Cost-effectiveness of PD-L1 testing to guide immunotherapy for patients with advanced non-small-cell lung cancer in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study aims to assess the cost-effectiveness of three major programmed death-ligand 1 (PD-L1) immunohistochemistry (IHC) testing assays in guiding immunotherapy for patients with advanced non-small-cell lung cancer (NSCLC) in China, and to provide empirical evidence on the selection of cost-effective diagnostics to support the immune checkpoint inhibitor monotherapy regimens for NSCLC patients. Materials & methods: From a healthcare system perspective, a decision tree model was constructed to simulate the cost and effectiveness of employing VENTANA PD-L1 (SP263) Assay, Dako PD-L1 IHC 22C3 assay, and Dako 22C3 antibody concentrate in advanced NSCLC patients in China. The cost-effectiveness of Ventana PD-L1 IHC SP263 assay compared with other testing methods was assessed through the incremental analysis. The robustness of the base case analysis results was validated by one-way sensitivity analysis and probabilistic sensitivity analysis. Results: The VENTANA PD-L1 (SP263) Assay, which can guide multiple immune checkpoint inhibitor monotherapies (e.g., atezolizumab and pembrolizumab) for advanced NSCLC patients, achieved a higher percentage of successfully diagnosed and treated, and a higher quality-adjusted life-year at a lower cost compared with Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate. The robustness of the base case results was confirmed by both one-way sensitivity analysis and probabilistic sensitivity analysis. Conclusion: The VENTANA PD-L1 (SP263) Assay is cost-effective compared with Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate for the immunotherapy treatment for advanced NSCLC patients in China.
Plain language summary
What is this article about?
This article examines the cost-effectiveness of three different PD-L1 testing methods used to guide immunotherapy for patients with advanced non-small-cell lung cancer in China. The goal is to determine which testing method provides the best value in terms of cost and effectiveness.
What were the results?
The study found that the VENTANA PD-L1 (SP263) Assay is more cost-effective compared with the Dako PD-L1 IHC 22C3 assay and the Dako 22C3 antibody concentrate. The VENTANA assay resulted in a higher percentage of patients being accurately diagnosed and treated, and it provided better quality-adjusted life years at a lower cost.
What do the results mean?
The results suggest that using the VENTANA PD-L1 (SP263) Assay for guiding immunotherapy in advanced non-small-cell lung cancer patients in China is a more economical and effective choice. This assay allows for a broader range of treatment options and improves patient outcomes by ensuring more accurate diagnoses.
Background
Lung cancer is the leading cause of morbidity and mortality among all malignancies in China, with approximately 1,060,600 new cases and 733,300 lung cancer-related deaths reported by the National Cancer Center [1]. Non-small-cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer patients, with 70% of NSCLC diagnoses occurring at advanced stages [2,3]. In recent years, immunotherapy, particularly inhibitors targeting programmed death-1 (PD-1)/programmed death-ligand 1 (PD-L1) checkpoints, has achieved significant breakthroughs in lung cancer treatment, resulting in notable survival benefits. The National Health Commission of the People's Republic of China (NHCPRC) guideline recommends immunotherapy as a first-line treatment for advanced NSCLC patients with high PD-L1 expression levels (tumor proportion score [TPS] ≥50% or tumor cells [TC] ≥50%) [4]. According to Chinese Expert Consensus on Standards of PD-L1 Immunohistochemistry (IHC) Testing for NSCLC to identify patients likely to benefit from PD-1/PD-L1 inhibitors, IHC is an effective and the most widely used method to assess PD-L1 expression in tumor tissue [5].
The clinical implementation of PD-L1 testing is complex. Different PD-1/PD-L1 inhibitors were originally developed with specific IHC assays, leading to a one-drug, one-diagnostic paradigm. This creates challenges for pathology labs regarding workflow and resource management. Different PD-1/PD-L1 inhibitors corresponds to different PD-L1 clones and platforms; thus, each requires specific PD-L1 IHC testing assays. When using assays with different clones to test PD-L1 expression in NSCLC tumor tissue, variations in results can occur due to differences in staining performance and other factors. In addition, the intra-assay consistency of the results can vary significantly depending on the antibody concentrate and assay used [6]. Therefore, the selection of assays can affect the sensitivity and specificity of PD-L1 testing in NSCLC patients, potentially leading to variations in diagnostic accuracy. This, in turn, may affect the selection of treatment regimens, ultimately impacting therapeutic outcomes and overall treatment costs. As such, excellent testing performance is critical for guiding appropriate selections of clinical medication and predicting patient prognosis. The Blueprint study is known as the pivotal investigation into the comparability of various IHC assays in both clinical and real-world settings. The Blueprint study found that while three PD-L1 IHC assays (SP263, 22C3 and 28-8) yielded largely concordant results, one assay (SP142) identified significantly fewer PD-L1-positive tumors than others. Such findings highlight the impact of assay variability on patient selection for immunotherapy and underscore the importance of choosing an appropriate PD-L1 test [7].
In China, several PD-L1 IHC testing assays have been approved for the use in guiding immunotherapy in NSCLC patients. VENTANA PD-L1 (SP263) Assay, Dako PD-L1 IHC 22C3 assay, and Dako 22C3 antibody concentrate will be the major PD-L1 IHC testing assays used as companion or complementary diagnostics for the immunotherapy that targets PD-1/PD-L1 in China market. This study aims to evaluate the cost-effectiveness of these three PD-L1 testing assays and provide evidence-based guidance for their clinical selection, considering testing costs, treatment costs and clinical benefit to patients. This study is, to our knowledge, one of the first to compare different PD-L1 diagnostic assays in terms of cost-effectiveness for NSCLC treatment in China, addressing a critical gap in current literature and providing novel insights for precision medicine strategies.
Materials & methods
Study design
This study employs a decision tree model to evaluate the cost and effectiveness of PD-L1 testing in guiding immunotherapy for NSCLC patients from the Chinese healthcare system perspective. Effectiveness outcomes were measured by the percentage of patients accurately diagnosed and treated, as well as quality-adjusted life year (QALY). Costs were presented in USD, using the USD-CNY exchange rate in 2024 H1 (1 USD = 7.24 CNY [Bank of China, exchange rate, available at: https://www.boc.cn/sourcedb/whpj/]).
The incremental cost-effectiveness ratio (ICER) is a widely used indicator in health economics that quantifies the average incremental cost required to achieve 1 additional unit of health benefit. A willingness to pay (WTP) value is often established by decision-makers as the ICER threshold to reflect the maximum amount a health system is willing to pay for that extra unit of benefit. An intervention is considered cost-effective when the ICER falls below this threshold. This study adopts China’s Gross Domestic Product (GDP) per capita in 2023 ($12,681) as the ICER threshold, a standard practice in many countries.
The time horizon was based on outcomes data from the KEYNOTE-024 and IMpower 110 clinical trial [8,9], where median treatment duration and median progression-free survival (mPFS) for advanced NSCLC patients were both under 12 months. Most of the patients would have progressed in 12 months this duration was deemed appropriate, especially since the study did not consider second-line treatments. A 12-month horizon is sufficient to simulate the disease progression of the NSCLC patients and capture the effectiveness and cost of PD-L1 testing accuracy. Moreover, cost and effectiveness simulation were conducted using Microsoft Excel 2016 version.
Expert interviews
Clinical and pathological experts in the field of NSCLC were interviewed to discuss the topics including the PD-L1 testing process, current clinical treatment patterns, healthcare resource utilization and clinical outcomes in China. The study conducted interviews with chief doctors or deputy chief doctors from the pathology, medical oncology and surgical oncology departments of seven leading national cancer centers and tertiary-level hospitals in major metropolitan areas, including Wuhan and Shanghai. These experts possess extensive clinical experience and specialized knowledge, making the interview results both representative and scientifically sound.
Model structure
A decision tree model, as shown in Figure 1, was constructed based on the NSCLC diagnosis and treatment guidelines in China and expert interviews [10,11]. This model used Ventana PD-L1 IHC SP263 assay as the intervention, with Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate assay as controls. Advanced NSCLC Patients received different treatments depending on their PD-L1 test results. A high PD-L1 expression was defined as TPS/TC ≥ 50% for advanced NSCLC patients [4]. If PD-L1 expression was high, the treatment options for the Ventana PD-L1 IHC SP263 assay group included atezolizumab monotherapy, pembrolizumab monotherapy, or chemotherapy alone. As the Dako PD-L1 IHC 22C3 assay was only approved for guiding pembrolizumab therapy, the treatment options for the Dako PD-L1 IHC 22C3 assay or Dako 22C3 antibody concentrate groups were limited to pembrolizumab therapy or chemotherapy alone. If TPS/TC < 50%, patients received chemotherapy. At the end of the decision tree, patients were classified into three states: progression-free, progression or death.
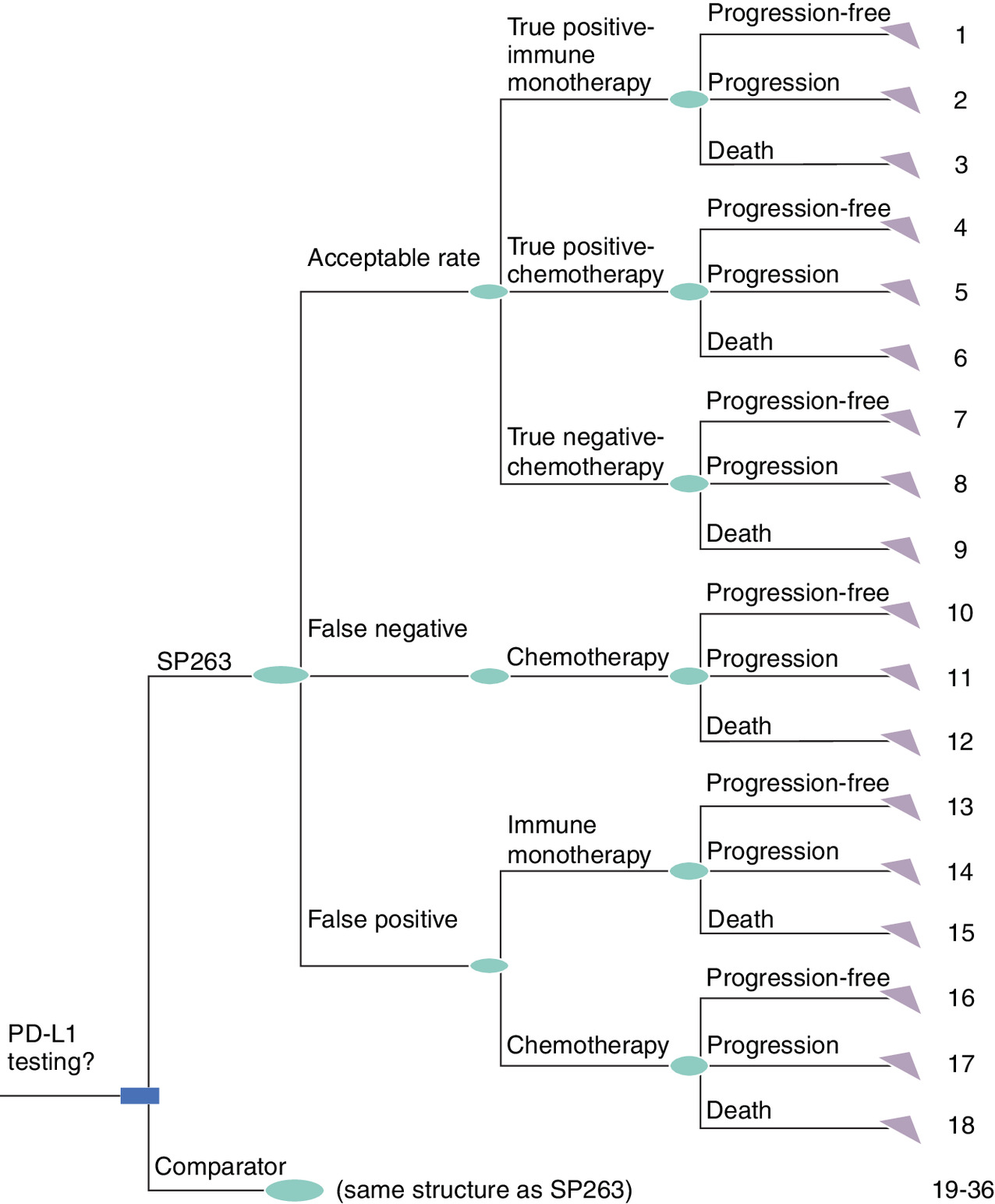
Figure 1. Decision tree model for PD-L1 testing guided immunotherapy in advanced non-small-cell lung cancer patients.
Acceptable rate: including true positive and true negative results, serving as a comprehensive indicator of sensitivity and specificity; reference testing methods included: Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate.
Model parameters
The key parameters and data sources in the model are shown in Table 1.
| Parameters | Values | Data sources | Ref. |
|---|---|---|---|
| Diagnostic performance | |||
| VENTANA PD-L1 (SP263) Assay acceptable rate | 90.55% | NordiQC, PD L1(Lung) Assessment Run C1∼C5(2017∼2019) | [12] |
| Dako PD-L1 IHC 22C3 assay acceptable rate | 85.81% | ||
| Dako 22C3 antibody concentrate acceptable rate | 75.63% | ||
| VENTANA PD-L1 (SP263) Assay false positive, false negative | 1.32%, 8.13% | ||
| Dako PD-L1 IHC 22C3 assay false positive, false negative | 1.98%, 12.21% | ||
| Dako 22C3 antibody concentrate false positive, false negative | 3.40%, 20.97% | ||
| Proportion of patients with positive PD-L1 expression | |||
| Proportion of advanced NSCLC patients with positive PD-L1 expression (TPS/TC ≥50%) | 23.76% | Qiang Zheng et al. (2021) | [13] |
| Proportion of drug treatment | |||
| Proportion of advanced NSCLC patients receiving chemotherapy after positive PD-L1 Testing | 19% | Expert interviews | |
| Proportion of advanced NSCLC patients treated with Atezolizumab and Pembrolizumab after positive PD-L1 Testing (TPS/TC ≥50%) | 32%: 68% | ||
| Clinical parameters | |||
| mPFS in advanced NSCLC patients treated with Atezolizumab monotherapy | 8.2 months | IMPOWER 110 | [8] |
| mPFS in advanced NSCLC patients treated with chemotherapy | 5.0 months | IMPOWER 110 | |
| mPFS in advanced NSCLC patients treated with Pembrolizumab monotherapy | 10.3 months | KEYNOTE 024 | [9] |
| mPFS in advanced NSCLC patients treated with chemotherapy | 6.0 months | KEYNOTE 024 | |
| Cost parameters (USD) | |||
| Testing cost | |||
| PD-L1 testing cost | $200 | Median price charges for medical services by province in China | |
| Drug treatment cost | |||
| Atezolizumab price (1200 mg) | $4518 | China Tendering Drugs Database | |
| Pembrolizumab price (100 mg) | $2468 | China Tendering Drugs Database | |
| BSC cost (3 weeks) | $260 | Ping Chen et al. 2022 | [14] |
| Cisplatin (10 mg) | $1 | China Tendering Drugs Database | |
| Carboplatin (50 mg) | $9 | China Tendering Drugs Database | |
| Pemetrexed (100 mg) | $43 | China Tendering Drugs Database | |
| Irinotecan (10 mg) | $31 | China Tendering Drugs Database | |
| Gemcitabine (200 mg) | $6 | China Tendering Drugs Database | |
| Docetaxel (20 mg) | $20 | China Tendering Drugs Database | |
| Adverse events administration costs | |||
| Anemia | $886 | Gu X et al. (2019) | [15] |
| Fatigue | $103 | Wu B et al. (2012) | [16] |
| Pneumonia | $344 | Liu X et al. (2021) | [17] |
| Thrombocytopenia | $1335 | Tang Y et al. (2023) | [18] |
| Neutropenia | $483 | Shi F et al. (2021) | [19] |
| Healthcare resource utilization costs | |||
| Complete blood count | $1 | Median price charges for medical services by province in China | |
| Comprehensive metabolic panel | $26 | ||
| Chest CT | $24 | ||
| MRI scan | $58 | ||
| PET-CT | $909 | ||
| Ultrasound scan | $4 | ||
| Whole body bone scan | $62 | ||
| Tumor markers | $32 | ||
| Health utility | |||
| Disease-free survival/Progression-free period utility | 0.8095 | Nafees Beenish et al. 2017 | [20] |
| Progression period utility | 0.3210 | ||
| Anemia disutility | 0.0735 | NICE guide (TA428) | [21] |
| Fatigue disutility | 0.0734 | NICE guide (TA428) | [21] |
| Pneumonia disutility | 0.0850 | NICE guide (TA428) | [21] |
| Thrombocytopenia disutility | 0.0053 | Zhang H et al. (2021) | [22] |
| Neutropenia disutility | 0.0900 | Nafees B et al. (2008) | [23] |
Diagnostic performance
The acceptable rate, which includes both true positives and true negatives, serves as a comprehensive indicator of sensitivity and specificity. The acceptable rate data for VENTANA PD-L1 (SP263) Assay, Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate were derived from five studies on the accuracy of PD-L1 IHC testing in lung cancer tissue samples conducted by Nordic Immunohistochemical Quality Control (NordiQC) from 2017 to 2019 [12]. However, the NordiQC studies did not report individual false-positive and false-negative rates for VENTANA PD-L1 (SP263) Assay, Dako PD-L1 IHC 22C3 assay, and Dako 22C3 antibody concentrate, but only an aggregated proportion of false positive and false negative. In the absence of public data, both domestically and internationally, this study estimated the false positive and false negative rates for each of the three testing methods based on the proportion of false positive/false negative and the acceptance rate data for VENTANA PD-L1 (SP263) Assay, Dako PD-L1 IHC 22C3 assay, and Dako 22C3 antibody concentrate reported by NordiQC.
Proportion of patients with positive PD-L1 expression
The proportion of advanced NSCLC patients with positive PD-L1 expression (TPS/TC ≥ 50%) was derived from a large, multicenter, real-world study conducted in China [13], which included 6295 NSCLC samples and was considered highly representative.
Treatment regimens proportion
Patients received different treatment regimens based on PD-L1 test results. The proportions of advanced NSCLC patients receiving chemotherapy, atezolizumab monotherapy, and pembrolizumab monotherapy in the VENTANA PD-L1 (SP263) Assay group were derived from clinical expert interviews.
Disease progression & death
Based on the health status of patients at the study end point, three statuses were identified: progression-free, progression and death. mPFS data were used to indicate the status of disease progression and guide second-line treatment decision in advanced NSCLC patients, while overall survival (OS) data were used to represent their survival status. mPFS data for patients with advanced NSCLC was obtained from the IMPOWER 110 and KEYNOTE 024 trials. PFS rates at the study end point (1 year) were extracted based on the PFS curves from these clinical trials. For patients with progression, it was assumed that the disease had not progressed before mPFS and had progressed after mPFS, with second-line treatment given after progression. For advanced NSCLC patients, if the first-line treatment was immunotherapy, chemotherapy was used after progression; if the first-line treatment was chemotherapy, best supportive care (BSC) was used after progression.
PD-L1 testing costs
Due to variations in pricing standards for medical services across different provinces in China, this study calculated the cost of PD-L1 testing based on the median price derived from 15 provinces and cities (data cut off: May 2023). The pricing data were obtained from either official medical service prices or hospital-specific pricing. Expert interviews were conducted to validate the cost of PD-L1 testing.
Drug treatment costs
Healthcare resource utilization
Examinations included complete blood count, comprehensive metabolic panel, chest CT, MRI, PET-CT, ultrasound, whole body bone scan, tumor marker tests, etc. The unit prices for each examination and test item were derived from the provincial medical service price manuals and verified through expert interviews; the frequency of examinations was based on expert interviews.
Adverse events
Adverse events (AEs) ≥ grade 3 and with high incidence rates were included. The AE rate for advanced NSCLC was derived from the IMPOWER110 and KEYNOTE-024 trials. The costs of AE management were derived from relevant Chinese literature in the context of the Chinese population.
Health utilities
To estimate the total QALYs, the survival time was adjusted by health-related quality of life. Health utilities were based on the status of the patients during treatment, and divided into utilities for progression-free survival and progression. Additionally, the study also considered the AE disabilities that occur during treatment. All utility data were obtained from the literature.
Sensitivity analysis
This study conducted a one-way sensitivity analysis (OWSA) to identify the factors with the greatest impact on the results by varying the parameters by ±20%. Furthermore, the study also conducted a probabilistic sensitivity analysis (PSA) to further test the robustness of the base case results. In the PSA, cost parameters followed gamma distributions, and utility parameters and diagnostic efficacy parameters followed beta distributions. The impact of all parameter variations on the results was analyzed through 1000 Monte Carlo simulations.
Results
Base case results
The base case results indicated that in advanced NSCLC patients, VENTANA PD-L1 (SP263) Assay, with higher sensitivity and specificity compared with the Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate, resulted in more accurate diagnoses and a higher proportion of patients receiving the appropriate treatment (86.46%, 81.93% and 72.21%, respectively). Compared with the Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate for guiding pembrolizumab monotherapy treatment only, VENTANA PD-L1 (SP263) Assay is eligible for multiple immune monotherapy regimens such as atezolizumab monotherapy and pembrolizumab monotherapy for patients with high PD-L1 expression (TPS/TC ≥ 50%). Consequently, the total cost for patients in the VENTANA PD-L1 (SP263) Assay group was lower due to the diversity of medication choices (Table 2). Overall, VENTANA PD-L1 (SP263) Assay had lower testing costs, higher percentage of patients receiving the correct diagnosis and treatment, and higher QALYs, making it a more cost-effective option with a higher net benefit compared with the Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate.
| Testing methods | Cost (USD) | Percentage of successfully diagnosed and treated | Incremental percentage of successfully diagnosed and treated | Effectiveness (QALY) | Incremental cost | Incremental effectiveness (ΔQALY) | ICER (Δcost/ΔQALY) |
|---|---|---|---|---|---|---|---|
| VENTANA PD-L1 (SP263) Assay | $8031 | 86.46% | 0.4693 | ||||
| Dako PD-L1 IHC 22C3 assay | $8501 | 81.93% | 4.53% | 0.4546 | -$470 | 0.0147 | VENTANA PD-L1 (SP263) Assay assay is cost-effective |
| Dako 22C3 antibody concentrate | $8452 | 72.21% | 14.25% | 0.4524 | -$421 | 0.0168 | VENTANA PD-L1 (SP263) Assay assay is cost-effective |
Sensitivity analysis results
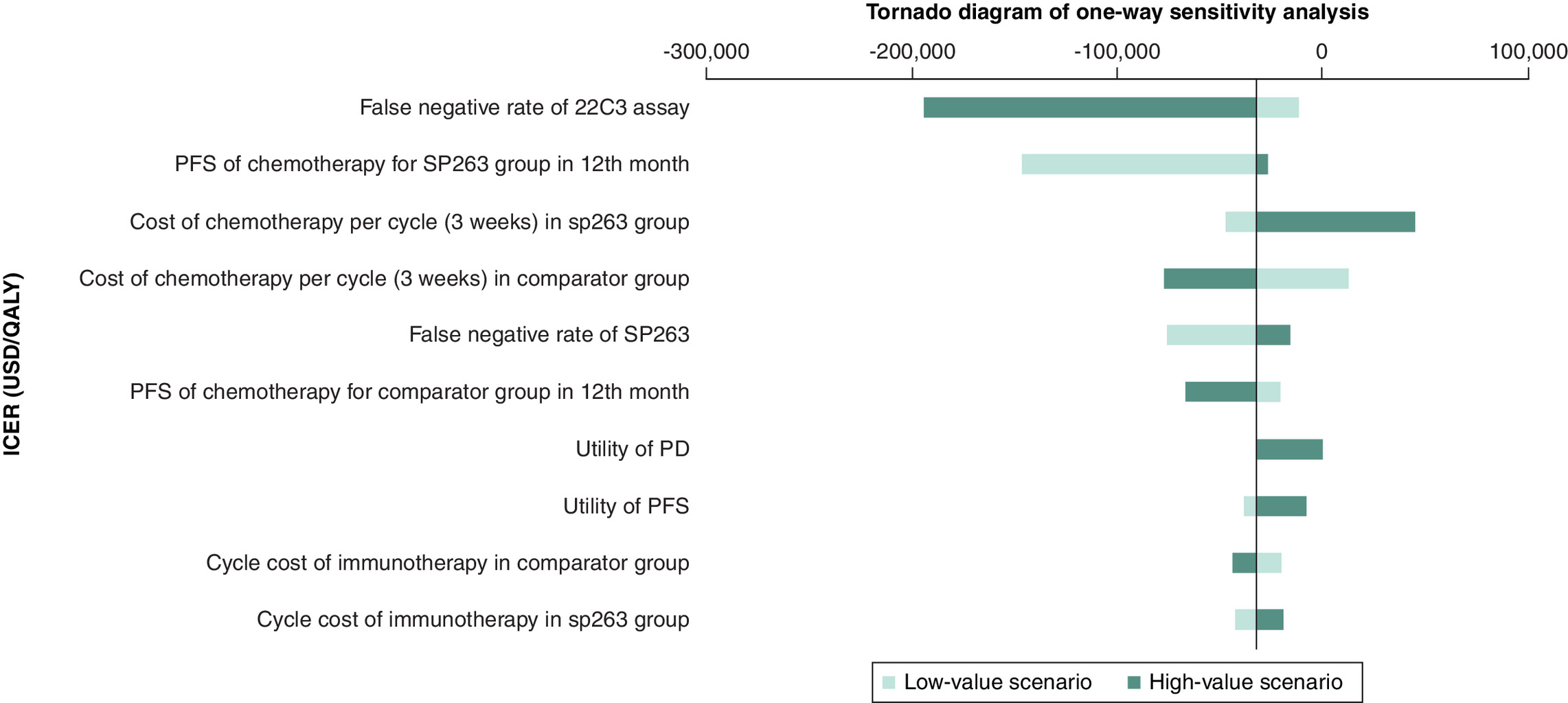
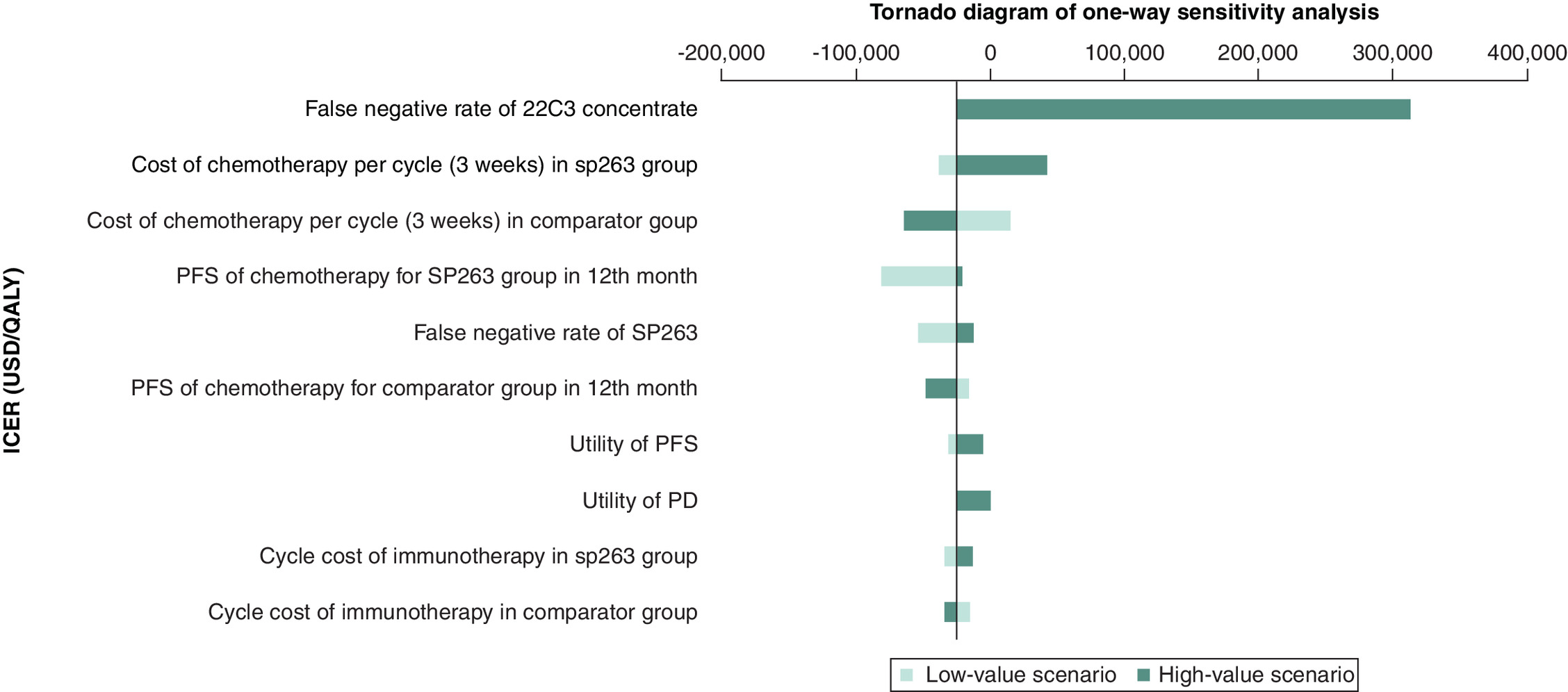
For advanced NSCLC patients, the OWSA of VENTANA PD-L1 (SP263) Assay compared with Dako PD-L1 IHC 22C3 assay (Figure 2) and Dako 22C3 antibody concentrate (Figure 4) revealed that the false negative rate of 22C3 assay or 22C3 antibody concentrate had the largest impact on the results. The tornado diagrams illustrate the influence of individual parameters on the ICER, with the length of each bar represents how much the ICER shifts when a parameter is varied by ±20%. When the parameters were varied by ±20%, the VENTANA PD-L1 (SP263) Assay remained cost-effective compared with Dako PD-L1 IHC 22C3 assay, with the cost per one additional QALY significantly below one-time GDP per capita threshold.
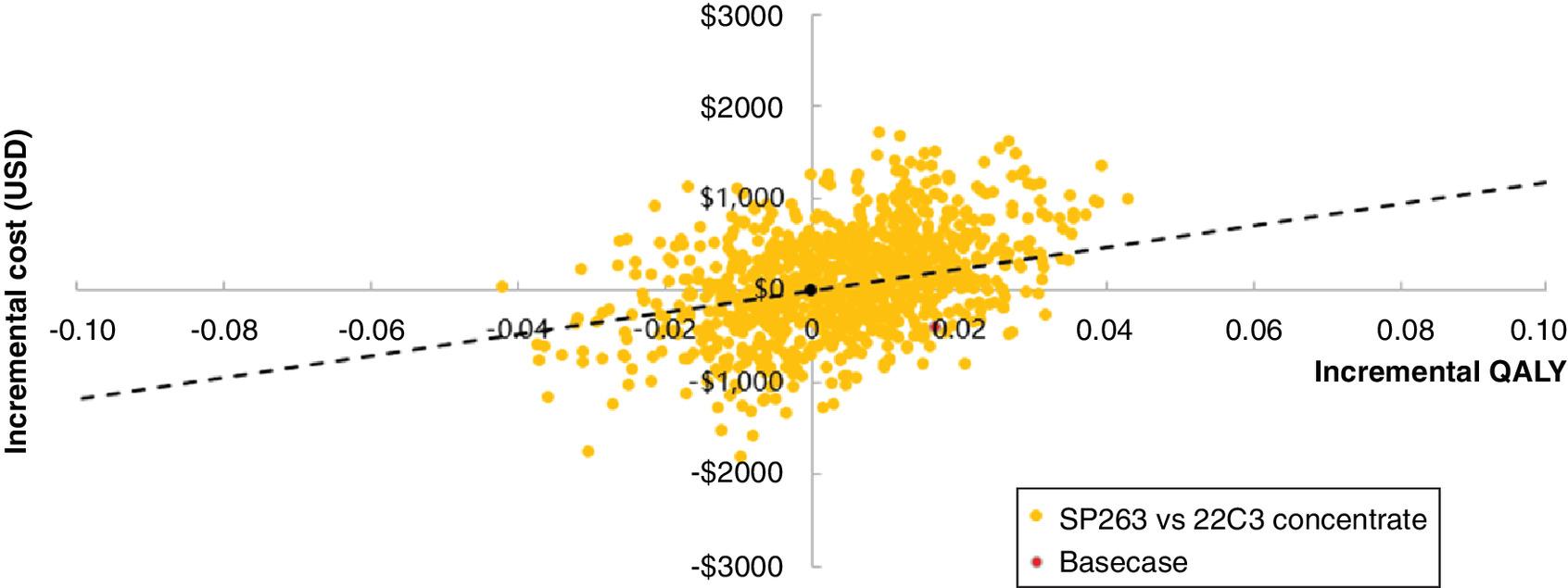
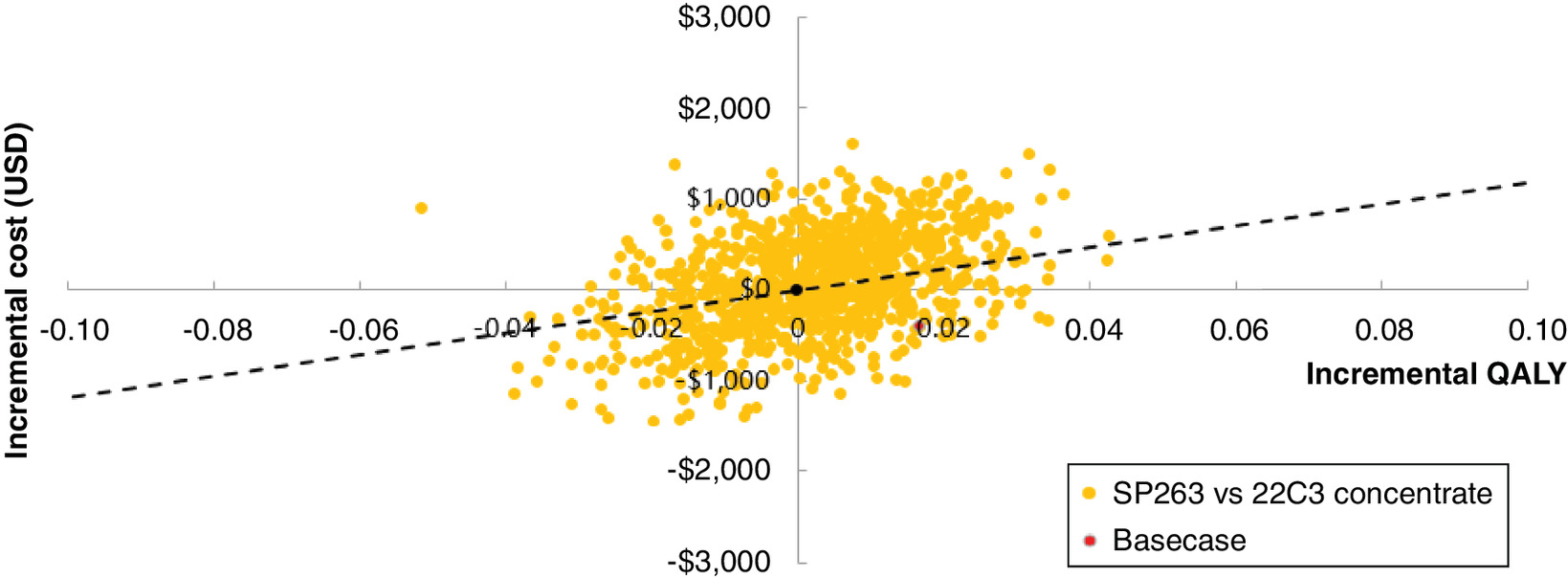
In the scatter plot, each point represents a simulation. Points located in the southeast quadrant indicate a more cost-effective strategy – one that is both more effective and less costly. The position of these points relative to the WTP threshold line determines whether the strategy falls within the acceptable WTP range. The PSA results demonstrated that the probability of VENTANA PD-L1 (SP263) Assay being cost-effective exceeded 50% compared with Dako PD-L1 IHC 22C3 assay (Figure 3) and Dako 22C3 antibody concentrate (Figure 5), which reinforce the robustness of the base-case conclusion in favor of the Ventana assay.
Discussion
IHC serves as a reliable and effective method for assessing PD-L1 expression in tumor tissues, providing predictive value for the efficacy of PD-1/PD-L1 inhibitors. This study calculated the costs and health outcomes of different PD-L1 IHC testing assays employed for and guiding immunotherapy in NSCLC patients using a decision tree model, further demonstrating the economic value of IHC assays. The results showed that VENTANA PD-L1 (SP263) Assay enhanced the sensitivity and specificity of PD-L1 testing, thereby reducing misdiagnosis and increasing the proportion of patients accurately diagnosed and treated. Additionally, for patients with advanced NSCLC, VENTANA PD-L1 (SP263) Assay can guide multiple PD-1/PD-L1 immune checkpoint inhibitors (ICIs) monotherapies, offering a broader range of treatment options. When compared with Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate which only guide a single immunotherapy treatment, VENTANA PD-L1 (SP263) Assay emerges as a cost-effective option. This finding aligns with other cost-effective studies over the world. For example, a cost-effectiveness study comparing in vitro diagnostic with laboratory developed test showed that although the in vitro diagnostic was slightly more expensive, it was more cost-effective and significantly more accurate for guiding immunotherapy in patients with positive PD-L1 expression. This increased the likelihood of patients receiving appropriate treatment and maximized health benefits [26]. Another cost-effectiveness study in Brazil compared the clinical and economic impact of two PD-L1 assays, SP142 versus 22C3, and found that SP142 assay is likely to improve PFS and generate cost savings [27].
In addition, our study found that the drug cost of immunotherapies and chemotherapy significantly impacted the ICER results. Similar observations were reported in several cost-effectiveness studies on the first-line treatment of advanced NSCLC. Studies from Swedish and USA demonstrated that immunotherapy is cost-effective as the first-line treatment for metastatic NSCLC expressing high levels of PD-L1 when comparing pembrolizumab with chemotherapy [28,29]. A study in Hong Kong, China, also found immunotherapy cost-effective under a threshold of three-times the per capita GDP [30]. However, these studies did not consider the impact of PD-L1 testing on the health outcome results. A study by Wan et al. considered both the PD-L1 testing results and the differences in the selection of subsequent treatment plans, and compared the cost-effectiveness of different testing strategies in both China and the United States. The study showed that compared with chemotherapy, the pembrolizumab-chemotherapy combination treatment of NSCLC is not cost-effective in the US and Chinese healthcare systems at the WTP threshold of $100,000/QALY for the US and $27,351/QALY for China, but using PD-L1 test for patient selection could improve the cost-effective probabilities of immunotherapy for NSCLC [31].
A unique feature of our study is that when using different PD-L1 testing assays, the corresponding immunotherapy selection option varies. After careful matching between the PD-L1 testing assay and subsequent immunotherapy, our study indicated that the VENTANA PD-L1 (SP263) Assay testing assay is more cost-effective compared with other testing assays.
The study was subject to the following limitations. First, the accuracy data for the VENTANA PD-L1 (SP263) Assay, Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate were derived from research reports of NordiQC. There was a notable absence of representative domestic statistical data in China, which should be further enriched in future research. Furthermore, false positive and false negative data for each of the three testing methods were not publicly reported, and were therefore estimated based on the aggregated proportion of false-positive and false-negative rates reported in the NordiQC’s reports, combined with the acceptable rates of the three testing methods, respectively. Our analysis may also oversimply the multifactorial nature of diagnostic accuracy, as inter-laboratory reproducibility and inter-observer variability are critical factors in clinical practice. These were not explicitly modeled, representing a limitation. To mitigate the uncertainty of data estimation, expert interviews were conducted in this study to verify the value, but further evaluation can be performed when relevant data becomes available in the future.
Second, advanced NSCLC patients with false positive results are treated with atezolizumab or pembrolizumab monotherapy. According to clinical experts interviews, patients with low PD-L1 expression response poorly to targeted treatment. Therefore, the actual efficacy of these treatments in patients was assumed to be equivalent to that of chemotherapy in the study due to limited data availability. This may potentially lead to an underestimation of the efficacy of immunotherapy in patients with false-positive results. Although the number of affected patients was small (<2%), more data are needed in the future to further validate the study results.
Finally, this study evaluated the costs and health outcomes to patients over a one-year time horizon. As it used the proportion of patients correctly diagnosed and treated as a measurement of health outcomes, it may not comprehensively reflect the long-term clinical benefits to patients. Future research could dive deeper into the cost-effectiveness in long-term scenarios (e.g., 3 years, 5 years, or life time).
Conclusion
Effective testing of biomarkers to accurately identify the population that will benefit is a key aspect of precision treatment. PD-L1 has been widely used as an efficacy predictive biomarker to guide the use of ICIs in the NSCLC treatment [29]. VENTANA PD-L1 (SP263) Assay, as a cost-effective PD-L1 assay, can be used to identify the group that will benefit most from immunotherapy and to predict patient prognosis [5,6].
In conclusion, this study demonstrated that VENTANA PD-L1 (SP263) Assay was a cost-effective PD-L1 assay to guide immunotherapy in advanced NSCLC patients, offering higher QALYs at lower costs compared with the Dako PD-L1 IHC 22C3 assay and Dako 22C3 antibody concentrate. From a policy perspective, the finding suggests that healthcare decision-makers in China should consider encouraging the use of accurate, validated assays as it yields better patient outcomes while at lower costs. For instance, clinical guidelines and hospital protocols may be updated to prefer the VENTANA PD-L1 (SP263) Assay for PD-L1 testing in advanced NSCLC. Standardizing PD-L1 testing around a high-performance, cost-effective assay can enhance the overall value of NSCLC treatment and ensure patients are accurately identified for the most appropriate therapies.
Despite limitations related to data availability and assumptions regarding false positive cases, VENTANA PD-L1 (SP263) Assay presents an economically viable option by providing a broader range of treatment choices. This study served as a scientific foundation for selecting cost-effective diagnostics and ICIs monotherapy plans for NSCLC patients in China, thereby advancing the development of precision diagnosis and treatment of NSCLC in China. Ultimately, this work supports the advancement of precision diagnosis and sustainable cancer care in China.
Summary points
•
The study assesses the cost-effectiveness of three common PD-L1 testing methods for advanced non-small-cell lung cancer (NSCLC) patients in China.
•
The study used a decision tree model to simulate costs and effectiveness from a healthcare system perspective.
•
The VENTANA PD-L1 (SP263) assay was found to be the most cost-effective option compared with the Dako PD-L1 IHC 22C3 assay and the Dako 22C3 antibody concentrate.
•
The VENTANA PD-L1 (SP263) assay resulted in a higher percentage of accurately diagnosed and treated patients and provided better quality-adjusted life years at a lower cost.
•
Sensitivity analyses confirmed the robustness of the base-case results.
•
Accurate PD-L1 testing is essential for guiding effective immunotherapy treatments.
•
The findings support the use of the VENTANA PD-L1 (SP263) Assay in clinical practice for advanced NSCLC patients in China.
•
The study highlights the importance of selecting cost-effective diagnostics to enhance precision treatment in NSCLC.
Author contributions
F Zhou and Y Li were responsible for study methodology, data interpretation, manuscript writing and providing medical advisory. J Ming was responsible for the study execution, literature review, data acquisition and analysis. C Zhou and Y Chen were responsible for study design, quality control, providing medical and health economics advisory, manuscript review and final approval.
Acknowledgments
The authors thank the oncologists and pathologists participating in this study for providing important suggestions.
Financial disclosure
This study was funded by Roche Diagnostics (Shanghai) Co., Ltd. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state this article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Data sharing statement
All data generated and analyzed during this study are included in this manuscript. Datasets are available through the corresponding author on reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Han B, Zheng R, Zeng H et al. Cancer incidence and mortality in China, 2022. J. Natl Cancer Cent. 4(1), 47–53 (2024).
2.
Liu G, Pei F, Yang F et al. Role of autophagy and apoptosis in non-small-cell lung cancer. Int. J. Mol. Sci. 18(2), 367 (2017).
3.
Goldstraw P, Ball D, Jett JR et al. Non-small-cell lung cancer. Lancet 378(9804), 1727–1740 (2011).
4.
National Health Commission of the People's Republic of China. National guidelines for diagnosis and treatment of lung cancer 2022 in China (English version). Chin. J. Cancer Res. 34(3), 176–206 (2022).
5.
Chinese expert consensus on standards of PD-L1 immunohistochemistry testing for non-small cell lung cancer. Chin. J. Lung Cancer 23(9), 733–740 (2020).
6.
Expert consensus on PD-L1 expression testing in non-small-cell lung cancer in China. Chin. J. Oncol. 42(7), 513–521 (2020).
• This consensus highlights the importance of PD-L1 assay selection for guiding appropriate clinical medication and predicting patient prognosis.
7.
Tsao MS, Kerr KM, Kockx M et al. PD-L1 immunohistochemistry comparability study in real-life clinical samples: results of Blueprint Phase 2 Project. J. Thorac. Oncol. 13(9), 1302–1311 (2018).
• This blueprint study is the key paper that changed the paradigm regarding PD-L1 testing in non-small-cell lung cancer (NSCLC) patients.
8.
Jassem J, de Marinis F, Giaccone G et al. Updated overall survival analysis from IMpower110: atezolizumab versus platinum-based chemotherapy in treatment-naive programmed death-ligand 1-selected NSCLC. J. Thorac. Oncol. 16(11), 1872–1882 (2021).
• Provides median progression-free survival (mPFS) data in advanced NSCLC patients treated with atezolizumab monotherapy and chemotherapy as important clinical parameters in model.
9.
Reck M, Rodríguez-Abreu D, Robinson AG et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 375(19), 1823–1833 (2016).
• Provides mPFS data in advanced NSCLC patients treated with pembrolizumab monotherapy and chemotherapy as important clinical parameters in model.
10.
Chinese Society of Clinical Oncology. Guidelines of Chinese Society of Clinical Oncology for non-small cell lung cancer 2023. People's Medical Publishing House, China (2023).
• This clinical guideline offers insights on clinical diagnosis and treatment pathway for decision tree model structuring.
11.
Chinese Medical Association. Guideline for clinical diagnosis and treatment of lung cancer (2023 edition). Natl Med. J. China 103(27), 2037–2074 (2023).
12.
NordiQC. PD-L1 (lung) assessment run C1–C5 (2017–2019). NordiQC. (2019). Available from: https://www.nordiqc.org/epitope.php?id=107
• Provides the study data of diagnostic performance for three PD-L1 testing methods.
13.
Zheng Q, Huang Y, Zeng X et al. Clinicopathological and molecular characteristics associated with PD-L1 expression in non-small cell lung cancer: a large-scale, multi-center, real-world study in China. J. Cancer Res. Clin. Oncol. 147(5), 1547–1556 (2021).
14.
Chen P, Yang Q, Li Y, Jing X, Chen J. Cost-effectiveness analysis of adjuvant therapy with atezolizumab in Chinese patients with stage IB–IIIA resectable NSCLC after adjuvant chemotherapy. Front. Oncol. 12, 894656 (2022).
15.
Gu X, Zhang Q, Chu YB et al. Cost-effectiveness of afatinib, gefitinib, erlotinib and pemetrexed-based chemotherapy as first-line treatments for advanced non-small cell lung cancer in China. Lung Cancer 127, 84–89 (2019).
16.
Wu B, Dong B, Xu Y et al. Economic evaluation of first-line treatments for metastatic renal cell carcinoma: a cost-effectiveness analysis in a health resource-limited setting. PLoS ONE 7(3), e32530 (2012).
17.
Liu X, Chen W. Pharmacoeconomic evaluation of osimertinib in the first-line treatment of locally advanced or metastatic NSCLC with an EGFR mutation. World Clin. Drugs 42(2), 135–142 (2021).
18.
Tang Y, Zhao M, Tang W. Pharmacoeconomic evaluation of sintilimab versus camrelizumab in the first-line treatment of patients with non-squamous advanced non-small cell lung cancer in China. Health Econ. Res. 40(2), 34–40 (2023).
19.
Shi F, Jin M, Wang Z, Meng R, Rui M, Ma A. Cost-utility analysis of camrelizumab versus chemotherapy regimens for second-line treatment of advanced or metastatic esophageal squamous cell carcinoma. Chin. Health Econ. 40(12), 73–77 (2021).
20.
Nafees B, Lloyd AJ, Dewilde S, Rajan N, Lorenzo M. Health state utilities in non-small cell lung cancer: an international study. Asia Pac. J. Clin. Oncol. 13(5), 25–32 (2017).
21.
National Institute for Health and Care Excellence (NICE). Pembrolizumab for treating PD-L1-positive non-small-cell lung cancer after chemotherapy (NICE technology appraisal guidance TA428) (2017).
22.
Zhang H, Zhang Y, Huang C, Wang J. Cost-effectiveness analysis of trastuzumab emtansine as second-line therapy for HER2-positive breast cancer in China. Clin. Drug Investig. 41(6), 569–577 (2021).
23.
Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual. Life Outcomes 6, 84 (2008).
24.
China Charity Federation Tai Shengqi Charity Assistance Project. https://tpap.yao2000.com.cn/flow.html
25.
China Primary Health Care Foundation's Key to Life-Tumor Immunotherapy Patient Assistance Project. http://www.jksb.com.cn/html/2021/treatment_0121/168818.html
26.
Hurwitz JT, Vaffis S, Grizzle AJ, Nielsen S, Dodson A, Parry S. Cost-effectiveness of PD-L1 testing in non-small cell lung cancer using in vitro diagnostic (IVD) versus laboratory-developed test (LDT). Oncol. Ther. 10(2), 391–409 (2022).
27.
Shimabukuro Ho R, Mioti Sebastião M, Venezian de Carvalho JP, Neves T, Nussbaum M. Cost-effectiveness analysis of the SP142 versus 22C3 PD-L1 assays in the treatment of atezolizumab plus nab-paclitaxel for patients with advanced triple-negative breast cancer in the Brazilian private healthcare system. J. Med. Econ. 23(11), 1340–1344 (2020).
28.
Bhadhuri A, Insinga R, Guggisberg P, Panje C, Schwenkglenks M. Cost effectiveness of pembrolizumab vs chemotherapy as first-line treatment for metastatic NSCLC that expresses high levels of PD-L1 in Switzerland. Swiss Med. Wkly 149, w20170 (2019).
29.
Huang M, Lou Y, Pellissier J et al. Cost effectiveness of pembrolizumab vs standard-of-care chemotherapy as first-line treatment for metastatic NSCLC that expresses high levels of PD-L1 in the United States. Pharmacoeconomics 35(8), 831–844 (2017).
30.
Loong HH, Wong CKH, Leung LKS et al. Cost effectiveness of PD-L1-based test-and-treat strategy with pembrolizumab as the first-line treatment for metastatic NSCLC in Hong Kong. Pharmacoecon. Open 4(2), 235–247 (2020).
31.
Wan N, Zhang TT, Hua SH et al. Cost-effectiveness analysis of pembrolizumab plus chemotherapy with PD L1 test for the first line treatment of NSCLC. Cancer Med. 9(5), 1683–1693 (2020).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 June 2025
Accepted: 3 October 2025
Published online: 14 November 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost-effectiveness of PD-L1 testing to guide immunotherapy for patients with advanced non-small-cell lung cancer in China. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0093
Export citation
Select the citation format you wish to export for this article or chapter.