A novel injection device to administer repository corticotropin injection for inflammatory disease treatment: findings from a market research study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The goal of this market research study was to determine the usability of a single-dose prefilled injector (SelfJect™) for administration of Acthar® Gel (manufactured by Mallinckrodt Pharmaceuticals, UK) in patients with inflammatory diseases by obtaining feedback from patient and practitioner user groups in the US. Materials & methods: Patients and healthcare professionals (HCPs) representing relevant therapeutic areas were enrolled in the study between February and March 2021. SelfJect was mailed to patients and HCPs prior to 90-min virtual video-recorded focus group sessions and 60-min 1:1 virtual interviews, respectively. Patients completed an online assignment prior to the group session, which included instructions on how to use SelfJect and questions about their initial reaction while handling the device. HCPs were instructed to not open the package until the interview. Feedback from patients and HCPs were captured by open-ended questions and ranking scales. Results: Twelve patients and 42 HCPs participated in the study. Most patients (9/12 [75%]) and HCPs (38/42 [90%]) had experience with injectable medications, and 7/12 (58%) and 30/42 [71%] had experience with Acthar injections, respectively. Most patients and HCPs reported that key benefits of SelfJect were accurate dose delivery and ease of use, including the ergonomic handle and elimination of drawing Acthar from a vial into a syringe. Patients expressed some concerns about storage and disposal, but the need to store SelfJect would not deter them from using it. Most patients (9/12 [75%]) felt prepared to inject Acthar after reviewing the instructions. HCPs anticipated that 75% to 100% of patients would benefit switching from the vial to SelfJect. Conclusion: All participants expressed positive perceptions for SelfJect including easy use, few preparation steps and potential reduced anxiety due to needle phobia. These attributes may help treatment adherence for patients and caregivers.
Shareable abstract
A market research study of the SelfJect™ single-dose prefilled injector for Acthar® Gel showed that patients with inflammatory diseases and healthcare professionals had positive perceptions. Ease of use and decreased needle-related anxiety may help improve treatment adherence.
Plain language summary
A market research study of a new injection device for Acthar® Gel
What is this article about?
Acthar® Gel is used to treat inflammatory diseases. The medication is administered by injection into the muscle or under the skin. Patients with a limited range of hand motion or fear of needles may have difficulty injecting themselves. SelfJect™ was developed to make self-injection easier. SelfJect is a device that contains Acthar in a prefilled syringe. This device includes a hidden needle to prevent needlestick injury, a handle to improve grip and an audible click that indicates administration of a complete dose. A study was conducted to get feedback from patients with inflammatory diseases, doctors and nurses on the usability of SelfJect. Patients were mailed SelfJect devices and instructions for its use. They were asked to complete an online survey about their reactions to using SelfJect. Patients also participated in virtual focus group sessions. Doctors and nurses were mailed SelfJect but were instructed to not open the package until their virtual interview.
What were the results?
Twelve patients and 42 doctors and nurses participated in the study. Most participants reported that SelfJect was easy to use. The features they liked most were the handle and not needing to fill a syringe with Acthar from a vial. Most patients felt prepared to inject Acthar after reading the instructions. Most doctors and nurses thought that patients would benefit from using SelfJect.
What do the results mean?
The easy use of SelfJect makes it more likely that patients will take their medication as prescribed.
Acthar® Gel (repository corticotropin injection; manufactured by Mallinckrodt Pharmaceuticals, UK) is a naturally sourced mixture of purified adrenocorticotropic hormone analogues and other pituitary peptides that has anti-inflammatory and immunomodulatory effects through activation of melanocortin receptors [1,2]. It is indicated for the treatment of several autoimmune disorders and inflammatory conditions including acute exacerbations of multiple sclerosis (MS), as a short-term adjunctive therapy of rheumatic disorders (e.g., rheumatoid arthritis [RA], psoriatic arthritis, ankylosing spondylitis), exacerbation or as maintenance therapy in select cases of systemic lupus erythematosus (SLE) and dermatomyositis/polymyositis, severe acute and chronic allergic and inflammatory processes in ophthalmic disease (e.g., keratitis, iritis, optic neuritis), symptomatic sarcoidosis and proteinuria in nephrotic syndrome [3].
Acthar is administered intramuscularly or subcutaneously and is available as a multidose vial for self-injection [3]. Dosing is individualized depending on the disease and medical condition of the patient and may require use as a maintenance therapy in some indications [3]. Barriers to self-injection of drugs include needle phobia, lack of confidence relating to the injection process, pain linked to swelling in the joints and limited manual dexterity [4,5]. These issues complicate self-injection and may contribute to poor medication adherence. User-friendly prefilled injection devices may overcome these challenges and provide additional benefits including easy self-administration and dosage accuracy [6]. For patients with visual impairment, particularly those with ophthalmic disease, an audible click that indicates completion of drug delivery is beneficial. Self-administration with a prefilled injection device may also decrease the travel time and expense to receive an injection in the clinic [6,7]. This has been shown to influence patients with RA who prefer to self-administer their medication [7]. Providing these various design benefits to meet patient needs may improve adherence to treatment and long-term treatment outcomes [6,8].
The single-dose prefilled injector (SelfJect™) for administration of Acthar was developed as a combination product of Acthar in a prefilled syringe and a single-dose drug delivery device. SelfJect is a manually operated, single-dose injector with a passive sharps protection feature to prevent needlestick injury that was designed to assist the user visually and audibly with a syringe prefilled with Acthar for subcutaneous injection in a home or clinical environment. SelfJect aims to address patients' unmet needs with features such as a push-down delivery system, a top ergonomic handle to support impaired dexterity through improved gripping, a viewing window to check medication visually and monitor injection progress, a hidden needle to reduce needle phobia and inadvertent needlestick injuries and audible clicks at the finish to give patients confidence that a full dose has been administered.
This market research study aimed to determine the usability of SelfJect in patients with inflammatory diseases in the US across patient and practitioner user groups. This study explored perspectives and preferences from patients and healthcare professionals (HCPs) regarding self-injection, such as interest in using SelfJect, feedback on perceived benefits and drawbacks of SelfJect use, training/education needs, impact of SelfJect on patient adherence to Acthar treatment and the logistics and barriers to its use.
Methods
Participants
Eligible patients (naive and experienced) were at least 18 years of age across 5 groups representing different disease states: MS, rheumatology (RA and SLE), ophthalmology, pulmonology and nephrology. Eligible HCPs included physicians, physician assistants, nurse practitioners and registered nurses in rheumatology, nephrology, pulmonology, ophthalmology and neurology. HCPs solely responsible for prescribing treatments to patients in their practice were screened to ensure that they have been in practice between 2 and 35 years and were currently in full-time practice, with >40% of their time treating/seeing patients if in an academic setting or >60% if practicing in a non-teaching hospital. HCPs who work with the treating physician were screened to ensure ≥1 year of experience. Other key screening criteria included: (i) awareness of Acthar or willingness to prescribe Acthar, (ii) primary setting is an office-based practice and (iii) located in the US except in Massachusetts, Minnesota or Vermont, as these states have legislation that prohibits HCPs from participating in or receiving incentives for market research.
Since this was a non-interventional market research study, prior approval of the protocol by an ethics committee was not required. The study was conducted in accordance with relevant market research guidelines, including the obtaining of informed consent and adherence to ethical reporting standards. All participants were provided written informed consent prior to participation in this study. Patients were compensated with a $150 eGift card and HCPs received a $450 honorarium for participating in the study.
Study design
An overview of the study design is provided in Figure 1. The patient study took place between 23 February 2021 and 9 March 2021. Prior to a 90-min virtual video-recorded focus group, patients were mailed a package containing SelfJect and a homework assignment to complete. The device was for demonstration purposes only and did not contain any needle or medication. Patients were instructed that the online homework would take 15 min to complete and included a brief description of Acthar, instructions on how to use the device and 9 questions relating to the patient's history of Acthar use, initial reactions and device logo ratings.

Figure 1. Study design overview.
aThe single-dose prefilled injector (SelfJect™) for administration of Acthar® Gel was mailed to the healthcare professionals (HCPs), and they were instructed not to open the box until their interview.
Patients reviewed the full 18-page Instructions for Use and the Quick Start Guide, which included color coding for the two doses, 40 USP U/0.5 ml and 80 USP U/ml of Acthar. Patient impressions were captured by both open-ended questions (e.g., lists of benefits and drawbacks) and ranking scales including possible benefits of using a patient-controlled injector (e.g., hidden needle, absence of separate syringes and vials). Patient focus groups consisted of two to four participants representing a mix of conditions. One group was comprised of Acthar nonusers and three groups were comprised of users. Patients were prompted by a moderator to provide feedback during the focus group. Compensation for participation was provided upon return of the device and homework assignments.
The HCP study took place between 9 February 2021 and 12 March 2021. HCPs participated in 60-min 1:1 virtual (webcam) interviews. Prior to the interview, SelfJect was mailed to the HCPs, and they were instructed to not open the box until the interview. HCPs were first given a 5-min introduction to orient them for the 1:1 interview and then asked a series of questions to gain an unaided review of perceived advantages and challenges of the device. Next, their likelihood of prescribing the device versus the syringe for different patient groups was evaluated. The honorarium for participation was provided upon return of the device.
Results
Patient & HCP characteristics
A total of 12 patients participated in the study (Table 1). The most represented patient groups were those with MS (n = 3) and RA (n = 3). Nine (75%) patients had experience with injectable medications, and seven (58%) had experience with Acthar injections. A total of 42 HCPs participated in the study, and the largest practitioner group was rheumatology (n = 11) (Table 2).
| Characteristics | Total (n = 12) |
|---|---|
| Sex, n (%) Male Female | 4 (33%) 8 (67%) |
| Diagnosis, n (%) Rheumatoid arthritis Multiple sclerosis Sarcoidosis Idiopathic membranous nephropathy Follicular glomerulosclerosis IgA nephropathy Ophthalmologic conditions† | 3 (25%) 3 (25%) 2 (17%) 1 (8%) 1 (8%) 1 (8%) 1 (8%) |
| Acthar use history, n (%) Experienced Naive | 7 (58%) 5 (42%) |
| Injectable medication use history, n (%) Experienced Naive | 9 (75%) 3 (25%) |
†
One patient had keratitis, iritis, iridocyclitis, diffuse posterior uveitis and choroiditis, optic neuritis and chorioretinitis.
IgA: Immunoglobulin A.
| Characteristics | Total (n = 42) |
|---|---|
| Therapeutic area, n (%) Rheumatology Nephrology Pulmonology Ophthalmology Neurology | 11 (26) 9 (21) 9 (21) 6 (14) 7 (17) |
| Acthar user status, n (%) Experienced Naive | 30 (71) 12 (29) |
| Administer injectable medications, n (%) Routinely Occasionally Never | 32 (76) 6 (14) 4 (10) |
| Train patients to administer in office, n (%) Routinely Occasionally Never | 28 (67) 8 (19) 6 (14) |
| Train patients to administer at home, n (%) Routinely Occasionally Never | 21 (50) 10 (24) 11 (26) |
| Train patients to administer virtually, n (%) Routinely Occasionally Never | 17 (40) 13 (31) 12 (29) |
| Answer patients' questions regarding injectable medications, n (%) Routinely Occasionally Never | 38 (90) 4 (10) 0 |
Patients: device assessment
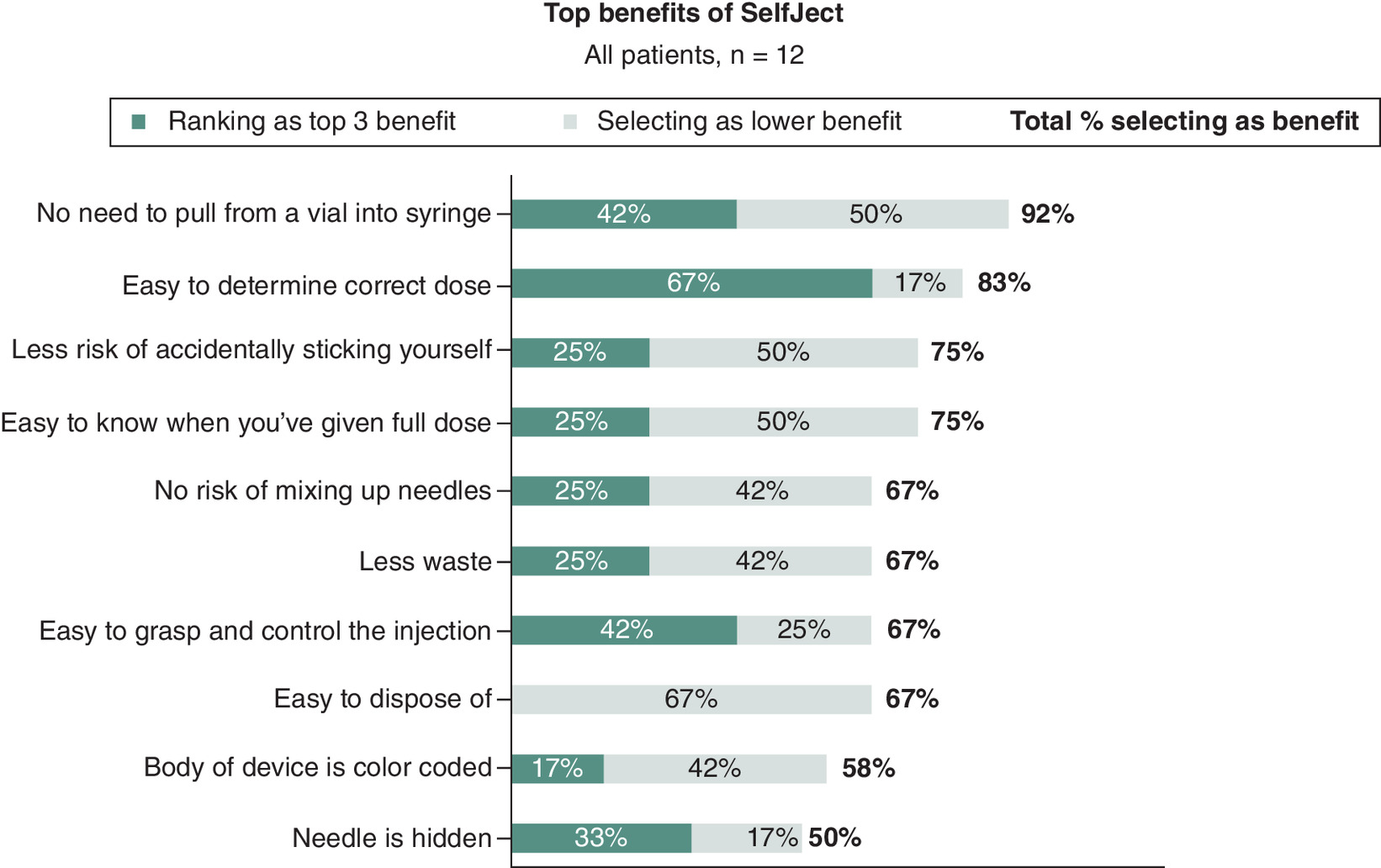
Patients reported multiple benefits of SelfJect including a simpler self-injection process due to the device being prefilled with the correct dose and the ease of holding a large round plunger. Another advantage includes a hidden needle, which prevents accidental needlestick injury and alleviates needle phobia. Moreover, patients who require assistance with injections believed they would have independence self-injecting with the device. While nearly all (11/12 [92%]) patients appreciated the ease of not needing to draw Acthar from a vial, ensuring delivery of the correct dose was reported as the most important benefit (Figure 2). The hidden needle was the least selected benefit (6/12 [50%] patients), although it was considered a significant benefit for those who selected it. Patients perceived slight drawbacks to the design including the need for refrigeration storage, inability to warm the device with their hands and resemblance of a toy, which raised concerns about children's safety.
Patients: logistical considerations
Many patients raised concerns for storage and disposal of the device. Those who currently inject Acthar multiple times per week reported that they may not have room in their refrigerator. These patients raised concerns about having to purchase a separate refrigerator to be able to use this device. Both Acthar-experienced and Acthar-naive patients estimated they could store 8 to 10 doses (e.g., 4–5 weeks supply at 80 U twice per week) at one-time without having to purchase a separate refrigerator. Users who currently inject ≤two-times weekly were less concerned about storage but acknowledged that it may be challenging. Acthar-naive patients were less concerned about storage. Both Acthar-experienced and Acthar-naive patients reported that the need for storage would not discourage them from using SelfJect. They were more concerned about how to properly dispose of the devices, owing to their much larger size, than having sufficient refrigerator space to store it. Patients felt that a standard sharps container would not be able to fit more than 5 SelfJect devices and were unsure what to do with a full sharps container (Table 3, Q1). Patients who have never self-injected medication were not aware of where to go or who to ask about disposing sharps and those who have had to dispose of sharps containers in the past had various unsatisfactory experiences. Patients were not concerned with traveling with the device (Table 3, Q2).
| Quote ID and topic | Quote |
|---|---|
| Patient feedback | |
| Q1/Disposal | “You might need a sharps dumpster to get rid of that.” – Rheumatology patient |
| Q2/Storage | “This would be great [for traveling]. It's a lot better, a lot easier to transport. You just grab these, put them in a cooler, and you can hit the road.” – Ophthalmology patient |
| Q3/Design | “Super easy to use. I like that it locks when the injection is done, so you know you've gotten all the medicine and won't get poked by the needle!” – Neurology patient |
| Q4/Design | “I would definitely prefer to use this over the needle they give us now – it's just so much easier and quicker!” – Pulmonology patient |
| Practitioner feedback | |
| Q5/Design | “This is so easy and simple to inject! It's easy to hold…you hear the click, and you know it's done. The window lets you see [Acthar] on both sides if I wasn't sure all the medication was administered.” – Pulmonology healthcare professional, Acthar user |
| Q6/Drug delivery | “90% of my Acthar patients will benefit from this injector. It's only those patients who are hesitant to switch to something new and doing very well on the vial that I won't offer it.” – Pulmonology healthcare professional, Acthar user |
| Q7/Dosing | “I start patients on 80 U every other week and go to 40 U monthly, after response. I have not used any other doses. I expect I will have to go back to [the vial] for any other dose, as you cannot use a partial dose on the injector. Therefore, I would like them to stay on vial if they're using atypical dosing.” – Nephrology healthcare professional, Acthar user |
Nearly all interviewed patients had experience using a specialty pharmacy. Some reported that it is challenging to get the initial prescription filled because of lack of coverage or completing approval paperwork. Once established with a specialty pharmacy, experiences were generally positive. Features the patients reported as positive include reminder phone calls and shipments arriving on time and refrigerated, though some were concerned about coordinating shipments. All patients expect that their specialty pharmacy would not accommodate their storage needs by breaking up shipments into more frequent, smaller sizes. Most believe that they will need to figure out how to store large shipments of SelfJect.
Patients: training support needs & information seeking behavior
Most patients (9/12 [75%]) felt prepared to inject based on the Instructions for Use and the Quick Start Guide, and 3/12 (25%) patients felt neutral about their preparedness (Figure 3A). They recommended fewer words and more graphic/infographic depictions in the Quick Start Guide. Eight patients (67%) reported that they would feel more comfortable self-injecting with SelfJect if provided an online injection training video (Figure 3B). One patient suggested including a QR code within the written instructions that links to the training video.

Figure 3. Patient preparedness from SelfJect instructions.
(A) Patient preparedness and (B) additional resource requests after reading instructions for administration of Acthar via SelfJect.
While a minority of patients reported wanting in-person training from a doctor or nurse prior to their first self-injection, no current user felt in-person training would be necessary to feel comfortable with the device (Figure 3B). Overall, the type and amount of support needed to feel comfortable prior to using SelfJect depended on whether the patient had previously used an injectable medication. Acthar-naive patients expressed hesitation around self-injection, especially those who have never used an injectable medication before.
Patients utilized a variety of sources for researching their condition (Figure 4). Some of those sources were more trusted than others, and HCPs were considered the most trustworthy sources. Patients cited manufacturer websites as especially useful resources. Patients were aware that manufacturer websites may be trying to market their medication but were also providing reliable information on safety, cost-saving programs and nurse support lines. Nearly all patients reported that social media is not a trusted source of information and that negative experiences are more likely to be posted than positive ones. However, some patients have found closed, condition-specific groups exceptionally useful for support.
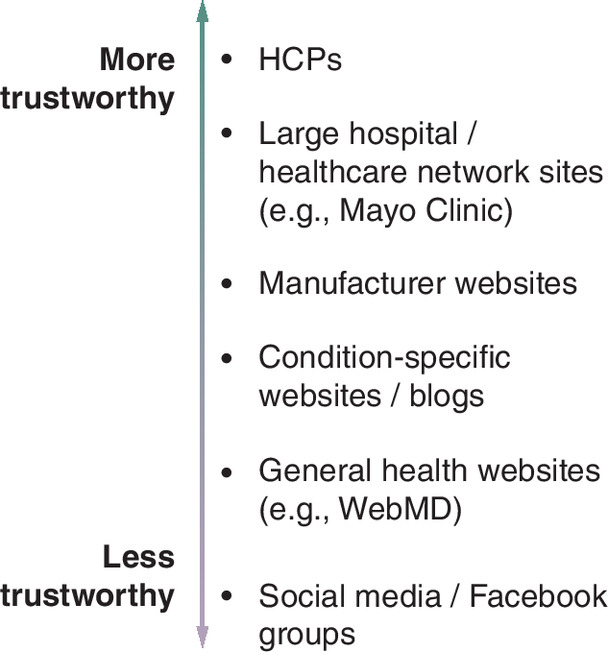
Figure 4. Sources of information used and their relative trustworthiness.
HCP: Healthcare professional.
Additional patient perceptions
Most patients (11/12 [92%]) agreed that SelfJect ensures proper injection of the medication and felt the device would be easy to use (Figure 5, Q3). Acthar-experienced patients reported feeling comfortable using the device, and most reported that they would need little to no instruction but would appreciate knowing that instructional resources were available (Table 3). Most patients reported they would switch if SelfJect was available due to the convenience and ease of self-administering Acthar with the device (Table 3, Q4). Acthar-naive patients were more hesitant, citing concerns with cost, efficacy of Acthar for their condition and whether their HCP would recommend it. These patients found the Quick Start Guide and Instructions for Use helpful, but they would want additional resources, such as an instructional video, to feel comfortable self-injecting.

HCP perceptions
Reactions to SelfJect attributes were positive across HCP specialty and role. HCPs reported that the top benefits of SelfJect included the ease of use and accurate dose administration. They viewed SelfJect as an improvement over vial/syringe administration (Table 3, Q5). The ergonomic top handle design and push-down feature is ideal for patients with dexterity and motion issues; however, the resistance from the push-down may be difficult for frail patients. The combination of the viewing window and an audible click gave HCPs confidence the full dose would be administered. Moreover, the hidden needle is anticipated to ease needle anxiety and needle phobia. Overall, the benefits have potential to increase treatment compliance and adherence.
HCPs expected that training procedures with SelfJect would be the same as those for vial administration (e.g., training and first dose administered would take place in office); however, training will take less time and be simpler for patients. Additional training resources include a demonstration injector, take-home pamphlet with step-by-step guide with text and graphics and a training video. Samples of SelfJect would be beneficial, particularly if waiting for insurance approval. HCPs anticipate prescribing SelfJect for 75% to 100% of patients currently prescribed Acthar. Several HCPs may wait until a current patient requests SelfJect, especially if patients have no complaints and are doing well with the vial and syringe (Table 3, Q6). Though rare, patients who need to titrate Acthar may not be prescribed SelfJect, specifically if doses other than 40 U and 80 U are required (Table 3, Q7).
Additional considerations for prescribing SelfJect include the availability of insurance coverage, cost concerns and insurance hurdles such as prior authorizations. For example, if vials are approved more quickly for MS relapse, neurologists are unlikely to wait for insurance approval for SelfJect. Some physicians will not offer self-injection treatment for patients who rely on caretakers or nursing home staff. The traditional vial and syringe route of administration may be challenging for some patients with dexterity issues and may hinder treatment adherence. Such barriers could be mitigated by demonstration to payers of improved treatment compliance and adherence with SelfJect.
Discussion
Patient involvement in designing medication delivery devices may support higher medication adherence and subsequently impact treatment outcomes [6,8,9]. Early identification of patient fear or misconceptions of therapy could aid in treatment decision-making and provide opportunities for education and early intervention. Nonadherence to therapy may be driven by difficulties patients face while taking their medication, such as dexterity issues or needle phobia. For patients with reduced hand dexterity, the usability of self-injection devices directly impacts adherence to treatment [4,5]. SelfJect was designed with enhanced features to address specific challenges associated with self-injection among patients with impaired dexterity, vision and coordination, as well as to address commonly reported concerns by patients regarding the self-injection process. Although storage of SelfJect was a concern for patients, weekly shipments with partial fills could help to alleviate concerns about sufficient refrigerator space. Patients reported that disposal of the devices was more challenging than storage. The manufacturer providing a large sharps container and guidance on locating an appropriate disposal location are feasible solutions.
Providing patients device training and teaching routines for self-injection may be useful strategies to reduce anxiety and improve treatment adherence [9,10]. Patients in the current study indicated visual training tools, such as a training video, as beneficial to improving their confidence in using SelfJect to self-administer Acthar. Similarly, HCPs indicated that additional training resources, such as a demonstration injector and a training video, would assist training prior to the first self-injection. Coping with chronic illness and the burden of managing treatment on a daily basis can overwhelm patients and their caregivers [11]. Peer support groups can provide a sense of purpose, connectedness and experiential knowledge to help others manage the same condition [12]. Group teaching and sharing experiences is a strategic educational technique in a nonformal setting [13], but the clinical value peer support groups provide is difficult to quantify [12]. Patients surveyed in the current study reported that closed, condition-specific groups on social media were exceptionally useful for support. These support groups can provide appropriate resources, such as links to training videos and instructional materials that may aid patients in self-injecting their medication.
Needle phobia is common and associated with all medical procedures, including venipunctures, which underscores the need to address needle phobia to improve the patient experience and ultimately medication adherence [14]. In the current study, six (50%) patients indicated the hidden needle as a significant benefit indicating that needle phobia and anxiety surrounding self-injection is important to address in the design of self-injecting devices. A separate study reviewing the prevalence of needle phobia in adult patients with chronic disease found needle phobia is common in this population, with an estimated prevalence of up to 80%, depending on disease [15]. Overcoming this issue would likely reduce patient distress, improve treatment adherence and prevent resulting complications. The incidence of errors associated with injectable medications is higher than with other formulations and the number of manipulations required to prepare the drug increase the risk of errors [16]. Syringe-to-vial manipulation of medication to prepare for administration increases the risk of error and may result in patient harm or insufficient dosing [16]. In the current study, nearly all patients appreciated not needing to draw Acthar from a vial and having the correct dose prepared for them, thus decreasing the number of manipulations or steps involved in the process of self-injecting. In addition to ensuring the correct dose is prepared in the prefilled syringe, reducing the number of steps required to self-administer Acthar simplified the process and increased patient confidence with self-administration.
Limitations
Prior experience with other injected medication may have impacted the patients' perceptions and satisfaction with the device. The study recruited only 12 patients and may not be representative of the diverse patient population for which Acthar is indicated. Traditionally, these types of studies are conducted in person. Due to the COVID-19 pandemic, this market research study was performed virtually; however, a virtual platform enabled flexibility for HCPs' schedules and reduced the burden on patients with mobility issues.
Future directions
If a larger study is conducted in the future, it would be interesting to determine whether there is a difference in patient or HCP perceptions of SelfJect in different demographic groups or diseases that are treated with Acthar.
Conclusion
Patients with inflammatory diseases in the US who were experienced with Acthar self-injection with vial and syringe generally reported feeling confident about SelfJect after reviewing written training materials and handling the device. HCPs and patients alike were generally positive about the potential for SelfJect to provide patients independence in self-injecting, reduce needle phobia and ensure proper dose delivery. Its ease of use coupled with few preparation steps for injection and decreased anxiety relating to needles are key attributes that may improve treatment compliance. Concerns with SelfJect that were identified in this market research study included insurance coverage, cost and logistical (storage and disposal) issues. HCPs are highly trusted by patients as a valued source of information on how to best manage their care and in providing support to aid patients' decision-making regarding commencing and adhering to Acthar treatment.
Summary points
•
Acthar® Gel is indicated for the treatment of several autoimmune disorders and inflammatory conditions and is currently available as a multidose vial for self-injection.
•
To circumvent the barriers associated with self-injection of drugs, including needle phobia and limited manual dexterity in some patients, the single-dose prefilled injector (SelfJect™) for administration of Acthar was developed as a combination product of Acthar in a prefilled syringe and a single-dose drug delivery device.
•
SelfJect addressed patients' unmet needs with several features such as a push-down delivery system, a top ergonomic handle to support impaired dexterity through improved gripping, a hidden needle to reduce needle phobia and inadvertent needlestick injuries and audible clicks at the finish to give patients confidence that a full dose has been administered.
•
The objective of this market research study was to determine the usability of SelfJect in patients with inflammatory diseases across patient and practitioner user groups in the US.
•
Most patients felt prepared to inject Acthar after reading the instructions, and most healthcare professionals thought that patients would benefit switching from the vial to SelfJect.
•
Patients and practitioner users provided positive feedback for SelfJect and viewed it as an improvement over vial/syringe administration in terms of ease of use with few preparation steps and potential reduction of anxiety in patients with needle phobia.
•
SelfJect's ease of use coupled with few preparation steps for injection and decreased anxiety relating to needles are key attributes that may improve adherence to treatment and long-term treatment outcomes.
•
A passive sharps protection feature to prevent accidental needlestick injury was a noted benefit.
•
Concerns with SelfJect identified in this market research study included insurance coverage, cost and logistical (storage and disposal) issues.
Author contributions
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship, take responsibility for integrity of the work, and have given final approval to the version to be published. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, or data analysis and interpretation; took part in drafting, revising, or critically reviewing the article; and have agreed on the journal to which the article has been submitted.
Acknowledgments
The authors are grateful for the patients and HCPs who participated in this study. The authors thank Andrea Chernoff, Director of Market Research at Mallinckrodt Pharmaceuticals, for review of the manuscript. The authors acknowledge D Kim from MedLogix Communications, LLC, for medical writing and editorial assistance based on the authors' input and direction.
Financial disclosure
This market research and manuscript were sponsored by Mallinckrodt Pharmaceuticals. All authors are employees of Mallinckrodt Pharmaceuticals. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
Third-party writing assistance for this manuscript was provided by D Kim from MedLogix Communications, LLC, and was funded by Mallinckrodt Pharmaceuticals in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Ethical conduct of research
Since this was a market research study, prior approval of the protocol by an ethics committee was not required. The study was conducted in accordance with relevant market research guidelines, including the obtaining of informed consent and adherence to ethical reporting standards. All participants were provided written informed consent prior to participation in this study. Patients were compensated with a $150 eGift card, and HCPs received a $450 honorarium for participating in the study.
Data sharing statement
Data from nonclinical studies are outside of Mallinckrodt Pharmaceuticals' data sharing policy and are unavailable for sharing.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Askanase AD, Zhao E, Zhu J, Connolly-Strong E, Furie RA. Acthar Gel (repository corticotropin injection) for persistently active SLE: study design and baseline characteristics from a multicentre, randomised, double-blind, placebo-controlled trial. Lupus Sci. Med. 7(1), e000383 (2020).
2.
Mirsaeidi M, Baughman RP. Repository corticotropin injection for the treatment of pulmonary sarcoidosis: a narrative review. Pulm. Ther. 8(1), 43–55 (2022).
3.
Acthar Gel (repository corticotropin injection). Package insert. Mallinckrodt Pharmaceuticals. (2021).
4.
Domanska B, Stumpp O, Poon S, Oray S, Mountian I, Pichon C. Using patient feedback to optimize the design of a certolizumab pegol electromechanical self-injection device: insights from human factors studies. Adv. Ther. 35(1), 100–115 (2018).
5.
Keininger D, Coteur G. Assessment of self-injection experience in patients with rheumatoid arthritis: psychometric validation of the Self-Injection Assessment Questionnaire (SIAQ). Health Qual. Life Outcomes 9, 2 (2011).
6.
van den Bemt BJF, Gettings L, Domanska B, Bruggraber R, Mountian I, Kristensen LE. A portfolio of biologic self-injection devices in rheumatology: how patient involvement in device design can improve treatment experience. Drug Deliv. 26(1), 384–392 (2019).
7.
Chilton F, Collett RA. Treatment choices, preferences and decision-making by patients with rheumatoid arthritis. Musculoskeletal Care 6(1), 1–14 (2008).
8.
Maniadakis N, Toth E, Schiff M et al. A targeted literature review examining biologic therapy compliance and persistence in chronic inflammatory diseases to identify the associated unmet needs, driving factors, and consequences. Adv. Ther. 35(9), 1333–1355 (2018).
9.
Schiff M, Saunderson S, Mountian I, Hartley P. Chronic disease and self-injection: ethnographic investigations into the patient experience during treatment. Rheumatol. Ther. 4(2), 445–463 (2017).
10.
Coyne M, Rinaldi A, Brigham K et al. Impact of routines and rituals on burden of treatment, patient training, cognitive load, and anxiety in self-injected biologic therapy. Patient Prefer. Adher. 16, 2593–2607 (2022).
11.
Huh J, Ackerman MS. Collaborative help in chronic disease management: supporting individualized problems. CSCW Conf. Comput. Support Coop. Work. 2012, 853–862 (2012).
12.
Thompson DM, Booth L, Moore D, Mathers J. Peer support for people with chronic conditions: a systematic review of reviews. BMC Health Serv. Res. 22(1), 427 (2022).
13.
Narchi H, Elghoudi A, Al Dhaheri K. Barriers and challenges affecting parents' use of adrenaline auto-injector in children with anaphylaxis. World J. Clin. Pediatr. 11(2), 151–159 (2022).
14.
Alsbrooks K, Hoerauf K. Prevalence, causes, impacts, and management of needle phobia: an international survey of a general adult population. PLOS ONE 17(11), e0276814 (2022).
15.
Duncanson E, Le Leu RK, Shanahan L et al. The prevalence and evidence-based management of needle fear in adults with chronic disease: a scoping review. PLOS ONE 16(6), e0253048 (2021).
16.
Grissinger M. Reducing errors with injectable medications: unlabeled syringes are surprisingly common. P T. 35(8), 428–451 (2010).
Information & Authors
Information
Published In
Copyright
© 2024 Mallinckrodt Pharmaceuticals. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 August 2024
Accepted: 22 October 2024
Published online: 11 November 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A novel injection device to administer repository corticotropin injection for inflammatory disease treatment: findings from a market research study. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0131
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jas Bindra, Ishveen Chopra, Kyle Hayes, John Niewoehner, Mary Panaccio, Sheila Elliott, Bobby Trawick, George J. Wan, Real-World Insights on Satisfaction and Experience with Acthar Gel via SelfJect (RISE™): A Cross-Sectional Patient Survey, Advances in Therapy, 10.1007/s12325-025-03232-5, 42, 7, (3386-3399), (2025).