Do disparities between populations in randomized controlled trials and the real world lead to differences in outcomes?
Abstract
Aim: To conduct a systematic review investigating reasons for the disparity between the efficacy and effectiveness rates reported in randomized controlled trials (RCTs) and observational studies of direct-acting antiviral treatment regimens licensed for use in genotype1 hepatitis C virus-infected individuals. Methods: This systematic review was conducted in accordance with the criteria of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses group. Results: Statistically significant (p < 0.05) differences in the baseline demographics and sustained virological response rates were observed between RCT and observational studies. Conclusion: In order for outcomes from RCTs to be generalizable to the real world, greater consideration needs to be taken to include patient populations that are more representative of those awaiting treatment in the clinical setting.
First draft submitted: 16 June 2016; Accepted for publication: 1 September 2016; Published online: 17 November 2016
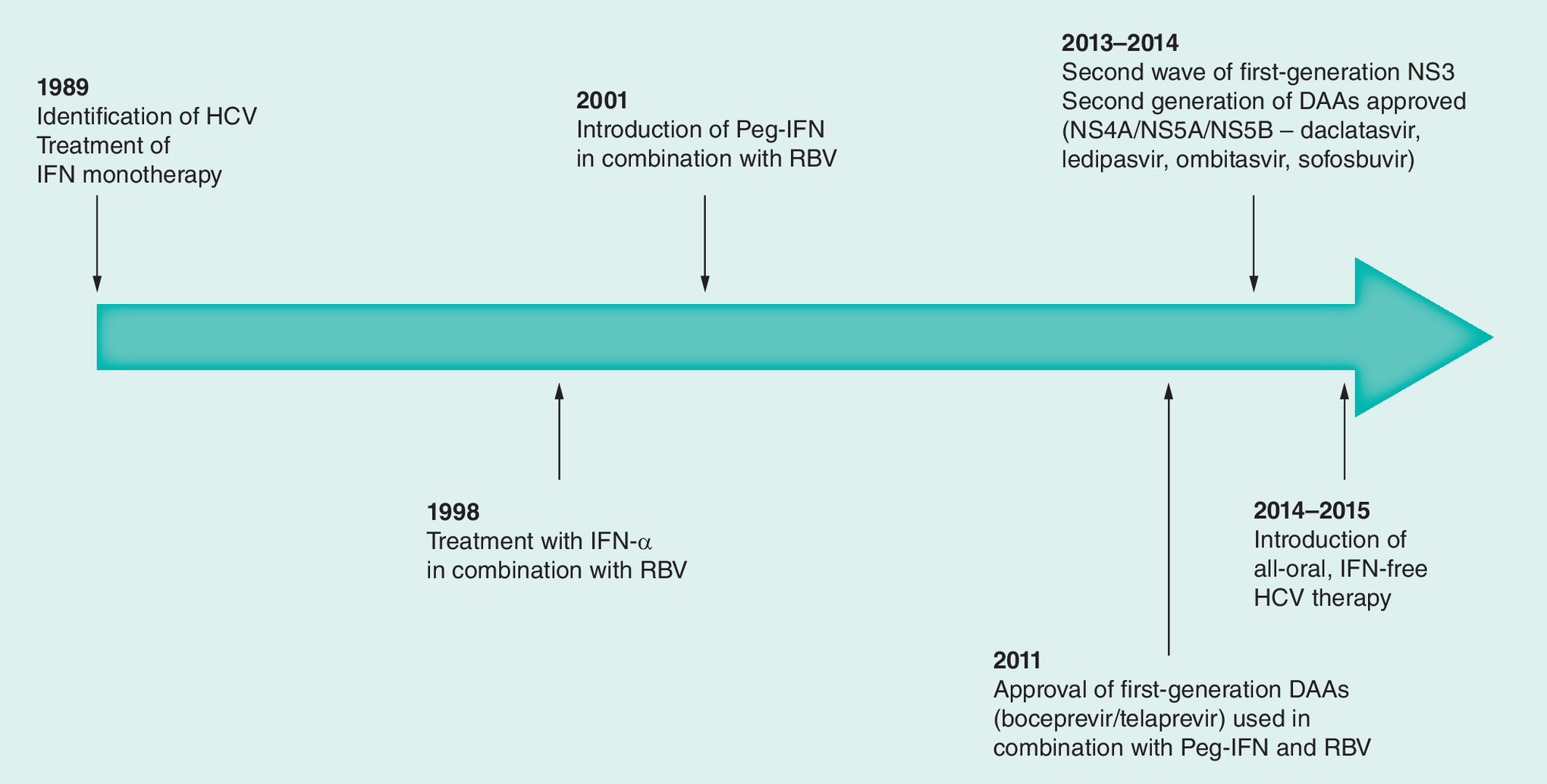
Figure 1. Hepatitis C treatment timeline: treatment has progressed from interferon monotherapy in 1989 to all-oral interferon-free dual directly acting antiviral combinations in 2014/2015.
DAA: Directly acting antiviral; HCV: Hepatitis C virus; IFN: Interferon; RBV: Ribavirin.
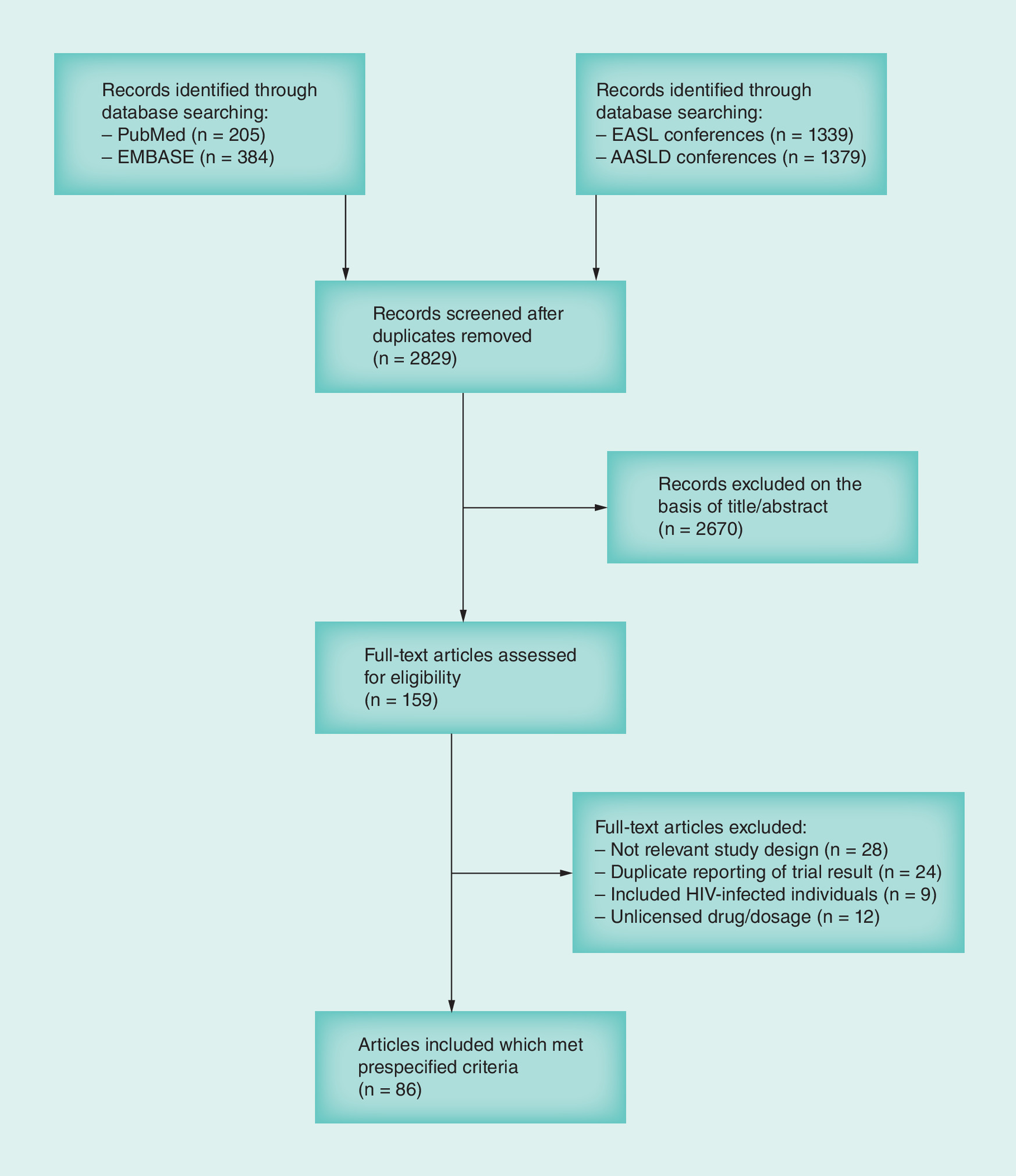
Figure 2. PRISMA flow diagram of the literature seach of randomized controlled trials and observational studies of licensed regimens for the treatment of hepatitis C virus genotype 1.
AASLD: American association for the Study of Liver Diseases; EASL: European Association for the Study of the Liver.
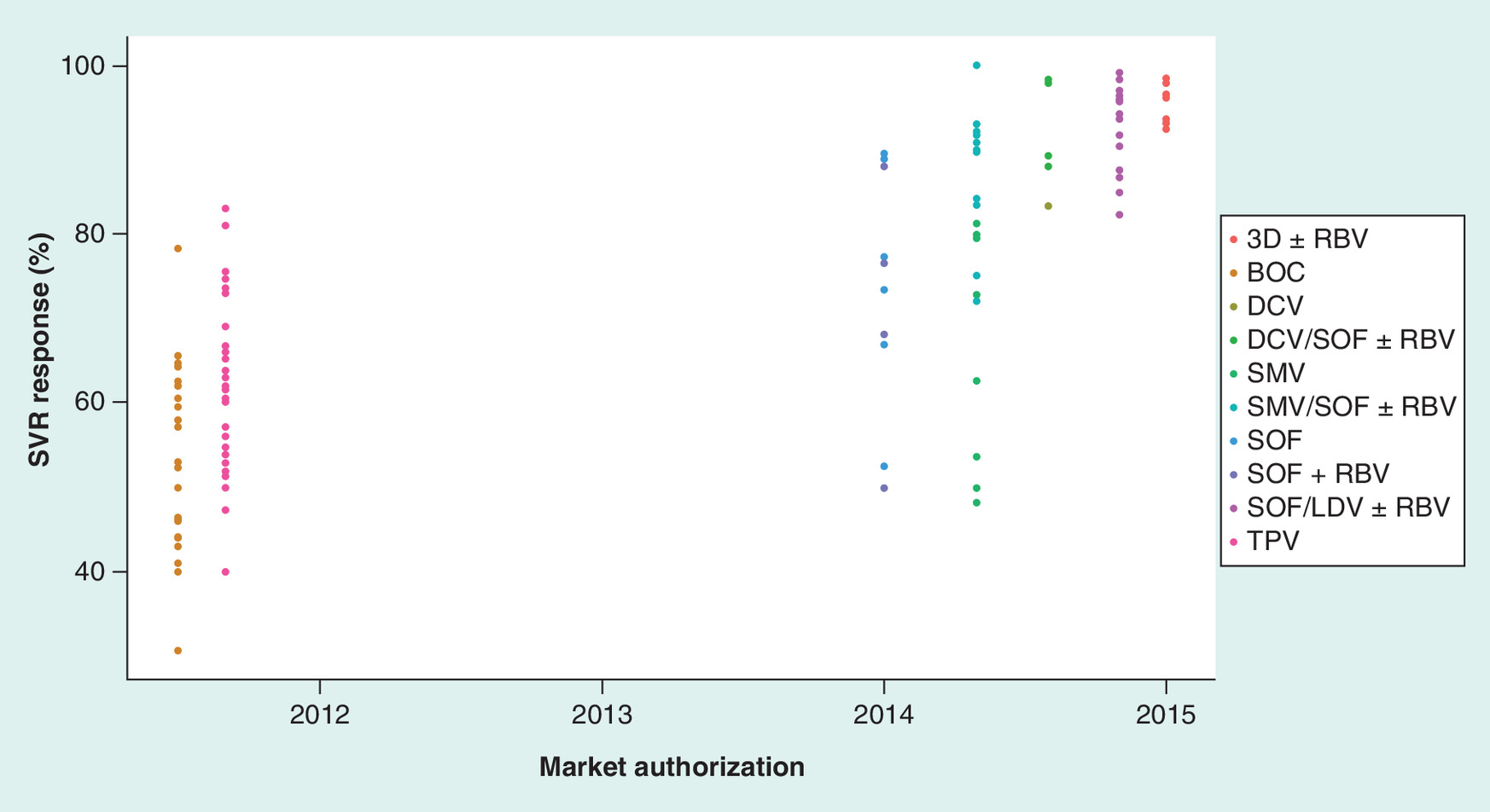
Figure 3. Plot of the pooled sustained virological response rates against the date of EMA marketing authorization.
3D ± RBV: Paritaprevir boosted with ritonavir, ombitasvir and dasabuvir with or without ribavirin; BOC/PR: Boceprevir in combination with pegylated interferon and ribavirin; DCV/PR: Daclatasvir in combination with pegylated interferon and ribavirin; SMV/PR: Simeprevir in combination with pegylated interferon and ribavirin; SMV/SOF ± RBV: Simeprevir combined with sofosbuvir with, or without ribavirin; SOF/PR: Sofosbuvir in combination with pegylated interferon and ribavirin; SOF + RBV: Sofosbuvir in combination with ribavirin; SVR: Sustained virological response; TPV/PR: Telaprevir in combination with pegylated interferon and ribavirin.
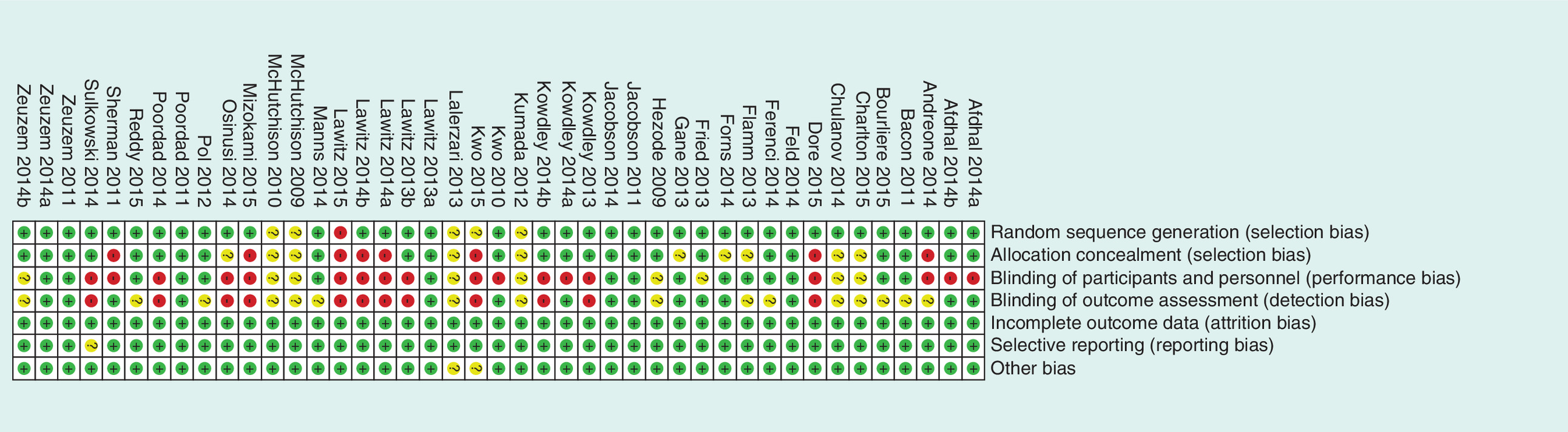
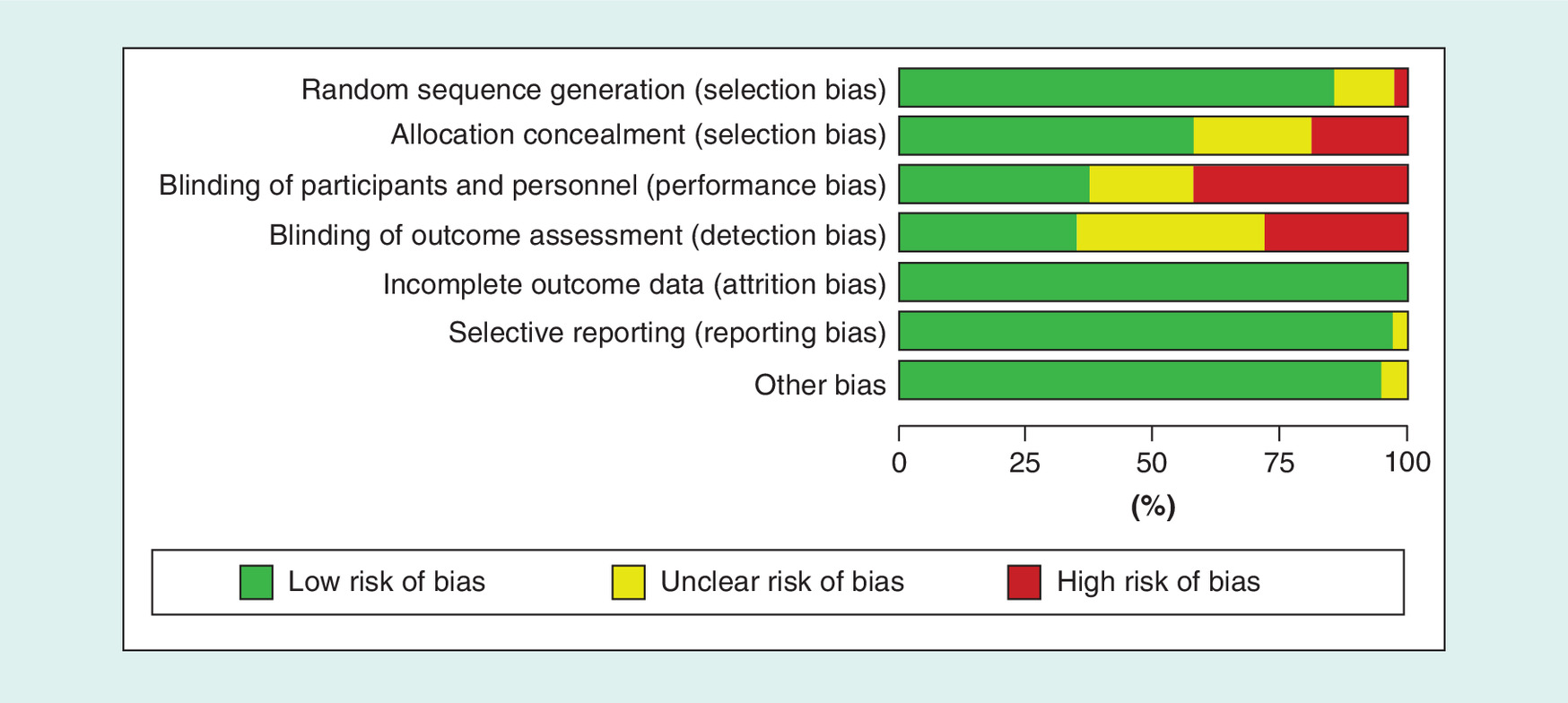
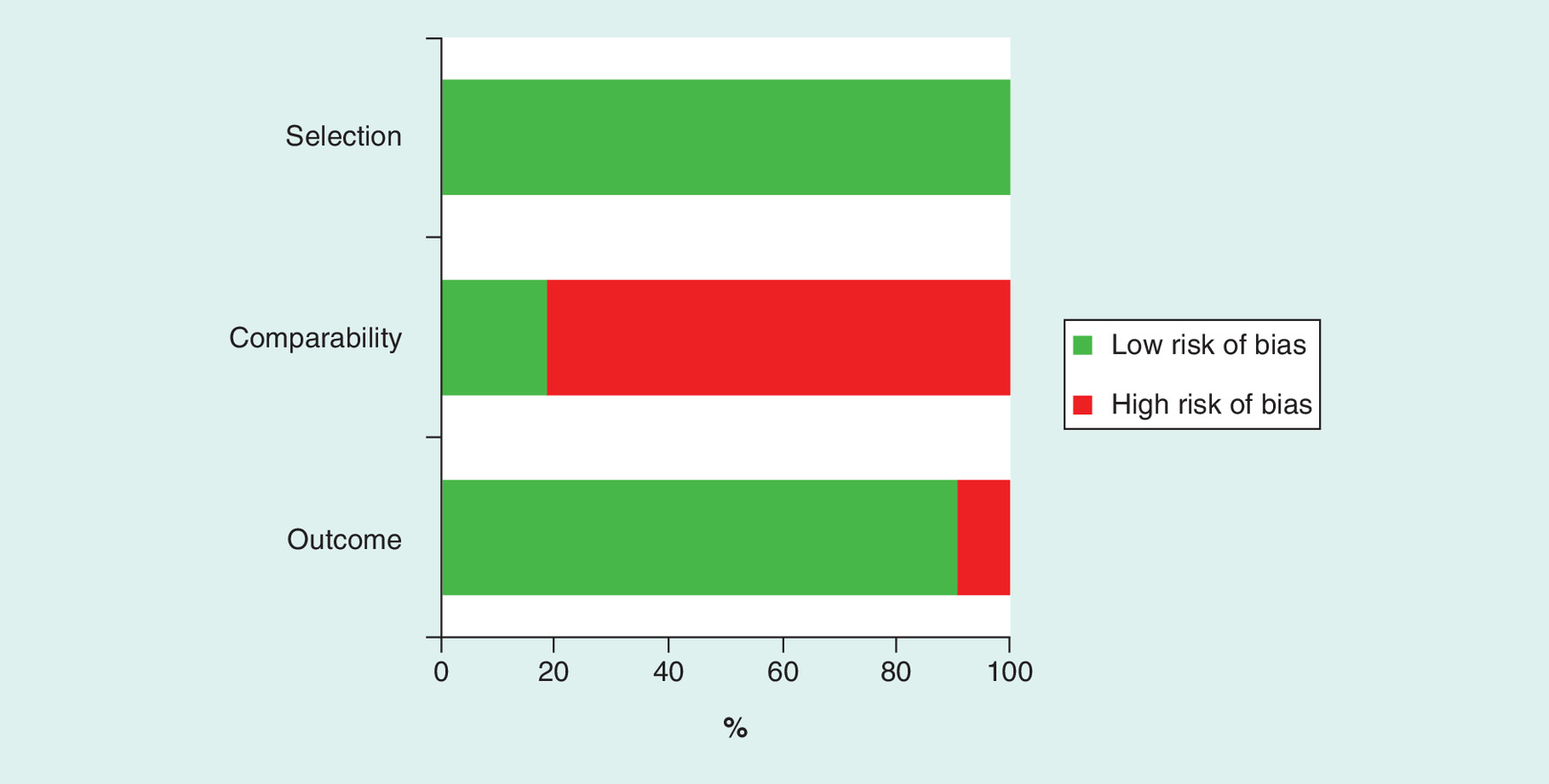
Figure 6. Risk of bias by domain in 43 observational cohort studies using the Newcastle Ottawa Scale.
The green bar represents the percentage of studies with a low risk of bias over the number of studies assessed.
Infection with the hepatitis C virus (HCV) is a major public health problem and a leading cause of chronic liver disease [1]. The WHO estimates that more than 185 million people are infected worldwide, a prevalence of approximately 3%, with geographical variations of between 0.5 and 4% [2,3]. Chronic hepatitis C is the most common global cause of cirrhosis and the most common indication for liver transplantation [4]. Complications of cirrhosis include hepatic decompensation, variceal bleeding and the development of hepatocellular carcinoma [5,6]. There are six major HCV genotypes (GT) [7]. GT1 is the most prevalent in HCV-infected individuals globally, accounting for 46% of all infections and in Ireland (55%) [8,9].
Recent years have seen a significant improvement in the treatment of HCV infection with the advent of directly acting antiviral (DAA) therapy and a move toward potent interferon-free regimens, with sustained virological response (SVR) rates above 90% [10]. Treatment has progressed from interferon-based monotherapy with SVR rates ranging from 10 to 20% [11], to protease inhibitors (PI) in combination with pegylated-interferon and ribavirin (PR) regimens providing rates of 70–85% [12–16]. Since 2014, a number of pangenotypic agents, NS3/4A, NS5A and NS5B oral inhibitors became available with SVR rates reported in clinical trials in the range of 75–99% (Figure 1) [15,17–28].
The breakthrough therapy designation (BTD), was established in 2012, after the PI regimens had been approved, by the US Congress to expedite the development of drugs that show promising early clinical evidence of benefit over available therapies [29,30]. Sofosbuvir (SOF), sofosbuvir with daclatasvir (SOF/DCV), sofosbuvir with ledipasvir (SOF/LDV) and paritaprevir, ombitasvir and ritonavir combined with dasabuvir (3D) were all designated as breakthrough therapies [31]. The clinical trial programs supporting product licensing for interferon-free regimens involved both comparative and noncomparative clinical trials. Evidence of efficacy in subpopulations of patients with HCV infection (GT, presence of cirrhosis, among others) was limited by small patient numbers and strict inclusion criteria, thus, limiting generalization to the real world clinical setting.
When designed appropriately, clinical trials report treatment ‘efficacy’, a measure of the capacity of a treatment to produce the desired effect in a controlled environment [32–34]. Treatment outcomes in routine clinical practice may be modified by concomitant comorbid medical conditions, substance abuse, poor adherence and loss to follow-up, resulting in potentially lower effectiveness rates than those obtained in clinical trials. It is important to evaluate how trial efficacy translates to real-world effectiveness [35]. Observational comparative effectiveness studies allow estimates of treatment effectiveness to be determined [32].
Following the availability of the breakthrough treatment regimens for HCV infection, a number of collaborative research networks were formed to conduct comparative effectiveness observational studies for patients treated under their care [36–38]. These studies are designed to determine real world effectiveness and to compare results with the clinical trial data.
Having searched PROSPERO [39], an international database of prospectively registered systematic reviews where there is a health-related outcome, we aimed to conduct a systematic review of the published literature to compare the outcomes reported in randomized controlled trials (RCTs) and observational studies of DAA treatment regimens licensed for use in GT1 HCV-infected individuals and to investigate possible reasons for the disparity between efficacy and effectiveness. The review was limited to treatment combinations for GT1 HCV for two reasons. First, GT1 is the most prevalent GT in HCV-infected individuals globally, accounting for 46% of all infections and in Ireland (55%) [8,9]. Second, in both the American Association for the Study of Liver Diseases and European Association for the Study of the Liver, GT1 individuals have the widest array of treatment options available [40,41].
Methods
This systematic review was conducted in accordance with the criteria of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses group [42].
Search strategy
Using a predefined search strategy, along with prespecified inclusion criteria incorporating the PICOS (Population, Intervention, Comparator, Outcome and Study design) structure for formulating a research protocol [43], an electronic literature search in PubMed, EMBASE and The Cochrane Database of Systematic Reviews was systematically performed on 6 May 2015, for comparative and noncomparative clinical trials and 9 July 2015, for observational studies (Table 1). Both searches were repeated on 24 November 2015. The search included all studies published up to 24 November 2015 (two abstracts identified during this period that met all inclusion criteria were subsequently published as full-text articles in early 2016 and thus, are referenced as such). Details of the search strategy can be found in the Supplementary Material. In order to reduce the effect of publication bias, a hand-search of conference abstracts, for both clinical trials and observational studies, from the American Association for the Study of Liver Diseases and European Association for the Study of the Liver conferences between 2010 and 2015 was performed. The bibliographies of identified articles were also hand searched for potentially relevant articles.
Eligibility criteria
RCTs, noncomparative clinical trials and observational or ‘real-world’ studies were included if the patient population consisted of HCV GT1-infected individuals (over 18 years of age) treated with one of the EMA approved treatment combinations. Inclusion and exclusion criteria are outlined in Table 1. Criteria specified that SVR12, or SVR24, must have been included as a primary or secondary end point. Dose-finding studies, studies presenting information exclusively about acute or non-GT1 HCV and studies that included HIV co-infected patients were excluded.
Screening & selection
The screening and selection process is outlined in Figure 2 and was undertaken by two reviewers (E Gray and A O’Leary). Search results from the electronic databases were transferred into the EndNote© referencing system. Due to the overlap in coverage of the electronic databases, there were a large number of duplicate citations that were excluded at this point. Initial screening of the title and abstract (if necessary) was conducted to exclude articles deemed not relevant. Articles that matched the inclusion criteria or those where the abstract did not provide sufficient information to include, or exclude, were selected for full-text review. These articles were then reviewed further for their relevance against the inclusion criteria by reading them in full-text. Papers that met the eligibility criteria were included in this study.
Data extraction
The authors used a specifically designed data collection tool to extract patient and study characteristics from included studies. If data were unavailable in published material, supplemental appendices were examined. If further data were required, additional information was sought by directly contacting corresponding authors. Data were extracted on the number of patients in each trial arm, the experimental and comparator regimens and relevant baseline demographics and clinical characteristics of patients including gender, GT1 subtype, presence of cirrhosis and previous treatment history. In addition, baseline viral characteristics such as viral load and GT subtype were also extracted. The primary outcome measure was SVR, calculated on an ‘intent-to-treat’ basis with all patients starting treatment contributing to the denominator.
Risk of bias for RCTs
The quality of included clinical trials was individually assessed by two reviewers (E Gray and A O’Leary) using the ‘Risk of Bias’ tool in the Cochrane Collaboration software Review Manager (RevMan) Version 5.3 (The Cochrane Collaboration, Copenhagen, Denmark) [44]. Each study was assessed for bias by the author under the following domains:
Random sequence generation (selection bias);
Allocation concealment bias (selection bias);
Blinding of participants and personnel (performance bias);
Blinding of outcome assessment (detection bias);
Incomplete outcome data (attrition bias);
Selective reporting bias (reporting bias);
Other bias (this included consideration of study authors conflicts on interests or whether they were a recipient of funding from the trial sponsor).
Risk of bias for observational studies
Of the available tools to assess methodological quality in nonrandomized observational studies, the Newcastle-Ottawa Scale (NOS) was selected based on recommendation by the Cochrane Collaboration 35, 36 [44,45]. The NOS scale is restricted to assessment of nine items, categorized into three dimensions including selection, comparability and outcome [46]. For each item, a series of response options are provided. A star system allows a semi-quantitative assessment of study quality, such that the highest quality studies are awarded a maximum of one star for each item with the exception of items related to comparability that confers the assignment of two stars. The total number of stars that can be achieved in a study is 9, indicating a complete absence of bias. NOS scores are categorized into three groups: very high risk of bias (0–3 NOS stars), high risk of bias (4–6 stars) and low risk of bias (7–9 stars) [47].
Statistical analysis
For each treatment regimen, the clinical trial and observational study data were pooled and tabulated in terms of gender and key HCV characteristics. The SVR rates from all studies matching the inclusion criteria were recorded. Descriptive statistics were used to describe the HCV characteristics and SVR rates for the study population. Categorical variables were reported as frequencies and percentages. Univariate analyses were performed using the Chi-square test as appropriate. A linear mixed effects model using variance to account for study size as well as adjusting for risk of bias was fitted to determine a difference in effect size due to design. A p < 0.05 was considered to be statistically significant. A sensitivity analysis was performed whereby both clinical trials and observational studies considered to be at high risk of bias were removed and the analysis subsequently repeated to determine the impact, if any, of including studies considered at high risk of bias. The analysis was performed using SPSS Version 21® (IBM Corp., NY, USA).
Results
3307 records were identified from PubMed, EMBASE and conference proceedings. After excluding duplicates, the title and abstract (where necessary) of 2829 studies were reviewed, resulting in the identification of 159 studies for further assessment. These consisted of both full-text articles and abstracts from conference proceedings. Following the application of eligibility criteria, 86 studies, which reported the efficacy or effectiveness of ten different treatment regimens, were selected for inclusion (Figure 2). Ten treatment regimens identified for the treatment of GT1 HCV infection. Five interferon-based regimens were included:
Telaprevir in combination with pegylated interferon and ribavirin (TPV/PR);
Boceprevir in combination with pegylated interferon and ribavirin (BOC/PR);
Simeprevir in combination with pegylated interferon and ribavirin (SMV/PR);
Sofosbuvir in combination with pegylated interferon and ribavirin (SOF/PR);
Daclatasvir in combination with pegylated interferon and ribavirin (DCV/PR).
Five interferon-free regimens were included:
Sofosbuvir in combination with ribavirin (SOF + RBV);
Simeprevir combined with sofosbuvir with, or without ribavirin (SMV/SOF ± RBV);
Paritaprevir boosted with ritonavir, ombitasvir and dasabuvir with or without ribavirin (3D ± RBV);
Sofosbuvir combined with ledipasvir with, or without ribavirin (SOF/LDV RBV);
Sofosbuvir combined with daclatasvir with, or without ribavirin (SOF/DCV ± RBV).
Among the 86 studies, 43 were clinical trials [22–23,25–28,48–84], both randomized and noncomparative studies and the remaining 43 studies were observational cohort studies [36,85–126]. Characteristics of the eligible studies are presented in the Supplementary Tables 1 & 2. The studies included a total of 40,796 patients of whom 71% were male, 55% were GT1a, 41% had previous treatment experience and cirrhosis was present in 32%. The profiles of the included studies are outlined in Table 2.
In the 20 RCTs that included a comparator group, PR was the comparator of choice in 17 of the remaining three, the comparators were TPV/PR (n = 2) and SOF + RBV (n = 1).
Overall, a large population of patients, treated with interferon-based regimens (TPV/PR, BOC/PR, SMV/PR, DCV/PR and SOF/PR), were included in both clinical trials and observational studies. However, there were exceptions; a limited number of observational studies reported the outcomes for patients treated with SMV/PR and one RCT reported outcomes for patients (n = 12) treated with DCV/PR. This treatment regimen was never reported in an observational study (Table 3).
For the five interferon-free regimens (SOF ± RBV, SMV/SOF ± RBV, 3D ± RBV, SOF/DCV ± RBV and SOF/LDV ± RBV), despite the introduction of the BTD, a substantial number of patients were included in RCTs for 3D ± RBV (n = 2598) and SOF/LDV ± RBV (n = 2106). However, for the remaining three regimens, the number of patients included in RCTs was significantly less (SMV/SOF ± RBV (n = 580), SOF + RBV (n = 97) and SOF/DCV ± RBV (n = 152) (Table 3).
Baseline characteristics: a comparison
Four baseline variables were compared between the RCTs and the observational studies: male gender, previous treatment experience, presence of cirrhosis and proportion of GT1a patients. The pooled baseline demographics and HCV characteristics for clinical trials and observational studies stratified according to treatment regimen are presented in Table 3. An analysis was undertaken to evaluate for disparity between RCT and observational study populations. For interferon-based regimens, both RCTs and observational studies were undertaken in four of the five treatment regimens (TPV/PR, BOC/PR, SMV/PR and SOF/PR). A statistically significant difference was observed in the proportion of males and individuals with previous treatment experience, with observational studies comprising of a higher proportion of both than in RCTs (p < 0.005). Similarly, in TPV/PR, BOC/PR and SOF/PR studies, there was a higher proportion of patients with cirrhosis in observational studies compared with RCTs (p ≤ 0.0001). The proportion of patients with GT1a varied for all regimens. With a limited number of patients in the SMV/PR observational studies (n = 32), it is difficult to make comparisons with the RCTs for the regimen.
In the interferon-free regimens SMV/SOF ± RBV and SOF/LDV ± RBV, a statistically significant difference was observed in the proportion of males and individuals with cirrhosis, with observational studies comprising of a higher proportion of both than in RCTs (p < 0.0001). There was a statistically significant difference in the proportion of patients with cirrhosis between the 3D ± RBV RCTs and the observational studies also. In contrast with interferon-based regimens, the proportion of patients with previous treatment experience was lower in the observational studies with statistically significant differences observed in the SMV/SOF ± RBV and SOF/LDV ± RBV regimens (p < 0.0001). The proportion of patients with GT1a varied for all three regimens.
In general, significant differences in the patient populations included in RCTs and observational studies were identified. Observational studies tended to include a higher proportion of males and a higher proportion of patients with cirrhosis. In interferon-based regimens, the proportion of patients with previous treatment experience tended to be higher in observational studies but this tended to be lower in observational studies reporting outcomes in interferon-free regimens.
Efficacy versus effectiveness: a comparison
The SVR rates for both RCTs and observational studies, following pooling, are presented in Table 4.
Interferon-based regimens
Prior to pooling, the efficacy rates in reported for first-generation PI (TPV/PR and BOC/PR) ranged from 51 to 83% [49–51,54,66,79–84]. The effectiveness rates were more varied and ranged between 31 and 81% [86–87,90–93,96–97,101–107,109–111,113–114,118–119,122,124,126]. Following pooling, the SVR rate in TPV/PR RCTs was 71% compared with 60% in the observational studies (p < 0.0001) with an absolute difference of 11%. In BOC/PR studies, the SVR rate in clinical trials was 64 and 52% in observational studies (p < 0.0001) with an absolute difference of 12%.
In second-generation PI (SMV/PR, DCV/PR and SOF/PR), the range of efficacy rates prior to pooling were slightly higher than the first generation PIs – between 50 and 89% [52,62,67,69–72,75–76,78]. The range of effectiveness rates was similar – between 48 and 80% [36,85,88,102,107,115]. No observational studies for DCV/PR were identified in the systematic review. Following pooling, the SVR rate in SMV/PR RCTs was 65 compared with 53% in the observational studies (p < 0.171). This represented an absolute difference of 12%. In SOF/PR studies, the pooled SVR rates were 89 and 69% in the clinical trials and observational studies, respectively (p < 0.0001), an absolute difference of 20%.
Interferon-free regimens
For SOF+RBV, a DAA in combination with RBV, the SVR rates in RCTs ranged from 50 to 77% [61,74,77] prior to pooling and the effectiveness also rates ranged from 50 to 77% [61,77] in observational studies. The pooled efficacy rate was 64% and with an effectiveness rate of 63%.
In the DAA dual combinations with or without ribavirin (SMV/SOF ± RBV, 3D ± RBV, SOF/DCV ± RBV and SOF/LDV ± RBV), the efficacy rates and effectiveness rates were higher than those observed for the interferon-based regimens. In RCTs, the efficacy rates ranged from 84 to 99% across the 19 studies [22–23,25–28,48,53,55–60,63–65,68,73] and effectiveness rates ranged from 72 to 100% across the 20 studies [36,85,88,94–95,98–100,102,108,112,115–117,120–121,123,125,127]. Following pooling, the SVR rate in SMV/SOF + RBV RCTs was 89% compared with 80% in the observational studies (p < 0.0001). This represented an absolute difference of 9%. In 3D ± RBV studies, the pooled SVR rates were 96 and 95% in the clinical trials and observational studies, respectively (p < 0.0001), representing an absolute difference of 1%. For SOF/DCV ± RBV and SOF/LDV ± RBV RCTs, the pooled SVR rates were 98 and 97%, respectively compared with 93% (p = 0.26) and 94% (p < 0.0001) for the observational studies. Correspondingly, these represented absolute differences of 5 and 3%.
Plotting the pooled SVR rate of each regimen against the date EMA marketing authorization date demonstrated the improvement in SVR rate over time, particularly with the introduction of the interferon-free regimens (Figure 3).
Quality assessment
Clinical trials
The risk of bias graph and risk of bias summary assessing the quality of the 43 clinical trials are presented in Figures 4 & 5. Following the assessment of quality, a high risk of bias was considered to be present in 2, 16, 42 and 28% in the domains of random sequence generation, allocation concealment, blinding of participants and personnel and blinding of outcome assessment, respectively. The remaining domains, incomplete outcome data, selective reporting and other bias, were considered to be at low risk of bias.
Observational studies
The quality of observational studies using the NOS is presented in Figure 6. The mean NOS score of the 43 included studies was 6, with a range from 5 to 8. Six studies had a rating of 8 stars, two studies had a rating of 7 stars, 24 had a rating of 6 stars and 11 had a 5 star rating. Risk of bias was greatest in the comparability domain with 81% considered at high risk of bias for confounding. Eight studies were awarded 2 stars indicating that these studies were adjusted for potential confounding factors. The remainder of the studies failed to score any stars for this domain. This is consistent with potential confounding by indication. Studies that did not undertake appropriate statistical analysis such as multivariate logistic regression or propensity scoring were at risk of confounding by indication. The risk of bias at the outcome level for 43 observational studies is summarized in Supplementary Table 3.
Adjusting for the risk of bias
Fitting a linear mixed effects model, in which the four demographic variables (gender, GT1, treatment experience and presence of cirrhosis), the study design and treatment, was regressed against SVR rate, yields a statistically significant design effect (p < 0.05). This concludes that there is evidence to suggest that a significantly higher effect is observed in clinical trials compared with observational studies.
Sensitivity analysis
In order to investigate the possible impact of bias on outcomes, all studies, both clinical trials and observational studies, identified as being associated with a ‘high risk of bias’ and with significant uncertainty around their risk of bias (Kumada 2012, Lalezari et al. 2013, McHutchison et al. 2009 and McHutchison 2010) were excluded and the outcome analysis was repeated. Pooled SVR rates are presented in the Supplementary Table 4. Following the exclusion of clinical trials and observational studies associated with a high risk and unclear levels of bias, no clinical trials remained reporting SVR rates for that for SMV/PR, DCV/PR, SMV/SOF ± RBV and SOF/DCV ± RBV. Similarly, when observational studies associated with a high risk of bias (NOS score ≤6) were excluded, no observational studies remained that reported SVR rates for SOF/PR, SOF + RBV and SOF/DCV ± RBV.
Analysis of the pooled SVR rates after excluding studies at high risk or unclear levels of bias resulted in some changes to the SVR rates. In the clinical trials, the SVR rates fell by 0.2–4% for all regimens, with the exception of SOF + RBV, which increased by 12%. The greatest reduction in SVR rate (-4.4%) occurred in the pooled analysis of SOF/LDV ± RBV clinical studies. In the observational studies, pooled SVR rates for TPV/PR, BOC/PR and SMV/PR fell by 2.8, 0.2 and 5%, respectively. There was no change in the SVR rate for 3D ± RBV studies while the pooled SVR rate for SOF/LDV ± RBV and SMV/SOF ± RBV increased by 0.2 and 4.6%, respectively, when high-risk studies were excluded.
Discussion
This study demonstrated the variation in outcomes that can be observed between clinical trials and observational comparative effectiveness studies. Ten DAA-based therapeutic combinations available for the treatment of GT1 HCV-infected patients were identified. The improvement in SVR rates that came with advances in the development of therapies that targeted more specific and distinct sites in the HCV replication process is clear from the data extracted in this review for both RCTs and real-world data. In addition, the most effective regimens for the treatment of HCV GT1 infection are the interferon-free, DAA dual combinations of SMV/SOF ± RBV, 3D ± RBV, SOF/DCV ± RBV and SOF/LDV ± RBV.
Further investigation into the variation in SVR rates highlighted the disparity in baseline demographics and HCV characteristics of the populations included in RCTs as compared with those included in observational studies. Statistically significant differences were found between the RCT and observational study populations. In the studies that included interferon-based regimens, the observational studies had a consistently greater proportion of males, but more significantly, a greater proportion of patients with previous treatment experience and cirrhosis. Similarly, in the studies of interferon-free regimens, the observational studies commonly included higher proportion of patients with cirrhosis but the proportion of patients with previous treatment experience was frequently lower in the observational studies.
The absolute difference in pooled SVR rates between RCTs and observational studies was significant for some regimens. It is possible that the disparity in population demographics may account for the differences between the efficacy and effectiveness rates observed. Analysis of the demographic data from RCTs that studied the efficacy of interferon-based regimens showed favorable SVR rates in patients who were treatment naive, noncirrhotic and were not co-infected with HIV. However, in the real world setting, the patients become increasingly diverse. With a greater proportion of patients considered ‘difficult-to-treat’, the effectiveness rate in the real-world clinical setting was 11–20% lower than those observed in RCTs. A lack of specific subpopulation data (i.e., SVR rates in patients with cirrhosis or those with previous treatment experience) prevented the direct comparisons of efficacy and effectiveness rates between these patient subgroups. Therefore, it is difficult to determine the true differences in SVR rates in patients with cirrhosis (particularly with advanced cirrhosis) between RCT and observational studies. However, we can hypothesize that the higher proportion of patients with cirrhosis in the observational studies may have contributed to the lower rates of effectiveness.
In the interferon-free, DAA dual combination (SMV/SOF ± RBV, 3D ± RBV, SOF/DCV ± RBV and SOF/LDV ± RBV) regimens, the gap between efficacy and effectiveness rates narrowed and in some cases, rates were almost identical, in particular for the 3D ± RBV regimen. Nonetheless, disparities in the baseline characteristics between the populations were still apparent. Patient with cirrhosis continued to be under-represented in RCTs but these dual combinations have demonstrated similarly high efficacy rates in both patients with, and without, cirrhosis.
The quality assessment tools, Cochrane’s risk of bias and the NOS allowed us to assess if the quality of the studies had an impact on the outcomes obtained. Our sensitivity analysis in which we re-analyzed the data following the exclusion of studies considered at high risk of bias (and those with significant uncertainty around the risk of bias), indicated that SVR rates did not differ substantially when studies considered at low risk of bias were analyzed alone, with the exception of one regimen SOF+RBV, where the exclusion of one study by Lalezari et al. resulted in a +12% difference in the SVR rates [61]. Additionally, after adjusting for the risk of bias, we concluded that there was statistically significant evidence of a residual difference in the SVR rates due to the study design (RCT vs observational studies). Therefore, there continues to be a requirement to utilize methods to address confounding in observational studies, such as multivariate logistic regression and propensity scoring. While observational studies may be more reflective of the real world populations, it is important that the studies are well-designed and conducted to allow the production of the highest quality of evidence. It is now more imperative than ever that decision-makers consider the evidence from observational studies, in addition to the RCT evidence and the quality of this evidence, to inform or revise policies and decisions about coverage and reimbursement of high cost treatments.
Given that the goal of the BTD program is to identify promising drug candidates early in the clinical development timeline, expedite the development and review process via intensive guidance from the US FDA and the EMA and provide patients access to approved therapies as quickly as possible, noncomparative data are often considered sufficient for providing evidence of early clinical benefit [128]. These clinical trials include limited numbers of carefully selected patients. Thus, it is not uncommon for selected patient subgroups, such as those with decompensated cirrhosis, renal failure, other comorbidities to be excluded from these studies [129]. These are often the most complex and difficult-to-treat patients in clinical practice, and marketing authorization can be granted without any evidence from these subgroups. Therefore, this study demonstrates the importance of including a patient population in RCTs that closely mimics the patient population in real world clinical practice with particular emphasis on the inclusion of ‘difficult-to-treat’ patients. This allows for meaningful determinations to be made about probable effectiveness rates in clinical practice.
From the perspective of the regulator (such as the FDA and EMA), observational studies can play an important role in the post-marketing surveillance and generation of evidence for these difficult-to-treat patient groups. If the inclusion of such patients in RCTs was not possible, the requirement for thorough, and early, post-marketing surveillance, would enable the effectiveness of the regimen to be established at an early stage following authorization.
There were several limitations to this study. It is possible that the systematic review was subject to publication bias. Publication bias occurs when studies of statistically significant or clinically favorable results are more likely to be published than studies with nonsignificant or unfavorable results. While all resources and search strategies were used to ensure all relevant studies were included, it is possible that trial sponsors failed to make results of unfavorable trials available and thus, the potential for publication bias must be considered. Additionally, pooling data from studies with heterogeneous design requires awareness of the potential to introduce bias. Pooling, as undertaken above, is the simplest and most naively intuitive way of summarizing the information from several clinical trials. However, this approach does not consider the validity of the comparisons, assumes all trial designs are the same and therefore, is often subject to bias [130].
Conclusion & future perspective
Recent therapeutic advances are transforming the hepatitis C landscape and there is now an unprecedented prospect of cure for this chronic viral infection, with the possibility of global eradication of the disease (subject to fiscal restraints). While demonstrating the superiority of DAA dual combination interferon-free treatment combinations above those that contain the PR backbone, this study highlights the need for clinical trials to include a patient population that is more representative of those encountered in the clinical setting.
This study provides evidence that the populations included in clinical trials tend not to reflect the population treated in the clinical setting and as a result, the efficacy rates often differ from the effectiveness rates reported in the real world. Clinical trials commonly exclude difficult-to-treat patients, those with the most severe presentation of a disease (e.g., decompensated cirrhosis) and/or those with co-morbid conditions (e.g., HIV-co-infection or renal insufficiency). While appropriate eligibility criteria are essential for the internal validity of the RCTs, it often results in the selection of an ‘ideal’ patient population most likely to demonstrate the efficacy and safety outcomes required to ensure regulatory approval.
Historically, RCT evidence has been considered the gold standard in the hierarchy of evidence for evaluating the efficacy and safety of interventions. The BTD aims to fast-track the approval of marketing authorizations for promising drugs, potentially relying exclusively on well-controlled, nonrandomized studies as appropriate evidence of efficacy for regulators. Thus, not only does the clinical trial population poorly reflect the clinical setting but we also consider whether the BTD compromises the scientific strength of the clinical trial evidence at the top of the evidence hierarchy. Without the requirement for randomization, blinding and concealment, the design of these studies and thus, the quality of evidence, for BTD designated treatments do not differ significantly from the design of observational studies. Licensing of treatments for HCV infection in recent years is a testament to this phenomenon whereby many agents and treatment regimens were licensed based on noncomparative, single-arm studies driven by the desire to bring treatments to the market as quickly as possible. This has also occurred in a number of other therapeutic areas. Therefore, as observational studies may be more reflective of the real-world populations and the quality of the evidence may not differ significantly from that of some clinical trials, it is now more important than ever that decision-makers consider the evidence from observational studies accrued prospectively in the post-HTA era, in addition to the RCT evidence and the quality of this evidence, to inform or revise policies and decisions about coverage and reimbursement.
Additionally, in instances where it is unethical or impossible to include a patient population representative of clinical practice in the RCTs, a regulatory requirement for observational studies may assist in the generation of further evidence for these patient groups and to allow for continued monitoring and analysis of outcomes, identifying adverse events or unwanted outcomes that did not appear during the drug approval process.
| Criteria | Details | Comments |
|---|---|---|
| Inclusion criteria | ||
| Patient population | HCV genotype 1 patients >18 years | |
| Intervention(s) | Telaprevir, boceprevir, bimeprevir, sofosbuvir, ledipasvir, daclatasvir, paritaprevir, ombitasvir, dasabuvir | Includes any licensed combinations of these drugs |
| Comparison therapy | Any comparator or non-comparative studies | |
| Patient outcomes | SVR12, SVR24 | |
| Study types | Phase II or Phase III randomized controlled trials, observational/real-world studies | Includes open-label, single-arm and single agent studies |
| Publication type | Full-text journal articles, conference abstracts reporting SVR outcomes | |
| Limits | Humans | |
| Exclusion criteria | ||
| Patient population | Non-genotype 1 patients, <18 years, HIV co-infection, HBV co-infection, patients post-orthotopic liver transplant | |
| Intervention(s) | Unlicensed drugs/drug combinations | |
| Comparison therapy | No limits | |
| Patient outcomes | Not reporting SVR | |
| Study types | Not Phase II or III, observational/real-world studies | |
| Publication types | Comments, editorials, letters | |
HBV: Hepatitis B; HCV: Hepatitis C; SVR: Sustained virological response.
| Study profile | Randomized controlled trials (n = 43) | Observational studies n = 43 |
|---|---|---|
| No comparator group | 23 | 20 |
| Cirrhotic patients (exclusively) | 5 | 4 |
| Non-cirrhotic patients (exclusively) | 16 | 1 |
| Treatment-naive patients (exclusively) | 11 | 8 |
| Treatment-experienced patients (exclusively) | 21 | 3 |
| Treatment regimen | Study type | Studies included (n) | n | Male (%) | p-value | GT1a (%) | p-value | Treatment experienced (%) | p-value | Presence of cirrhosis (%) | p-value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| TPV/PR | Clinical trials | 7 | 1813 | 63.8 | 0.00012* | 53.7 | <0.0001* | 35.6 | <0.0001* | 12.2 | <0.0001* |
| Observational studies | 19 | 7309 | 86.8 | 56.8 | 74.6 | 46.5 | |||||
| BOC/PR | Clinical trials | 4 | 1397 | 62 | <0.0001* | 60.8 | <0.0001* | 32.7 | <0.0001* | 8.3 | <0.0001* |
| Observational studies | 23 | 7916 | 89.7 | 52.5 | 48.6 | 33.5 | |||||
| SMV/PR | Clinical trials | 6 | 1515 | 61.5 | 0.004* | 45 | 0.889 | 55.3 | <0.0001* | 23.3 | 0.063 |
| Observational studies | 2 | 32 | 89.5 | 44.8 | 18.7 | 9.4 | |||||
| DCV/PR | Clinical trials | 1 | 12 | 58.3 | – | 75 | – | 0 | – | 0 | – |
| Observational studies | – | – | – | – | – | – | |||||
| SOF/PR | Clinical trials | 3 | 500 | 61.2 | <0.0001* | 77 | <0.0001* | 0 | <0.0001* | 58.4 | <0.0001* |
| Observational studies | 4 | 1717 | 87.6 | 62.7 | 39.2 | 35.6 | |||||
| SOF + RBV | Clinical trials | 3 | 97 | 76 | – | 79 | 0.203 | 0 | – | 49 | 0.222 |
| Observational studies | 2 | 72 | N/A | 79 | 0 | 82 | |||||
| SMV/SOF ± RBV | Clinical trials | 3 | 580 | 64.1 | <0.0001* | 77.2 | <0.0001* | 46.9 | <0.0001* | 24.8 | <0.0001* |
| Observational studies | 8 | 3571 | 80.9 | 58.4 | 38.1 | 61.8 | |||||
| 3D + RBV | Clinical trials | 7 | 2598 | 57.3 | 0.936 | 49.3 | 0.013* | 32.6 | 0.28 | 14.6 | 0.0004* |
| Observational studies | 2 | 102 | 56.8 | 32.8 | 27.5 | 60.8 | |||||
| SOF/DCV ± RBV | Clinical trials | 1 | 152 | 54 | – | 80 | <0.0001* | 27 | – | 0 | – |
| Observational studies | 3 | 243 | N/A | 46 | N/A | N/A | |||||
| SOF/LDV ± RBV | Clinical trials | 8 | 2106 | 57.7 | <0.0001* | 64.5 | <0.0001* | 33.6 | <0.0001* | 22.2 | <0.0001* |
| Observational studies | 9 | 5976 | 71.6 | 69.1 | 19.7 | 39.7 |
*Statistically significant.
3D ± RBV: Paritaprevir boosted with ritonavir, ombitasvir and dasabuvir with or without ribavirin; BOC/PR: Boceprevir in combination with pegylated interferon and ribavirin; DCV/PR: Daclatasvir in combination with pegylated interferon and ribavirin; N/A: Not applicable; SMV/PR: Simeprevir in combination with pegylated interferon and ribavirin; SMV/SOF ± RBV: Simeprevir combined with sofosbuvir with, or without ribavirin; SOF/PR: Sofosbuvir in combination with pegylated interferon and ribavirin; SOF + RBV: Sofosbuvir in combination with ribavirin; TPV/PR: Telaprevir in combination with pegylated interferon and ribavirin.
| Treatment regimen | Study type | n | SVR12/24(%) | p-value |
|---|---|---|---|---|
| TPV/PR | Clinical trials | 1813 | 71 | <0.0001* |
| Observational studies | 7309 | 60 | ||
| BOC/PR | Clinical trials | 1397 | 64 | <0.0001* |
| Observational studies | 7916 | 52 | ||
| SMV/PR | Clinical trials | 1515 | 65 | 0.171 |
| Observational studies | 32 | 53 | ||
| DCV/PR | Clinical trials | 12 | 83 | – |
| Observational studies | – | – | ||
| SOF/PR | Clinical trials | 500 | 89 | <0.0001* |
| Observational studies | 1717 | 69 | ||
| SOF + RBV | Clinical trials | 97 | 64 | 0.85 |
| Observational studies | 72 | 63 | ||
| SMV/SOF + RBV | Clinical trials | 580 | 89 | <0.0001* |
| Observational studies | 3571 | 80 | ||
| 3D+RBV | Clinical trials | 2598 | 96 | 0.638 |
| Observational studies | 102 | 95 | ||
| SOF/DCV ± RBV | Clinical trials | 152 | 98 | 0.026 |
| Observational studies | 243 | 93 | ||
| SOF/LDV ± RBV | Clinical trials | 2106 | 97 | <0.0001* |
| Observational studies | 5976 | 94 |
*Statistically significant.
3D ± RBV: Paritaprevir boosted with ritonavir, ombitasvir and dasabuvir with or without ribavirin; BOC/PR: Boceprevir in combination with pegylated interferon and ribavirin; DCV/PR: Daclatasvir in combination with pegylated interferon and ribavirin; SMV/PR: Simeprevir in combination with pegylated interferon and ribavirin; SMV/SOF ± RBV: Simeprevir combined with sofosbuvir with, or without ribavirin; SOF/PR: Sofosbuvir in combination with pegylated interferon and ribavirin; SOF + RBV: Sofosbuvir in combination with ribavirin; TPV/PR: Telaprevir in combination with pegylated interferon and ribavirin.
Disparities between outcomes reported in randomized controlled trials & observational studies
Statistically significant (p < 0.05) differences in the baseline demographics and sustained virological response rates were observed between randomized controlled trial and observational studies.
The breakthrough therapy designation (BTD) aims to fast-track the approval of marketing authorizations for promising drugs, potentially relying exclusively on well-controlled, nonrandomized studies as appropriate evidence of efficacy for regulators. Without the requirement for randomization, blinding and concealment, the design of these studies for BTD designated treatments do not differ significantly from the design of observational studies. The BTD may be compromising the scientific strength of the clinical trial evidence at the top of the evidence hierarchy.
Evolution of the hepatitis C treatment landscape
Directly acting antiviral dual combination interferon-free treatment regimens demonstrated superior sustained virological response rates to those regimens that contain the pegylated-interferon and ribavirin backbone.
Value of observational studies
Observational studies can play an important role in the generation of further evidence for difficult-to-treat patient groups where it is unethical for them to be included in randomized controlled trials. Additionally, they allow for continued monitoring and analysis of outcomes, identifying adverse events or unwanted outcomes that did not appear during the drug approval process.
Financial & competing interests’ disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_material.doc)
- Download
- 336.50 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Ghany MG, Strader DB, Thomas DL, Seeff LB. Diagnosis, management, and treatment of hepatitis C: an update. Hepatology 49(4), 1335–1374 (2009).
2.
Pol S, Vallet-Pichard A, Corouge M, Mallet VO. Hepatitis C: epidemiology, diagnosis, natural history and therapy. Contrib. Nephrol. 176, 1–9 (2012).
3.
Vietri J, Prajapati G, El Khoury AC. The burden of Hepatitis C in Europe from the patients’ perspective: a survey in 5 countries. BMC Gastroenterol. 13, 16 (2013).
4.
Chen SL, Morgan TR. The natural history of hepatitis C virus (HCV) infection. Int. J. Med. Sci. 3(2), 47–52 (2006).
5.
Massard J, Ratziu V, Thabut D et al. Natural history and predictors of disease severity in chronic hepatitis C. J. Hepatol. 44(1 Suppl.), S19–S24 (2006).
6.
Maasoumy B, Wedemeyer H. Natural history of acute and chronic hepatitis C. Best Pract. Res. Clin. Gastroenterol. 26(4), 401–412 (2012).
7.
Lee MH, Yang HI, Yuan Y, L’italien G, Chen CJ. Epidemiology and natural history of hepatitis C virus infection. World J. Gastroenterol. 20(28), 9270–9280 (2014).
8.
Thornton L, Murphy N, Jones L et al. Determination of the burden of hepatitis C virus infection in Ireland. Epidemiol. Infect. 140(8), 1461–1468 (2012).
9.
Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J. Hepatol. 61(1 Suppl.), S45–S57 (2014).
10.
Martinello M, Dore GJ. Editorial commentary: interferon-free hepatitis C treatment efficacy from clinical trials will translate to “Real World” outcomes. Clin. Infect. Dis. 62(7), 927–928 (2016).
11.
Hayashi N, Takehara T. Antiviral therapy for chronic hepatitis C: past, present, and future. J. Gastroenterol. 41(1), 17–27 (2006).
12.
Liang TJ, Ghany MG. Current and future therapies for hepatitis C virus infection. N. Engl. J. Med. 368(20), 1907–1917 (2013).
13.
Trembling PM, Tanwar S, Dusheiko GM. Boceprevir: an oral protease inhibitor for the treatment of chronic HCV infection. Expert Rev. Anti Infect. Ther. 10(3), 269–279 (2012).
14.
Chang MH, Gordon LA, Fung HB. Boceprevir: a protease inhibitor for the treatment of hepatitis C. Clin. Ther. 34(10), 2021–2038 (2012).
15.
Park C, Jiang S, Lawson KA. Efficacy and safety of telaprevir and boceprevir in patients with hepatitis C genotype 1: a meta-analysis. J. Clin. Pharm. Ther. 39(1), 14–24 (2014).
16.
Wendt A, Bourliere M. An update on the treatment of genotype-1 chronic hepatitis C infection: lessons from recent clinical trials. Ther. Adv. Infect. Dis. 1(6), 191–208 (2013).
17.
Zeuzem S, Berg T, Gane E et al. Simeprevir increases rate of sustained virologic response among treatment-experienced patients with HCV genotype-1 infection: a Phase IIb trial. Gastroenterology 146(2), 430.e436–e441. (2014).
18.
Pawlotsky JM. New hepatitis C therapies: the toolbox, strategies, and challenges. Gastroenterology 146(5), 1176–1192 (2014).
19.
Gentile I, Borgia F, Coppola N, Buonomo AR, Castaldo G, Borgia G. Daclatasvir: the first of a new class of drugs targeted against hepatitis C virus NS5A. Curr. Med. Chem. 21(12), 1391–1404 (2014).
20.
Flisiak R, Jaroszewicz J, Parfieniuk-Kowerda A. Emerging treatments for hepatitis C. Expert Opin. Emerg. Drugs 18(4), 461–475 (2013).
21.
Degasperi E, Aghemo A. Sofosbuvir for the treatment of chronic hepatitis C: between current evidence and future perspectives. Hepat. Med. 6, 25–33 (2014).
22.
Afdhal N, Zeuzem S, Kwo P et al. Ledipasvir and sofosbuvir for untreated HCV genotype 1 infection. N. Engl. J. Med. 370(20), 1889–1898 (2014).
23.
Afdhal N, Reddy KR, Nelson DR et al. Ledipasvir and sofosbuvir for previously treated HCV genotype 1 infection. N. Engl. J. Med. 370(16), 1483–1493 (2014).
24.
Kowdley KV, Gordon SC, Reddy KR et al. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N. Engl. J. Med. 370(20), 1879–1888 (2014).
25.
Feld JJ, Kowdley KV, Coakley E et al. Treatment of HCV with ABT-450/r-ombitasvir and dasabuvir with ribavirin. N. Engl. J. Med. 370(17), 1594–1603 (2014).
26.
Zeuzem S, Jacobson IM, Baykal T et al. Retreatment of HCV with ABT-450/r-ombitasvir and dasabuvir with ribavirin. N. Engl. J. Med. 370(17), 1604–1614 (2014).
27.
Poordad F, Hezode C, Trinh R et al. ABT-450/r-ombitasvir and dasabuvir with ribavirin for hepatitis C with cirrhosis. N. Engl. J. Med. 370(21), 1973–1982 (2014).
28.
Ferenci P, Bernstein D, Lalezari J et al. ABT-450/r-ombitasvir and dasabuvir with or without ribavirin for HCV. N. Engl. J. Med. 370(21), 1983–1992 (2014).
29.
Shea M, Ostermann L, Hohman R et al. Regulatory watch: impact of breakthrough therapy designation on cancer drug development. Nat. Rev. Drug Discov. 15(3), 152 (2016).
• Rationale for establishing the breakthrough therapy designation.
30.
Chizkov RR, Million RP. Trends in breakthrough therapy designation. Nat. Rev. Drug Discov. 14(9), 597–598 (2015).
31.
Graul AI, Cruces E, Stringer M. The year’s new drugs & biologics, 2014: part I. Drugs. Today (Barc). 51(1), 37–87 (2015).
• Hepatitis C virus drugs listed under the breakthrough therapy designation.
32.
Schumock GT, Pickard AS. Comparative effectiveness research: relevance and applications to pharmacy. Am. J. Health Syst. Pharm. 66(14), 1278–1286 (2009).
•• Review of comparative effectiveness research and its relevance and importance to decision-makers.
33.
Schwartz D, Lellouch J. Explanatory and pragmatic attitudes in therapeutical trials. J. Clin. Epidemiol. 62(5), 499–505 (2009).
• Insightful paper discussing how the design can inflence the outcomes reported in clinical trials.
34.
Loudon K, Treweek S, Sullivan F, Donnan P, Thorpe KE, Zwarenstein M. The PRECIS-2 tool: designing trials that are fit for purpose. BMJ 350, h2147 (2015).
35.
Mathes T, Antoine SL, Pieper D. Factors influencing adherence in hepatitis-C infected patients: a systematic review. BMC Infect. Dis. 14, 203 (2014).
36.
Dieterich DT, Bacon B, Flamm SL et al. Final evaluation of 955 HCV patients treated with 12 week regimens containing sofosbuvir +/− simeprevir in the trio network: academic and community treatment of a real-world, heterogeneous population. Gastroenterology 148(4), S1001 (2015).
37.
Gordon SC, Muir AJ, Lim JK et al. Safety profile of boceprevir and telaprevir in chronic hepatitis C: Real world experience from HCV-TARGET. J. Hepatol. 62(2), 286–293 (2015).
38.
Gray E, O’leary A, Walsh C, Bergin CJ, Norris S. Outcomes from the Irish national hepatitis C prospective treatment registry. Hepatology 60, A689–A690 (2014).
39.
NHS. PROSPERO International Prospective Register of Systematic Reviews. 2016. www.crd.york.ac.uk/PROSPERO/
40.
Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology 62(3), 932–954 (2015).
41.
EASL recommendations on treatment of Hepatitis C 2015. J. Hepatol. 63(1), 199–236 (2015).
42.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int. J. Surg. 8(5), 336–341 (2010).
•• PRISMA guidelines for appropriate reporting of systematic reviews.
43.
Aslam S, Emmanuel P. Formulating a researchable question: a critical step for facilitating good clinical research. Indian J. Sex Transm. Dis. 31(1), 47 (2010).
44.
Higgins J, Green S. The Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration, London, UK (2011).
•• Justifies the use of the Newcastle Ottawa Scale for assessing the quality of observational studies.
45.
Wells G, Shea B, O’Connell D et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. (2016). www.ohri.ca/programs/clinical_epidemiology/oxford.asp
46.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 25(9), 603–605 (2010).
47.
Lo CK-L, Mertz D, Loeb M. Newcastle-Ottawa Scale: comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 14(1), 1–5 (2014).
48.
Andreone P, Colombo MG, Enejosa JV et al. ABT-450, ritonavir, ombitasvir, and dasabuvir achieves 97% and 100% sustained virologic response with or without ribavirin in treatment-experienced patients with HCV genotype 1b infection. Gastroenterology 147(2), e359–e365 (2014).
49.
Bacon BR, Gordon SC, Lawitz E et al. Boceprevir for previously treated chronic HCV genotype 1 infection. N. Engl. J. Med. 364(13), 1207–1217 (2011).
50.
Poordad F, Mccone J Jr., Bacon BR et al. Boceprevir for untreated chronic HCV genotype 1 infection. N. Engl. J. Med. 364(13), 1195–1206 (2011).
51.
Flamm SL, Lawitz E, Jacobson I et al. Boceprevir with peginterferon alfa-2a-ribavirin is effective for previously treated chronic hepatitis C genotype 1 infection. Clin. Gastroenterol. Hepatol. 11(1), 81–87 (2013).
52.
Pol S, Ghalib RH, Rustgi VK et al. Daclatasvir for previously untreated chronic hepatitis C genotype-1 infection: a randomised, parallel-group, double-blind, placebo-controlled, dose-finding, Phase 2a trial. Lancet Infect. Dis. 12(9), 671–677 (2012).
53.
Sulkowski MS, Gardiner DF, Rodriguez-Torres M et al. Daclatasvir plus sofosbuvir for previously treated or untreated chronic HCV infection. N. Engl. J. Med. 370(3), 211–221 (2014).
54.
Kwo PY, Lawitz EJ, Mccone J et al. Efficacy of boceprevir, an NS3 protease inhibitor, in combination with peginterferon alfa-2b and ribavirin in treatment-naive patients with genotype 1 hepatitis C infection (SPRINT-1): an open-label, randomised, multicentre Phase 2 trial. Lancet 376(9742), 705–716 (2010).
55.
Gane EJ, Stedman CA, Hyland RH et al. Efficacy of nucleotide polymerase inhibitor sofosbuvir plus the NS5A inhibitor ledipasvir or the NS5B non-nucleoside inhibitor GS-9669 against HCV genotype 1 infection. Gastroenterology 146(3), e736–e743. (2014).
56.
Mizokami M, Yokosuka O, Takehara T et al. Ledipasvir and sofosbuvir fixed-dose combination with and without ribavirin for 12 weeks in treatment-naive and previously treated Japanese patients with genotype 1 hepatitis C: an open-label, randomised, Phase 3 trial. Lancet Infect. Dis. 15(6), 645–653 (2015).
57.
Kowdley KV, Gordon SC, Reddy KR et al. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N. Engl. J. Med. 370(20), 1879–1888 (2014).
58.
Charlton M, Everson GT, Flamm SL et al. Ledipasvir and Sofosbuvir Plus Ribavirin for treatment of HCV infection in patients with advanced liver disease. Gastroenterology 149(3), 649–659 (2015).
59.
Bourliere M, Bronowicki JP, De Ledinghen V et al. Ledipasvir-sofosbuvir with or without ribavirin to treat patients with HCV genotype 1 infection and cirrhosis non-responsive to previous protease-inhibitor therapy: a randomised, double-blind, Phase 2 trial (SIRIUS). Lancet Infect. Dis. 15(4), 397–404 (2015).
60.
Dore GJ, Knysz B, Luo Y et al. MALACHITE-II: Phase 3B trial of ombitasvir/paritaprevir/r and dasabuvir + ribavirin or telaprevir + peginterferon/ribavirin in peginterferon/ribavirin treatment-experienced adults with HCV genotype 1. J. Hepatol. 62(S1), S656 (2015).
61.
Lalezari J, Nelson D, Hyland RH et al. Once daily sofosbuvir plus ribavirin for 12 weeks and 24 weeks in treatment-naive patients with HCV infection: the Quantum Study. J. Hepatol. 58(S1), S346 (2013).
62.
Fried MW, Buti M, Dore GJ et al. Once-daily simeprevir (TMC435) with pegylated interferon and ribavirin in treatment-naive genotype 1 hepatitis C: the randomized PILLAR study. Hepatology 58(6), 1918–1929 (2013).
63.
Kowdley KV, Lawitz E, Poordad F et al. Phase 2b trial of interferon-free therapy for hepatitis C virus genotype 1. N. Engl. J. Med. 370(3), 222–232 (2014).
64.
Lawitz E, Matusow G, Dejesus E et al. A Phase 3, open-label, single-arm study to evaluate the efficacy and safety of 12 weeks of simeprevir (SMV) plus sofosbuvir (SOF) in treatment-naive or -experienced pateints with chronic HCV genotype 1 infection and cirrhosis: OPTIMIST-2. J. Hepatol. 62(S1), S264 (2015).
65.
Kwo P, Gitlin N, Nahass R et al. A Phase 3, randomised, open-label study to evaluate the efficacy and safety of 8 and 12 weeks of simeprevir (SMV) plus sofosbuvir (SOF) in treatment naive and -experienced patients with chronic HCV genotype 1 infection without cirrhosis: Optimist 1. J. Hepatol. 62(S1), S270 (2015).
66.
Sherman KE, Flamm SL, Afdhal NH et al. Response-guided telaprevir combination treatment for hepatitis C virus infection. N. Engl. J. Med. 365(11), 1014–1024 (2011).
67.
Zeuzem S, Berg T, Gane E et al. Simeprevir increases rate of sustained virologic response among treatment-experienced patients with HCV genotype-1 infection: a Phase IIb trial. Gastroenterology 146(2), e430–e441. (2014).
68.
Lawitz E, Sulkowski MS, Ghalib R et al. Simeprevir plus sofosbuvir, with or without ribavirin, to treat chronic infection with hepatitis C virus genotype 1 in non-responders to pegylated interferon and ribavirin and treatment-naive patients: the COSMOS randomised study. Lancet 384(9956), 1756–1765 (2014).
69.
Reddy KR, Zeuzem S, Zoulim F et al. Simeprevir versus telaprevir with peginterferon and ribavirin in previous null or partial responders with chronic hepatitis C virus genotype 1 infection (ATTAIN): a randomised, double-blind, non-inferiority Phase 3 trial. Lancet Infect. Dis. 15(1), 27–35 (2015).
70.
Forns X, Lawitz E, Zeuzem S et al. Simeprevir with peginterferon and ribavirin leads to high rates of SVR in patients with HCV genotype 1 who relapsed after previous therapy: a Phase 3 trial. Gastroenterology 146(7), e1669–e1679. (2014).
71.
Manns M, Marcellin P, Poordad F et al. Simeprevir with pegylated interferon alfa 2a or 2b plus ribavirin in treatment-naive patients with chronic hepatitis C virus genotype 1 infection (QUEST-2): a randomised, double-blind, placebo-controlled Phase 3 trial. Lancet 384(9941), 414–426 (2014).
72.
Jacobson IM, Dore GJ, Foster GR et al. Simeprevir with pegylated interferon alfa 2a plus ribavirin in treatment-naive patients with chronic hepatitis C virus genotype 1 infection (QUEST-1): a Phase 3, randomised, double-blind, placebo-controlled trial. Lancet 384(9941), 403–413 (2014).
73.
Lawitz E, Poordad FF, Pang PS et al. Sofosbuvir and ledipasvir fixed-dose combination with and without ribavirin in treatment-naive and previously treated patients with genotype 1 hepatitis C virus infection (LONESTAR) an open-label, randomised, Phase 2 trial. Lancet 383(9916), 515–523 (2014).
74.
Osinusi A, Meissner EG, Lee YJ et al. Sofosbuvir and ribavirin for hepatitis C genotype 1 in patients with unfavorable treatment characteristics: a randomized clinical trial. JAMA 310(8), 804–811 (2013).
75.
Lawitz E, Mangia A, Wyles D et al. Sofosbuvir for previously untreated chronic hepatitis C infection. N. Engl. J. Med. 368(20), 1878–1887 (2013).
76.
Lawitz E, Lalezari JP, Hassanein T et al. Sofosbuvir in combination with peginterferon alfa-2a and ribavirin for non-cirrhotic, treatment-naive patients with genotypes 1, 2, and 3 hepatitis C infection: a randomised, double-blind, Phase 2 trial. Lancet Infect. Dis. 13(5), 401–408 (2013).
77.
Chulanov V, Zhdanov K, Kersey K et al. Sofosbuvir plus Ribavirin for the treatment of Russian patients with chronic HCV genotype 1 or 3 infection. Hepatology 60(4S), A676 (2014).
78.
Kowdley KV, Lawitz E, Crespo I et al. Sofosbuvir with pegylated interferon alfa-2a and ribavirin for treatment-naive patients with hepatitis C genotype-1 infection (ATOMIC): an open-label, randomised, multicentre Phase 2 trial. Lancet 381(9883), 2100–2107 (2013).
79.
Hezode C, Forestier N, Dusheiko G et al. Telaprevir and peginterferon with or without ribavirin for chronic HCV infection. N. Engl. J. Med. 360(18), 1839–1850 (2009).
80.
Mchutchison JG, Manns MP, Muir AJ et al. Telaprevir for previously treated chronic HCV infection. N. Engl. J. Med. 362(14), 1292–1303 (2010).
81.
Jacobson IM, Mchutchison JG, Dusheiko G et al. Telaprevir for previously untreated chronic hepatitis C virus infection. N. Engl. J. Med. 364(25), 2405–2416 (2011).
82.
Zeuzem S, Andreone P, Pol S et al. Telaprevir for retreatment of HCV infection. N. Engl. J. Med. 364(25), 2417–2428 (2011).
83.
Mchutchison JG, Everson GT, Gordon SC et al. Telaprevir with peginterferon and ribavirin for chronic HCV genotype 1 infection. N. Engl. J. Med. 360(18), 1827–1838 (2009).
84.
Kumada H, Toyota J, Okanoue T, Chayama K, Tsubouchi H, Hayashi N. Telaprevir with peginterferon and ribavirin for treatment-naive patients chronically infected with HCV of genotype 1 in Japan. J. Hepatol. 56(1), 78–84. 2012
85.
Alam I, Manch R, Naggie S et al. Effectiveness of simeprevir (SMV)-containing regimens among patients with chronic hepatitis C virus (HCV) in various us practice settings: interim analysis of the SONET study. J. Hepatol. 62, S646–S647 (2015).
86.
Alric L, Guivarch M, Berard E et al. Sustained virological response to telaprevir and boceprevir in previously non-responder HCV genotype 1 patients with severe liver fibrosis: results of a prospective multi-centric study. Hepatol. A 58(Suppl 4.), A1155 (2013).
87.
Backus LI, Belperio PS, Shahoumian TA, Cheung R, Mole LA. Comparative effectiveness of the hepatitis C virus protease inhibitors boceprevir and telaprevir in a large U.S. cohort. Aliment. Pharmacol. Ther. 39(1), 93–103 (2014).
88.
Backus LI, Belperio PS, Shahoumian TA, Loomis TP, Mole LA. Effectiveness of sofosbuvir-based regimens in genotype 1 and 2 hepatitis C virus infection in 4026 U.S. Veterans. Aliment. Pharmacol. Ther. 42(5), 559–573 (2015).
89.
Backus LI, Belperio PS, Shahoumian TA, Mole LA. Effectiveness of sofosbuvir-based hepatitis C (HCV) antiviral regimens in a large U.S. veteran cohort. Gastroenterology 148(4), S978–S979 (2015).
90.
Bonnet D, Guivarch M, Berard E et al. Telaprevir- and boceprevir-based tritherapies in real practice for F3-F4 pretreated hepatitis C virus patients. World J. Hepatol. 6(9), 660–669 (2014).
91.
Bruno S, Bollani S, Zignego AL et al. Efficacy and safety of boceprevir-based therapy in HCVG1 treatment-experienced patients with advanced fibrosis/cirrhosis: Italian NPP survey. Dig. Liver Dis. 46, e12 (2014).
92.
Calleja JL, Pascasio JM, Ruiz-Antoran B et al. Safety and efficacy of triple therapy with peginterferon, ribavirin and boceprevir within an early access programme in Spanish patients with hepatitis C genotype 1 with severe fibrosis: SVRw12 analysis. Liver Int. 35(1), 90–100 (2015).
93.
Colombo M, Strasser S, Moreno C et al. Sustained virological response with telaprevir in 1078 patients with advanced hepatitis C: The international telaprevir access program. J. Hepatol. 61(5), 976–983 (2014).
94.
Curry MP, Bacon B, Flamm SL et al. Effectiveness of 12 or 24 week LDV/SOF and 12 week LDV/SOF + RBV in treatment-experienced patients with cirrhotic, genotype 1 hepatitis C: real-world experience from the Trio network. Hepatology A62, A755 (2015).
95.
Curry MP, Bacon B, Flamm SL et al. Effectiveness of 8 or 12 week LDV/SOF in treatment-naive patients with non-cirrhotic, genotype 1 hepatitis C: real-world experience from the TRIO network. Hepatology A62, 721 (2015).
96.
Dev AT, Mitchell J, Polkinghorne K et al. Treatment safety and efficacy of Boceprevir-based triple therapy in genotype 1 hepatitis C: the Australian multicentre Boceprevir real world experience (SABRE-C). Hepatology A60, A674 (2014).
97.
Fernandez C, Munoz De Rueda P, Alonso S et al. Effectiveness of triple therapy with boceprevir or telaprevir in a multicentre clinical practice cohort of HCV treatment-experienced patients wtih advanced hepatitic fibrosis: SVR 12W after treatment. J. Hepatol. 60(Suppl.1), S488 (2014).
98.
Fontaine H, Lacombe K, Dhiver C et al. LP23: Daclatasvir plus sofosbuvir with or without ribavirin in patients with HIV–HCV co-infection: interim analysis of a French multicenter compassionate use program. J. Hepatol. 62(Suppl. 2), S275 (2015).
99.
Foster GR, Irving WL, Cheung MC et al. Cohort study of the impact of direct acting antiviral therapy in patients with chronic hepatitis C and decompensated cirrhosis. J. Hepatol. 64 6 1224–1231 (2016).
100.
Gill K, Fante G, Nafisi S et al. Sofosbuvir and ledipasvir for the treatment of HCV GT-1, cirrhotics and non-cirrhotics: real-world effectiveness. Hepatology 62, 757.64(6), 1224–1231 (2016).
101.
Gordon SC, Muir AJ, Lim JK et al. Safety profile of boceprevir and telaprevir in chronic hepatitis C: real world experience from HCV-TARGET. J. Hepatol. 62(2), 286–293 (2015).
102.
Gray E, O’Leary A, C B, Norris S. Real-world effectiveness of DAA Regimens for HCV infection from an Irish national HCV registry. Pharmacoepidemiol. Drug Saf. 25(S3), (2016).
103.
Hezode C, Fontaine H, Dorival C et al. Triple therapy in treatment-experienced patients with HCV-cirrhosis in a multicentre cohort of the French Early Access Programme (ANRS CO20-CUPIC) - NCT01514890. J. Hepatol. 59(3), 434–441 (2013).
104.
Ioannou GN, Beste LA, Green PK. Similar effectiveness of boceprevir and telaprevir treatment regimens for hepatitis C virus infection on the basis of a nationwide study of veterans. Clin. Gastroenterol. Hepatol. 12(8), 1371–1380 (2014).
105.
Khalid H, Khalid O, Hilton R, Bhatia R, Bhatti F, Bacon BR. Telaprevir: a real world experience. Gastroenterology 144(5), S980–981 (2013).
106.
Khalid O, Khalid H, Hilton R, Bhatia R, Bhatti F, Bacon BR. Boceprevir: a real world experience. Gastroenterology 144(5), S984 (2013).
107.
Lai C, Witt DJ, M.A W. Real-world effectiveness of sofosbuvir (SOF), telaprevir and boceprevir (T, B) based in therapy for hepatitis C virus (HCV): an analysis in a large integrated health care system. J. Hepatol. 2015(Suppl.1), S658 (2015).
108.
Lebovics E, Maranino AN, Zahiruddin A et al. Single-center real-world experience of sofosbuvir plus simeprevir for 12 weeks for genotype 1 chronic hepatitis C with advanced fibrosis. Gastroenterology 148(4), S1084 (2015).
109.
Mauss S, Böker K, Buggisch P et al. Real-life experience with first generation HCV protease inhibitor therapy in Germany: the prospective, non-interventional PAN cohort. Z. Gastroenterol. 53(7), 644–654 (2015).
110.
Mauss S, Buti M, Ryder SD et al. SVR rates with telaprevir and boceprevir in us clinical practice. Gastroenterology 146(5), S-980 (2014).
111.
Nazareth S, Fragomeli V, Colman A et al. The first Australasian experience with boceprevir: treatment outcomes, adverse events and adherence. Hepatol. Int. 8(1), S184 (2014).
112.
Nguyen-Khac E, Pariente A, Lesgourgues B et al. Simeprevir plus sofosbuvir for the treatment of hepatitis C genotype 1 and 4 in a French mulitcenter cohort in real life: real SimSof study. Hepatology 62(S1), A735–A736 (2015).
113.
Petersen J, Olah K, Unger S et al. Real world treatment with first generation triple therapy for HCV-GT1 difficult-to-treat patients: final results of an observational study in patients with advanced liver disease and non-response. J. Hepatol. 60(Suppl.1), S486 (2014).
114.
Price JC, Murphy RC, Shvachko VA, Pauly MP, Manos MM. Effectiveness of telaprevir and boceprevir triple therapy for patients with hepatitis C virus infection in a large integrated care setting. Dig. Dis. Sci. 59(12), 3043–3052 (2014).
115.
Reddy R, Lim JK, Kuo A et al. All oral HCV therapy is safe and effective in patients with decompensated cirrhosis: interim report from the HCV-target real world experience. J. Hepatol. 62, S193 (2015).
116.
Rodriguez EA, Levy C, Martin P, Bhamidimarri KR. Efficacy of sofosbuvir and simeprevir (COSMOS regimen) in hepatitis C genotype 1 in decompensated cirrhosis: a tertiary-center experience. Hepatology 62, A806–A807 (2015).
117.
Roytman M, Tang A, Wu C et al. Real life experience with sofobuvir and ledipasvir fixed dose regimen in the multicentric cohort of patients with chronic hepatitis C. Hepatology 62(S1), A761–A762 (2015).
118.
Salmeron J, Vinaixa C, Berenguer R et al. Effectiveness and safety of first-generation protease inhibitors in clinical practice: hepatitis C virus patients with advanced fibrosis. World J. Gastroenterol. 21(30), 9163–9174 (2015).
119.
Sukeepaisarnjaroen W, Pham T, Tanwandee T et al. Boceprevir early-access for advanced-fibrosis/cirrhosis in Asia-Pacific hepatitis C virus genotype 1 non-responders/relapsers. World J. Gastroenterol. 21(28), 8660–8669 (2015).
120.
Sulkowski MS, Vargas HE, Di Bisceglie AM et al. Effectiveness of Simeprevir plus Sofosbuvir, with or without Ribavirin, in real-world patients with HCV genotype 1 infection. Gastroenterology 150(2), 419–429 (2016).
121.
Terrault N, Zeuzem S, Di Bisceglie AM et al. Treatment outcomes with 8, 12 and 24 week regimens of ledipasvir/sofosbuvir for the treatment of hepatitis C infection: analysis of a multicenter prospective observational study. Hepatology 62, 256A (2015).
122.
Vo KP, Vutien P, Akiyama MJ et al. Poor sustained virological response in a multicenter real-life cohort of chronic hepatitis C patients treated with pegylated interferon and ribavirin plus telaprevir or boceprevir. Dig. Dis. Sci. 60(4), 1045–1051 (2015).
123.
Walker DR, Pedrosa MC, Manthena SR, Patel N, Marx SE. Early view of the effectiveness of new direct-acting antiviral (DAA) regimens in patients with hepatitis C virus (HCV). Adv. Ther. 32(11), 1117–1127 (2015).
124.
Wehmeyer MH, Eissing F, Jordan S et al. Safety and efficacy of protease inhibitor based combination therapy in a single-center “real-life” cohort of 110 patients with chronic hepatitis C genotype 1 infection. BMC Gastroenterol. 14, 87 (2014).
125.
Welzel T, Herzer K, Ferenci P et al. Daclatasvir plus sofosbuvirwith or without ribavirin for the treatment of HCV in patients with severe liver disease: interim results of a compassionate use program. J. Viral Hepat. 22, 4–5 (2015).
126.
Werner CR, Franz C, Egetemeyr DP et al. First-generation protease inhibitor-triple therapy: SVR 24, safety, and predictors of response in a large single center cohort. Virol J. 12, 37 (2015).
127.
Backus LI, Belperio PS, Shahoumian T, Loomis TP, Mole LA. Effectiveness of ledipasvir/sofosbuvir in treatment naive genotype 1 patients treated in routine medical practice. Hepatology 62, A255–A256 (2015).
128.
Kwok M, Foster T, Steinberg M. Expedited programs for serious conditions: an update on breakthrough therapy designation. Clin. Ther. 37(9), 2104–2120 (2015).
129.
Sterling RK, Dharel N. Treatment of hepatitis C, then, now and tomorrow. Evid. Based Med. 20(1), 23 (2015).
• Discusses the exclusion of ‘difficult-to-treat’ patient subgroups from clinical trials.
130.
Lievre M, Cucherat M, Leizorovicz A. Pooling, meta-analysis, and the evaluation of drug safety. Curr. Control Trials Cardiovasc. Med. 3(1), 6 (2002).
•• Discusses one of the limitations to this study – the naive pooling of the efficacy data.
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 17 November 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Do disparities between populations in randomized controlled trials and the real world lead to differences in outcomes?. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0042
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Rachel Giblon, Chengyang Gao, Kuan Liu, Yongdong Ouyang, Jessie Cunningham, Allen L. Pimienta, Ewan C. Goligher, Anna Heath, Who benefits? Uncovering hidden heterogeneity of treatment effects in adaptive trials using Bayesian methods: a systematic review, Trials, 10.1186/s13063-025-09291-x, 26, 1, (2025).
- Ingrid Toews, Andrew Anglemyer, John LZ Nyirenda, Dima Alsaid, Sara Balduzzi, Kathrin Grummich, Lukas Schwingshackl, Lisa Bero, Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials: a meta-epidemiological study, Cochrane Database of Systematic Reviews, 10.1002/14651858.MR000034.pub3, 2024, 1, (2024).
- Bridget M. Nugent, Rajanikanth Madabushi, Barbara Buch, Vasum Peiris, Victor Crentsil, Virginia M. Miller, Jonca Bull, Marjorie R. Jenkins, Heterogeneity in treatment effects across diverse populations, Pharmaceutical Statistics, 10.1002/pst.2161, 20, 5, (929-938), (2021).
- Tim Mathes, Tanja Rombey, Oliver Kuss, Dawid Pieper, No inexplicable disagreements between real-world data–based nonrandomized controlled studies and randomized controlled trials were found, Journal of Clinical Epidemiology, 10.1016/j.jclinepi.2020.12.019, 133, (1-13), (2021).
- Hegler C. Tissot, Anoop D. Shah, David Brealey, Steve Harris, Ruth Agbakoba, Amos Folarin, Luis Romao, Lukasz Roguski, Richard Dobson, Folkert W. Asselbergs, Natural Language Processing for Mimicking Clinical Trial Recruitment in Critical Care: A Semi-Automated Simulation Based on the LeoPARDS Trial, IEEE Journal of Biomedical and Health Informatics, 10.1109/JBHI.2020.2977925, 24, 10, (2950-2959), (2020).
- Rolf H.H. Groenwold, Olaf M. Dekkers, Designing pragmatic trials—what can we learn from lessons learned?, Journal of Clinical Epidemiology, 10.1016/j.jclinepi.2017.06.006, 90, (3-5), (2017).