A comparison of healthcare resource utilization and costs between patients with chronic lymphocytic leukemia treated with first-line ibrutinib or acalabrutinib using two large US real-world databases
Publication: Journal of Comparative Effectiveness Research
Abstract
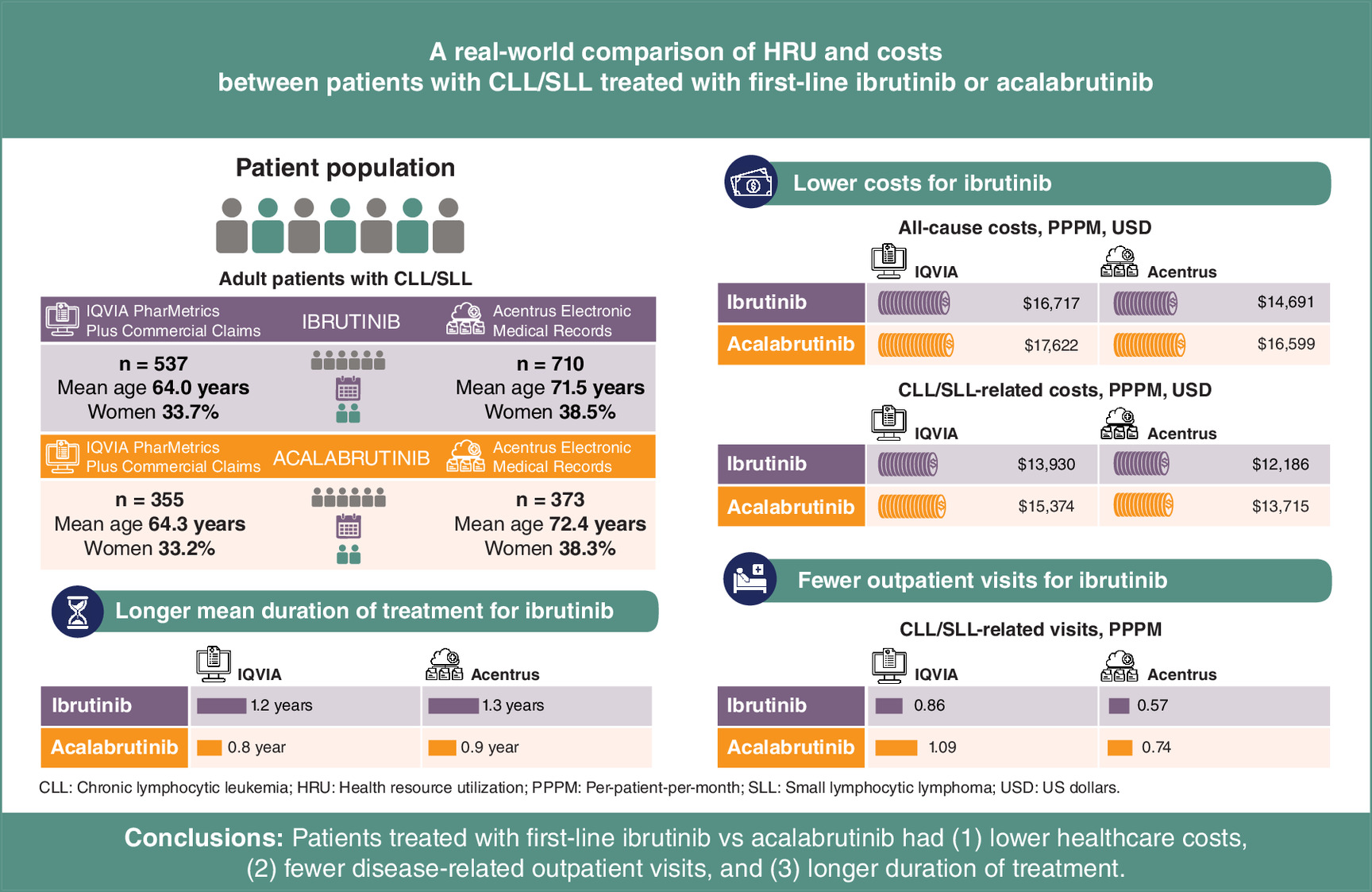
Aim: Real-world evidence comparing healthcare resource utilization (HRU) and costs between ibrutinib and acalabrutinib, two Bruton’s tyrosine kinase inhibitors for the treatment of chronic lymphocytic leukemia and small lymphocytic lymphoma (CLL/SLL) is limited. Materials & methods: Commercial claims from IQVIA PharMetrics Plus and electronic medical records from Acentrus were used to separately evaluate HRU and costs in CLL/SLL patients initiating first-line (1L) single-agent ibrutinib or acalabrutinib on or after 21 November 2019 (index date). Imputed costs were used for Acentrus using previously published assumptions. Regression analyses adjusted for baseline characteristics were used to compare HRU and costs between ibrutinib and acalabrutinib during 1L therapy. Results: In IQVIA, 537 and 355 patients initiated 1L ibrutinib and acalabrutinib, respectively; in Acentrus, 710 and 373 patients initiated 1L ibrutinib and acalabrutinib, respectively. The mean duration of 1L (in years) was longer for ibrutinib (IQVIA: 1.2; Acentrus: 1.3) than acalabrutinib (IQVIA: 0.8; Acentrus: 0.9). The number of CLL/SLL-related outpatient visits were significantly lower for ibrutinib versus acalabrutinib (IQVIA: 0.86 vs 1.09 per-patient-per-month, rate ratio: 0.85, p = 0.018; Acentrus: 0.57 vs 0.74 per-patient-per-month, rate ratio: 0.80, p = 0.036). Using claims data for IQVIA and imputed costs for Acentrus, total all-cause costs (IQVIA: mean monthly cost difference [MMCD]: -$764, p = 0.279; Acentrus: MMCD: -$1355, p = 0.004) and CLL/SLL related costs (IQVIA: MMCD: -$649, p = 0.133; Acentrus: MMCD: -$1215, p = 0.004) were lower for ibrutinib versus acalabrutinib. Conclusion: In this large real-world study using a mix of claims data and imputed cost estimates, CLL/SLL patients treated with ibrutinib had longer duration of 1L, fewer days with CLL/SLL-related outpatient services and numerically lower all-cause and CLL/SLL-related costs versus acalabrutinib, showing that ibrutinib can be an optimal cost-effective option in 1L.
Plain language summary
What is this article about?
Ibrutinib and acalabrutinib are recommended for first-line (1L) treatment for chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL). This study compared the number of hospital admissions and outpatient visits, as well as healthcare costs between patients with CLL/SLL treated with either ibrutinib or acalabrutinib using two large databases representative of the US population.
What were the results?
Findings were similar for the two databases. Patients treated with ibrutinib had longer duration of 1L, fewer disease-related outpatient visits and consistently similar or lower healthcare costs compared with patients treated with acalabrutinib.
What do the results mean?
The use of two large databases allows for improved generalizability of study findings, and suggests that ibrutinib is a cost-effective option for 1L CLL/SLL therapy compared with acalabrutinib.
Tweetable abstract
A study found that patients with CLL/SLL treated with ibrutinib had fewer disease-related outpatient visits and similar or lower healthcare costs compared with patients treated with acalabrutinib. Results suggest ibrutinib can be a more cost-effective option for first-line CLL/SLL therapy.
Graphical abstract
Background
Chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL) is a type of hematologic cancer characterized by the clonal expansion of mature B lymphocytes [1]. It is the most common form of leukemia in adults in the US, with a 5-year survival rate of 88.5% [1]. The American Cancer Society estimates that there will be approximately 23,690 new cases of CLL and 4460 deaths from CLL in the US in 2025 [2].
With the advent of oral targeted therapies, Bruton tyrosine kinase inhibitors (BTKis) such as ibrutinib (once-daily) and acalabrutinib (twice-daily) have become standard-of-care first-line (1L) treatments for CLL/SLL [3]. Since the approval of ibrutinib in February 2014 for relapsed/refractory CLL, followed by its approval in 1L in March 2016 [3], insurance claims data on file from the IQVIA database have reported that over 250,000 patients with CLL/SLL have been treated with ibrutinib in the US. In addition, several phase III clinical trials and real-world studies with long-term follow-up have demonstrated improved progression-free survival and overall survival in CLL/SLL patients initiating 1L ibrutinib versus comparator cohorts [4–12]. In November 2019, acalabrutinib was also approved for the treatment of CLL/SLL, either as a monotherapy or in combination with obinutuzumab [13]. While there is currently no clinical trial comparing ibrutinib and acalabrutinib in the 1L setting, real-world evidence comparing these two treatments in 1L is emerging, including some real-world studies reporting higher adherence and longer time to next treatment (TTNT; overall and among a subgroup with high-risk characteristics) for ibrutinib relative to acalabrutinib [14–17]. Dose adjustment with ibrutinib, which allows patients to maintain ibrutinib efficacy while preventing recurrence or worsening of adverse events [18–22], was also associated with numerically longer duration of treatment and TTNT compared with acalabrutinib [23].
In addition to clinical outcomes, ibrutinib has been shown to result in net healthcare cost savings relative to other therapy classes such as anti-CD20 based chemoimmunotherapy (CIT) regimens [24,25]. However, except for an early analysis with short follow-up [26], there are limited real-world studies comparing healthcare resource utilization (HRU) and costs between different BTKis in 1L. As emerging real-world data suggests improved clinical outcomes for patients initiated on ibrutinib versus acalabrutinib [14–17], there is a need to evaluate the corresponding HRU and costs for these treatments in the real-world setting and over longer follow-up time. Therefore, the current study was conducted to compare HRU and costs between patients with CLL/SLL treated with 1L single-agent ibrutinib and acalabrutinib using two large real-world databases covering a diversified population.
Materials & methods
Data sources
Claims data from IQVIA PharMetrics Plus (IQVIA) from 21 November 2018 to most recent at the time the study was conducted (30 September 2022) and electronic medical records (EMR) from Acentrus from 21 November 2018 to most recent at the time the study was conducted (30 April 2022) for patients initiating ibrutinib or acalabrutinib in 1L on or after 21 November 2019 were used to maximize generalizability and robustness of results. Claims data from 21 November 2018 were accessed for both databases to ensure at least 1 year of data prior to initiation of treatment.
The IQVIA database is an adjudicated health plan claims database. It is made up of fully adjudicated health plan claims data and enrollment information for more than 215 million unique individuals with commercial health insurance. IQVIA comprises information from over 70 contributing health plans and self-insured employer groups throughout the US with more than 140 million unique enrollees. The database includes medical and pharmacy claims data, patient-level enrollment records and patient demographics and is representative of the commercially insured US population.
Acentrus is a health system solution used by 128,000 prescribers, containing inpatient and outpatient data from 27 sites. This includes six National Comprehensive Cancer Network members and ten National Cancer Institute designated sites, all contributing data from both medication orders and refills. Acentrus includes patient records from 15 academic and 12 nonteaching hospital systems across 15 US states.
Data from both the IQVIA and Acentrus databases are de-identified and comply with the patient requirements of the Health Insurance Portability and Accountability Act (HIPAA).
Study design
A retrospective cohort study design was used. Analyses were conducted separately for IQVIA and Acentrus. In both databases, adult patients initiating 1L single-agent ibrutinib or acalabrutinib on or after 21 November 2019 (acalabrutinib approval) were analyzed, with the index date defined as the date of initiation of ibrutinib or acalabrutinib. A window of 28 days post-index was used to ascertain that no other antineoplastic agents were used in combination with ibrutinib or acalabrutinib (Figure 1). In IQVIA analyses, a washout period of at least 6 months of continuous eligibility prior to the index date was used to confirm 1L therapy and assess baseline characteristics (6 months was required instead of 12 months, to account for plan member turnover associated with commercial plans, with or without changing the medical providers), while in Acentrus, a washout period of at least 12 months of data availability (insurance eligibility not available in Acentrus) prior to the index date was used. The follow-up period was defined as the period from the index date to the earliest of initiation of second-line (2L) therapy, death (only available in Acentrus), end of continuous enrollment (only available in IQVIA), or end of data availability. As add-on of certain anticancer therapies may indicate late initiation of agents as part of a combination regimen in 1L rather than disease progression, patients were censored on the date of add-on if they had an anti-CD20 antibody (i.e., obinutuzumab or rituximab) or venetoclax add-on to the index BTKi within 180 days post-index, as done in a previous study [17] based on prescribing guidelines recommending initiation of the second agent within 6 months of therapy initiation [13,27–30]. Furthermore, patients switching to another BTKi were censored at the date of switch, as this may indicate a switch due to tolerability rather than disease progression [31–34]. These censoring rules were implemented to make sure HRU and costs are evaluated during 1L single-agent therapy use and prior to a potential indicator of disease progression.

Figure 1. Study design for IQVIA and Acentrus analyses.
1A 6-month baseline period was used in IQVIA. A 12-month baseline period was used in Acentrus.
2Patients were censored on the date of switch or add-on if they had one of the following: a within-class BTKi switch (i.e., the next treatment is also a BTKi) or an anti-CD20 antibody (i.e., obinutuzumab or rituximab) or venetoclax add-on to the index BTKi within 180 days post-index.
3End of continuous enrollment was used as an indicator of end of follow-up in IQVIA analyses only.
4End of data availability in IQVIA was 30 September 2022. End of data availability in Acentrus was 30 April 2022.
1L: First-line; BTKi: Bruton’s tyrosine kinase inhibitor.
Study population
In both IQVIA and Acentrus analyses, patients were required to meet the following criteria: at least 18 years of age, initiation of ibrutinib or acalabrutinib in 1L on or after 21 November 2019 (index date), at least 6 months of continuous enrollment (IQVIA) or at least 12 months of data availability (Acentrus) prior to the index date, and at least one diagnosis for CLL/SLL prior to the index date (International Classification of Disease, 9th Revision, Clinical Modification [ICD-9 CM]: 204.1; International Classification of Disease, 10th Revision, Clinical Modification [ICD-10-CM]: C91.1, C83.0). Patients with other malignancies or end-stage renal disease prior to the index date were excluded. Additional details regarding inclusion and exclusion criteria are presented in Figure 2.
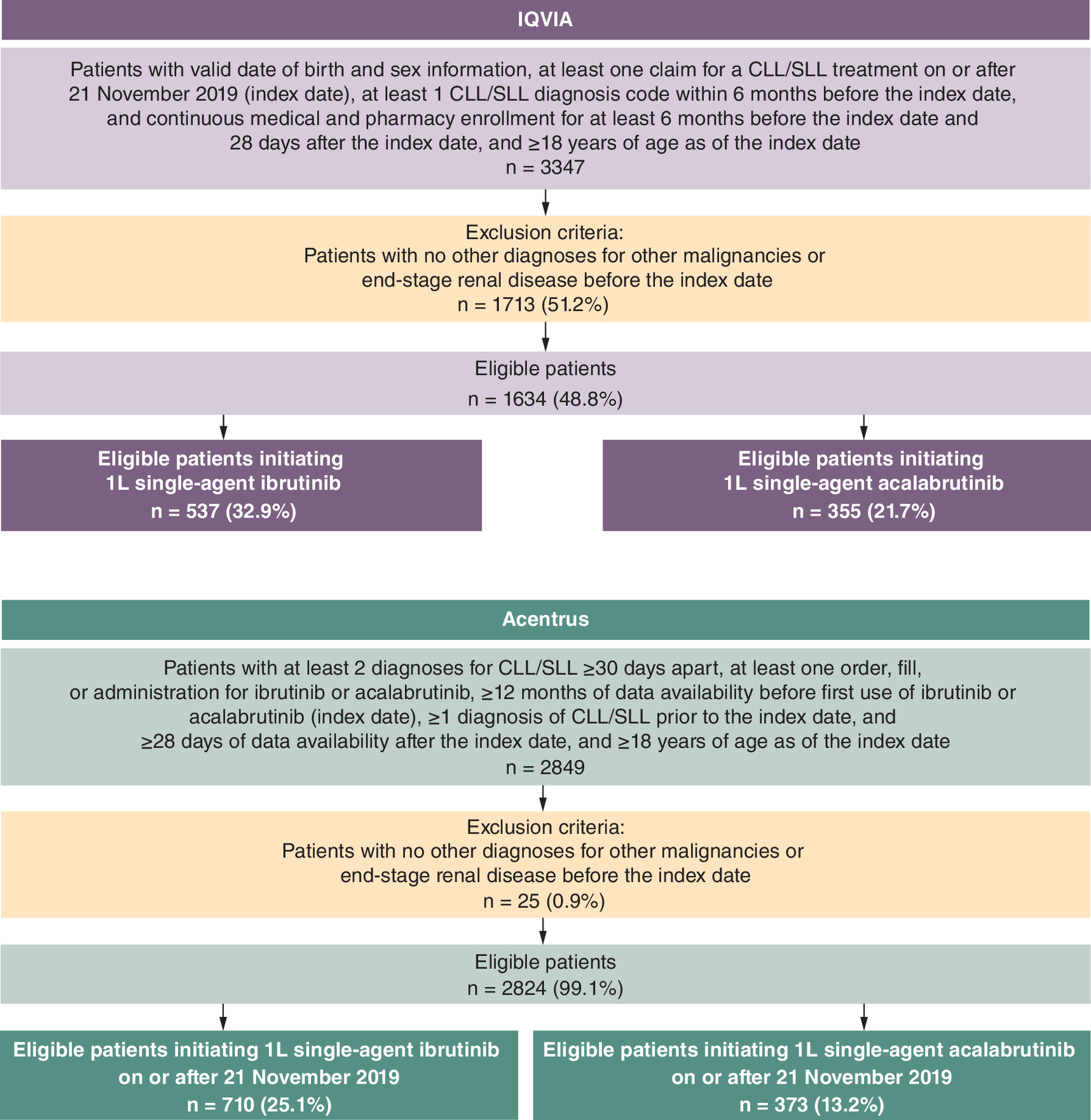
Figure 2. Study population selection.
1L: First line; CLL: Chronic lymphocytic leukemia; SLL: Small lymphocytic lymphoma.
Study measures
Patient demographics and clinical characteristics (i.e., Quan-Charlson Comorbidity Index [Quan-CCI], comorbidities, cardiovascular risk and medication use) were evaluated during the baseline period (i.e., 6 months pre-index for IQVIA and 12 months pre-index for Acentrus).
HRU and cost outcomes were evaluated during the follow-up period (i.e., during 1L therapy). All-cause and CLL/SLL-related HRU outcomes included inpatient admissions and outpatient visits (including emergency department visits). All-cause and CLL/SLL-related healthcare costs included pharmacy (broken down into BTKi costs and other pharmacy costs for IQVIA) and medical costs, with medical costs further broken down into inpatient and outpatient costs. CLL/SLL-related HRU and medical costs were defined as services with a diagnosis code for CLL/SLL. CLL/SLL-related pharmacy costs were defined as costs related to BTKi treatment.
In IQVIA, costs were based on paid claims while in Acentrus, costs were not available and were thus imputed based on available literature, to estimate costs from a mixed commercial and Medicare population. More specifically, guided by prior literature using cost imputation methods [35–38], costs were calculated based on HRU results observed in Acentrus and relevant available literature on healthcare costs for CLL/SLL patients treated with BTKis. In particular, published data from Fradley et al. [26] evaluating costs for 1L ibrutinib and acalabrutinib were used. As Fradley et al. did not present costs for each medical service separately, data from Huang et al. [24] was used to estimate the proportion of costs attributable to each category under medical costs, which were then summed to report total medical costs. All-cause and CLL/SLL-related pharmacy costs were also imputed based on Fradley et al. [26], using per-patient-per-month [PPPM] pharmacy costs and medication adherence information. Details of the calculations and assumptions are presented in Supplementary Table 1 for medical costs and Supplementary Table 2 for pharmacy costs.
In both IQVIA and Acentrus analyses, HRU and costs were reported PPPM, to account for varying durations of follow-up between patients. All cost estimates were inflated to 2022 US dollars using the medical care component of the Consumer Price Index.
Statistical analyses
All analyses were performed using SAS (SAS Institute, NC, USA). Baseline characteristics were described using means, standard deviations, and medians for continuous variables and frequencies and proportions for categorical variables. Standardized differences (std diff.) were calculated in both analyses to compare baseline characteristics (characteristics with differences <10% were considered similar [39]). To account for differences in baseline characteristics between cohorts, baseline demographics, comorbidities, CLL/SLL-related symptoms, medications, HRU and costs were adjusted for. Additional details regarding the characteristics adjusted for in each analysis are provided in Supplementary Table 3. All-cause and CLL/SLL-related HRU were compared between the two cohorts using Poisson regression models, with results reported as rate ratios (RRs). Healthcare costs were compared between the two cohorts using ordinary least squares regression models, with results reported as adjusted mean monthly cost differences (MMCDs).
Results
Study population & baseline characteristics
In IQVIA, a total of 537 and 355 patients with CLL/SLL initiating 1L single-agent ibrutinib or acalabrutinib were included, respectively (Figure 2). Mean observed duration of 1L treatment was 1.2 years and 0.8 years for ibrutinib and acalabrutinib. Mean age (ibrutinib vs acalabrutinib: 64.0 vs 64.3 years, std diff.: 3.1%), proportion of women (33.7 vs 33.2%, std diff.: 1.0%), mean Quan-CCI score (2.7 vs 2.7, std diff.: 3.0%), and mean CHA2DS2-VASc risk score (as an indicator of cardiovascular risk; 1.7 vs 1.7, std diff.: 3.4%) were similar between cohorts (Table 1).
| IQVIA | Acentrus | |||||
|---|---|---|---|---|---|---|
| Ibrutinib (n = 537) | Acalabrutinib (n = 355) | Standardized difference, % | Ibrutinib (n = 710) | Acalabrutinib (n = 373) | Standardized difference, % | |
| Demographics‡ | ||||||
| Age at index date, years, mean (SD) | 64.0 (10.4) | 64.3 (10.2) | 3.1 | 71.5 (10.4) | 72.4 (9.8) | 9.1 |
| Women, n (%) | 181 (33.7) | 118 (33.2) | 1.0 | 273 (38.5) | 143 (38.3) | 0.2 |
| Year of index date, n (%) | ||||||
| 2019 | – | – | – | 45 (6.3) | 7 (1.9) | 22.6† |
| 2020 | 287 (53.4) | 73 (20.6) | 72.4† | 408 (57.5) | 119 (31.9) | 53.2† |
| 2021 | 178 (33.1) | 141 (39.7) | 13.7† | 217 (30.6) | 200 (53.6) | 48.0† |
| 2022 | 72 (13.4) | 141 (39.7) | 62.4† | 40 (5.6) | 47 (12.6) | 24.4† |
| Payer type§, n (%) | ||||||
| Medicare¶ | 138 (25.7) | 85 (23.9) | 4.1 | 196 (27.6) | 104 (27.9) | 0.6 |
| Managed care | – | – | – | 61 (8.6) | 34 (9.1) | 1.8 |
| Medicaid | – | – | – | 15 (2.1) | 0 (0.0) | 20.8† |
| Commercial | 280 (52.1) | 192 (54.1) | 3.9 | – | – | – |
| Self-insured | 119 (22.2) | 78 (22.0) | 0.5 | – | – | – |
| Other | – | – | – | 252 (35.5) | 137 (36.7) | 2.6 |
| Unknown | – | – | – | 186 (26.2) | 98 (26.3) | 0.2 |
| US region, n (%) | ||||||
| South | 210 (39.1) | 144 (40.6) | 3.0 | 213 (30.0) | 138 (37.0) | 14.9† |
| West | 86 (16.0) | 61 (17.2) | 3.1 | 212 (29.9) | 118 (31.6) | 3.9 |
| Midwest | 173 (32.2) | 104 (29.3) | 6.3 | 188 (26.5) | 86 (23.1) | 7.9 |
| Northeast | – | – | – | 21 (3.0) | 9 (2.4) | 3.4 |
| East | 68 (12.7) | 46 (13.0) | 0.9 | – | – | – |
| Unknown | – | – | – | 76 (10.7) | 22 (5.9) | 17.5† |
| Race, n (%) | ||||||
| White | – | – | – | 320 (45.1) | 150 (40.2) | 9.8 |
| Black | – | – | – | 25 (3.5) | 19 (5.1) | 7.8 |
| Asian | – | – | – | 13 (1.8) | 7 (1.9) | 0.3 |
| Other | – | – | – | 352 (49.6) | 197 (52.8) | 6.5 |
| Clinical characteristics# | ||||||
| Quan-CCI††, mean ± SD [median] | 2.7 (1.2) | 2.7 (1.3) | 3.0 | 3.1 (1.7) | 3.0 (1.7) | 3.4 |
| Baseline comorbidities, n (%) | ||||||
| Hypertension | 294 (41.4) | 120 (32.2) | 19.2† | |||
| Atrial fibrillation | 30 (5.6) | 22 (6.2) | 2.6 | 50 (7.0) | 37 (9.9) | 10.3† |
| Atrial flutter | 6 (1.1) | 3 (0.8) | 2.8 | 8 (1.1) | 0 (0.0) | 15.1† |
| Bleeding/hemorrhage | 20 (3.7) | 16 (4.5) | 3.9 | 14 (2.0) | 8 (2.1) | 1.2 |
| Gastrointestinal symptoms | 92 (17.1) | 62 (17.5) | 0.9 | 120 (16.9) | 47 (12.6) | 12.2† |
| Metastatic cancer | – | – | – | 17 (2.4) | 17 (4.6) | 11.8† |
| CHA2DS2-VASc, mean (SD)‡‡ | 1.7 (1.5) | 1.7 (1.5) | 3.4 | 2.3 (1.5) | 2.3 (1.4) | 5.6 |
| Baseline medication, n (%) | ||||||
| Use of corticosteroids | – | – | – | 103 (14.5) | 75 (20.1) | 14.8† |
| Use of antiplatelets | – | – | – | 50 (7.0) | 13 (3.5) | 16.0† |
| H2-receptor antagonists | 15 (2.8) | 7 (2.0) | 5.4 | 36 (5.1) | 16 (4.3) | 3.7 |
| Anticoagulants | 40 (7.4) | 28 (7.9) | 1.6 | 87 (12.3) | 42 (11.3) | 3.1 |
| ACE inhibitors | 181 (33.7) | 127 (35.8) | 4.3 | – | – | – |
| Diuretics | 83 (15.5) | 52 (14.6) | 2.3 | – | – | – |
| Beta blockers | 98 (18.3) | 80 (22.5) | 10.7† | 99 (13.9) | 53 (14.2) | 0.8 |
| Antihyperlipidemics | 198 (36.9) | 142 (4.0) | 6.4 | 140 (19.7) | 68 (18.2) | 3.8 |
†
Standardized difference ≥10%.
‡
Demographic characteristics were evaluated on the date of treatment initiation.
§
Insurance coverage type is identified by selecting the payer record closest to index date.
¶
For IQVIA, the Medicare category includes Medicare Advantage and Medicare Supplemental.
#
Clinical characteristics evaluated during the 6-month (IQVIA) or 12-month (Acentrus) baseline period, excluding the date of treatment initiation.
††
Reference: [40].
‡‡
ACE: Angiotensin-converting enzyme; Quan-CCI: Quan-Charlson Comorbidity Index; SD: standard deviation US: United States.
In Acentrus, a total of 710 and 373 patients with CLL/SLL initiating 1L single-agent ibrutinib or acalabrutinib were included, respectively (Figure 2). Mean observed duration of 1L treatment was 1.3 and 0.9 years for ibrutinib and acalabrutinib, respectively. Mean age (ibrutinib vs acalabrutinib: 71.5 vs 72.4 years, std diff.: 9.1%), proportion of women (38.5% vs 38.3%, std diff.: 0.2%), mean Quan-CCI (3.1 vs 3.0, std diff.: 3.4%) and mean CHA2DS2-VASc risk score (2.3 vs 2.3, std diff.: 5.6%) were similar between the two cohorts (Table 1).
Comparison of HRU & costs
In both databases, the number of all-cause inpatient admissions was comparable for ibrutinib versus acalabrutinib (IQVIA: 0.08 vs 0.07 PPPM, RR: 0.96, p = 0.614; Acentrus: 0.06 PPPM for both cohorts, RR: 1.08, p = 0.730) (Figure 3). A similar trend was observed for CLL/SLL-related inpatient admissions (IQVIA: 0.03 PPPM for both cohorts, RR: 0.90, p = 0.763; Acentrus: 0.03 vs 0.04 PPPM, RR: 0.78, p = 0.381). CLL/SLL-related outpatient visits were significantly lower in both databases for ibrutinib versus acalabrutinib (IQVIA: 0.86 vs 1.09 PPPM, RR: 0.85, p = 0.018; Acentrus: 0.57 vs 0.74 PPPM, RR: 0.80, p = 0.036).
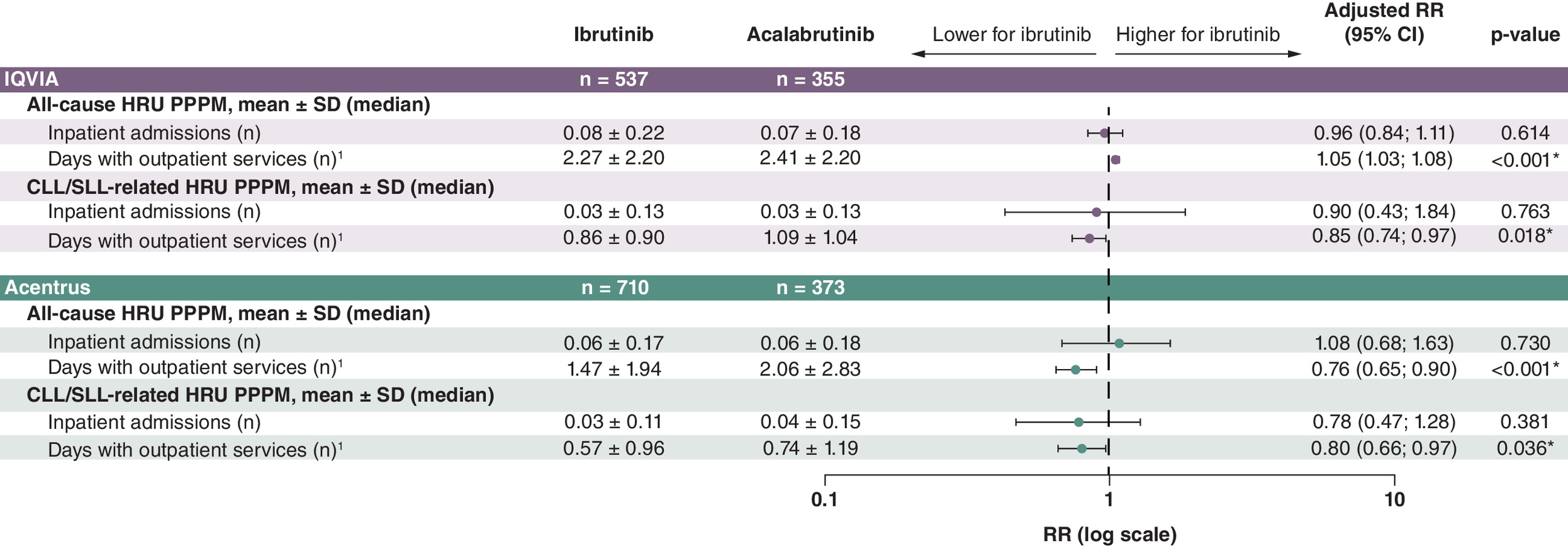
Figure 3. Comparison of healthcare resource use in chronic lymphocytic leukemia/small lymphocytic lymphoma patients initiating first-line ibrutinib or acalabrutinib.
1Outpatient services included outpatient and emergency department visits.
*p-value ≤ 0.05.
1L: First-line; CI: Confidence interval; CLL: Chronic lymphocytic leukemia; HRU: Healthcare resource use; PPPM: Per-patient-per-month; RR: Rate ratio; SD: Standard deviation; SLL: Small lymphocytic lymphoma.
Healthcare costs were numerically lower for ibrutinib versus acalabrutinib (Figure 4). In IQVIA, total all-cause costs (including medical and pharmacy costs) were $16,717 and $17,622 for the ibrutinib and acalabrutinib cohorts, respectively (MMCD: -$764, p = 0.279), with the majority of costs being CLL/SLL-related ($13,930 and $15,374 for the ibrutinib and acalabrutinib cohorts, respectively; MMCD: -$649, p = 0.133). While statistically nonsignificant, BTKi drug costs were a driver of lower all-cause and CLL/SLL-related costs for ibrutinib versus acalabrutinib (MMCD: -$467, p = 0.248), along with inpatient costs (MMCD: -$379, p = 0.479).

Figure 4. Comparison of costs in chronic lymphocytic leukemia/small lymphocytic lymphoma patients initiating first-line ibrutinib or acalabrutinib.
1Outpatient service costs included outpatient and emergency department visit-related costs.
*p-value ≤ 0.05.
1L: First-line; CI: Confidence interval; CLL: Chronic lymphocytic leukemia; MMCD: Mean monthly cost difference; PPPM: Per-patient-per-month; SD: Standard deviation; SLL: Small lymphocytic lymphoma; USD: United States dollar.
In Acentrus, total imputed (estimated) all-cause and CLL/SLL-related costs (including medical and pharmacy costs) were significantly lower in the ibrutinib versus acalabrutinib cohort. More specifically, total all-cause imputed (estimated) costs were $14,691 and $16,599 for the ibrutinib and acalabrutinib cohorts, respectively (MMCD: -$1355, p = 0.004), while total CLL/SLL-related imputed (estimated) costs were $12,186 and $13,715 for the ibrutinib and acalabrutinib cohorts, respectively (MMCD: -$1215, p = 0.004). Imputed (estimated) pharmacy costs were significantly lower for both all-cause and CLL/SLL-related costs (MMCD: -$940, p = 0.008), and were a driver of lower costs for the ibrutinib versus acalabrutinib cohort.
Discussion
To our knowledge, the current study is one of the largest to report on HRU and costs of patients with CLL/SLL treated with 1L ibrutinib or acalabrutinib. Two separate real-world databases were analyzed in this study, covering patients with various characteristics and insurance types, increasing the generalizability of study findings. The results showed longer duration of 1L, lower CLL/SLL-related outpatient visits, as well as numerically lower all-cause and CLL/SLL-related healthcare costs based on a mix of cost data from claims (IQVIA) and imputed cost data (Acentrus) for patients treated with ibrutinib compared with acalabrutinib.
There is limited literature comparing the economic outcomes associated with ibrutinib and acalabrutinib treatment in patients with CLL/SLL. In a previous real-world analysis of patients initiated on 1L ibrutinib or acalabrutinib by Fradley et al. CLL/SLL-related HRU and costs were similar in both cohorts (number of outpatient visits: 1.44 vs 1.47 PPPM, p = 0.624; total costs: $15,451 vs $15,169, p = 0.220) [26]. These costs are generally consistent with those observed in the current study, but this early analysis was conducted with data up to December 2021. The current study builds on the previously observed trends in HRU and costs [26] by using two distinct real-world databases and shows that over longer follow-up (September and April 2022, for IQVIA and Acentrus analyses, respectively), lower HRU and costs are observed for patients treated with ibrutinib compared with acalabrutinib.
While the reason for the difference in CLL/SLL-related outpatient visits could not be assessed and warrants additional research, it is possible that the lower number of visits for patients treated with ibrutinib was due to less monitoring compared with acalabrutinib, given that ibrutinib has been a well-established 1L treatment for CLL/SLL for a longer period of time. Indeed, based on further explorations of the data, it was found that the lower number of CLL/SLL-related outpatient visits for ibrutinib may have been due to a lower number of visits for management of CLL/SLL and associated laboratory testing (e.g., complete blood count or metabolic panel). Other potential reasons for the lower HRU and costs observed for ibrutinib may be related to the clinical outcomes observed for the two BTKis in prior real-world studies [14–17]. For instance, ibrutinib has been associated with higher treatment adherence [14,15] and longer TTNT compared with acalabrutinib for 1L CLL/SLL patients [16,17]. As treatment non-adherence has been associated with higher healthcare costs in previous studies [43,44], potentially due to increased rates of adverse events [45,46], the generally lower costs found for ibrutinib therapy in the current study may potentially be explained by higher adherence. Similarly, longer TTNT, as a proxy for progression-free disease [47,48], may indicate improved tolerability and a reduced need for patient follow-up and management. Finally, the possibility of dose reduction with ibrutinib may have contributed to lower pharmacy costs compared with acalabrutinib by extending the duration of ibrutinib prescriptions. Recent real-world analyses reported that 14.4–19.6% [49,50] of patients initiating ibrutinib in 1L for the treatment of CLL/SLL have a dose reduction, which may reduce the risk of adverse events and improve treatment adherence [51], while maintaining efficacy compared with those without a dose reduction [49,50]. Therefore, dose reduction may further improve TTNT and overall survival for the overall population of patients treated with ibrutinib compared with acalabrutinib [17,52], and contribute to the extended follow-up time and reduced pharmacy costs observed for ibrutinib.
Overall, with the current emerging real-world evidence for ibrutinib and acalabrutinib, the current study provides another perspective, contrasting with other economic evaluations including cost effectiveness analyses (CEAs), by capturing current clinical practice and implications on actual costs incurred in the management of CLL/SLL with BTKis. A recent publication on CEA comparing BTKis found higher costs per quality-adjusted life-year for ibrutinib compared with acalabrutinib, based on disease progression and extrapolated survival data, and with estimation of treatment duration, adverse event frequency, and all-cause death probability [53]. The CEA model also used the wholesale acquisition cost to estimate BTKis costs, which is different from actual paid amounts based on plan-negotiated contracts with providers. Finally, TTNT and real-world clinical practice involving dose reductions were not accounted for, despite their impact on real-world costs. In contrast, this real-world study captured all-cause medical services reimbursed by the payer for each patient, including costs related to BTKis and other treatments received for comorbidities. Given that patients with CLL/SLL with diverse characteristics initiating BTKis live longer and require a variety of medical services, this comprehensive approach with adjustment of covariates addresses the need for a real-world perspective on the cost burden to payers managing patients with CLL/SLL. Our study found lower per-patient all-cause costs for patients with CLL/SLL treated with ibrutinib versus acalabrutinib (IQVIA MMCD: -$764, Acentrus MMCD: -$1355) after accounting for age, comorbidity burden, and other differences in patient characteristics. Therefore, by leveraging real-world data, the economic evaluation of BTKi treatment in this study addresses key limitations associated with CEAs in the current literature. As the current results show, along with previous real-world evidence on improved clinical outcomes in patients treated with 1L ibrutinib compared with acalabrutinib, ibrutinib can be a cost-effective option for the 1L treatment of CLL/SLL.
The analyses presented in the current study are subject to some limitations. First, analyses were based on real-world claims and EMR data, which may contain omissions or inaccuracies. However, these should equally impact all patients and thus should not affect the overarching results. In addition, Acentrus is a provider-based data source, where records are only available for patient visits that occur in the network of academic and nonteaching hospital systems that are included in the database, which may explain the slightly lower number of visits observed in this database compared with IQVIA. Furthermore, both analyses used washout periods to define 1L use of ibrutinib and acalabrutinib (IQVIA: 6 months; Acentrus: 12 months). While these definitions have been extensively used in real-world studies [24,54–57], they may have allowed for patients with longer remission periods after a previous anticancer therapy to be included in the study populations. In the Acentrus analyses, claims data were unavailable; therefore, costs were imputed using literature-based estimates from a mix of commercial and Medicare patients, with the assumption that the mean cost was the same for all units of a given HRU. As such, the intensity of a unit of HRU did not vary between patients and costs may not be representative of the Acentrus patient population receiving 1L ibrutinib or acalabrutinib treatment for CLL/SLL. Lastly, while all analyses accounted for differences in baseline characteristics, it is possible that residual or unmeasured confounding (e.g., mutation status) remains.
Conclusion
In this real-world study of two large databases covering various populations, CLL/SLL patients initiating 1L single-agent ibrutinib had longer duration of 1L, significantly lower CLL/SLL-related outpatient visits and numerically lower costs compared with patients initiating 1L single-agent acalabrutinib. These findings, along with previous real-world studies showing higher treatment adherence [14,15] and longer TTNT [16,17] for 1L ibrutinib as compared with acalabrutinib, suggest that ibrutinib can be a cost-effective 1L therapy for CLL/SLL.
Summary points
•
This study evaluated healthcare resource use (HRU) and costs between first-line (1L) single-agent ibrutinib and acalabrutinib in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) using real-world data from claims and electronic medical records.
•
IQVIA PharMetrics Plus claims data and Acentrus electronic medical records data were used. Previously published cost assumptions were used to impute costs in Acentrus.
•
Patients initiating 1L ibrutinib or acalabrutinib treatment after 21 November 2019 were included. Sample sizes were 537 and 355 for IQVIA, and 710 and 373 for Acentrus, for ibrutinib and acalabrutinib, respectively.
•
Regression analyses adjusted for baseline differences were used to compare HRU and costs.
•
Patients initiating ibrutinib had longer duration of 1L than those on acalabrutinib.
•
Patients initiating ibrutinib had significantly fewer outpatient visits than those on acalabrutinib, indicating reduced need for outpatient services with ibrutinib in both datasets.
•
Total all-cause and CLL/SLL related costs were numerically lower for ibrutinib versus acalabrutinib in both datasets.
•
These findings suggest that ibrutinib can be a cost-effective 1L therapy for CLL/SLL.
•
The use of two large real-world databases bolstered the generalizability of study findings.
Author contributions
ZP Qureshi, J He, A Bokun, Z Ding contributed to study conception and design, and drafting and revision of the manuscript; MH Lafeuille, B Emond and P Gogna contributed to study conception and design, acquisition of data, data analysis and drafting and revision of the manuscript; KA Rogers, B Muluneh and M Fradley contributed to study conception and design and drafting and revision of the manuscript. All authors have provided final approval of this version to be published and agree to be accountable for all aspects of the work.
Financial disclosure
This study was funded by Janssen Scientific Affairs, LLC, a Johnson & Johnson company. The study sponsor was involved in several aspects of the research, including the study design, interpretation of data and writing of the manuscript. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
MH Lafeuille, B Emond and P Gogna are employees of Analysis Group, Inc., which has received research funding from Janssen Scientific Affairs, LLC, a Johnson & Johnson company. ZP Qureshi, J He and A Bokun are employees of Janssen Scientific Affairs, LLC, a Johnson & Johnson company and stockholders of Johnson & Johnson. Z Ding was an employee of Janssen Scientific Affairs, LLC, a Johnson & Johnson company at the time the study was conducted. KA Rogers received research funding from Genentech, AbbVie, AstraZeneca and LOXO@lilly and consults for Genentech, AbbVie, Janssen, Pharmacyclics, BeiGene, LOXO@Lilly, Alpine Immune Sciences. M Fradley received research funding from AstraZeneca and Medtronic, and consults for AstraZeneca, Pfizer, Johnson and Johnson, AbbVie, Janssen and Zoll. B Muluneh’s spouse is an employee and stockholder in Novartis Pharmaceuticals. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Data sharing statement
The data that support the findings of this study are available from IQVIA and Acentrus, but restrictions apply to the availability of these data, which were used pursuant to a data use agreement. The data are available through requests made directly to IQVIA and Acentrus, subject to their respective requirements for access.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 26.83 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
National Cancer Institute Surveillance Epidemiology and End Results Program. Cancer stat facts: leukemia — chronic lymphocytic leukemia (CLL) 2025 [cited: 28 March 2025]. Available from: https://seer.cancer.gov/statfacts/html/clyl.html
2.
American Cancer Society. Key statistics for chronic lymphocytic leukemia 2025. Available from: https://www.cancer.org/cancer/types/chronic-lymphocytic-leukemia/about/key-statistics.html
3.
Patel K, Pagel JM. Current and future treatment strategies in chronic lymphocytic leukemia. J. Hematol. Oncol. 14(1), 69 (2021).
4.
Barr PM, Owen C, Robak T et al. Up to 8-year follow-up from RESONATE-2: first-line ibrutinib treatment for patients with chronic lymphocytic leukemia. Blood Adv. 6(11), 3440–3450 (2022).
• Extended follow-up data from the RESONATE-2 phase III clinical trial in treatment-naïve chronic lymphocytic leukemia (CLL) patients. Over an 8-year follow-up period, ibrutinib was associated with significantly improved progression-free survival and overall survival compared with chlorambucil.
5.
Fraser GAM, Chanan-Khan A, Demirkan F et al. Final 5-year findings from the phase III HELIOS study of ibrutinib plus bendamustine and rituximab in patients with relapsed/refractory chronic lymphocytic leukemia/small lymphocytic lymphoma. Leuk. Lymphoma 61(13), 3188–3197 (2020).
6.
Moreno C, Greil R, Demirkan F et al. First-line treatment of chronic lymphocytic leukemia with ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab: final analysis of the randomized, phase III iLLUMINATE trial. Haematologica 107(9), 2108–2120 (2022).
7.
Shanafelt TD, Wang XV, Hanson CA et al. Long-term outcomes for ibrutinib-rituximab and chemoimmunotherapy in CLL: updated results of the E1912 trial. Blood 140(2), 112–120 (2022).
8.
Woyach JA, Ruppert AS, Heerema NA et al. Long-term results of Alliance A041202 show continued advantage of ibrutinib-based regimens compared with bendamustine plus rituximab (br) chemoimmunotherapy. Blood 138(Suppl. 1), 639 (2021).
9.
Burger JA, Barr PM, Robak T et al. Long-term efficacy and safety of first-line ibrutinib treatment for patients with CLL/SLL: 5 years of follow-up from the phase III RESONATE-2 study. Leukemia 34(3), 787–798 (2020).
10.
Moreno C, Greil R, Demirkan F et al. Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in first-line treatment of chronic lymphocytic leukaemia (iLLUMINATE): a multicentre, randomised, open-label, phase III trial. Lancet Oncol. 20(1), 43–56 (2019).
11.
Shanafelt TD, Wang XV, Kay NE et al. Ibrutinib-rituximab or chemoimmunotherapy for chronic lymphocytic leukemia. N. Engl. J. Med. 381(5), 432–443 (2019).
12.
Woyach JA, Ruppert AS, Heerema NA et al. Ibrutinib regimens versus chemoimmunotherapy in older patients with untreated CLL. N. Engl. J. Med. 379(26), 2517–2528 (2018).
13.
CALQUENCE (acalabrutinib). Prescribing Information. AstraZeneca Pharmaceuticals LP, DE, USA (2022).
14.
Lu X, Emond B, Qureshi Z et al. CLL-492 Real-world adherence to first-line ibrutinib and acalabrutinib single-agent among patients with chronic lymphocytic leukemia/small lymphocytic lymphoma. Clin. Lymph. Myeloma Leuk. 22, S280–S281 (2022).
15.
Lu X, Emond B, Morrison L et al. Real-world comparison of first-line treatment adherence between single-agent ibrutinib and acalabrutinib in patients with chronic lymphocytic leukemia. Patient Pref. Adhere. 17, 2073–2084 (2023).
• Retrospective, real-world study comparing adherence between CLL/SLL patients treated with first-line (1L) ibrutinib or acalabrutinib in the US using electronic medical records (EMR) data. The study concluded that patients treated with 1L ibrutinib had higher adherence to treatment than patients treated with 1L acalabrutinib.
16.
Jacobs R, Levy M, Yazbeck V et al. Comparison of time to next treatment between patients with chronic lymphocytic leukemia initiating first-line ibrutinib or acalabrutinib, overall and in a subgroup with high-risk characteristics. Presented at: International Ultmann Chicago Lymphoma Symposium and Eurporean Hematology Association (2024).
17.
Jacobs R, Lu X, Emond B et al. Time to next treatment in patients with chronic lymphocytic leukemia initiating first-line ibrutinib or acalabrutinib. Future Oncol. 20(1), 39–53 (2024).
• Retrospective, real-world study comparing time to next treatment in patients with CLL/SLL treated with 1L ibrutinib or acalabrutinib in the US using EMR data. The study concluded that next treatment (a clinically meaningful measure for real-world progression) occurred less often with 1L ibrutinib.
18.
Akhtar OS, Attwood K, Lund I et al. Dose reductions in ibrutinib therapy are not associated with inferior outcomes in patients with chronic lymphocytic leukemia (CLL). Leuk. Lymphoma 60(7), 1650–1655 (2019).
19.
Ghosh N, Qureshi ZP, Ding Z et al. Ibrutinib dose adjustment does not impact time to next treatment in first-line patients with chronic lymphocytic leukemia: a real-world analysis of electronic medical records from academic and non-teaching hospitals using target trial emulation. Blood 142, 1915 (2023).
20.
Ghosh N, Wang R, Ding Z et al. Comparative effectiveness of ibrutinib flexible dosing treatment strategies on time to next treatment in a largely community-based claims database: a target trial emulation study. Blood 142, 270 (2023).
•• Retrospective, real-world study evaluating time to next treatment in 1L ibrutinib patients with CLL/SLL with or without a dose reduction. After emulation of a target trial, dose reduction was not associated with increased risk of initiating a next treatment.
21.
Stephens DM, Brown JR, Shuo M et al. Ibrutinib dose modifications for management of cardiac adverse events in patients with B-cell malignancies: pooled analysis of 10 clinical trials. J. Clin. Oncol. 41(Suppl. 16), 7538 (2023).
22.
Woyach JA, Barr PM, Kipps TJ et al. Characteristics and clinical outcomes of patients with chronic lymphocytic leukemia/small lymphocytic lymphoma receiving ibrutinib for >/= 5 years in the RESONATE-2 study. Cancers (Basel) 15(2), 507 (2023).
23.
Shadman M, Karve S, Abbazio C et al. P1846: real-world clinical outcomes of first-line ibrutinib dose reduction versus acalabrutinib among patients with chronic lymphocytic leukemia or small lymphocytic lymphoma. Presented at: European Hematology Association, Madrid, Spain, 13–16 June 2024.
24.
Huang Q, Emond B, Lafeuille M-H et al. Healthcare resource utilization and costs associated with first-line ibrutinib compared to chemoimmunotherapy treatment among Medicare beneficiaries with chronic lymphocytic leukemia. Curr. Med. Res. Opin. 36(12), 2009–2018 (2020).
•• Retrospective, real-world study comparing healthcare resource utilization and costs for Medicare beneficiaries with CLL/SLL who received ibrutinib versus chemoimmunotherapy (CIT) in 1L. The study found that single-agent 1L ibrutinib was associated with lower monthly costs relative to CIT.
25.
Emond B, Sundaram M, Romdhani H et al. Comparison of time to next treatment, health care resource utilization, and costs in patients with chronic lymphocytic leukemia initiated on front-line ibrutinib or chemoimmunotherapy. Clin. Lymph. Myeloma Leuk. 19(12), 763–775.e2 (2019).
•• Retrospective, real-world study comparing time to next treatment, health care resource utilization (HRU) and total direct costs in patients with CLL initiating 1L ibrutinib or CIT. The study found that ibrutinib was associated with longer time to next treatment, fewer monthly days with outpatient visits and lower total monthly costs.
26.
Fradley M, Lafeuille MH, Emond B et al. Early adherence and persistence to first-line ibrutinib or acalabrutinib among patients with chronic lymphocytic leukemia/small lymphocytic lymphoma and atrial fibrillation. Presented at: American Society of Hematology Annual Meeting, New Orleans, LA, USA, 10–13 December 2022.
27.
Davids M, Mato A, Hum J et al. Majic: a phase III prospective, multicenter, randomized, open-label trial of acalabrutinib plus venetoclax versus venetoclax plus obinutuzumab in previously untreated chronic lymphocytic leukemia or small lymphocytic lymphoma. Blood 138(Suppl. 1), 1553–1554 (2021).
28.
Davids M, Lampson B, Tyekucheva S et al. Acalabrutinib, venetoclax, and obinutuzumab as frontline treatment for chronic lymphocytic leukaemia: a single-arm, open-label, phase II study. Lancet Oncol. 22(10), 1391–1402 (2021).
29.
Jain N, Keating M, Thompson P et al. Ibrutinib and venetoclax for first-line treatment of CLL. N. Engl. J. Med. 380(22), 2095–2103 (2019).
30.
IMBRUVICA (ibrutinib). Prescribing Information. Janssen Biotech, Inc, PA, USA (2022).
31.
Muñoz J, Sarosiek S, Castillo JJ. Managing ibrutinib-intolerant patients with B-cell malignancies. Oncologist 28(4), 309–318 (2023).
32.
Stephens DM, Byrd JC. How I manage ibrutinib intolerance and complications in patients with chronic lymphocytic leukemia. Blood 133(12), 1298–1307 (2019).
33.
Hallek M, Al-Sawaf O. Chronic lymphocytic leukemia: 2022 update on diagnostic and therapeutic procedures. Am. J. Hematol. 96(12), 1679–1705 (2021).
34.
O'Brien SM, Brown JR, Byrd JC et al. Monitoring and managing BTK inhibitor treatment-related adverse events in clinical practice. Front. Oncol. 11, 720704 (2021).
35.
Morrison L, Lin D, Benson C et al. Projecting the economic outcomes of switching patients with schizophrenia from oral atypical antipsychotics to once-monthly, once-every-3-months, and once-every-6-months paliperidone palmitate. J. Manag. Care Spec. Pharm. 29(2), 161–171 (2023).
36.
Maeng DD, Stewart WF, Yan X et al. Use of electronic health records for early detection of high-cost, low back pain patients. Pain Res. Manag. 20(5), 234–240 (2015).
37.
Sheffield BS, Eaton K, Emond B et al. Cost savings of expedited care with upfront next-generation sequencing testing versus single-gene testing among patients with metastatic non-small cell lung cancer based on current canadian practices. Curr. Oncol. 30(2), 2348–2365 (2023).
38.
Korjian S, Daaboul Y, Laliberté F et al. Cost implications of anticoagulation strategies after percutaneous coronary intervention among patients with atrial fibrillation (A PIONEER-AF PCI analysis). Am. J. Cardiol. 123(3), 355–360 (2019).
39.
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 28(25), 3083–3107 (2009).
40.
Quan H, Li B, Couris CM et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
41.
Melgaard L,Gorst-Rasmussen A, Lane DA, Rasmussen LH, Larsen TB, Lip GYH, , Assessment of the CHA2DS2-VASc Score in Predicting Ischemic Stroke, Thromboembolism and Death in Patients With Heart Failure With and Without Atrial Fibrillation. JAMA. 314(10), 1030 (2015).
42.
January CT, Wann LS, Calkins H et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation. 140(2), e125–e1 (2019).
43.
Cutler RL, Fernandez-Llimos F, Frommer M et al. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open 8(1), e016982 (2018).
44.
Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag. Healthcare Pol. 7, 35–44 (2014).
45.
Santoleri F, Sorice P, Lasala R et al. Patient adherence and persistence with imatinib, nilotinib, dasatinib in clinical practice. PLoS ONE 8(2), e56813 (2013).
46.
Gillespie CW, Morin PE, Tucker JM et al. Medication adherence, health care utilization, and spending among privately insured adults with chronic conditions in the United States, 2010–2016. Am. J. Med. 133(6), 690–704.e19 (2020).
47.
Li Q, Zhang H, Chen Z et al. Validation of real-world data-based endpoint measures of cancer treatment outcomes. AMIA Annu. Symp. Proc. 2021, 716–725 (2021).
48.
Rivera DR, Henk HJ, Garrett-Mayer E et al. The friends of cancer research real-world data collaboration pilot 2.0: methodological recommendations from oncology case studies. Clin. Pharmacol. Ther. 111(1), 283–292 (2022).
49.
Shadman M, Salkar M, Srivastava B et al. Real-world outcomes following ibrutinib dose reduction in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma. Leuk. Lymphoma 66(1), 44–53 (2025).
50.
Ghosh N, Wang R, Qureshi ZP et al. Impact of ibrutinib dose adjustment on TTNT in first-line CLL/SLL: a real-world analysis using target trial emulation. Blood Neoplasia 1(3), 100022 (2024).
51.
Rogers KA, Lu X, Emond B et al. Real-world (RW) dosing patterns and outcomes among chronic lymphocytic leukemia (CLL) patients (pts) with or without an ibrutinib (IBR) dose adjustment (DA) in first-line (1L). J. Clin. Oncol. 41(16), 7537 (2023).
52.
Fitzgerald L, Khan W, Bokun A et al. Overall survival of patients with chronic lymphocytic leukemia treated with frontline bruton's tyrosine kinase inhibitors: an analysis of the United States Veterans Health Administration database. Blood 144, 7753 (2024).
53.
Alrawashdh N, McBride A, Abraham I. Cost-effectiveness analyses of first line ibrutinib versus acalabrutinib versus zanubrutinib followed by second line venetoclax plus rituximab in previously untreated chronic lymphocytic leukemia (CLL) patients. Blood 140(Suppl. 1), 2155–2156 (2022).
54.
Paludo J, Sarosiek SR, von Keudell GR et al. Real-world treatment patterns and healthcare resource utilization in patients with waldenström macroglobulinemia initiating first-line treatment with ibrutinib or zanubrutinib. Blood 142, 7385 (2023).
55.
Seiter K, Latremouille-Viau D, Guerin A et al. Burden of infections among chronic myeloid leukemia patients receiving dasatinib or nilotinib: a real-world retrospective healthcare claims study in the United States. Adv. Ther. 35(10), 1671–1685 (2018).
56.
Narezkina A, Akhter N, Lu X et al. Real-world persistence and time to next treatment with ibrutinib in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma including patients at high risk for atrial fibrillation or stroke. Clin. Lymph. Myeloma Leuk. 22(11), e959–e971 (2022).
57.
Kabadi SM, Goyal RK, Nagar SP, Kaye JA, Davis KL. Treatment patterns, adverse events, and economic burden in a privately insured population of patients with chronic lymphocytic leukemia in the United States. Cancer Med. 8(8), 3803–3810 (2019).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 8 November 2024
Accepted: 7 April 2025
Published online: 22 April 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A comparison of healthcare resource utilization and costs between patients with chronic lymphocytic leukemia treated with first-line ibrutinib or acalabrutinib using two large US real-world databases. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0210
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Murali Janakiram, Sabyasachi Ghosh, Victoria Alegria, Matthew Perciavalle, Bruno Emond, Jessica Maitland, Todd Bixby, Saurabh P Nagar, Zaina P Qureshi, Dimitra Rafailia Bakaloudi, Danai Dima, Healthcare resource utilization and costs in patients with multiple myeloma administered ciltacabtagene autoleucel in outpatient versus inpatient settings after one to three prior lines of therapy, Journal of Comparative Effectiveness Research, 10.57264/cer-2026-0052, 15, 7, (2026).
- Lindsey Fitzgerald, Sabyasachi Ghosh, Alex Bokun, Angela Lax, Fan Mu, Eric Wu, Yilu Lin, Lizheng Shi, Zaina P Qureshi, Solomon A Graf, Healthcare cost comparison between first-line ibrutinib and acalabrutinib in chronic lymphocytic leukemia patients in the Veterans Affairs, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0084, 14, 11, (2025).