Confirmatory long-term efficacy and safety results of ataluren in patients with nmDMD from Study 041, an international, randomized, double-blind, placebo-controlled, Phase III trial
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To report the efficacy and safety of ataluren in patients with nonsense mutation Duchenne muscular dystrophy (nmDMD) from the phase III, 72-week, placebo-controlled period of Study 041. Materials & methods: Inclusion criteria: boys with nmDMD aged ≥5 years, on a stable corticosteroid regimen for ≥12 months, and baseline 6-minute walk distance (6MWD) ≥150 m. Randomization: 1:1, ataluren (40 mg/kg/day):placebo. Primary end point: slope of 6MWD change (average rate of change). Secondary end points: changes in 6MWD, time to 10% persistent worsening in 6MWD, North Star Ambulatory Assessment score, timed function tests and safety. Study populations: intention-to-treat; patients aged ≥7 to ≤16 years with baseline 6MWD ≥300 m and stand from supine ≥5 s; patients with baseline 6MWD 300–400 m. Results: In the intention-to-treat population (n = 359), over 72 weeks, ataluren reduced the rate of 6MWD decline by 21% (p = 0.0248), reduced the average 6MWD change (p = 0.0248), delayed time to 10% persistent worsening in 6MWD (p = 0.0078), and reduced North Star Ambulatory Assessment total score decline (p = 0.0235), change in 10 m walk/run time (p = 0.0422) and change in time to climb four stairs (p = 0.0293) versus placebo. In the 6MWD 300–400 m subgroup (n = 169), ataluren reduced the rate of 6MWD decline by 30% (p = 0.0310) versus placebo. Ataluren treatment benefits were seen in secondary end points in this subgroup, except for change in time to descend four stairs. In the 6MWD ≥300 m and time to stand from supine ≥5s subgroup (n = 185), there was a 9% slower rate of 6MWD decline for ataluren versus placebo over 72 weeks (p = 0.3626). Ataluren reduced change in time to climb four stairs (p = 0.0179) versus placebo in this subgroup; no treatment benefits were seen for other secondary end points. Ataluren was well tolerated (serious adverse events: ataluren, 7.1%; placebo, 6.8%); no deaths occurred. Conclusion: Long-term ataluren treatment has a favorable benefit–risk profile, slowing motor function decline in the largest phase III nmDMD study to date.
Plain language summary: Results from a phase III clinical trial describing the effect of treatment with ataluren on muscle function decline & assessing its safety in patients with nmDMD
What is this article about?
This article describes findings from Study 041. Study 041 was a clinical trial that aimed to confirm if ataluren, a treatment for people with nonsense mutation Duchenne muscular dystrophy (nmDMD), worked compared with placebo (a substance with no therapeutic effect) in a large number of participants with nmDMD over a period of 72 weeks. Ataluren has previously been compared with placebo in 48-week clinical trials. The aim of Study 041 was to confirm if ataluren slows muscle function decline compared with placebo and to assess ataluren safety results over 72 weeks.
What were the results?
In a group of 359 participants, ataluren slowed the decline in the participants’ ability to walk, physical function and ability to perform everyday activities that rely on lower limbs and upper limbs compared with placebo over 72 weeks. There were no safety concerns associated with taking ataluren. Results from this study were similar to those from previous ataluren clinical trials.
What do the results of the study mean?
These results helped to confirm that ataluren slows muscle function decline compared with placebo, without safety concerns, in participants with nmDMD over 72 weeks in the largest phase III study of nmDMD yet.
Duchenne muscular dystrophy (DMD) is a rare, progressive, neuromuscular disorder [1]. DMD is caused by a mutation in the DMD gene, leading to the absence of functional dystrophin protein that provides mechanical stability to muscle cells during contraction [1]. Approximately 10–15% of patients with DMD have a nonsense mutation in the DMD gene (nonsense mutation Duchenne muscular dystrophy [nmDMD]). This results in a premature stop codon in the dystrophin mRNA, preventing translation of full-length, functional dystrophin [2,3].
Ataluren is indicated for use by patients with nmDMD and was identified by high-throughput screening [4]. Even though the precise molecular target for ataluren is unknown, it is thought to promote protein production by enabling the ribosomal readthrough of mRNA containing a premature stop codon (the highest readthrough of ataluren is at UGA, followed by UAG, and then UAA) [4]. This enables the expression of a full-length functional dystrophin protein [5]. Ataluren functions at the level of translation; it does not interfere with transcription or mRNA stability and does not alter the levels of mRNA with premature stop codons or wild-type mRNA [5].
In a randomized, placebo-controlled, phase IIb study (Study 007; NCT00592553), although the primary end point was not met, ataluren (40 mg/kg/day) slowed the rate of decline of walking ability and achieved the targeted mean 30 m difference between ataluren and placebo in 6-minute walk distance (6MWD) over 48 weeks [6,7]. The benefit–risk of ataluren was affirmed in the phase III Ataluren Confirmatory Trial in DMD (ACT DMD; NCT01826487) [7,8]. In ACT DMD, the change in 6MWD between ataluren- and placebo-treated patients in the intention-to-treat (ITT) population was not significant; however, the effect of ataluren was more evident in the prespecified subgroup of patients with a baseline 6MWD of ≥300 m to <400 m. Ataluren was well tolerated and had a favorable safety profile in both Study 007 and ACT DMD [6,8].
The long-term safety and effectiveness of ataluren was evaluated in real-world, routine clinical practice in the Strategic Targeting of Registries and International Database of Excellence (STRIDE) Registry, the first international, observational safety and effectiveness study of ataluren in patients with nmDMD [9–11]. Results from the STRIDE Registry demonstrated that long-term, real-world treatment with ataluren plus standard of care (SoC) delays time to loss of ambulation (LoA) and decline in forced vital capacity in individuals with nmDMD [9–11].
PTC124-GD-041-DMD (Study 041; NCT03179631) was a phase III confirmatory trial of ataluren in patients with nmDMD, with a 72-week, double-blind, placebo-controlled phase followed by a 72-week, open-label phase. Study 041 was conducted as a specific obligation to contribute to the comprehensive data on ataluren summarized above. Here, we describe the efficacy and safety results from the 72-week, placebo-controlled treatment period of Study 041. Our primary objective was to determine the effect of ataluren on ambulation, assessed by the 6-minute walk test (6MWT).
Materials & methods
Study design & end points
Study 041 was designed and monitored in accordance with the ethical principles of Good Clinical Practice and the Declaration of Helsinki. Written informed consent was obtained from patients or their legally accepted representative according to the International Conference on Harmonisation Good Clinical Practice and the regulatory and legal requirements of the participating country.
This study was an international, randomized, double-blind, placebo-controlled, phase III, 72-week trial of ataluren in patients with nmDMD, followed by a 72-week open-label period (Supplementary Figure 1). The first patient was enrolled on 14 August 2017, and the last patient completed the double-blind treatment period on 5 March 2022.
The primary end point of the double-blind period was the slope of change (average rate of change) in 6MWD from baseline to week 72 (m/week). Secondary end points included: changes from baseline to week 72 in 6MWD, time to 10% persistent worsening in 6MWD, LoA over 72 weeks, a modified (16-item [excludes head lift]) North Star Ambulatory Assessment (NSAA) total and linear score, timed function test (TFT) composite score, time to perform TFTs (10 m walk/run, climb four stairs and descend four stairs) and the safety profile of ataluren. The exploratory end point described is the change from baseline to week 72 in performance of upper limb (PUL) total score and domain subscores. Visits for the analysis of these end points occurred every 12 weeks throughout the double-blind period.
Post hoc analyses included time to 5% persistent worsening and 30 m decline in 6MWD, and LoA over 48 weeks. Pooled analyses from the ITT populations and the 6MWD of ≥300 to <400 m subgroups (herein referred to as the 6MWD 300–400 m subgroups) of Study 041, ACT DMD and Study 007 were also performed. More information on this is presented in the Supplementary Appendix.
The slope of change in 6MWD was selected as the primary end point of this study because this end point is a standardized measure of ambulation and endurance of lower limb skeletal muscle and has been validated in patients with DMD from the age of 5 years [12]. Moreover, the slope of change accounts for the time to LoA, which is not accounted for when analyzing 6MWD change from baseline [13].
Patient eligibility
Eligibility criteria are described in full in the Supplementary Appendix. In brief, eligible patients were male, aged 5 years or older, had a confirmed genetic diagnosis of nmDMD, and provided written informed consent. Other eligibility criteria included systemic corticosteroid use (deflazacort, prednisone/prednisolone) for ≥12 months, with no significant changes in dosing regimen for ≥3 months before the start of study treatment. Boys were also eligible if they had a 6MWD of ≥150 m at baseline and the ability to perform TFTs (10 m walk/run, climb four stairs, descend four stairs and stand from supine) within 30 s at screening and baseline.
Patients were not eligible if they received prior or ongoing therapy with ataluren, received any other investigational drug in the 6 months before the start of study treatment, or were participating in any ongoing clinical trial.
Study treatment
Patients were randomized to receive ataluren or placebo (1:1). Randomization was established and performed centrally through an interactive response technology system to maximize the integrity and security of the randomization. Patients were assigned to receive ataluren or placebo using a stratified, block randomization approach to ensure balance with respect to the predefined stratification factors, as well as for the number of patients in each treatment group.
Patients received double-blind ataluren or placebo daily for 72 weeks. Study treatment was taken three-times per day at doses of 10, 10, and 20 mg/kg of body weight for morning, midday and evening doses, respectively. Information on treatment allocation and patient stratification is included in the Supplementary Appendix.
Study populations
The as-treated population included all randomized patients who received at least one dose of study treatment, with treatment assignments designated according to actual treatment received. This population was used to analyze safety end points.
The ITT population, used for the analysis of efficacy end points, included all patients randomized to receive ataluren or placebo regardless of whether they received a different study treatment from one to which they were originally randomized. Patients in this population were required to have a valid 6MWT baseline result, and at least one valid post-baseline 6MWT result. The ITT population was included in a pooled analysis with the ITT populations from ACT DMD and Study 007 (Supplementary Appendix) [6,8].
A prespecified subgroup of patients with a baseline 6MWD of 300–400 m was used for assessing ataluren efficacy. Patients with these baseline characteristics have been shown to be a ‘transition phase’ group of patients who experience a linear rate of muscle function decline and are, therefore, more sensitive than a broader population for capturing ataluren treatment effects within the time frame of a clinical trial [7,8]. Patients with a baseline 6MWD of >400 m are likely to experience relative stability throughout the duration of a clinical trial, making it difficult to ascertain favorable impact on disease progression as assessed by 6MWD. Patients with a baseline 6MWD of <300 m are in a phase of steep decline and will likely lose ambulation rapidly and with a greater degree of variability. This makes it challenging to determine the impact on 6MWD regardless of the presence of a therapeutic benefit [8].
Another prespecified subgroup included patients in the ITT population who met the following additional criteria: ≥7 years to ≤16 years of age with a 6MWD of ≥300 m and a time to stand from supine of ≥5 s at baseline (herein referred to as the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup). This was the primary analysis population and was used for the primary and secondary efficacy end point analyses. This subgroup was selected in an attempt to further optimize the characteristics of the 6MWD 300–400 m subgroup and to select for a population in whom treatment effect could be better captured. Patients in this subgroup were expected to experience a linear rate of decline during the 72-week treatment period; previous data suggested that patients with a 6MWD of ≥300 m were unlikely to lose ambulation during the study, and those with a time to stand from supine of ≥5 s would likely experience functional decline [8]. Therefore, based on previous studies, the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup was selected as the primary analysis subgroup because it was intended to represent patients who were in the consistent decline phase of nmDMD, whereas the ITT population was more heterogeneous because it included patients who were younger than 7 years of age and were therefore more likely to be in the stable disease phase [8,14,15].
Statistical analysis
Study hypothesis
The study hypothesis was that the slope of change in 6MWD from baseline to week 72 would be 1.0 m/week lower in the ataluren arm than the placebo arm within the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup.
Study size
Using 1:1 randomization, 154 patients were required in the primary analysis population (77 in the ataluren arm and 77 in the placebo arm) to detect a difference of 1.0 m/week in the average change in 6MWD between ataluren and placebo recipients with 85% power (two-sided α = 0.05), assuming a common standard deviation of 2.058 m/week, as was done previously in Study 007 and ACT DMD [6,8]. Assuming a premature discontinuation rate of ∼5%, 162 patients in total (81 in the ataluren arm and 81 in the placebo arm) would be enrolled in the primary analysis population. The ITT population was a broader, more heterogeneous population than the primary analysis population, thus a smaller treatment difference and a bigger variation were expected. A post hoc sample size calculation with a common standard deviation of 1.35 m/week observed in this study suggested that a sample size of 344 patients (172 in the ataluren arm and 172 in the placebo arm) would have 85% power to detect a treatment difference of 0.44 m/week in the average change in 6MWD over 72 weeks between ataluren and placebo recipients in the ITT population.
Analysis of efficacy end points
For the analysis of primary, secondary and exploratory efficacy end points, unless otherwise specified, a mixed model for repeated measures (MMRM) was employed with a random intercept. For the assessment of the primary end point in the ITT population, the MMRM included baseline concomitant corticosteroid type (deflazacort, prednisone/prednisolone), baseline 6MWD category (<300 m, 300 to <350 m, 350 to <400 m, ≥400 m), baseline 6MWD, baseline time to stand from supine (<5 s, ≥5 s), treatment, visit (as a categorical variable), the interaction of visit and baseline 6MWD and the interaction of visit and treatment. For the 6MWD 300–400 m subgroup, the baseline 6MWD categories were updated in the model to include 300 to <350 m and 350 to <400 m. For the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup, baseline time to stand from supine (<5 s, ≥5 s) was removed in the testing model. The MMRM used for the analysis of individual TFTs was the same as the model used for the primary end point, but with baseline 6MWD replaced with the baseline results for the corresponding TFTs (10 m walk/run, climb four stairs or descend four stairs).
An additional analysis evaluated a composite end point of the average changes in 10 m walk/run time, time to climb four stairs and time to descend four stairs. The MMRM was the same as the model used for the primary end point, but with baseline 6MWD replaced with the average time of the three TFTs at baseline. Patients who were unable to perform a TFT within 30 s were assigned a value of 30 s for the analysis.
The NSAA consists of 17 activities, each scored as 0, 1 or 2 [16]. In this study, a modified NSAA was implemented, excluding head lift. This is because this activity has not been shown to perform in a hierarchical manner with other items using Rasch analysis [16], meaning that this item displayed misfit unlike other items in the NSAA [17].
Total NSAA scores were the sum of scores from 16 activities and ranged from 0 to 32, with higher scores indicating better function. Function loss was defined as a reduction in score from 1 or 2 at baseline to a score of 0 at the specified post-baseline visit. If an activity could not be performed owing to disease progression, a score of 0 was assigned. If fewer than 13 of the 16 activities were performed, the total score was considered missing. If 13–15 activities were performed, the total score was standardized as follows: (observed total score/number of non-missing activities) × 16. The total score was then transformed into a linear score via logit transformation according to Mayhew et al. [16]. Transformed scores ranged from 0 to 100 [16]. The missing assessments at postbaseline visits were imputed using the last observation carried forward method. The MMRM used for the analysis of modified NSAA scores was the same as the model used for the primary end point, but with baseline 6MWD replaced with the baseline modified NSAA score (total or linear).
Time-to-event variables (time to 10% persistent worsening in 6MWD, 5% persistent worsening in 6MWD, 30 m decline in 6MWD, and LoA) were evaluated using a log-rank test and Kaplan–Meier analysis. The Cox proportional hazards model included baseline concomitant corticosteroid type (deflazacort, prednisone/prednisolone), baseline 6MWD category (<300 m, ≥300 to <350 m, ≥350 to <400 m, ≥400 m), baseline time to stand from supine (<5 s, ≥5 s), baseline 6MWD (categorical variable), treatment (ataluren, placebo), analysis visit (categorical variable), the interaction of analysis visit with baseline 6MWD and the interaction of analysis visit with treatment. LoA was defined as a persistent inability to perform the 10 m walk/run test within 30 s at any postbaseline visit and for all remaining visits. The median time to LoA was calculated from Kaplan–Meier estimates. Patients who did not experience an event were censored.
The pooled analysis of Study 041, ACT DMD and Study 007 employed an analysis of covariance (ANCOVA) model. Inferential analyses at week 48 were performed because week 48 was the latest common visit among the three studies. Similarly, by-visit summaries were presented for the common visits among the three studies only at baseline, week 24 and week 48.
Details of PUL statistical analyses are detailed in the Supplementary Appendix.
Results
Patient disposition & baseline characteristics
Study 041 was conducted at 69 sites in 18 countries/provinces (Supplementary Table 1). In total, 439 patients were screened; of these, 363 were randomized to double-blind treatment (Supplementary Figure 2). Three patients were randomized in error and therefore did not receive study treatment. Therefore, 176 patients received placebo and 184 patients received ataluren and were included in the as-treated population (Supplementary Table 2). One patient who received ataluren withdrew from the study before the first assessment and was not included in the ITT population.
Baseline characteristics in the ITT population, the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup, and the 6MWD 300–400 m subgroup were well balanced between treatment arms (Table 1). In total, 179 patients (97.8%) in the ataluren group and 172 patients (97.7%) in the placebo group completed the placebo-controlled period. Reasons for discontinuation included withdrawing consent (n = 4), loss to follow-up (n = 1), protocol noncompliance (n = 2) and other reasons (n = 5; Supplementary Figure 2).
| Baseline characteristic | ITT | 6MWD 300–400 m | 6MWD ≥300 m and time to stand from supine ≥5 s† | |||
|---|---|---|---|---|---|---|
| Ataluren (n = 183) | Placebo (n = 176) | Ataluren (n = 86) | Placebo (n = 83) | Ataluren (n = 92) | Placebo (n = 93) | |
| Age at enrollment, years, mean (min, max) | 8.1 (5, 14) | 8.2 (5, 14) | 8.1 (5, 14) | 8.5 (5, 14) | 8.9 (7, 14) | 8.9 (6, 14) |
| 6MWD, n (%) | ||||||
| <300 m | 21 (11.5) | 21 (11.9) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| 300 to <350 m | 40 (21.9) | 37 (21.0) | 40 (46.5) | 37 (44.6) | 29 (31.5) | 32 (34.4) |
| 350 to <400 m | 46 (25.1) | 46 (26.1) | 46 (53.5) | 46 (55.4) | 33 (35.9) | 31 (33.3) |
| ≥400 m | 76 (41.5) | 72 (40.9) | 0 (0) | 0 (0) | 30 (32.6) | 30 (32.3) |
| Corticosteroid use, n (%) | ||||||
| Deflazacort | 79 (43.2) | 73 (41.5) | 37 (43.0) | 35 (42.2) | 41 (44.6) | 41 (44.1) |
| Prednisone/prednisolone | 104 (56.8) | 103 (58.5) | 49 (57.0) | 48 (57.8) | 51 (55.4) | 52 (55.9) |
| Baseline time to stand from supine, n (%) | ||||||
| <5 s | 62 (33.9) | 55 (31.3) | 16 (18.6) | 15 (18.1) | 0 (0) | 0 (0) |
| ≥5 s | 121 (66.1) | 121 (68.8) | 70 (81.4) | 68 (81.9) | 92 (100) | 93 (100) |
†
Primary analysis subgroup (≥7 years to ≤16 years of age with a 6MWD of ≥300 m and a time to stand from supine of ≥5 s at baseline).
6MWD: 6-minute walk distance; ITT: Intention-to-treat; max: Maximum; min: Minimum.
Safety of ataluren
Treatment-emergent adverse events (TEAEs) were reported for 157 patients (85.3%) who received ataluren and 149 (84.7%) who received placebo in the as-treated population (Table 2). TEAEs were mostly mild (ataluren, n = 67 [36.4%]; placebo, n = [35.8%]) or moderate (ataluren, n = 77 [41.8%]; placebo, n = 70 [39.8%]).
| n (%) | Ataluren (n = 184) | Placebo (n = 176) |
|---|---|---|
| At least one TEAE | 157 (85.3) | 149 (84.7) |
| Maximum severity of TEAEs | ||
| Mild | 67 (36.4) | 63 (35.8) |
| Moderate | 77 (41.8) | 70 (39.8) |
| Severe | 13 (7.1) | 16 (9.1) |
| Life-threatening | 0 (0) | 0 (0) |
| Fatal | 0 (0) | 0 (0) |
| At least one treatment-related TEAE | 32 (17.4) | 36 (20.5) |
| Probable | 10 (5.4) | 9 (5.1) |
| Possible | 22 (12.0) | 27 (15.3) |
| At least one TESAE | 13 (7.1) | 12 (6.8) |
| At least one treatment-related TESAE | 2 (1.1) | 0 (0) |
| Probable | 0 (0) | 0 (0) |
| Possible | 2 (1.1) | 0 (0) |
| Discontinued study owing to TEAE | 0 (0) | 0 (0) |
| Discontinued study owing to treatment-related TEAE | 0 (0) | 0 (0) |
Adverse events were coded using MedDRA, version 24.1. TEAEs were defined as any adverse events with an end date on or after the first dose of study drug and up to 4 weeks after the last dose of double-blind study drug. Patients who reported two or more occurrences with the same preferred term were counted only once for that term.
Before their first assessment, one patient withdrew from the study after receiving one dose of ataluren.
ITT: Intention-to-treat; MedDRA: Medical Dictionary for Regulatory Activities; TEAE: Treatment-emergent adverse event; TESAE: Treatment-emergent serious adverse event.
Thirteen patients (7.1%) in the ataluren group and 12 patients (6.8%) in the placebo group experienced treatment-emergent serious adverse events (TESAEs). Among the 13 ataluren-treated patients who experienced TESAEs, two patients (1.1%) had treatment-related TESAEs (Table 2).
The most common individual TEAEs (occurring in ≥5% of all patients) are shown in Supplementary Table 3.
Efficacy end points in the ITT population
Primary end point
The difference in the average slope of change in 6MWD over 72 weeks between the ataluren and placebo groups was nominally significant (-0.74 m/week and -0.94 m/week in the ataluren and placebo groups, respectively; difference [95% CI]: 0.20 [0.03, 0.38]; p = 0.0248), equivalent to a 21% slower rate of decline in the ataluren group (Table 3).
| End point assessment 6MWD | ITT population | 6MWD 300–400 m | 6MWD ≥300 m and time to stand from supine ≥5 s† | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Ataluren (n = 183) | Placebo (n = 176) | Treatment difference‡ | Ataluren (n = 86) | Placebo (n = 83) | Treatment difference‡ | Ataluren (n = 92) | Placebo (n = 93) | Treatment difference‡ | ||
| Rate of change, m/week | LS mean change | -0.74 | -0.94 | 0.20 | -0.77 | -1.11 | 0.34 | -1.14 | -1.25 | 0.11 |
| (95% CI) | (-0.88, -0.60) | (-1.08, -0.79) | (0.03, 0.38) | (-0.99, -0.56) | (-1.33, -0.89) | (0.03, 0.64) | (-1.31, -0.96) | (-1.43, -1.08) | (-0.13, 0.36) | |
| p-value | 0.0248 | 0.0310 | 0.3626 | |||||||
| Change from baseline to week 72, m | LS mean change | -53.01 | -67.43 | 14.42 | -55.78 | -79.99 | 24.21 | -81.83 | -90.09 | 8.26 |
| (95% CI) | (-63.15, -42.88) | (-78.03, -56.84) | (1.83, 27.01) | (-71.24, -40.32) | (-95.83, -64.14) | (2.22, 46.20) | (-94.51, -69.16) | (-102.61, -77.58) | (-9.53, 26.05) | |
| p-value | 0.0248 | 0.0310 | 0.3626 | |||||||
| LoA at week 72, n (%) | 12 (6.6) | 20 (11.4) | NA | 5 (5.8) | 10 (12.0) | NA | 5 (5.4) | 9 (9.7) | NA | |
Baseline was defined as the maximum measurement of valid day 1 and day 2 6MWD values. Patients who lost ambulation during the study were assigned a value of 0 for the first visit and for all subsequent visits while they participated in the study.
†
Primary analysis subgroup (≥7 years to ≤16 years of age with 6MWD of ≥300 m and a time to stand from supine of ≥5 s at baseline).
‡
Treatment difference (ataluren – placebo).
6MWD: 6-minute walk distance; CI: Confidence interval; HR: Hazard ratio; ITT: Intention-to-treat; LoA: Loss of ambulation; LS: least-square; NA: Not available.
Secondary end points
The least-squares (LS) average change in 6MWD from baseline to week 72 was -53.01 m in the ataluren group and -67.43 m in the placebo group, representing a nominally significant treatment difference of 14.42 m (95% CI: 1.83, 27.01; p = 0.0248; Figure 1 & Table 3).
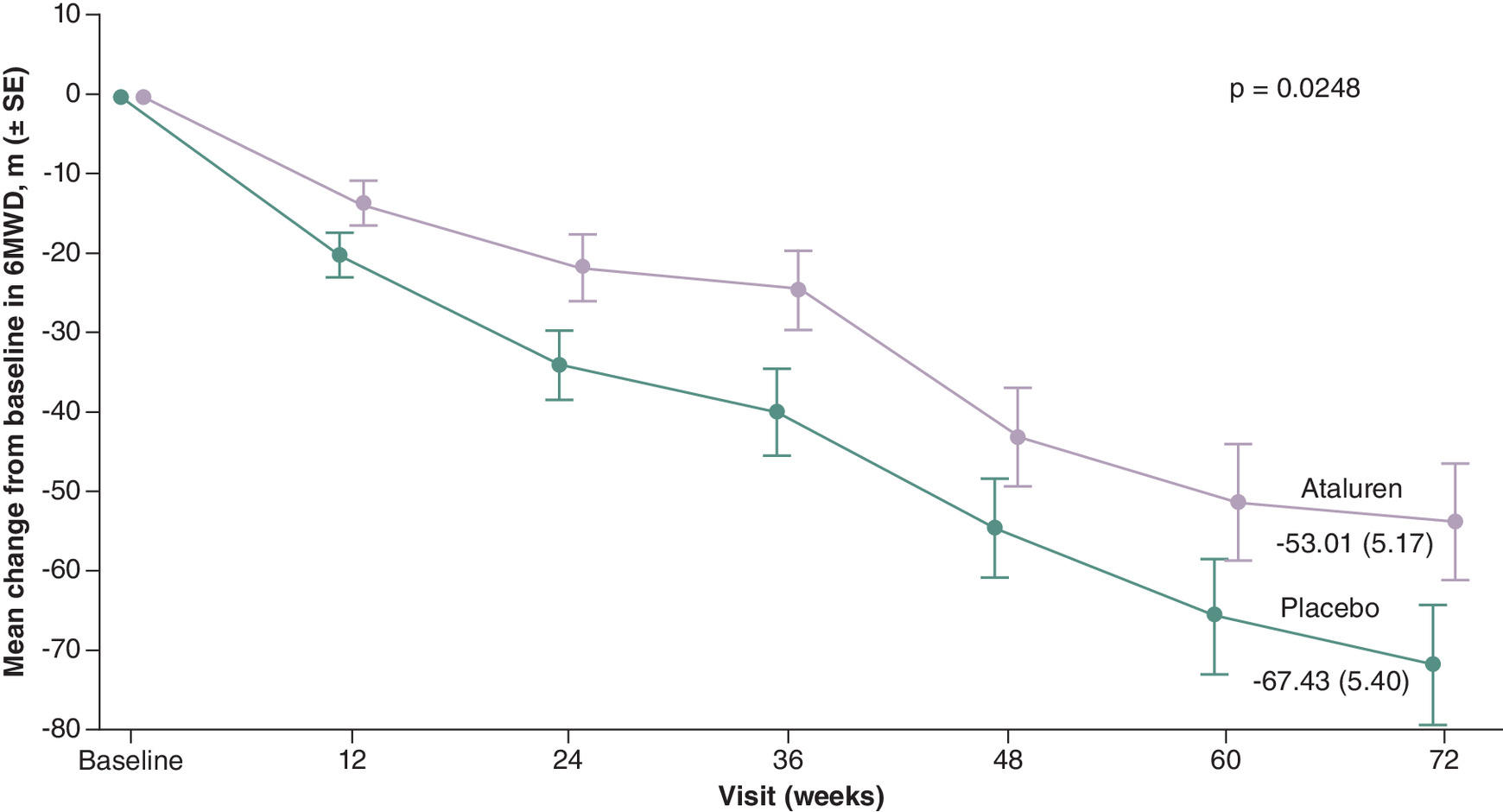
Figure 1. Mean change from baseline in 6-minute walk distance in the intention-to-treat population over 72 weeks.
Baseline was defined as the maximum measurement of valid day 1 and day 2 6MWD values. Patients who lost ambulation during the study were assigned a value of 0 for the first visit and set as missing for all subsequent visits while they participated in the study.
6MWD: 6-minute walk distance; ITT: Intention-to-treat; SE: Standard error.
By week 72, 12/183 ataluren-treated patients (6.6%) lost ambulation compared with 20/176 placebo-treated patients (11.4%; Table 3). Median time to LoA could not be estimated in either treatment group owing to the low number of events. In this population, 12/12 ataluren-treated patients (100%) and 19/20 placebo-treated patients (95.0%) who lost ambulation had a baseline time to stand from supine of >5 s (Supplementary Table 4). Results for LoA at week 48 are described in the Supplementary Appendix (Supplementary Table 5).
There were treatment benefits in the prespecified median time to 10% persistent worsening of 6MWD in ataluren-treated patients (74 weeks) compared with placebo (48 weeks; p = 0.0078). Ataluren-treated patients experienced a 31% lower risk of 10% persistent worsening in 6MWD compared with placebo by week 72; 48.1% of ataluren-treated patients and 61.9% of placebo-treated patients had 10% persistent worsening in 6MWD by week 72 (hazard ratio [HR]: 0.69; 95% CI: 0.52, 0.91); Figure 2 & Table 4). Results for time to 5% persistent worsening and 30 m decline in 6MWD are described in the Supplementary Appendix (Supplementary Table 6 & Supplementary Figure 3).
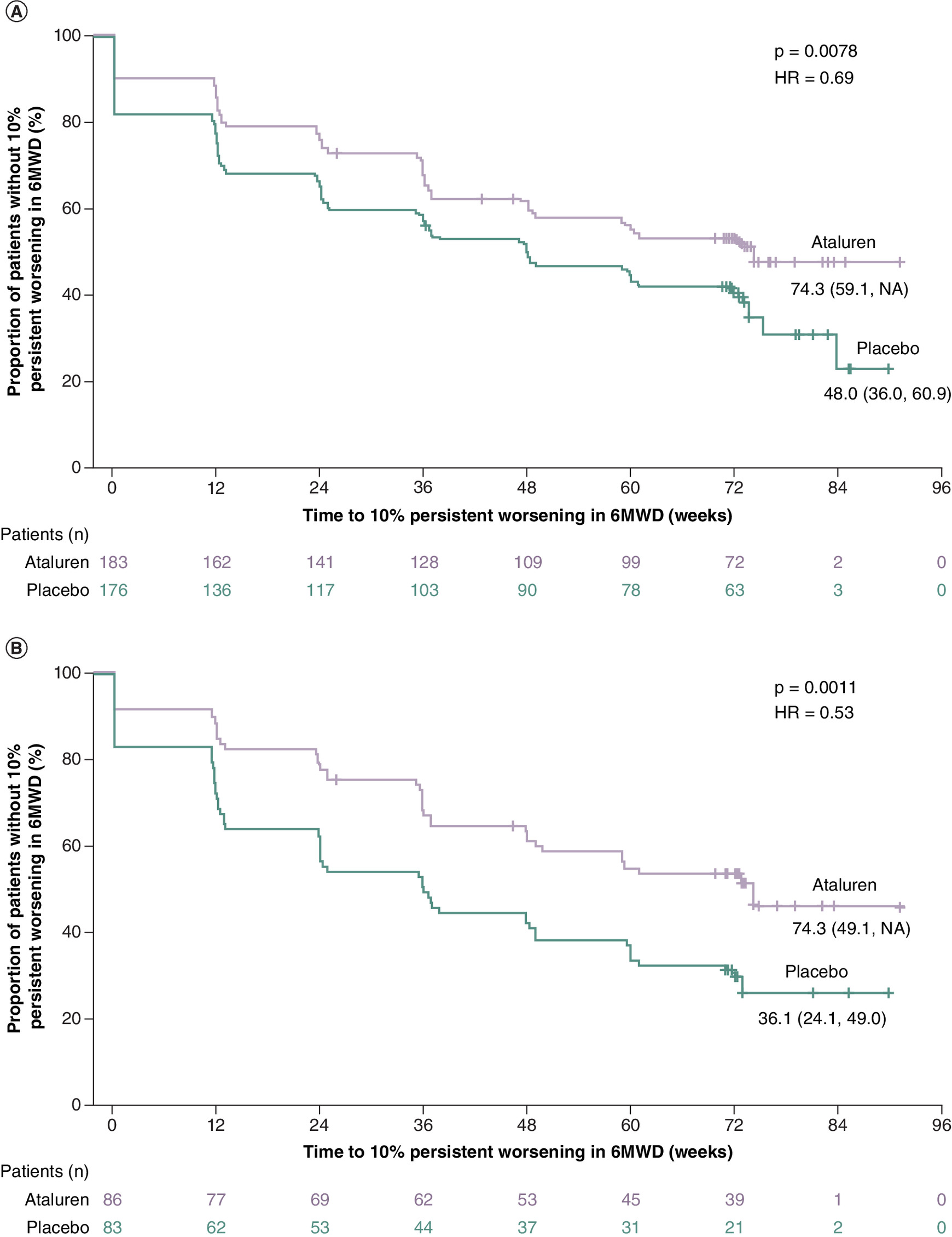
Figure 2. Median time to a 10% persistent worsening in 6-minute walk distance.
(A) Intention-to-treat population. (B) 6MWD 300–400 m subgroup. Time to a 10% persistent worsening in 6MWD was defined as the last time that 6MWD was not 10% worse than baseline. Patients who did not have a 10% persistent worsening in 6MWD were censored at the time of the last 6MWT during the double-blind period. Owing to COVID-19, some patients’ week 72 visits were delayed and the final data collection for the double-blind period occurred at week 90 or later.
6MWD: 6-minute walk distance; 6MWT: 6-minute walk test; HR: Hazard ratio; ITT: Intention-to-treat.
| ITT population | 6MWD 300–400 m | 6MWD ≥300 m and time to stand from supine ≥5 s† | ||||
|---|---|---|---|---|---|---|
| Ataluren (n = 183) | Placebo (n = 176) | Ataluren (n = 86) | Placebo (n = 83) | Ataluren (n = 92) | Placebo (n = 93) | |
| Patients with 10% persistent worsening by week 72, n (%) | 88 (48.1) | 109 (61.9) | 41 (47.7) | 59 (71.1) | 58 (63.0) | 71 (76.3) |
| Patients censored, n (%) | 95 (51.9) | 67 (38.1) | 45 (52.3) | 24 (28.9) | 34 (37.0) | 22 (23.7) |
| Time to 10% persistent worsening Kaplan–Meier estimate, weeks | ||||||
| Median (95% CI) | 74.3 (59.1, NA) | 48.0 (36.0, 60.9) | 74.3 (49.1, NA) | 36.1 (24.1, 49.0) | 36.7 (36.0, 60.0) | 35.6 (23.7, 48.0) |
| Min, max | 0.1, 91.4+ | 0.1, 90.0+ | 0.1, 91.4+ | 0.1, 90.0+ | 0.1, 91.4+ | 0.1, 90.0+ |
| Log-rank p-value | 0.0078 | 0.0011 | 0.0659 | |||
| Cox proportional hazards model | ||||||
| HR, ataluren to placebo (95% CI) | 0.69 (0.52, 0.91) | 0.53 (0.35, 0.79) | 0.73 (0.52, 1.03) | |||
Time to a 10% persistent worsening in 6MWD was defined as the last time that 6MWD was not 10% worse than baseline. Patients who did not have a 10% 6MWD worsening were censored at the time of the last 6MWT during the double-blind period (+ indicates that the observation was censored).
The Cox proportional hazard model includes baseline concomitant corticosteroid type (deflazacort, prednisone/prednisolone), baseline 6MWD category (<300 m, 300 m to <350 m, 350 m to <400 m, ≥400 m), baseline time to stand from supine (<5 s, ≥5 s), baseline 6MWD and treatment.
Bold p-values are significant.
†
Primary analysis subgroup (≥7 years to ≤16 years of age with 6MWD of ≥300 m and a time to stand from supine of ≥5 s at baseline).
6MWD: 6-minute walk distance; 6MWT: 6-minute walk test; HR: Hazard ratio; ITT: Intention-to-treat; max: Maximum; min: Minimum.
Ataluren-treated patients experienced a nominally significant lower decline in NSAA total score than placebo-treated patients (difference [95% CI]: 0.9 [0.1, 1.6]; p = 0.0235), and in NSAA linear score (difference [95% CI]: 2.3 [0.3, 4.3]; p = 0.0246; Table 5). Relative declines in both total and linear NSAA scores were approximately 19% smaller in the ataluren arm than in the placebo arm.
| ITT population | 6MWD 300–400 m | 6MWD ≥300 m and time to stand from supine ≥5 s† | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Ataluren (n = 183) | Placebo (n = 176) | Treatment difference‡ | Ataluren (n = 86) | Placebo (n = 83) | Treatment difference‡ | Ataluren (n = 92) | Placebo (n = 83) | Treatment difference‡ | ||
| NSAA total score | LS mean change at week 72 (95% CI) | -3.7 | -4.5 | 0.9 (0.1, 1.6) | -4.4 | -5.5 (-6.4, -4.6) | 1.1 | -5.2 | -6.1 | 0.9 (-0.2, 2.0) |
| (-4.2, -3.1) | (-5.1, -4.0) | (-5.3, -3.5) | (-0.1, 2.4) | (-6.0, -4.4) | (-6.9, -5.3) | |||||
| p-value | 0.0235 | 0.0837 | 0.1258 | |||||||
| NSAA linear score | LS mean change (95% CI) | -9.6 (-11.1, -8.2) | -11.9 (-13.5, -10.4) | 2.3 (0.3, 4.3) | -10.0 (-12.2, -7.8) | -13.3 (-15.6, -11.0) | 3.3 (0.1, 6.4) | -11.4 (-13.3, -9.5) | -14.0 (-15.9, -12.1) | 2.5 (-0.2, 5.2) |
| p-value | 0.0246 | 0.0419 | 0.0656 | |||||||
The total score in the original scale is the sum of scores from 16 activities (excluding head lift) and ranges from 0 to 32, in which higher scores indicate better functionality. If fewer than 13 of the 16 activities were performed, the total score is considered missing. If 13–16 activities were performed, the total score is standardized by (observed total score/number of non-missing activities) × 16. If an activity cannot be performed owing to disease progression, a score of 0 was assigned. Baseline was defined as the last observed measurement on or before the first dose of study drug.
†
Primary analysis subgroup (≥7 years to ≤16 years of age with 6MWD of ≥300 m and a time to stand from supine of ≥5 s at baseline).
‡
Treatment difference (ataluren – placebo).
6MWD: 6-minute walk distance; ITT: Intention-to-treat; LS: Least-square; NSAA: North Star Ambulatory Assessment.
Ataluren-treated patients experienced nominally significant smaller LS average increases (corresponding to less decline in function) from baseline than placebo-treated patients in 10 m walk/run time (difference [95% CI]: -0.78 [-1.53, -0.03] s; p = 0.0422) and time to climb four stairs (difference [95% CI]: -1.06 [-2.02, -0.11] s; p = 0.0293), but not in time to descend four stairs (difference [95% CI]: -0.29 [-1.30, 0.72] s; p = 0.5749; Table 6). Relative differences between ataluren and placebo in change in 10 m walk/run time, time to climb four stairs, and time to descend four stairs from baseline to week 72 were -20.4%, -17.9% and -5.5%, respectively. Longitudinal changes from baseline to week 72 in individual TFT items for the ITT population are included in the Supplementary Appendix (Supplementary Figure 4).
| Change from baseline to week 72 (s) | ITT population | 6MWD 300–400 m | 6MWD ≥300 m and time to stand from supine ≥5 s† | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Ataluren (n = 183) | Placebo (n = 176) | Treatment difference‡ | Ataluren (n = 86) | Placebo (n = 83) | Treatment difference‡ | Ataluren (n = 92) | Placebo (n = 93) | Treatment difference‡ | ||
| Composite score | LS mean change at week 72 (95% CI) | 4.24 (3.63, 4.84) | 4.93 (4.31, 5.56) | -0.70 (-1.51, 0.11) | 4.20 (3.24, 5.16) | 5.75 (4.77, 6.74) | 1.56 (-2.93, -0.18) | 9.92 (8.69, 11.15) | 10.77 (9.55, 11.99) | -0.85 (-2.58, 0.87) |
| p-value | 0.0904 | 0.0262 | 0.3327 | |||||||
| 10 m walk/run | LS mean change at week 72 (95% CI) | 3.04 (2.48, 3.61) | 3.82 (3.24, 4.40) | -0.78 (-1.53, -0.03) | 2.99 (2.11, 3.86) | 4.28 (3.38, 5.18) | -1.29 (-2.54, -0.04) | 3.06 (2.29, 3.83) | 3.79 (3.03, 4.55) | -0.73 (-1.81, 0.36) |
| p-value | 0.0422 | 0.0429 | 0.1877 | |||||||
| Climb four stairs | LS mean change at week 72 (95% CI) | 4.98 (4.27, 5.69) | 6.04 (5.31, 6.78) | -1.06 (-2.02, -0.11) | 5.26 (4.14, 6.37) | 7.55 (6.40, 8.69) | -2.29 (-3.88, -0.69) | 5.25 (4.23, 6.26) | 6.98 (5.97, 7.98) | -1.73 (-3.16, -0.30) |
| p-value | 0.0293 | 0.0050 | 0.0179 | |||||||
| Descend four stairs | LS mean change at week 72 (95% CI) | 4.96 (4.21, 5.71) | 5.25 (4.47, 6.03) | -0.29 (-1.30, 0.72) | 4.62 (3.41, 5.83) | 5.59 (4.34, 6.83) | -0.97 (-2.69, 0.76) | 4.58 (3.51, 5.66) | 4.78 (3.72, 5.84) | -0.19 (-1.70, 1.31) |
| p-value | 0.5749 | 0.2714 | 0.7997 | |||||||
Baseline was defined as the last observed measurement on or before the first dose of study drug. Patients who could not perform a TFT within 30 s, including those with loss of ambulation, were assigned a value of 30 s for the respective test.
†
Primary analysis subgroup (≥7 years to ≤16 years of age with a 6MWD of ≥300 m and a time to stand from supine of ≥5 s at baseline).
‡
Treatment difference (ataluren – placebo).
6MWD: 6-minute walk distance; ITT: Intention-to-treat; LS: Least-square; TFT: Timed function test.
Changes in PUL scores and results from the pooled analysis of the Study 041, ACT DMD and Study 007 ITT populations are described in the Supplementary Appendix (Supplementary Table 7 & Supplementary Figure 5).
Efficacy end points in the 6MWD 300–400 m subgroup
Primary end point
The difference in the average slope of change in 6MWD over 72 weeks between the ataluren and placebo group was nominally significant (-0.77 m/week and -1.11 m/week in the ataluren and placebo groups, respectively; difference [95% CI]: 0.34 [0.03, 0.64]; p = 0.0310), equivalent to a 30% slower rate of decline in the ataluren group (Table 3).
Secondary end points
LS average change in 6MWD from baseline to week 72 was -55.78 m in the ataluren group and -79.99 m in the placebo group, representing a nominally significant treatment difference of 24.21 m (95% CI: 2.22, 46.20; p = 0.0310; Table 3).
By week 72, 5/86 ataluren-treated patients (5.8%) lost ambulation compared with 10/83 placebo-treated patients (12.0%; Table 3). Median time to LoA could not be estimated in either treatment group owing to the low number of events. Results for LoA at week 48 are described in the Supplementary Appendix (Supplementary Table 5).
Ataluren reduced the risk of 10% persistent worsening in 6MWD by 47% compared with placebo (HR: 0.53; 95% CI: 0.35, 0.79). The median time to decline to this critical milestone was 74.3 weeks in the ataluren group and 36.1 weeks in the placebo group (p = 0.0011; Figure 2 & Table 4). Results for time to 5% persistent worsening and 30 m decline in 6MWD are described in the Supplementary Appendix (Supplementary Table 6 & Supplementary Figure 3).
Ataluren-treated patients experienced a nominally significant lower decline in LS mean NSAA linear score than placebo-treated patients (difference [95% CI]: 3.3 [0.1, 6.4]; p = 0.0419), but not in NSAA total score (difference [95% CI]: 1.1 [-0.1, 2.4]; p = 0.0837; Table 5). Relative declines in total and linear NSAA scores were 20% and 25% smaller, respectively, in the ataluren arm than in the placebo arm.
In ataluren-treated patients, nominally significant differences were observed compared with placebo for 10 m walk/run time (difference [95% CI]: -1.29 [-2.54, 0.04] s; p = 0.0429) and time to climb four stairs (difference [95% CI]: -2.29 [-3.88, -0.69] s; p = 0.0050), but not for time to descend four stairs (difference [95% CI]: -0.97 [-2.69, 0.76] s; p = 0.2714; Table 6). Relative differences between ataluren and placebo in change in 10 m walk/run time, time to climb four stairs and time to descend four stairs from baseline to week 72 were -30.2%, -30.3% and -17.3%, respectively.
Changes in PUL scores are described in the Supplementary Appendix (Supplementary Table 7).
Efficacy end points in the 6MWD ≥300 m & time to stand from supine ≥5 s subgroup (primary analysis subgroup)
Primary end point
The average slope of change in 6MWD over 72 weeks was -1.14 m/week and -1.25 m/week in the ataluren and placebo groups, respectively (difference [95% CI]: 0.11 [-0.13, 0.36]; p = 0.3626), equivalent to a 9% slower rate of decline in the ataluren group (not significant; Table 3).
Secondary end points
LS average change in 6MWD from baseline to week 72 was -81.83 m in the ataluren group and -90.09 m in the placebo group (difference [95% CI]: 8.26 [-9.53, 26.05] m; p = 0.3626; Table 3).
By week 72, 5/92 ataluren-treated patients (5.4%) lost ambulation compared with 9/93 placebo-treated patients (9.7%; Table 3). Median time to LoA could not be estimated in either treatment group owing to the low number of events. Results for LoA at week 48 are described in the Supplementary Appendix (Supplementary Table 5).
Ataluren reduced the risk of 10% persistent worsening in 6MWD by 27% compared with placebo (HR: 0.73; 95% CI: 0.52, 1.03). Median time to decline to this critical milestone was 36.7 weeks in the ataluren group and 35.6 weeks in the placebo group (p = 0.0659; Table 4).
Ataluren-treated patients did not experience a nominally significant difference in LS mean decline in either NSAA total score (difference [95% CI]: 0.9 [-0.2, 2.0]; p = 0.1258) or in NSAA linear score (difference [95% CI]: 2.5 [-0.2, 5.2]; p = 0.0656) compared with placebo (Table 5). Relative declines in total and linear NSAA scores were 14.5% and 18.5% smaller, respectively, in the ataluren arm than in the placebo arm.
In ataluren-treated patients, a nominally significant difference was observed for time to climb four stairs compared with placebo (difference [95% CI]: -1.73 [-3.16, -0.30] s; p = 0.0179), but no significant changes were seen for other TFTs (Table 6). Relative differences between ataluren and placebo in change in 10 m walk/run time, time to climb four stairs, and time to descend four stairs from baseline to week 72 were -19.2%, -24.8% and -4.1%, respectively.
Discussion
Study 041 included a large, broad ITT population of 359 boys aged 5 years or older with nmDMD (Table 1). In this heterogeneous patient group, ataluren demonstrated slowing of muscle function decline across the primary and key secondary end points of slope of change in 6MWD, NSAA score and TFTs over 72 weeks. In the ITT population, ataluren-treated patients had a 21% slower rate of decline in 6MWD and a difference in 6MWD of 14.42 m compared with placebo-treated patients (Table 3).
Furthermore, in this study, ataluren was associated with reductions in the risk of 10% (Table 4 & Figure 2) and 5% persistent worsening in 6MWD of 31% and 30%, respectively, and a reduced risk of 30 m decline by 31%, compared with placebo (Supplementary Table 6 & Supplementary Figure 3). It has previously been demonstrated that 10% persistent worsening in 6MWD is predictive of LoA, with patients who have 10% persistent worsening in 6MWD in a 12-month period being significantly more likely to lose ambulation in 4 years [18]. It has also been shown that patients who experience a loss of approximately 30 m in 6MWD are more likely to experience a steep decline in 6MWD, leading to LoA [19]. Therefore, a decline of 30 m in 6MWD is considered clinically meaningful and has been shown to have real-world significance for patients, for example in terms of keeping up with their peers, traveling to a bus stop or making it to a restroom [15]. In Study 041, ataluren-treated patients experienced a decline of 30 m at a median time of 49.1 weeks, compared with 36.0 weeks for placebo-treated patients, giving a median delay of 13 weeks (Supplementary Table 6 & Supplementary Figure 3). This represents a 31% reduction in the risk of reaching this important threshold with ataluren compared with placebo. An approximately 5% persistent worsening in 6MWD has also been established as a threshold for clinically meaningful progression for a range of similar diseases with compromised neuromuscular and pulmonary function [6,16,20].
In the sensitive 6MWD 300–400 m subgroup (previously used in ACT DMD) [8], ataluren-treated patients had a 30% slower rate of decline in 6MWD and a difference in 6MWD of 24.21 m compared with placebo-treated patients (Table 3). Ataluren also reduced the risk of 30 m decline by 47% and reduced the risks of 10% and 5% persistent worsening in 6MWD by 47% and 42%, respectively (Table 4 & Supplementary Table 6). These results may suggest that treatment differences observed in 6MWD are indicative of a clinically meaningful delay in progressing to milestones that are prognostic for LoA in this patient subgroup. In this subgroup, ataluren-treated patients experienced a decline of 30 m at a median of 61.1 weeks, compared with 25.0 weeks for placebo-treated patients, representing a median delay of 36 weeks (Supplementary Table 6 & Supplementary Figure 3). This further highlights the sensitivity of this patient subgroup and the delayed LoA experienced by patients treated with ataluren compared with placebo. In the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup, there was no difference observed for slope of change in 6MWD or in 10% persistent worsening in 6MWD between ataluren and placebo.
The NSAA provides complementary information to the 6MWT on different aspects of motor function relating to everyday functional abilities that are not captured by either the 6MWT or the NSAA alone [21]. Results of the NSAA demonstrated that the declines in both total and linear NSAA scores were statistically steeper in placebo-treated patients than in ataluren-treated patients in the ITT population, and in linear score for the 6MWD 300–400 m subgroup (Table 5). In the ITT population of this study, ataluren-treated patients gained a 2.3-point advantage in NSAA linear score compared with placebo. In ACT DMD, ataluren-treated patients gained a 1.5-point advantage compared with placebo, highlighting that a longer treatment duration with ataluren may lead to a greater benefit with a more pronounced separation in NSAA scores compared with placebo [8]. This may indicate a slower long-term decline of muscle function with ataluren treatment compared with placebo; the numerically moderate treatment differences in the 72 weeks of this study translate to clinically meaningful slowing of disease progression [22]. Modest changes in NSAA scores were also seen in other DMD studies. Vamorolone, a corticosteroid alternative for patients with DMD, led to an increase in NSAA score of 0.49 at week 48 when taken at 6 mg/kg/day compared with 2 mg/kg/day [23]. Unlike vamorolone, ataluren use is indicated for boys with nmDMD in addition to corticosteroids (part of SoC). Significant differences were not observed in the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup for total or linear NSAA scores, or in the 6MWD 300–400 m subgroup for total NSAA score.
TFTs, which measure functional ability and evaluate response to therapy, have also been shown to be valuable outcome measures for patients with DMD [15,24]. Nominally significant differences between ataluren- and placebo-treated patients were observed for 10 m walk/run time in the ITT population and 6MWD 300–400 m subgroup and for time to climb four stairs in all three patient populations (Table 6). The differences in time to climb four stairs between ataluren and placebo for the ITT population, the 6MWD 300–400 m subgroup and the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup were -1.06, -2.29, and -1.73 s, respectively. A difference of approximately 1.5–2.2 s is considered clinically meaningful [6,15], demonstrating the benefit of ataluren in the 6MWD 300–400 m subgroup and in the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup. It has been shown previously that functional abilities in DMD are lost sequentially, with the ability to stand from supine being lost first, followed by the loss of ability to climb four stairs, and finally the loss of ability to walk/run 10 m [13]. This suggests that patients in the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup may be more stable than expected, which may explain why no differences were seen in the ability to walk/run 10 m between ataluren- and placebo-treated patients.
Results from Study 041 build upon the body of evidence demonstrating that ataluren slows motor function decline and is associated with a favorable benefit–risk profile (a consistent adverse event profile) in patients with nmDMD [7]. To add to the totality of evidence, pooled analyses of a large, heterogeneous population of 701 patients from the ITT populations of Study 041, ACT DMD and Study 007 were performed; these results show that ataluren treatment resulted in a reduced decline in motor function across multiple clinically meaningful end points compared with placebo (Supplementary Figure 5). Pooled analyses can also be useful when assessing subgroup effects as they can increase the sample size [25]; the pooled analysis of the 6MWD 300–400 m subgroups from these studies also showed an even greater reduction in decline in 6MWD with ataluren compared with placebo, highlighting the consistent effect of ataluren treatment on slowing motor function decline.
As DMD progresses, all patients will eventually lose ambulation [26]. Although ataluren slows disease progression, it does not halt it, meaning that patients receiving ataluren will still lose ambulation but the time to LoA will likely be delayed, as demonstrated by data from Study 019 [27]. This was a phase III trial assessing ataluren safety in patients with nmDMD who received ataluren plus SoC. In this study, ataluren plus SoC was associated with a 2.2-year delay in LoA (p = 0.0006) compared with SoC alone in propensity score-matched patients from the Cooperative International Neuromuscular Research Group (CINRG) Duchenne Natural History Study (DNHS) [27]. In the STRIDE Registry, as of January 2023, ataluren plus SoC significantly delayed age at LoA by 3.5 years compared with SoC alone in CINRG DNHS patients (data not published) [11]. In the first 48 weeks of Study 041, 4/183 ataluren-treated patients (2.2%) and 8/176 patients who received placebo (4.5%) lost ambulation in the ITT population. These findings are consistent with those from previous 48-week trials: in Study 007, 4/57 ataluren-treated patients (7%) and 6/57 patients who received placebo (11%) lost ambulation; and in ACT DMD, 9/114 ataluren-treated patients (8%) and 14/114 patients who received placebo (12%) lost ambulation (Supplementary Table 5) [6,8]. By week 72 of Study 041, as expected with further disease progression, 12/183 ataluren-treated patients (6.6%) and 20/176 patients who received placebo (11.4%) lost ambulation. Similar LoA results were observed in the 6MWD 300–400 m subgroup both at 48 and 72 weeks. Interestingly, 12/12 ataluren-treated patients (100%) and 19/20 placebo-treated patients (95.0%) who lost ambulation had a baseline time to stand from supine of <5 s, which is a prognostic indicator of functional decline and subsequent LoA (Supplementary Table 4) [28].
In addition to delaying time to LoA, ataluren plus SoC significantly delayed age at decline to percent-predicted forced vital capacity of <60% and <50% by 1.8 and 2.3 years, respectively [10], demonstrating the benefits of ataluren after LoA. Furthermore, in a study looking at off-label ataluren use in nonambulatory patients, serial echocardiography, pulmonary lung function tests and assessment of muscle strength indicated mild attenuation of disease progression 18–26 months after the initiation of ataluren treatment [29]. Study 041 was the first trial of ataluren to investigate changes in upper limb function. Although there were no differences in any of the PUL assessments in the ITT population, probably owing to the relatively young patients in this population (Table 1), differences from baseline to week 72 were seen between ataluren- and placebo-treated patients in high-level shoulder scores and in mid-level elbow scores in the sensitive 6MWD 300–400 m subgroup. This further demonstrates the beneficial effect of ataluren treatment on milestones beyond those relating to ambulation (Supplementary Table 7).
Safety results for ataluren were similar to those for placebo, indicating that TEAEs were largely attributable to underlying disease and current SoC, including concomitant corticosteroid treatment. Overall, the safety profile of ataluren was favorable (Table 2) and consistent with previous clinical trials and the STRIDE Registry [6,8–10,27,30]. In fact, in a study of ataluren use in nonambulatory patients, a reduction in body mass index was observed [29]. There were no adverse clinical effects or relevant abnormalities in routine laboratory values [29]. In ACT DMD, ataluren was generally well tolerated and no new safety signals were identified. The data showing clinical benefit are particularly important when considering the fatal nature of nmDMD [8].
Concerns have been raised about the safety profile of givinostat, a histone deacetylase inhibitor for treating DMD [31]. Givinostat has been reported to cause thrombocytopenia and hypertriglyceridemia [32]. Therefore, platelet count and triglyceride level monitoring are necessary, and dose adjustments, treatment suspension or treatment discontinuation may be required [32]. These safety concerns have not been reported with ataluren use.
Treatment effects are likely to vary owing to the heterogeneity of DMD [33], making subgroup analyses necessary [25]. Historically in DMD clinical trials, subgroups have been defined by baseline levels of function to enrich for predictable disease progression to show a more robust short-term effect, particularly when there is a concern that the broader ITT population is not sufficiently powered to demonstrate a short-term treatment benefit [6,8]. This was the largest phase III study ever conducted in DMD; therefore, it was adequately powered to demonstrate a significant treatment effect in the broad ITT population. The prespecified subgroups in this study (6MWD 300–400 m, and 6MWD ≥300 m and time to stand from supine ≥5 s) were selected to include patients who were likely to experience functional decline during the study period and in whom a treatment effect could be better captured. Both subgroups included the ≥300 m threshold in 6MWD. The use of time to stand from supine ≥5 s as an inclusion criterion for the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup was unsuccessful in enriching for patients who experienced a treatment effect, and no differences between ataluren and placebo were observed for 6MWD, time to 10% persistent worsening in 6MWD, NSAA, 10 m walk/run time and time to descend four stairs in this subgroup. This is likely because this group includes patients who have a 6MWD of >350–400 m. Findings from natural history studies show that patients with a baseline 6MWD of >400 m have fewer declines across multiple measures of physical function compared with patients with a baseline 6MWD of <400 m [8,15]. This may explain why the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup was less sensitive than the ITT population and why the 6MWD 300–400 m subgroup was the most sensitive in showing a treatment benefit for the selected end points in this study. Of the 185 patients in the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup, 60 (32.4%) had a 6MWD ≥400 m; motor function remained more stable in these patients throughout the study than in the other patients in this subgroup, regardless of whether they received ataluren or placebo. This may also explain why results for the primary end point and several secondary end points in this subgroup numerically favored ataluren but did not reach statistical significance.
Considering the complexity and heterogeneity of DMD in terms of disease severity and progression, observing statistically significant treatment effects on disease progression in the short term duration of a clinical trial is challenging; a longer follow-up time is required to observe a true treatment effect [33]. The 18-month, placebo-controlled period of Study 041 enabled a statistically significant treatment effect of ataluren to be attained in a broad ITT population. This study is the first to demonstrate statistically significant delays in motor function decline among multiple clinically meaningful outcomes with ataluren treatment compared with placebo in the ITT population, which includes patients from 69 international sites receiving SoC, including corticosteroids. Nominally significant differences in time to 10% persistent worsening, 5% persistent worsening and 30 m decline in 6MWD were seen in the ITT population and the 6MWD 300–400 m subgroup. Furthermore, ataluren-treated patients had a 36-week median delay in 30 m decline in 6MWD compared with placebo-treated patients, which may be meaningful for patients’ quality of life. A robust treatment effect in 6MWD, TFTs and NSAA was also seen in the sensitive 6MWD 300–400 m subgroup at a magnitude previously demonstrated in ACT DMD [8].
Factors that could be investigated further to help to contextualize the Study 041 data include the potential variability in adherence to DMD SoC guidelines in different participating countries and the impact of the COVID-19 pandemic, which overlapped with Study 041. The results from the open-label period of Study 041 will help to consolidate findings from the 72-week double-blind period [34].
Summary points
•
Ataluren is indicated for patients with nonsense mutation Duchenne muscular dystrophy (nmDMD); it promotes the readthrough of premature stop codons in dystrophin mRNA to enable the production of full-length dystrophin protein.
•
Study 041 was an international, randomized, double-blind, placebo-controlled, phase III, 72-week trial of ataluren in patients with nmDMD followed by a 72-week open-label period. The primary end point of the placebo-controlled period was the slope of change (average rate of change) in 6-minute walk distance (6MWD) from baseline to week 72 (m/week).
•
The analysis of efficacy end points was carried out in the intention-to-treat (ITT) population (n = 359) and two prespecified subgroups: the 6MWD 300–400 m subgroup (n = 169) and the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup (n = 185).
•
In the ITT population, ataluren treatment reduced the average rate of 6MWD change, equivalent to a 21% slower rate of decline in the ataluren group compared with placebo (p = 0.0248).
•
In the 6MWD 300–400 m subgroup, ataluren treatment reduced the average rate of 6MWD change, equivalent to a 30% slower rate of decline in the ataluren group compared with placebo (p = 0.0310).
•
In the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup, there was a 9% slower rate of decline in the ataluren group compared with placebo, but this was not significant (p = 0.3626).
•
A 10% persistent worsening of 6MWD is a clinically meaningful milestone, which is predictive of loss of ambulation. Ataluren treatment delayed the median time to 10% persistent worsening of 6MWD compared with placebo in the ITT population and in the 6MWD 300–400 m subgroup (p = 0.0078 and p = 0.0011, respectively), but not in the 6MWD ≥300 m and time to stand from supine ≥5 s subgroup (p = 0.0659).
•
Ataluren was well tolerated in patients with nmDMD and had a safety profile consistent with that shown in previous clinical trials and in the Strategic Targeting of Registries and International Database of Excellence.
•
Study 041 is the largest study of patients with Duchenne muscular dystrophy to date and builds upon the body of evidence demonstrating the benefits of ataluren in slowing motor function decline along with a favorable benefit–risk profile in patients with nmDMD.
Author contributions
D Vlodavets, S Wu, A Kostera-Pruszczyk, J-H Chae, S Gulati, J-H Shin, Michelle Lorentzos, Anita Cairns, Yuh-Jyh Jong, H Komaki1, J Statland1, A Prufer de Queiroz Campos Araujo, J Gurgel-Giannetti, Y Takeshima, RE Escobar Cedillo, P Karachunski, K Haginoya and V Penematsa contributed to data curation, writing – reviewed and edited the manuscript draft, and approved the final version that was submitted. C Chou contributed to the formal analysis and interpretation of data, writing – reviewed and edited the manuscript draft, and approved the final version that was submitted. P Williams and C Werner contributed to the interpretation of data, writing – reviewed and edited the manuscript draft, and approved the final version that was submitted.19, CM McDonald contributed to conceptualization, data curation, writing – reviewed and edited the manuscript draft, and approved the final version that was submitted.
Acknowledgments
The authors thank the patients and their families for their participation in the Study 041 clinical trial, and the individuals involved in the conduct of this study. The authors also thank the Study 041 investigators: Hoda Abdel-Hamid, Russell Butterfield, Saunder Bernes, Craig Campbell, Sophelia Chan Hoi Shan, Arijit Chattopadhyay, John Day, Darryl De Vivo, Micaela del Rosari Avila Cobo, Hacer Durmus, Maria Bernadete Dutra de Resende, Erika Finanger, Velina Guergueltcheva, Maina Kava, Jeehun Lee, Wang-Tso Lee, Hanns Lochmuller, Tim Lotze, Xinguo Lu, Neeharika Lakshmi Mathukumalli, Yoshihiro Maegaki, Weldon Mauney III, Tsuyoshi Matsumura, Ryan Monique, Sumitha Murugesu, Aditya Nair, Atchayaram Nalini, Erin Neil Knierbein, Katsuhisa Ogata, Shiro Ozasa, Seth Perlman, Leigh Ramos-Platt, Matilde Ruiz-Garcia, Crystal Proud, Dimitry Rudenko, Shinji Saitoh, Naveen Sankhyan, Oranee Sanmaneechai, Siddharth Shah, Jonathan Strober, Cuixia Tian, Meow Keong Thong, Vrajesh Udani, Venkataraman Viswanathan, Ning Wang, Fei Yin, Takeshi Yoshida and Shuizhen Zhou. The authors also thank Greg Gordon, Panayiota Trifillis and Shu-Jui Liang for their contributions to the study. Finally, the authors thank Jill Castle, a parent of a patient with nmDMD, who has helped with the development of the Plain Language Summary abstract.
Financial disclosure
This work was funded by PTC Therapeutics.
Competing interests disclosure
S Wu, J-H Chae, S Gulati, Y Takeshima, P Karachunski and K Haginoya have no conflicts of interest. D Vlodavets has acted as a principal investigator of clinical trials for BIOCAD, Biogen, Modis Therapeutics, Novartis, NS Pharma, Pfizer, PTC Therapeutics, Roche and Sarepta Therapeutics. A Kostera-Pruszczyk has received advisory board fees from Pfizer, PTC Therapeutics, Roche and Sarepta Therapeutics; has received lecture fees and travel support from PTC Therapeutics and Roche; and has acted as a pricipal investigator for DMD clinical trials sponsored by GlaxoSmithKline, Pfizer, PTC Therapeutics and Sarepta Therapeutics. J-H Shin has acted as a principal investigator on DMD clinical trials sponsored by PTC Therapeutics, Pfizer, Sarepta Therapeutics and Nippon Shinyaku. M Lorentzos has acted as a principal investigator on clinical trials for PTC Therapeutics, Sarepta Therapeutics, Pfizer, and NS Pharma and has consulted on advisory boards for Roche, Sarepta Therapeutics and Biogen. A Cairns has acted as a principal investigator of clinical trials for Biogen, NS Pharma, Pfizer, PTC Therapeutics and Sarepta Therapeutics; and has received fees for participation in advisory boards from Biogen, Novartis and Roche. YJ Jong has acted as a principal investigator of clinical trials for Biogen, Novartis, NS Pharma, Pfizer, PTC Therapeutics, Roche and Sarepta Therapeutics. H Komaki has acted as a consultant on clinical trials for Kaneka, Taiho Pharmaceutical and Takeda; and has received research support for clinical trials from Nippon Shinyaku, Pfizer, PTC Therapeutics, Sarepta Therapeutics and Taiho Pharmaceutical. J Statland has received grant funding from the Friends of FSH Research, FSHD Canada, FSHD Society, MDA and NIH; and is a consultant or has served on advisory boards for Avidity Biosciences, Dyne Therapeutics, Fulcrum Therapeutics, ML Bio, Roche and Sarepta Therapeutics. A Prufer de Queiroz Campos Araujo has acted as a principal investigator of clinical trials for GlaxoSmithKline, PTC Therapeutics, Roche and Sarepta Therapeutics. J Gurgel-Giannetti has acted as a principal investigator of clinical trials for PTC Therapeutics, Biogen, Novartis and Roche, and has served on advisory boards for Roche, Biogen and Novartis. RE Escobar Cedillo has acted as a principal investigator of clinical trials for PTC Therapeutics. V Penematsa, C Chou, P Williams and C Werner are employees of PTC Therapeutics. CM McDonald has acted as a consultant for DMD clinical trials for Astellas, Capricor Therapeutics, Catabasis Pharmaceuticals, Catalyst Pharmaceuticals, Edgewise Therapeutics, Epirium Bio (formerly Cardero Therapeutics), FibroGen, Italfarmaco, Pfizer, PTC Therapeutics, Santhera Pharmaceuticals, Sarepta Therapeutics and Solid Biosciences; and has received research support for clinical trials from Capricor Therapeutics, Catabasis, Catalyst Pharmaceuticals, Edgewise Therapeutics, Italfarmaco, Pfizer, PTC Therapeutics, Santhera Pharmaceuticals, Sarepta Therapeutics and Solid Biosciences. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by Dina Dakkak and Tim Ellison of PharmaGenesis London, London, UK and was funded by PTC Therapeutics.
Data sharing statement
The authors certify that this manuscript reports clinical trial data (NCT03179631). The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available owing to privacy or ethical restrictions.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Birnkrant DJ, Bushby K, Bann CM et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular, rehabilitation, endocrine, and gastrointestinal and nutritional management. Lancet Neurol. 17(3), 251–267 (2018).
2.
Bello L, Pegoraro E. Genetic diagnosis as a tool for personalized treatment of Duchenne muscular dystrophy. Acta Myol. 35(3), 121–127 (2016).
3.
Pichavant C, Aartsma-Rus A, Clemens PR et al. Current status of pharmaceutical and genetic therapeutic approaches to treat DMD. Mol. Ther. 19(5), 830–840 (2011).
4.
Welch EM, Barton ER, Zhuo J et al. PTC124 targets genetic disorders caused by nonsense mutations. Nature 447(7140), 87–91 (2007).
•• Describes ataluren's mechanism of action including its oral bioavailability and pharmacological properties.
5.
Haas M, Vlcek V, Balabanov P et al. European Medicines Agency review of ataluren for the treatment of ambulant patients aged 5 years and older with Duchenne muscular dystrophy resulting from a nonsense mutation in the dystrophin gene. Neuromuscul. Disord. 25(1), 5–13 (2015).
6.
Bushby K, Finkel R, Wong B et al. Ataluren treatment of patients with nonsense mutation dystrophinopathy. Muscle Nerve 50(4), 477–487 (2014).
•• Reports findings from a phase IIb, randomized, double-blind, placebo-controlled, multicenter trial of ataluren in patients with nonsense mutation Duchenne muscular dystrophy (nmDMD) aged 5 years or older.
7.
Campbell C, Barohn RJ, Bertini E et al. Meta-analyses of ataluren randomized controlled trials in nonsense mutation Duchenne muscular dystrophy. J. Comp. Eff. Res. 9(14), 973–984 (2020).
•• Reports results from meta-analyses of two randomized, placebo-controlled trials of ataluren in patients with nmDMD (phase IIb and phase III).
8.
McDonald CM, Campbell C, Torricelli RE et al. Ataluren in patients with nonsense mutation Duchenne muscular dystrophy (ACT DMD): a multicentre, randomised, double-blind, placebo-controlled, Phase III trial. Lancet 390(10101), 1489–1498 (2017).
•• Reports findings from a phase III, randomized, double-blind, placebo-controlled, multicenter trial of ataluren in patients with nmDMD aged 7–16 years.
9.
Mercuri E, Muntoni F, Osorio AN et al. Safety and effectiveness of ataluren: comparison of results from the STRIDE Registry and CINRG DMD Natural History Study. J. Comp. Eff. Res. 9(5), 341–360 (2020).
10.
Mercuri E, Osorio AN, Muntoni F et al. Safety and effectiveness of ataluren in patients with nonsense mutation DMD in the STRIDE Registry compared with the CINRG Duchenne Natural History Study (2015–2022): 2022 interim analysis. J. Neurol. 1–18 (2023).
•• Reports real-world data on the safety and effectiveness of ataluren in patients with nmDMD from the Strategic Targeting of Registries and International Database of Excellence (STRIDE) Registry, from the January 2022 data cut.
11.
Muntoni F, Desguerre I, Guglieri M et al. Ataluren use in patients with nonsense mutation Duchenne muscular dystrophy: patient demographics and characteristics from the STRIDE Registry. J. Comp. Eff. Res. 8(14), 1187–1200 (2019).
12.
Straub V, Mercuri E, Aartsma-Rus A et al. Report on the workshop: meaningful outcome measures for Duchenne muscular dystrophy, London, UK, 30–31 January 2017. Neuromuscul. Disord. 28(8), 690–701 (2018).
13.
Arora H, Willcocks RJ, Lott DJ et al. Longitudinal timed function tests in Duchenne muscular dystrophy: imaging DMD cohort natural history. Muscle Nerve 58(5), 631–638 (2018).
14.
Goemans N, Vanden Hauwe M, Signorovitch J et al. Individualized prediction of changes in 6-minute walk distance for patients with Duchenne muscular dystrophy. PLoS One 11(10), e0164684 (2016).
15.
McDonald CM, Henricson EK, Abresch RT et al. The 6-minute walk test and other endpoints in Duchenne muscular dystrophy: longitudinal natural history observations over 48 weeks from a multicenter study. Muscle Nerve 48(3), 343–356 (2013).
• Determines the natural history of clinical measures of disease progression in ambulatory patients with Duchenne muscular dystrophy (DMD), estimates the probability and predictors of clinically meaningful disease progression (defined as persistent 10% worsening in 6-minute walk distance [6MWD]), and assesses the relationship between 6MWD and loss of ambulation from a phase IIb trial.
16.
Mayhew A, Cano S, Scott E et al. North Star Clinical Network for Neuromuscular Disease. Detecting meaningful change using the North Star Ambulatory Assessment in Duchenne muscular dystrophy. Dev. Med. Child Neurol. 55(11), 1046–1052 (2013).
17.
Mayhew A, Cano S, Scott E et al. Moving towards meaningful measurement: Rasch analysis of the North Star Ambulatory Assessment in Duchenne muscular dystrophy. Dev. Med. Child Neurol. 53(6), 535–542 (2011).
18.
McDonald C, Duong T, Henricson E et al. P. 2.11 CINRG Duchenne Natural History Study: relationship of longitudinal measures of ambulatory timed function tests and loss of clinical milestones. Neuromuscul. Disord. 23(9), 752 (2013).
19.
McDonald CM, Henricson EK, Abresch RT et al. The 6-minute walk test and other clinical endpoints in Duchenne muscular dystrophy: reliability, concurrent validity, and minimal clinically important differences from a multicenter study. Muscle Nerve 48(3), 357–368 (2013).
20.
Bohannon RW, Crouch R. Minimal clinically important difference for change in 6-minute walk test distance of adults with pathology: a systematic review. J. Eval. Clin. Pract. 23(2), 377–381 (2017).
21.
Mazzone E, Martinelli D, Berardinelli A et al. North Star Ambulatory Assessment, 6-minute walk test and timed items in ambulant boys with Duchenne muscular dystrophy. Neuromuscul. Disord. 20(11), 712–716 (2010).
22.
Ayyar Gupta V, Pitchforth JM, Domingos J et al. Determining minimal clinically important differences in the North Star Ambulatory Assessment (NSAA) for patients with Duchenne muscular dystrophy. PLoS One 18(4), e0283669 (2023).
23.
Dang UJ, Damsker JM, Guglieri M et al. Efficacy and safety of vamorolone over 48 weeks in boys with Duchenne muscular dystrophy: a randomized controlled trial. Neurology 102(5), e208112 (2024).
24.
McDonald CM. Timed function tests have withstood the test of time as clinically meaningful and responsive endpoints in Duchenne muscular dystrophy. Muscle Nerve 58(5), 614–617 (2018).
25.
Rothwell PM. Treating individuals 2. Subgroup analysis in randomised controlled trials: importance, indications, and interpretation. Lancet 365(9454), 176–186; 17709-5 (2005).
26.
McDonald CM, Marden JR, Shieh PB et al. Disease progression rates in ambulatory Duchenne muscular dystrophy by steroid type, patient age and functional status. J. Comp. Eff. Res. 12(4), e220190 (2023).
27.
McDonald CM, Muntoni F, Penematsa V et al. Ataluren delays loss of ambulation and respiratory decline in nonsense mutation Duchenne muscular dystrophy patients. J. Comp. Eff. Res. 11(3), 139–155 (2021).
28.
Zambon AA, Ayyar Gupta V, Ridout D et al. Peak functional ability and age at loss of ambulation in Duchenne muscular dystrophy. Dev. Med. Child Neurol. 64(8), 979–988 (2022).
• Investigates the relationship between functional abilities and age at loss of ambulation in patients with DMD.
29.
Ebrahimi-Fakhari D, Dillmann U, Flotats-Bastardas M et al. Off-label use of ataluren in four non-ambulatory patients with Duchenne muscular dystrophy: effects on cardiac and pulmonary function and muscle strength. Front. Pediatr. 6316 (2018).
30.
Roy B, Friesen WJ, Tomizawa Y et al. Ataluren stimulates ribosomal selection of near-cognate tRNAs to promote nonsense suppression. Proc. Natl Acad. Sci. U.S.A. 113(44), 12508–12513 (2016).
31.
Bettica P, Petrini S, D'Oria V et al. Histological effects of givinostat in boys with Duchenne muscular dystrophy. Neuromuscul. Disord. 26(10), 643–649 (2016).
32.
Anjum AF, Anjum MB, ur Rehman R. Unleashing the potential of givinostat: a novel therapy for Duchenne muscular dystrophy. Curr. Ther. Res., 102100787 (2025).
33.
Fang Y, McDonald CM, Clemens PR et al. Modeling early heterogeneous rates of progression in boys with Duchenne muscular dystrophy. J. Neuromuscul. Dis. 10(3), 349–364 (2023).
34.
McDonald CM, Henricson EK, Abresch RT et al. Long-term effects of glucocorticoids on function, quality of life, and survival in patients with Duchenne muscular dystrophy: a prospective cohort study. Lancet 391(10119), 451–461 (2018).
Information & Authors
Information
Published In
Copyright
© 2025 PTC Therapeutics. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 20 December 2024
Accepted: 21 July 2025
Published online: 22 August 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Confirmatory long-term efficacy and safety results of ataluren in patients with nmDMD from Study 041, an international, randomized, double-blind, placebo-controlled, Phase III trial. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0238
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Genevieve Edobor, Ronald Huber, Christoph Reiter, Hanna Gercke, Niklas Kaefer, Elli Kronsteiner, Bjoern Wimmer, Marlies Wimmer, Thomas Karl, Mark Rinnerthaler, Jan Krauß, Heinrich Krobath, Thomas Mohr, Christopher Gerner, Joerg von Hagen, Norbert Müller, Helmut Hintner, Bernadette Liemberger, Ulrich Koller, Johann W. Bauer, Gazmend Temaj, Hannelore Breitenbach-Koller, RiboScreenTM Technology Delivers Small-Molecule Ribodrugs to Convert Ribosomal Proteins into Molecular Valves for Tailored Protein Production Levels in Rare and Prevalent Disease, Biomedicines, 10.3390/biomedicines14071419, 14, 7, (1419), (2026).
- Leyken Wilson, Lucy M. Johnson, Daniel J. Berlau, Advances in the pharmacotherapeutic management of duchenne muscular dystrophy: an update, Expert Opinion on Pharmacotherapy, 10.1080/14656566.2026.2652459, 27, 4, (365-378), (2026).