Sociodemographic disparities in treatment and survival of small localized renal cell carcinoma: surgical resection versus thermal ablation
Abstract
Aim: To investigate national practice trends in the use of surgical resection (SX) versus thermal ablation (TA) for the management of T1aN0M0 renal cell carcinoma with regard to sociodemographic factors and associated outcomes. Materials & methods: Patients diagnosed in 2004–2011 were identified using the Surveillance, Epidemiology and End Results registry. Sociodemographic factors predicting the use of surgery versus TA were determined using logistic regression. Cancer-specific survival was estimated using Kaplan–Meier method. Results: Overall, 19,136 (92.9%) patients underwent SX versus 1468 (7.1%) TA. Patients who were unmarried, diagnosed between 2008 and 2011, Caucasian, aged ≥70 years, insured, residing in Pacific Coast and Northern Plains, and in metropolitan areas with higher median family income had higher likelihoods of undergoing TA. Age-adjusted cancer-specific survival was similar in the two groups. Conclusion: Despite similar survival outcomes between SX versus TA, management of T1a renal cell carcinoma lesions may be influenced by a variety of nonclinical sociodemographic factors.
First draft submitted: 28 February 2016; Accepted for publication: 22 April 2016; Published online: 18 July 2016
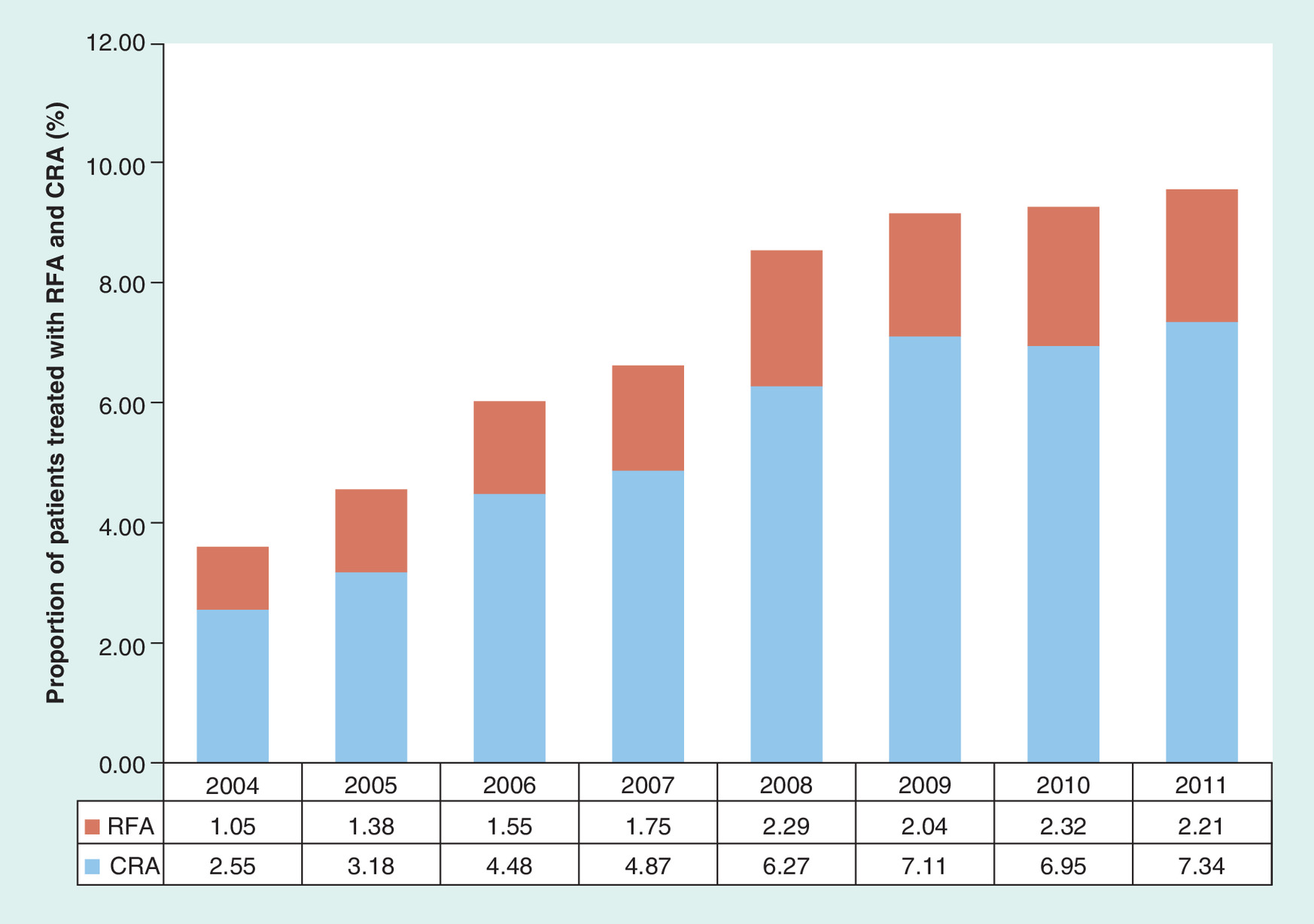
Figure 1. Longitudinal trends in the utilization of thermal ablation for treatment of T1a renal cell carcinoma lesions demonstrating significantly increased used of thermal ablation, specifically cryoablation between 2004 and 2011.
However, the proportion all T1a lesions treated with thermal ablation remains below 10%.
CRA: Cryoablation; RFA: Radiofrequency ablation (x-axis representing % of patients treated with either RFA or CRA).
With approximately 65,000 new cases diagnosed each year, renal cell carcinoma (RCC) is the most common primary kidney cancer in the USA [1]. Over the past several decades, there has been a steady increase in the incidence of RCC, particularly in its early stages as an incidental finding [2,3], thought to be in large part attributable to the increased utilization of cross-sectional imaging in the USA as well as epidemiological factors such as an aging population, obesity and tobacco use [2–4]. The annual cost of treatment of RCC in the elderly population is estimated to be up to US$4 billion [5]. While radical nephrectomy (RN) has traditionally been the treatment of choice for small organ-confined RCC, more recent transnational recommendations advocate nephron sparing partial nephrectomy (PN) as the standard of care in order to maximize renal function preservation and minimize associated long-term comorbidities [6,7].
Both US and European guidelines include less invasive thermal ablation (TA) techniques – specifically radiofrequency ablation (RFA) and cryoablation (CRA) – as recommended treatments for organ confined lesions ≤4 cm (T1aN0M0) in patients with significant comorbidities and surgical risks [6,7]. However, they also recommend that these ablative techniques be discussed with low-risk patients with T1a lesions as less invasive treatment options [6,7].
Single center studies have shown that long-term overall and progression-free survival are similar in patients with organ confined lesions ≤4 cm (T1aN0M0) managed by either surgical resection (SX; PN and RN) or less invasive TA (RFA and CRA) [8,9]. Although PN has shown to preserve renal function with similar disease recurrence and survival outcomes as compared with RN [10,11], there is substantial morbidity associated with both open and laparoscopic PN that could be minimized if TA were adopted more broadly [10].
Using a large US national oncologic database, we aimed to evaluate contemporary clinical practice in the utilization of surgery versus TA in the management of T1a RCC, to determine sociodemographic factors that may predict receipt of surgery versus ablation, and to evaluate the survival efficacy of both treatment modalities.
Materials & methods
Data source
The patient de-identified Surveillance, Epidemiology, and End Results (SEER) database used for this study is HIPAA compliant and publicly available. Local institutional review board exemption was obtained.
The National Cancer Institute SEER database comprises 18 regional registries in the USA covering 28% of the US population [12]. We utilized the database released in December 2014 containing patients diagnosed through 31 December 2011 and followed through 31 December 2012. The SEER registry contains information on type of cancer, staging, survival outcome and detailed patient demographics. It also contains various socioeconomic variables related to patients’ residential ZIP codes based on 2010 US Census data. Information on patients’ first course of cancer therapy is included, as well the date and cause of death. Because TA only became widely utilized as a viable treatment option during the last decade, only data since year 2004 forward were included.
Patient selection
We identified RCC patients diagnosed between 2004 and 2011 using International Classification of Disease for Oncology ICD-O3 code C64.9 (‘kidney, not otherwise specified’). Using available histologic data, all patients with urothelial carcinoma and other non-RCC tumors were excluded. Only patients with T1aN0M0 (≤4 cm renal confined tumor) stage disease according to latest American Joint Committee on Cancer (AJCC) staging system [13] were considered. We limited the sample to patients receiving TA (RFA [SEER code 15] and CRA [SEER codes 13 & 23], open SX [renal-sparing/partial nephrectomy (PN [SEER code 30])], and radical nephrectomy [RN (SEER codes 40, 70, 80)]). Patient sociodemographic information analysis included age, gender, ethnicity, marital status, geographic location, and education and income level based patient’s residential ZIP code. SEER registry clinical data, including tumor histology and size were also evaluated as predictor of receipt of certain type of curative therapy.
Statistical analysis
Sociodemographic, geographic and clinical determinants of the use of surgery versus TA were evaluated using Chi-square and logistic regression models. To evaluate more recent changes in the utilization of treatment modalities, subanalysis of differences in the utilization of TA between 2004 and 2007 versus 2008 and 2011 was also performed. Cancer-specific survival (CSS) was estimated by Kaplan–Meier (KM) analysis from time of diagnosis to ‘death related to specific cancer diagnosis’ as recorded in SEER. Log-rank test (univariate) and cox-regression (multivariate) analyses were performed to identify predictors of survival. All database programming, statistical analysis and data management were performed using SAS (version 10, Cary, NC, USA).
Results
Baseline characteristics
Between years 2004 and 2011, 22,735 patients with T1aN0M0 RCC as their first primary cancer were identified. The median age of the cohort was 63.5 years (standard deviation [SD]: 12.9 years) and 13,618 (59.9%) were male. Overall, 20,604 patients underwent either SX or TA. SX was performed in 19,136 (92.9%) patients whereas 1468 (7.1%) patients underwent a form of TA therapy. Within the surgical group, 10,313 (50.1%) patients underwent RN and 8823 (42.8%) underwent PN. In the TA group, 1091 (5.3%) were treated with CRA whereas 377 (1.8%) were treated with RFA. The 2131 patients who did not receive any curative cancer-directed therapy demonstrated a significantly older median age of 72.1 years (SD: 10.3 years) vs 60.1 years (SD: 11.7 years) for those who underwent curative therapy (p < 0.001). Table 1 summarizes the baseline characteristics of patients undergoing surgery versus TA.
Sociodemographic & clinical predictors of receiving TA
On univariate analysis (UVA), patients who were unmarried, ≥70 years of age, of Caucasian ethnicity, diagnosed after year 2007, living in metropolitan areas, in Pacific Coast or Northern Plains regions, residing in areas with higher median family income, and those with health insurance demonstrated increased likelihoods of undergoing TA (Table 2). In terms of tumor characteristics, there was a statistically significant difference in the use for TA for lesion ≤2 cm versus those between 2.1 and 4.0 cm (p = 0.012). Furthermore, patients with an unspecified histology result (‘RCC nonspecified’) as well as those with papillary RCC were found to be more likely to undergo TA as compared with other histologies. When comparing recent changes in the use of TA, there has been a significant increase in the use of TA compared with surgery in more recent years. Between 2004 and 2007, on average 5.2% of all T1N0M0 RCC’s were treated with TA (Figure 1); this increased to 9.1% between 2008 and 2011 (p<0.001).
In multivariate analysis (MVA), age ≥70 years, diagnosis after 2007, living in the Pacific region, being of Caucasian decent, living in large metropolitan areas with higher median family incomes, and better insurance status were all found to be independent determinants of receipt of TA (Table 2). Tumor size of ≤2 cm was also found to be predictor of receipt of TA over surgery (p < 0.001).
Therapeutic outcome
Median follow-up for the entire cohort was 33.1 months (SD: 23.4 months). CSS from time of diagnosis was estimated by KM analysis. All further analysis was performed based on CSS for patients who received curative therapy. For patients undergoing curative therapy, CSS from the time of diagnosis was 81.3 months (95% CI: 81–81.4 months). Median CSS could not be calculated because the majority of patients (98%) remained alive throughout follow-up. The cohort’s 1-, 2- and 3-year survival rates were 98.7, 98.4 and 98.2%, respectively. There were no statistically significant difference in the survival rates of patients undergoing surgical treatment versus those undergoing TA. Specifically, the 1-, 2- and 3-year survival rates for the surgery group were 98.7, 98.4 and 98.2% versus 98.6, 98.5 and 98.3% for the TA group (p > 0.05).
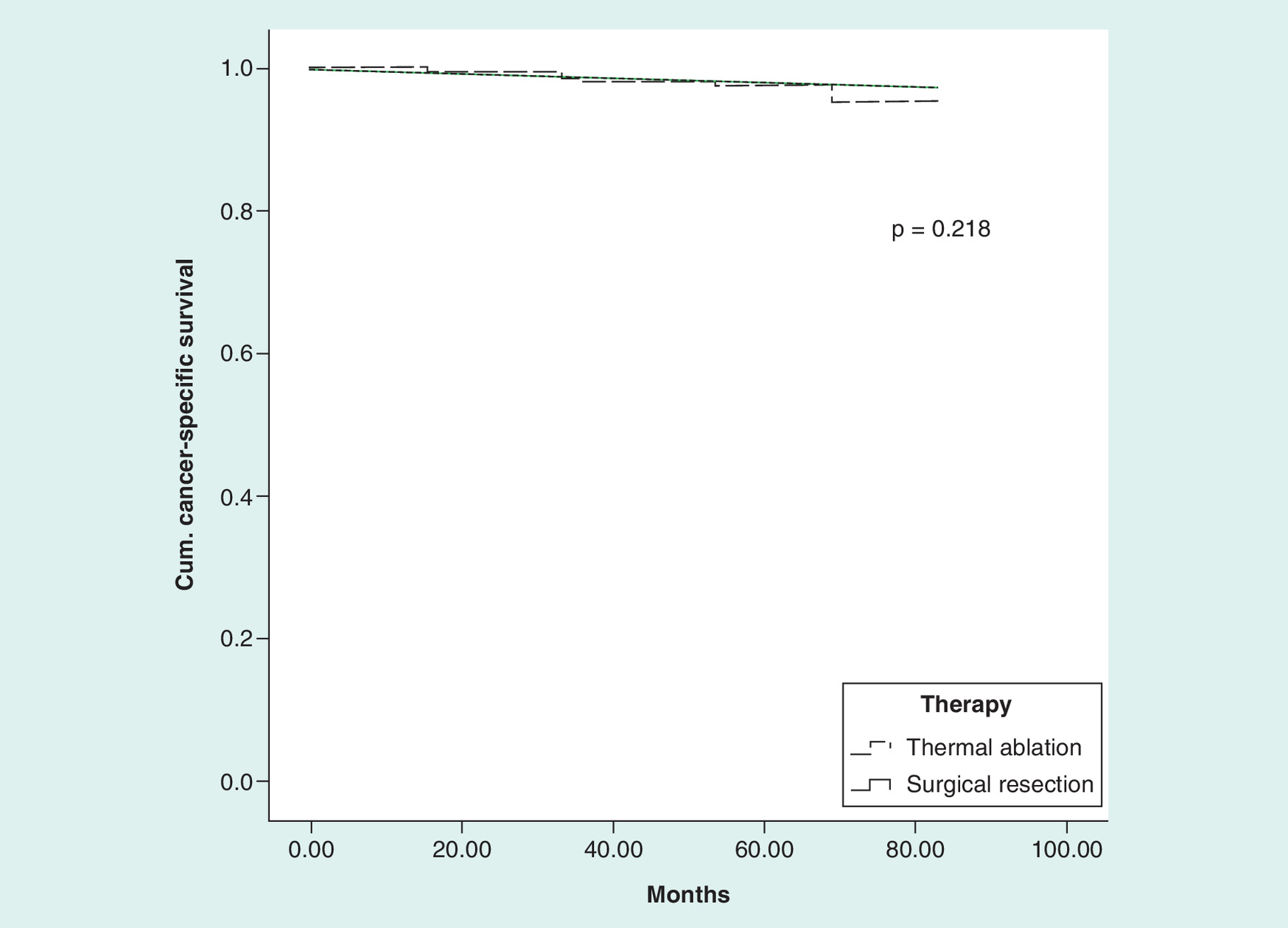
When adjusted for age, using cox regression model, there was no statistical difference in CSS between the surgery versus TA groups (p = 0.218; Figure 2). illustrates KM survival analysis of patients in the surgery and TA groups. Age was found to be independent predictor of survival in patients undergoing curative therapy both on UVA and MVA (Table 3). Insurance status was found to be predictor of survival on UVA. When adjusted for age, no sociodemographic or clinical factor was found to be predictor of survival on MVA.
Discussion
According to both guidelines of both USA and European urological societies, nephron sparing surgery is the treatment of choice for patients with T1a lesions who are suitable surgical candidates [6,7]. These guidelines recommend TA or active surveillance for T1a lesions in patients who are poor surgical candidates, with both guidelines acknowledging higher local tumor recurrence rates and incomplete ablation in patients treated with TA [6,7]. Those recommendations, however, are based on older ablation data with incomplete ablation rates of up to 20% [14]. This is likely playing a major role on the type of therapies patients have received in recent years, in other words, 90%+ patients undergoing surgery.
More recent predominantly single-center studies report similar oncologic outcomes between surgery and TA with regard to both overall and recurrence-free survival for T1a and T1b lesions upon long-term follow-up [8,9]. With newer ablative technology and techniques, local tumor recurrence requiring second ablations ranges from 4 to 8% for T1a RCC tumors [9,15]. Using a large national cancer database with median follow-up period of approximately 3 years, our study confirms similar oncologic outcome for T1a lesions between surgical and TA groups.
Studying SEER data for patients with T1N0M0 RCC lesions (≤7 cm) diagnosed between 2004 and 2007, Choueiri et al. reported that only 3.8% of patients underwent TA, with male gender, older age, single relationship status and tumor size of ≤4 cm all identifiable as independent predictors of receipt of TA [16]. With approximately 2 years median follow-up, the same study demonstrated no statistically significant difference in CSS or OS [16]. An older SEER study investigating patients with lesions less than 4 cm between 1998 and 2007 reported a twofold increased risk of kidney cancer death with TA compared with nephron-sparing surgery (hazard ratio [HR]: 1.9; 95% CI: 1.1–3.3 [p = 0.02]); however, the absolute difference in survival at 5 years was very small (98.3% for surgery vs 96.6% for TA) and was thought to be significant only in patients in long life expectancies [17]. In our study, with longer follow-up, we also found no difference in CSS when adjusted for age. Similar to Choueiri et al. study, we found older age and single relationship status to be predictors of receipt of TA.
Additionally, several regional, ethnic and sociodemographic disparities predicting the receipt of TA over surgery were identified; these included Caucasian ethnicity, living in metropolitan or large urban area, living in the Pacific Coast or Northern Plains SEER regions, living in ZIP code areas with higher levels of college education and median family income and better insurance coverage. The socioeconomic and demographic differences could be in part related to a wider availability of ablative technology in larger (hence urban/academic) centers that in turn are more likely to be accessible to higher socioeconomic status with more ease.
While the findings in our study confirm similar efficacy of surgery and TA for T1a RCC lesion as suggested by more recent single-center studies [8,9], it also demonstrates substantial potential underutilization of TA based on regional and sociodemographic disparities. These suggest issues related to access to more contemporaneous therapy (i.e., less invasive TA). Although PN aims to preserve renal function in the long term, there remains a substantial risk of chronic kidney disease due to warm ischemia, particularly in the setting of laparoscopic PN [18]. Furthermore, despite a shorter recovery time and less blood loss in laparoscopic PN, it is associated with increased major complication rates compared with open PN [10,19]. On the other hand, TA techniques have lower complication rates, shorter recovery periods and improved long-term renal function preservation compared with SX [9,20]. There is also significantly lower direct procedural cost associated with TA compared with surgery; the predominantly outpatient management of TA patient also eliminates the need for postprocedural hospital stays, further decreasing the associated short-term economic burden of TA [21].
As previously demonstrated by Pandharipande and colleagues, with similar efficacy between surgery and TA, the lower direct procedural costs and indirect costs as well as favorable short- and long-term complications of TA compared with SX makes TA therapy more attractive, particularly in an era of healthcare reform with tremendous emphasis on promoting cost-effective therapies [22].
The limitations of this study include the inability to differentiate percutaneous and surgical ablation using the SEER database alone. Furthermore, the SEER database only records the first curative therapy patients receive and does not record recurrence-free survival. Hence, the true rate of further therapies related to tumor recurrence as well as associated short- and long-term complications cannot be analyzed. Moreover, the median follow-up period achieved in this was relatively short (∼3 years) which may cause inadequate evaluation of difference in CSS between TA and surgery. Additionally, the SEER database does not contain billing information and hence does not track follow-up imaging studies the patients undergo after either TA or surgery. Furthermore, the retrospective nature of the study makes the relationship between sociodemographic factors and likelihood of receiving various therapies less definitive. Finally, the presence of comorbidity affecting survival and type of therapy received is not available on SEER dataset. Several of these limitations can be addressed using SEER-Medicare database utilizing detailed patient-specific Medicare claims information. Our group is currently pursuing subsequent more detailed work using linked SEER-Medicare claims data.
Conclusion
An analysis of large national cancer database demonstrates significant sociodemographic disparities that may influence the use of surgery versus TA to treat small localized RCCs. Despite similar oncologic efficacies of both therapies, there is relative underutilization of less invasive TA procedures.
| Baseline characteristics | CRA, n (%) | RFA, n (%) | TA, n (%) | PN, n (%) | RN, n (%) | SX (RN and PN), n (%) |
|---|---|---|---|---|---|---|
| n = 20,604 | 1091 (5.3) | 377 (1.8) | 1468 (7.1) | 8823 (42.8) | 103,131 (50.1) | 19,136 (92.9) |
| Gender: | ||||||
| – Male | 673 (5.4) | 216 (1.7) | 889 (7.2) | 5482 (44.4) | 5987 (48.4) | 11,469 (92.8) |
| – Female | 418 (5.1) | 161 (2.0) | 579 (7.1) | 3341 (40.5) | 4326 (52.5) | 7667 (93) |
| Age (years): | ||||||
| – <70 | 598 (3.8) | 190 (1.2) | 788 (5) | 7393 (46.5) | 7704 (48.5) | 15,097 (95) |
| – ≥70 | 493 (10.4) | 187 (4.0) | 680 (14.4) | 1430 (30.3) | 2609 (55.3) | 4039 (85.6) |
| Race: | ||||||
| – Caucasian | 941 (5.5) | 309 (1.8) | 1250 (7.3) | 7346 (43.2) | 8413 (49.5) | 15,759 (92.7) |
| – African–American | 94 (4.1) | 35 (1.5) | 129 (5.6) | 888 (38.6) | 1284 (55.8) | 2172 (94.4) |
| – Asian | 31 (3.4) | 29 (3.2) | 60 (6.6) | 412 (45.1) | 441 (48.3) | 853 (93.4) |
| – Others | 25 (6.6) | 7 (1.8) | 32 (8.4) | 177 (46.5) | 175 (45.9) | 352 (91.6) |
| Regional characteristics: | ||||||
| – Metropolitan or large urban area (pop >250K) | 1057 (5.3) | 365 (1.8) | 1422 (7.1) | 8545 (42.9) | 9968 (50) | 18,513 (92.9) |
| – Small urban or rural area | 34 (5.1) | 12 (1.8) | 46 (6.9) | 278 (41.6) | 345 (51.6) | 623 (93.1) |
| Region: | ||||||
| – Pacific Coast | 509 (5.7) | 201 (2.3) | 710 (8) | 3797 (42.6) | 4414 (49.5) | 8211 (92) |
| – East | 373 (4.3) | 122 (1.4) | 495 (5.7) | 3863 (44.1) | 4395 (50.2) | 8258 (94.3) |
| – Northern Plains | 161 (7.5) | 44 (2.1) | 205 (9.6) | 864 (40.5) | 1065 (49.9) | 1929 (90.4) |
| – Southwest | 45 (5.9) | 10 (1.3) | 55 (7.2) | 288 (37.7) | 420 (55) | 708 (92.8) |
| – Alaska | 3 (9.1) | 0 (0) | 3 (9.1) | 11 (33.3) | 19 (57.6) | 30 (90.9) |
| Family status: | ||||||
| – Single/divorced/widowed | 378 (5.8) | 134 (2.0) | 512 (7.8) | 2643 (40.4) | 3392 (51.8) | 6035 (92.2) |
| – Married/domestic partner | 663 (5) | 234 (1.8) | 897 (6.8) | 5797 (43.9) | 6518 (49.3) | 12,315 (93.2) |
| – Unknown | 50 (5.9) | 9 (1.1) | 59 (7) | 383 (45.3) | 403 (47.7) | 786 (93) |
| Education level (% with bachelor degrees): | ||||||
| – <35 | 829 (5.3) | 293 (1.8) | 1122 (7.2) | 6566 (42.3) | 7850 (50.5) | 14,416 (92.8) |
| – ≥35 | 262 (5.2) | 84 (1.7) | 346 (6.9) | 2257 (44.6) | 2463 (48.6) | 4720 (93.2) |
| Median family income (US$): | ||||||
| – ≤58,000/year | 543 (4.9) | 195 (1.8) | 738 (6.7) | 4503 (41) | 5752 (52.3) | 10,255 (93.3) |
| – >58,000/year | 548 (5.7) | 182 (1.9) | 730 (7.6) | 4320 (44.9) | 4561 (47.5) | 8881 (92.4) |
| Insurance status: | ||||||
| – Insured (private/Medicare) | 815 (6.5) | 271 (2.2) | 1086 (8.7) | 5802 (46.5) | 5592 (44.8) | 11,394 (91.3) |
| – Uninsured | 5 (1.4) | 4 (1.1) | 9 (2.5) | 173 (48.6) | 174 (48.9) | 347 (97.5) |
| – Unknown | 271 (3.5) | 102 (1.3) | 373 (4.8) | 2848 (36.7) | 5447 (58.5) | 8295 (95.7) |
| Year of diagnosis: | ||||||
| – 2004–2007 | 408 (3.9) | 154 (1.5) | 562 (5.3) | 3963 (37.7) | 6000 (57) | 9963 (94.7%) |
| – 2008–2011 | 683 (6.8) | 223 (2.2) | 906 (9) | 4860 (48.2) | 4313 (42.8) | 9173 (91%) |
| Tumor size: | ||||||
| – ≤2 cm | 334 (5.8) | 112 (2.0) | 446 (7.8) | 3373 (58.9) | 1907 (33.3) | 5280 (92.2) |
| – 2.1–4 cm | 757 (5.1) | 265 (1.8) | 1022 (6.9) | 5450 (36.6) | 8406 (56.5) | 13856 (93.1) |
| Histology: | ||||||
| – RCC (nonsepcified) | 520 (5.5) | 213 (2.3) | 733 (7.8) | 3952 (41.8) | 4771 (50.5) | 8723 (92.2) |
| – Clear cell | 362 (4.4) | 110 (1.4) | 472 (5.8) 8218 | 3708 (45.1) | 4038 (49.1) | 7746 (94.3) |
| – Papillary | 174 (6.6) | 47 (1.8) | 221 (8.4) 2619 | 1021 (40) | 1377 (52.6) | 2398 (91.6) |
| – Chromophobe | 32 (11.5) | 7 (2.5) | 39 (14) 278 | 131 (47.1) | 108 (38.8) | 239 (86) |
CRA: Cryoablation; PN: Partial nephrectomy; RCC: Renal cell carcinoma; RFA: Radiofrequency ablation; RN: Radical nephrectomy; SX: Surgical resection; TA: Thermal ablation.
| Baseline characteristics | UVA (Chi-square test) | MVA (logistic regression) | ||
|---|---|---|---|---|
| OR (95% CI) TA vs SX (PN or RN) | p-value | OR (95% CI) TA vs SX (PN or RN) | p-value | |
| Gender: | ||||
| – Male | 1.03 (0.921–1.14) | 0.638 | 1.10 (0.99–1.23) | 0.09 |
| – Female | Reference | |||
| Age (years): | ||||
| – <70 | Reference | <0.001 | 3.40 (3.05–3.80)† | <0.001 |
| – ≥70 | 3.23 (2.90–3.59)† | |||
| Race: | ||||
| – Caucasian | 2.14 (1.55–2.73)† | <0.001 | 1.07 (0.976–1.170) | 0.151 |
| – African–American | Reference | |||
| – Asian | 1.45 (0.83–1.81) | |||
| – Others | 0.89 (0.63–1.19) | |||
| Regional characteristics: | ||||
| – Metropolitan or large urban area (pop>250K) | 1.15 (1.02–1.29)† | 0.029 | 1.021 (0.97–1.40) | 0.158 |
| – Small urban or rural area | Reference | |||
| Region: | ||||
| – Pacific Coast | 2.14 (1.38–2.67)† | <0.001 | 1.74 (1.21–1.96)† | 0.012 |
| – East | 1.42 (0.89–2.23) | |||
| – Northern Plains | 3.45 (2.71–3.83)† | |||
| – Southwest | 1.53(0.97–2.15) | |||
| – Alaska | Reference | |||
| Family status: | ||||
| – Single/divorced/widowed | 1.27 (1.07–1.63)† | 0.020 | 1.08 (0.99–1.18) | 0.087 |
| – Married/domestic partner | 0.94 (0.84–1.31) | |||
| – Unknown | Reference | |||
| Education level (% bachelor degrees): | ||||
| – <35 | Reference | 0.347 | 1.19 (1.03–1.37)† | 0.018 |
| – ≥35 | 0.96 (0.71–1.30) | |||
| Median family income (US$): | ||||
| – ≤58,000/year | Reference | 0.014 | 1.15 (1.03–1.29)† | 0.012 |
| – >58,000/year | 1.14 (1.03–1.27)† | |||
| Insurance status: | ||||
| – Insured (private/Medicare) | 4.13 (3.68–4.69)† | <0.001 | 1.23 (1.13–1.34)† | <0.001 |
| – Uninsured | 1.12 (0.64–1.49) | |||
| – Unknown | Reference | |||
| Year of diagnosis: | ||||
| – 2004–2007 | Reference | <0.001 | 1.41 (1.21–1.64)† | <0.001 |
| – 2008–2011 | 1.75 (1.57–1.95)† | |||
| Tumor size: | ||||
| – ≤2 cm | 1.15 (1.02–1.29)† | 0.021 | 1.26 (1.12–1.41)† | <0.001 |
| – 2.1–4 cm | Reference | |||
| Histology: | ||||
| – RCC (nonspecified) | 2.14 (1.83– 2.59)† | <0.001 | 1.13 (1.02–1.41)† | 0.019 |
| – Clear cell | 0.71 (0.52–1.27) | |||
| – Papillary | 1.96 (1.70–2.42)† | |||
| – Chromophobe | Reference | |||
†Statistically significant values.
MVA: Multivariate analysis; RN: Radical nephrectomy; OR: Odds ratio; PN: Partial nephrectomy; RCC: Renal cell carcinoma; SX: Surgical resection; TA: Thermal ablation; UVA: Univariate analysis.
| Prognostic factor | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| Mean survival months | p-value | HR | p-value | |
| Age (years): | ||||
| – <70 years | 82.2 | <0.001 | 1.93 | <0.001 |
| – ≥70 years | 80.9 | |||
| Gender: | ||||
| – Male | 81.5 | 0.47 | 1.08 | 0.34 |
| – Female | 81.7 | |||
| Race: | ||||
| – Caucasian | 81.8 | 0.18 | 0.89 | 0.49 |
| – Black | 80.9 | |||
| – Others | 81.7 | |||
| Urban vs rural: | ||||
| – Metropolitan | 81.1 | 0.13 | 1.13 | 0.51 |
| – Small urban | 81.4 | |||
| – Rural | 80.7 | |||
| Region: | ||||
| –Alaska | 80.5 | 0.71 | 1.21 | 0.38 |
| – Northern Plains | 81.4 | |||
| – Pacific Coast | 81.7 | |||
| – East | 81.1 | |||
| – Southwest | 80.9 | |||
| Family status: | ||||
| – Single | 81.8 | 0.08 | 1.03 | 0.41 |
| – Married | 81.5 | |||
| Education (% bachelor degrees): | ||||
| – <20 | 81.3 | 0.06 | 0.95 | 0.31 |
| – ≥20 | 81.8 | |||
| Median family income (US$): | ||||
| – ≤58,000/year | 81.2 | 0.54 | 0.87 | 0.63 |
| – >58,000/year | 81.7 | |||
| Insurance status: | ||||
| – Insured | 82.1 | 0.001 | 1.26 | 0.09 |
| – Uninsured | 80.4 | |||
| Tumor size: | ||||
| – ≤2 cm | N/A | N/A | N/A | N/A |
| – 2.1–4 cm | ||||
| Histology: | ||||
| – RCC (unspecified) | 81.3 | 0.46 | 0.94 | 0.43 |
| – Clear cell | 81.5 | |||
| – Papillary | 81.1 | |||
| – Chromophobe | 81.2 | |||
| Treatment: | ||||
| – TA | 81.7 | 0.56 | 1.03 | 0.27 |
| – Surgery | 80.9 | |||
HR: Hazard ratio; N/A: Not applicable; RCC: Renal cell carcinoma; TA: Thermal ablation.
Increased incidence of early stage renal cell carcinoma (RCC) in the past 20 years due to increased use of cross-sectional imaging.
Current American and European Urologic Associations guidelines recommend thermal ablation (TA) only in patients who are not good surgical candidates.
These guidelines are based on older data that reported significantly higher rate of local disease recurrence in patients treated with TA.
Newer data suggest similar recurrence rate and oncologic outcome between TA and surgery in T1a RCC lesions.
This study demonstrated significant underutilization of TA compared with surgery for management of T1a RCC lesions.
The cancer-free survival was similar between the two groups.
Several demographic and socioeconomic factors may play a role in the likelihood of patients receiving TA versus surgery.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest
1.
Lang K, Danchenko N, Gondek K, Schwartz B, Thompson D. The burden of illness associated with renal cell carcinoma in the United States. Urol. Oncol. 25(5), 368–375 (2007).
2.
Cohen HT, McGovern FJ. Renal-cell carcinoma. N. Engl. J. Med. 353(23), 2477–2490 (2005).
3.
Pantuck AJ, Zisman A, Belldegrun AS. The changing natural history of renal cell carcinoma. J. Urol. 166(5), 1611–1623 (2001).
4.
Lowrance WT, Thompson RH, Yee DS, Kaag M, Donat SM, Russo P. Obesity is associated with a higher risk of clear-cell renal cell carcinoma than with other histologies. BJU Int. 105(1), 16–20 (2010).
5.
Allareddy V, Konety B. Inpatient costs for bladder, kidney, and prostate cancers in the year 2002. A study using the NIS sample. Presented at: American Urological Association Annual Meeting. Atlanta, GA, USA, 21 May 2006.
6.
Campbell SC, Novick AC, Belldegrun A et al. Guideline for management of the clinical T1 renal mass. J. Urol. 182(4), 1271–1279 (2009).
• 2009 American Urological Association guideline recommending thermal ablation (TA)-only patients who are not surgical candidates.
7.
Ljungberg B, Bensalah K, Canfield S et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur. Urol. 67(5), 913–924 (2015).
• 2015 European Association of Urology guideline recommending TA-only patients who are not surgical candidates.
8.
Thompson RH, Atwell T, Schmit G et al. Comparison of partial nephrectomy and percutaneous ablation for cT1 renal masses. Eur. Urol. 67(2), 252–259 (2015).
• Single-center study showing that long-term overall and progression-free survival are similar in patients with organ-confined lesions ≤4 cm (T1aN0M0) managed by either surgical resection or TA.
9.
Olweny EO, Park SK, Tan YK, Best SL, Trimmer C, Cadeddu JA. Radiofrequency ablation versus partial nephrectomy in patients with solitary clinical T1a renal cell carcinoma: comparable oncologic outcomes at a minimum of 5 years of follow-up. Eur. Urol. 61(6), 1156–1161 (2012).
• Surveillance, Epidemiology, and End Results database, the data source for this study with detailed explanation of advantages and limitations of the database.
10.
Huang WC, Levey AS, Serio AM et al. Chronic kidney disease after nephrectomy in patients with renal cortical tumours: a retrospective cohort study. Lancet Oncol. 7(9), 735–740 (2006).
11.
Hui GC, Tuncali K, Tatli S, Morrison PR, Silverman SG. Comparison of percutaneous and surgical approaches to renal tumor ablation: metaanalysis of effectiveness and complication rates. J. Vasc. Interv. Radiol. 19(9), 1311–1320 (2008).
12.
SEER Cancer Statistics Review, 1975–2011. Based on December 2014 SEER data submission. http://seer.cancer.gov/archive/csr/1975_2011/
13.
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A (Eds). AJCC Cancer Staging Manual, 7th edition. Springer, France (2010).
14.
Gervais DA, McGovern FJ, Arellano RS, McDougal WS, Mueller PR. Radiofrequency ablation of renal cell carcinoma: part 1, indications, results, and role in patient management over a 6-year period and ablation of 100 tumors. Am. J. Roentgenol. 185(1), 64–71 (2005).
15.
Psutka SP, Feldman AS, McDougal WS, McGovern FJ, Mueller P, Gervais DA. Long-term oncologic outcomes after radiofrequency ablation for T1 renal cell carcinoma. Eur. Urol. 63(3), 486–492 (2013).
16.
Choueiri TK, Schutz FA, Hevelone ND et al. Thermal ablation vs surgery for localized kidney cancer: a Surveillance, Epidemiology, and End Results (SEER) database analysis. Urology 78(1), 93–98 (2011).
• Older Surveillance, Epidemiology, and End Results data (2004–2007) demonstrating that only 3.8% of patients with with T1N0M0 renal cell carcinoma lesions (≤7 cm) received TA, with male gender, older age, single relationship status and tumor size of ≤4 cm, all identifiable as independent predictors of receipt of TA.
17.
Whitson JM, Harris CR, Meng MV. Population-based comparative effectiveness of nephron-sparing surgery vs ablation for small renal masses. BJU Int. 110(10), 1438–1443 (2012).
18.
Gill IS, Kavoussi LR, Lane BR et al. Comparison of 1,800 laparoscopic and open partial nephrectomies for single renal tumors. J. Urol. 178(1), 41–46 (2007).
19.
Fergany AF, Hafez KS, Novick AC. Long-term results of nephron sparing surgery for localized renal cell carcinoma: 10-year follow up. J. Urol. 163(2), 442–445 (2000).
20.
Lucas SM, Stern JM, Adibi M, Zeltser IS, Cadeddu JA, Raj GV. Renal function outcomes in patients treated for renal masses smaller than 4 cm by ablative and extirpative techniques. J. Urol. 179(1), 75–79 (2008).
21.
Castle SM, Gorbatiy V, Avallone MA, Eldefrawy A, Caulton DE, Leveillee RJ. Cost comparison of nephron-sparing treatments for cT1a renal masses. Urol. Oncol. 31(7), 1327–1332 (2013).
22.
Pandharipande PV, Gervais DA, Mueller PR, Hur C, Gazelle GS. Radiofrequency ablation versus nephron-sparing surgery for small unilateral renal cell carcinoma: cost–effectiveness analysis. Radiology 248(1), 169–178 (2008).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 18 July 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Sociodemographic disparities in treatment and survival of small localized renal cell carcinoma: surgical resection versus thermal ablation. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0014
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- B. Malik Wahba, Claudia Ramirez Marcano, Evan Suzman, Kyle A. Blum, Timothy D. McClure, Jim C. Hu, Population-based utilization and survival of competing treatments for small renal masses: The growing role of thermal ablation, Urologic Oncology: Seminars and Original Investigations, 10.1016/j.urolonc.2025.09.010, 44, 1, (67.e19-67.e26), (2026).
- Tarig S. Elhakim, Taha Lodhi, Wilton Fidelis, Allison Brea, Ana Mort, Maryam Mohagheghtabar, Azadeh Tabari, Samuel R. Davis, Raul N. Uppot, Ronald S. Arellano, Michael Dezube, Dania Daye, Management of renal cell carcinoma with ablation in comparison to nephrectomy: A 5-year analysis of inpatient procedural data to evaluate utilization disparities in the United States, Clinical Imaging, 10.1016/j.clinimag.2025.110412, 119, (110412), (2025).
- Kristina Imeen Ringe, Perkutane lokal-ablative Therapie beim kleinen Nierenzellkarzinom, TumorDiagnostik & Therapie, 10.1055/a-1711-0559, 43, 01, (54-60), (2022).
- Kristina Imeen Ringe, Perkutane lokal-ablative Therapie beim kleinen Nierenzellkarzinom, Aktuelle Urologie, 10.1055/a-1364-4633, 52, 05, (445-451), (2021).
- Marguerite M Hoyler, Mark D Abramovitz, Xiaoyue Ma, Diana Khatib, Richard Thalappillil, Christopher W Tam, Jon D Samuels, Robert S White, Social determinants of health affect unplanned readmissions following acute myocardial infarction, Journal of Comparative Effectiveness Research, 10.2217/cer-2020-0135, 10, 1, (39-54), (2021).
- Sharath K. Bhagavatula, Kemal Tuncali, Paul B. Shyn, Vincent M. Levesque, Steven L. Chang, Stuart G. Silverman, Percutaneous CT- and MRI-guided Cryoablation of cT1 Renal Cell Carcinoma: Intermediate- to Long-term Outcomes in 307 Patients, Radiology, 10.1148/radiol.2020200149, 296, 3, (687-695), (2020).
- Roberto Luigi Cazzato, Julien Garnon, Pierre De Marini, Pierre Auloge, Guillaume Koch, Danoob Dalili, Xavier Buy, Jean Palussiere, Pramod Prabhakar Rao, Thibault Tricard, Hervé Lang, Afshin Gangi, Is percutaneous image-guided renal tumour ablation ready for prime time?, The British Journal of Radiology, 10.1259/bjr.20200284, 93, 1114, (2020).
- Christopher S. Morris, Mark O. Baerlocher, Sean R. Dariushnia, Eric D. McLoney, Nadine Abi-Jaoudeh, Kari Nelson, Marco Cura, Ahmed Kamel Abdel Aal, Jason W. Mitchell, Sreekumar Madassery, Sasan Partovi, Timothy D. McClure, Alda L. Tam, Sheena Patel, Society of Interventional Radiology Position Statement on the Role of Percutaneous Ablation in Renal Cell Carcinoma, Journal of Vascular and Interventional Radiology, 10.1016/j.jvir.2019.11.001, 31, 2, (189-194.e3), (2020).
- Johannes Uhlig, Nima Kokabi, Minzhi Xing, Hyun S. Kim, Ablation versus Resection for Stage 1A Renal Cell Carcinoma: National Variation in Clinical Management and Selected Outcomes, Radiology, 10.1148/radiol.2018172960, 288, 3, (889-897), (2018).
- Omar Abdel-Rahman, Impact of histological subtype on outcomes of renal cell carcinoma patients, Journal of Drug Assessment, 10.1080/21556660.2018.1439831, 7, 1, (14-20), (2018).