Transportability of nonlocal real-world evidence and its relevance to health technology assessment: a primer
Publication: Journal of Comparative Effectiveness Research
Abstract
Real-world evidence (RWE) from outside Canada or the UK is sometimes included in submissions to health technology assessments by Canada’s Drug Agency/L'Agence des médicaments du Canada (CDA-AMC) and National Institute for Health and Care Excellence when local data are lacking, particularly in rare diseases. However, differences in population demographics, healthcare systems and clinical practice patterns between different jurisdictions can pose challenges for contextualizing nonlocal data for health technology assessments. This primer outlines the challenges of using nonlocal RWE for decision-making, presents assumptions necessary for transportability of RWE, and describes quantitative methods to address these challenges. This primer is written for a broad audience, including industry stakeholders, researchers and clinicians, who are seeking accessible guidance on the use of nonlocal RWE and developments in the field of transportability.
Clinical research aims to determine the safety and effectiveness of new therapies with the goal of improving overall health outcomes. Increasingly, real-world data (RWD) collected outside the controlled settings of clinical trials, such as via electronic health records, administrative claims and patient registries, are used alongside clinical trials to generate evidence (‘real-world evidence’ or RWE) on long-term safety and effectiveness, cost–effectiveness and resource utilization of therapies in routine care [1,2]. However, the growing use of RWE across different health systems, including submissions of RWE from other countries for health technology assessments (HTA), can present challenges for decision making. This primer summarizes these challenges, outlines the statistical framework for transportability of evidence across settings, and reviews selected CDA-AMC and NICE submissions that highlight practical considerations for generalizability and transportability in HTA.
Generalizability refers to the extent to which study findings apply to the broader population from which study patients were selected (Figure 1). For example, studies with strict eligibility criteria that do not reflect the wider real-world patient population that study patients were recruited from may have low real-world generalizability [3]. In contrast, transportability concerns applying treatment effect estimates to a target population that is partially or entirely distinct from the study population [4]. It is particularly relevant when using RWE generated in one country to inform decisions in another. Formally, generalizability is a special case of transportability, and both share the same methodological framework [4]. However, transportability often requires stronger assumptions when populations differ substantially (these assumptions are described in the following sections and in Table 1).
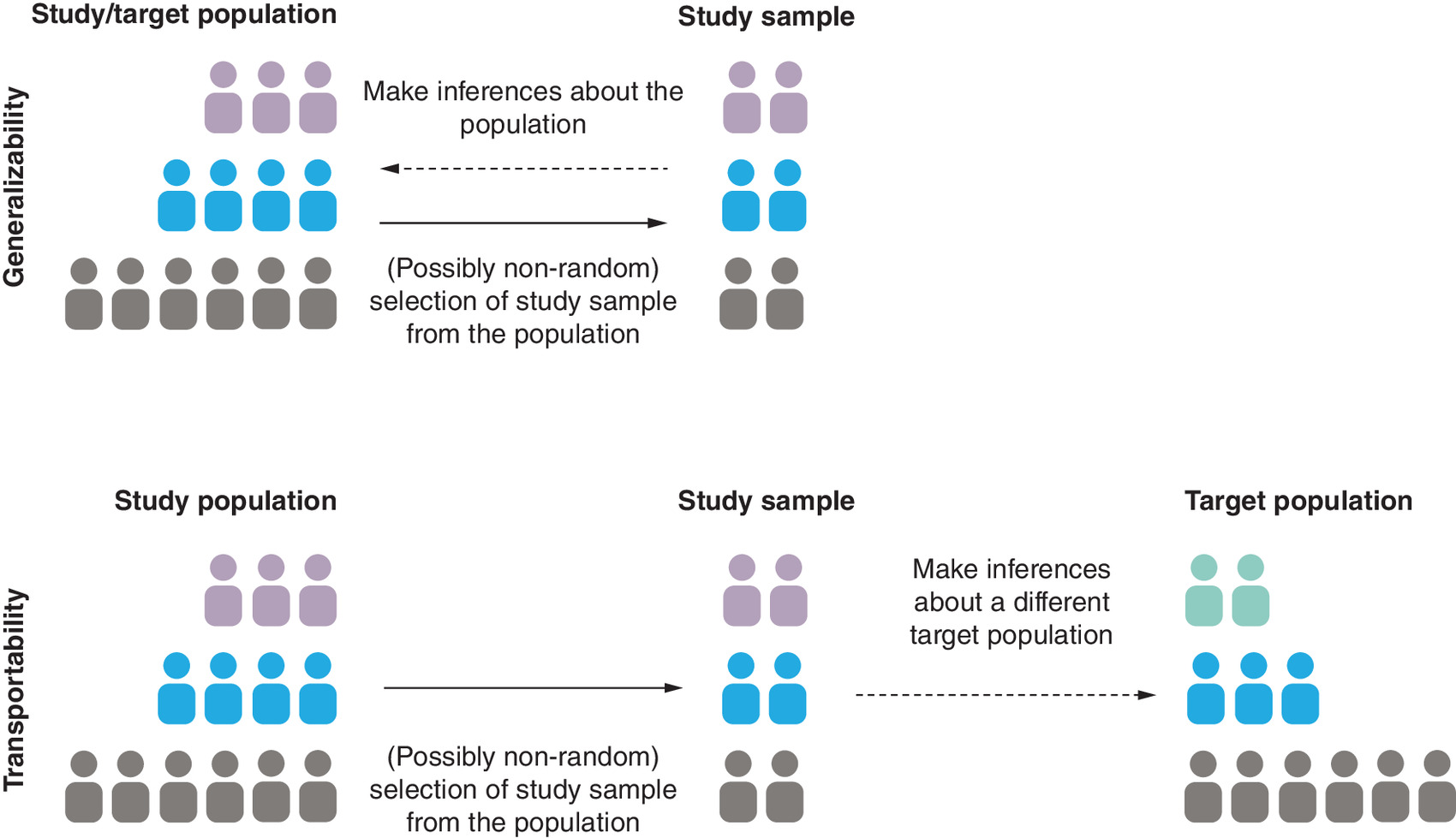
Figure 1. Visualization of generalizability and transportability.
In some cases, such as the one shown below for transportability, the target population may include individuals not represented in the study population (green individuals). In these cases, external information may be required to complement data from the study population to achieve transportability. Colors represent heterogeneity in prognosis or response to treatment.
| Assumption | What it means | Why it can fail | How to address it |
|---|---|---|---|
| Consistency | Patients in both settings are receiving the same version of treatment (dose, regimen and combination) | Treatment versions differ across countries. For example, subsequent therapies vary in availability or usage or dose varies | Define treatment precisely (e.g., include dose ‘drug X at dose Y’) |
| Positivity | The patients we want to apply results to are actually represented in the nonlocal data | No overlap in key traits (e.g., race, biomarkers and insurance coverage) between local and nonlocal contexts | Use proxies (e.g., genetic variant status instead of race); bring in external data or restrict the target population of patients to just those for whom nonlocal data are available |
| Conditional Exchangeability | Any relevant differences between populations (e.g., prognostic variables) can be measured and adjusted for | Important variables (e.g., socioeconomic status, adherence and quality-of-life) may not be recorded or available in routine data | Link to other datasets for proxies (e.g., income); if unmeasured, conduct sensitivity analysis |
Challenges of using nonlocal evidence in health technology assessment
When evaluating RWE from different geographic or healthcare contexts, it can be challenging to determine how differences in patient characteristics, clinical practices, access to care, healthcare systems and medication use affect its relevance to the local context. Importantly, RWE from countries outside the HTA jurisdiction is increasingly used in HTA, prompting the development of guidance on its use (e.g., see section on ‘External validity bias’ in NICE’s real-world evidence framework [5]). Examples on the use of nonlocal RWE for HTA include the use of RWD from the US to inform survival extrapolations (e.g., atezolizumab for treatment of metastatic lung cancer; NICE technology appraisal TA520), and to derive external comparator arms (e.g., sotorasib for KRAS G12C mutation-positive lung cancer; NICE technology appraisal TA781).
Nonlocal RWE, by which we refer to RWE originating from outside the specific geographic, health system or population context being evaluated for HTA, is essential when local data are unavailable. For instance, countries with stronger clinical research infrastructure and funding to support extensive RWD collection, such as the US, may offer a broader evidentiary base than local RWD at the time of HTA submission for the following reasons:
•
Lack of local usage data, such as for newly introduced technologies, or those with limited adoption so far.
•
Insufficient sample sizes or follow-up, especially for rare populations or new therapies.
•
Privacy and data sharing limitations.
•
Limited local infrastructure or expertise for capturing or analyzing RWD.
In such cases, nonlocal RWE may be the only available or timely source of real-world insights. The goal of transportability analysis is to adapt nonlocal RWE to the local context by using statistical adjustments to ensure its relevance to the specific population and healthcare system of interest.
In practice, drug manufacturers may collect RWD in one country – such as Japan or China – and submit it to HTA bodies in Europe or Canada. Limited local sample sizes or short follow-up lengths may necessitate use of nonlocal RWE to improve precision, particularly in rare disease settings or for drugs that are granted accelerated regulatory approval, which are typically approved due to high unmet disease burden or breakthrough therapeutic activity. If both local and nonlocal data are available, combining them can be challenging due to differences in data collection, processing, governance and measurement methods (e.g., claims vs electronic records) in addition to differences in patient and healthcare characteristics.
Clinician perceptions of nonlocal evidence
Clinical input routinely informs HTAs, expert committee deliberations and guideline development. While no systematic review has specifically examined clinician perceptions of nonlocal RWE in HTA ([6] reviewed HTA recommendations on the topic), clinicians often advise on the appropriateness of end points and the generalizability of data to patients seen in practice. We expect that clinicians often will discriminate between local and nonlocal evidence, considering differences in patient populations, clinical practice, treatment regimens, healthcare infrastructure and lifestyle factors. For instance, they may perceive disease incidence or cost estimates from other countries as less relevant to their own. In contrast, they may more readily accept results from randomized clinical trials conducted in other countries. There is considerable variation in clinician perceptions toward the use of RWE in general; however, most clinicians judge it favorably for addressing uncertainties in the use of novel treatments in clinical practice [7].
As an example of criticism of nonlocal evidence by clinicians, consider differences in treatment patterns across jurisdictions described by Sharp et al. [8]. Based on a systematic review of trials in kidney cell carcinoma, the authors reported low rates of second-line immunotherapy in clinical trial control arms due to high costs of immunotherapy drugs in some countries where patients were enrolled [8]. This can lead to an overestimation of benefits from the new therapies evaluated in the trials when applying their results to settings where such therapies are more common (this corresponds to violation of the consistency assumption described in Table 1). Indeed, intention-to-treat effect estimates may have limited generalizability or transportability when subsequent therapies and adherence patterns differ. Emerging approaches, such as the local average treatment effect [9] or per-protocol effects adjusted for nonadherence [10] can improve comparability across jurisdictions by aligning estimates with realistic adherence patterns, despite some challenges in interpretability and estimation relative to intention-to-treat effects.
Evaluating the generalizability of nonlocal data
Clearly, clinical and HTA decision-making should rely ideally on local data. Findings from studies conducted in different geographies, time periods or comparator landscapes may be difficult to interpret for current clinical decision making. Evaluating the transportability of such studies requires substantive cross-country knowledge of differences in clinical practice, patient demographics and treatment standards.
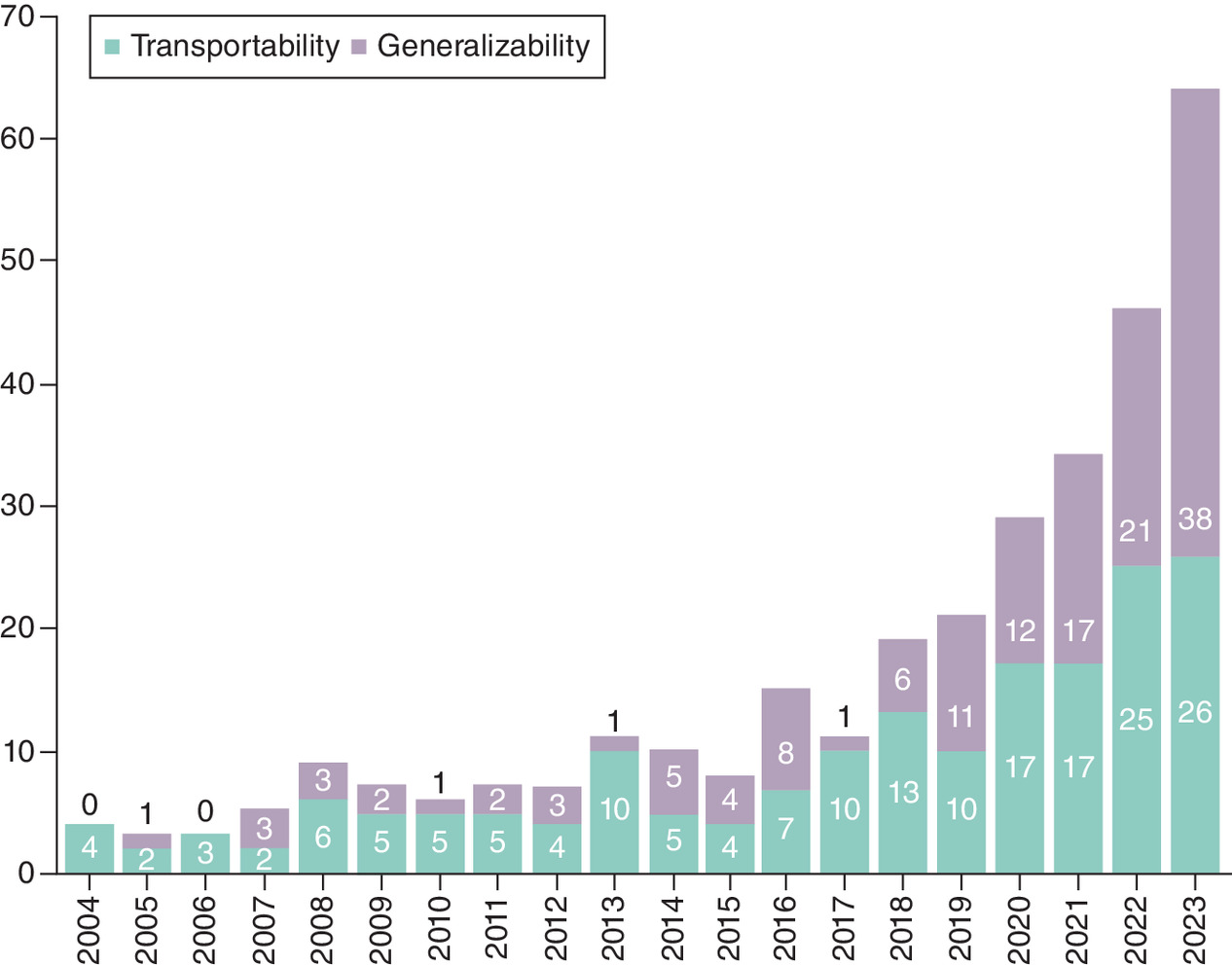
This primer supplements recent reviews on transportability [6,11] and growing research in the area (Figure 2), building on our previous work [12,13] and experience with CDA-AMC and NICE. We provide an overview of the challenges in using nonlocal data for HTA and demonstrate, using a targeted review of HTA appraisals, that common criticisms by CDA-AMC and NICE span all three assumptions required for transportability, which we describe next.
Assumptions for transportability
When evaluating transportability of RWE in the context of a specific setting or study, it is essential to understand the foundational assumptions that determine whether transportability is feasible, what is needed to support it, and where intentional or unintentional errors may arise. There are three core assumptions for transportability: consistency, positivity and conditional exchangeability [4]. These are described further below and summarized in Table 1:
•
Consistency requires that treatment outcomes are consistent between the study and target populations. Practically, this implies that differences in treatment characteristics (e.g., dosage, regimen and combinations) and post-treatment exposures, such as subsequent therapies, that can affect patient outcomes of interest, do not differ between the nonlocal and local contexts. For instance, if Japanese patients receive a higher dose of a drug than Canadian patients, and if a higher dose enhances the treatment’s effect, then results from a Japanese RWE study cannot be interpreted in a Canadian context straightforwardly. Differences in follow-up or rescue therapies can also violate the consistency assumption.
Mitigation strategies include specifying treatments more granularly (e.g., separate treatment groups based on dose). Note that if differences in treatment characteristics do not affect outcomes (see [14] for an example), then even if there are cross-setting differences in treatment characteristics, they can be appropriately ignored for the purposes of assessing transportability.
a.
Technical point: An alternative framing of these assumptions includes the stable unit treatment value assumption, or SUTVA, which involves noninterference between treatment groups. Interference between patients in different geographies is not commonly a problem, so for simplicity we focus on the assumption of consistency, particularly of treatment versions.
•
Positivity requires that for every patient subgroup in the local context, a comparable subgroup exists in the nonlocal dataset. This is crucial because without nonlocal RWE for each local subgroup of interest, it becomes difficult – or even impossible – to make defensible inferences about them. For example, suppose that we are interested in using RWE on treatment outcomes from a Japanese database to understand treatment outcomes in the UK. If racial differences between Japanese and UK patients affect treatment outcomes, perhaps because of differences in underlying genetic susceptibilities to treatment or lifestyle factors, it is unlikely that we can infer anything about the UK based on Japanese RWD without any British patients represented.
A mitigation strategy is simply to restrict the patient population that we can evaluate therapies for to those for which some data or information is available. Alternatively, in the example above, we may wish to account for the underlying genetic markers or lifestyle factors instead of ethnicity or race.
•
Conditional exchangeability requires that all relevant factors that differ between the local and nonlocal contexts are accounted for in the analysis. This requires first identifying all factors that affect treatment outcomes, and second, accounting for them using methods described in the next section to ‘adjust’ the nonlocal RWE to the local context.
In many RWD, variables such as socioeconomic status, health-seeking behavior or quality of life scores that can affect treatment outcomes are often unmeasured or captured inconsistently across jurisdictions. When such variables are believed to influence outcomes or treatment response, their absence poses a serious issue for evaluating transportability. Linking auxiliary data sources, such as administrative records, income proxies or survey data, can help address this gap.
a.
Note that in general, the transportability of relative measures of effect (e.g., hazard ratios or odds ratios) may be more justified in practice than that of absolute measures (e.g., incidence of outcomes or healthcare costs) because factors affecting relative effects (i.e., effect measure modifiers) will typically be fewer in number than those affecting absolute measures of risk (i.e., prognostic factors).
These assumptions and the statistical methods for addressing them described below, apply whether populations are fully overlapping (generalizability) or partially external (transportability), although differences across populations in the latter case makes fulfilling these assumptions more difficult. Therefore, transportability analyses involving nonoverlapping populations may be subject to greater risk of bias. Importantly, transportability of relative treatment effects requires that treatment groups in the nonlocal data were compared without bias, which depends on fulfilling a similar set of assumptions within the study dataset [4].
Notably, these assumptions cannot typically be verified directly using data and usually require expert judgment informed by substantive knowledge of both the local and nonlocal populations and RWD, and differences between them (some general guidance is discussed in [6]). Later in the primer, we map criticisms of nonlocal RWE in HTA appraisals to these assumptions to illustrate their practical implications. A systematic approach to study planning and reporting can enhance rigor and transparency in the evaluation of these assumptions and identification of the relevant variables. We have found that explicitly specifying eligibility, treatment regimens, follow-up, outcomes and analysis plans for the source and target populations can help clarify potential threats to validity and strategies to address them [13].
Methods to account for population differences
Once transportability assumptions have been evaluated and assumed to hold for the given setting, population, treatments and outcomes, statistical methods can be used to adjust for population-level factors. These methods include matching, weighting and standardization, and are described in more detail in Table 2. A conceptual overview of how transportability analysis using these methods works is shown in Figure 3.
| What it does | Strengths | Limitations | |
|---|---|---|---|
| Matching | Pairs patients in the study dataset with similar patients from the target population based on key characteristics (e.g., age, sex and biomarkers) | Easy to explain; useful when working with a few well-measured variables | Works best for time-fixed variables; less flexible for complex or high-dimensional data |
| Weighting | Reweights patients in nonlocal data to resemble the local population based on shared characteristics, so the average result reflects the local group | Commonly implemented in statistical packages | Can produce imprecise estimates if the overlap in characteristics between local and nonlocal contexts is low |
| Standardization | Predicts outcomes based on nonlocal patient traits and then applies those predictions to the local context | Relatively simple to implement and explain to a nontechnical audience | Risk of bias if the ‘prediction model’ is wrong |
| Doubly robust methods | Combines weighting and standardization, offering protection against errors in either method | Stronger protection against bias | More complex to implement and explain to nontechnical audiences |
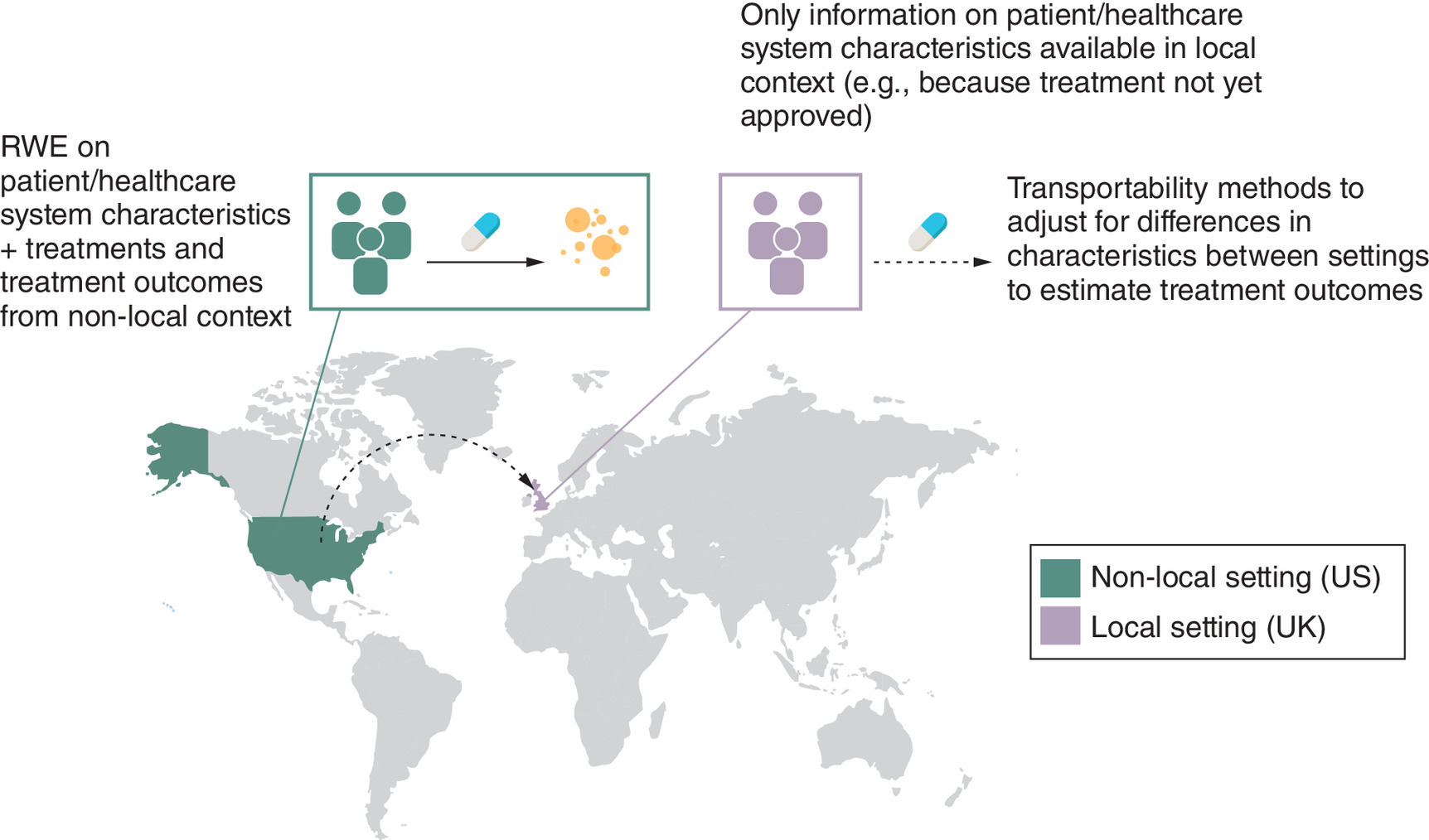
Figure 3. Conceptual overview of how transportability analysis works.
Here an example is shown of transportability from US to UK.
Examples of nonlocal RWE in HTA submissions
As practical examples, we identified CDA-AMC and NICE appraisals that included criticisms relating to the use of nonlocal RWE and related these criticisms to the foundational assumptions for transportability as framed previously. These are shown in Table 3. To generate these examples, we queried publicly available NICE and CDA-AMC appraisals between 2015 and 2024 using keywords ‘generalizability’ and ‘real-world’. Information from select appraisals that included RWD as primary or supportive evidence was extracted to showcase a variety of criticisms, with disagreements about underlying assumptions resolved through discussion between coauthors. This is not meant to be a comprehensive or systematic review of HTA appraisals.
| Therapy (disease) | Agency | Criticism | Assumptions affected | Ref. | |
|---|---|---|---|---|---|
| Teclistamab (relapsed/refractory myeloma) | CDA-AMC | PC0332 | Use of US external control arm; therapies used in US cohort not relevant to Canadian standard of care; comparator data outdated (2018–2021 for 2024 assessment); concerns about unmeasured confounding. | Consistency, positivity, exchangeability | [16] |
| Elranatamab (relapsed/refractory myeloma) | CDA-AMC | PC0315 | Differences in standards of care (US vs Canada); potential differences in study population vs general Canadian population. | Consistency, exchangeability | [17] |
| Pralsetinib (RET+ NSCLC) | CDA-AMC | Pharmacoeconomic review | External control arm analysis criticized due to differences in distribution and dosage of subsequent therapies vs Canadian practice. | Consistency | [18] |
| Nusinersen (spinal muscular atrophy in adults) | CDA-AMC | SR0713 | Concerns over nonrepresentative patient characteristics relative to Canadian practice; potential self-selection bias; observational studies may not generalize to Canadian adult patients. | Exchangeability, positivity | [19] |
| Nusinersen (spinal muscular atrophy) | NICE | TA588 | US registry data deemed less relevant for England; European data (Germany, Italy, Spain) considered more applicable due to healthcare system similarities. | Consistency | [20] |
| Tepotinib (NSCLC) | NICE | TA789 | Lack of generalizability to NHS clinical practice for subsequent therapies in single-arm trial; differences in comparator treatments and patient populations in indirect comparisons. | Consistency, exchangeability, positivity | [21] |
CDA-AMC: Cancer Drug Alliance – Access to Medicines Committee; NICE: National Institute for Health and Care Excellence; NSCLC: Non-small cell lung cancer; RET: Rearranged during transfection.
As shown in Table 3, criticisms about the transportability or generalizability of RWE in HTA appraisals are specific to the RWD, disease and intervention. Thematically, these criticisms often map to concerns about one or more – and frequently all three – transportability assumptions. Occasionally, clinical experts providing input to NICE have also concluded that US RWE may be generalizable to the UK for certain therapeutic areas (e.g., initial decision on mobocertinib in TA855). This further highlights the importance of assessing cross-country transportability on a case-by-case basis.
It can be difficult to quantify the impact of concerns about generalizability on the final decision because reimbursement decisions depend on various aspects of the submission. Nonetheless, if these concerns could have been addressed by study sponsors, it is possible that the submission package would have been viewed more favorably. In cases where the primary evidence was from an external control arm analysis (e.g., Table 3 – pralsetinib for RET+ non-small cell lung cancer), consideration of transportability issues at the study design phase may have considerably improved the understanding of their relevance to the local contexts.
Other practical considerations
When using nonlocal RWD to potentially inform HTA or clinical decision-making, it is ideal to consider transportability issues early in the study design phase. Outlining key assumptions (see Table 1) can help guide variable selection and RWD assessments of fitness for purpose. As described previously, structured frameworks can help guide the identification of relevant differences in healthcare systems, treatment pathways, disease prevalence and patient characteristics [6,11,22] but not all differences will matter in every analysis. While prior work has focused primarily on clinical outcomes such as survival or disease progression, the same framework for evaluating transportability assumptions applies to other end points, including quality-of-life (QoL) measures. For instance, EQ-5D health states are often assumed to be comparable across countries, but differences in patient interpretation, cultural norms or healthcare expectations may affect their cross-country transportability [23,24]. Extending transportability analyses to QoL outcomes would involve assessing whether such factors modify reporting or valuation of health states across populations. This is especially relevant when QoL is a key driver of cost–effectiveness in HTA.
In practice, some key variables for transportability assessment or adjustment will often be unmeasured or captured with non-negligible levels of missingness in existing RWD. This can pose a challenge for transportability analyses. Quantitative bias analysis (QBA) methods can help address this by exploring how unmeasured or mismeasured variables could impact study findings as a part of sensitivity analyses [12,25]. For example, suppose clinicians note that adherence to oral antivirals for COVID-19 is higher in the nonlocal jurisdiction, but that adherence data are not available in the nonlocal RWD to be able to implement transportability analysis directly. QBA allows analysts to
•
Perform tipping point analyses to quantify the magnitude of differences in adherence to treatment between different populations that would be needed to alter the study's conclusions (see [26] for example).
•
Use simulation-based approaches, applying clinically informed estimates to adjust effect estimates for potential adherence differences [27].
QBA can be conducted using deterministic (single scenario) or probabilistic (range of scenarios) approaches to test the robustness of findings. This helps decision-makers understand how reliable evidence is despite the lack of measurement of some important variables. For details, see a recent primer on QBA [28] and its application to external control arm analysis [13].
Conclusion
HTA increasingly considers the real-world relevance of study findings and the use of RWE [29]. When high-quality, locally sourced data are lacking, using RWD from other countries can be attractive but requires a nuanced understanding of geographic and clinical contexts. Understanding when and how evidence from elsewhere can be used is essential for making informed, transparent decisions. While methods for evaluating transportability are advancing, clear guidance and practical examples can help HTA agencies, regulators and industry stakeholders use nonlocal data more confidently. Ethical considerations and stakeholder involvement remain critical to ensure that the application of transportability methods aligns with patient and system priorities. Indeed, the thoughtful use of RWE, whether local or nonlocal, can ultimately accelerate patient access to novel therapies.
Executive summary
•
Clearer guidance and practical examples will support the confident use of nonlocal real-world evidence in health technology assessment.
•
Collaboration among health technology assessment bodies, researchers, clinicians, and industry is essential to understand challenges in evidence transportability and to validate and apply transportability methods.
•
Ethical and stakeholder considerations should be integrated when deciding to apply transportability analyses.
•
Thoughtful use of nonlocal evidence can help accelerate patient access to effective therapies.
Financial disclosure
This work was funded by AstraZeneca Canada.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Liu F, Panagiotakos D. Real-world data: a brief review of the methods, applications, challenges, and opportunities. BMC Med. Res. Methodol. 22, 287 (2022).
2.
Makady A, Ten Ham R, de Boer A, Hillege H, Klungel O, Goettsch W. Policies for use of real-world data in health technology assessment (HTA): a comparative study of six HTA agencies. Value Health 20(4), 520–532 (2017).
3.
Stuart EA, Bradshaw CP, Leaf PJ. Assessing the generalizability of randomized trial results to target populations. Prev. Sci. 16(3), 475–485 (2015).
4.
Degtiar I, Rose S. A review of generalizability and transportability. Annu. Rev. Stat. Appl. 10, 501–524 (2023).
• Provides a comprehensive and accessible review of generalizability and transportability concepts and methods, making it a cornerstone reference for applying these frameworks in real-world data (RWD) and health technology assessment (HTA) contexts.
5.
National Institute for Health and Care Excellence. NICE real-world evidence framework corporate document [ECD9]. Available at: https://www.nice.org.uk/corporate/ecd9/chapter/overview
6.
Jaksa A, Arena PJ, Chan KKW, Ben-Joseph RH, Jónsson P, Campbell UB. Transferability of real-world data across borders for regulatory and health technology assessment decision-making. Front. Med. 9, 1073678 (2022).
• Reviews practical challenges and opportunities for cross-border RWD use, relevant for understanding the limitations and potential of data sharing across HTA jurisdictions.
7.
Saesen R, Kantidakis G, Marinus A, Lacombe D, Huys I. How do cancer clinicians perceive real-world data, and the evidence derived therefrom? Findings from an international survey of the European Organisation for Research and Treatment of Cancer. Front. Pharmacol. 13, 969778 (2022).
8.
Sharp J, Khaki AR, Prasad V. Use of second-line immunotherapy in control arms of randomized clinical trials in kidney cancer: a systematic review. JAMA Netw. Open 4(9), e2124728 (2021).
9.
Angrist JD, Hull P. Instrumental variables methods reconcile intention-to-screen effects across pragmatic cancer screening trials. Proc. Natl Acad. Sci. U.S.A. 120(51), e2311556120 (2023).
10.
Hernán MA, Robins JM. Per-protocol analyses of pragmatic trials. N. Engl. J. Med. 377(14), 1391–1398 (2017).
11.
Turner AJ, Sammon C, Latimer N et al. Transporting comparative effectiveness evidence between countries: considerations for health technology assessments. Pharmacoeconomics 42(2), 165–176 (2024).
12.
Ramagopalan SV, Popat S, Gupta A et al. Transportability of overall survival estimates from US to Canadian patients with advanced non–small cell lung cancer with implications for regulatory and health technology assessment. JAMA Netw. Open 5(11), e2239874 (2022).
• Provides a detailed case study applying transportability methods to lung cancer from US RWD to Canada.
13.
Gupta A, Hsu G, Kent S et al. Quantitative bias analysis for single-arm trials with external control arms. JAMA Netw. Open 8(3), e252152 (2025).
14.
Zhao X, Suryawanshi S, Hruska M et al. Assessment of nivolumab benefit–risk profile of a 240-mg flat dose relative to a 3-mg/kg dosing regimen in patients with advanced tumors. Ann. Oncol. 28(8), 2002–2008 (2017).
15.
Kent S, Mpofu P, Duffield S et al. Evaluating transportability of overall survival estimates from US to UK populations receiving first-line treatment for advanced non-small cell lung cancer: a retrospective cohort study. BMJ Open 14(12), e085722 (2024).
• Demonstrates applied transportability in lung cancer treatment from the US to the UK.
16.
Canadian Agency for Drugs and Technologies in Health (CADTH). Draft reimbursement recommendation: teclistamab (Tecvayli). PC0332 (2024).
17.
Canadian Agency for Drugs and Technologies in Health (CADTH). Combined review report: pcP–related 2024 assessment. Report No.: PC0315 (2024). Available at: https://www.cda-amc.ca/sites/default/files/DRR/2024/PC0315-Combined_Report.pdf
18.
Canadian Agency for Drugs and Technologies in Health. Pralsetinib (Gavreto): CADTH reimbursement review: therapeutic area: rET fusion–positive non–small cell lung cancer. Report No.: NBK601720 (2023). Available at: https://www.ncbi.nlm.nih.gov/books/NBK601720/
19.
Canadian Agency for Drugs and Technologies in Health (CADTH). Reassessment report: nusinersen (Spinraza). Report No.: SR0713 (2022). Available at: https://www.cda-amc.ca/sites/default/files/DRR/2022/SR0713-Spinraza-Reassessment.pdf
20.
National Institute for Health and Care Excellence. Nusinersen for treating spinal muscular atrophy. NICE Technol. Appraisals, TA588 (2019). Available at: https://www.nice.org.uk/guidance/ta588
21.
National Institute for Health and Care Excellence. Tepotinib for treating advanced non-small-cell lung cancer with MET gene alterations. NICE Technol. Appraisals, TA789 (2022). Available at: https://www.nice.org.uk/guidance/ta789
22.
Levy NS, Arena PJ, Jemielita T et al. Use of transportability methods for real-world evidence generation: a review of current applications. J. Comp. Eff. Res. 13(3), e240064 (2024).
23.
Devlin N, Roudijk B, Ludwig K. Value sets for EQ-5D-5L: a compendium, comparative review & user guide. Value Health 25, 276–289 (2022).
24.
Wang Z, Luo N, Wang P. A comparative analysis of EQ-5D-5L general population norms across 23 countries: gender and age disparities. Pharmacoecon. Policy (2025) (In Press).
25.
Fox MP, MacLehose RF, Lash TL. Applying quantitative bias analysis to epidemiologic data. Springer, NY, USA (2021).
26.
Zhang M, Falconer M, Taylor L. A quantitative bias analysis of the confounding effects due to smoking on the association between fluoroquinolones and risk of aortic aneurysm. Pharmacoepidemiol. Drug Saf. 29(8), 958–961 (2020).
27.
Banack HR, Hayes-Larson E, Mayeda ER. Monte Carlo simulation approaches for quantitative bias analysis: a tutorial. Epidemiol. Rev. 43(1), 106–117 (2022).
28.
Thorlund K, Duffield S, Popat S et al. Quantitative bias analysis for external control arms using real-world data in clinical trials: a primer for clinical researchers. J. Comp. Eff. Res. 13(3), e230147 (2024).
29.
Harricharan S, Curran E, Lin HM et al. Real-world evidence in lung and hematologic oncology health technology appraisals: a review of six assessment agencies. Future Oncol. 19(8), 603–616 (2023).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 26 March 2024
Accepted: 18 July 2025
Published online: 21 August 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Transportability of nonlocal real-world evidence and its relevance to health technology assessment: a primer. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0041
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ashley A. Jaksa, Blythe Adamson, Robert Szulkin, Christian Dehlendorff, Emma Hernlund, Vandana Ayyar Gupta, Melinda Hanisch, Jing Wang-Silvanto, Karen M. Facey, Demonstrating transportability of real-world evidence: what do HTA bodies and health technology developers need?, International Journal of Technology Assessment in Health Care, 10.1017/S0266462326103924, 42, 1, (2026).
- Min-Hua Jen, Zhihong Cai, Haitao Chu, Ursula Becker, Joseph C. Cappelleri, Liang Chen, Orlando Dohring, Yinglei Li, Shahrul Mt-Isa, Min Ren, Ian Bridges, Statisticians at the Forefront of Health Technology Assessment: Aligning Regulatory and HTA Evidence Through Transdisciplinary Collaboration, Statistics in Biopharmaceutical Research, 10.1080/19466315.2026.2669302, (1-20), (2026).
- Paul Arora, Sreeram V Ramagopalan, R WE ready for reimbursement? A round-up of developments in real-world evidence relating to health technology assessment: part 23, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0196, 15, 1, (2025).