Cost-per-response of Acthar Gel versus standard of care for the treatment of noninfectious keratitis: a United States healthcare perspective
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Persistently active noninfectious keratitis can lead to permanent corneal damage and loss of vision. Given the limited treatment options, Acthar Gel, a US FDA-approved treatment for ocular inflammatory conditions, can be a potential therapy. This study evaluated the cost-per-response of Acthar® Gel compared with standard of care ([SoC]; adalimumab or infliximab) for noninfectious keratitis from a US healthcare payer perspective over 1–3 years. Materials & methods: A probabilistic, cohort-level state-transition decision-analytic model was developed to assess the economic value of Acthar Gel. The model simulated the treatment pathway over 3 years, divided into 3-month cycles. Patients started with active keratitis and received Acthar Gel or SoC. Based on treatment success, patients transitioned between relapse, response and no-response states, with no response potentially leading to complications. Clinical parameters for Acthar Gel were derived from a phase IV open-label study and for SoC from observational studies. Healthcare resource utilization and costs were derived from administrative claims data or published literature. Results: Over 1 year, Acthar Gel demonstrated a lower cost per response ($167,928) than SoC, adalimumab ($228,450) and infliximab ($195,083). This benefit for Acthar Gel over SoC was sustained for 2 and 3 years. Acthar Gel, despite having a higher acquisition cost than SoC, had lower disease management costs and incurred no treatment-related (administration, monitoring or adverse event) costs over 1 year. Acthar Gel also demonstrated a lower overall cost of care than SoC at 2 and 3 years. Further, Acthar Gel had higher response rates versus SoC over 1–3 years. Acthar Gel was a dominant treatment option versus SoC at 2 and 3 years. Conclusion: From a US healthcare payer perspective, Acthar Gel may be a cost-effective, value-based treatment option for appropriate patients with noninfectious keratitis.
Plain language summary
What is this article about?
This study explores the cost–effectiveness of Acthar Gel compared with standard treatments for difficult-to-treat inflammatory form of keratitis, a serious eye condition. Keratitis, when persistently active, can lead to permanent corneal damage and vision loss. Acthar Gel is a medication approved for treating noninfectious keratitis. This study specifically examined whether Acthar Gel provides better value for money than standard treatments, including adalimumab or infliximab, for patients in the US who have ongoing, long-lasting noninfectious keratitis. The study analyzed the costs and effectiveness of these treatments over 1–3 years from the healthcare payers’ perspective.
What were the results?
Acthar Gel demonstrated a lower cost per response than standard of care treatments over 1–3 years. It was more effective at controlling active noninfectious keratitis and had lower overall treatment costs over 3 years than the standard of care.
What do the results mean?
Acthar Gel is a cost-effective option, primarily due to its higher response rate and subsequent reduction in healthcare resource utilization. Acthar Gel minimized the need for additional interventions, hospitalizations, outpatient services, physician office visits and treatment-related toxicity. The findings may assist clinicians and payers in supporting evidence-based decision-making when selecting an optimal choice for treating noninfectious keratitis for appropriate patients.
Noninfectious keratitis is an often painful inflammation of the cornea that can result from various causes, including dry eye, local injury (e.g., prolonged use of contact lenses), or an ocular manifestation of underlying systemic autoimmune disorders (e.g., rheumatoid arthritis and systemic lupus erythematosus), although it may be relatively painless in many rheumatoid arthritis cases [1–3]. The clinical presentation can vary, but common symptoms include pain, photophobia, redness, tearing and visual disturbance [2,4]. Persistently active noninfectious keratitis with repeated and long-lasting episodes can lead to severe complications such as permanent corneal damage and loss of vision [2,4]. Further, patients with severe keratitis and underlying concomitant systemic inflammatory conditions may also develop complications, such as corneal neovascularization, scarring or thinning, keratinization of the ocular surface, or sterile or microbial ulceration of the cornea with possible perforation [2,5].
Timely management of noninfectious keratitis with appropriate treatments is crucial for preserving vision and improving quality of life. Management of noninfectious keratitis primarily focuses on symptom control and prevention of corneal damage [6]. Noninfectious keratitis can be managed with topical lubricants, topical cyclosporine, lifitegrast, topical or systemic corticosteroids and immunosuppressants [6]. There are limited treatment options for severe and persistent keratitis that is difficult to treat [2], other than systemic corticosteroids and systemic immunosuppressants [3,6]. However, these treatments have unfavorable safety profiles [7–9]. Therefore, alternative treatments are needed for patients with noninfectious keratitis.
Acthar® Gel (repository corticotropin injection, Mallinckrodt Pharmaceuticals) is approved by the US FDA for the treatment of severe acute and chronic allergic and inflammatory processes involving the eye and its adnexa such as keratitis, iritis, iridocyclitis, diffuse posterior uveitis and choroiditis, optic neuritis, chorioretinitis or anterior segment inflammation [10]. Acthar Gel is a naturally sourced complex mixture of adrenocorticotropic hormone analogues and other pituitary peptides that interacts with all five melanocortin receptors [10]. Thus, its therapeutic effects in noninfectious keratitis may be attributed to activating several potential anti-inflammatory pathways through both glucocorticoid-dependent and independent mechanisms [10]. Acthar Gel may help appropriate patients with persistent and active systemic inflammatory disorders that have not responded to conventional therapies [11]. A recent consensus panel recommended Acthar Gel for treating keratitis in patients with underlying inflammatory disorders, noting its preferable side effect profile [3]. Further, in a phase IV multicenter, open-label study, Acthar Gel was shown to be an important treatment option for appropriate patients with noninfectious keratitis that has not improved with other conventional therapies [2]. However, studies have not examined the economic value of Acthar Gel in noninfectious keratitis.
Interventions must be evaluated using data on clinical outcomes, healthcare resource utilization (HCRU) and costs for clinicians and payers to make informed decisions. This study assessed the cost per response of Acthar Gel compared with the standard of care ([SoC]; adalimumab or infliximab) for noninfectious keratitis from a US healthcare payer perspective over 1–3 years.
Materials & methods
Model structure
A probabilistic, cohort-level state-transition decision-analytic model was developed to assess the economic value of Acthar Gel. This model simulated patient progression through different health states, accounting for uncertainties in the input data. Specifically, the model compared the cost per response of Acthar Gel to SoC (tumor necrosis factor-alpha [TNF-α] inhibitors [adalimumab and infliximab]) for moderate-to-severe refractory noninfectious keratitis that failed conventional treatments. TNF-α inhibitors were selected as comparators based on current recommendations for noninfectious keratitis [3]. However, it is important to note that their use for noninfectious keratitis in the US is off-label [12,13]. Therefore, the FDA has not established the efficacy and safety of adalimumab or infliximab for this indication. The analysis was performed from a US healthcare payer perspective, spanning a 1- to 3-year timeframe. The model was developed using Microsoft® Excel 2024.
The model simulated the treatment pathway for patients with active keratitis, divided into 3-month cycles (Figure 1). For this model, active keratitis was considered the relapse state. Initially, all patients began in the ‘active keratitis’ state and received either Acthar Gel or SoC. At the end of each 3-month cycle, treatment response was assessed. Based on the probability of treatment success, patients in the relapse state could remain in the relapse state, move to a response state or move to a no-response state. Patients could experience sustained response, relapse or no response if a response was achieved. Patients who responded to Acthar Gel discontinued treatment, while those responding to SoC continued maintenance therapy as per treatment recommendations. If relapse was not resolved, patients remained on their respective treatments and were reassessed for response in the subsequent cycle. Patients who experienced a relapse returned to the ‘active keratitis’ state and received further treatment. Critically, patients in the ‘no response’ state could develop keratitis-related complications. The simulated patient population remained constant throughout the 3-year timeframe. No patient attrition, such as mortality, was modeled. Costs were tracked for each patient within each state (response, no response, relapse, complications) at the end of every 3-month cycle.
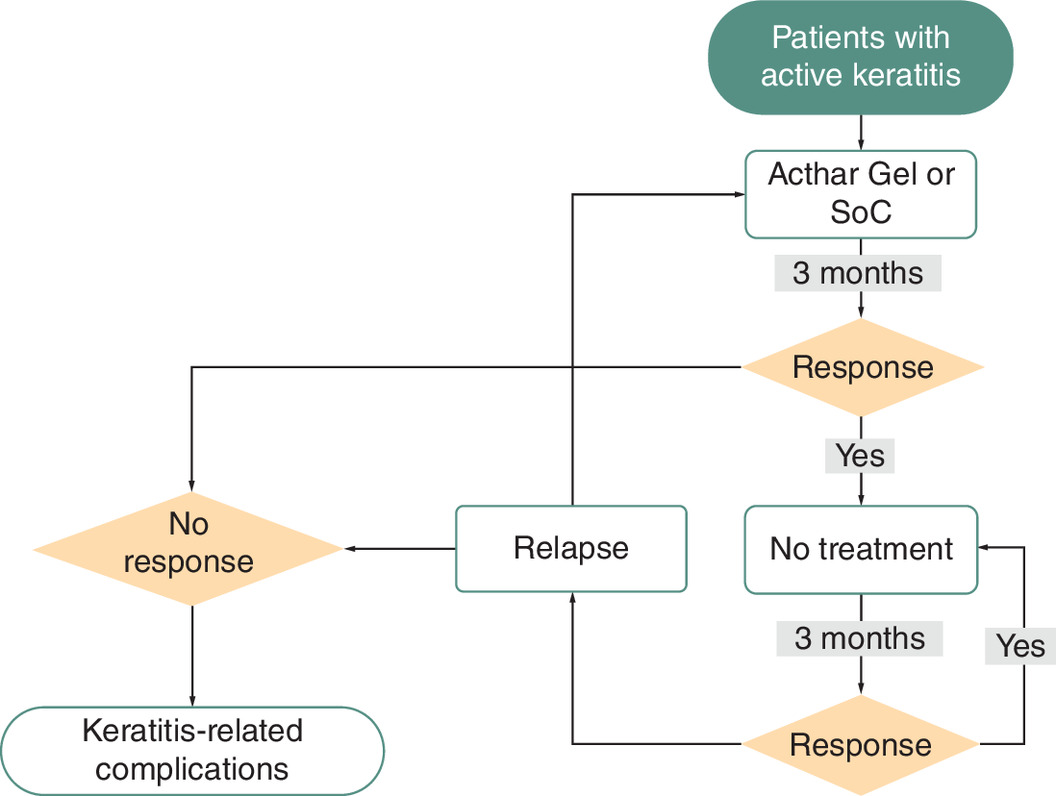
Figure 1. Schematic of the probabilistic cohort-level state-transition decision-analytic model.
SoC: Standard of care.
Model inputs
Clinical inputs
Clinical effectiveness data for Acthar Gel were obtained from a phase IV, open-label, multicenter study conducted at eight US sites (ClinicalTrials.gov: NCT04169061) [Table 1] [2]. This study enrolled adults with a confirmed diagnosis of noninfectious keratitis, excluding bacterial or viral causes, who had experienced severe keratitis unresponsive to or intolerant of topical cyclosporine or lifitegrast. Participants were not allowed to use the following treatments during the study period: corticosteroids (topical, inhaled, intra-articular, intraocular or systemic), systemic immunosuppressants, immunomodulators or systemic biologic agents. Patients self-administered 80 U of Acthar Gel subcutaneously twice weekly for 12 weeks [2]. The primary study endpoint was the proportion of patients achieving a ≥12-point improvement in the symptom bother domain of the Impact of Dry Eye on Everyday Life (IDEEL) Questionnaire at week 12. This 12-point improvement threshold was selected based on the minimal clinically meaningful difference proposed by Fairchild et al. [14]. The clinical response data used in the model were derived from the modified intent-to-treat population, which included all patients who received ≥1 dose of Acthar Gel and provided post-baseline efficacy data [2]. The response was defined by improvement in the IDEEL questionnaire’s symptom bother domain. The observed response rates were 52.9% at week 2, 52.9% at week 4, 55.9% at week 6 and 50.0% at week 12 [2]. Treatment failure was defined as the progression of keratitis symptoms (from mild to moderate or moderate to severe) or presence of severe keratitis at baseline among patients with no response to treatment [2].
| Parameters† | Value | Source | Ref. |
|---|---|---|---|
| Acthar Gel | |||
| Probability of response | 50.0% | Wirta et al. | [2] |
| Probability of treatment failure‡ | 29.4% | Data on File¶ | |
| Probability of relapse | 3.8% | Data on File¶ | |
| Adalimumab | |||
| Probability of response | 41.2% | Arcinue et al. | [15] |
| Probability of treatment failure‡ | 33.0% | Sharma et al. | [16] |
| Probability of on-treatment failure§ | 2.2% | Tang Lee Say et al. | [17] |
| Probability of relapse | 7.4% | Eurelings et al. | [18] |
| Infliximab | |||
| Probability of response | 37.9% | Calculated# | |
| Probability of treatment failure‡ | 22.2% | Sobrin et al. | [19] |
| Probability of on-treatment failure§ | 4.7% | Kruh et al. | [20] |
| Probability of relapse | 5.3% | Sharma et al. | [16] |
†
All parameters from the literature were converted to a 3-month probability, where applicable.
‡
Treatment failure during the induction phase, often termed ‘primary non-response’, occurs when a patient fails to demonstrate a significant clinical improvement following the full course of the prescribed initial treatment.
§
On-treatment failure, also known as secondary loss of response, refers to patients who initially respond to induction therapy but subsequently lose that response during maintenance treatment. This is relevant for therapies like adalimumab and infliximab, which require ongoing maintenance to sustain clinical benefit.
¶
Data on file (Mallinckrodt Pharmaceuticals): derived from phase IV open-label study.
#
Calculated using response rate for adalimumab and odds ratio of improvement with infliximab vs adalimumab; odds ratio sourced from Liu et al. [21].
Effectiveness data for adalimumab or infliximab were obtained from published studies on noninfectious ocular inflammatory conditions, as these agents are used to treat such conditions by targeting TNF-α, a key inflammatory cytokine (Table 1) [3,12,13]. TNF-α inhibitors are less established for keratitis than uveitis or scleritis, but these conditions share similar inflammatory pathways [12,13,22,23]. Therefore, data from broader ocular inflammatory conditions were used. Adalimumab response rates were derived from a retrospective study of patients with ocular inflammatory disease; the response was calculated from the reported improvement in inflammation [15]. Infliximab response was estimated using adalimumab response data and an odds ratio from a meta-analysis comparing these two agents in ocular inflammatory conditions [21]. Treatment failure probabilities for both adalimumab and infliximab were sourced from prospective cohort studies [16,19]. On-treatment failure (treatment change or discontinuation due to ineffectiveness) was derived from a retrospective chart review of refractory uveitis patients [17,20]. Relapse data were obtained from a retrospective study on adalimumab [18] and a prospective study on infliximab [16].
Relapse severity was determined using baseline data from the phase IV open-label study on Acthar Gel [2]. The severity of symptoms, as measured by the IDEEL questionnaire’s symptom bother domain, was categorized as follows: none (0–16), mild (17–38), moderate (39–65) and severe (66+) [24]. The probability of mild relapse was 2.9%, moderate relapse 52.9% and severe relapse 44.1%. It was assumed that the distribution of relapse severity was the same for both Acthar Gel and SoC.
Data on ophthalmic complications associated with noninfectious inflammatory keratitis was obtained from Symphony Health’s Integrated Dataverse anonymized patient-level data (1 January 2016 to 1 January 2023). At least one complication was observed in 49.4% of patients with noninfectious keratitis. Among patients with complications, 2.6% experienced blindness, 29.6% developed cataracts, 1.4% had cystoid macular degeneration, 20.8% had glaucoma, 2.2% experienced retinal detachment and 14.4% reported visual disturbances.
Serious adverse events were only considered in the economic evaluation. For TNF-α inhibitors, the probability of severe infection and the distribution of infection type were considered; based on a retrospective cohort study, 4.2% of infections require hospitalization [9]. Hospitalized patients with infections showed the following distribution: respiratory infections: 45.3%, gastrointestinal infections: 16.3%, sepsis: 9.3%, skin and soft tissue infections: 6.2%, tuberculosis: 3.1%, herpetic infections: 2.8%, septic arthritis: 2.4%, urinary tract infections: 2.4% and other infection types: 9.3% [16]. Based on a meta-analysis, infliximab has 1.65 times higher odds of adverse events versus adalimumab and was thus accounted for in the model [21]. For infliximab, the probability of anaphylaxis was 3.0%, and severe infusion-related reaction was 9.0% [16]. In a Phase IV open-label study of Acthar Gel, no serious adverse events were reported [2]; consequently, serious adverse events were not factored into the analysis for Acthar Gel.
Healthcare resource utilization & cost inputs
Wholesale acquisition costs (WAC) for Acthar Gel and SoC drugs, as of 1 January 2025, were obtained from the Micromedex Red Book (Merative, Ann Arbor, MI) [25]. The WAC for a 5 ml multidose vial of Acthar Gel is $45,304. Based on 2023 specialty pharmacy dispensing data, the average use per patient was 7.81 vials in the 12 months ending 31 December 2023. The total cost of SoC medications was calculated using dosing, strength and WAC; dosing information on adalimumab [26] and infliximab [19,27] was sourced from the prescribing information and literature. Because biosimilars are available for these TNF-α inhibitors, the cost calculation incorporated the market share of biologics and their respective biosimilars. The annual cost of adalimumab was $88,458 and infliximab was $42,541.
Drug administration and monitoring costs were derived from the published literature. Administration costs were only applied to infliximab, as it is administered via intravenous infusion, with an administration cost of $636 per infusion [28]. Monitoring costs were $480 for both adalimumab and infliximab [28].
Costs related to adverse events were obtained from published literature. The costs per event for various infection types were as follows: respiratory infections: $18,547 [29], gastrointestinal infections: $7214 [30], sepsis: $24,489 [31], skin and soft tissue infections: $3676 [32], tuberculosis: $18,984 [33], herpetic infections: $189 [34] septic arthritis: $51,785 [35], urinary tract: $8128 [36] and other infections (assumed based on the average of other infection types), $16,626. Anaphylaxis was assigned a cost of $26,773 per event [37]. Severe infusion-related reactions were assigned a cost of $9386 per event [38].
HCRU and costs related to noninfectious keratitis included medications for keratitis management, eye-related procedures/surgical interventions, disease management costs (inpatient, emergency room visits, physician office visits, other outpatient visits and home health agencies for blindness/low vision), corticosteroid-related toxicity and medications for pain and depression (Table 2). HCRU and costs were derived from Symphony Health’s Integrated Dataverse (1 January 2016 to 1 January 2023) and published literature [8,39–45].
| Parameters | Utilization, patients (%) | Annual costs† | ||
|---|---|---|---|---|
| Other treatments | Without complication | With ≥1 complication | Without complication | With ≥1 complication |
| Other keratitis-related medications‡ | ||||
| Artificial tears | 2.4% | 3.0% | $193 | $145 |
| Immunosuppressives | 5.1% | 7.3% | $4304 | $4628 |
| Ophthalmic treatments | 12.9% | 14.1% | $667 | $662 |
| Ophthalmic corticoids | 22.1% | 28.7% | $443 | $557 |
| Systemic corticosteroids | 19.2% | 20.6% | $125 | $122 |
| Targeted synthetic DMARDs | 0.1% | 0.1% | $46,179 | $46,754 |
| Eye-related procedures‡ | ||||
| Punctal plugs | 2.56% | 5.01% | $3816 | $4470 |
| Amniotic membrane (on ocular surface) | 1.33% | 2.67% | $14,151 | $17,238 |
| Tear film imaging | 0.02% | 0.02% | $226 | $187 |
| Closure of the lacrimal punctum by thermocauterization, ligation or laser | 0.27% | 0.52% | $3422 | $3719 |
| Dilation of lacrimal punctum | 0.09% | 0.18% | $3889 | $4637 |
| Meibography | 0.00% | 0.01% | $0 | $263 |
| Anterior segment photography | 6.37% | 9.87% | $1063 | $1283 |
| Unlisted ophthalmological service or procedure | 0.10% | 0.14% | $10,616 | $7349 |
| Tear osmolarity | 0.54% | 0.83% | $310 | $369 |
| Meibomian gland expression | 0.10% | 0.14% | $10,616 | $7349 |
| Intense pulsed light therapy | 0.01% | 0.03% | $12,146 | $5567 |
| Surgical cautery occlusion of the lacrimal drainage system | 0.27% | 0.52% | $3422 | $3719 |
| Surgical interventions‡ | ||||
| Corneal or corneoscleral patching for an impending or frank perforation | 0.05% | 0.1% | $14,183 | $21,031 |
| Cataract surgery | 0.00% | 7.9% | $20,706 | $25,312 |
| Retinal procedure | 0.90% | 4.4% | $12,143 | $14,728 |
| LASIK/refractive surgery | 0.17% | 0.3% | $12,152 | $8752 |
| Glaucoma surgery | 0.00% | 0.2% | $0 | $29,105 |
| Corneal transplant§ | – | 2.6% | – | $38,818 |
| Pain and depression medications | ||||
| NSAIDs¶ | 16.9% | 24.7% | $204 | $204 |
| Opioids# | – | 3.6% | – | $4071 |
| Antidepressants†† | 16.9% | 33.0% | $345 | $345 |
| Disease management | ||||
| Keratitis-related‡ | ||||
| Inpatient admission | 10.4% | 13.4% | $22,998 | $35,178 |
| Emergency room visit | 18.0% | 20.3% | $6818 | $7273 |
| Office visit | 11.1% | 15.3% | $4063 | $5338 |
| Other outpatient visits | 45.0% | 66.6% | $18,292 | $29,638 |
| Non-keratitis-related‡ | ||||
| Inpatient admission | 18.1% | 19.8% | $62,745 | $109,875 |
| Emergency room visit | 46.2% | 32.4% | $7644 | $8351 |
| Office visit | 26.6% | 29.3% | $9110 | $9984 |
| Other outpatient visits | 88.1% | 94.9% | $29,765 | $43,195 |
| Home health agencies‡‡ | ||||
| Blindness | – | 2.6% | – | $8661 |
| Low vision | – | 46.8% | – | $5392 |
| Medication toxicity | ||||
| Systemic CS§§,¶¶ | 19.2% | – | $87,592 | – |
†
All costs inflated to 2025 US Dollars.
‡
Data on File (Mallinckrodt Pharmaceuticals): HCRU and costs derived from Symphony Health's Integrated Dataverse (1 January 2016 to 1 January 2023).
§
HCRU sourced from Symphony Health’s Integrated Dataverse (1 January 2016 to 1 January 2023); cost sourced from Bentley et al. [40].
‡‡
HCRU sourced from Symphony Health’s Integrated Dataverse (1 January 2016 to 1 January 2023); cost sourced from Koberlein et al. [39].
§§
HCRU sourced from Symphony Health’s Integrated Dataverse (1 January 2016 to 1 January 2023); cost sourced from Rice et al. [8].
¶¶
Systemic CS toxicity costs were applied only to the SoC arm during relapse because SoC patients receive concomitant CS for immunosuppression, which may continue into the response state following a severe relapse. Acthar Gel patients, as per the phase IV open-label study [2], did not use concomitant CS, eliminating the need to model related toxicity. In the no-response state, CS-related toxicity was not separately modeled for either arm, as nonkeratitis management, which includes potential CS use, was already accounted for in the overall cost calculations.
CS: Corticosteroid; DMARD: Disease-modifying antirheumatic drug; HCRU: Healthcare resource utilization; LASIK: Laser-assisted in situ keratomileusis; NSAID: Non-steroidal anti-inflammatory drug; SoC: Standard of care.
All costs were standardized to 2025 US Dollars whenever applicable. Costs not initially reported in 2025 US Dollars were adjusted using the US Consumer Price Index for medical care services for urban consumers [46]. Unless otherwise stated, all costs were discounted at a rate of 3.5%.
Cost per response analysis
The primary outcome (base case) was the cost per response for Acthar Gel and SoC over 1 year, estimated by dividing the total mean cost of care per patient by the proportion of patients with resolved relapse for each treatment. Cost per response was also assessed at 2 and 3 years. In addition, incremental cost-per-response, calculated by dividing the difference in each intervention’s total cost of care (incremental cost) by the difference in the proportion of patients with responses for each intervention (incremental response) over the specified time horizon, was also assessed.
Sensitivity analyses were conducted for the cost per response for Acthar Gel versus SoC over 1 year. Model inputs and base case assumptions were evaluated using one-way deterministic sensitivity analysis and multivariable probabilistic sensitivity analysis. The deterministic sensitivity analysis varied effectiveness data by ±20%, complications and relapse severity by ±30%, drug acquisition costs by ±10% and HCRU-related costs by ±25%. The probabilistic sensitivity analysis employed 5000 iterations, simulating parameter values from predefined probability distributions to assess joint uncertainty. The choice of distributions was guided by the data’s nature and limitations, effectively capturing the full spectrum of potential uncertainty.
Results
Over 1 year, Acthar Gel demonstrated a lower cost per response ($167,928) compared with adalimumab ($228,450) and infliximab ($195,083) (Figure 2). Specifically, Acthar Gel resulted in a $11,165 lower total cost of care per patient and a 15.3% higher response rate than adalimumab (Figure 3). Compared with infliximab, Acthar Gel, while costing $8765 more per patient, yielded a 15.1% higher response rate. Acthar Gel, despite having a $18,406 higher drug acquisition cost than adalimumab and a $65,546 higher drug acquisition cost than infliximab, resulted in lower overall medical costs and incurred no treatment-related (administration/monitoring and adverse events) costs over 1 year.
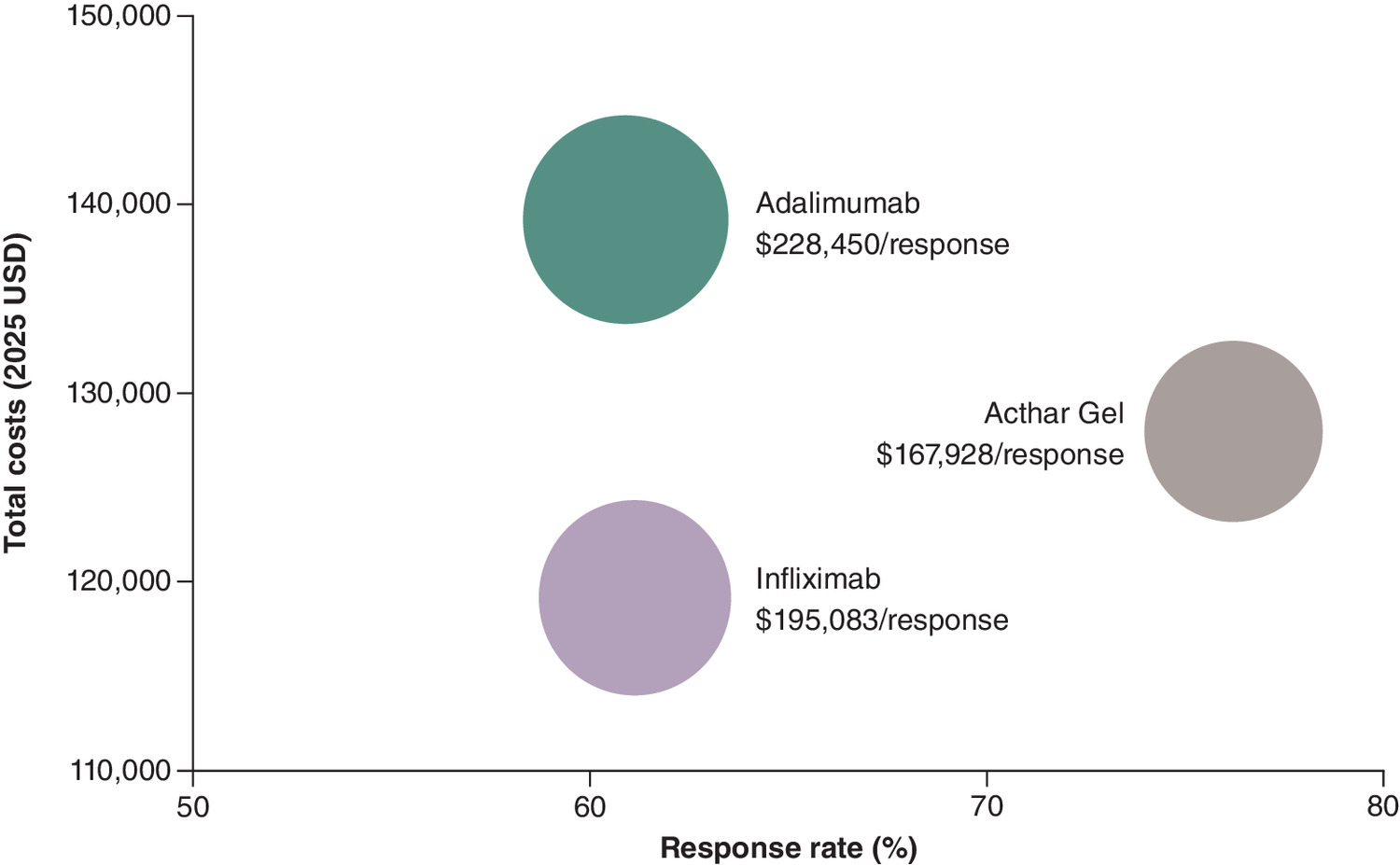
Figure 2. Cost per response over 1 year from a US payer perspective.
Results are presented on a per-person basis; all costs inflated to 2025 US Dollars.
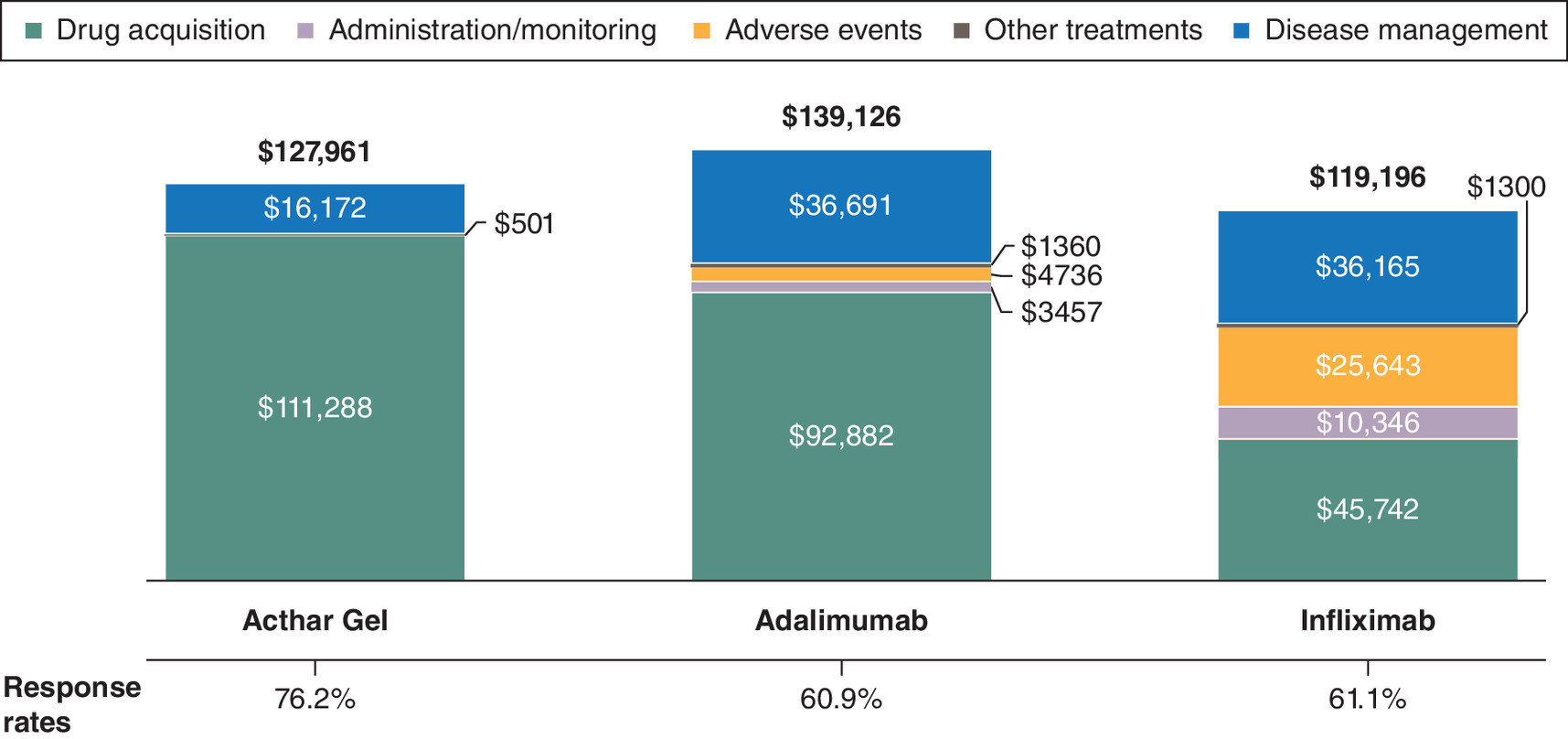
Figure 3. Overall cost of care and response rate over 1 year from a US payer perspective.
All costs inflated to 2025 US Dollars. Results are presented on a per-person basis. Other treatments include keratitis-related medication, procedures and surgery, as well as pain and depression-related medications. Disease management includes keratitis- and nonkeratitis-related inpatient, outpatient, physician office visits, emergency room and home health agency services as well as systemic corticosteroid-related toxicity.
This study also assessed cost per response over a timeframe of 2 and 3 years. This cost per response advantage for Acthar Gel over adalimumab or infliximab was sustained at 2 and 3 years (Table 3). Acthar Gel demonstrated lower overall cost of care and higher response rates compared with adalimumab or infliximab at 2 and 3 years. The overall cost of care patterns at 2 and 3 years were consistent with those observed at 1 year (Table 4).
| Timeframe and Intervention | Costs per patient | Response rate | Cost-per-response† |
|---|---|---|---|
| 2 years | |||
| Acthar Gel | $154,277 | 72.3% | $213,385 |
| Adalimumab | $225,846 | 49.6% | $455,335 |
| Infliximab | $194,286 | 48.6% | $399,765 |
| 3 years | |||
| Acthar Gel | $181,079 | 68.5% | $264,349 |
| Adalimumab | $304,173 | 40.1% | $758,536 |
| Infliximab | $263,970 | 37.6% | $702,048 |
†
Results are presented on a per-person basis.
| Cost components†,‡ | Acthar Gel | Adalimumab | Infliximab |
|---|---|---|---|
| 2 years | |||
| Drug acquisition | $119,754 | $140,583 | $68,480 |
| Administration/monitoring | $0 | $4444 | $14,724 |
| Adverse events | $0 | $6088 | $36,662 |
| Other treatments§ | $1221 | $2963 | $2914 |
| Disease management¶ | $33,302 | $71,768 | $71,506 |
| 3 years | |||
| Drug acquisition | $126,846 | $175,595 | $84,270 |
| Administration/monitoring | $0 | $5157 | $17,750 |
| Adverse events | $0 | $7065 | $44,283 |
| Other treatments§ | $2020 | $4747 | $4765 |
| Disease management¶ | $52,213 | $111,609 | $112,902 |
†
Results are presented on a per-person basis.
‡
All costs inflated to 2025 US Dollars.
§
Other treatments include keratitis-related medication, procedures and surgery, as well as pain and depression related medications.
¶
Disease management includes keratitis- and nonkeratitis-related inpatient, outpatient, physician office visits, emergency room and home health agency services, as well as systemic corticosteroid-related toxicity.
Acthar Gel emerged as a dominant treatment option compared with adalimumab over 1 year, exhibiting lower costs and higher response rates (Table 5). This dominance was also observed at 2 and 3 years against adalimumab or infliximab.
| Timeframe and Intervention | Incremental costs†,‡ | Incremental response | Incremental cost-per-response†,‡ |
|---|---|---|---|
| 1 year | |||
| Acthar Gel vs adalimumab | -$11,165 | 15.3% | Dominant |
| Acthar Gel vs infliximab | $8765 | 15.1% | $58,046 |
| 2 years | |||
| Acthar Gel vs adalimumab | -$71,569 | 22.7% | Dominant |
| Acthar Gel vs infliximab | -$40,009 | 23.7% | Dominant |
| 3 years | |||
| Acthar Gel vs adalimumab | -$123,094 | 28.4% | Dominant |
| Acthar Gel vs infliximab | -$82,891 | 30.9% | Dominant |
†
All costs inflated to 2025 US Dollars.
‡
Results are presented on a per-person basis.
The deterministic sensitivity analysis identified the major contributors to cost per response over 1 year. For Acthar Gel versus adalimumab, the major contributors to cost per response were the Acthar Gel response rate and drug acquisition cost of both treatments. For Acthar Gel versus infliximab, the major contributors to cost per response were the response rate of both treatments and the drug acquisition cost of Acthar Gel (Figure 4).
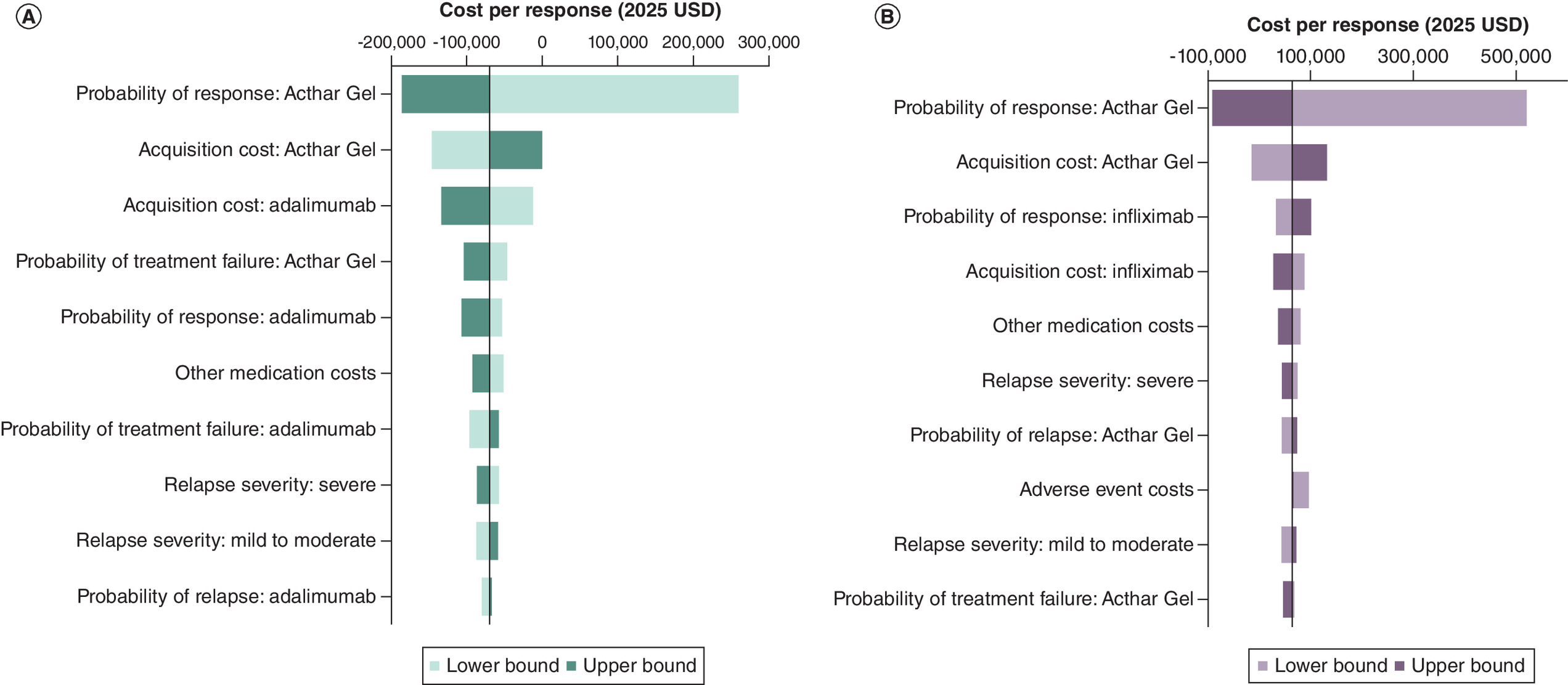
Figure 4. Key drivers of cost per response based on deterministic sensitivity analysis of Acthar Gel versus adalimumab and infliximab over 1 year from a US payer perspective.
(A) Adalimumab. (B) Infliximab. Bars represent the variation in the cost per response corresponding to high and low variation on a parameter’s point estimate. The ‘lower bound’ represents the model outcome when a specific parameter is set to its minimum value within the specified range, while holding all other parameters at their base or central values. The ‘upper bound’ represents the model outcome when a specific parameter is set to its maximum value within the specified range, while holding all other parameters at their base or central values. The vertical line dividing the lower and upper bound bars represents the base case cost per response when all inputs are set to their base case estimates. Parameters are presented in a ranked order, with the most influential variables at the top. The length of the bars represents the magnitude of impact, and their direction (left or right) indicates whether the impact is positive or negative. If the impact of an input is positively related, then increasing the input estimate increases the cost per response (upper bound bar extends to the right; lower bound bar to the left) and vice versa. Conversely, if the impact of an input is negatively related, then increasing the input estimate decreases the cost per response (upper bound bar extends to the left; lower bound bar to the right) and vice versa.
CPR: Cost-per-response.
The probabilistic sensitivity analysis showed that, at a willingness-to-pay threshold of $150,000 per response over 1 year, Acthar Gel was cost-effective in 92.3% of iterations versus adalimumab and in 72.7% of iterations versus infliximab (Figure 5).
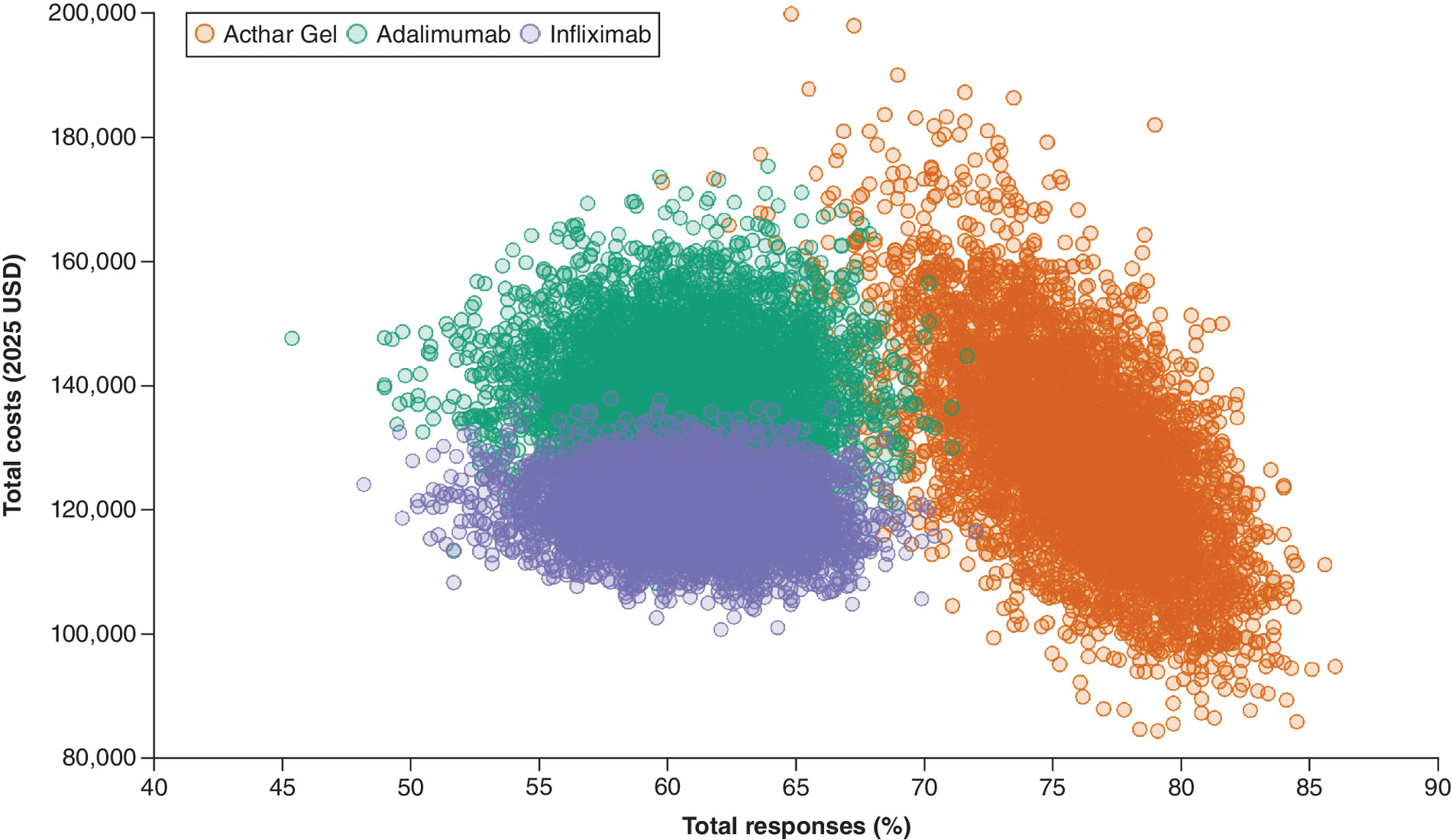
Figure 5. Scatter plot of Acthar Gel versus adalimumab or infliximab over 1 year from a US payer perspective.
All costs inflated to 2025 US Dollars.
Discussion
Persistently active noninfectious keratitis, characterized by recurrent and prolonged episodes, can result in severe complications, including permanent corneal damage and vision loss [2,4]. Given the limited treatment options for noninfectious keratitis, Acthar Gel, an FDA-approved treatment for ocular inflammatory conditions, has emerged as a potential therapy [10]. A phase IV open-label study evaluated its safety and effectiveness in patients unresponsive to conventional treatments [2]. While TNF-α inhibitors are also used off-label for this condition, observational studies and randomized controlled trials for keratitis are lacking [12,13]. This study represents the first economic evaluation comparing the clinical benefits and costs of Acthar Gel to unapproved treatments for noninfectious keratitis in the US from a payer perspective.
This cost per response analysis, conducted over a 1–3-year period, revealed that Acthar Gel exhibited a lower cost per response compared with unapproved SoC, specifically adalimumab or infliximab. This finding remained consistent across various sensitivity analyses. The deterministic sensitivity analysis indicated that the response rate of Acthar Gel was the primary driver of its lower cost per response compared with SoC. Furthermore, Acthar Gel was identified as a dominant strategy, exhibiting lower costs and higher response rates over 2 and 3 years. Despite its higher acquisition cost, Acthar Gel resulted in lower direct medical costs than SoC throughout the evaluation period. This cost reduction with Acthar Gel was attributed to its decreased utilization of keratitis-related medications, procedures/surgery, pain/depression medications, and disease management resources (inpatient, emergency room visits, physician office visits, other outpatient visits and home health agencies for blindness/low vision). Notably, Acthar Gel incurred no treatment-related costs for administration, monitoring or adverse events, further contributing to its cost–effectiveness.
The management of noninfectious keratitis focuses on symptom relief, improved patient health and minimizing HCRU and its associated financial burden. In addition, effective healthcare decision-making requires evaluating treatments based on their ability to deliver positive outcomes in a cost-efficient manner [47]. This study underscores the critical role of improved response rate with Acthar Gel as a key contributor in determining cost per response for refractory noninfectious keratitis. The higher response rate observed with Acthar Gel versus unapproved SoC (adalimumab or infliximab) directly resulted in lower HCRU and overall costs despite the higher drug acquisition cost. This emphasizes the potential for treatments with better response rates to achieve treatment goals and provide cost savings for healthcare systems. Furthermore, the acquisition cost of Acthar Gel is also one of the major contributors to this economic evaluation. The observed lower cost per response of Acthar Gel versus SoC can present a significant financial advantage. This economic benefit can be further amplified through strategic pricing mechanisms, such as rebates and discounts, that can translate directly into an even more favorable cost per response profile of Acthar Gel. Consequently, this supports the value proposition of Acthar Gel within this analysis and positions it as a potentially value-based treatment option over SoC, offering substantial cost savings.
This economic evaluation suggests that Acthar Gel is a cost-effective option, primarily due to its higher response rate and subsequent reduction in HCRU. This decreased utilization led to lower overall healthcare costs, as the higher response rate minimized the need for additional interventions and healthcare services, offsetting its initial drug acquisition costs. This study, thus, highlights the significance of adopting a value-based approach to treatment selection, emphasizing therapies that enhance patient outcomes and optimize healthcare resource allocation.
This study contributes valuable data to the limited literature on treatment options for this challenging condition. This analysis also provides a foundation for future research, including studies exploring long-term outcomes and subgroup analyses to identify patient populations best suited for Acthar Gel. Furthermore, these findings offer clinicians and payers essential information for informed treatment decisions. Given the significant clinical and economic burden of noninfectious keratitis, treatment choices should be guided by clinical judgment, resource availability and individual patient profiles.
Several limitations should be considered when interpreting these findings. First, this cost-effectiveness analysis adopts a US payer perspective, potentially limiting its generalizability to other healthcare systems with varying treatment guidelines for noninfectious keratitis. Second, the clinical data for Acthar Gel were derived from a phase IV open-label study, which, due to its design and small sample size, may not accurately reflect real-world effectiveness and could introduce bias; furthermore, the extrapolation of 12-week study data to 2 and 3-year outcomes may affect the long-term effectiveness estimates. Third, the SoC clinical data were derived from observational studies and HCRU and costs were derived from the administrative claims data or published literature, potentially leading to under- or over-estimation of actual costs. Fourth, the precise impact of noninfectious keratitis on health and healthcare is difficult to quantify due to limited quantitative data in the literature. Fifth, potential manufacturer discounts or rebates on drug costs were not considered. Finally, the absence of head-to-head randomized controlled trials necessitates the use of indirect comparative data, and the off-label use of TNF-α inhibitors, with limited keratitis-specific studies, adds further uncertainty, despite shared inflammatory pathways with better-studied conditions like uveitis and scleritis. Nevertheless, sensitivity analyses performed to assess the impact of variations in costs and response rates showed a favorable cost per response for Acthar Gel, mitigating some of these limitations.
Conclusions
Acthar Gel is a cost-effective, value-based treatment option for appropriate patients with noninfectious keratitis from a US healthcare payer perspective. Further research is required to examine the long-term clinical effectiveness and economic benefit of Acthar Gel for noninfectious keratitis.
Summary points
•
Persistently active keratitis with repeated and long-lasting episodes can lead to permanent corneal damage and loss of vision.
•
Acthar® Gel is approved by the US FDA for the treatment of severe acute and chronic allergic and inflammatory processes involving the eye and its adnexa, such as keratitis.
•
This study evaluated the cost per response of Acthar Gel compared with standard of care for noninfectious keratitis from a US healthcare payer perspective over 1–3 years.
•
A probabilistic, cohort-level state-transition decision-analytic model was developed to assess the economic value of Acthar Gel.
•
Over 1 year, Acthar Gel demonstrated a lower cost per response ($167,928) compared with both adalimumab ($228,450) or infliximab ($195,083).
•
Acthar Gel, despite having a higher drug acquisition cost than adalimumab or infliximab, resulted in lower overall medical costs over 1 year.
•
Acthar Gel also demonstrated a lower overall cost of care and higher response rates compared with standard of care at 2 and 3 years.
•
Acthar Gel may be a cost-effective, value-based treatment option for appropriate patients with noninfectious keratitis from a US healthcare payer perspective.
•
Further research is required to examine the long-term clinical effectiveness and economic benefit of Acthar Gel for noninfectious keratitis.
Author contributions
All authors made a significant contribution to the work reported, including study conception, design, execution, acquisition of data, analysis and interpretation, and in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Financial disclosure
This study was sponsored by Mallinckrodt Pharmaceuticals (NJ, USA). The authors had complete editorial control of the paper and provided their final approval of all content. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
K Hayes, J Niewoehner and GJ Wan are employees of Mallinckrodt Pharmaceuticals. I Chopra, J Bindra and M Panaccio are paid research consultants for the study. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This economic analysis is based on data from the published literature or data from Symphony Health’s Integrated Dataverse (1 January 2016 to 1 January 2023) and, therefore, did not involve any new studies of human or animal subjects.
Data sharing statement
The data used in the current study are available within the manuscript. The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Srinivasan M, Mascarenhas J, Prashanth CN. Distinguishing infective versus noninfective keratitis. Indian J. Ophthalmol. 56(3), 203–207 (2008).
2.
Wirta D, McLaurin E, Ousler G et al. Repository corticotropin injection (Acthar® Gel) for refractory severe noninfectious keratitis: efficacy and safety from a Phase IV, multicenter, open-label study. Ophthalmol. Ther. 10(4), 1077–1092 (2021).
•• This phase IV, multicenter, open-label study evaluated the efficacy and safety of Acthar Gel in treating refractory severe noninfectious keratitis.
3.
Perez VL, Ayres B, Toyos M, Toyos R. Noninfectious keratitis: an expert panel recommendation. (2019). [cited 2024 December 23]; Available from: https://v2.evolvemeded.com/wp-content/uploads/2019/04/0319JCRS_Noninfectious-keratitis-expert-panel_013119.pdf
•• This review details the various types of noninfectious keratitis and offers management recommendations.
4.
Dargin JM, Lowenstein RA. The painful eye. Emerg. Med. Clin. North Am. 26(1), 199–216; viii (2008).
5.
Akpek EK, Amescua G, Farid M et al. Dry eye syndrome preferred practice pattern®. Ophthalmology 126(1), P286–P334 (2019).
6.
Durrani K, Zakka FR, Ahmed M et al. Systemic therapy with conventional and novel immunomodulatory agents for ocular inflammatory disease. Surv. Ophthalmol. 56(6), 474–510 (2011).
7.
Rice JB, White AG, Johnson M et al. Quantitative characterization of the relationship between levels of extended corticosteroid use and related adverse events in a US population. Curr. Med. Res. Opin. 34(8), 1519–1527 (2018).
8.
Rice JB, White AG, Johnson M et al. Healthcare resource use and cost associated with varying dosages of extended corticosteroid exposure in a US population. J. Med. Econ. 21(9), 846–852 (2018).
9.
Quartuccio L, Zabotti A, Del Zotto S et al. Risk of serious infection among patients receiving biologics for chronic inflammatory diseases: usefulness of administrative data. J. Adv. Res. 15, 87–93 (2019).
10.
Mallinckrodt Pharmaceuticals. Acthar® Gel prescribing information. (1952). (Revised October 2021). Available from: https://www.acthar.com/pdf/Acthar-PI.pdf
11.
Wan GJ, Niewoehner J, Hayes K. Acthar Gel (RCI): a narrative literature review of clinical and economic evidence. Clinicoecon. Outcomes Res. 15, 499–512 (2023).
• This narrative review summarizes evidence on Acthar Gel’s impact on clinical, health and economic outcomes across its US FDA approved inflammatory and autoimmune conditions.
12.
Pasadhika S, Rosenbaum JT. Update on the use of systemic biologic agents in the treatment of noninfectious uveitis. Biologics 8, 67–81 (2014).
13.
Durrani K, Kempen JH, Ying GS et al. Adalimumab for ocular inflammation. Ocul. Immunol. Inflamm. 25(3), 405–412 (2017).
14.
Fairchild CJ, Chalmers RL, Begley CG. Clinically important difference in dry eye: change in IDEEL-symptom bother. Optom. Vis. Sci. 85(8), 699–707 (2008).
• Investigates the 20-item IDEEL-SB’s discriminatory power about self-assessed dry eye severity and aims to define the clinically meaningful difference in its score. The IDEEL-SB was utilized by Wirta et al. to assess the effectiveness of Acthar Gel.
15.
Arcinue CA, Durrani K, Artornsombudh P et al. The efficacy and safety of adalimumab in ocular inflammatory disease. Orphan Drugs 5, 69–74 (2015).
16.
Sharma SM, Damato E, Hinchcliffe AE et al. Long-term efficacy and tolerability of TNFalpha inhibitors in the treatment of non-infectious ocular inflammation: an 8-year prospective surveillance study. Br. J. Ophthalmol. 105(9), 1256–1262 (2021).
17.
Tang Lee Say TL, Yang V, Fingret JM et al. Adalimumab in patients with vision-threatening uveitis: real-world clinical experience. BMJ Open Ophthalmol. 6(1), e000819 (2021).
18.
Eurelings LEM, Missotten T, van Velthoven MEJ et al. Long-term follow-up of patients with uveitis treated with adalimumab: response rates and reasons for discontinuation of therapy. Am. J. Ophthalmol. 240, 194–204 (2022).
19.
Sobrin L, Kim EC, Christen W et al. Infliximab therapy for the treatment of refractory ocular inflammatory disease. Arch. Ophthalmol. 125(7), 895–900 (2007).
20.
Kruh JN, Yang P, Suelves AM, Foster CS. Infliximab for the treatment of refractory noninfectious uveitis: a study of 88 patients with long-term follow-up. Ophthalmology 121(1), 358–364 (2014).
21.
Liu W, Bai D, Kou L. Comparison of infliximab with adalimumab for the treatment of non-infectious uveitis: a systematic review and meta-analysis. BMC Ophthalmol. 23(1), 240 (2023).
22.
Galor A, Thorne JE. Scleritis and peripheral ulcerative keratitis. Rheum. Dis. Clin. North Am. 33(4), 835–54; vii (2007).
23.
Sainz de la Maza M, Foster CS, Jabbur NS, Baltatzis S. Ocular characteristics and disease associations in scleritis-associated peripheral keratopathy. Arch. Ophthalmol. 120(1), 15–19 (2002).
24.
Acaster S, Verboven Y, Begley C et al. PSS32 Impact of Dry Eye on Everyday Life (IDEEL) - Symptom Bother: estimating cut-off scores for dry eye severity groups. Value Health 14(7), A507–A508 (2011).
25.
Micromedex® RED BOOK®. (2025).
26.
AbbVie Inc. HUMIRA® (adalimumab): prescribing information. (2024). Available from: https://www.rxabbvie.com/pdf/humira.pdf
27.
Janssen Biotech Inc. REMICADE (infliximab): prescribing information. (2021). Available from: https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/REMICADE-pi.pdf
28.
Schmier J, Ogden K, Nickman N et al. Costs of providing infusion therapy for rheumatoid arthritis in a hospital-based infusion center setting. Clin. Ther. 39(8), 1600–1617 (2017).
29.
Latif M, Guo N, Tereshchenko LG, Rothberg MB. Association of hospital spending with care patterns and mortality in patients hospitalized with community-acquired pneumonia. J. Hosp. Med. 18(11), 986–993 (2023).
30.
Peery AF, Crockett SD, Murphy CC et al. Burden and cost of gastrointestinal, liver, and pancreatic diseases in the United States: update 2018. Gastroenterology 156(1), 254–272; e11 (2019).
31.
Paoli CJ, Reynolds MA, Sinha M, Gitlin M, Crouser E. Epidemiology and costs of sepsis in the United States-an analysis based on timing of diagnosis and severity level. Crit. Care Med. 46(12), 1889–1897 (2018).
32.
Vella V, Derreumaux D, Aris E et al. The Incidence of skin and soft tissue infections in the United States and associated healthcare utilization between 2010 and 2020. Open Forum Infect. Dis. 11(6), ofae267 (2024).
33.
Winston CA, Marks SM, Carr W. Estimated costs of 4-month pulmonary tuberculosis treatment regimen, United States. Emerg. Infect. Dis. 29(10), 2102–2104 (2023).
34.
Eppink ST, Kumar S, Miele K, Chesson HW. Lifetime medical costs of genital herpes in the United States: estimates from insurance claims. Sex. Transm. Dis. 48(4), 266–272 (2021).
35.
Singh JA, Yu S. The burden of septic arthritis on the U.S. inpatient care: a national study. PLoS ONE 12(8), e0182577 (2017).
36.
Nagpal M, Chu J, Dobberfuhl A. MP39-20 Cost of urinary tract infections with and without antibiotic resistance in the United States from 2012–2019. J. Urol. 209, e544 (2023).
37.
Candrilli S, Kurosky SK. Recent trends in anaphylaxis-related hospitalization in the United States. Value Health 18(7), A503 (2015).
38.
Foley KA, Wang PF, Barber BL et al. Clinical and economic impact of infusion reactions in patients with colorectal cancer treated with cetuximab. Ann. Oncol. 21(7), 1455–1461 (2010).
39.
Koberlein J, Beifus K, Schaffert C, Finger RP. The economic burden of visual impairment and blindness: a systematic review. BMJ Open 3(11), e003471 (2013).
40.
Bentley TS, Ortner N. 2020 U.S. organ and tissue transplants: cost estimates, discussion, and emerging issues. (2020). [cited 2025 January 9]; Available from: https://www.milliman.com/en/insight/2020-us-organ-and-tissue-transplants
41.
Ding Y, Miller GE. Total expenses, total utilization, and sources of payment for outpatient prescription opioids in the U.S. adult civilian noninstitutionalized population, 2017, in Statistical Brief (Medical Expenditure Panel Survey (US)). Rockville (MD) (2001).
42.
Nelson WW, Rice JB, White AG et al. Predictors of high-cost patients with noninfectious inflammatory eye diseases. Clin. Ther. 41(11), 2331–2342 (2019).
43.
Thibodeau AR, Niziol LM, Tannen BL, Ballouz D, Woodward MA. Opioid prescribing patterns for ulcerative keratitis. Cornea 41(4), 484–490 (2022).
44.
Zafar S, Wang P, Schein OD et al. Prescribing patterns and costs associated with postoperative eye drop use in Medicare beneficiaries undergoing cataract surgery. Ophthalmology 127(5), 573–581 (2020).
45.
Vlahiotis A, Devine ST, Eichholz J, Kautzner A. Discontinuation rates and health care costs in adult patients starting generic versus brand SSRI or SNRI antidepressants in commercial health plans. J. Manag. Care Pharm. 17(2), 123–132 (2011).
46.
US Bureau of Labor Statistics. CPI for all urban consumers. Medical care in U.S. city average, all urban consumers, seasonally adjusted. (2024). Available from: https://data.bls.gov/
47.
Porter ME. What is value in health care? N. Engl. J. Med. 363(26), 2477–2481 (2010).
•• Offers insights into defining healthcare value, a key concept for stakeholders deciding interventions based on clinical and economic benefits.
Information & Authors
Information
Published In
Copyright
© 2025 Mallinckrodt Pharmaceuticals. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 June 2025
Accepted: 30 June 2025
Published online: 17 July 2025
Keywords:
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost-per-response of Acthar Gel versus standard of care for the treatment of noninfectious keratitis: a United States healthcare perspective. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0088
Export citation
Select the citation format you wish to export for this article or chapter.