Clinical assessment of the potential use of a novel single-dose prefilled injection device for the administration of Acthar Gel in children: a narrative review
Publication: Journal of Comparative Effectiveness Research
Abstract
Acthar® Gel (repository corticotropin injection; Mallinckrodt Pharmaceuticals, NJ, USA) is indicated for the treatment of myriad inflammatory disorders and is currently administered manually via a vial and syringe. The administration of Acthar via a single-dose prefilled injector (SelfJect™) is intended to simplify its subcutaneous (SC) delivery. The purpose of this review was to determine whether SelfJect is suitable for use in pediatric patients through a literature assessment of various factors, including skin depth, needle length and gauge, dosage, force required for injection, and potential harms. Infants and young children, who commonly have skin-to-muscle distances less than the minimum depth of SelfJect administration, may have risk of unintentional intramuscular (IM) injection; however, an inadvertent IM injection poses no additional risk to children because of the bioequivalence between SC and IM administration of Acthar. The needle gauge of SelfJect is acceptable for pediatric patients and aligns with the Centers for Disease Control and Prevention recommendations for SC injections. The dosage delivered by SelfJect is only appropriate for children over 2 years of age. Although adolescents would likely be able to achieve the minimum force required to remove the protective cap and deliver a full dose of Acthar with SelfJect, an adult (18 years of age and older) should administer SelfJect to pediatric patients. In addition to the commonly reported postmarketing adverse events (AEs) from Acthar administration (e.g., asthenic conditions, fluid retention, insomnia, headache and increased blood glucose), injection site-related AEs common to injection devices may occur with SelfJect use. The risk of needlestick injury from SelfJect is mitigated by a needle guard. In summary, this review of injection device considerations demonstrates that SelfJect is appropriate for use in the pediatric population.
Shareable abstract
This narrative review found that a single-dose prefilled injector (SelfJect™) for administration of Acthar® Gel (repository corticotropin injection) is appropriate for use in pediatric patients if administered by an adult 18 years of age and older. #ActharGel #SelfJect
Plain language summary of a narrative review on the potential use of a novel injection device for Acthar Gel in children
What is this article about?
Acthar® Gel (repository corticotropin injection) may be prescribed for inflammatory diseases, such as rheumatoid arthritis and lupus. Acthar must be injected under the skin using a vial and syringe. A novel injection device (SelfJect™) has been developed to simplify Acthar injection. This review assessed if SelfJect may be used in pediatric patients (less than 18 years of age).
What were the results?
In infants and young children, Acthar may accidentally be injected too deeply into the muscle because of small distances from the skin to the underlying muscle. However, Acthar functions the same whether it is injected beneath the skin or into the muscle, and there is no risk for children if Acthar is injected too deeply. The size of the SelfJect needle is acceptable for pediatric patients and is in line with injection recommendations from the Centers for Disease Control and Prevention. The medication dosage delivered with SelfJect is only appropriate for children greater than 2 years of age. Although adolescents are likely strong enough to operate SelfJect, it is currently recommended that SelfJect injections be given to pediatric patients by adults 18 years of age and older. Side effects, such as pain, redness and swelling, may occur at the site of injection. A needle guard prevents inadvertently contacting the device needle.
What do the results of the study mean?
The novel SelfJect device for injection of Acthar is appropriate for use in pediatric patients if an adult operates the device.
Acthar® Gel (repository corticotropin injection; Mallinckrodt Pharmaceuticals, NJ, USA) is a complex mixture of porcine adrenocorticotrophic hormone analogs and other pituitary peptides formulated in a sterile 16% gelatin preparation for extended release after intramuscular (IM) or subcutaneous (SC) injection [1]. Acthar induces anti-inflammatory and immunomodulatory effects by activating melanocortin receptors on various cell types throughout the body [2]. Acthar is indicated for the treatment of various inflammatory disorders, including infantile spasms, acute exacerbations of multiple sclerosis, rheumatoid arthritis, systemic lupus erythematosus, symptomatic sarcoidosis, certain nephrotic syndromes and ophthalmic diseases [1]. In pediatric patients, Acthar has been shown to be safe and effective for the treatment of infantile spasms and for diuresis and remission of proteinuria in nephrotic syndrome [2–7].
Supplied as a 5-ml multidose vial containing 80 U/ml, the manual administration of Acthar has numerous steps, including calculating the required injection amount, uncapping the vial, cleaning the rubber stopper with an alcohol swab, using a wide-bore needle to draw up the medication, attaching a smaller gauge needle in preparation for injection, cleaning the appropriate injection site, priming the needle and finally injecting the medication [8]. However, a new single-dose prefilled injector (SelfJect™) was recently approved by the US FDA as a combination product of Acthar in a prefilled syringe and a single-dose drug delivery device, which was designed to improve the speed and ease of delivery.
Numerous injection devices are currently on the market for a wide range of diseases, including Type 1 and 2 diabetes, rheumatoid arthritis, systemic lupus erythematosus, atopic dermatitis and other inflammatory disorders [9–13]. Injection devices are designed to be easy to use and are intended to provide quick and accurate administration of a medication, eliminating the need for ampoules, syringes and needles [14,15]. They are specifically designed to reduce the risk of user error, which can be particularly important in emergency situations where appropriate dosing and administration technique are critical [14]. Injection devices commonly have built-in safety features, such as needle shields and locking mechanisms, to prevent accidental needlestick injuries and to ensure proper dosing and injection technique [16]. The use of injection devices in children can provide a consistent and reliable method of administering medications, especially for children with chronic conditions that require regular injections [16].
The purpose of this clinical review is to determine whether SelfJect is suitable for use in patients under 18 years of age. Factors such as skin depth, needle length and gauge, dosage, force required for injection and potential harms were investigated.
Cutaneous & SC tissue depth
Skin depth is an important consideration for SelfJect use in children in order to achieve the intended SC administration (Figure 1). However, information on skin thickness of infants and children is limited.
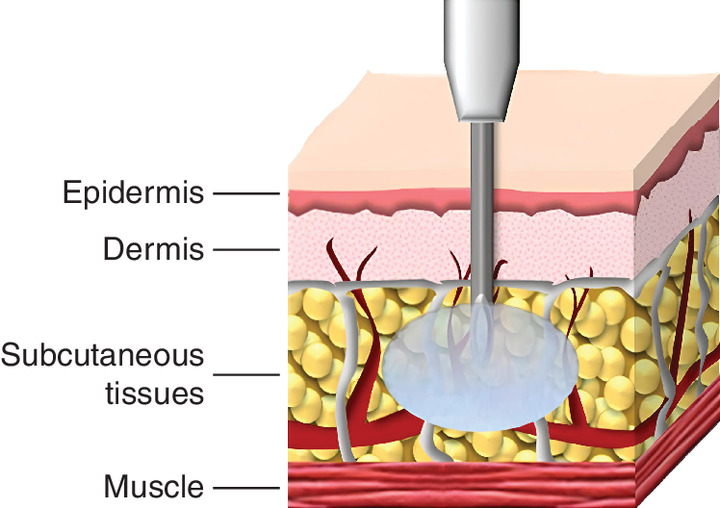
Figure 1. Depiction of traditional subcutaneous injection.
Reproduced from Kim H, Park H, Lee SJ. Effective method for drug injection into subcutaneous tissue. Sci Rep. 2017;7(1):9613. doi:10.1038/s41598-017-10110-w
Using ultrasound echography, Saitoh et al. found that mean skin thickness in Japanese infants aged 2 months was 1.67 mm in the deltoid region and 1.83 mm in the suprascapular region [17]. Infants who were remeasured at 6 months saw a significant increase in mean deltoid skin thickness (1.84 mm) but no significant difference in suprascapular skin thickness. As expected, skin thickness gradually increased from age 2 months to adolescence. There was also a positive correlation between body weight and deltoid and suprascapular skin thickness in adolescents and sex did not correlate with skin thickness.
A similar study in Caucasian children aged 8 weeks to 18 years assessed skin thickness via high-frequency ultrasound [18]. Mean skin thickness of the proximal ventral forearm, the proximal dorsal forearm, and the lateral upper leg (only measured in children ages 8 weeks to 2 years) was 0.99 mm, 1.20 mm and 1.28 mm, respectively. The greatest mean skin thickness was 1.32 mm in the deltoid region, which is less than the mean deltoid skin thickness of 1.67 mm in Japanese infants aged 2 months [17], perhaps owing to differences in race/ethnicity. Like the study by Saitoh et al. [17], skin thickness correlated significantly with age and BMI and sex did not have an association with skin thickness.
Lo Presti et al. measured both skin and SC tissue depth in children to assess the distance from skin to muscle [19]. The study enrolled 101 children aged 2 to 17 years with Type 1 diabetes and divided them into three age groups: 2 to 6 years, 7 to 13 years and 14 to 17 years. Skin thickness alone increased significantly with age, with the thickest skin in the buttocks of adolescents (mean: 2.29 mm) and the thinnest skin in the arms of the youngest children (mean: 1.58 mm). Combined skin and SC tissue depth showed a similar trend, albeit with greater overall variability, with thickness increasing in the order of arm, thigh, abdomen and buttocks in all age groups. The thickest average skin and SC tissue was in the buttocks of the 7- to 13-year age group (8.73 mm), while the thinnest was in the arms of the 2- to 6-year age group (4.89 mm). Although there was no significant difference in skin thickness based on sex, girls overall had significantly higher combined skin and SC tissue depth.
Needle length & gauge
Older studies using needles up to 12.7 mm in length showed that unexpected IM insulin injections that were intended to be SC were common in children with diabetes [20,21]. As shorter needles were introduced, the risk of IM injection decreased; a study published in 1999 demonstrated a frequency of IM injection of 86% with 12.7-mm needles, which fell to 38% with 8-mm needles [22]. Birkebaek et al. studied even shorter needles and found that significantly fewer IM injections, given perpendicular to the skin without a skinfold in the abdomen and thigh, occurred with a 4-mm needle than with a 6-mm needle [23].
Lo Presti et al. proposed recommendations for needle lengths and injection techniques based on the skin-to-muscle distance in children [19]. This study demonstrated that numerous children had skin-to-muscle distances of less than 4 mm, a threshold representing the length of a short pen insulin needle. This was seen at all 4 injection sites (arm, thigh, abdomen and buttocks) and across the range of BMI values, albeit more so in younger patients. With a 90-degree injection and non-pinch-up technique, the rate of IM injection in the 2- to 6-year age group with a 4-mm pen needle was expected to be 20.2%. This rate more than doubled when a 5-mm needle was used and more than tripled with a 6-mm needle. Using the same technique, the rates of IM injection with a 4-mm pen needle in the 7- to 13- and 14- to 17-year age group were 4.6% and 2.4%, respectively, and those rates similarly increased as needle length rose to 5 or 6 mm.
Lo Presti et al. showed that the youngest children are at high risk for unintentional IM injection with their smaller skin-to-muscle distances [19]. There was also risk of IM injection in older pediatric groups, particularly as needle length increased beyond 4 mm. As such, the 4-mm needle was deemed by the authors to be the safest needle length for all children to avoid inadvertent IM medication delivery. For the 2- to 6-year age group, the authors recommended using the pinch-up technique at all injection sites, even with a 4-mm needle, to increase the skin-to-muscle distance.
Further, several studies demonstrate that an angled needle insertion technique can reduce the risk of IM injection in children [24,25]. This, however, is not practical with injection devices, which are generally held perpendicular to the skin. Proper needle length and injection technique (i.e., pinch-up) with injection devices thus becomes even more important to ensure proper SC drug administration.
Regarding SelfJect, the injector controls needle insertion depth to deliver medication to dermal tissue at a depth of 4 to 8 mm beneath the outer surface of the skin. The injector also does not commence drug delivery until the needle guard is depressed such that the needle protrudes past the needle guard by at least 4 mm. A needle length ≥4 mm carries a risk of IM injection in children, particularly when given perpendicular to the skin [19].
However, Acthar has been shown to be bioequivalent when administered IM or SC [26]. Brod et al. demonstrated that there was no statistically significant difference in total serum cortisol levels between SC or IM administration of identical doses of Acthar [26]. This implies that SelfJect does not pose any additional risks beyond those associated with potential IM injection.
Regarding needle gauge, the Centers for Disease Control and Prevention (CDC) recommend using a 23- to 25-gauge needle for SC injections for all ages [27]. SelfJect uses a 0.5-inch (12.7-mm), 23-gauge, thin wall needle (3 bevel), which, per CDC guidelines [27], is appropriate for administration to pediatric patients.
Dosage
Appropriate medication dosage is an important consideration with injection device use. Regarding Acthar, the recommended dosing regimen in children varies depending on the treatment indication, age of the patient and the patient's general medical condition [1]. Frequency and dose of the drug should be determined by considering the severity of the disease and the initial response of the patient [1]. Close monitoring is recommended to ensure efficacy and minimize the risk of adverse events (AEs).
For children over 2 years of age, the usual dose of Acthar is 40 to 80 U given IM or SC every 24 to 72 hours [1]. SelfJect delivers either 0.5 ml (40 U) or 1.0 ml (80 U) minimum dose volume, an amount comparable with the upper volume limit of other injection devices (Table 1) [28]. Thus, the dosage for SelfJect is appropriate for children over 2 years of age.
| Drug | Manufacturer | Volume (ml) | Injection duration (s)† |
|---|---|---|---|
| Vyleesi® (bremelanotide) | AMAG | 0.3 | 7 |
| Acthar® Gel (repository corticotropin injection) | Mallinckrodt | 0.5 or 1.0 | 15 |
| Actemra® (tocilizumab) | Roche/Genentech | 0.9 | 10 |
| Fasenra® (benralizumab) | AstraZeneca | 1.0 | 15 |
| Nucala® (mepolizumab) | GlaxoSmithKline | 1.0 | 15 |
| Emgality® (galcanezumab) | Lilly | 1.0 | 10 |
| Aimovig® (erenumab) | Amgen | 1.0 | 15 |
| Taltz® (ixekizumab) | Lilly | 1.0 | 10 |
| Benlysta® (belimumab) | GlaxoSmithKline | 1.0 | 15 |
| Kevzara® (sarilumab) | Sanofi Aventis | 1.14 | 15 |
†
The duration shown in the prescribing information refers to the actual duration required to deliver the drug product (i.e., the injection duration) and an additional holding time and safety margin.
Reproduced with permission from Taylor & Francis Ltd (http://www.tandfonline.com/) from Schneider A, Mueller P, Jordi C et al. Hold the device against the skin: the impact of injection duration on user's force for handheld autoinjectors. Expert Opin. Drug Deliv. 17(2), 225–236 (2020). doi:10.1080/17425247.2020.1704730.
For infants and children under 2 years of age with infantile spasms, Acthar is administered IM with a recommended daily dose of 150 U/m2, divided into twice daily IM injections of 75 U/m2, administered over a 2-week period [1]. Because of this different dosage and the requirement for IM administration, SelfJect cannot be used in infants and children under 2 years of age.
Force
There is a lack of data on the minimum force required for injection device use in pediatric patients and estimating the lower range of force for this age group is challenging. However, it can be assumed that smaller and lighter patients may require less force for successful SC injection. Proper training and education on injection device use are essential to ensure safe and effective administration in pediatric patients.
Schneider et al. sought to understand how injection duration affected a user's force when holding an injection device against the skin [28]. In the study, 19 patients (including adolescents [n = 6], adults [n = 6] and elders [n = 7]), 6 caregivers and 7 healthcare professionals simulated three single, high-volume (2 ml) injections of polyethylene glycol of differing viscosities and durations, ranging from short (mean: 7.9 s) to long (mean: 27.1 s). There was a negative correlation between injection duration and mean force applied during injection (Figure 2). Increasing the injection duration from short to long did not increase the number of usage errors, usage difficulties, or other deviations from proper use. Additionally, potential impairments such as age-related conditions or poor dexterity did not influence participants' ability to complete the injections. Adolescent patients exerted the least amount of force during the injections, but all study participants were able to cross the minimum force threshold for successful administration.
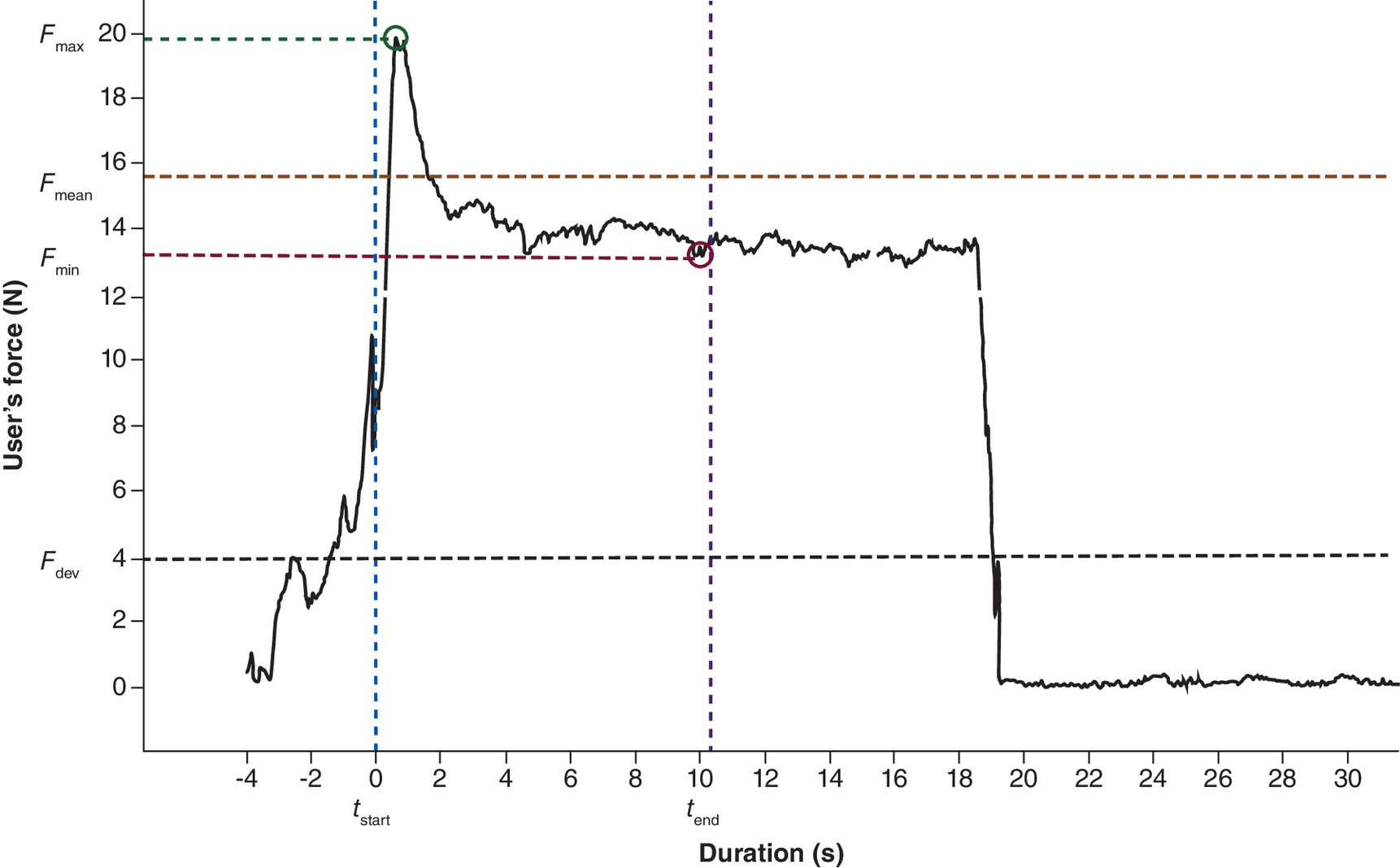
Figure 2. Example of user force measurement using an injection device.
tstart and tend are the time of injection start and end, respectively.
Fmin and Fmax are the minimum and maximum user's force applied during injection, respectively.
Fmean is the mean user's force applied during injection.
Fdev is the user's force threshold specified by the injection device required to complete the injection.
Reproduced with permission from Taylor & Francis Ltd (http://www.tandfonline.com/) from Schneider A, Mueller P, Jordi C et al. Hold the device against the skin: the impact of injection duration on user's force for handheld autoinjectors. Expert Opin. Drug Deliv. 17(2), 225–236 (2020). doi:10.1080/17425247.2020.1704730
F: Force; t: Time.
Regarding SelfJect, the peak axial force to deliver the drug at a rate of 150 ± 5 mm/min (nominal 15 s dispense) is ≤35 N, a force comparable to inserting a plug into an outlet [29], when used at 20 to 25°C. It is unclear whether a child could apply the force required to deliver a full dose. However, even if a patient who is under 18 years of age is prescribed Acthar via SelfJect, an adult 18 years of age and older, such as a caregiver, family member, or healthcare provider (HCP), should use the device and administer the drug to the patient.
Although pediatric patients should not be using SelfJect themselves, it is helpful to consider them as potential future users when investigating the pull force and dexterity required to remove the Tyvek lid and cap. If the same device and packaging are used for and by pediatric populations, then the pull force required to remove the lid and cap of an injection device would be the same as for adults. The minimum pull force would depend on the design of the packaging and the specific product being used. It is recommended to consult the manufacturer's instructions for the specific product to determine if it is safe for a child to open the packaging themselves.
Schneider et al. furthered their study of injection devices by analyzing users' ability to remove the cap of an injection device [30]. In the study, 29 patients (including adolescents [n = 6], adults [n = 11] and elders [n = 12]), 6 caregivers and 7 healthcare professionals were tasked with removing the protective cap of a nonfunctional, mock-up injection device with different target cap removal forces between 25 N and 55 N. All participants were able to effectively remove the injection device caps, regardless of sex, age, dexterity impairments, or professional education. However, the perceived ease of uncapping decreased with higher cap removal force and dexterity impairment, with some participants visibly struggling to remove the caps with the highest cap removal forces.
The tensile force required to remove the SelfJect cap is between 4 N and 35 N, which is either below the range tested in the aforementioned study [30] or at the low end of required force. Given that 6 adolescents and other participants with severe dexterity impairments were able to remove the injection device caps in the study by Schneider et al. [30], it is anticipated that pediatric patients would be able to remove the SelfJect cap, should they be allowed to use SelfJect in the future. Based on the available data, however, there are no specific considerations for the pull force of the protective cap for pediatric patients. Additionally, most injection devices are developed for adults to use, and there is limited research on the ability of children to open product caps themselves.
The pull force required to remove the SelfJect sealed lid from the tray is between 0.25 and 1.5 pounds of force. There is no data to examine whether a child or adolescent could apply the required pull force to open the injector tray.
Potential harms
In a 12-month clinical trial of patients with migraine, Stauffer et al. compared the usability and tolerability of a manually operated, prefilled syringe versus an automated injection device for SC administration of galcanezumab, a monoclonal antibody blocking calcitonin gene-related protein [31]. The most common AE for both the prefilled syringe and injection device was injection-site pain, and there were no significant differences in injection site-related AEs. Among the 179 patients who used both the prefilled syringe and injection device at least once, 29 patients reported at least one injection site-related AE with first prefilled syringe use compared with 38 patients with the injection device. After three injections with the same product (n = 143), 26 patients reported at least one injection site-related AE with the prefilled syringe compared with 28 patients with the injection device. Most of the patients reported the AEs to be mild to moderate, and only 1 patient in each group rated the injection-site pain as severe after the first injection. Although galcanezumab has different physical and chemical properties than Acthar, and therefore the viscosity and injection force may not be the same, this study highlights the injection site-related AEs common to injection devices, such as SelfJect.
Regarding Acthar, commonly reported postmarketing adverse reactions include injection-site reaction, asthenic conditions (including fatigue, malaise, asthenia and lethargy), fluid retention (including peripheral swelling), insomnia, headache and increased blood glucose [1]. For SC injections in general, complications include injection-site reactions, such as pain, burning, discomfort, redness and swelling [32].
Needlestick injury is also a potential concern with any type of injection, particularly if needles must be changed. However, SelfJect has several safeguards to protect against this. With automatic activation of the needle guard, users should not have to place their hand(s) adjacent to or in front of the sharp when used as intended. Also, the needle guard transitions to its locked-out position (safe mode) as the injector is removed from the injection site, prior to transfer to the point of disposal. During this process, the needle is recessed by at least 3.33 mm from the outer surface of the needle guard, thus minimizing accidental access to the sharp.
Finally, if specific injection instructions are not followed, then there is a possibility of incomplete or aborted dose with early device withdrawal. However, in a validation study of 160 untrained participants, including patients, caregivers and HCPs, there were no use errors pertaining to the use task of lifting the device off the injection site [33].
SelfJect review
Table 2 demonstrates patient-related design requirements and the acceptability of SelfJect use for patients under 18 years of age. Certain requirements where the related forces are high to prevent misuse (i.e., forces to override needle guard lockout or forces the device needs to withstand to prevent delivery when in an incorrect position) were excluded as it is assumed that the force capabilities of a user under 18 years of age would be less than or equal to those of an adult. No labeling changes were implemented to improve usability of SelfJect for children or adolescents if they chose to self-inject.
| Device feature | Related requirement per specific PRD | Is the device feature acceptable for patients under 18 years of age? |
|---|---|---|
| Needle depth during delivery | Injector needle insertion depth: The injector shall control needle insertion depth to deliver medication to dermal tissue at a depth of 4–8 mm beneath the outer surface of the skin. Injector drug delivery depth: The injector shall not commence drug delivery until the needle guard is depressed such that the needle protrudes past the needle guard by ≥4.0 mm. | Acceptable: As noted in the needle length and gauge section, using a 4-mm needle in children under 18 years of age carries a risk of intramuscular injection. However, Acthar, whether administered intramuscularly or subcutaneously, has the same pharmacokinetic/pharmacodynamic profile. This implies that Acthar does not pose any additional risks beyond those associated with intramuscular injection. |
| Needle gauge | Injector needle compatibility: The injector shall function with a 0.5 inch 23-gauge thin wall needle (3 bevel) as per all relevant performance requirements. | Acceptable: A 23-gauge needle is appropriate for administration to pediatric patients as per the Centers for Disease Control and Prevention guidance. |
| Dosage | 0.5 ml minimum deliverable volume injector configuration: A configuration of the injector shall deliver 0.5 ml minimum dose volume. 1.0 ml minimum deliverable volume injector configuration: A configuration of the injector shall deliver 1.0 ml minimum dose volume. | Acceptable: 40 U and 80 U doses are appropriate for children over 2 years of age. As outlined in the dosage section, the usual dose of Acthar for children over 2 years of age is 40–80 U given intramuscularly or subcutaneously. |
| Force required – drug delivery | User force limit to inject: The peak axial force to deliver the labeled volume of Acthar drug product at a rate of 150 ± 5 mm/min (nominal 15 s dispense) shall be ≤35N when used at 20–25°C. | Acceptable (as injection should be delivered by an adult): As per the labeling instructions, even if a patient who is under 18 years of age is prescribed SelfJect, the device should be used and drug should be administered to the patient by an adult, such as a caregiver, family member, or HCP. As outlined in the force section, there is limited information available on whether a child could apply the force required to deliver a full dose. |
| Force required – Tyvek removal | Injector tray secured to Tyvek tray lid: The pull force required to remove the sealed lid from the tray shall be 0.25–1.5 lbf. | Acceptable (as device should be accessed by an adult): As per the labeling instructions, even if a patient who is under 18 years of age is prescribed SelfJect, the device should be used and drug should be administered to the patient by an adult, such as a caregiver, family member, or HCP. As outlined in the force section, there was no data obtained on whether a child or adolescent could apply the required pull force to open the injector tray. |
| Force required – cap removal | Cap removal force: The tensile force required to remove the cap shall be 4–35 N. | Acceptable (as injection should be delivered by an adult): As per the labeling instructions, even if a patient who is under 18 years of age is prescribed SelfJect, the device should be used and drug should be administered to the patient by an adult, such as a caregiver, family member, or HCP. As outlined in the force section, it is anticipated that a child would be able to apply sufficient tensile force to remove the cap. |
| Harms – needlestick injury | Hands behind the exposed contaminated sharp: Automatic activation of the needle guard shall not require the user to place their hand(s) adjacent to or in front of the sharp when used as intended. Needle guard safe-mode timing: The injector needle guard shall transition to its locked-out position (safe-mode) as the injector is removed from the injection site, prior to transfer to the point of disposal. Minimizing accidental access to the sharp: After completion of injection, the needle shall be recessed by ≥3.33 mm from the outer surface of the needle guard. | Acceptable (as injection should be delivered by an adult): As per the labeling instructions, even if a patient who is under 18 years of age is prescribed SelfJect, the device should be used and drug should be administered to the patient by an adult, such as a caregiver, family member, or HCP. As outlined in the potential harms section, needlestick injury was identified as a potential harm associated with the device. There is no increased risk of needlestick injury based on the anticipated labeling modifications for SelfJect. |
HCP: Healthcare provider; lbf: Pounds of force; PRD: Product requirement document.
Conclusion
SelfJect is appropriate for use in pediatric patients if administered by an adult (18 years of age and older) caregiver, family member, or HCP. Needle length and gauge are fitting for this age group, although infants and young children are at the highest risk for unintentional IM injection because of smaller skin-to-muscle distances. Dosage is appropriate for children over 2 years of age, but not for infants and children under 2 years of age. Few studies have shown that adolescents can achieve the minimum force threshold to complete self-injections and remove an injection device cap [28,30], but there is a lack of data pertaining to force requirements of injection devices in children. Aside from the potential adverse reactions from Acthar itself, injection site-related AEs are the main concern with SelfJect use.
Future perspective
Future studies assessing use and handling of the SelfJect device by pediatric patients (less than 18 years of age) will be informative, as SelfJect is currently only appropriate for use in pediatric patients if administered by an adult. Additionally, future research is needed to incorporate SelfJect dosages appropriate for infants and children under 2 years of age with infantile spasms.
Summary points
•
A new single-dose prefilled injector (SelfJect™) has recently been developed as a combination product of Acthar in a prefilled syringe and a single-dose drug delivery device, which was designed to improve the speed and ease of delivery.
•
This narrative review assessed whether SelfJect is suitable for use in pediatric patients with inflammatory disorders.
•
Although designed for subcutaneous delivery of Acthar, unintentional intramuscular injection via SelfJect is possible in infants and young children due to small skin-to-muscle distances; however, Acthar is bioequivalent when administered intramuscularly or subcutaneously.
•
The needle gauge of SelfJect is acceptable for use in pediatric patients and SelfJect dosages (0.5 ml [40 U] or 1.0 ml [80 U]) are only appropriate for children over 2 years of age.
•
A caregiver, family member, or healthcare provider 18 years of age and older should administer SelfJect to pediatric patients.
•
Additional studies are needed to confirm whether pediatric patients can apply the required forces to open the injector tray, remove the SelfJect cap and deliver a full dose of medication.
•
SelfJect includes safety features such as automatic needle guard activation and ensuring the needle is retracted by at least 3.33 mm to minimize accidental access to the sharp.
•
Injection-site reactions are a potential adverse event with SelfJect use, as with other subcutaneous injections.
Author contributions
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship, take responsibility for integrity of the work, and have given final approval to the version to be published. All authors made a significant contribution to the work reported; took part in drafting, revising, or critically reviewing the article; and have agreed on the journal to which the article has been submitted.
Financial disclosure
J Purcell and S Elliott are employees of Mallinckrodt Pharmaceuticals. Sponsorship for this study, including medical writing and editorial support, was funded by Mallinckrodt Pharmaceuticals (NJ, USA). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
Medical writing and editorial support were provided by A Jacobson from MedLogix Communications, LLC, a Citrus Health Group, Inc., company (IL, USA), and were funded by Mallinckrodt Pharmaceuticals.
Ethical conduct of research
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Food and Drug Administration. Acthar® Gel, Prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/008372s074lbl.pdf (2024).
2.
Hladunewich MA, Cattran D, Beck LH et al. A pilot study to determine the dose and effectiveness of adrenocorticotrophic hormone (H.P. Acthar® Gel) in nephrotic syndrome due to idiopathic membranous nephropathy. Nephrol. Dial. Transplant. 29(8), 1570–1577 (2014).
3.
Baram TZ, Mitchell WG, Tournay A, Snead OC, Hanson RA, Horton EJ. High-dose corticotropin (ACTH) versus prednisone for infantile spasms: a prospective, randomized, blinded study. Pediatrics 97(3), 375–379 (1996).
4.
Chugani HT, Kumar A. Neuroinflammation in children with infantile spasms: a prospective study before and after treatment with Acthar Gel (repository corticotropin injection). J. Child Neurol. 35(12), 808–812 (2020).
5.
Madan A, Mijovic-Das S, Stankovic A, Teehan G, Milward AS, Khastgir A. Acthar gel in the treatment of nephrotic syndrome: a multicenter retrospective case series. BMC Nephrol. 17, 37 (2016).
6.
Bomback AS, Canetta PA, Beck LH Jr, Ayalon R, Radhakrishnan J, Appel GB. Treatment of resistant glomerular diseases with adrenocorticotropic hormone gel: a prospective trial. Am. J. Nephrol. 36(1), 58–67 (2012).
7.
Watson MJ. Membranous glomerulopathy and treatment with Acthar®: a case study. Int. J. Nephrol. Renovasc. Dis. 6, 229–232 (2013).
8.
Mallinckrodt Pharmaceuticals. Acthar® Gel, Patient support. https://acthar.com/Static/pdf/PSR_Step_By_Step_Injection_Guide_English.pdf (2021).
9.
Zuberi Z, Sauli E, Cun L et al. Insulin-delivery methods for children and adolescents with type 1 diabetes. Ther. Adv. Endocrinol. Metab. 11, 2042018820906016 (2020).
10.
Wysham CH, Rosenstock J, Vetter ML, Wang H, Hardy E, Iqbal N. Further improvement in glycemic control after switching from exenatide two times per day to exenatide once-weekly autoinjected suspension in patients with type 2 diabetes: 52-week results from the DURATION-NEO-1 study. BMJ Open Diabetes Res. Care. 8(1), e000773 (2020).
11.
Tischer B, Mehl A. Patients' and nurses' preferences for autoinjectors for rheumatoid arthritis: results of a European survey. Patient Prefer. Adherence. 12, 1413–1424 (2018).
12.
Dashiell-Aje E, Harding G, Pascoe K, DeVries J, Berry P, Ramachandran S. Patient evaluation of satisfaction and outcomes with an autoinjector for self-administration of subcutaneous belimumab in patients with systemic lupus erythematosus. Patient. 11(1), 119–129 (2018).
13.
Cohen YZ, Zhang X, Xia B et al. Pharmacokinetics of subcutaneous dupilumab injection with an autoinjector device or prefilled syringe. Clin. Pharmacol. Drug Dev. 11(5), 675–681 (2022).
14.
Dostal P, Taubel J, Lorch U, Aggarwal V, York T. The reliability of auto-injectors in clinical use: a systematic review. Cureus. 15(7), e41601 (2023).
15.
Sicherer SH, Simons FER, Mahr TA et al. Epinephrine for first-aid management of anaphylaxis. Pediatrics 139(3), e20164006 (2017).
16.
Frew AJ. What are the ‘ideal’ features of an adrenaline (epinephrine) auto-injector in the treatment of anaphylaxis? Allergy 66(1), 15–24 (2011).
17.
Saitoh A, Aizawa Y, Sato I, Hirano H, Sakai T, Mori M. Skin thickness in young infants and adolescents: applications for intradermal vaccination. Vaccine 33(29), 3384–3391 (2015).
• This study used ultrasound echography to measure skin thickness in Japanese infants aged 2 months and adolescents aged 13–15 years. Skin thickness increased from age 2 months to 13–15 years; however, no consistent trend was observed based on measurement site, gender, or age. Findings suggested that a needle length of less than 1.2 mm is appropriate for infants and children, indicating a need for special devices with shorter needles for this age group.
18.
Van Mulder TJS, Van Nuffel D, Demolder M et al. Skin thickness measurements for optimal intradermal injections in children. Vaccine 38(4), 763–768 (2020).
• Epidermal and dermal thickness at the proximal ventral and dorsal forearm and deltoid region in children aged 8 weeks to 18 years were assessed. Significant differences in skin thickness at these areas were observed based on age and BMI.
19.
Lo Presti D, Ingegnosi C, Strauss K. Skin and subcutaneous thickness at injecting sites in children with diabetes: ultrasound findings and recommendations for giving injection. Pediatr. Diabetes. 13(7), 525–533 (2012).
• Children with Type 1 diabetes were divided into three age groups; ultrasound was used to measure skin and subcutaneous tissue thickness at injection sites. Skin thickness varied based on age and body site, informing evidence-based needle choices for insulin injections.
20.
Smith CP, Sargent MA, Wilson BP, Price DA. Subcutaneous or intramuscular insulin injections. Arch. Dis. Child. 66(7), 879–882 (1991).
21.
Polak M, Beregszaszi M, Belarbi N et al. Subcutaneous or intramuscular injections of insulin in children. Are we injecting where we think we are? Diabetes Care 19(12), 1434–1436 (1996).
22.
Tubiana-Rufi N, Belarbi N, Du Pasquier-Fediaevsky L et al. Short needles (8 mm) reduce the risk of intramuscular injections in children with type 1 diabetes. Diabetes Care 22(10), 1621–1625 (1999).
23.
Birkebaek NH, Solvig J, Hansen B, Jorgensen C, Smedegaard J, Christiansen JS. A 4-mm needle reduces the risk of intramuscular injections without increasing backflow to skin surface in lean diabetic children and adults. Diabetes Care 31(9), e65 (2008).
24.
Hofman PL, Lawton SA, Peart JM et al. An angled insertion technique using 6-mm needles markedly reduces the risk of intramuscular injections in children and adolescents. Diabet. Med. 24(12), 1400–1405 (2007).
25.
Hofman PL, Derraik JG, Pinto TE et al. Defining the ideal injection techniques when using 5-mm needles in children and adults. Diabetes Care 33(9), 1940–1944 (2010).
26.
Brod SA, Morales MM. Bio-equivalence of IM and SQ H.P. Acthar Gel. Biomed. Pharmacother. 63(4), 251–253 (2009).
27.
Kroger A, Bahta L, Long S, Sanchez P. Centers for Disease Control and Prevention's Advisory Committee on Immunization Practices. General best practice guidelines for immunization. https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/index.html (2023).
28.
Schneider A, Mueller P, Jordi C et al. Hold the device against the skin: the impact of injection duration on user's force for handheld autoinjectors. Expert Opin. Drug Deliv. 17(2), 225–236 (2020).
• The effects of injection duration on users' ability to apply injections while holding an injector device against the skin at the injection site were assessed. Participants were able to successfully administer long-duration injections using handheld autoinjectors, regardless of their health conditions or impairments.
29.
Smaby N, Johanson ME, Baker B, Kenney DE, Murray WM, Hentz VR. Identification of key pinch forces required to complete functional tasks. J. Rehabil. Res. Dev. 41(2), 215–224 (2004).
30.
Schneider A, Richard P, Mueller P, Jordi C, Yovanoff M, Lange J. User-centric approach to specifying technical attributes of drug delivery devices: empirical study of autoinjector-cap removal forces. Patient Prefer. Adherence. 15, 159–168 (2021).
• Participants tested the removal of protective caps from non-functional autoinjector devices with varying cap-removal forces. This study showed that increasing the cap-removal force and dexterity impairments made decapping more difficult.
31.
Stauffer VL, Sides R, Lanteri-Minet M et al. Comparison between prefilled syringe and autoinjector devices on patient-reported experiences and pharmacokinetics in galcanezumab studies. Patient Prefer. Adherence. 12, 1785–1795 (2018).
• Patients with migraine compared the usability of an autoinjector with that of a prefilled syringe. The majority of patients had positive experiences with the autoinjector. No notable differences were observed in ease of use or tolerability between the prefilled syringe and autoinjector during the first self-administration.
32.
Bolge SC, Goren A, Tandon N. Reasons for discontinuation of subcutaneous biologic therapy in the treatment of rheumatoid arthritis: a patient perspective. Patient Prefer. Adherence. 9, 121–131 (2015).
33.
Linnane A, Lau M, Miranda P, Elliott S. Formative and validation human factors studies of a new disposable prefilled injection device for subcutaneous delivery of acthar gel (repository corticotropin injection). Expert Opin. Drug Deliv. 21(8), 1263–1278 (2024).
Information & Authors
Information
Published In
Copyright
© 2024 Mallinckrodt Pharmaceuticals. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 August 2024
Accepted: 8 October 2024
Published online: 25 October 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Clinical assessment of the potential use of a novel single-dose prefilled injection device for the administration of Acthar Gel in children: a narrative review. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0132
Export citation
Select the citation format you wish to export for this article or chapter.