Matching-adjusted indirect comparison of ribociclib + nonsteroidal aromatase inhibitor versus abemaciclib + endocrine therapy in hormone receptor-positive/HER2-negative early breast cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Ribociclib + nonsteroidal aromatase inhibitor (NSAI) and abemaciclib + endocrine therapy (ET) are approved for high-risk hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2-) early breast cancer based on data from the NATALEE and monarchE trials, respectively. No trials have directly compared efficacy and safety of adjuvant ribociclib and abemaciclib. This study compared relative efficacy and safety of adjuvant ribociclib + NSAI versus abemaciclib + ET using matching-adjusted indirect comparison (MAIC). Materials & methods: Individual patient data from NATALEE and aggregate data from monarchE were analyzed, with patients from NATALEE selected to match the key eligibility criteria of monarchE cohort 1. Unanchored MAIC was used to compare invasive disease-free survival, distant relapse–free survival, and grade ≥3 treatment-emergent adverse events between treatment arms in NATALEE versus monarchE. Cox regression was used to estimate hazard ratios pre- and post-MAIC weighting. Logistic regression was used to estimate odds ratios (ORs). Results: After weighting, the effective sample size for the ribociclib + NSAI arm of NATALEE was 448. Cox regression yielded similar invasive disease-free survival with weighted ribociclib + NSAI versus abemaciclib + ET (hazard ratio, 0.901; 95% CI: 0.678–1.197). Unweighted efficacy comparisons were consistent with the weighted approach. Lower odds (OR <1) for diarrhea, leukopenia and lymphopenia and higher odds (OR >1) for increased alanine aminotransferase and neutropenia with ribociclib + NSAI versus abemaciclib + ET were noted before and after weighting. Sensitivity analyses were consistent with the primary analysis. Conclusion: This MAIC suggests similar efficacy between ribociclib + NSAI and abemaciclib + ET but different safety profiles in the HR+/HER2- early breast cancer patient population corresponding to the monarchE cohort 1, which has implications for treatment decisions. This analysis has limitations inherent to unanchored MAIC and should be interpreted in context of the trials and with clinical judgement.
Plain language summary
What is this article about?
Most patients with breast cancer are diagnosed at an early stage. For patients with hormone receptor-positive/human epidermal growth factor receptor 2–negative (HR+/HER2-) early breast cancer (EBC), endocrine therapy (ET) has been the standard treatment in clinics. However, in many of these patients, there is a high risk of the cancer coming back even after ET. Phase III clinical trials NATALEE and monarchE have shown that when ribociclib and abemaciclib, respectively, are added to ET, patients with EBC are able to live cancer free longer. Thus, ribociclib and abemaciclib, with ET, have now been approved to treat patients with HR+/HER2- EBC who have a high risk of the cancer coming back. This study used data from NATALEE and monarchE to compare benefits of adding ribociclib and abemaciclib, respectively, to ET. As patients that are allowed to participate in different trials may have different clinical characteristics, these differences need to be adjusted for accurate comparisons.
What were the results?
Following adjustment for these differences, this study found that patients with HR+/HER2- EBC treated with ribociclib + ET were cancer free for a similar length of time as patients treated with abemaciclib + ET. Finally, patients on abemaciclib had higher risk of diarrhea and lower white blood cell counts and lymphocyte counts as side effects, while patients on ribociclib had higher risk of liver enzyme elevation and lower neutrophil counts.
What do the results mean?
While these data are not conclusive, they can be useful when deciding on a treatment course for patients with high-risk HR+/HER2- EBC.
Breast cancer (BC) was the second leading cause of global cancer incidence in 2022, comprising 11.6% of all newly diagnosed cancer cases [1]. Hormone receptor-positive/human epidermal growth factor receptor 2–negative (HR+/HER2-) subtype is the most common BC subtype (~70%) [2]. Most patients (95%) with BC are diagnosed at an early stage, with the tumor localized to the breast tissue and nearby lymph nodes [3]. Even with standard-of-care (SOC) adjuvant endocrine therapy (ET) for at least 5 years (with or without chemotherapy) for systemic treatment of HR+/HER2- early BC (EBC), risk of recurrence continues to be a concern, with recurrences peaking in the first 5 years and continuing for the following decades [4–8]. A large, retrospective real-world study (n = 7564) recently reported considerable 5-year recurrence risk in patients with positive nodal status (12.8% and 33.8% in patients with 1–3 and ≥4 positive lymph nodes, respectively) and in patients with high-risk node-negative disease (12.6%) [4].
To address this unmet treatment need among patients with high-risk HR+/HER2- EBC, cyclin-dependent kinase 4/6 inhibitors (CDK4/6is) have been investigated as an addition to SOC ET in the adjuvant setting. Two of these phase III trials of CDK4/6is in the adjuvant setting, NATALEE for ribociclib and monarchE for abemaciclib, have reported positive results [9,10]. At an interim prespecified median follow-up at 27.7 months, NATALEE reported a statistically significant invasive disease-free survival (iDFS) benefit with adjuvant ribociclib + a nonsteroidal aromatase inhibitor (NSAI; letrozole or anastrozole) versus an NSAI alone (hazard ratio, 0.75; 95% CI: 0.62–0.91; p = 0.003) in a broad population of patients with HR+/HER2- EBC at risk of recurrence (stage II/III disease irrespective of lymph node status; stage IIA T2N0 disease required grade 2 tumor with Ki-67 of ≥20% or high genomic risk; grade 3 tumor) [9]. Importantly, this iDFS benefit was sustained at a later follow-up at 44.2 months after all patients were off ribociclib (4-year landmark analysis; HR: 0.715; 95% CI: 0.609–0.840; p < 0.0001) [11]. The monarchE trial, at a median follow-up of 15.5 months, also reported a statistically significant iDFS benefit with adjuvant abemaciclib + ET versus ET (choice of letrozole [NSAI], anastrozole [NSAI], exemestane [aromatase inhibitor; AI], or tamoxifen [a selective estrogen receptor modulator; SERM]) alone (HR: 0.75; 95% CI: 0.60–0.93; p = 0.01), which was sustained at a median follow-up of 54 months (5-year efficacy outcome analysis; hazard ratio, 0.68; 95% CI: 0.60–0.77; p < 0.001) in patients with node-positive HR+/HER2- EBC [10,12]. Most patients in the monarchE (91%) trial were included based on cohort 1 criteria (≥4 positive lymph nodes or 1 to 3 positive lymph nodes with grade 3 tumor or tumor size ≥5 cm), while only 9% of patients were included based on cohort 2 criteria (1 to 3 positive lymph nodes and Ki-67 of ≥20%, tumor grade <3, and tumor size <5 cm) [12,13].
Based on patients included in NATALEE and in monarch E cohort 1, these trial data have led to regulatory approval for both ribociclib and abemaciclib, respectively, in patients with high-risk HR+/HER2- EBC in the US and EU [14–18].
Understanding the relative efficacy and safety of ribociclib + NSAI versus relevant comparators in the EBC patient population is important for many reasons. Reimbursement and market access in many regions requires submission of evidence of cost-effectiveness to reimbursement and/or health technology assessment authorities, which is based in part on the relative efficacy and safety of drugs. Such comparisons also help clinicians make shared and personalized decisions on treatment choices for patients with EBC. To date, there have been no head-to-head trials comparing ribociclib + NSAI with interventions other than NSAI alone for patients with HR+/HER2- EBC. The objective of this study was to conduct a matching-adjusted indirect comparison (MAIC) between ribociclib + NSAI and abemaciclib + ET to estimate the relative efficacy (iDFS and distant relapse–free survival [DRFS]) and safety of these two drugs in the adjuvant setting for the overlapping population from both trials. As abemaciclib is approved in the US and EU only as treatment for patients who would be eligible for cohort 1 of the monarchE trial, patients included in this cohort were the focus of the present comparison, with NATALEE patients selected for this comparison matching the cohort 1 key eligibility criteria [14,18].
Materials & methods
Systematic literature review
A systematic literature review (SLR) was conducted by searching Embase, MEDLINE and CENTRAL databases (from database inception to 25 June 2024) to identify all relevant publications assessing the relative efficacy of adjuvant treatments for HR+/HER2- EBC. The search strings used to identify the relevant literature are described in Supplementary Table 1. The SLR was performed and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Forty-four unique studies were included in the clinical SLR. While patient-level data for the Breast International Group (BIG) 1-98 study investigating tamoxifen and letrozole in the adjuvant setting were available, because this study was from 2005 and had primary end points that were defined differently from those currently used, it was not considered further in this analysis [19]. Of all studies analyzed initially, six were identified that included a population at high risk of recurrence. Different parameters were used across these studies for segregating risk categories into low, high and mixed, which included nodal status, tumor size, histological grade, Ki-67 index, age and HR status. Of the six studies that included patients with high risk of recurrence, two studies were excluded from the indirect treatment comparison (ITC) as the risk classifications were not aligned with high-risk characteristics in the target population (Supplementary Table 2). Specifically, patients in SUCCESS-C were classified as having high risk disease with tumors ≥2 cm and no requirements regarding nodal involvement [20]. In a study analyzing patients who met the inclusion criteria of the TAILORx trial, the high-risk subpopulation was characterized by presence of metastases, which was an exclusion criterion for the ITC analyses [21]. The PENELOPE-B trial of palbociclib + ET and the SWOG S1207 and UNIRAD trials of everolimus + ET were excluded because these trials failed to demonstrate clinical benefit of the tested drugs, and these drugs were thus not approved for use in the adjuvant setting [22–24].
Finally, cohort 1 of monarchE met all eligibility criteria (patients with ≥4 positive lymph nodes or 1 to 3 positive lymph nodes with either tumor size ≥5 cm or histological grade 3 disease) for the present study and had reported positive results for the comparator of interest and was, therefore, included in the ITC. In addition, access to patient-level data from the NATALEE trial allowed for selection of patients who met the cohort 1 criteria. Thus, the NATALEE trial, assessing ribociclib + NSAI versus NSAI alone, and the monarchE trial, assessing abemaciclib + ET versus ET alone, were finally considered suitable for inclusion in this ITC.
Inclusion criteria of comparator trials
This ITC used individual patient data (IPD) from the NATALEE trial (data cutoff, 29 April 2024; median follow-up, 49.6 months) and aggregate data reported for cohort 1 of the monarchE trial (data cutoff, 3 July 2023; median follow-up, 54.0 months) [12,13,17,25,26]. For context, the sample sizes and number of iDFS and DRFS events per outcome in the primary publications of these clinical trials for these data cutoffs are described in Supplementary Table 3.
The intent-to-treat (ITT) population of NATALEE included adults with high-risk node-positive and node-negative HR+/HER2- EBC. Specifically, those included in the NATALEE trial were patients with anatomic stage II or III disease regardless of nodal status; patients with stage IIA N0 (T2 N0) disease were required to have grade 3 disease, or grade 2 disease with evidence of additional high-risk features (i.e., Ki-67 of ≥20% or determination of high risk by genomic assay: Oncotype DX Breast Recurrence Score of ≥26 or high-risk scores by Prosigna/PAM50, MammaPrint or EndoPredict) [9,27]. In contrast, monarchE was composed exclusively of adult patients with high-risk node-positive HR+/HER2- EBC. Cohort 1 of monarchE included patients with ≥4 positive lymph nodes or 1 to 3 positive lymph nodes with at least one of the following features: tumor size ≥5 cm or histological grade 3 disease regardless of Ki-67 status. Cohort 2 of monarchE included patients with 1 to 3 positive lymph nodes, with Ki-67 of ≥20%, tumor grade <3, and tumor size <5 cm [10,13,28]. Table 1 provides the key eligibility criteria for the two trials from which the target populations (monarchE cohort 1-eligible patients) were compared in this MAIC.
| Characteristic | monarchE (NCT03155997) | NATALEE (NCT03701334) |
|---|---|---|
| Key inclusion criteria | ||
| Nodal involvement | Cohort 1: • ≥4 nodes; or • 1–3 nodes and ≥1 of the following: ○ Tumor size ≥5 cm ○ Grade 3 Cohort 2: • 1–3 nodes and Ki-67 ≥20%, tumor grade <3, and tumor size <5 cm (cohort 2) | Anatomic stage II (IIA with either N0 with grade 2–3 or N1; IIB) or III EBC |
| HR status | HR+ | HR+ |
| HER2 status | HER2- | HER2- |
| Disease stage | Early-stage resected invasive breast cancer without evidence of distant metastases (stage IIA [with specific characteristics], IIB, or III) | Anatomic stage II (IIA with either N0 with grade 2–3 or N1; IIB) or III EBC |
| Menopausal status | Any | Any |
| Surgery | Undergone definitive surgery for the primary breast tumor | Undergone definitive surgery for the primary breast tumor |
| Prior therapy for early disease | Up to 12 weeks of ET until randomization following the last non-endocrine therapy (surgery, chemotherapy, or radiation) | Completion of chemotherapy and radiotherapy if indicated; patients receiving standard (neo)adjuvant ET were eligible only if this treatment was initiated within 12 months of randomization |
| Key exclusion criteria | ||
| Disease stage | Metastatic disease excluded (stage IV according to AJCC, 8th edition) | Metastatic disease excluded (stage IV according to AJCC, 8th edition) |
| Prior therapy | Any prior CDK4/6 inhibitor; prior ET for breast cancer prevention (tamoxifen or AIs), raloxifene | Any prior CDK4/6 inhibitor; prior ET for breast cancer prevention (tamoxifen or AIs), raloxifene |
AI: Aromatase inhibitor; AJCC: American Joint Committee on Cancer; CDK4/6: Cyclin-dependent kinase 4/6; EBC: Early breast cancer; ET: Endocrine therapy; HER2: Human epidermal growth factor receptor 2; HR: Hormone receptor.
Cohort 1 of monarchE corresponds to the patient population in which abemaciclib + ET has received positive recommendations from the National Institute for Health and Care Excellence (NICE) and the European Medicines Agency [16,29]. Therefore, abemaciclib was approved to only be available to these patients in clinical practice, and thus cohort 1 was the focus of this indirect comparison. Patients in NATALEE who met the key eligibility criteria of monarchE cohort 1 were selected (selected NATALEE population).
Overview of the MAIC analyses
Following the SLR, the two trials (NATALEE and monarchE) considered suitable for inclusion in this ITC were compared regarding the efficacy and safety with ribociclib + NSAI versus abemaciclib + ET as adjuvant treatment for patients with high-risk HR+/HER2- EBC. A feasibility assessment, as described below, determined that an unanchored MAIC was the most appropriate approach for comparing relative efficacy (iDFS and DRFS) and safety between ribociclib + NSAI and abemaciclib + ET in the target population (monarchE cohort 1-eligible patients), which served as the primary analysis. Sensitivity analyses were performed to test the robustness of the assumptions made in the primary analysis.
Feasibility assessment
Prior to performing the ITC analyses, a feasibility assessment was conducted. The feasibility assessment considered differences in the control ET arm and differences in efficacy and safety follow-up durations between NATALEE and monarchE. The following components of ITCs were considered: pairwise meta-analysis versus network meta-analysis, anchored versus unanchored ITC approaches and application of population-adjustment methods. A pairwise meta-analysis was deemed necessary as only two trials, NATALEE and monarchE, could be included; no other trials identified by the SLR reported outcomes of interest for the target population of the ITC.
The possibility of using an anchored approach was also assessed. The NATALEE control arm comprised NSAI only (i.e., letrozole and anastrozole) while the monarchE control arm comprised NSAIs, exemestane and tamoxifen. There is evidence that the efficacy of NSAIs and exemestane are similar in EBC [30,31]. However, the results of previous meta-analyses have shown that tamoxifen has worse efficacy compared with NSAIs as adjuvant treatment for HR+/HER2- EBC [32,33]. As such, an anchored MAIC would have required restricting analysis to abemaciclib + AI, excluding patients who received tamoxifen, who comprised approximately 30% of the monarchE trial population [10]. This restriction would not reflect the fully approved indication of abemaciclib in clinical practice, thus limiting generalizability [14,17].
Finally, a comparison of the NATALEE and monarchE study eligibility criteria and baseline characteristics revealed between-study heterogeneity that would potentially bias the ITC. Moreover, the monarchE trial had narrower eligibility criteria than NATALEE and only had aggregate data published; therefore, it was necessary to select NATALEE patients who met the monarchE cohort 1 eligibility criteria. After matching NATALEE patients to monarchE (the selected NATALEE population), residual differences in many baseline characteristics were observed. These differences could bias the ITC if the characteristics were treatment effect modifiers or important prognostic factors for EBC. Unanchored ITCs assume all prognostic factors and effect modifiers are accounted for and are therefore subject to bias or confounding from differences in such characteristics between study populations [34]. Population adjustment methods such as an unanchored MAIC reduce the risk of bias due to differences in characteristics between studies and thus were chosen for this analysis. Based on these findings from the feasibility assessment, an unanchored MAIC was considered the most appropriate approach for comparing ribociclib + NSAI versus abemaciclib + ET in the target population (monarchE cohort 1-eligible patients).
Prognostic factors & effect modifiers
Characteristics that were feasible to be included in the MAIC were identified from published studies of the monarchE trial. The importance of baseline characteristics as effect modifiers or prognostic factors for efficacy was determined qualitatively and quantitatively. External clinicians were interviewed to determine the baseline characteristics that are known to be prognostic factors for efficacy in EBC, by varying degrees of influence. Each of the three clinicians interviewed were able to identify a number of factors that they considered to be relevant as prognostic factors based on their expertise and experience. The clinicians interviewed were selected based on their clinical expertise in treating BC patients and covering different regions as well as for their prior experience with health technology assessments in BC. Supplementary Table 4 shows the clinician ranking of prognostic factors by levels of ‘high importance’, ‘low importance,’ and not important (i.e., ‘—’) for a list of variables used in primary and sensitivity analyses. The identified factors generally corresponded to prognostic factors determined to be important in a prior analysis from NATALEE [35]. Conversely, confounding factors for safety outcomes are generally less established than those for efficacy. All prognostic factors identified for efficacy outcomes were thus used for weighting the IPD from the NATALEE trial for safety outcomes as well.
Using IPD from NATALEE, p-values were also generated as a tool to distinguish between treatment effect modifiers and prognostic factors using IPD from NATALEE. Treatment effect modification was assessed for each clinical characteristic based on p-value for the interaction effects with treatment using Cox proportional hazards regression of patient-level failure time data for the iDFS outcome. Cox models were specified with covariates for treatment, a given clinical characteristic, and the interaction of treatment arm with that characteristic. The p-values for the interaction terms were then used to assess whether the treatment effect with ribociclib + NSAI was modified based on an α of 0.05. A p-value > 0.05 for a characteristic suggested that there was no adequate evidence to treat it as an effect modifier on iDFS (Supplementary Figure 1). To help inform selection of effect modifiers and prognostic factors, p-values from interaction and log-rank tests were used as descriptive tools to help inform selection of effect modifiers and prognostic factors. However, these should not be interpreted as confirmatory due to the exploratory nature of the analysis.
Statistical assessments for prognostic factors were conducted based on p-values obtained from log-rank tests for iDFS outcomes in the selected NATALEE patient population, irrespective of treatment. The log-rank p-value was used to determine whether there was supporting evidence for a difference in iDFS events among the Kaplan–Meier (KM) curves with respect to the characteristic. A p-value < 0.05 suggested that the characteristic was prognostic. All quantitative assessments for treatment effect modification and prognostic factors are summarized in Supplementary Table 5.
MAIC weighting & adjustment factors used in primary & sensitivity analyses
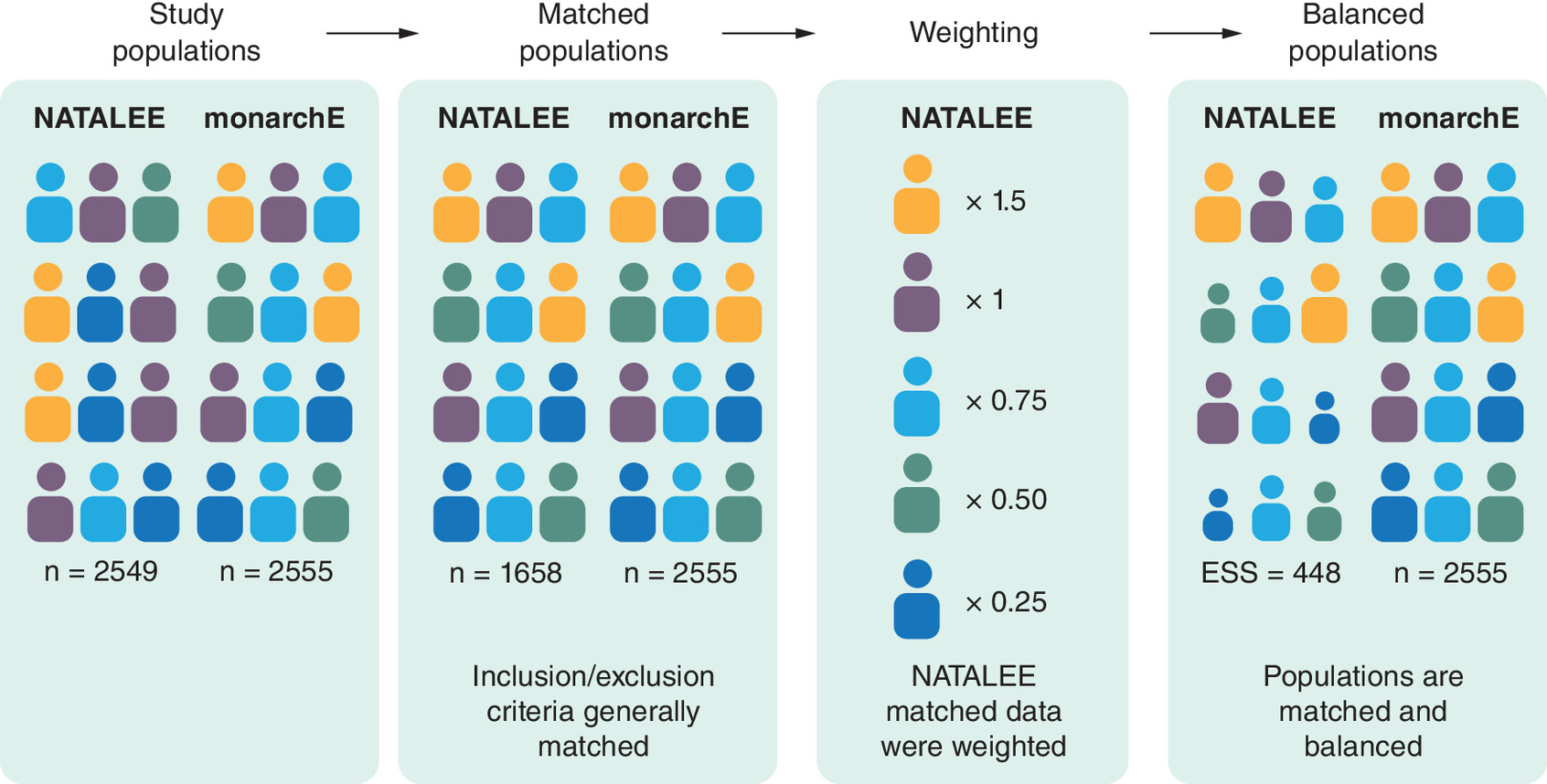
To enable MAIC, patients were weighted by inverse odds of propensity scores (which measure the probability of the patient being included in NATALEE) using available patient-level data (from NATALEE) to adjust the distribution of patient characteristics (prognostic factors or effect modifiers) to match with the aggregate monarchE data (Figure 1) [36,37]. To elaborate, the weight assigned to each patient in the selected NATALEE population was proportional to the inverse of the probability or relative likelihood of their covariates occurring in the selected NATALEE population relative to monarchE cohort 1. Weights were assigned to individual patients in the ribociclib + NSAI treatment arm and NSAI alone treatment arm such that the mean baseline characteristics in the NATALEE trial matched with the abemaciclib + ET and ET alone arms of monarchE cohort 1, respectively. Given that only aggregate data were available for monarchE, it was possible to adjust only for characteristics that were available at baseline for cohort 1 of the monarchE trial in the literature.
The primary analysis for the unanchored MAIC was conducted using all the available characteristics shown in Table 2, consistent with guidance for unanchored MAICs from NICE Decision Support Unit Technical Support Documents (DSU TSDs) 18 [34,36,37]. According to the guidance, adjusting for factors that are not prognostic does not bias the unanchored comparison, but it may reduce effective sample size (ESS) unnecessarily. The primary analysis adjusted for all variables that were indicated as having prognostic influence by clinicians, all variables that modified treatment effect based on interaction tests, all variables that were prognostic based on stratified log-rank tests and available variables without evidence of prognostic influence (Table 2).
| Characteristic | Prognostic | Effect modifier† | Included in analysis | |||||
|---|---|---|---|---|---|---|---|---|
| Clinician ranking | Log-rank test | NATALEE | monarchE | Primary‡ | SA 1§ | SA 2¶ | ||
| A | Pathologic diagnosis term | High | — | — | — | ✓ | ✓ | ✓ |
| HR status | High | Significant | — | — | ✓ | ✓ | ✓ | |
| Positive axillary lymph nodes, n | High | Significant | — | — | ✓ | ✓ | ✓ | |
| Histopathology at diagnosis | High | Significant | — | — | ✓ | ✓ | ✓ | |
| TNM stage | High | Significant | — | — | ✓ | ✓ | ✓ | |
| Pathologic tumor size, cm | High | Significant | — | Significant | ✓ | ✓ | ✓ | |
| Ki-67 index | High | — | — | — | ✓ | ✓ | ✓ | |
| B | Menopausal status | Low | — | — | — | ✓ | ✓ | |
| Age, years | Low | Significant | — | — | ✓ | ✓ | ||
| Weight, kg | Low | — | — | — | ✓ | ✓ | ||
| BMI, kg/m2 | Low | — | — | — | ✓ | ✓ | ||
| Prior chemotherapy | Low | Significant | — | — | ✓ | ✓ | ||
| Prior radiotherapy | Low | — | — | — | ✓ | ✓ | ||
| ECOG PS | Low | — | — | — | ✓ | ✓ | ||
| Tumor side | Low | — | — | — | ✓ | ✓ | ||
| C | Female sex | — | — | — | — | ✓ | ||
| Race | — | — | — | — | ✓ | |||
| Ethnicity | — | — | — | — | ✓ | |||
| Region | — | — | — | — | ✓ | |||
‘—’ indicates not important (per clinician interview) or not statistically significant at α = 0.05 (if statistical test).
The group A rows indicate characteristics for which there was a consensus among clinicians of ‘high importance’ as a prognostic factor for efficacy in EBC (consensus of high importance was defined as ≥2 clinicians ranking a given characteristic as highly important). The group B rows correspond to the factors that were deemed to have some level of importance in EBC prognosis by ≥1 clinician (i.e., ≥1 clinician indicated low importance as a prognostic factor for efficacy in EBC). The group C rows correspond to the factors that clinicians did not indicate as having important prognostic influence in EBC.
†
Based on p-value for interaction test.
‡
All available characteristics.
§
High importance based on clinician interviews.
¶
Any importance based on clinician interviews and/or statistically significant based on statistical test.
ECOG PS: Eastern Cooperative Oncology Group performance status; HR: Hormone receptor; SA: Sensitivity analysis; TNM: Tumor, node, metastasis.
Additionally, sensitivity analyses were conducted to assess the range of plausible estimates for the relative treatment effects (Table 2). Two alternative sets of MAIC weights were estimated to explore the impact of adjusting for fewer variables (i.e., baseline disease and demographic characteristics). Variables included in these sensitivity analyses were based on clinical input and statistical tests for treatment effect modification and prognostic factors. Sensitivity analysis 1 included characteristics rated highly prognostic by two or more clinicians. Sensitivity analysis 2 included characteristics that had at least some prognostic value according to clinicians (i.e., low importance or high importance by at least 1 clinician) and all variables with statistically significant findings for interaction tests or tests of prognostic factors with evidence of prognostic influence based on statistical tests. Weights estimated in these sensitivity analyses were then used in the comparison of outcomes, following the same procedures as the primary analysis.
Results were estimated separately for MAIC with primary analysis weights, unweighted MAIC and sensitivity analysis weights applied for the selected NATALEE population. Covariate balance was assessed using standardized mean differences (SMDs) before and after weighting (Supplementary Tables 6 & 7). An SMD of <0.1 was considered a negligible difference, an SMD of 0.1 to <0.2 was considered a small difference (which is acceptable if it is not an effect modifier), an SMD of 0.2 to <0.5 was considered a moderate difference, and an SMD of ≥0.5 was considered a large difference.
Software for MAIC weights calculation
Calculation of MAIC weights was conducted in R (R Core Team; 2013) using an adaptation of sample code from the NICE DSU TSD 18. Standardized MAIC weights (mean value equal to 1.0) were generated using the method of moments, with active (ribociclib + NSAI and abemaciclib + ET) treatment and control (NSAI only and ET only) arms matched separately to ensure that any residual imbalances between active and control arms in monarchE were replicated in the matched NATALEE sample.
Outcomes analyses
A Cox regression model (semiparametric) was chosen to compare ribociclib + NSAI with abemaciclib + ET for the time-to-event analyses as this is a commonly used approach that can be specified as a proportional hazard model and allowed the estimation of hazard ratios. This univariate Cox proportional hazards model was fitted to MAIC-weighted IPD from the selected NATALEE patient population and reconstructed data from monarchE cohort 1. Outcomes for the ITCs were iDFS, DRFS and safety events that were classified as grade ≥3 treatment-emergent adverse events (TEAEs).
iDFS, in both the NATALEE and monarchE trial, was evaluated based on Standardized Definitions for Efficacy End Points (STEEP) criteria (definition consistent with STEEP 2.0) as the time from randomization until local/regional, contralateral, distant recurrence, second primary nonbreast malignancy, or death from any cause, whichever occurred first [38,39]. Likewise, DRFS in both the NATALEE and monarchE trial, also per STEEP(definition consistent with STEEP 2.0), was defined as time from randomization to distant recurrence or death from any cause, whichever occurred first [38,39]. For time-to-event outcomes, patients with no event by the last visit date were censored. Time-to-event data for iDFS and DRFS outcomes in patients in the monarchE trial were obtained by digitizing published KM curves. Pseudo-IPD from monarchE cohort 1 were reconstructed via digitalization of published KM curves using the Guyot algorithm. The reconstructed pseudo failure time data for abemaciclib + ET and ET only arms from cohort 1 of monarchE were assessed by comparing the numbers of patients at risk over time and landmark survival estimates at 24, 36, 48 and 60 months against those reported in the primary publications for monarchE. The number of patients at risk in the reconstructed KM curves for abemaciclib arms matched with the numbers reported in the monarchE publication and the landmark survival estimates matched within +/- 0.001 of the reported survival rates at 24, 36, 48 and 60 months validating the reconstructed data [12]. While visually similar to published survival curves, reconstructed data may not fully replicate original IPD. KM curve estimation and Cox regression were conducted using SAS (SAS Institute; Cary NC) [40].
For safety analysis, grade ≥3 TEAEs with an incidence of ≥5% were calculated using logistic regression, and ORs for these TEAEs between each treatment were estimated.
Assessment of proportional hazards assumption
The validity of the proportional hazards assumption between ribociclib + NSAI and abemaciclib + ET, before and after weighting, was tested by a visual inspection of the log-cumulative hazard plots as well as by the Schoenfeld global test of proportionality. Schoenfeld residuals were generated to assess the proportional hazards assumption for iDFS and DRFS with ribociclib + NSAI versus abemaciclib + ET before and after weighting. If the proportional hazards assumption was violated, survival curves were still presented descriptively to support visual comparisons of time-to-event trends; however, interpretation of the hazard ratios may be limited.
Results
Selection of patients in NATALEE
Among the 5101 patients from the NATALEE trial ITT population, 3307 patients (ribociclib + NSAI, n = 1658; NSAI alone, n = 1649) met the key eligibility criteria for cohort 1 of monarchE (n = 5120; abemaciclib + ET, n = 2555; ET alone arm, n = 2565). MAIC weights were estimated adjusting for all baseline characteristics, and most weights for both treatment arms were below 5.0 in the primary analysis (Supplementary Figure 2). There were 22 patients in the selected NATALEE population with an estimated weight of 0.0, suggesting that they did not have sufficient overlap with those in monarchE cohort 1 to be meaningfully reweighted. Most of the estimated weights for both treatment arms were below 5.0. The maximum weight values in the ribociclib plus NSAI arm and the NSAI only arms were 16.2 and 24.0, respectively. For the primary analysis, after weighting, the ESS for the ribociclib + NSAI and NSAI only arms were 448 and 453, respectively, constituting an estimated reduction of 72.5%–73% from the selected sample size in each arm. Given that the ESS remained above 400 per treatment arm after weighting, use of the MAIC with full covariate adjustment was deemed appropriate. Table 3 is an attrition table for the selected NATALEE population included in this ITC to compare with the monarchE cohort 1 population.
| Characteristic, n | Ribociclib + NSAI | NSAI only | ||
|---|---|---|---|---|
| Met criteria | Excluded | Met criteria | Excluded | |
| Full analysis set | 2549 | 2552 | ||
| No nodal involvement (N0)† | – | 285 | – | 328 |
| Nodal status missing† | – | 3 | – | 5 |
| N1–3† | 2261 | 2219 | ||
| ≥4 pathologic axillary LNs (N2+)† | 1172 | – | 1180 | – |
| 1 to 3 pathologic axillary LNs (N1)† | 1089 | 1039 | ||
| Tumor size ≥5 cm†,‡ | 327 | – | 288 | – |
| Histological grade 3§ | 230 | – | 244 | – |
| Tumor size ≥5 cm or grade 3¶ | 486 | 603 | 469 | 570 |
| Total | 1658 | 891 | 1649 | 903 |
| Effective sample size after weighting# | 448 | 453 | ||
†
Based on the worst of measurements taken at the time of diagnosis and surgical specimen following resection.
‡
Assumed to be TNM classification T3 or T4 due to lack of data on explicit tumor size.
§
Based on histological grade derived from surgical specimen.
¶
Patients with 1 to 3 nodes who either had tumor size T3 or T4 based on TNM classification or grade 3 based on surgical specimen.
#
Patient weights estimated using MAIC.
LN: Lymph node; MAIC: Matching-adjusted indirect comparison; N1-3: 1–3 positive axillary lymph nodes; N2: 4–9 positive axillary lymph nodes; N3: ≥10 positive axillary lymph nodes; NSAI: Nonsteroidal aromatase inhibitor; TNM: Tumor, node, metastasis.
The ESS for sensitivity analysis 1, which only included highly prognostic variables, was 821 patients for the ribociclib + NSAI arm and 767 for the NSAI alone arm in the selected NATALEE population, constituting an estimated reduction of 50.5% and 53.5% from the selected sample size in each arm, respectively. The ESS for sensitivity analysis 2, which included any variables with some prognostic value, was 617 patients for the ribociclib + NSAI arm and 620 patients for the NSAI alone arm, constituting an estimated reduction of 62.8% and 62.4% from the selected sample size in each arm, respectively.
Baseline characteristics before & after adjustment
The two trials were well balanced for many of the reported characteristics at baseline before adjustment for the selected NATALEE population, with SMDs from the monarchE cohort 1 patient population below 50% for most characteristics (Supplementary Table 6). For two characteristics (region and missing Ki-67 status), the SMDs exceeded 50%, which were adjusted. The SMDs exceeded 20% for the proportions of patients with a Ki-67 index of ≥20%, those residing in geographic region reported as ‘other’ (i.e., not North America, Europe or Asia), those whose ethnicity was not Hispanic or Latino, those with stage IIA or IIIA disease, and those with prior neoadjuvant chemotherapy. An SMD between 20% and 50% suggests differences between studies (i.e., not insignificant), which were adjusted [40]. After weighting, the SMDs between the patient characteristics of the weighted NATALEE population and the monarchE cohort 1 population were relatively small or zero (Supplementary Table 7).
Invasive disease-free survival
Based on the MAIC analyses, no statistically significant difference was observed in the iDFS between the ribociclib + NSAI versus abemaciclib + ET arm in the target populations (monarchE cohort 1-eligible patients). After applying the MAIC weights, Cox regression yielded similar iDFS with the ribociclib + NSAI arm in the selected NATALEE population versus the abemaciclib + ET arm in the monarchE cohort 1 subset (hazard ratio: 0.901; 95% CI: 0.678–1.197; nominal p = 0.470) (Figures 2 & 3). Likewise, unweighted iDFS with ribociclib + NSAI was similar in the ribociclib + NSAI arm and the abemaciclib + ET arm in the target population (hazard ratio: 1.055; 95% CI: 0.887–1.255; nominal p = 0.545) (Figure 3). Comparisons of the NSAI only arm in the selected NATALEE population versus the ET only arm in cohort 1 of monarchE yielded similar iDFS for the weighted comparison (hazard ratio: 0.890; 95% CI: 0.703–1.126; nominal p = 0.332) and unweighted analysis (hazard ratio: 0.987; 95% CI: 0.849–1.147; nominal p = 0.862) (Figure 3). Schoenfeld residuals of weighted and unweighted iDFS in the ribociclib + NSAI arm versus the abemaciclib + ET arm (weighted: p = 0.667; unweighted: p = 0.516) for the population analyzed suggested that the proportional hazards assumption was not violated (Supplementary Figure 3).
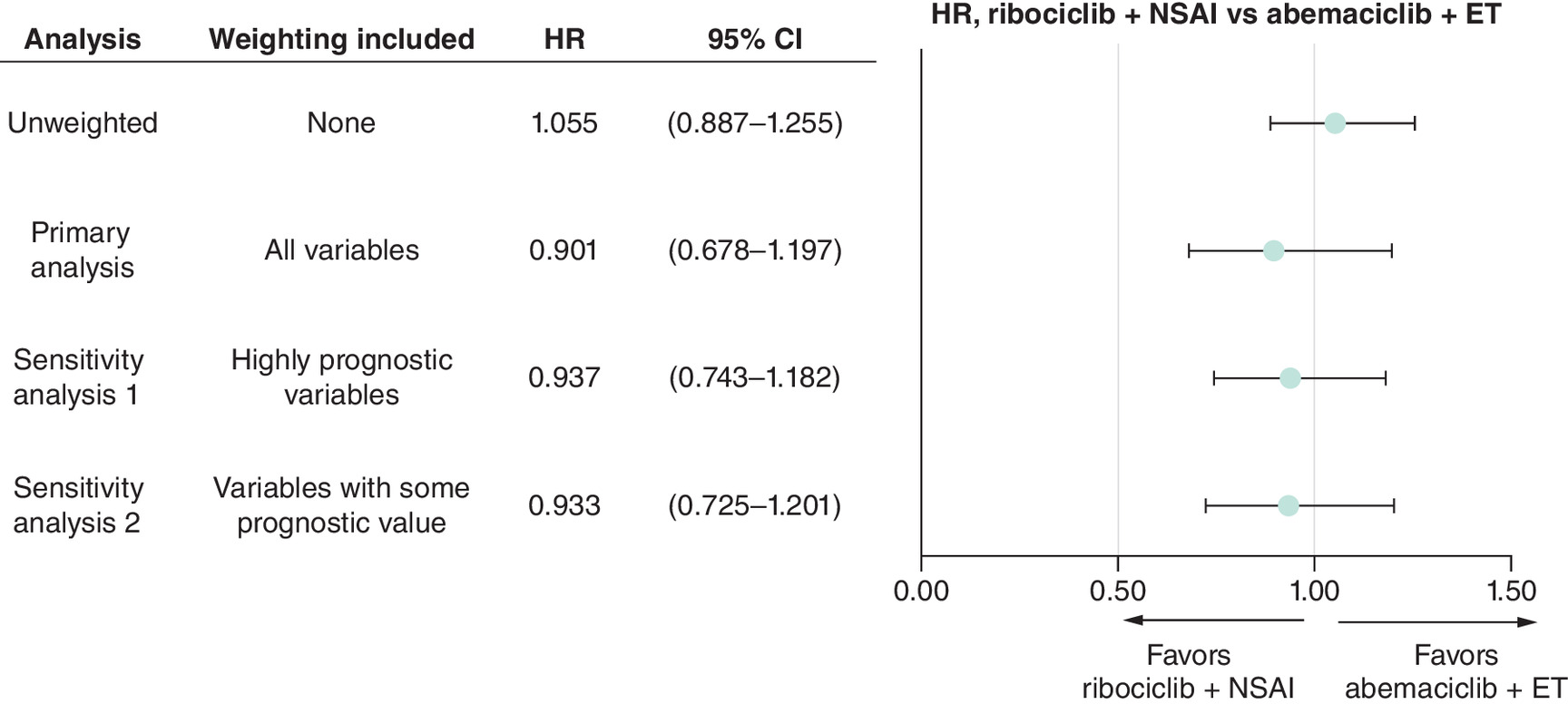
Figure 2. Summary of invasive disease-free survival hazard ratios from unanchored matching-adjusted indirect comparison analyses: ribociclib + nonsteroidal aromatase inhibitor in selected NATALEE population versus abemaciclib + endocrine therapy in monarchE cohort 1.
CI: Confidence interval; ET: Endocrine therapy; HR: Hazard ratio; NSAI: Nonsteroidal aromatase inhibitor.
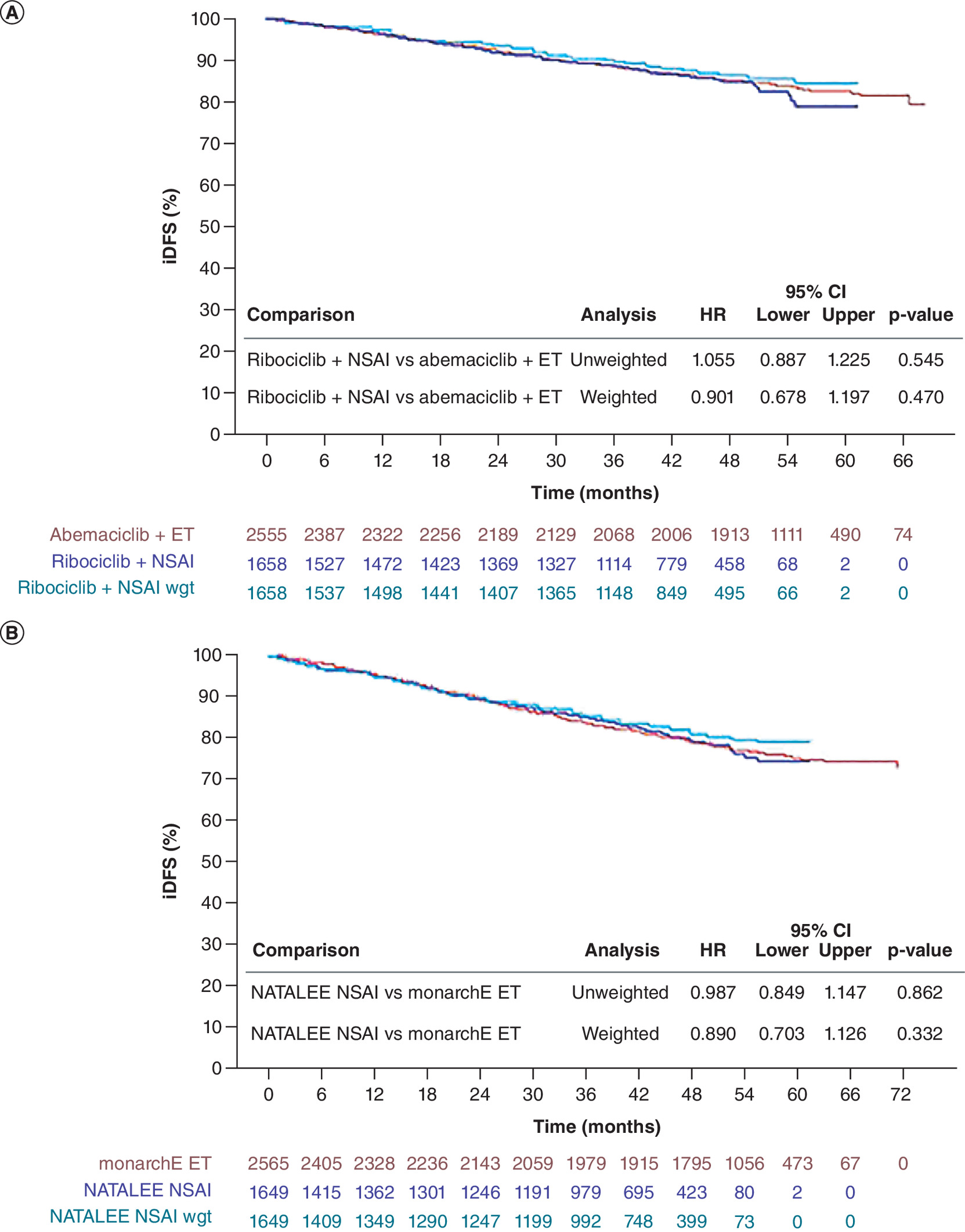
Figure 3. Primary analysis.
(A) iDFS KM curve for ribociclib + NSAI in selected NATALEE population versus abemaciclib + ET in monarchE cohort 1 and (B) iDFS KM curve for ET arms for the same patient subgroups.
CI: Confidence interval; iDFS: Invasive disease-free survival; ET: Endocrine therapy; KM: Kaplan–Meier; NSAI: Nonsteroidal aromatase inhibitor; wgt: Weight.
Findings from sensitivity analyses for iDFS were generally consistent with the primary analysis (Figure 2 & Supplementary Table 8). For sensitivity analysis 1, Cox regression yielded a hazard ratio of 0.937 (95% CI: 0.743–1.182; nominal p = 0.545) for weighted iDFS between the ribociclib + NSAI arm of the selected NATALEE population and the abemaciclib + ET arm of monarchE cohort 1. For sensitivity analysis 2, Cox regression yielded a hazard ratio of 0.933 (95% CI: 0.725–1.201; nominal p = 0.591) for weighted iDFS between the ribociclib + NSAI arm and the abemaciclib + ET arm.
Distant relapse–free survival
Based on the MAIC analyses, there was insufficient evidence to suggest differences in DRFS between the ribociclib + NSAI versus abemaciclib + ET analysis in the target populations (monarchE cohort 1-eligible patients). Weighted DRFS was similar in the ribociclib + NSAI selected NATALEE population compared with abemaciclib + ET in the monarchE cohort 1 subset (hazard ratio: 0.946; 95% CI: 0.686–1.305; nominal p = 0.734) (Figures 4 & 5). Unweighted DRFS with ribociclib + NSAI in the selected NATALEE population was similar to that with abemaciclib + ET in the monarchE cohort 1 subset (hazard ratio: 0.980; 95% CI: 0.811–1.184; nominal p = 0.832) (Figures 4 & 5). Comparisons of the NSAI alone arm in the selected NATALEE patient population versus the ET alone arm in monarchE cohort 1 before and after weighting yielded similar DRFS for unweighted (hazard ratio: 0.920; 95% CI: 0.782–1.083; nominal p = 0.315) and weighted comparison (hazard ratio: 0.828; 95% CI: 0.649–1.058; nominal p = 0.131) (Figure 5). Schoenfeld residuals of unweighted and weighted DRFS in the ribociclib + NSAI arm versus the abemaciclib + ET arm (unweighted: p = 0.014; weighted: p < 0.001) for the trial populations analyzed suggested that the proportional hazards assumption may have been violated (Supplementary Figure 4).
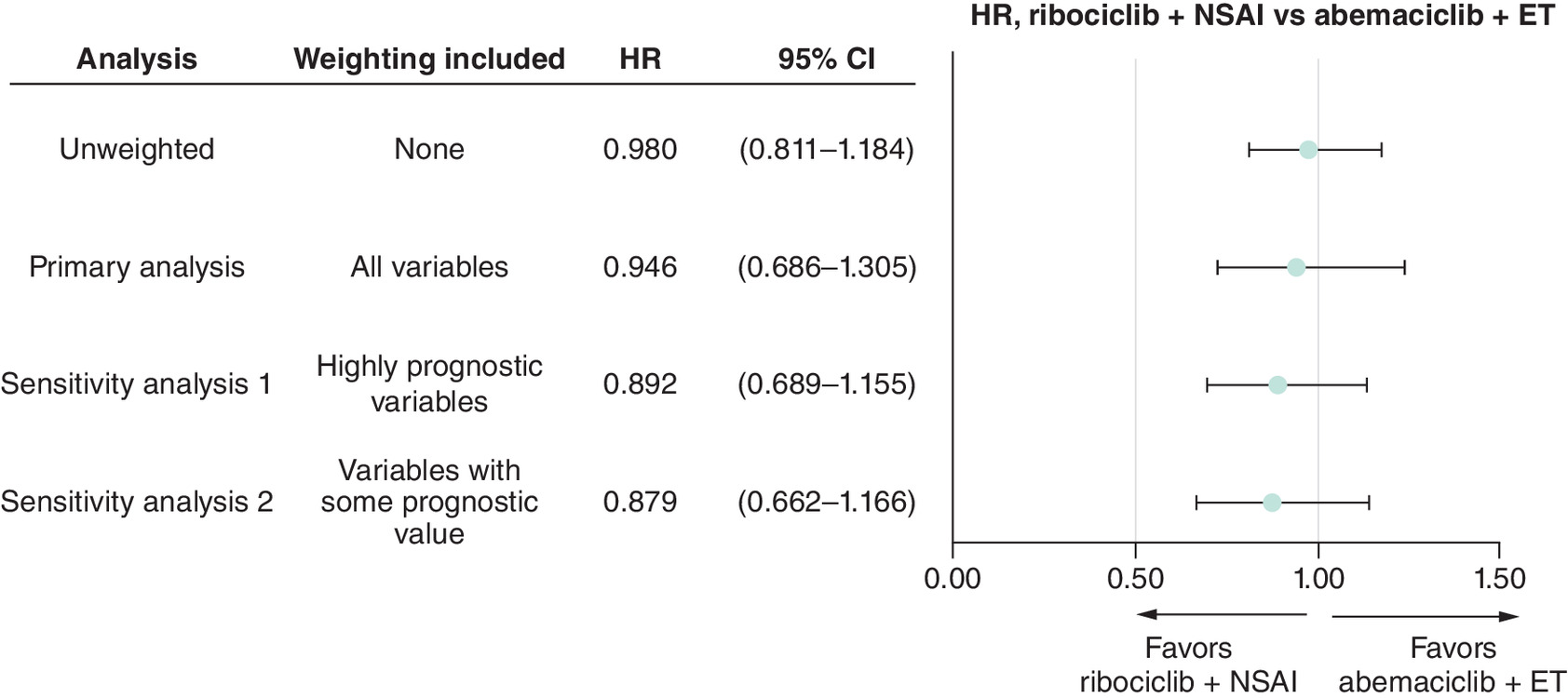
Figure 4. Summary of DRFS hazard ratios from unanchored MAIC analyses: Ribociclib + NSAI in selected NATALEE population versus abemaciclib + ET in monarchE cohort 1.
CI: Confidence interval; DRFS: Distant recurrence-free survival; ET: Endocrine therapy; HR: Hazard ratio; MAIC: Matching-adjusted indirect comparison; NSAI: Nonsteroidal aromatase inhibitor.
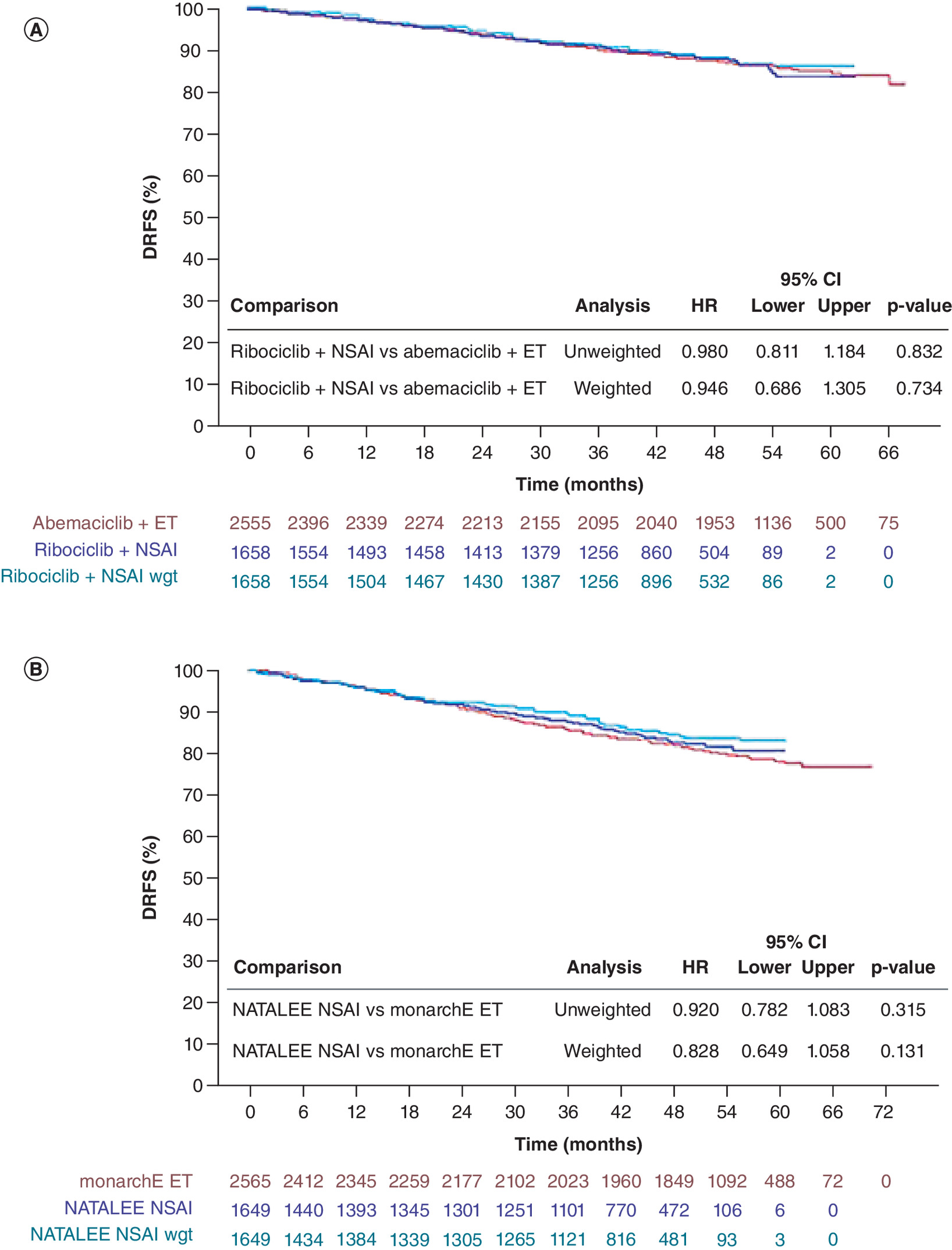
Figure 5. Primary analysis.
(A) DRFS KM curve for ribociclib + NSAI in selected NATALEE population versus abemaciclib + ET in monarchE cohort 1 and (B) DRFS KM curve for ET arms for the same patient subgroups.
CI: Confidence interval; DRFS: Distant recurrence-free survival; ET: Endocrine therapy; KM: Kaplan–Meier; NSAI: Nonsteroidal aromatase inhibitor; wgt: Weight.
Findings of sensitivity analyses for DRFS were generally consistent with the primary analysis (Figure 4 & Supplementary Table 9). For sensitivity analysis 1, weighted analysis yielded a hazard ratio of 0.892 (95% CI: 0.689–1.155; nominal p = 0.385) for DRFS between the ribociclib + ET arm of the selected NATALEE population and the abemaciclib + ET arm of monarchE cohort 1. For sensitivity analysis 2, weighted analysis yielded a hazard ratio of 0.879 (95% CI: 0.662–1.166; nominal p = 0.370) for DRFS between the ribociclib + NSAI arm of NATALEE and the abemaciclib + ET arm.
Safety
Comparisons of grade ≥3 TEAEs suggested lower odds (OR <1) for diarrhea, leukopenia and lymphopenia before and after MAIC weighting in patients treated with ribociclib + NSAI in the selected NATALEE population compared with abemaciclib + ET in monarchE cohort 1 (Figure 6 & Supplementary Table 10). For increased alanine aminotransferase (ALT) and neutropenia, the analysis suggested significantly greater odds (OR >1) in the ribociclib + NSAI arm compared with the abemaciclib + ET arm.
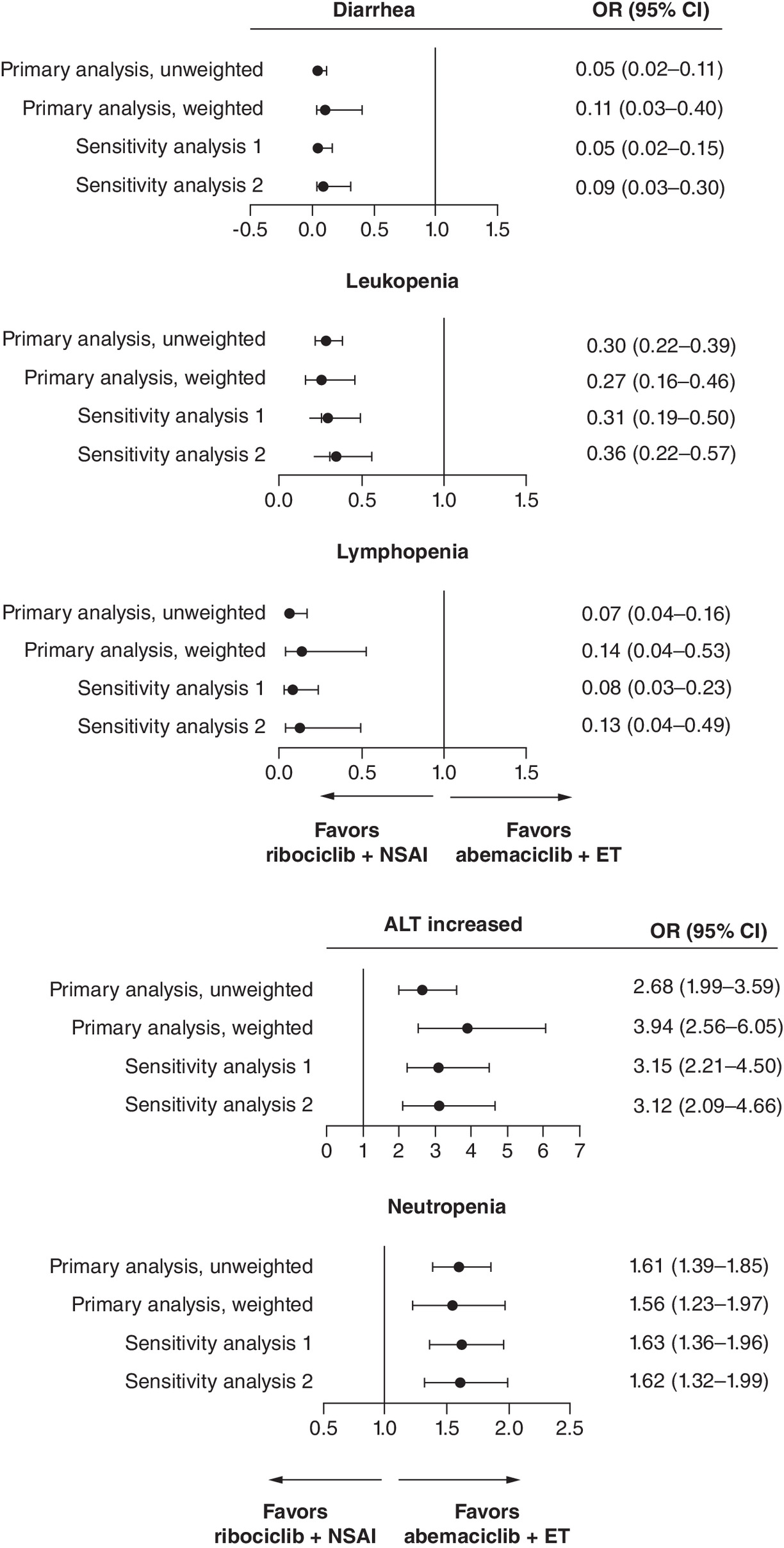
Figure 6. Summary of odds ratios (95% CI) for primary safety analysis comparing ribociclib + NSAI in selected NATALEE population versus abemaciclib + ET in monarchE cohort 1.
ALT: Alanine aminotransferase; CI: Confidence interval; ET: Endocrine therapy; MAIC: Matching-adjusted indirect comparison; NSAI: Nonsteroidal aromatase inhibitor; OR: Odds ratio.
Results of the sensitivity analyses for the safety outcomes were also consistent with those observed in the primary analyses (Supplementary Table 11). For sensitivity analysis 1, as seen in the primary analysis, increased ALT and neutropenia were the only TEAEs for which ribociclib + ET had significantly greater odds than abemaciclib + ET in the population analyzed. For sensitivity analysis 2, consistent with primary analysis, ribociclib + ET had statistically significantly greater odds for increased ALT and neutropenia than abemaciclib + ET.
Discussion
This study aimed to compare efficacy and safety outcomes in patients with high-risk HR+/HER2- EBC receiving ribociclib + NSAI (NATALEE) versus abemaciclib + ET (monarchE) using ITC methods in the absence of head-to-head trials. These unanchored MAIC analyses between a subset of the NATALEE population matched to cohort 1 of the monarchE trial (patients with ≥4 positive lymph nodes or 1 to 3 positive lymph nodes with tumor size ≥5 cm or histological grade 3 disease) found insufficient evidence to suggest statistically significant differences in efficacy outcomes, namely iDFS and DRFS, in patients who received ribociclib + NSAI versus abemaciclib + ET at a median follow-up of approximately 4 years. However, differences in the safety profiles of these two CDK4/6is were observed.
The comparative efficacy analysis of this study should be viewed in the context of current adjuvant treatment guidelines. Specifically, NATALEE and monarchE have led to inclusion of adjuvant ribociclib and abemaciclib in guidelines from the American Society of Clinical Oncology, European Society for Medical Oncology (ESMO-Magnitude of Clinical Benefit Scale score A), National Comprehensive Cancer Network (category 1) and Chinese Society of Clinical Oncology for their respective HR+/HER2- EBC trial populations [41–45]. Ribociclib + NSAI is recommended for use in a broader EBC patient population, which includes high-risk node-negative patients and all patients with macroscopic N1 disease, than abemaciclib + ET [45]. A recent analysis of a large real-world database found that the broader eligibility criteria for NATALEE ITT versus monarchE cohort 1 presents the potential opportunity of adding a CDK4/6i to SOC ET for a greater proportion of patients with EBC at an increased risk of recurrence [46]. For the patients with EBC whose disease characteristics overlapped between NATALEE and monarchE cohort 1 (the US FDA- and EMA-approved population for monarchE), the current study, within its limitations, suggests no difference in efficacy outcomes between ribociclib and abemaciclib [14,17].
The differences in the ribociclib and abemaciclib safety profiles observed in this analysis have implications on decision-making in the adjuvant setting. In this analysis, largely asymptomatic AEs (neutropenia and liver-related AEs) had higher odds of occurrence with ribociclib + NSAI versus abemaciclib + ET. Importantly, safety follow-up duration differed between the two trials: NATALEE collected safety data for up to 3 years, while monarchE collected safety data for up to 2 years [9,10]. This longer observation window in NATALEE increases the opportunity to capture AEs, particularly those with late onset of occurrence. For AEs for which ribociclib + NSAI showed lower odds (OR <1) compared with abemaciclib + ET (e.g., diarrhea), the observed advantage with ribociclib may have been underestimated, and the true difference may be even greater if both studies used the same follow-up duration. Conversely, for AEs for which ribociclib + NSAI showed higher odds (OR >1) (e.g., neutropenia or ALT increase), part of the observed difference could be due to longer AE surveillance, and the difference may have been attenuated if the follow-ups were similar between the two studies.
Analyses from the NATALEE trial showed that most AEs occurred and were resolved early in treatment [47]. Furthermore, an analysis across the Phase III trials of ribociclib in EBC and advanced BC (ABC) found that liver-related AEs occurred in a subset of patients (<20%), with a majority of grade ≥3 events resolved within 2 months from onset [48]. The current analysis showed higher odds of symptomatic diarrhea associated with abemaciclib + ET; this becomes notably more important clinically due to its impact on the quality of life of patients with BC. In a recent survey of clinicians and patients, 71% of patients with ABC treated with CDK4/6is reported that diarrhea had a moderate to severe impact on their quality of life [49]. Treatment decisions in clinical settings for patients with HR+/HER2- EBC should take into account these distinct AE profiles between ribociclib and abemaciclib. In a discrete choice experiment, patients with HR+/HER2- EBC ranked the following in importance for treatment preference: efficacy (iDFS), followed by reduction in risk of AEs (venous thromboembolic events, neutropenia and diarrhea) [50]. The current analysis shows that efficacy (the most important consideration by patients for treatment preference) was similar between the ribociclib arm and abemaciclib arm within the overlapping monarchE cohort 1 patient population. Therefore, patient preferences will likely take into account differences between the safety profiles of the two drugs and duration of treatment.
It is also important to interpret the findings of this MAIC with respect to the ET backbone of the CDK4/6i. While NATALEE included an NSAI as an ET partner for all patients in the ribociclib + ET arm, tamoxifen, a SERM, was allowed as an ET partner in monarchE, with 31.4% receiving tamoxifen as the first ET on study treatment [10,27]. Trial level meta-analysis has shown that AIs are more effective than tamoxifen in treating patients with HR+/HER2- EBC in the adjuvant setting, particularly those at higher risk of recurrence [33]. Furthermore, there are data that suggest that the magnitude of benefit of adjuvant abemaciclib is greater when it is combined with tamoxifen than with AI [12,25]. Any bias in estimated treatment effects from different ET backbones would impact both anchored and unanchored approaches. For this unanchored MAIC, the limitation is that only ribociclib + NSAI versus abemaciclib + ET were compared and not ribociclib + NSAI versus abemaciclib + NSAI. However, for feasibility reasons, we could not separately analyze and compare to the abemaciclib + NSAI subgroup alone (as described in Methods). It would be of significant clinical interest to see a similar analysis comparing ribociclib + NSAI and abemaciclib + NSAI to better understand any impact of the differences in ET backbone on efficacy between the two CDK4/6i agents in adjuvant treatment.
The results of the primary analysis of this study are supported by the sensitivity analyses. Based on our feasibility assessment, the use of unanchored weighted MAIC methods allowed for a more robust comparison versus an unadjusted and anchored ITC. The primary analysis employed MAIC weights adjusted for all available baseline characteristics reported for monarchE, whereas sensitivity analyses considered alternative sets of baseline characteristics (based on clinical input) for weighting. In the first sensitivity analysis, NATALEE patients were adjusted only for characteristics that clinicians agreed were highly prognostic, which included hormone receptor status, number of lymph nodes, histopathology at diagnosis, TNM stage, tumor size, pathologic diagnosis term and Ki-67 index scores. In the second sensitivity analysis, NATALEE patients were adjusted for all characteristics that clinicians indicated as having some prognostic value as well as all characteristics with evidence of prognostic influence based on quantitative tests. The results of these two sensitivity analyses were consistent with those of the primary analysis. That the efficacy and safety outcomes in these sensitivity analyses, with a lower estimated reduction from original trial sample size (∼52% for first sensitivity analysis and ∼63% for second sensitivity analyses), were consistent with the primary analysis (that had a ∼73% reduction) shows the robustness of the primary MAIC analysis.
Apart from the consistent results seen with the sensitivity analysis, further evidence substantiated the reliability of the primary analysis. The estimated treatment effect in the ribociclib + NSAI arm based on the unweighted NATALEE sample (i.e., a 0% reduction in ESS) versus abemaciclib + ET arm of monarchE cohort 1, suggested no evidence of a statistically significant difference in efficacy between them. Also, the 73% reduction as seen in the ESS of our analysis, is similar to the median reduction of 74.2% from the original sample size reported in 16 other NICE technology appraisals [51]. Additionally, an ESS in the range of 450, as seen in our analysis, is higher than an ESS of 185, which was described as sufficiently large in the NICS DSU report [52]. Finally, clinical experts, in the NICE 2025 draft guidelines for ribociclib, have broadly agreed with the equal-efficacy assumption between ribociclib + NSAI and abemaciclib + ET based on the current MAIC analysis [53].
Limitations
This analysis encountered several limitations related to differences in these adjuvant CDK4/6i trials. First, unlike anchored ITCs, where differences in unknown prognostic factors between trials do not affect the validity of the comparison, the current unanchored ITC analysis – while using MAIC weights to adjust for all available baseline characteristics reported for monarchE – was limited by the lack of access to IPD from monarchE. Thus, even though an extensive number of reported patient baseline characteristics from monarchE were taken into account, it is possible that there were unreported prognostic factors that were not possible to include in the estimation of MAIC weights. This poses a risk of residual confounding, which is an inherent limitation of all unanchored comparisons [51]. Second, the SMD for missing Ki-67 test results exceeded 50%, while for Ki-67 index of ≥20%, it was 32.1%. As the Ki-67 index was one of the characteristics with clinician consensus on prognostic importance, the imbalance could introduce bias if not fully adjusted despite weighting. Third, the findings of this study could be biased to the extent that there is any residual confounding after MAIC weighting. Fourth, patients from NATALEE who would be eligible for inclusion in the monarchE trial constituted a subset of the total ITT NATALEE patient population. After selection and weighting the MAIC, a reduction in the ESS from the original trial sample size may have led to loss of statistical power and a break in randomization from the original NATALEE ITT population. Fifth, due to its exploratory nature, unmeasured confounders and differences in safety reporting, this cross-trial safety comparison should be interpreted with caution. Also, a longer AE follow-up period in NATALEE than monarchE may have led to overestimation of ORs for AEs with longer follow-up. However, for early-onset AEs such as diarrhea, the shorter follow-up in monarchE may still suffice, supporting the validity of OR comparisons. Potential instability of estimates for rare AEs was also a limitation. Sixth, the proportional hazards assumption may have been violated for DRFS. As a result, hazard ratio estimates should be interpreted alongside survival curve shapes and absolute risk differences, rather than as constant relative risk over time. Finally, another limitation is the differential follow-up time between the NATALEE and monarchE trials, which was a modest 4 month difference in follow-up that is unlikely to bias efficacy outcome comparisons.
Some of the other limitations of this ITC are commonly noted in such comparisons. The KM curves from the monarchE trial used in this analysis were based on reconstructed IPD. While the KM curves estimated from the reconstructed data were similar to those reported in the monarchE publications, the pseudo-failure time data may not have matched the patient-level failure time data with complete accuracy. However, as the differences between the reported hazard ratios and the hazard ratios estimated from pseudo-failure time data were relatively small, they were unlikely to bias the findings reported here.
Conclusion
Previous MAICs and network meta-analysis have been conducted comparing efficacy, safety and quality of life outcomes between CDK4/6i trials in the ABC setting [54–56]. This, however, is the first MAIC analysis comparing two CDK4/6is in the adjuvant setting. Overall, this study provides valuable insights into the comparative efficacy and safety of ribociclib and abemaciclib in the adjuvant treatment of HR+/HER2- EBC, despite limitations inherent to unanchored MAIC. While no statistically significant differences in efficacy outcomes were observed between ribociclib and abemaciclib in the studied population, differences in safety profiles may inform treatment selection based on individual patient considerations.
Summary points
•
Ribociclib and abemaciclib are both approved for the treatment of patients with high-risk hormone receptor-positive/human epidermal growth factor receptor 2–negative (HR+/HER2-) early breast cancer based on positive data in the phase III NATALEE and monarchE trials, respectively.
•
Estimates of the relative efficacy and safety of ribociclib + nonsteroidal aromatase inhibitor (NSAI) versus relevant comparators is important for evidence of cost-effectiveness to reimbursement and/or health technology assessment authorities, which is required in many regions.
•
To date, no trials have directly compared the efficacy and safety of adjuvant ribociclib and abemaciclib.
•
This study performed an unanchored matching-adjusted indirect comparison using individual patient data from NATALEE and aggregate data for monarchE cohort 1.
•
This analysis assessed the relative efficacy (invasive disease-free survival and distant relapse–free survival) and safety (grade ≥3 treatment-emergent adverse events) of ribociclib + NSAI versus abemaciclib + endocrine therapy (ET) in a matched target population.
•
Cox regression yielded similar invasive disease-free survival and distant relapse–free survival for weighted ribociclib + NSAI versus abemaciclib + ET in the patients of interest from NATALEE and monarchE.
•
The comparison suggested lower odds for diarrhea, leukopenia and lymphopenia and higher odds for increased alanine aminotransferase and neutropenia with ribociclib + NSAI versus abemaciclib + ET.
•
These safety comparisons should be interpreted with caution due to differences in AE follow-up duration between NATALEE (3 years) and monarchE (2 years), which may affect cumulative AE detection.
•
This comparative analysis was limited only to a selected NATALEE population that matched eligibility for cohort 1 of monarchE, while ribociclib + NSAI is recommended by treatment guidelines for use in a much broader early breast cancer patient population.
•
There were some limitations to this study, although all indications including sensitivity analysis suggest sample size is adequate, and estimates are robust.
•
While no significant differences in efficacy outcomes were observed, potential differences in safety profiles between ribociclib + NSAI and abemaciclib + ET may inform treatment selection based on individual patient considerations.
Author contributions
D Stellato was involved with study conception and analysis interpretation; A Danyliv, I Ferrusi, H Hu and M Akdere were involved with study conception, analysis interpretation, manuscript drafting and revision. S Chia, J Li, F Ma and A Makris were involved with analysis interpretation, manuscript drafting and revision.
Acknowledgments
The authors thank M Kalra of Novartis for his contribution in preparation of this manuscript.
Financial disclosure
The study was sponsored by Novartis. The funder of this study, in agreement with the authors and the study steering committee members, designed this study. Representatives of the trial sponsor performed data collection and the subsequent analysis. All authors have reviewed and approved the data, contributed to the development and approval of the manuscript, and acknowledged the decision to submit the manuscript for publication. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
S Chia has received personal fees and funds to his institution from Novartis, Pfizer, F. Hoffmann-La Roche, Eli Lilly, Merck and AstraZeneca. J Li has nothing to disclose. F Ma has nothing to disclose. D Stellato has received consulting fees from Novartis. A Danyliv, I Ferrusi, H Hu and M Akdere report employment with and stock ownership in Novartis. A Makris has received personal fees from Novartis. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing and editorial support were provided by S Tandon of Nucleus Global and were funded by Novartis.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis utilizing NATALEE trial data that have been shared with them, and that the use of these shared data is in accordance with the terms agreed upon their receipt. Data were provided by Novartis. The monarchE trial data used in this analysis were from published reports.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 221.00 KB
References
Papers of special note have been highlighted as: • of interest
1.
Bray F, Laversanne M, Sung H et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74(3), 229–263 (2024).
2.
Howlader N, Altekruse SF, Li CI et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J. Natl Cancer Inst. 106(5), dju055 (2014).
3.
Iqbal J, Ginsburg O, Rochon PA et al. Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA 313(2), 165–173 (2015).
4.
Jhaveri K, Pegram M, Neven P et al. Real-world evidence on risk of recurrence (ROR) in patients (pts) with node-negative (N0) and node-positive HR+/HER2- early breast cancer (EBC) from US electronic health records (EHR). Ann. Oncol. 35(Suppl. 2), Abstract 292P (2024).
5.
Curigliano G, Ciruelos E, Kalinsky K et al. Short-term risk of recurrence in patients with HR+/HER2- early breast cancer treated with endocrine therapy in randomized clinical trials: a meta-analysis. J. Clin. Oncol. 42(Suppl. 16), Abstract 541 (2024).
6.
Pan H, Gray R, Braybrooke J et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N. Engl. J. Med. 377(19), 1836–1846 (2017).
7.
Early Breast Cancer Trialists' Collaborative Group. Reductions in recurrence in women with early breast cancer entering clinical trials between 1990 and 2009: a pooled analysis of 155746 women in 151 trials. Lancet 404(10461), 1407–1418 (2024).
8.
O'Shaughnessy J, Tolaney SM, Yardley DA et al. Real-world risk of recurrence and treatment outcomes with adjuvant endocrine therapy in patients with stage II-III HR+/HER2- early breast cancer. Breast 81, 104437 (2025).
• Highlights the risk of recurrence with adjuvant endocrine therapy in patients with stage II or III HR+/HER2- EBC (including node-negative disease).
9.
Slamon D, Lipatov O, Nowecki Z et al. Ribociclib plus endocrine therapy in early breast cancer. N. Engl. J. Med. 390(12), 1080–1091 (2024).
• Presents the prespecified interim analysis of the phase III NATALEE trial.
10.
Johnston SRD, Harbeck N, Hegg R et al. Abemaciclib combined with endocrine therapy for the adjuvant treatment of HR+, HER2-, node-positive, high-risk, early breast cancer (monarchE). J. Clin. Oncol. 38(34), 3987–3998 (2020).
• Presents the preplanned efficacy interim analysis of the phase III monarchE trial.
11.
Fasching PA, Stroyakovskiy D, Yardley D et al. Adjuvant ribociclib (RIB) plus nonsteroidal aromatase inhibitor (NSAI) in patients (pts) with HR+/HER2- early breast cancer (EBC): 4-year outcomes from the NATALEE trial. Ann. Oncol. 35(Suppl. 2), Abstract LBA13 (2024).
• Presents the 4-year landmark analysis from the phase III NATALEE trial.
12.
Rastogi P, O'Shaughnessy J, Martin M et al. Adjuvant abemaciclib plus endocrine therapy for hormone receptor-positive, human epidermal growth factor receptor 2-negative, high-risk early breast cancer: results from a preplanned monarchE overall survival interim analysis, including 5-year efficacy outcomes. J. Clin. Oncol. 42(9), 987–993 (2024).
• Presents the 5-year efficacy results from the phase III monarchE trial.
13.
Toi M, Boyle F, Im YH et al. Adjuvant abemaciclib combined with endocrine therapy: efficacy results in monarchE cohort 1. Oncologist 28(1), e77–e81 (2023).
14.
US Food and Drug Administration. FDA expands early breast cancer indication for abemaciclib with endocrine therapy. Available at: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-expands-early-breast-cancer-indication-abemaciclib-endocrine-therapy (Accessed: 10 May 2025).
15.
Novartis. Kisqali prescribing information. Available at: https://www.novartis.com/us-en/sites/novartis_us/files/kisqali.pdf (Accessed: 10 May 2025).
16.
European Medicines Agency. Kisqali: ribociclib. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/kisqali (Accessed: 10 May 2025).
17.
European Medicines Agency. Verzenios: abemaciclib. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/verzenios (Accessed: 10 May 2025).
18.
Lilly. Verzenio prescribing information. Available at: https://pi.lilly.com/us/verzenio-uspi.pdf (Accessed: 10 May 2025).
19.
Breast International Group (BIG) 1-98 Collaborative Group. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N. Engl. J. Med. 353(26), 2747–2757 (2005).
20.
Schochter F, Rack B, Tzschaschel M et al. Endocrine treatment with 2 years of tamoxifen versus 2 years of exemestane in postmenopausal patients with high-risk early breast cancer and persisting circulating tumor cells - first results of the SUCCESS C endocrine treatment sub-study. Oncol. Res. Treat. 41(3), 93–98 (2018).
21.
Xiang HY, Liu YH, Zhang H et al. Clinicopathologic analysis of 722 breast cancer patients who met the inclusion criteria of the TAILORx trial. Chin. Med. J. (Engl.) 132(24), 2914–2919 (2019).
22.
Chavez-MacGregor M, Miao J, Pusztai L et al. Phase III randomized, placebo-controlled trial of endocrine therapy ± 1 year of everolimus in patients with high-risk, hormone receptor-positive, early-stage breast cancer. J. Clin. Oncol. 42(25), 3012–3021 (2024).
23.
Bachelot T, Cottu P, Chabaud S et al. Everolimus added to adjuvant endocrine therapy in patients with high-risk hormone receptor-positive, human epidermal growth factor receptor 2-negative primary breast cancer. J. Clin. Oncol. 40(32), 3699–3708 (2022).
24.
Loibl S, Marmé F, Martin M et al. Palbociclib for residual high-risk invasive HR-positive and HER2-negative early breast cancer-the Penelope-B trial. J. Clin. Oncol. 39(14), 1518–1530 (2021).
25.
Harbeck N, Rastogi P, O'Shaughnessy J et al. Adjuvant abemaciclib plus endocrine therapy for HR+, HER2-, high-risk early breast cancer: results from a preplanned monarchE overall survival interim analysis, including 5-year efficacy outcomes. Ann. Oncol. 34(Suppl. 2), Abstract LBA17 (2023).
26.
Novartis. A phase III, multicenter, randomized, open-label trial to evaluate efficacy and safety of ribociclib with endocrine therapy as an adjuvant treatment in patients with hormone receptor-positive, HER2-negative, early breast cancer: efficacy analysis and safety update (21 July 2023 data cutoff). Data on file. (2023).
27.
Slamon DJ, Fasching PA, Hurvitz S et al. Rationale and trial design of NATALEE: a phase III trial of adjuvant ribociclib + endocrine therapy versus endocrine therapy alone in patients with HR+/HER2- early breast cancer. Ther. Adv. Med. Oncol. 15, 17588359231178125 (2023).
28.
Johnston SRD, Toi M, O'Shaughnessy J et al. Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol. 24(1), 77–90 (2023).
29.
National Institute for Health and Care Excellence. Abemaciclib with endocrine therapy for adjuvant treatment of hormone receptor-positive, HER2-negative, node-positive early breast cancer at high risk of recurrence. Published: 20 July 2022. Available at: https://www.nice.org.uk/guidance/ta810
30.
Robinson A. A review of the use of exemestane in early breast cancer. Ther. Clin. Risk Manag. 5(1), 91–98 (2009).
31.
Goss PE, Ingle JN, Pritchard KI et al. Exemestane versus anastrozole in postmenopausal women with early breast cancer: NCIC CTG MA.27–a randomized controlled phase III trial. J. Clin. Oncol. 31(11), 1398–1404 (2013).
32.
Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in premenopausal women with oestrogen receptor-positive early-stage breast cancer treated with ovarian suppression: a patient-level meta-analysis of 7030 women from four randomised trials. Lancet Oncol. 23(3), 382–392 (2022).
33.
Janni W, Untch M, Harbeck N et al. Systematic literature review and trial-level meta-analysis of aromatase inhibitors vs tamoxifen in patients with HR+/HER2- early breast cancer. Breast 81, 104429 (2025).
34.
Phillippo DM, Ades AE, Dias S et al. Methods for population-adjusted indirect comparisons in health technology appraisal. Med. Decis. Making 38(2), 200–211 (2018).
35.
Fasching PA, Barrios CH, Lim E et al. Prognostic variables for risk of recurrence in patients (pts) with HR+/HER2–early breast cancer (EBC) using data from the NATALEE trial: a machine learning (ML) model–based analysis. Breast 80, Abstract P001 (2025).
• Highlights critical prognostic variables identified by machine learning approach that affect recurrence risk in patients with HR+/HER2- EBC.
36.
Signorovitch JE, Sikirica V, Erder MH et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health 15(6), 940–947 (2012).
37.
Signorovitch JE, Wu EQ, Yu AP et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics 28(10), 935–945 (2010).
38.
Hudis CA, Barlow WE, Costantino JP et al. Proposal for standardized definitions for efficacy end points in adjuvant breast cancer trials: the STEEP system. J. Clin. Oncol. 25(15), 2127–2132 (2007).
39.
Tolaney SM, Garrett-Mayer E, White J et al. Updated Standardized Definitions for Efficacy End Points (STEEP) in adjuvant breast cancer clinical trials: STEEP Version 2.0. J. Clin. Oncol. 39(24), 2720–2731 (2021).
40.
Guyot P, Ades AE, Ouwens MJ et al. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 12, 9 (2012).
41.
Li J, Hao C, Wang K et al. Chinese Society of Clinical Oncology (CSCO) breast cancer guidelines 2024. Transl. Breast Cancer Res. 5, 18 (2024).
42.
European Society for Medical Oncology. ESMO-MCBS scorecard. Ribociclib. Available at: https://www.esmo.org/guidelines/esmo-mcbs/esmo-mcbs-for-solid-tumours/esmo-mcbs-scorecards/scorecard-468-1 (Accessed: 10 May 2025).
43.
European Society for Medical Oncology. ESMO-MCBS scorecard. Abemaciclib. Available at: https://www.esmo.org/guidelines/esmo-mcbs/esmo-mcbs-for-solid-tumours/esmo-mcbs-scorecards/scorecard-371-1 (Accessed: 10 May 2025).
44.
Caswell-Jin JL, Freedman RA, Hassett MJ et al. Optimal adjuvant chemotherapy and targeted therapy for early breast cancer—CDK4/6 inhibitors: ASCO rapid guideline update clinical insights. JCO Oncol. Pract. 21(3), 287–291 (2025).
45.
National Comprehensive Cancer Network. NCCN Clinical PracticeGuidelines. Breast Cancer Version 4.2025. (Accessed: 10 May 2025).
46.
Tarantino P, Rugo HS, Curigliano G et al. Characteristics of real-world (RW) NATALEE and monarchE eligible populations: a US electronic health records (EHR) database analysis. Ann. Oncol. 35(Suppl. 2), Abstract 245P (2024).
47.
Barrios CH, Harbeck N, Hortobagyi GN et al. NATALEE update: safety and treatment (tx) duration of ribociclib (RIB) + nonsteroidal aromatase inhibitor (NSAI) in patients (pts) with HR+/HER2- early breast cancer (EBC). ESMO Open 9(Suppl. 4), Abstract 113MO (2024).
48.
Harbeck N, Jacot W, Ezquerra MB et al. Descriptive analysis of hepatic safety for patients (pts) with HR+/HER2- breast cancer (BC) treated with ribociclib (RIB) + endocrine therapy (ET). ESMO Open 9(Suppl. 4), Abstract 277P (2024).
49.
Cardoso F, Rihani J, Harmer V et al. Quality of life and treatment-related side effects in patients with HR+/HER2- advanced breast cancer: findings from a multicountry survey. Oncologist 28(10), 856–865 (2023).
• Presents results of a survey of oncologists, nurses and patients with HR+/HER2- advanced BC on the impact of side effects on quality-of-life in clinical settings.
50.
Harmer V, Ammendolea C, Ryan M et al. Patient preferences for HR+/HER2- early breast cancer adjuvant treatment: a multicountry discrete choice experiment. Breast Care (Basel) 20(1), 16–26 (2025).
51.
Phillippo DM, Dias S, Elsada A et al. Population adjustment methods for indirect comparisons: a review of National Institute for Health and Care Excellence technology appraisals. Int. J. Technol. Assess. Health Care 35(3), 221–228 (2019).
52.
Phillippo D, Ades T, Dias S et al. NICE DSU technical support document 18: methods for population-adjusted indirect comparisons in submissions to NICE (Appendix D). (2016). Available at: https://research-information.bris.ac.uk/files/94868465/Appendix_D_Worked_example_of_MAIC_and_STC.pdf (Accessed 10 May 2025).
53.
National Institute for Health and Care Excellence Draft Guidance 2025. Ribociclib with an aromatase inhibitor for adjuvant treatment of hormone receptor-positive, HER2-negative early breast cancer [ID6153]. Available at: https://www.nice.org.uk/guidance/GID-TA11090/documents/draft-guidance (Accessed 10 July 2025).
54.
Rugo HS, Harmer V, O'Shaughnessy J et al. Quality of life with ribociclib versus abemaciclib as first-line treatment of HR+/HER2- advanced breast cancer: a matching-adjusted indirect comparison. Ther. Adv. Med. Oncol. 15, 17588359231152843 (2023).
55.
Shao H, Zhao M, Guan A-J et al. A network meta-analysis of efficacy and safety for first-line and second/further-line therapies in postmenopausal women with hormone receptor-positive, HER2-negative, advanced breast cancer. BMC Medicine 22(1), 13 (2024).
56.
Jhaveri K, O'Shaughnessy J, Fasching PA et al. Matching-adjusted indirect comparison of PFS and OS comparing ribociclib plus letrozole versus palbociclib plus letrozole as first-line treatment of HR+/HER2- advanced breast cancer. Ther. Adv. Med. Oncol. 15, 17588359231216095 (2023).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 29 May 2025
Accepted: 23 July 2025
Published online: 29 August 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Matching-adjusted indirect comparison of ribociclib + nonsteroidal aromatase inhibitor versus abemaciclib + endocrine therapy in hormone receptor-positive/HER2-negative early breast cancer. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0082
Export citation
Select the citation format you wish to export for this article or chapter.