.uk/colic-infantile.
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 24 January 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Efficacy and safety of APT198K for the treatment of infantile colic: a pilot study. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0059
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hanne Delcourt, Liesbet Verbrugghe, Yvan Vandenplas, Koen Huysentruyt, Systematic review and meta-analysis of randomized controlled trials on pre-, pro-, post- and synbiotic supplementation in follow-on formula, Clinical Nutrition, 10.1016/j.clnu.2025.05.022, 51, (101-114), (2025).
- Gayatri Athalye-Jape, Meera Esvaran, Sanjay Patole, Elizabeth A Nathan, Dorota A Doherty, Edric Sim, Lakshmi Chandrasekaran, Chooi Kok, Stephan Schuster, Patricia Conway, Effects of a live versus heat-inactivated probiotic Bifidobacterium spp in preterm infants: a randomised clinical trial , Archives of Disease in Childhood - Fetal and Neonatal Edition, 10.1136/archdischild-2023-326667, 110, 2, (177-184), (2024).
- Sáskia Ribeiro Vaz, Marise Helena Tofoli, Melissa Ameloti Gomes Avelino, Paulo Sérgio Sucasas da Costa, Probiotics for infantile colic: Is there evidence beyond doubt? A meta‐analysis and systematic review, Acta Paediatrica, 10.1111/apa.17036, 113, 2, (170-182), (2023).
- Ali Salehi, Parvaneh Naserzadeh, Parastoo Tarighi, Elham Afjeh-Dana, Masoud Akhshik, Amir Jafari, Pooyan Mackvandi, Behnaz Ashtari, Masoud Mozafari, Fabrication of a microfluidic device for probiotic drug's dosage screening: Precision Medicine for Breast Cancer Treatment, Translational Oncology, 10.1016/j.tranon.2023.101674, 34, (101674), (2023).
- XueBing HAN, XiangNan YUAN, Jun FANG, HongMei JIANG, Gang LIU, Role of lactic acid bacteria in maintaining animal intestinal health, SCIENTIA SINICA Vitae, 10.1360/SSV-2022-0032, 53, 4, (464-479), (2023).
- Zihan Yu, Jihua Chen, Yaxin Liu, Qingguo Meng, Hang Liu, Qinyan Yao, Wenxuan Song, Xiangfeng Ren, Xin Chen, The role of potential probiotic strains Lactobacillus reuteri in various intestinal diseases: New roles for an old player, Frontiers in Microbiology, 10.3389/fmicb.2023.1095555, 14, (2023).
- J. Esquena-Moret, A Review of Xyloglucan: Self-Aggregation, Hydrogel Formation, Mucoadhesion and Uses in Medical Devices, Macromol, 10.3390/macromol2040037, 2, 4, (562-590), (2022).
- Manish Narang, Dheeraj Shah, Oral lactase for infantile colic: a randomized double-blind placebo-controlled trial, BMC Pediatrics, 10.1186/s12887-022-03531-8, 22, 1, (2022).
- Ralf Jäger, Alex E. Mohr, Katie C. Carpenter, Chad M. Kerksick, Martin Purpura, Adel Moussa, Jeremy R. Townsend, Manfred Lamprecht, Nicholas P. West, Katherine Black, Michael Gleeson, David B. Pyne, Shawn D. Wells, Shawn M. Arent, Abbie E. Smith-Ryan, Richard B. Kreider, Bill I. Campbell, Laurent Bannock, Jonathan Scheiman, Craig J. Wissent, Marco Pane, Douglas S. Kalman, Jamie N. Pugh, Jessica A. ter Haar, Jose Antonio, International Society of Sports Nutrition Position Stand: Probiotics, Journal of the International Society of Sports Nutrition, 10.1186/s12970-019-0329-0, 16, 1, (2022).
- YoHan Nam, Seokmin Yoon, Jihye Baek, Jong-Hwa Kim, Miri Park, KwangWoo Hwang, Wonyong Kim, Heat-Killed Lactiplantibacillus plantarum LRCC5314 Mitigates the Effects of Stress-Related Type 2 Diabetes in Mice via Gut Microbiome Modulation , Journal of Microbiology and Biotechnology, 10.4014/jmb.2111.11008, 32, 3, (324-332), (2022).