Matching-adjusted indirect comparisons of diroximel fumarate, ocrelizumab and interferon beta-1a for relapsing multiple sclerosis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study compares the efficacy of diroximel fumarate (DRF) with ocrelizumab (OCR) and interferon beta-1a (IFNβ-1a) for treating relapsing multiple sclerosis (MS) through matching-adjusted indirect comparisons (MAICs). Materials & methods: We used individual patient data from the EVOLVE-MS-1 (NCT02634307) study, the phase III trial of DRF (n = 1057), and group-level data from the OPERA I/II studies (NCT01247324 and NCT01412333), the 96-week, randomized, double-blind, phase III trials of OCR (n = 827) and IFNβ-1a (n = 829). EVOLVE-MS-1 data were adjusted to match the inclusion/exclusion criteria and baseline characteristics of OPERA I/II participants. Comparisons were made for annualized relapse rates (ARRs), confirmed disability progression (CDP) and radiological outcomes. Results: Baseline characteristics were balanced post-adjustment. ARR comparisons at 96 weeks showed no significant difference for DRF versus OCR (0.18 vs 0.16, p = 0.347) but favored DRF over IFNβ-1a (0.19 vs 0.29, p = 0.002). At 96 weeks, there were no significant differences in rates of 12-week or 24-week CDP between DRF and OCR (12 week: 6.4 vs 9.1%, p = 0.074; 24 week: 4.8 vs 6.9%, p = 0.14); both CDP outcomes favored DRF over IFNβ-1a (12 week: 6.5 vs 13.6%, p < 0.0001; 24 week: 4.9 vs 10.5%, p < 0.0001). The proportion of patients with gadolinium-enhancing lesions was higher for DRF versus OCR (16.4 vs 9.1%, p < 0.0001) but lower for DRF versus IFNβ-1a (15.7 vs 33.2%, p < 0.0001). The proportion of patients with new/newly enlarging T2 lesions was higher for DRF versus OCR (59.5 vs 38.7%, p < 0.0001), but there was no significant difference for DRF versus IFNβ-1a (58.4 vs 61.7%). Conclusion: While there were no significant differences in clinical outcomes (ARR, 12-week CDP and 24-week CDP) observed for DRF versus OCR, radiological outcomes indicated favorability for OCR. All outcomes favored DRF over IFNβ-1a, except from new/newly enlarging T2 lesions, which showed no significant difference.
Plain language summary
What is this article about?
This article looks at how three different multiple sclerosis (MS) treatments – diroximel fumarate (DRF), ocrelizumab (OCR) and interferon beta-1a (IFNβ-1a) – compare for people with relapsing MS. The authors applied a statistical approach to balance differences among patients in separate studies, aiming to see how well each medication reduces the number of relapses, slows disability progression and affects brain lesions seen on MRI scans.
What were the results?
DRF and OCR had similar effects on relapse rates and disability progression; however, OCR showed fewer new or active brain lesions. When compared with IFNβ-1a, DRF resulted in fewer relapses and lower rates of disability, though it did not differ much from IFNβ-1a in some types of lesions.
What do the results mean?
These findings suggest that in some cases, DRF may be a good treatment option to reduce relapses and stabilize disability. DRF also appears more effective than IFNβ-1a overall. This information can help people with MS and their healthcare providers consider the pros and cons of each treatment option, but it is important to note that these comparisons are based on indirect analyses, which have limitations. Individual patient factors and preferences should always be considered when choosing a treatment. Therefore, a personalized approach is essential when starting a new therapy for relapsing MS.
Multiple sclerosis (MS) is a chronic demyelinating disease of the central nervous system, affecting approximately 2.8 million people globally [1], and has substantial economic impact and high burden for patients and their caregivers [2,3], especially when treatment is suboptimal [4].
Diroximel fumarate (DRF), ocrelizumab (OCR) and interferon beta-1a (IFNβ-1a) are disease-modifying therapies (DMTs) approved in the USA for the treatment of relapsing forms of MS, and in Europe, DRF and IFNβ-1a are approved for the treatment of relapsing-remitting MS, while OCR is approved for relapsing forms of MS [5–11]. The route of administration of DMTs and frequency of dosing are important considerations for patients with MS with many patients preferring oral DMTs over infusions and injections [12]. The convenience of oral DMTs may contribute to improved patient satisfaction and increased treatment adherence [13,14].
DRF is an oral DMT taken twice daily, approved based on bioequivalence with dimethyl fumarate (DMF), that has demonstrated better tolerability and fewer discontinuations than DMF [15–17], which could lead to increased adherence. Efficacy and safety of DRF were evaluated in the 2-year, open-label, single-arm, phase III EVOLVE-MS-1 study (NCT02634307) [18]. OCR is a humanized monoclonal antibody that selectively depletes B cells with CD20 markers [19]. IFNβ-1a is an immunomodulatory cytokine that reduces T-cell migration across the blood-brain barrier and shifts cytokine expression from pro-inflammatory to anti-inflammatory [20]. In two identical 2-year, randomized, double-blind, active-controlled, phase III studies, OPERA I (NCT01247324) and OPERA II (NCT01412333), intravenous OCR was associated with lower rates of clinical and MRI measures of disease activity versus subcutaneous IFNβ-1a in patients with relapsing MS [19]. In EVOLVE-MS-1, DRF demonstrated a favorable safety profile with a discontinuation rate due to adverse events (AEs) of 8.0% over 96 weeks, with gastrointestinal or flushing/flushing-related accounting for <2% of AEs [17]. In the OPERA I/II studies, discontinuation rates due to AEs were 3.5% in those treated with OCR and 6.2% in those treated with IFNβ-1a [19].
Matching-adjusted indirect comparisons (MAICs) can be used to adjust for potential cross-trial differences in patient populations and compare the efficacy of MS DMTs from separate studies. In previous investigations using the MAIC method, DRF had similar efficacy to sphingosine1-phosphate receptor modulators and better efficacy than teriflunomide and IFNβ-1a in all clinical and most radiological outcomes [21,22]. However, no prior MAICs have compared DRF with OCR. A comparison of the efficacy of DRF versus OCR and IFNβ-1a is of value to patients and clinicians when selecting treatment options, but no randomized trials have directly compared DRF versus OCR or IFNβ-1a. Therefore, we conducted an MAIC to evaluate the comparative efficacy of DRF, OCR and IFNβ-1a.
The objectives of this study were to compare the efficacy of DRF versus OCR and DRF versus IFNβ-1a for clinical outcomes (annualized relapse rate [ARR], 12-week confirmed disability progression [CDP], and 24-week CDP) and radiological outcomes (absence of gadolinium-enhancing [Gd+] T1 lesions and absence of new/newly enlarging [N/NE] T2 lesions) using MAIC.
Materials & methods
Study design
This analysis included individual patient data from EVOLVE-MS-1, a 96-week, open-label, single-arm, phase III study of DRF (462 mg bid; n = 1057) [17], and group-level data from the phase III, randomized, double-blind OPERA I/II studies of OCR (600 mg every 24 weeks; n = 827) and IFNβ-1a (44 μg three-times weekly; n = 829) (Figure 1) [19]. OPERA I/II was selected as the comparator study for several reasons: it represents a phase III trial of OCR with the same trial duration and MS diagnostic criteria as EVOLVE-MS-1, which is important because newer phase III MS trials tend to have lower ARRs than older trials; the IFNβ-1a population was already randomized and matched with the OCR population within OPERA I/II, enabling us to conduct two MAICs with matched populations and we have successfully applied this methodology in previous MAICs [21,23]. OPERA I and OPERA II used identical study protocols but were conducted independently at nonoverlapping trial sites. Study designs for EVOLVE-MS-1 and OPERA I/II were previously reported [17,19].
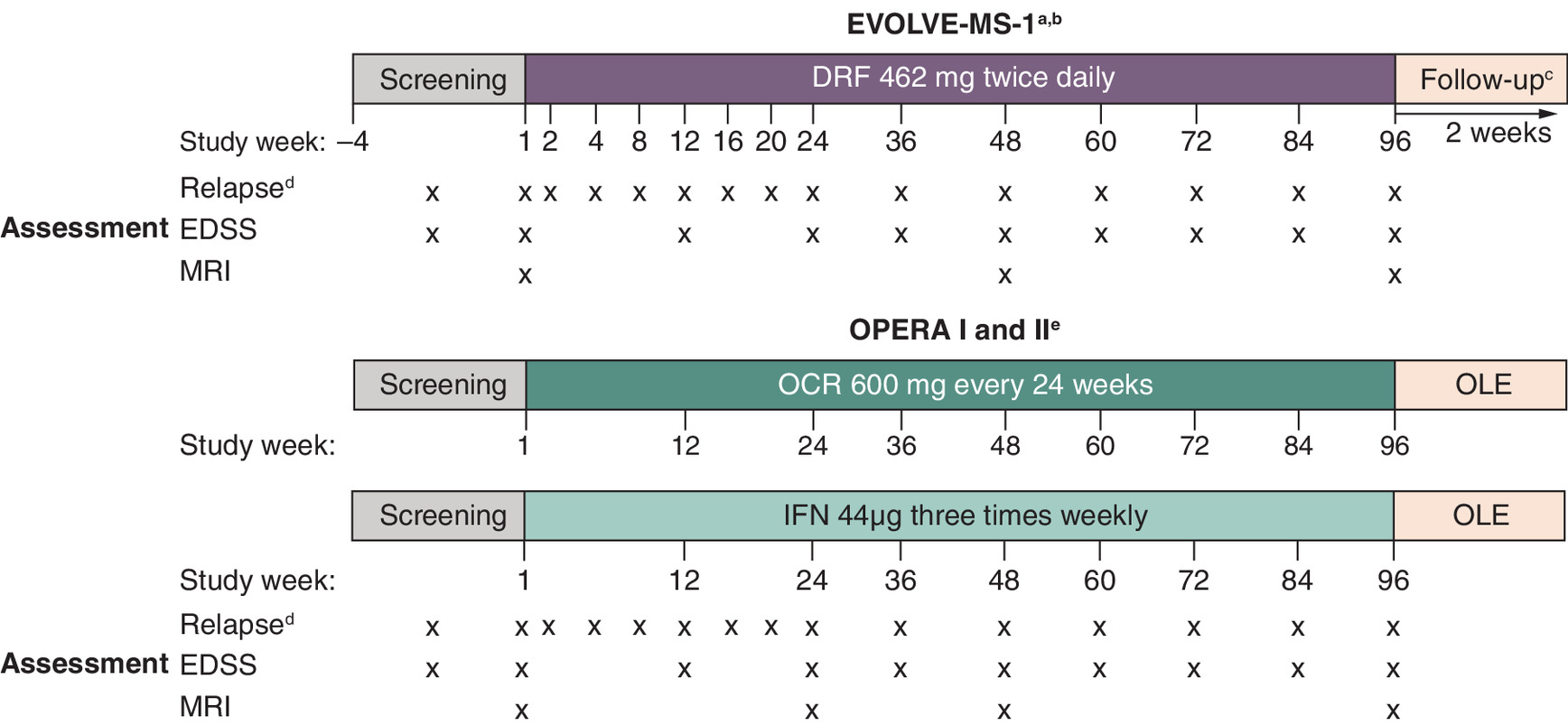
Figure 1. Study designs of EVOLVE-MS-1 and OPERA I/II.
Adapted from Naismith RT et al. [24].
bA subset of patients (n = 464; 43.9%) in EVOLVE-MS-1 rolled over from the 5-week, phase III EVOLVE-MS-2 study (NCT03093324) of DRF or DMF. Efficacy outcomes were assessed in EVOLVE-MS-1.
cA 2-week safety follow-up was required for all patients in EVOLVE-MS-1; lymphocyte monitoring follow-up visits were required for a further 6 months for patients who discontinued or completed treatment with absolute lymphocyte count <0.8 × 109/l.
dIn the event of a suspected relapse, unscheduled relapse visits were conducted.
eAdapted from Hauser SL et al. [19].
DMF: Dimethyl fumarate; DRF: Diroximel fumarate; EDSS: Expanded Disability Status Scale; IFNβ-1a: Interferon beta-1a; OCR: Ocrelizumab; OLE: Open label extension.
To match the trial populations, we compared the inclusion and exclusion criteria for EVOLVE-MS-1 and OPERA I/II. Consistent with the inclusion and exclusion criteria of OPERA I/II, we restricted the EVOLVE-MS-1 sample to patients aged between 18 and 55 years at baseline, had an Expanded Disability Status Scale (EDSS) score of 0–5.5 at baseline, and had a diagnosis of MS in line with the revised McDonald criteria (2010). The EVOLVE-MS-1 sample was also restricted by key exclusion criteria from OPERA I/II including disease duration >10 years in patients with EDSS ≤2.0 at screening and known presence of the following disorders: neuromyelitis optica, Lyme disease, untreated vitamin B12 deficiency, neurosarcoidosis, cerebrovascular disorders, tuberculosis, HIV and syphilis. EVOLVE-MS-1 data were then weighted separately to match baseline characteristics in the OCR and IFNβ-1a treatment arms of the combined data from OPERA I and II.
Baseline variables that could influence treatment selection and response and affect treatment measures in comparisons of DRF versus OCR and DRF versus IFNβ-1a for the clinical and radiological outcomes included age, sex, race, time since first MS symptoms, time since MS diagnosis, number of relapses in the 12 months before study entry (matched by both mean and standard deviation), EDSS score, brain MRI Gd+ lesions, T2 lesion volume at baseline, MS DMT history and region (US vs countries outside of the US).
Efficacy outcomes
Clinical end points were ARRs over 96 weeks and time to onset of 12- and 24-week CDP on the EDSS. In EVOLVE-MS-1, CDP was determined according to the methodology outlined in the ‘Trial Procedures and End Points’ section of Hauser et al. [19]. Definitions and schedules of assessment of MS relapse, disability progression and EDSS in EVOLVE-MS-1 and OPERA I/II are summarized in Supplementary Table 1. Absence of Gd+ T1 lesions and N/NE T2 lesions were assessed using MRI. In EVOLVE-MS-1, brain MRIs were performed at weeks 1, 48 and 96. In OPERA I/II, brain MRIs were obtained at weeks 1, 24, 48 and 96. Week 96 outcomes were compared between EVOLVE-MS-1 and OPERA I/II.
Statistical analysis
The summary statistics of baseline characteristics were compared in the EVOLVE-MS-1 sample after applying restrictions based on the inclusion and exclusion criteria for OPERA I/II. We summarized binary variables using proportions and continuous variables using means and standard deviations. To account for cross-trial differences in observed baseline characteristics, we conducted unanchored MAIC analyses. An unanchored MAIC analysis was performed due to the lack of a common comparator between EVOLVE-MS-1 and OPERA I/II. EVOLVE-MS-1 was a single-arm study of DRF, while OPERA I/II compared OCR versus IFNβ-1a. Therefore, individuals in the restricted EVOLVE-MS-1 sample were assigned weights that corresponded to their odds of being enrolled in OPERA I/II versus EVOLVE-MS-1. These weights were derived based on the baseline variables described in the study design section. After weighting patients in EVOLVE-MS-1, we compared DRF versus OCR and DRF versus IFNβ-1a for ARR, 12- and 24-week CDP, absence of Gd+ T1 lesions and absence of N/NE T2 lesions. For both DRF versus OCR and DRF versus IFNβ-1a comparisons, 95% confidence intervals (CIs) were calculated using the Bootstrap method for the outcome of interest as well as differences/ratios. ARR was estimated in the weighted EVOLVE-MS-1 sample using a Poisson regression model with an offset for the logarithm of time on study (years). Incidence rate differences and incidence rate ratios were subsequently calculated, comparing the weighted ARR in DRF-treated patients with the ARRs in OCR- and IFNβ-1a-treated patients. The risk of 12- and 24-week CDP in the weighted EVOLVE-MS-1 sample was estimated using the Kaplan–Meier product-limit method and then risk differences (RDs) and risk ratios (RRs) were calculated for DRF versus OCR and DRF versus IFNβ-1a for 12- and 24-week CDP. The proportion of patients without Gd+ T1 lesions and N/NE T2 lesions was calculated among those with evaluable radiological data at the end of follow-up. We then calculated RDs and RRs for DRF versus OCR and DRF versus IFNβ-1a. Bootstrapping with 1000 samples was used to obtain 95% CIs and p-values around the estimates for all outcomes of interest, accounting for uncertainty in both the sampling error and the weights.
As the EVOLVE-MS-1 population included patients who had received DMF or DRF as part of EVOLVE-MS-2 and then rolled over into EVOLVE-MS-1, a sensitivity analysis was conducted in which the EVOLVE-MS-1 population was limited to only patients who were enrolled de novo. The results for EVOLVE-MS-1 patients who were newly enrolled were comparable with the original results for the full EVOLVE-MS-1 sample.
Results
Characteristics of study patients
After restrictions, 702 patients were retained from the EVOLVE-MS-1 population for these analyses. Baseline characteristics are presented in Table 1. After restriction and weighting, baseline characteristics were well-balanced and comparable for DRF versus OCR and DRF versus IFNβ-1a. Among patients with prior DMT use, interferon was the most common (15.5–19.5%), followed by glatiramer acetate (9.3–10.4%), while natalizumab (0.1–2.4%), fingolimod (0–2.4%) and DMF (0–1.4%) were used minimally (Supplementary Table 2).
| EVOLVE-MS-1 | DRF vs OCR | DRF vs IFNβ-1a | ||||
|---|---|---|---|---|---|---|
| DRF original sample (n = 1057) | DRF restricted sample (n = 702)† | EVOLVE-MS-1 after weighting to match baseline characteristics of OCR (ESS = 273)‡ | OPERA I/II, OCR arm (n = 827) | EVOLVE-MS-1 after weighting to match baseline characteristics of IFNβ-1a (ESS = 280)‡ | OPERA I/II, IFNβ-1a arm (n = 829) | |
| Age, years, mean (SD) | 42.5 (10.8) | 38.9 (9.2) | 37.2 (9.0) | 37.2 (9.2) | 37.2 (9.0) | 37.2 (9.2) |
| Female, % | 72.1 | 70.9 | 65.4 | 65.4 | 66.6 | 66.6 |
| White, % | 92.0 | 91.9 | 89.9 | 89.9 | 91.3 | 91.3 |
| Relapses in past 12 months, n, mean (SD) | 0.72 (0.77) | 0.79 (0.78) | 1.32 (0.67) | 1.32 (0.67) | 1.34 (0.69) | 1.34 (0.69) |
| EDSS score, mean (SD) | 2.7 (1.5) | 2.5 (1.2) | 2.8 (1.2) | 2.8 (1.3) | 2.8 (1.2) | 2.8 (1.3) |
| Gd+ T1 lesions, % | 29.6 | 34.6 | 41.9 | 41.9 | 39.8 | 39.8 |
| T2 lesion volume, cm3, mean (SD) | 12.0 (13.1) | 10.8 (11.5) | 10.8 (14.1) | 10.2 (10.7) | 10.2 (11.8) | |
| Prior DMT use¶, % | 64.4 | 59.1 | 26.7 | 26.7 | 26.6 | 26.6 |
| Time since MS onset, years, mean (SD) | 9.8 (8.3) | 7.3 (6.8) | 6.7 (7.5) | 6.7 (6.2) | 6.5 (7.2) | 6.5 (6.1) |
| Time since MS diagnosis, years, mean (SD) | 7.6 (7.3)# | 5.7 (6.0) | 4.0 (5.9) | 4.0 (4.9) | 3.9 (5.8) | 3.9 (4.9) |
| US, % | 42.9 | 39.3 | 26.2 | 26.2 | 26.4 | 26.4 |
†
Restricted sample after applying OPERA I/II inclusion/exclusion criteria.
‡
Effective sample size after MAIC weighting.
§
Data on baseline characteristics in OCR and IFNβ-1a arms of OPERA I/II were obtained from Hauser et al. taken from [19]. Summary statistics are pooled.
¶
Prior DMT includes immunomodulatory and immunosuppressant (investigational or approved).
#
n = 1056.
DMT: Disease-modifying therapy; DRF: Diroximel fumarate; EDSS: Expanded Disability Status Scale; ESS: Effective sample size; Gd+: Gadolinium-enhancing; IFNβ-1a: Interferon beta-1a; MAIC: Matching-adjusted indirect comparison; MS: Multiple sclerosis; OCR: Ocrelizumab; SD: Standard deviation.
DRF versus OCR
The ARR for DRF-treated patients after weighting was 0.18 (95% CI: 0.14–0.22) compared with 0.16 (95% CI: 0.13–0.19) in OCR-treated patients, indicating no statistically significant difference (incidence rate difference, 0.02 [95% CI: -0.03–0.07], p = 0.347) (Table 2 & Figure 2).
| OPERA I/II† | EVOLVE-MS-1 | DRF vs OCR | DRF vs IFNβ-1a | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OCR | IFNβ-1a | DRF restricted sample | EVOLVE-MS-1, DRF, weighted | Weighted rate/risk difference‡ | Weighted rate/risk ratio‡ | EVOLVE-MS-1, DRF, weighted | Weighted rate/risk difference‡,§ | Weighted rate/risk ratio‡,§ | |
| ARR¶ (95% CI) | n = 827 | n = 829 | n = 705 | ESS = 273 | ESS = 280 | ||||
| 0.16 (0.13–0.19) | 0.29 (0.25–0.33) | 0.15 (0.13–0.18) | 0.18 (0.14–0.22) | 0.02 (-0.03–0.07) | 1.15 (0.78–1.44) | 0.18 (0.14–0.22) | -0.11 (-0.17 to -0.05) | 0.63 (0.45–0.79) | |
| Proportion of patients with disability progression for 12 weeks#, % (95% CI) | n = 827 | n = 829 | n = 705 | ESS = 273 | ESS = 280 | ||||
| 9.1 (7.1–11.1) | 13.6 (11.3–15.9) | 9.6 (7.5–11.8) | 6.4 (3.8–8.7) | -2.7 (-5.9–0.36) | 0.71 (0.37–0.99) | 6.5 (3.8–8.7) | -7.1 (-10.4 to -3.9) | 0.48 (0.26–0.66) | |
| Proportion of patients with disability progression for 24 weeks#, % (95% CI) | n = 827 | n = 829 | n = 705 | ESS = 273 | ESS = 280 | ||||
| 6.9 (5.2–8.7) | 10.5 (8.4–12.7) | 7.1 (5.2–9.1)¶ | 4.8 (2.6–6.9)¶ | -2.1 (-4.9–0.65)¶ | 0.71 (0.29–1.04)¶ | 4.9 (2.6–6.9)¶ | -5.6 (-8.8 to -2.5) | 0.47 (0.19–0.67) | |
| Patients with Gd+ T1 lesions, % (95% CI) | n = 827 | n = 829 | n = 633 | ESS = 250 | ESS = 256 | ||||
| 9.1 (7.1–11.0) | 33.2 (30.0–36.4) | 13.7 (11.1–16.4) | 16.4 (12.1–20.7) | 7.4 (3.1–11.7) | 1.84 (1.19–2.37) | 15.7 (11.4–19.8) | -17.4 (-22.4 to -12.6) | 0.48 (0.35–0.59) | |
| Patients with N/NE T2 lesions, % (95% CI) | n = 827 | n = 829 | n = 633 | ESS = 250 | ESS = 256 | ||||
| 38.7 (35.4–42.0) | 61.7 (58.3–64.9) | 53.4 (49.5–57.3) | 59.5 (55.2–64.6) | 20.9 (14.9–27.0) | 1.54 (1.35–1.72) | 58.4 (53.8–63.5) | -3.2 (-9.2–2.9) | 0.95 (0.85–1.04) | |
†
Data on outcomes in OPERA I/II were obtained from Hauser et al. taken from [19].
‡
Weighted incidence rate differences and incidence rate ratios are presented for ARR. Weighted risk differences and risk ratios are presented for the outcomes of 12- and 24-week CDP, absence of Gd+ T1 lesions, and absence of N/NE T2 lesions.
§
For DRF vs IFNβ-1a, one-sided CIs are presented for weighted incidence rate differences and incidence rate ratios.
¶
ARR was estimated using Poisson regression with robust error variance.
#
Definition for CDP used in OPERA I/II was applied to EVOLVE-MS-1.
ARR: Annualized relapse rate; CDP: Confirmed disability progression; CI: Confidence interval; DRF: Diroximel fumarate; ESS: Effective sample size; Gd+: Gadolinium-enhancing; IFNβ-1a: Interferon beta-1a; MAIC: Matching-adjusted indirect comparison; N/NE: New/newly enlarging; OCR: Ocrelizumab.
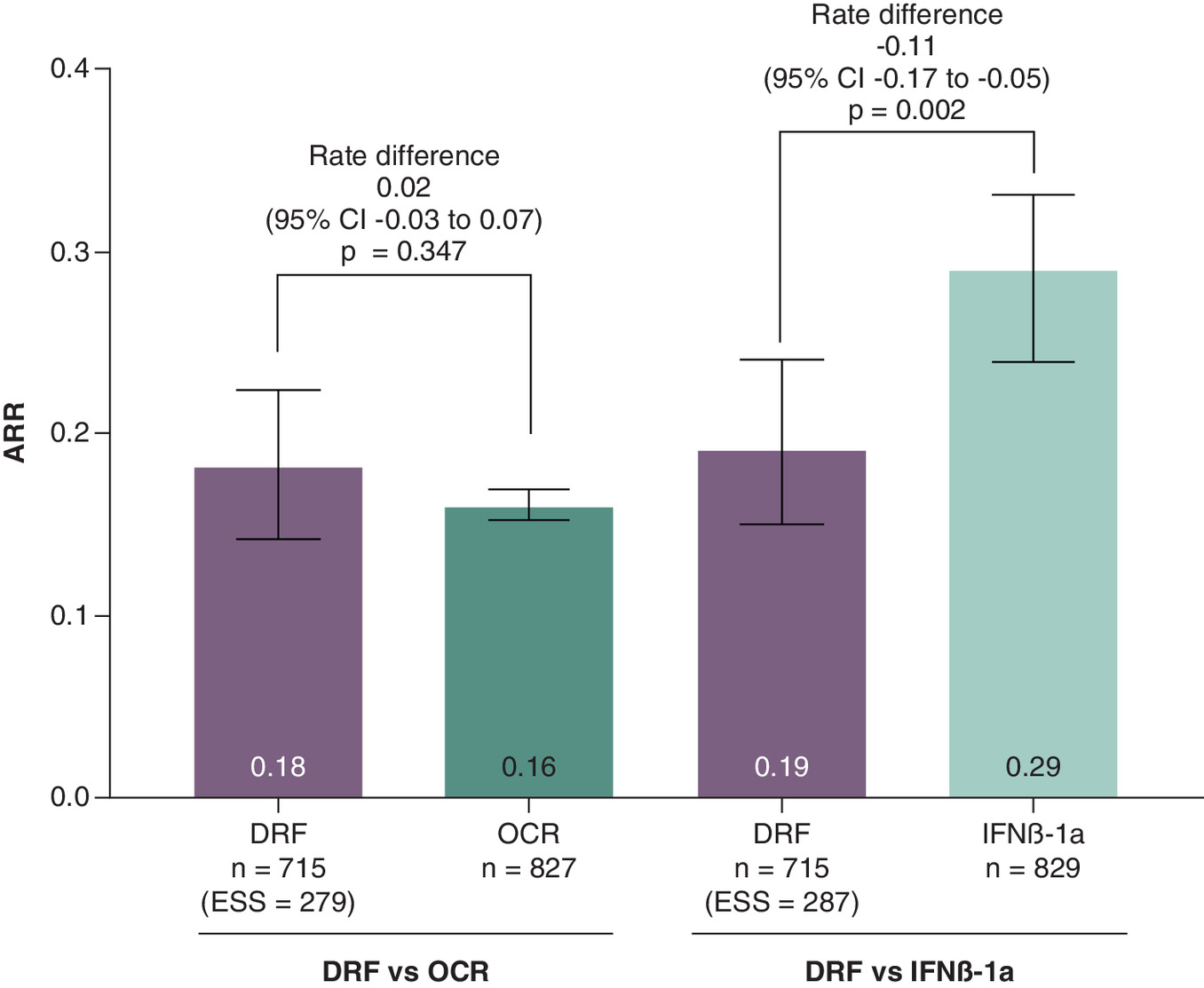
Figure 2. Annualized relapse rate for diroximel fumarate versus ocrelizumab and diroximel fumarate versus IFNβ-1a after matching-adjusted indirect comparison weighting.
aData on outcomes in OPERA I/II were obtained from Hauser SL et al. [19].
ARR: Annualized relapse rate; DRF: Diroximel fumarate; EDSS: Expanded Disability Status Scale; ESS: Effective sample size; IFNβ-1a: Interferon beta-1a; MAIC: Matching-adjusted indirect comparison; OCR: Ocrelizumab.
There were no statistically significant differences between DRF and OCR in the proportions of patients with disability progression sustained for 12 weeks (RD: -2.7%; [95% CI: -5.9–0.4]; RR: 0.7; [95% CI: 0.4–1.0]; p = 0.074) and 24 weeks (RD: -2.1%; [95% CI: -4.9–0.7]; RR: 0.7; [95% CI: 0.3–1.0]; p = 0.14) (Table 2 & Figure 3). The proportion of patients with Gd+ T1 lesions was significantly higher for DRF versus OCR (16.4% [95% CI: 12.1–20.7] vs 9.1% [95% CI: 7.1–11.0]; p < 0.0001) (Table 2 & Figure 4). After weighting, 59.5% of DRF-treated patients had N/NE T2 lesions compared with 38.7% of OCR treated patients (RD: 20.9% [95% CI: 14.9–27.0]; p < 0.0001) (Table 2 & Figure 4).
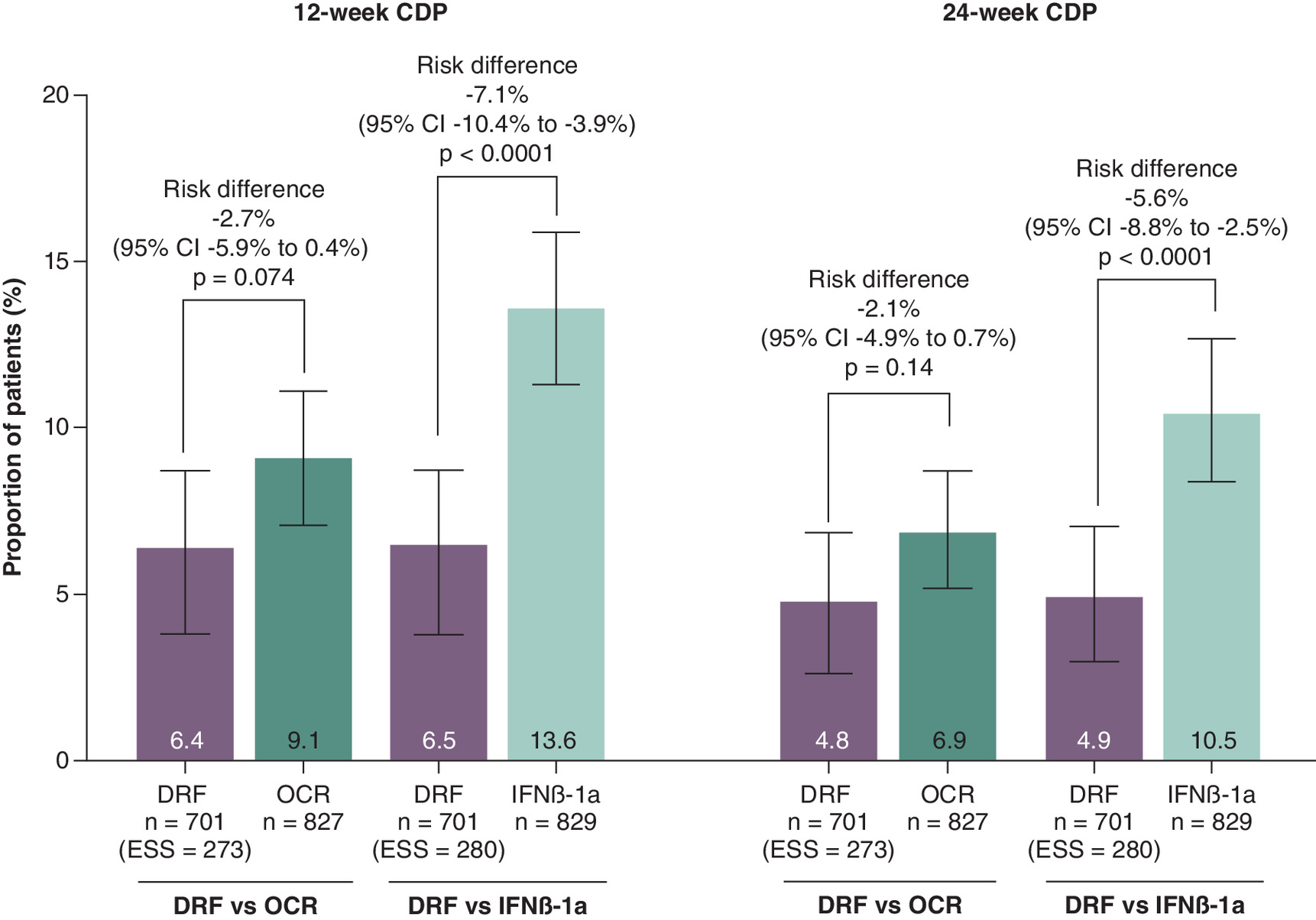
Figure 3. Twelve- and 24-week confirmed disability progressiona for diroximel fumarate versus ocrelizumab and diroximel fumarate versus IFNβ-1a after matching-adjusted indirect comparison weighting.
Data on outcomes in OPERA I/II were obtained from Hauser SL et al. taken from [19].
aOPERA’s definition of CDP was applied to EVOLVE-MS-1.
CDP: Confirmed disability progression; DRF: Diroximel fumarate; EDSS: Expanded Disability Status Scale; ESS: Effective sample size; IFNβ-1a: Interferon beta-1a; MAIC: Matching-adjusted indirect comparison; OCR: Ocrelizumab.
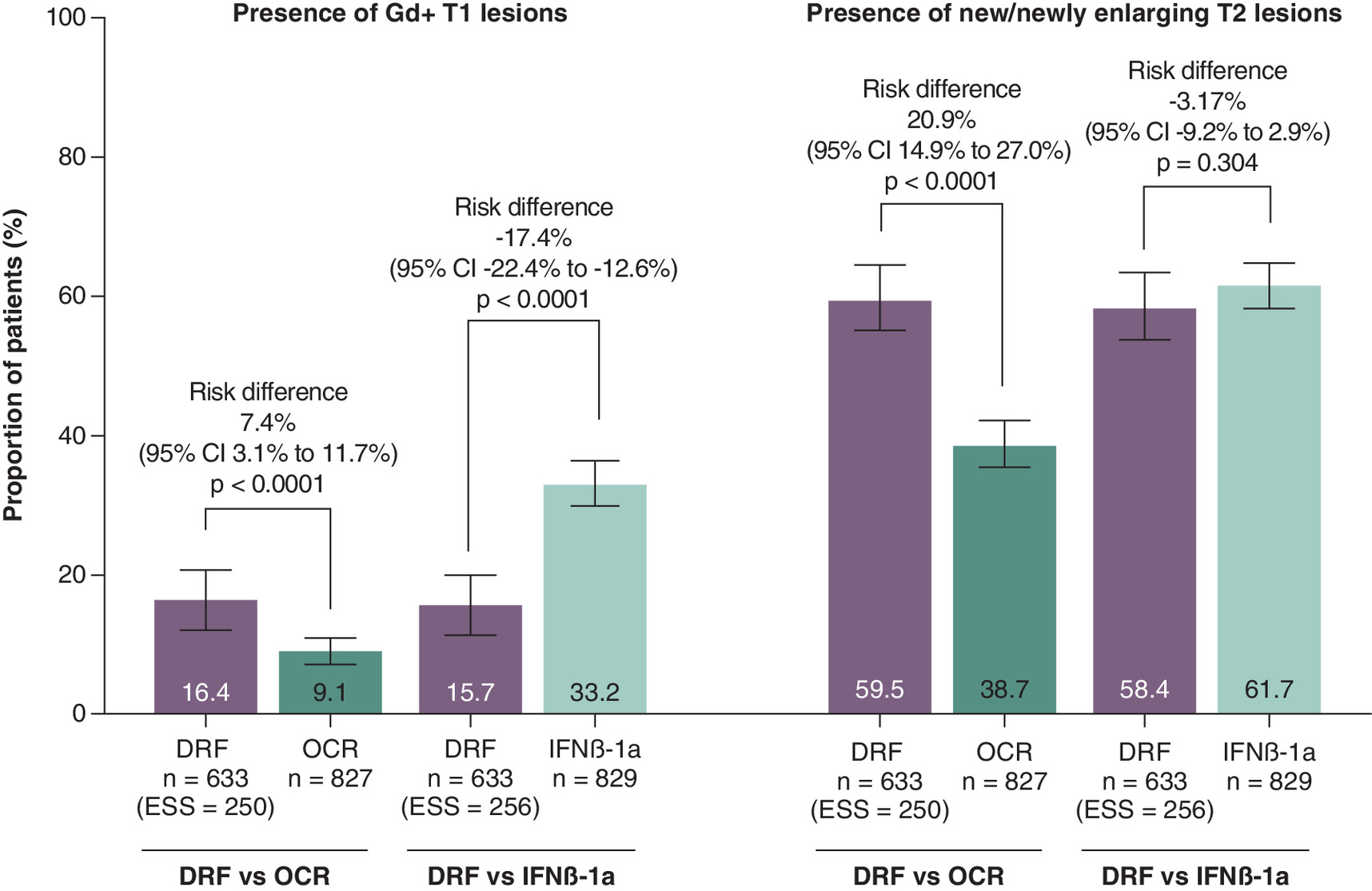
Figure 4. Presence of Gd+ T1 lesions and N/NE T2 lesions for diroximel fumarate versus ocrelizumab and diroximel fumarate versus IFNβ-1a after matching-adjusted indirect comparison weighting.
Data on absence of Gd+ T1 lesions and N/NE T2 lesions for OPERA were obtained from Hauser SL et al. taken from [19].
DRF: Diroximel fumarate; ESS: Effective sample size; Gd+: Gadolinium-enhancing; IFNβ-1a: Interferon beta-1a; MAIC: Matching-adjusted indirect comparison; N/NE: New/newly enlarging; OCR: Ocrelizumab.
DRF versus IFNβ-1a
After weighting, ARR was significantly lower in DRF-treated patients (0.18 [95% CI: 0.14–0.22]) than IFNβ-1a-treated patients (0.29 [95% CI: 0.24–0.33]), representing a 34% reduction in the ARR (weighted rate difference, -0.11; 95% CI: -0.17 to -0.05; p = 0.002) (Table 2 & Figure 2). Compared with IFNβ-1a, significantly lower proportions of DRF-treated patients had CDP sustained for 12 weeks (RD: -7.1%; 95% CI: -10.4 to -3.9; RR: 0.48; 95% CI: 0.26–0.66; p < 0.0001) and 24 weeks (RD: -5.6%; 95% CI: -8.8 to -2.5; RR: 0.47; 95% CI: 0.19–0.67; p < 0.0001) (Table 2 & Figure 3). After weighting, the proportion of patients with Gd+ T1 lesions was significantly lower for DRF (15.7% [95% CI: 11.4–19.8]) versus IFNβ-1a (33.2% [95% CI: 30.0–36.4]; p < 0.0001) (Table 2 & Figure 4). No significant difference was found in N/NE T2 lesions between DRF and IFNβ-1a (58.4% [95% CI: 53.8–63.5] vs 61.7% [95% CI: 58.3–64.9]; p = 0.304) (Table 2 & Figure 4).
Sensitivity analysis
The sensitivity analysis was conducted only in patients who were newly enrolled in EVOLVE-MS-1 and excluded those who had rolled over from receiving prior DMF or prior DRF in EVOLVE-MS-2. After restriction, 417 patients were included. Clinical and radiological outcomes before and after restriction and MAIC weighting in newly enrolled EVOLVE-MS-1 patients are presented in Table 3. All comparisons were similar to those observed in the original comparative analyses.
| OPERA I/II† | EVOLVE-MS-1 | DRF vs OCR | DRF vs IFNβ-1a | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OCR | IFNβ-1a | DRF restricted sample | EVOLVE-MS-1, DRF, weighted | Weighted incidence rate/risk difference‡ | Weighted incidence rate/risk ratio‡ | EVOLVE-MS-1, DRF, weighted | Weighted incidence rate/risk difference‡,§ | Weighted incidence rate/risk ratio‡,§ | |
| ARR¶ (95% CI) | n = 827 | n = 829 | n = 417 | ESS = 156 | ESS = 161 | ||||
| 0.16 (0.13–0.19) | 0.29 (0.25–0.33) | 0.16 (0.12–0.20) | 0.17 (0.13–0.22) | 0.02 (-0.04–0.07) | 1.10 (0.75–1.42) | 0.17 (0.13–0.22) | -0.12 (-0.18 to -0.06) | 0.60 (0.42–0.77) | |
| Proportion of patients with disability progression for 12 weeks#, % (95% CI) | n = 827 | n = 829 | n = 417 | ESS = 156 | ESS = 161 | ||||
| 9.1 (7.1–11.1) | 13.6 (11.3–15.9) | 8.3 (5.8–11.0) | 6.9 (3.0–10.3) | -2.2 (-6.1–1.5) | 0.77 (0.34–1.12) | 7.0 (3.2–10.4) | -6.6 (-10.8 to -2.8) | 0.52 (0.22–0.75) | |
| Proportion of patients with disability progression for 24 weeks#, % (95% CI) | n = 827 | n = 829 | n = 417 | ESS = 156 | ESS = 161 | ||||
| 6.9 (5.2–8.7) | 10.5 (8.4–12.7) | 6.0 (3.9–8.4) | 4.5 (1.5–7.2) | -2.4 (-5.8–0.67) | 0.66 (0.16–1.04) | 4.5 (1.6–7.0) | -6.1 (-9.8 to -2.6) | 0.43 (0.11–0.67) | |
| Patients with Gd+ T1 lesions, % (95% CI) | n = 827 | n = 829 | n = 382 | ESS = 138 | ESS = 143 | ||||
| 9.1 (7.1–11.0) | 33.2 (30.0–36.4) | 15.2 (11.6–18.8) | 15.3 (9.6–20.0) | 6.0 (0.7–11.1) | 1.69 (0.96–2.28) | 14.7 (9.3–19.0) | -18.7 (-24.5 to -13.1) | 0.44 (0.28–0.58) | |
| Patients with N/NE T2 lesions, % (95% CI) | n = 827 | n = 829 | n = 382 | ESS = 138 | ESS = 143 | ||||
| 38.7 (35.4–42.0) | 61.7 (58.3–64.9) | 58.6 (53.7–63.6) | 62.3 (54.9–68.7) | 23.5 (16.2–30.9) | 1.61 (1.38–1.82) | 61.2 (54.1–67.6) | -0.56 (-7.86–6.79) | 0.99 (0.87–1.11) | |
†
Data on outcomes in OPERA I/II were obtained from Hauser et al. taken from [19].
‡
Weighted incidence rate differences and incidence rate ratios are presented for ARR. Weighted risk differences and risk ratios are presented for the outcomes of 12- and 24-week CDP, absence of Gd+ T1 lesions, and absence of N/NE T2 lesions.
§
For DRF vs IFNβ-1a, one-sided CIs are presented for weighted incidence rate differences and incidence rate ratios.
¶
ARR was estimated using Poisson regression with robust error variance.
#
Definition for CDP used in OPERA I/II was applied to EVOLVE-MS-1.
ARR: Annualized relapse rate; CDP: Confirmed disability progression; CI: Confidence interval; DRF: Diroximel fumarate; EDSS: Expanded Disability Status Scale; ESS: Effective sample size; Gd+: Gadolinium-enhancing; IFNβ-1a: Interferon beta-1a; MAIC: Matching-adjusted indirect comparison; N/NE: New/newly enlarging; OCR: Ocrelizumab.
Discussion
Comparative efficacy studies for recently approved DMTs such as DRF are limited. This study used existing data from separate clinical trials, EVOLVE-MS-1, and the two identical phase III studies OPERA I and OPERA II, to evaluate the comparative efficacy of oral DRF to OCR and IFNβ-1a using indirect treatment comparisons. We conducted an unanchored MAIC after balancing differences in baseline characteristics between EVOLVE-MS-1 and OPERA I/II.
Our findings indicate no statistically significant differences were observed between DRF and OCR for clinical outcomes such as ARR and 12- and 24-week CDP. However, DRF was associated with a greater likelihood of Gd+ T1 lesions and N/NE T2 lesions compared with OCR. Long-term studies of DMF, which is bioequivalent to DRF, demonstrated that DMF is particularly effective in slowing disease progression with 72% of patients experiencing no 24-week CDP after 10 years and 81% among newly diagnosed patients [25]. More recently, 10-year effectiveness data for OCR reported 76.6% of patients with relapsing MS were free of 48-week CDP [26].
These comparative efficacy results demonstrated minimal observed differences in clinical outcomes between DRF and OCR. While both DMF/DRF and OCR have been effective in reducing brain MRI lesions, the presence of new T2 lesions might be a more sensitive indicator of ongoing macroinflammatory disease, though these lesions may not always correlate with clinical outcomes, especially if they are located in less eloquent topographical regions [27,28]. Additionally, due to the lack of long-term data in our study, we may not fully appreciate potential differences in clinical outcomes over extended periods resulting from MRI outcome differences. Recent trials of Bruton’s tyrosine kinase inhibitors evobrutinib and tolebrutinib also showed a discrepancy between Gd+ lesions and clinical outcomes, including ARR and CDP [29,30]. It is also possible that the difference in T1 Gd+ lesions and N/NE T2 lesions was not large enough to generate detectable differences in clinical outcomes between the two treatments. Given these complexities, treatment selection should remain an individualized decision made through shared discussion between clinicians and patients. Additionally, the lack of comparative data on other MRI metrics, such as spinal cord lesions and brain atrophy, is an acknowledged limitation.
DRF had greater efficacy than IFNβ-1a for all clinical and radiological outcomes, except for absence of N/NE T2 lesions, for which there was no strong statistical evidence favoring DRF. These results are generally consistent with data from other comparative effectiveness studies of fumarates versus IFNβ-1a and of fumarates versus anti-CD20 monoclonal antibodies, although there have been very few studies for the latter comparison. In a retrospective cohort study of patients with relapsing-remitting MS, relapse, MRI and no evidence of disease activity outcomes favored DMF over IFNβ-1a [31]. Rituximab (RTX), another anti-CD20 therapy, was superior to DMF in effectiveness and persistence, but not in disability outcomes, in patients with early relapsing MS [32,33]. It is noteworthy that the study by Vollmer et al. (2020) had methodological limitations, including its retrospective study design and lack of disability outcomes [33]. Further, the phase III study by Svenningson et al. that evaluated the efficacy of DMF versus RTX was open-label and rather small in sample size. Complementing these findings, Vollmer et al. reported that while patients younger than 45 years receiving oral DMTs experienced significantly higher odds of disease activity compared with those on infusible therapies, this difference was not apparent in patients aged 45 years or older [34]. Similarly, a meta-analysis on MS clinical trials found that high-efficacy DMTs compared with low-efficacy DMTs were only better at reducing MS disability outcomes in patients younger than 40.5 years [35]. With its better tolerability and safety profile, DRF may be associated with enhanced persistence and adherence [15,36] that could lead to better long-term outcomes. Specifically, EVOLVE-MS-1 reported a discontinuation rate due to AEs of 8.0% for DRF over 96 weeks (with gastrointestinal or flushing-related events accounting for <2%), while OPERA I/II showed lower discontinuation rates of 3.5% for OCR and 6.2% for IFNβ-1a [17,19]. In line with this, a recent study from the Komodo database also showed similar relapse outcomes between DRF and anti-CD20 treatments in a US population, adding to the comparative results between the two drug classes [37]. In previous MAICs that utilized data from EVOLVE-MS-1, DRF demonstrated similar efficacy outcomes to the sphingosine1-phosphate receptor modulators ponesimod and ozanimod and improved efficacy outcomes compared with teriflunomide and IFNβ-1a [21,22].
This study has several strengths that enhance the validity of its findings. The sample sizes from EVOLVE-MS-1 and OPERA I/II, while moderate, were sufficient to allow for effective matching and weighting, resulting in well-balanced treatment arms that reduced the potential for indication bias. Additionally, the data were sourced from rigorously designed and well-conducted studies with clearly defined end points, which adds to the robustness of the comparisons made. The careful weighting process ensured that baseline characteristics were comparable across the DRF, OCR and IFNβ-1a treatment groups, allowing for a more accurate assessment of DRF’s relative efficacy. These factors contribute to the reliability of the results and support the study’s conclusions.
These indirect comparisons of outcomes from EVOLVE-MS-1 and OPERA I and II have several limitations. First, this was an unanchored MAIC due to the lack of a common comparator between the EVOLVE-MS-1 and OPERA I/II studies. The absence of a common comparator meant that an anchored MAIC was not possible, and therefore we could not assess residual confounding after MAIC weighting. A second limitation is that after weighting the EVOLVE-MS-1 restricted population, the effective sample size was reduced that reflexively lowered the statistical power. A third potential limitation is that EVOLVE-MS-1 and OPERA I/II had different schedules of MRI assessments, and fewer MRIs in EVOLVE-MS-1 may have resulted in some Gd+ lesions not being captured. Specifically, EVOLVE-MS-1 did not include an MRI assessment at week 24, which could have resulted in missed detection of transient Gd+ lesions that appeared between scheduled scans, potentially underestimating the true number of Gd+ lesions in the DRF arm. However, this difference would not affect the N/NE T2 lesion counts, as these represent the cumulative total of all lesions over the study period. Additionally, differences observed in lesion formation may have translated into clinical differences if a longer follow-up had been available. While there was a difference in the rates of participants residing in the US versus outside the US, trial site region was included as a matching covariate in the weighted model to balance this out. In addition, a number of participants in EVOLVE-MS-1 had rolled over from the preceding EVOLVE-MS-2 study and had received prior treatment with DMF or DRF. However, a subgroup analysis limited to de novo patients showed similar outcomes, indicating that the inclusion of patients with fumarate treatment prior to EVOLVE-MS-1 had minimal overall impact on the comparative outcomes. Despite our successful efforts to balance patient populations across relevant demographic, disease, and trial factors important for treatment selection and response, unmeasured confounders may still have existed, potentially leading to hidden bias in the comparative efficacy analysis. Selection bias might have occurred because of different motivations to participate in an open-label versus double-blind study. Also because of differences in trial design, safety outcomes were not compared between EVOLVE-MS-1 and OPERA I/II.
Conclusions
This indirect comparison contributes to earlier MAICs of efficacy outcomes for DRF and other DMTs and indicates that over 2 years, DRF may have similar clinical outcomes compared with OCR and better efficacy outcomes than IFN. However, radiological outcomes favor OCR over DRF, suggesting better acute inflammatory control with anti-CD20 therapy. Such data may be valuable for informing decision-making around treatments for MS. However, it is important to note that our data serve only as a group-level estimate and had several limitations. Individualized treatment decisions must be made on a case-by-case basis taking into account clinical and radiographic MS activity, side effect and tolerability profiles, patient preferences, baseline comorbidities, access to DMT, family planning wishes and other relevant factors. DMT efficacy, tolerability and safety should be considered in these personalized treatment decisions.
Summary points
•
Diroximel fumarate (DRF), ocrelizumab (OCR) and interferon beta-1a (IFNβ-1a) are widely used disease-modifying therapies (DMTs) for relapsing multiple sclerosis (MS), yet they have not been directly compared in randomized clinical trials.
•
This study applied a matching-adjusted indirect comparison (MAIC) approach to individual patient data from the EVOLVE-MS-1 trial (DRF) and published data from the OPERA I/II trials (OCR vs IFNβ-1a).
•
After restricting and weighting the DRF population to match baseline characteristics in the OCR and IFNβ-1a cohorts, the populations were well-balanced.
•
Relapse rates, disability progression and MRI findings were compared between DRF versus OCR and DRF versus IFNβ-1a.
•
DRF showed no significant difference in relapse rates or confirmed disability progression compared with OCR, but OCR had more favorable MRI outcomes including fewer gadolinium-enhancing (Gd+) and new/newly enlarging T2 lesions.
•
Compared with IFNβ-1a, DRF was associated with fewer relapses, lower rates of disability progression and fewer Gd+ lesions, although differences in new/newly enlarging T2 lesions were not statistically significant.
•
The unanchored MAIC design is useful but has inherent limitations, such as differing MRI schedules across trials and reduced sample sizes after weighting.
•
These findings may inform clinical decision-making by highlighting the efficacy across different DMTs and their modes of action. However, individual treatment decisions should be made depending on various factors.
•
More head-to-head studies are needed to show the comparative efficacy of different DMTs.
Author contributions
CM Hersh and Y Aladro-Benito participated in the collection of data. CM Hersh, JB Lewin, C Shen, I Božin and Z Sun participated in the study design and statistical analysis plan. CM Hersh, Y Aladro-Benito, JB Lewin, C Shen, I Božin and Z Sun participated in the analysis and interpretation of data. C Shen and Z Sun performed the statistical analysis. CM Hersh, Y Aladro-Benito, JB Lewin, C Shen, I Božin and Z Sun participated in drafting and critically revising the manuscript.
Financial disclosure
Funding was provided by Biogen.
Competing interests disclosure
EVOLVE-MS-1 and the current analysis were sponsored by Biogen (Cambridge, MA, USA). CM Hersh: speaking, consulting and advisory board fees from Genentech, Genzyme, Biogen, Novartis, EMD-Serono, Bristol Myers Squibb, TG Therapeutics, Horizon Therapeutics, and Alexion. She has received research support paid to her institution by Biogen, Novartis, Bristol Myers Squibb, Patient-Centered Outcomes Research Institute and NIH-NINDS 1U01NS111678-01A1 sub-award. Y Aladro-Benito: research grants, travel support and speaking and consulting fees from Bayer, Biogen, Roche, Merck, Novartis, Almirall, Sanofi-Genzyme, Janssen and Bristol Myers Squibb. JB Lewin, I Božin and Z Sun: employees of Biogen and may hold stock in the company. C Shen: was an employee of Biogen at the time of study and may hold stock in the company. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support for the preparation of this manuscript was provided by Samantha Pluta, PharmD, on behalf of Excel Medical Affairs (CT, USA), Kat Ayling-Rouse, PhD, on behalf of Excel Scientific Solutions (Horsham, UK) and David Pertab, PhD, Excel Scientific Solutions (Glasgow, UK), under the direction of the authors. Cara Farrell, on behalf of Excel Medical Affairs (CT, USA), copyedited and styled the manuscript per journal requirements.
Ethical conduct of research
Data sharing statement
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 58.42 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Multiple Sclerosis International Federation. Atlas of MS (3rd edition). Available from: https://www.msif.org/wp-content/uploads/2020/10/Atlas-3rd-Edition-Epidemiology-report-EN-updated-30-9-20.pdf
2.
Battaglia MA, Bezzini D, Cecchini I et al. Patients with multiple sclerosis: a burden and cost of illness study. J. Neurol. 269(9), 5127–5135 (2022).
3.
Benini S, Pellegrini E, Descovich C, Lugaresi A. Burden and resources in caregivers of people with multiple sclerosis: a qualitative study. PLoS ONE 18(4), e0265297 (2023).
4.
Hersh CM, Brook RA, Beren IA et al. The implications of suboptimal year-1 outcomes with disease-modifying therapy in employees with multiple sclerosis. J. Med. Econ. 24(1), 479–486 (2021).
5.
Biogen. VUMERITY® (diroximel fumarate) delayed-release capsules, for oral use (2024). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/211855s015lbl.pdf (Accessed: 30 May 2024).
6.
Genentech. OCREVUS® (ocrelizumab) injection, for intravenous use (2024). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/761053s034lbl.pdf (Accessed: 30 May 2024).
7.
EMD Serono. REBIF (interferon beta-1a), for subcutaneous injection (2023). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/103780s5214lbl.pdf (Accessed: 30 May 2024).
8.
European Medicines Agency. Rebif summary of product characteristics (2023). Available from: https://www.ema.europa.eu/en/documents/product-information/rebif-epar-product-information_en.pdf (Accessed: 30 May 2024).
9.
European Medicines Agency. Ocrevus summary of product characteristics (2025). Available from: https://www.ema.europa.eu/en/documents/product-information/ocrevus-epar-product-information_en.pdf (Accessed: 6 July 2025).
10.
European Medicines Agency. Vumerity summary of product characteristics (2024). Available from: https://www.ema.europa.eu/en/documents/product-information/vumerity-epar-product-information_en.pdf (Accessed: 30 May 2024).
11.
Amin M, Hersh CM. Updates and advances in multiple sclerosis neurotherapeutics. Neurodegener. Dis. Manag. 13(1), 47–70 (2023).
12.
Jonker MF, Donkers B, Goossens LMA et al. Summarizing patient preferences for the competitive landscape of multiple sclerosis treatment options. Med. Decis. Making 40(2), 198–211 (2020).
13.
Molazadeh N, Sahraian MA, Ghajarzadeh M. Disease-modifying therapy in multiple sclerosis: evaluation of patients satisfaction in Iranian multiple sclerosis population. Caspian J. Intern. Med. 14(1), 89–93 (2023).
14.
Utz KS, Hoog J, Wentrup A et al. Patient preferences for disease-modifying drugs in multiple sclerosis therapy: a choice-based conjoint analysis. Ther. Adv. Neurol. Disord. 7(6), 263–275 (2014).
15.
Naismith RT, Wundes A, Ziemssen T et al. Diroximel fumarate demonstrates an improved gastrointestinal tolerability profile compared with dimethyl fumarate in patients with relapsing-remitting multiple sclerosis: results from the randomized, double-blind, phase III EVOLVE-MS-2 study. CNS Drugs 34(2), 185–196 (2020).
• This head-to-head phase III trial shows that diroximel fumarate (DRF) significantly reduces gastrointestinal symptom days and adverse events compared with dimethyl fumarate in relapsing-remitting multiple sclerosis (MS) patients, potentially enhancing treatment adherence through improved tolerability.
16.
Wundes A, Wray S, Gold R et al. Improved gastrointestinal profile with diroximel fumarate is associated with a positive impact on quality of life compared with dimethyl fumarate: results from the randomized, double-blind, phase III EVOLVE-MS-2 study. Ther. Adv. Neurol. Disord. 14, 1–14 (2021).
17.
Singer BA, Arnold DL, Drulovic J et al. Diroximel fumarate in patients with relapsing-remitting multiple sclerosis: final safety and efficacy results from the phase 3 EVOLVE-MS-1 study. Mult. Scler. 29(14), 1795–1807 (2023).
•• This phase III study provides final 2-year data showing that DRF is well tolerated with low gastrointestinal discontinuation rates and demonstrates robust efficacy in reducing relapse rates and MRI lesions in patients with relapsing-remitting multiple sclerosis, reinforcing its therapeutic potential.
18.
Wray S, Then Bergh F, Wundes A et al. Efficacy and safety outcomes with diroximel fumarate after switching from prior therapies or continuing on DRF: results from the phase 3 EVOLVE-MS-1 study. Adv. Ther. 39(4), 1810–1831 (2022).
19.
Hauser SL, Bar-Or A, Comi G et al. Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N. Engl. J. Med. 376(3), 221–234 (2017).
•• This pivotal phase III trial shows that ocrelizumab significantly reduces relapse rates, disability progression and MRI lesion counts compared with interferon beta-1a, underscoring its superior efficacy in relapsing MS.
20.
Kieseier BC. The mechanism of action of interferon-beta in relapsing multiple sclerosis. CNS Drugs 25(6), 491–502 (2011).
21.
Jiang T, Ziemssen T, Wray S et al. Matching-adjusted indirect comparisons of diroximel fumarate, ponesimod, and teriflunomide for relapsing multiple sclerosis. CNS Drugs 37(5), 441–452 (2023).
• This study uses matching-adjusted indirect comparisons to show that DRF offers comparable relapse and disability outcomes to ponesimod, with a higher proportion of patients free of Gd+ lesions, and superior efficacy to teriflunomide across most endpoints in relapsing MS.
22.
Jiang T, Bozin I, Lewin JB, Shen C, Soderbarg K, Arnold DL. Matching-adjusted indirect comparisons of diroximel fumarate, ozanimod, and interferon beta-1a for relapsing MS. Presented at: European Academy of Neurology (EAN), Budapest, Hungary (2023).
•• This matching-adjusted indirect comparison indicates that DRF achieves comparable relapse rates to ozanimod while providing superior disability and MRI outcomes compared with both ozanimod and interferon beta-1a, underscoring its favorable efficacy profile in relapsing MS despite inherent indirect comparison limitations.
23.
Jiang T, Shanmugasundaram M, Bozin I et al. Comparative efficacy of diroximel fumarate, ozanimod and interferon beta-1a for relapsing multiple sclerosis using matching-adjusted indirect comparisons. J. Comp. Eff. Res. 13(10), e230161 (2024).
24.
Naismith RT, Wolinsky JS, Wundes A et al. Diroximel fumarate (DRF) in patients with relapsing-remitting multiple sclerosis: interim safety and efficacy results from the phase III EVOLVE-MS-1 study. Mult. Scler. 26(13), 1729–1739 (2020).
25.
Gold R, Arnold DL, Bar-Or A et al. Long-term safety and efficacy of dimethyl fumarate for up to 13 years in patients with relapsing-remitting multiple sclerosis: final ENDORSE study results. Mult. Scler. 28(5), 801–816 (2022).
26.
Hauser S, Kappos L, Filippi M et al. 10 years of ocrelizumab treatment in multiple sclerosis: long-term efficacy and safety clinical trial data (S31.005). Neurology 102(1 Suppl. 17), 5124 (2024).
27.
Chard D, Trip SA. Resolving the clinico-radiological paradox in multiple sclerosis. F1000 Res. 6, 1828 (2017).
28.
Hartmann A, Noro F, Bahia PRV et al. The clinical-radiological paradox in multiple sclerosis: myth or truth? Arq. Neuropsiquiatr. 81(1), 55–61 (2023).
29.
Montalban X, Vermersch P, Arnold DL et al. Safety and efficacy of evobrutinib in relapsing multiple sclerosis (evolutionRMS1 and evolutionRMS2): two multicentre, randomised, double-blind, active-controlled, phase III trials. Lancet Neurol. 23(11), 1119–1132 (2024).
30.
Oh J, Arnold DL, Cree BAC et al. Efficacy and safety of tolebrutinib versus teriflunomide in relapsing multiple sclerosis: results from the phase 3 GEMINI 1 and 2 trials. Presented at: European Committee for Treatment & Research in Multiple Sclerosis (ECTRIMS), Copenhagen, Denmark (2024).
31.
Sattarnezhad N, Healy BC, Baharnoori M et al. Comparison of dimethyl fumarate and interferon outcomes in an MS cohort. BMC Neurol. 22(1), 252 (2022).
32.
Svenningsson A, Frisell T, Burman J et al. Safety and efficacy of rituximab versus dimethyl fumarate in patients with relapsing-remitting multiple sclerosis or clinically isolated syndrome in Sweden: a rater-blinded, phase III, randomised controlled trial. Lancet Neurol. 21(8), 693–703 (2022).
33.
Vollmer BL, Nair K, Sillau S, Corboy JR, Vollmer T, Alvarez E. Rituximab versus natalizumab, fingolimod, and dimethyl fumarate in multiple sclerosis treatment. Ann. Clin. Transl. Neurol. 7(9), 1466–1476 (2020).
34.
Vollmer BL, Wolf AB, Sillau S, Corboy JR, Alvarez E. Evolution of disease modifying therapy benefits and risks: an argument for de-escalation as a treatment paradigm for patients with multiple sclerosis. Front. Neurol. 12, 799138 (2021).
35.
Weideman AM, Tapia-Maltos MA, Johnson K, Greenwood M, Bielekova B. Meta-analysis of the age-dependent efficacy of multiple sclerosis treatments. Front. Neurol. 8, 577 (2017).
• This meta-analysis found that high-efficacy disease-modifying therapies (DMTs) compared with low-efficacy DMTs only showed a better reduction in MS disability for patients under the age of 40.5 years.
36.
Lager B, Liseno J, Bozin I et al. Real-world analysis affirms the high persistence and adherence observed with diroximel fumarate in patients with multiple sclerosis. Neurol. Ther. 12(1), 145–159 (2023).
37.
Obeidat AZ, Betz M, Straus Farber RS et al. Comparative effectiveness and risk of serious infection in adult patients treated with diroximel fumarate versus anti-CD20 monoclonal antibodies: a real-world claims analysis. Presented at: European Committee for Treatment & Research in Multiple Sclerosis (ECTRIMS), Copenhagen, Denmark (2024).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 1 May 2025
Accepted: 8 August 2025
Published online: 12 September 2025
Keywords:
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Matching-adjusted indirect comparisons of diroximel fumarate, ocrelizumab and interferon beta-1a for relapsing multiple sclerosis. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0061
Export citation
Select the citation format you wish to export for this article or chapter.