Economic burden of complicated ureteral stent removal in patients with kidney stone disease in the USA
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To examine the medical costs of simple versus complicated ureteral stent removal. Materials & methods: We included adults with kidney stones undergoing simple or complicated cystoscopy-based stent removal (CBSR) post ureteroscopy from the 2014 to 2018 Merative™ MarketScan® Commercial Database. The medical costs of patients with complicated and simple CBSR were compared. Results: Among 16,682 patients, 2.8% had complicated CBSR. Medical costs for patients with complicated CBSR were higher than for simple CBSR ($2182 [USD] vs $1162; p < 0.0001). Increased stenting time, increased age, southern US geography and encrusted stent diagnoses were significantly associated with complicated CBSR. Conclusion: Complicated ureteral stent removal doubled the medical costs associated with CBSR. Ureteral stents with anti-encrustation qualities may reduce the need for complicated CBSR and associated costs.
Over the last four decades, the prevalence of kidney stone disease in the USA has more than tripled from 3.2% in 1980 to 10.1% in 2016 [1]. In 2018, the prevalence of stone disease was 10.9% in men and 9.5% in women [2]. This condition primarily affects working-age adults between 20 and 60 years of age [3,4]. The total annual cost for treating kidney stone disease in 2000 was estimated to be $4.5 billion in the USA ($9 billion in 2021 USD) [4]. Indirect costs, such as missed workdays, among privately insured adults have been estimated to be $775 million per year [4].
Ureteroscopy is the most common interventional treatment for kidney stone disease and one of the most frequent urology procedures performed [5]. Stents are routinely placed by urologists in approximately 80% of ureteroscopy procedures [6]. The removal of the ureteral stent often requires a return visit for the patient and a cystoscopic procedure. While ureteral stents can maintain the outflow of urine from the kidney to the bladder, the removal of these stents may be complicated due to encrustation of mineral crystals from urine on the surface or lumen of the stent [7]. This calcification of the ureteral stent may raise the risk of stent fracture (due to loss of tensile strength), obstruct drainage through the stent lumen and interact with the urothelial lining, causing ureteral trauma during stent removal [7]. In recognition of this adverse event, the American Urological Association (AUA) recommends a specific Current Procedural Terminology (CPT)® code (52315) be used to code for the complex removal of an encrusted stent [8].
Several potential risk factors may influence the occurrence of ureteral stent encrustation, including the duration of stent indwelling time (time from procedure to stent removal), the stent’s physical characteristics, recurring urinary tract infections and patient demographic factors such as age, gender and comorbidities (i.e., chronic renal failure or diabetes) [7]. Ureteral stent encrustation may result in significant costs due to the multiple additional procedures required for the stent’s removal [7]. So far, no studies have quantified the economic burden of complicated ureteral stent removal in a real-world practice setting using large-scale patient data.
The objectives of this study were to: investigate the predictive factors associated with complicated ureteral stent removal among commercially insured patients undergoing ureteroscopy for kidney stone disease in the USA; and examine the medical costs associated with simple versus complicated ureteral stent removal. Our findings will help urologists better understand the predictive factors associated with complicated ureteral stent removal as well as the economic consequences of these complications when they occur.
Materials & methods
Data source & study population
A retrospective claims data analysis was conducted using the Merative™ MarketScan® Commercial Database to identify patients who underwent ureteroscopy with stent placement (index surgery) for kidney stone disease between January 2014 and June 2018 (Figure 1) The Merative MarketScan Commercial Database is a nationally representative data sample of the US population with employer-sponsored health insurance [9]. This database contains de-identified individual patient-level data and medical service claims for all settings of care among approximately 40 million covered individuals from 160 contributing employers and 40 contributing health plans [9]. Consequently, no institutional review board approval was needed for this study. Ureteroscopy with stent placement was defined using CPT code 52356.
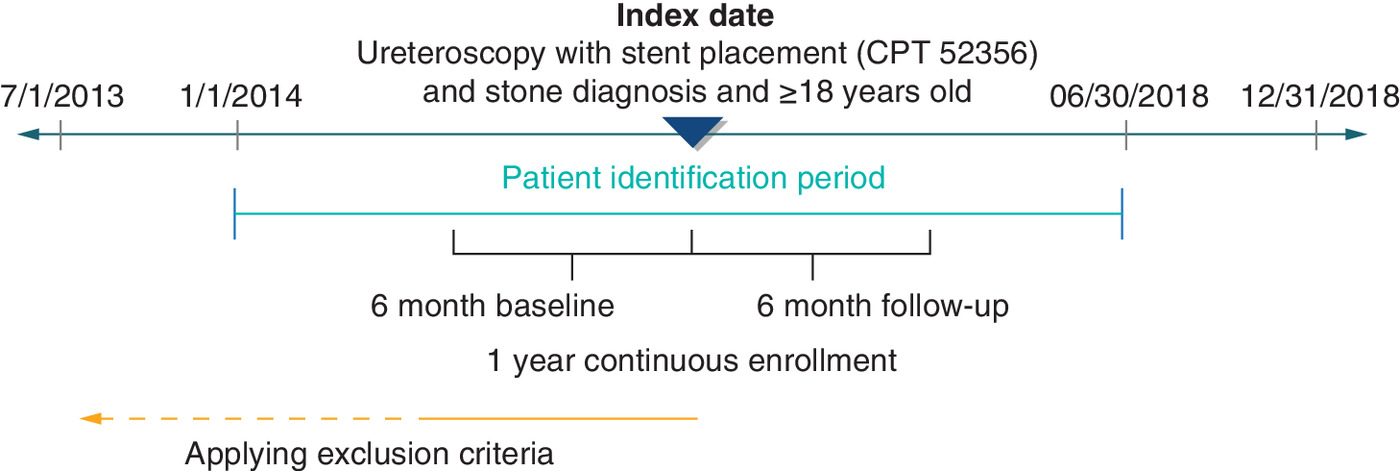
Figure 1. Patient identification scheme.
CPT: Current procedural terminology.
CPT is a registered trademark of the American Medical Association.
Patients were included if they were ≥18 years old, had 6 months of continuous enrollment in a commercial plan pre- and post-index procedure and had cystoscopy-based stent removal (CBSR) within 6 months post-index ureteroscopy (Figure 2). Patients were excluded if they had stone diagnoses or stent-related procedures at least 6 months before the index surgery or had medical costs for CBSR less than $0. Patients with CBSR were categorized into two groups using CPT codes for stent removal events: simple cystoscopic stent removal (CPT 52310) or complicated cystoscopic stent removal (CPT 52315). No data were available regarding the extent of stent encrustation (e.g., how encrustation was assessed, quantification of encrustation).
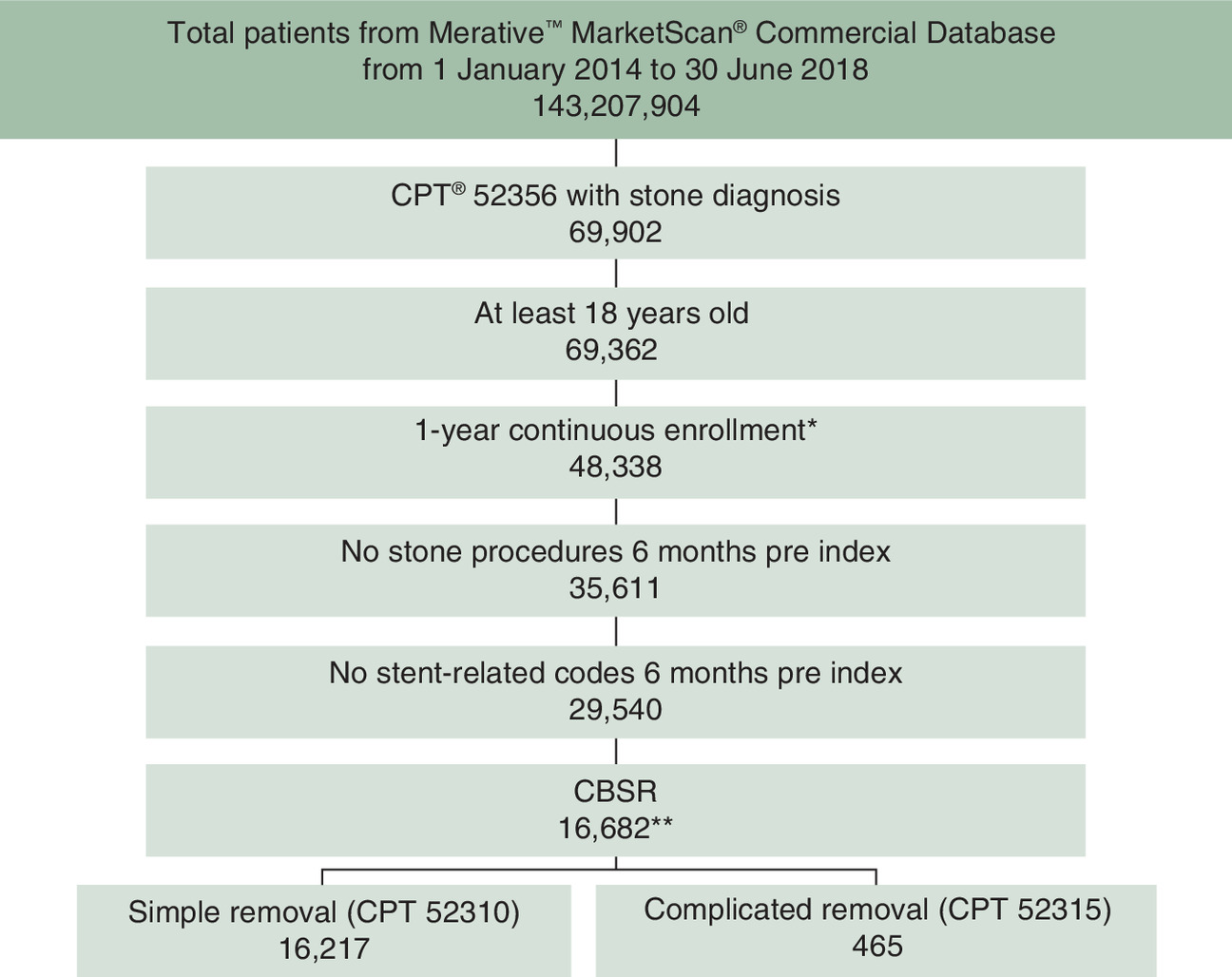
Figure 2. Inclusion and exclusion criteria.
CBSR: Cystoscopy-based stent removal; CPT: Current procedural terminology.
Patient characteristics & outcomes
Factors assessed included patient demographics, comorbidities, time to stent removal, stent removal site of service and encrusted stent diagnoses. Patient demographic factors examined included age, gender and geographic region. Comorbidities examined included diabetes, dyslipidemia, gout, hypertension, obesity, stone disease and/or renal disease as defined by Quan et al. [10]. These comorbidities were selected as they are associated with stone disease and have been included in previously published studies of stent placement [11]. Comorbidities were defined based on ICD-9 and ICD-10 codes that were observed during the 6 month pre-index (baseline) period. Time to CBSR was calculated as the number of days between the index surgery and the CBSR. The settings of care for stent removal were categorized into physician office, ambulatory surgical center, outpatient, emergency department or inpatient based on place of service codes. Medical costs of simple and complicated stent removal encounters occurring within 6 months post-index ureteroscopy were calculated to estimate the economic burden. Since stone disease is common among the working-age population, this analysis focused on the direct medical costs of simple or complicated CBSR in working-aged adults enrolled in employer-sponsored private health insurance plans [3,4]. Direct medical costs paid by other types of insurers, such as Medicare, were not included in this analysis.
Statistical analyses
The patient characteristics and comorbidities of patients with simple and complicated CBSR were compared using χ2 tests for categorical variables and t-tests for continuous variables. Multivariate regression was used to identify the factors associated with the occurrence of complicated stent removal.
To investigate the economic burden of complicated CBSR, greedy propensity-score matching (PSM) was used with a caliper of 0.02 without replacement to match patients with complicated and simple CBSR (1:5 matching) by their age, gender and region to compare the medical costs of simple and complicated stent removal encounters. Both pre- and post-PSM medical costs of CBSR were reported and compared using t-tests. PSM was selected as it is a common technique used to reduce or eliminate the effects of confounding when analyzing observational data [12]. All medical costs were adjusted to 2020 USD using the medical component of consumer price index [13]. The Instant Health Data software (Panalgo, MA, USA) and R, version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria) were used to perform the analyses of this study.
Results
Patient characteristics
Patient characteristics and comorbidities are presented in Table 1. Of the 16,682 patients undergoing CBSR after ureteroscopy with stent placement, 16,217 (97.2%) had simple CBSR and 465 (2.8%) had complicated CBSR within 6 months post-index ureteroscopy.
| Patient characteristic | Simple CBSR (n = 16,217) | Complicated CBSR (n = 465) | p-value |
|---|---|---|---|
| Group (%) | 97.2% | 2.8% | NA |
| Age group at index surgery (years) | |||
| 18–34 | 12.5% | 8.8% | 0.082 |
| 35–44 | 18.9% | 17.9% | |
| 45–54 | 31.2% | 33.6% | |
| 55–64 | 37.5% | 39.8% | |
| Male gender (%) | 52.9% | 58.1% | 0.033 |
| Geographical region (%) | |||
| Midwest | 23.1% | 11.8% | <0.0001 |
| Northeast | 18.6% | 23.1% | |
| South | 41.2% | 52.2% | |
| West | 17.0% | 12.9% | |
| Comorbidity | |||
| Diabetes | 14.6% | 16.3% | 0.312 |
| Dyslipidemia | 28.0% | 28.2% | 0.961 |
| Gout | 1.8% | 1.9% | 0.993 |
| Hypertension | 32.7% | 32.9% | 0.973 |
| Obesity | 11.3% | 11.2% | 0.998 |
| Renal disease | 2.5% | 2.2% | 0.741 |
| Stone | 55.4% | 55.7% | 0.949 |
| Year of stent removal | |||
| 2014 | 22.5% | 21.7% | 0.240 |
| 2015 | 22.6% | 19.8% | |
| 2016 | 22.5% | 21.3% | |
| 2017 | 21.1% | 25.0% | |
| 2018 | 11.3% | 12.3% | |
| Mean days to stent removal (SD) | 13.2 (13.8) | 16.5 (19.9) | 0.000 |
| Stent removal site of service | |||
| Office | 69.9% | 67.5% | 0.323 |
| Non office | 30.1% | 32.5% | |
| Encrusted stent diagnoses | 0.6% | 1.5% | NA |
The p-values in bold are significantly different at 0.05.
CBSR: Cystoscopy-based stent removal; SD: Standard deviation.
A majority of simple and complicated CBSR patients were male (52.9 vs 58.1%; p = 0.03), aged 55–64 years (37.5 vs 39.8%; p = 0.08), located in the south geographical region (41.2 vs 52.2%; p < 0.0001) and had stone disease prior to the index ureteroscopy with stent placement (55.4 vs 55.7%; p = 0.95). The mean number of days from procedure to stent removal for complicated CBSR patients was significantly higher than in patients with simple CBSR (16.5 vs 13.2 days; p = 0.000).
Factors associated with complicated CBSR
The results of the multivariate logistic regression showed increased time from procedure to stent removal, increased age, southern US geography and encrusted stent diagnoses were significantly associated with complicated CBSR (c-statistic = 0.61; Table 2). On the other hand, patient comorbidities and stent removal site of service were not predictors of complicated CBSR.
| Factor | OR | 95% CI | p-value |
|---|---|---|---|
| Age at index ureteroscopy (years)† | |||
| 35–44 | 1.275 | 0.861, 1.889 | 0.225 |
| 45–54 | 1.471 | 1.022, 2.118 | 0.038 |
| 55–64 | 1.469 | 1.017, 2.124 | 0.041 |
| Male gender† | 1.205 | 0.989, 1.468 | 0.064 |
| Geographical region† | |||
| Midwest | 0.396 | 0.291, 0.539 | <0.0001 |
| Northeast | 0.945 | 0.742, 1.204 | 0.649 |
| West | 0.591 | 0.438, 0.797 | 0.001 |
| Comorbidities | |||
| Diabetes | 1.096 | 0.823, 1.460 | 0.530 |
| Dyslipidemia | 0.903 | 0.708, 1.151 | 0.410 |
| Gout | 0.910 | 0.443, 1.868 | 0.797 |
| Hypertension | 0.896 | 0.710, 1.130 | 0.353 |
| Obesity | 1.031 | 0.755, 1.407 | 0.849 |
| Renal disease | 0.821 | 0.430, 1.570 | 0.552 |
| Stone | 1.051 | 0.864, 1.277 | 0.619 |
| Days to stent removal | 1.009 | 1.005, 1.014 | 0.000 |
| Non-office stent removal† | 1.141 | 0.929, 1.401 | 0.209 |
| Encrusted stent diagnoses | 2.359 | 1.075, 5.177 | 0.032 |
†
References are 18–34 years of age, females, south geographical region and office stent removal.
The p-values in bold are significantly different at 0.05.
OR: Odds ratio.
Economic burden of complicated CBSR
Supplementary Table 1 shows patient characteristics before and after PSM. Before PSM, the medical costs of complicated CBSR were significantly higher than the medical costs of simple CBSR ($2206 vs $1149; p < 0.0001). Among the total of 2598 propensity score matched patients (2165 simple CBSR vs 433 complicated CBSR patients), the average medical costs of CBSR encounters for matched simple and complicated CBSR patients were $1162 and $2182, respectively (p < 0.0001; Figure 3).
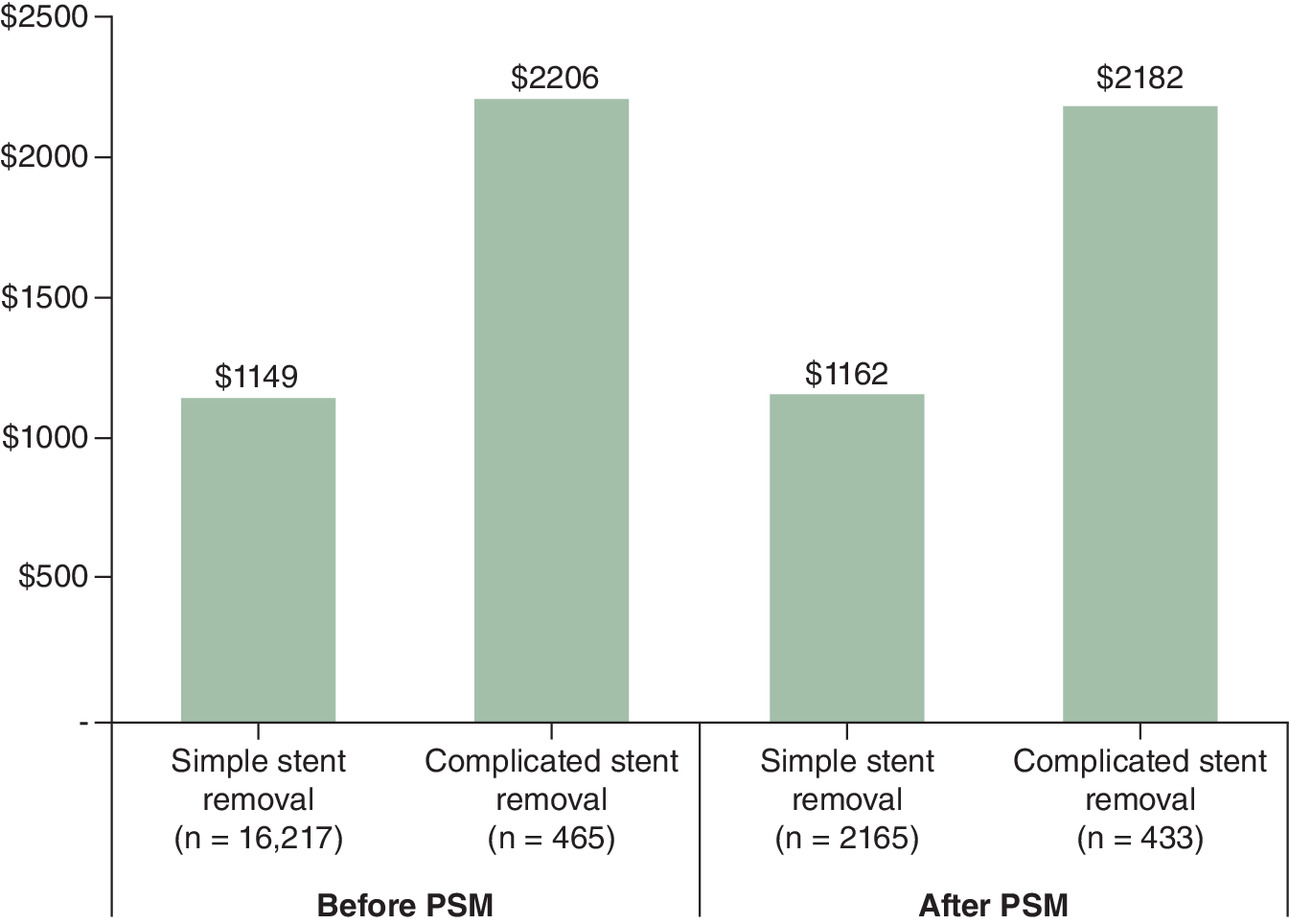
Figure 3. Medical costs of simple versus complicated cystoscopy-based stent removal before and after propensity-score matching.
PSM: Propensity-score matching.
Discussion
This was the first real-world study to examine the predictive factors and costs associated with complicated stent removal among working-aged patients undergoing ureteroscopy for kidney stone disease. Results indicate a greater number of days from procedure to stent removal (stent dwelling time), increased patient age, southern US geography and encrusted stent diagnoses were factors significantly associated with complicated CBSR when compared with simple CBSR. Simple and complex patients were similar in their comorbid profile, a finding consistent with recent literature [11]. The medical costs of complicated CBSR were also significantly higher than those of simple CBSR. The results from this commercial claims data analysis are consistent with the Medicare reimbursement rates. Specifically, while Medicare reimbursement to hospitals or ambulatory surgery centers is the same for simple and complex CBSR cases, reimbursement to physicians performing the stent removal is slightly higher for complicated CBSRs in both hospitals and office settings [14–16].
This study’s findings on the relationship between stent indwelling time and encrustation are consistent with previously published studies [17–20]. Kawahara and colleagues investigated the correlation between stent indwelling time and stent encrustation in 330 ureteral stents in 181 patients and found 155 (47.0%) of the stents were encrusted, and the encrustation rate was 26.8% at less than 6 weeks, 56.9% at 6 to 12 weeks and 75.9% at more than 12 weeks [17]. The authors also reported that heavily encrusted ureteral stents necessitating additional procedures for removal occurred within an indwelling time of 3 months [17]. El-Faqih et al. examined the complications associated with the use of 299 ureteral stents in a series of 290 stone patients and found signs of encrustation in 9.2% of the stents retrieved before 6 weeks, 47.5% retrieved between 6 and 12 weeks and 76.3% retrieved after 12 weeks [18]. A more recent study by Legrand and coworkers examined the relationship between stent indwelling times and encrustation rates in 473 stents from six European centers and found that the rate of stent encrustation for a stone disease indication was 8% for stents with indwelling times under 4 months and 17% for stents with indwelling times longer than 4 months [19].
In addition to a longer stent dwelling time, this study revealed that increased patient age and southern US geography were associated with an increased risk of complicated CBSR. It is feasible that an aging population has a higher risk of an increased uric acid level, resulting in a higher likelihood of encrustation [20]. Limited research has not addressed the relationship between US geography and the risk of complicated CBSR; further studies could examine this potential relationship which could help healthcare providers from different geographical regions better prepare for different risk levels of possible complicated procedures.
The findings of the present study on the increased costs associated with complicated CBSR are consistent with other studies that reported on the high costs due to multiple additional procedures required to remove an encrusted stent [21–23]. Staubli and colleagues examined the economic burden arising from stent-related problems in 74 patients with indwelling ureteral stents in Germany and found the total costs arising from stent-related problems averaged $1,802 per patient [23]. A retrospective review by Kartal and colleagues examining 69 patients with indwelling and forgotten ureteral stents for more than 6 months after urolithiasis treatment found that 26.1% of patients (n = 18) were treated by removing the ureteral stent under simple cystoscopy guidance, while the remaining 73.9% (n = 51) required surgical intervention to remove an encrusted stent [21]. Of those requiring surgery, multimodal surgical sessions were required in 70.5% of patients (n = 36 of 51) [21].
In addition to stent indwell time, the surface materials and coating of the stent may impact the rate of stent encrustation [7]. Several different stent technologies have been developed to reduce the burden of stent encrustation, including stents with hydrophilic coatings, stents composed of polyurethane, polyurethane polymer blends, silicone or nickel-titanium alloy and biodegradable stents [7]. Many of these technologies are designed to improve biocompatibility and reduce the calcium and magnesium salt adhesion associated with stent encrustation [7]. These technological innovations in stent design have the potential to reduce healthcare costs by reducing the rate of encrustation.
This study is not without limitations. First, stent removal, as defined by the study protocol, included only stents removed by cystoscopy [11]. Data for stents removed either by the patients themselves or by providers without the use of cystoscopy were not available in the Merative Marketscan database, as these types of encounters are not reimbursed and paid for by insurers. These results are not generalizable to provider-performed stent removal in a non-operating room setting, such as in the physician office. Second, this study was based on administrative claims data which provided rich information about the patients and their healthcare utilization and costs associated with their stone treatment and stent-related procedures; however, the clinical parameters captured via this type of data source are limited. For example, the claims data cannot be used to explain the small indwelling time difference between patients with simple and complicated CBSR. Further research using different data sources, including electronic medical records, could be used to explore this research gap. Third, the number of patients with complicated stent removal was relatively low. Although the AUA recommends using the complicated stent removal codes for encrusted stents (CPT code 52315), it is plausible that urologists were not aware of this code. While it is unknown which providers adhered to the AUA coding recommendations, it is possible that our study captured a lower number of complicated stent removal events compared with the number of actual events. Coding practices could also vary by geography although the claims data used in this study do not allow for further analysis of regional differences. Future studies could utilize other methods, such as interviews or surveys, to better understand differences in billing patterns by treatment site. It is also possible that patients with encrusted stents were treated with more invasive procedures, such as laser lithotripsy or percutaneous procedures, without the use of CPT Code 52315, potentially resulting in underestimation of complicated stent removal rates in this study. Further analyses, including analyses of clinically relevant subgroups, could be conducted to add different clinical relevance to the practice of ureteral stent care processes.
Regardless of the limitations, this study has several strengths. This is the first study to quantify the economic burden of complicated ureteral stent removal from the perspective of commercial insurers in the US and to identify the key predictive factors associated with complicated CBSR in a real-world setting. Additionally, this analysis used a large-scale dataset representing all geographic regions in the USA and all settings of care, which improves the generalizability of the findings. Finally, the results from the sensitivity analysis were consistent with the results of the main analysis, indicating the robustness of the findings.
Conclusion
Cystoscopy-based stent removal is one of the most common procedures following ureteroscopy with stent placement. This study found that approximately 3% of patients have complicated stent removal at the time of cystoscopy. Factors associated with complicated stent removal among commercially insured patients in the USA include increased patient age, south geographical region, longer stent dwell time and encrusted stent diagnoses. Medical costs of complicated stent removal were significantly higher than those of simple stent removal. Shorter indwell times, as well as the use of ureteral stents with anti-encrustation qualities, may reduce the need for complicated stent removal and potentially reduce costs to the US healthcare system.
•
There is no data on the economic burden of complicated ureteral stent removal in a real-world setting.
•
This study investigated factors associated with complicated stent removal among patients undergoing ureteroscopy for kidney stone disease.
•
Adults with kidney stones who underwent ureteroscopy and had simple or complicated cystoscopy-based stent removal (CBSR) were identified from the 2014 to 2018 Merative™ MarketScan® Commercial Database.
•
Patients with complicated and simple CBSR were 1:5 propensity score matched, and their medical costs (2020 USD) paid by insurers for CBSR encounters were compared to estimate the economic burden of CBSR.
•
The mean number of days from procedure to stent removal for complicated CBSR patients was significantly higher than in patients with simple CBSR (16.5 vs 13.2 days; p = 0.0004).
•
Regression analyses found increased time to stent removal, older age, southern US geography and encrusted stent diagnoses were significantly associated with complicated CBSR.
•
Medical costs of matched patients with complicated CBSR were significantly higher than simple CBSR ($2182 vs $1162; p < 0.0001).
•
Given that complicated ureteral stent removal doubles the medical costs associated with CBSR, ureteral stents with anti-encrustation qualities may reduce the risk of complicated CBSR and its associated costs.
Author contributions
All of the authors met the following criteria: made substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; drafted the work or revised it critically for important intellectual content; approved the final version to be published; agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Financial & competing interests disclosure
Support for this research was provided by Boston Scientific (MA, USA). KR Ghani is a Professor of Urology at the University of Michigan and is a paid clinical consultant for Boston Scientific, Coloplast, Ambu, Karl Storz and Olympus. AE Krambeck is a Professor of Urology at Northwestern University and is a paid clinical consultant for Boston Scientific, Lumenis, Virtuoso, Storz, Wolf and Sonomotion. KR Ghani and AE Krambeck were not compensated for their participation in this study. S Rojanasarot, B Cutone and SK Bhattacharyya are employees of Boston Scientific. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by M Mafilios at Health Economics Associates (CA, USA) and M Cleary at Cleary Medical Intelligence (GA, USA). Support for writing assistance was provided by Boston Scientific.
Acknowledgements
The authors would like to thank Alysha McGovern for her editorial support.
Ethical conduct of research
Since this study does not involve human participants, neither institutional review board approval nor participant consent was obtained.
Data sharing statement
This study used administrative claims data from Merative. Due to data use agreements signed with Merative, the raw data cannot be provided externally. Other researchers can purchase the same dataset to carry out similar analyses.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary table 1.pdf)
- Download
- 74.83 KB
References
1.
Chewcharat A, Curhan G. Trends in the prevalence of kidney stones in the United States from 2007 to 2016. Urolithiasis 49(1), 27–39 (2021).
2.
Abufaraj M, Xu T, Cao C et al. Prevalence and trends in kidney stone among adults in the USA: analyses of National Health and Nutrition Examination Survey 2007–2018 data. Eur. Urol. Focus 7(6), 1468–1475 (2020).
3.
Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic diseases in America project. Prevalence of kidney stones in the United States. Eur. Urol. 62(1), 160–165 (2012).
4.
Hyams ES, Matlaga BR. Economic impact of urinary stones. Transl. Androl. Urol. 3(3), 278–283 (2014).
5.
De Coninck V, Keller EX, Somani B et al. Complications of ureteroscopy: a complete overview. World J. Urol. 38(9), 2147–2166 (2020).
6.
Hiller SC, Daignault-Newton S, Pimentel H et al. Ureteral stent placement following ureteroscopy increases emergency department visits in a statewide surgical collaborative. J. Urol. 205(6), 1710–1717 (2021).
7.
Tomer N, Garden E, Small A, Palese M. Ureteral stent encrustation: epidemiology, pathophysiology, management and current technology. J. Urol. 205(1), 68–77 (2021).
8.
American Urological Association. Coding corner: how to code for indwelling ureteral stent removal. Policy and Advocacy Brief (2019). https://community.auanet.org/blogs/policy-brief/2019/07/02/coding-corner-how-to-code-for-indwelling-ureteral
9.
IBM Watson Health. IBM MarketScan research databases for life sciences researchers. https://www.ibm.com/downloads/cas/OWZWJ0QO
10.
Quan H, Sundararajan V, Halfon P et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 43(11), 1130–1139 (2005).
11.
Ghani KR, Rojanasarot S, Cutone B, Bhattacharyya SK, Krambeck AE. The economic burden of cystoscopy-based ureteral stent removal in the United States: an analysis of nearly 30,000 patients. Urol. Pract. 9(1), 40–46 (2022).
12.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
13.
US Bureau of Labor Statistics. Consumer price index. https://www.bls.gov/cpi/
14.
Centers for Medicare & Medicaid Services. Addendum A and Addendum B updates (2022). https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Addendum-A-and-Addendum-B-Updates
15.
Centers for Medicare & Medicaid Services. ASC payment rates – Addenda (2022). https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ASCPayment/11_Addenda_Updates
16.
Centers for Medicare & Medicaid Services. Physician fee schedule (2022). https://www.cms.gov/medicare/medicare-fee-for-service-payment/physicianfeesched
17.
Kawahara T, Ito H, Terao H, Yoshida M, Matsuzaki J. Ureteral stent encrustation, incrustation, and coloring: morbidity related to indwelling times. J. Endourol. 26(2), 178–182 (2012).
18.
El-Faqih SR, Shamsuddin AB, Chakrabarti A et al. Polyurethane internal ureteral stents in treatment of stone patients: morbidity related to indwelling times. J. Urol. 146(6), 1487–1491 (1991).
19.
Legrand F, Saussez T, Ruffion A et al. Double loop ureteral stent encrustation according to indwelling time: results of a European multicentric study. J. Endourol. 35(1), 84–90 (2021).
20.
Bouzidi H, Traxer O, Doré B et al. Caractéristiques des incrustations des endoprothèses urétérales chez les patients lithiasiques [characteristics of encrustation of ureteric stents in patients with urinary stones]. Prog. Urol. 18(4), 230–237 (2008).
21.
Kartal IG, Baylan B, Gok A et al. The association of encrustation and ureteral stent indwelling time in urolithiasis and KUB grading system. Urol. J. 15(6), 323–328 (2018).
22.
Sali GM, Joshi HB. Ureteric stents: overview of current clinical applications and economic implications. Int. J. Urol. 27(1), 7–15 (2020).
23.
Staubli SE, Mordasini L, Engeler DS, Sauter R, Schmid HP, Abt D. Economic aspects of morbidity caused by ureteral stents. Urol. Int. 97(1), 91–97 (2016).
Information & Authors
Information
Published In
Pages: 1253 - 1261
PubMed: 36259761
Copyright
© 2022 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 25 August 2022
Accepted: 30 September 2022
Published online: 19 October 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Economic burden of complicated ureteral stent removal in patients with kidney stone disease in the USA. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0153
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Serdar Basboga, Ahmet Burak Yilmaz, Kamal Karimzada, Ali Yasin Ozercan, Tanju Keten, Ozer Guzel, Altug Tuncel, Comparison of different encrustation severity scores for residual stone fragments after encrusted double J stent removal, Actas Urológicas Españolas (English Edition), 10.1016/j.acuroe.2026.502003, (502003), (2026).
- S. Basboga, A.B. Yilmaz, K. Karimzada, A.Y. Ozercan, T. Keten, O. Guzel, A. Tuncel, Comparación de diferentes sistemas de clasificación de la incrustación del catéter doble J para predecir fragmentos litiásicos residuales tras su retirada, Actas Urológicas Españolas, 10.1016/j.acuro.2026.502003, (502003), (2026).
- Vincent Khor, Bhaskar Kumar Somani, Mohamad Fairuz Mohamad Sharin, Omar Fahmy, Christopher Kheng Siang Lee, Saiful Azli Mohd Zainuddin, Mohd Ghani Khairul-Asri, Olivier Traxer, Vineet Gauhar, Smartphone application stent registry with automatic short-message service reminders mitigates the issue of forgotten ureteral stents: A multi-center retrospective cohort study in Malaysia—a European association of urology section of Endourology collaboration, Asian Journal of Urology, 10.1016/j.ajur.2025.11.007, (2026).
- Margarida Pacheco, Francesco D’Elia, Hanna Nilsson-Åhman, Estêvão Lima, Alexandre Barros, Cecilia Persson, Rui L. Reis, Additively manufactured WE43 for biodegradable urinary devices: Exploring the corrosion profile under in vitro urinary tract conditions, Applied Materials Today, 10.1016/j.apmt.2025.102975, 47, (102975), (2025).
- Sidharth Misra, Rahul Bisht, Zainab Yusufali Motiwala, Aditya Puniyani, Arusha Desai, Nihar Duddu, Danny Darlington Carbin, Is it prime time for stent-less robotic radical cystectomy? A scoping review, Journal of Robotic Surgery, 10.1007/s11701-025-02740-4, 19, 1, (2025).
- Zhicong Huang, Qilin Yang, Zhen Zhou, Gguoyao Ai, Guangyuan Zhang, Guohua Zeng, Yuqun Li, Association between low-dose aspirin use and kidney stone disease in middle-aged and older Americans: Data from the national health and nutrition examination survey 2011–2018, Asian Journal of Urology, 10.1016/j.ajur.2025.06.005, (2025).
- Anita Vergatti, Veronica Abate, Matteo Della Monica, Alfonso Varriale, Simone Magelli, Francesca Garofano, Lanfranco D'Elia, Antonio Barbato, Gianpaolo De Filippo, Domenico Rendina, Kidney stones and metabolic bone diseases not linked to parathyroid disfunction: a proposal for an integrated management, Archivio Italiano di Urologia e Andrologia, 10.4081/aiua.2025.13870, 97, 2, (2025).
- Kaiqiang Sun, Ningbin Zhao, Peizheng Shi, Zhuang Sun, Chen Ye, Li Fu, Dan Dai, Wubo Chu, Tao Cai, Hsu-Sheng Tsai, Cheng-Te Lin, Early Detection and Monitoring of Nephrolithiasis: The Potential of Electrochemical Sensors, Sensors, 10.3390/s25082547, 25, 8, (2547), (2025).
- Hidar Alibrahim, Sarya Swed, Bisher Sawaf, Mohammed Alkhanafsa, Fadel AlQatati, Tareq Alzughayyar, Namir Amer Abdeljawwad Abumunshar, Mulham Alom, Qutaiba Qafisheh, Roa'a Aljunaidi, Osayd Mosleh, Muhamad Oum, Agyad Bakkour, Lolwa Barakat, Kidney Stone Prevalence Among US Population: Updated Estimation from NHANES Data Set, JU Open Plus, 10.1097/JU9.0000000000000217, 2, 11, (2024).
- A. A. Aloyan, I. A. Gorgotsky, N. S. Korbina, V. P. Britov, I. V. Semenyakin, D. D. Shkarupa, N. K. Gadzhiev, Bioabsorbable ureteral stents: current state-of-the-art, Urology Herald, 10.21886/2308-6424-2024-12-2-76-86, 12, 2, (76-86), (2024).
- See more