Development of healthcare and social care services for the elderly population
Publication: Journal of Comparative Effectiveness Research
Abstract
Background & aim: The percentage of older people has been growing in all economically developed countries over the past several decades. The purpose of this research was to optimize the healthcare and social care model based on the in-depth study of social, hygienic and clinical characteristics of elderly individuals. Materials & methods: The authors' study included individuals aged 65 years and older. Results: The proportion of elderly and senile individuals increased from 15.3% in 2011 to 18.6% in 2020. The authors found that the existing healthcare system does not meet the needs of the aging population and thus developed a new organizational model for healthcare and social care services designed to integrate the activities of social welfare centers and local polyclinics. Conclusion: Implementation of the authors' model enables a range of healthcare and social care services and allows for management of a patient's health based on individual characteristics.
Over the past 50 years, the average life expectancy of people in advanced economies has grown 1.5–2.0 times [1]. According to the UN, the number of seniors in the world will exceed 1.1 billion by 2025 [2]. An aging population is one of the most significant demographic problems of modern times, as it entails a number of consequences, including social, economic, psychological, medical and legal consequences [3]. Provision of healthcare to this category of citizens is associated with a wide range of social, organizational, economic and psychological problems that accumulate as a result of age-related changes in the body, chronic conditions, anatomical and physiological changes, etc. [4,5]. Current conditions highlight the growing importance of healthcare services that have not only therapeutic but also preventive and hygienic purposes and are geared toward medical assistance to older age groups [6–8]. The WHO Global Strategy and Action Plan on Aging and Health addresses the growing needs of older people and promotes their inclusion in society as well as healthcare system adaptation [9]. In addition, this report emphasizes the need to implement long-term rehabilitation programs for seniors so that they can achieve and maintain an optimal level of independence and good quality of life.
The current demographic situation in Russia is characterized by an increase in the absolute and relative number of elderly people [10]. To illustrate, as of 1 January 2018, the share of older Russians averaged 25.0%, whereas only 15 years prior (2003), it was 20.4%. Considering the increasing number of cases of age-related chronic disease as well as the high prevalence of disability and dependence on others for care, older people should be offered improved geriatric healthcare [11,12].
Currently, there is no unified approach to the healthcare of older people in the Russian Federation. A number of authors have highlighted the need to first address the social and economic problems of the elderly [13–15]. Coordination between healthcare and social welfare institutions providing assistance to older citizens [16,17] must be strengthened, and primary healthcare must become more accessible and acceptable [18].
The geriatric population's need for high-quality care can be met through development and adequate use of all components of the national healthcare system, including both public and private healthcare facilities [19]. It is known that approximately 90% of elderly and senile Russians receive healthcare services at outpatient facilities [20]. Thus, polyclinics play a leading role in managing preventive and rehabilitation programs designed for older patients. However, to date, polyclinics lack a unified approach to management of such patients, who require more attention, time-consuming examinations, involvement of specially trained physicians, etc. [21]. Organization of senior patient management at the primary healthcare level is not effective and does not allow for achievement of the desired result. Thus, it seems reasonable to search for new ways to improve primary healthcare for this category of people. In light of the aforementioned issues, it is recognized in the Russian Federation that improved geriatric healthcare and social care services and strong infrastructure that will enable the delivery of comprehensive healthcare and social care services to older citizens are pressing medical and social needs.
Such improvement may be achieved only upon a detailed review of the health status, risk factors, quality of life and living conditions of elderly and senile people [21]. A few regions in Russia have conducted research to study certain aspects of the health status of elderly and senile individuals [22,23]. Several regional studies have examined the quality of life of elderly people in the physical, psychological, social and spiritual domains [24,25]. Still, there are a lack of sufficient studies covering all regions and considering all aspects of the problem. Studies that focus on the organization of healthcare and social care services for the older generation – and elderly people with disabilities in particular – based on their satisfaction with social support and rehabilitation and test hypotheses and prove them from a scientific point of view are still highly demanded [26]. As indicated earlier, the purpose of this study was to optimize the healthcare and social care model based on the in-depth study of social, hygienic and clinical characteristics of elderly and senile individuals as well as analysis of current efforts made by healthcare and social welfare institutions to help seniors and assessment of performance of social welfare center (SWC) employees.
Materials & methods
The present study involved persons aged 65 years who lived in the northeastern administrative district of Moscow. The study was conducted from 2016 to 2020. Demographics and health status of elderly and senile individuals were collected from the official statistical sources. Health and demographic data were taken from reports on population health status and efforts of healthcare facilities prepared by the Moscow Health Department, informational and analytical reports on disability in Moscow prepared by the city's Bureau of Medical and Social Expertise and records of the State Statistics Service for Moscow. The authors captured data from 2011 to 2020.
Social status and lifestyle of elderly and senile people living in the surveyed area were assessed by asking elderly and senile individuals to complete a few questionnaires. In completing the proposed questionnaires, senior individuals specified their passport data, assessed their own health and provided information about the frequency of acute disease and presence of chronic disease as well as educational background, work experience, financial status, living conditions, addictions, lifestyle, healthcare facility visit rates and health promotion activities. A total of 600 respondents were interviewed.
To evaluate older people's quality of life, the authors used the Russian language version of the Medical Outcomes Study Short Form 36 international questionnaire. Quality of life was assessed on eight scales: physical functioning, role limitation due to physical health, bodily pain, general health, vitality, social functioning, role limitation due to emotional problems and mental health.
Satisfaction of elderly and senile individuals with the healthcare and social care services they received was assessed by administering a specially designed questionnaire. The questionnaire determined each respondent's satisfaction with the available volume of diagnostic and treatment procedures, conditions for delivery of various healthcare and social care services, organization and operation of hospital departments, performance of healthcare professionals and professional training of healthcare professionals and social workers and their attitude toward patients.
The authors explored the outpatient care provided to elderly and senile recipients of social welfare services based on data concerning the material, technical and human resources of SWCs and local polyclinics. For this purpose, the following scientific and statistical questionnaires were developed: examination card of the elderly person receiving home-based social welfare services, guaranteed social welfare services timing and questionnaire card for local polyclinic physicians. The questionnaires satisfied the technical, organizational and ethical requirements applicable to social and hygienic studies. To assess the capabilities of SWCs and local polyclinics, the authors used a strengths, weaknesses, opportunities and threats analysis. Initially, the authors entered the most significant factors characterizing the identified organizational weaknesses or strengths of the healthcare and social care system into the strengths, weaknesses, opportunities and threats matrix. The authors also studied the social and hygienic characteristics of social workers employed at SWCs. A model was then developed for optimization of the outpatient healthcare and home-based social care services provided to elderly and senile individuals. Statistical processing and analysis of material were performed using the standard Microsoft Office 2016 software products: Word, Access and Excel (Microsoft Corporation, WA, USA).
Results
Clinical & demographic profiles of older people
The dynamics of clinical and demographic processes in the northeastern administrative district of Moscow are characterized by population aging and a significant number of seniors with disabilities. The proportion of elderly and senile people increased from 15.3% in 2011 to 18.6% in 2020. The number of primary disability cases among elderly and senile people increased from 43.4% in 2015 to 54.8% in 2020, with group 2 disabilities being the most prevalent (64.12%). In 2020, a total of 2678 elderly and senile individuals received healthcare and social care services in the outpatient care setting. Of 600 respondents receiving healthcare and social care services in the outpatient care setting, 53.8% were aged 60–70 years, 42.3% were aged 70–89 years and 3.9% were aged 90 years and older. In addition, 39.8% were men and 60.2% were women. The average age was 71.2 ± 3.4 years for men and 74.4 ± 4.2 years for women.
With regard to education, 14.4% of respondents had a primary education, 33.2% had a secondary education, 24.2% had a secondary vocational education and 28.2% had a higher education. Thus, the majority (71.8%) of respondents did not have a higher education. Among interviewed individuals over the age of 60 years, 68.4% were found to be disabled.
With 86.3% of respondents living separately, there was a high correlation between estimate of living conditions and age. Persons aged 60–74 years assessed their living conditions as good in 62% of cases, whereas persons aged 75–89 years assessed their living conditions as good in only 45% of cases. Living conditions were rated as satisfactory by 34 and 22.7% of respondents aged 60–74 and 75–89 years, respectively. With regard to marital status, widowed persons accounted for 48.4% of respondents. The authors noted 34.8% legally married respondents, of whom 70.2% were in their first marriage. A total of 8.4% of respondents lived in a common law marriage, 6.2% were never married or single and 2.4% were divorced.
One-third (34.2%) of elderly and senile individuals lived alone. Among seniors living alone, more women than men (60.3 and 39.7%, respectively) were observed. It should be noted that living alone was not always associated with having no children. Only 10.2% of respondents did not have children, whereas 41.7% had two children, 36.3% had one child, 9.5% had three children, 2.1% had four children and 0.2% had more than four children. The authors found that the percentage of people living alone increased with age, from 22.5% in respondents aged 65–69 years to 62.1% in respondents older than 80 years. An inverse relationship was seen for respondents living with a spouse.
According to the survey results, only 33.5% of respondents socialized with their relatives often, whereas 26.6% contacted their relatives from time to time, 19.5% contacted their relatives rarely and 18.3% were not able to communicate with their relatives. The authors recorded that 2.1% of respondents were unwilling to communicate with their family members. A total of 38.4% of respondents assessed their relationships with relatives, neighbors and close friends as good, with 30.2% assessing their relationships as very good. A quarter (25.4%) of respondents indicated that their relationships with relatives, neighbors and close friends could be better, and 6.0% assessed their relationships as poor
Finally, the authors noted that 28.6% of respondents lived below the subsistence level. Food, healthcare and pharmaceutical products predominated in the spending patterns of 84.6% of respondents (Table 1). The majority (68.9%) of respondents estimated their diet quality as medium. Diet quality was assessed as high by 10.8% of respondents and as low by one-fifth (20.3%). A total of 62% of elderly and senile individuals indicated they ate a diet rich in vegetables and meat, whereas 38% of respondents indicated they ate a diet rich in dairy products and baked goods.
| Expense | Approximate monthly expenses (%) |
|---|---|
| Food | 55 |
| Healthcare and pharmaceutical products | 17.5 |
| Clothing | 5.5 |
| Utilities | 16 |
| Other expenses | 6 |
| Total | 100 |
The main concerns for elderly and senile individuals were health (85.0%), social care services (13.0%) and material welfare (3.0%). The authors assessed social integration of persons aged 65 years and older as extremely low. Only 3.0% of respondents were members of public organizations, and less than 1.0% were members of political parties. A total of 16.2% of elderly persons engaged in leisure activities, including amateur performances and art or sports clubs, and the majority (88.6%) of these were women (average age: 72 years).
Table 2 illustrates the quality of life of elderly and senile individuals living in the northeastern administrative district of Moscow. The authors documented that general quality of life in persons aged 65 years and older was characterized by a low level of physical and social functioning (49.8 and 64.8 points, respectively, on a 100-point scale), with high pain scale scores. The results of the study showed that all respondents had experienced pain over the past 4 weeks, with 72.3% describing it as severe. The indicators of quality of life were significantly different for men and women. Differences were most obvious in individuals aged 65–70 years and gradually disappeared by the age of 81 years. In the 65–70 years age group, the indicators of physical functioning were significantly lower among women compared with men (58.5 and 77.4 points, respectively, on a 100-point scale). Similarly, the pain scores for women aged 65–70 years were higher than those observed for men (58.0 and 29.5 points, respectively, on a 100-point scale), with differences disappearing by the age of 81 years (64.5 and 63.7 points, respectively, on a 100-point scale). Quality of life indicators reflected a general tendency toward age-related decline in quality of life. Thus, older persons (aged over 70 years) indicated a steady decline in their quality of life on most scales and reported loss of not only physical but also psychological functioning (Figure 1).
| Characteristic | Quality of life indicator | |||||||
|---|---|---|---|---|---|---|---|---|
| PF | RP | BP | GH | VT | SF | RE | MH | |
| Men aged 65–70 years | 77.4 | 26.0 | 29.5 | 49.2 | 63.0 | 48.0 | 76.0 | 76.0 |
| Women aged 65–70 years | 58.5 | 57.0 | 58.0 | 58.6 | 65.0 | 44.3 | 36.3 | 46.8 |
| Men aged 71–80 years | 54.0 | 72.0 | 51.0 | 57.0 | 62.0 | 50.0 | 71.0 | 64.0 |
| Women aged 71–80 years | 39.3 | 79.5 | 60.0 | 54.0 | 63.0 | 46.6 | 33.3 | 45.9 |
| Men aged 81 years and older | 20.5 | 89.0 | 64.5 | 51.0 | 62.0 | 45.8 | 25.9 | 56.1 |
| Women aged 81 years and older | 18.9 | 89.0 | 63.7 | 51.0 | 61.0 | 47.2 | 23.4 | 38.9 |
| Mean value | 49.8 | 64.8 | 55.9 | 53.6 | 63.2 | 46.3 | 47.8 | 55.0 |
BP: Bodily pain; GH: General health; MH: Mental health; PF: Physical functioning; RE: Role limitation due to emotional problems; RP: Role limitation due to physical health; SF: Social functioning; VT: Vitality.
| Risk factor for health deterioration and social isolation | Assessment criterion | Score |
|---|---|---|
| Social and hygienic characteristics | ||
| Age (years) | 60–74 | 1 |
| 75–89 | 3 | |
| 90 and older | 6 | |
| Confirmed disability | None | 0 |
| Group 3 | 2 | |
| Group 2 | 4 | |
| Group 1 | 6 | |
| Living conditions | Good | 1 |
| Satisfactory | 3 | |
| Unsatisfactory | 6 | |
| Household size | Both spouse and children | 1 |
| Either spouse or children | 3 | |
| Single | 5 | |
| Family relationships | Good | 1 |
| Satisfactory | 3 | |
| Unsatisfactory | 6 | |
| Health status | ||
|---|---|---|
| Chronic diseases | 1 | 2 |
| 2–4 | 4 | |
| ≥5 | 6 | |
| Chronic disease course | Compensated | 1 |
| Subcompensated | 3 | |
| Decompensated | 6 | |
| Mental disorders | None | 0 |
| Mild | 2 | |
| Moderate to severe | 6 | |
| Acute diseases over the past year | None | 0 |
| 1–2 | 3 | |
| ≥3 | 6 | |
| Hospital admissions over the past year | None | 0 |
| 1–2 | 3 | |
| ≥3 | 6 | |
| Health self-assessment | Good | 1 |
| Declining | 3 | |
| Poor | 6 | |
| Vital functioning | ||
|---|---|---|
| Self-care capacity | Preserved | 0 |
| Stage 1 deficit | 2 | |
| Stage 2 deficit | 4 | |
| Stage 3 deficit | 6 | |
| Independent mobility | Preserved | 0 |
| Stage 1 loss | 2 | |
| Stage 2 loss | 4 | |
| Stage 3 loss | 6 | |
| Spatial and temporal orientation | Preserved | 0 |
| Stage 1 disorientation | 2 | |
| Stage 2 disorientation | 4 | |
| Stage 3 disorientation | 6 | |
| Communication skills | Preserved | 0 |
| Stage 1 disorder | 2 | |
| Stage 2 disorder | 4 | |
| Stage 3 disorder | 6 | |
| Self-control | Preserved | 0 |
| Stage 1 lack | 2 | |
| Stage 2 lack | 4 | |
| Stage 3 lack | 6 | |
| Risk factors | ||
|---|---|---|
| Body weight | Normal | 1 |
| Overweight | 4 | |
| Underweight | 4 | |
| Addictions | None | 0 |
| Non-serious | 2 | |
| Serious | 6 | |
| Stress and conflict | None | 0 |
| Occasionally | 3 | |
| Frequently | 6 | |
| Income | High | 0 |
| Moderate | 2 | |
| Low | 6 | |
| Access to healthcare | Easy | 2 |
| Reduced | 4 | |
| Restricted | 6 | |
| Access to social care | Easy | 2 |
| Reduced | 4 | |
| Restricted | 6 | |
| Diet quality | High | 2 |
| Medium | 4 | |
| Low | 6 | |
| Drug supply | Abundant | 2 |
| Sufficient | 4 | |
| Limited | 6 | |
| Personalized health and social adaptation program | Yes | 2 |
| No | 6 | |
| Life philosophy | Active longevity | 2 |
| Passive aging | 5 | |
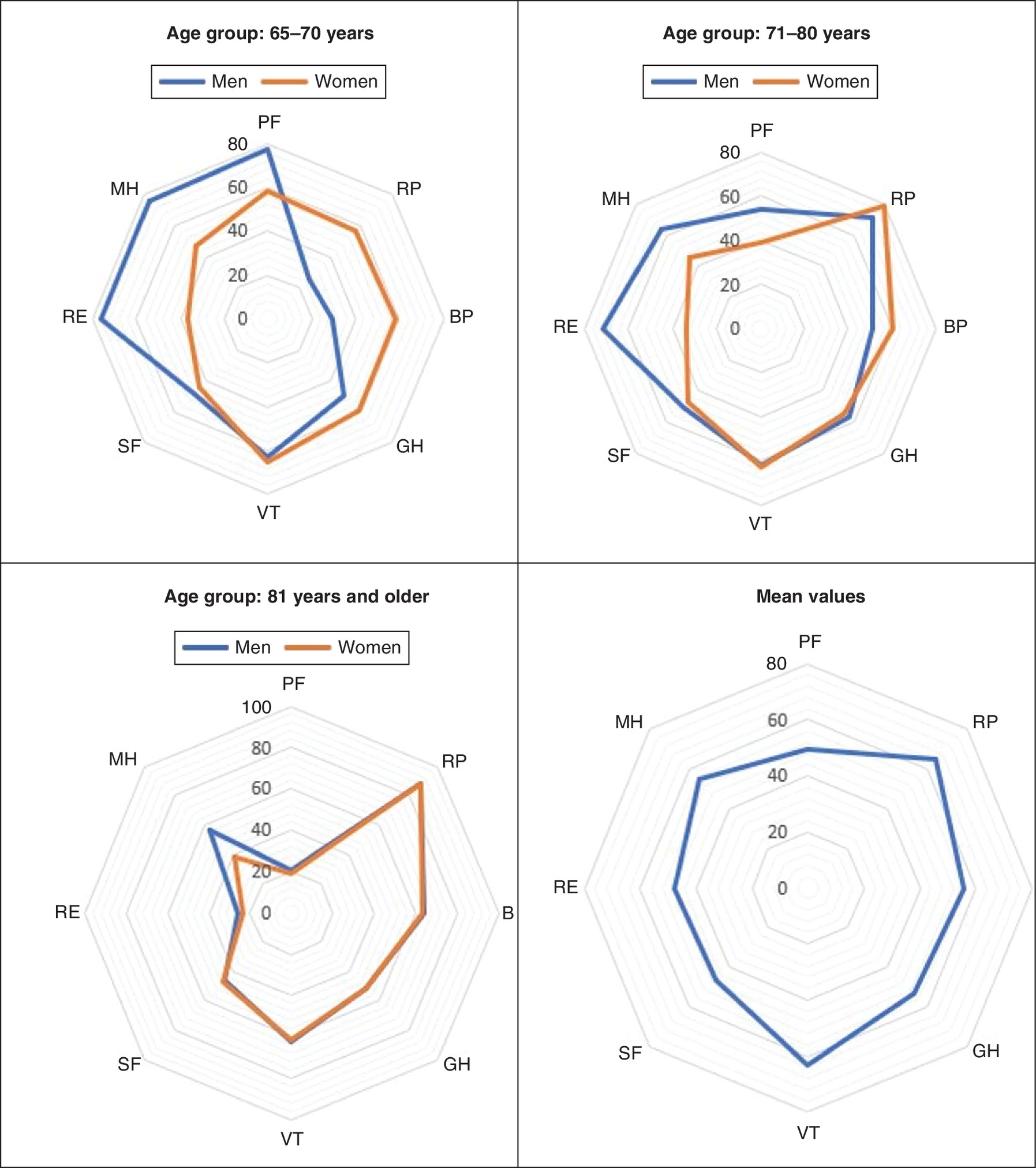
Figure 1. Quality of life profiles for male and female respondents of varying age.
BP: Bodily pain; GH: General health; MH: Mental health; PF: Physical functioning; RE: Role limitation due to emotional problems; RP: Role limitation due to physical health; SF: Social functioning; VT: Vitality.
The majority (87.6%) of respondents assessed their health as poor. The main difficulties experienced by older individuals in their daily life were impaired vision (65.3%), memory loss (27.6%), hearing loss or deafness (14.3%) and speech disorders (5.4%). Among the elderly, pain level was almost 1.5 times higher than that observed in other population groups. In addition, 94.5% of respondents reported deteriorating health over the past 12 months. Self-care capacity was reduced in 86.1% of older persons. Moving around the home was difficult for 45.4% of respondents. The health status of interviewed patients was characterized by multiple pathologies. A total of 62.5% of elderly and senile individuals indicated the presence of four to five chronic diseases and frequent exacerbations (more than five times a year).
The following diseases were prevalent in the morbidity pattern: cardiovascular diseases (74%), nervous system diseases (71%), gastrointestinal diseases (62%), musculoskeletal diseases (53%), respiratory diseases (51%) and excretory system diseases (43%). The incidence of disease was 2.3 times higher (p < 0.01) among men than women. Considering the overall morbidity rate, both men (72.3%) and women (73.7%) visited physicians to manage their previously known chronic diseases rather than to find the new ones. The frequency of exacerbations in patients with chronic diseases was not associated with hospitalizations, as only 16.5% of respondents were hospitalized two or more times a year. An unmet need for vision correction was revealed in 62.5% of interviewed patients, 35% of whom were diagnosed with cataracts in one or both eyes. The authors estimated the need for ophthalmological care among elderly and senile persons to be 928.2 ± 6.45 per 1000 people. The need for dental care was reported by 74.3% of respondents, and the need for dental care in elderly and senile individuals was estimated to be 734.6 ± 7.27 per 1000 people.
Only 12.3% of respondents followed a personalized rehabilitation program. Respondents were not interested in applying for such programs since – after confirming their disability status and engaging in a personalized rehabilitation program – 98% did not see any improvement in the healthcare and social care they received. It should be mentioned that personalized rehabilitation programs are available in one standard form for both the disabled and the elderly requiring healthcare and social care, which does not promote healthcare and social care system quality. Elderly and senile patients visited local polyclinics for the following reasons: treatment and diagnostics (63.2%), consultations with healthcare professionals (26.2%) and rehabilitation (10.6%).
Healthcare & social care organization, access & quality as estimated by elderly & senile individuals
Based on the survey regarding healthcare and social care organization, access and quality, the majority (82%) of elderly and senile persons attended state-funded healthcare facilities (local polyclinics). Alternatively, 8% visited private medical centers, and 10% were registered in the newly established specialized healthcare and social care geriatric center. If offered a range of specialized healthcare services (geriatricians, cardiologists, neurologists and psychotherapists) and social assistance (psychologists, social workers and lawyers).
In 2020, the healthcare network offering services to the urban adult population included 12 healthcare facilities, comprising 36 outpatient departments and 24 day hospitals. With regard to healthcare network staffing, there were 5474 healthcare professionals in 2011 and 5678 healthcare professionals in 2020 (an increase of 3.7%). The number of healthcare workers per a population of 10,000 varied slightly during the examined period and averaged 112.4 (the average for the Russian Federation in 2020 was 44.0 per a population of 10,000). During the examined period, the number of nursing staff members did not change significantly, amounting to 9363 nurses in 2011 and 9256 nurses in 2020. At the same time, the number of nurses per a population of 10,000 decreased by 6.6%, from 171.2 to 160.6 (the average for the Russian Federation was 92.4 per a population of 10,000). The number of outpatient visits was 14,548 in 2011 and 15,933 in 2020 (an increase of 8.7%). The number of outpatient visits per a population of 10,000 was 271.8 in 2011 and 279.4 in 2020 (an increase of 2.8%). This variable exceeded the average for the Russian Federation by 22.3%.
Home health services were provided by SWCs. As of 2020, a total of 6297 individuals were receiving home care. The total number of SWC employees directly engaged in home care for older people was 654. The number of in-home services provided per person increased from 345 in 2011 to 467 in 2020 (an increase of 35%). Healthcare and social care services were often delivered to elderly and senile people without regard to age, concomitant disease or self-care capacity. Patients were normally selected without a physician's involvement, and 33.7% of respondents had not had their indications for outpatient care revised for 5 or more years. Moreover, more than 20% of patients had their mobility and self-care levels preserved. Low-quality healthcare and social care were explained by the following: insufficient population density (46.4%), long queues at polyclinics to see a primary care physician and other specialists (86.3%), poor time management of social workers (76.7%) and lack of differentiated standards for social care (72.4%). The typical portrait of a social worker was described as follows: female aged 40–59 years (81.1%) who obtained higher education, had more than 5 years of work experience in the system and underwent special training in social work (62%). For 98% of social workers, employment at SWCs was full-time. Social workers were found to be highly motivated. A total of 95.4% considered their work important to the social environment, and more than half (54.6%) of respondents were completely satisfied with it. The majority (53.4%) of social workers prioritized life experience, compassion and personal qualities over professional knowledge, and such a philosophy affected their work performance. Consequently, 57% of respondents indicated a lack of legal, social and psychological knowledge.
Satisfaction of older generations with healthcare & social care services
The survey exploring satisfaction of patients aged 60 years and older with outpatient and inpatient care and various social welfare services demonstrated that 10.4% of patients visited their primary care physician only once a year and 11.4% visited their primary care physician twice a year. Almost half (48.4%) of patients saw their primary care physician every month, 22.3% saw their primary care physician twice a month, 7.2% saw their primary care physician once a week and 0.3% saw their primary care physician more than once a week. Importantly, 86.4% of patients indicated that they faced various problems at the stage of contacting a polyclinic (no healthcare professionals available, remote polyclinic, long waiting lists, inconvenient appointment time, etc.). Respondents noted that the situation with home visit physicians was more favorable. Only 21.2% of patients found themselves unable to get through to the polyclinic. The majority (72.3%) of respondents assessed the volume of diagnostic procedures they received in the inpatient setting as sufficient, whereas 23.6% of patients considered the volume insufficient and 4.1% felt it was excessive. The volume of healthcare interventions was characterized as sufficient by only 39.9% of respondents. Notably, 59.7% of patients assessed healthcare interventions as insufficient, and only 0.4% considered them excessive. Dissatisfaction with the volume of healthcare interventions was associated with drug shortages in hospitals (reported by 68.4% of respondents). Drug supply was described as satisfactory and sufficient by 31.2 and 0.4% of respondents, respectively. None of the respondents assessed drug supply as abundant.
The survey revealed that the satisfaction of elderly and senile individuals with quality of outpatient care was generally low (not exceeding 14.8%). At the same time, satisfaction with inpatient care was slightly higher (23.4%). The following gaps were identified in outpatient care: unsuccessful attempts to contact polyclinic (72.2%), long wait time for an appointment with a primary care physician (64.7%), lack of information regarding diagnostic and therapeutic procedures performed (39.2%) and insufficient volume of healthcare interventions (21.7%). With regard to inpatient care, respondents indicated the following gaps: long waiting lists for planned hospital care (73.2%), limited drug supply (68.4%) and lack of information concerning diagnostic and therapeutic procedures performed (63.2%).
Social welfare services provided to elderly and senile persons were assessed as mainly satisfactory (76.4%). However, the volume of social welfare services was assessed as insufficient by 42.4% of respondents and as sufficient by 38.4%. With respect to satisfaction of elderly and senile individuals with social welfare organization, the results revealed that only 21.2% of respondents, of whom 42.4% were disabled, regularly used the services offered by social welfare institutions. The aforementioned services were sometimes used by 12.4% of respondents, of whom 24.6% were disabled, and 13.4% of respondents indicated that it was difficult to apply for social welfare programs, as it was necessary to prepare a large number of documents and wait. Men applied for social welfare programs less than women (15.2 and 24.8%, respectively). The number of candidates for social welfare programs increased with age (12.2% among citizens aged 65–70 years and 34.6% among citizens aged over 70 years). Elderly recipients of social welfare services were completely satisfied with the services they received in 12.4% of cases, partially satisfied in 31.0% of cases and dissatisfied in 56.6% of cases.
Organization & function of geriatric healthcare & social care
Using a knowledge-based approach, the authors created a scale for assessing health and social isolation risk in individuals receiving home-based social welfare services (Table 3). Each criterion was given a score. The experts involved were geriatricians, primary care physicians, social workers and psychologists who were members of the healthcare and social care expert commissions. The scale consisted of four sections covering the social and hygienic characteristics of respondents (5 criteria) as well as their health status (6 criteria), vital functioning (5 criteria) and risk factors (10 criteria). Depending on the score obtained, recipients of social welfare services fell into one of the following groups: low health and social isolation risk (score: 33–73), medium health and social isolation risk (score: 74–114) and high health and social isolation risk (score: 115–152).
Initially, the most significant factors characterizing the identified organizational weaknesses or strengths of the healthcare and social care system were entered into the strengths, weaknesses, opportunities and threats matrix. Based on the results of the analysis, the authors developed a new organizational model for healthcare and social care services designed to integrate the activities of SWCs and local polyclinics (Figure 2).
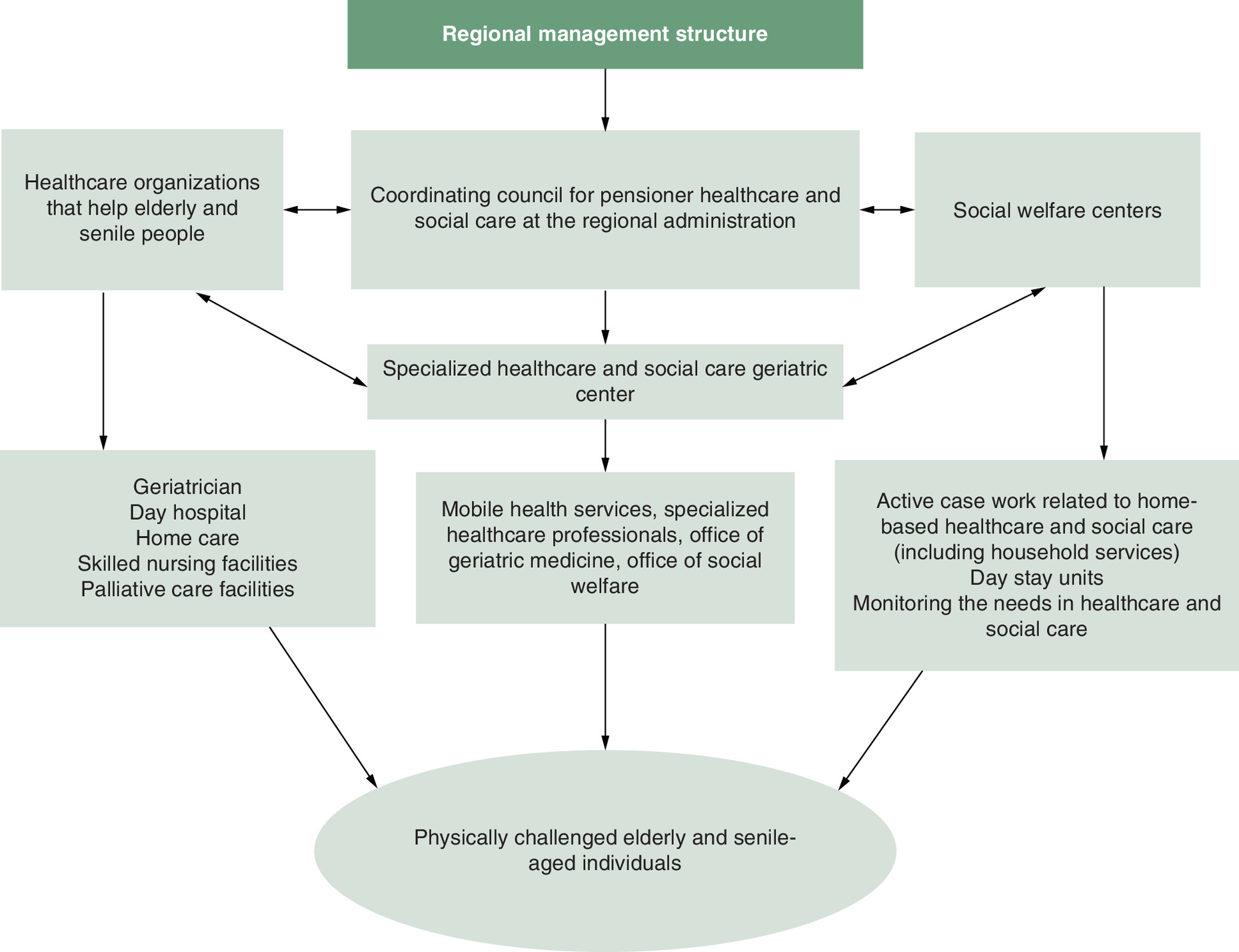
Because geriatric healthcare had been separated from social care by institutional barriers, these sectors were functionally integrated through creation of a coordinating council for pensioner healthcare and social care at the regional administration. The functions of the coordinating council included resolving common problems arising in geriatric healthcare and social care, assessing the need for healthcare and social care and monitoring the access to and quality of healthcare and social care services provided.
In addition to the organizational and functional model, a number of information technologies were developed, which made it possible to automate some routine functions and served as the basis for adaptation of the healthcare system to the needs of older people. Based on a single regional register, an algorithm for monitoring the health of elderly and senile people was developed and introduced into the activities of healthcare organizations (Figure 3). This algorithm describes the interdisciplinary and interinstitutional work of healthcare professionals. Automated screening of needs recorded by healthcare professionals makes it possible to develop a personalized program of health precautions and rehabilitation measures for senior individuals.
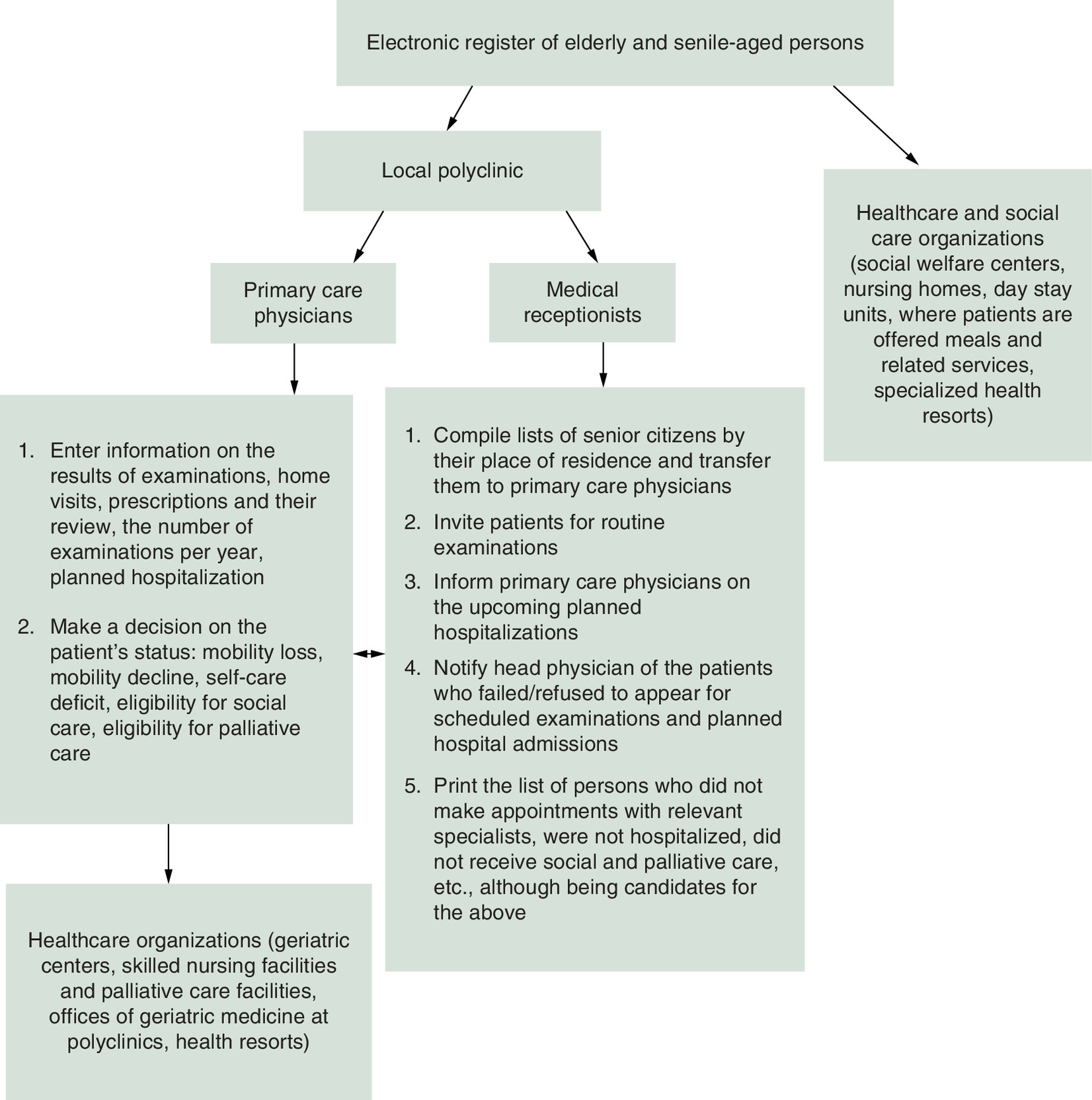
The personal data of assigned patients are sent to the healthcare organization that provides outpatient care (local polyclinic). The register of elderly and senile persons automatically selects a group of individuals. Primary care physicians have access to records of patients residing in the service area. In addition to the standard clinical information, physicians enter into the register information about limited mobility or reduced self-care capacity, eligibility for social care services, date of the patient's next examination, estimated length of hospital stay, eligibility for palliative care, etc.
One more program was developed and subsequently implemented at the reception desks. Known as Elderly Monitoring, it automatically reminds the patient of scheduled examinations or admissions. The registrar arranges the patient's appointment with the appropriate specialist, documents the required information and invites the patient for an office visit at the fixed time. The primary care physician monitors and regulates the procedure for planned hospitalization. Social workers store information regarding the care provided, the patient's identified needs and the time interval for the next expected visit. The relevant lists (which are generated automatically) are sent to the coordinating council for pensioner healthcare and social care at the beginning of each month.
Discussion
The results of the authors' study show that the proportion of elderly and senile people increased from 15.3% in 2011 to 18.6% in 2020. The number of primary disability cases among elderly and senile people increased from 43.4% in 2015 to 54.8% in 2020, with group 2 disabilities being the most prevalent (64.12%). In 2020, a total of 2678 elderly and senile individuals received healthcare and social care services in the outpatient care setting. Of 600 respondents receiving healthcare and social care services in the outpatient care setting, 53.8% were aged 60–70, 42.3% were aged 70–89 years and 3.9% were aged 90 years and older. In addition, 39.8% were men and 60.2% were women. The average age was 71.2 ± 3.4 years for men and 74.4 ± 4.2 years for women.
The authors found that the dynamics of clinical and demographic processes in the northeastern administrative district of Moscow are characterized by population aging and a significant number of seniors with disabilities. These results correlate with other regional studies and cumulative data for the Russian Federation [10,27]. The poor health of the elderly and senile population is explained by their living with several chronic diseases. Based on the study data, medical and social characteristics of elderly and senile individuals were identified and were associated with social, educational and economic inequality. The Medical Outcomes Study Short Form 36 was administered to assess the quality of life of men and women aged 65 years and older. The survey revealed that the elderly and senile urban population was not satisfied with their access to and the quality of healthcare and social care. Quality of and access to healthcare and social care depend on the qualifications of social workers, the application of scientific principles in their work and the interaction between healthcare and social care services. As indicated earlier, more than half of social workers prioritized life experience, compassion and personal qualities over professional knowledge, and such a philosophy affected their work performance. Furthermore, 67.4% of social workers did not understand the fundamentals of a healthy diet. As a result, they bought foods that were contraindicated for their clients. Finally, 57% of social workers surveyed reported a lack of legal, social and psychological knowledge.
The model for optimization of outpatient healthcare and social care services provided to elderly and senile people must be focused on maintaining their health and must be evaluated under efficiency criteria in terms of clinical, social and economic value [16,21]. The results of the authors' study form a methodological basis for planning and improving the organization of healthcare and social care for elderly and senile individuals living in large industrial cities. The aforementioned services should be aimed at improving the access to and quality of healthcare and social care services. The information obtained regarding the elderly and senile urban population's satisfaction with healthcare and social care services not only allows for integration of established procedures and standards into the healthcare and social care quality management system but also highlights the age characteristics and needs of this category of patients.
Based on the obtained data, the methods for improving organization of healthcare and social care services offered to the urban population aged 65 years and older are substantiated from a scientific point of view. Introduction of the proposed organizational and functional model of healthcare and social care for the elderly enabled implementation of mobile health services for the examination of all individuals who had been receiving social care for more than 5 years. The authors found that more than 15% of those examined did not meet the criteria for social care. Home care was also implemented in the healthcare system, which contributed to health improvements in patients suffering from cardiovascular, bronchial, lung and neurological diseases. In 2020, the number of hospitalizations among the studied population decreased by 21.4%, and the number of ambulance calls decreased by 10.3%. Social workers were assigned to local polyclinic physicians, and this allowed for a reduction in crowding at polyclinics as well as avoidance of conflict situations and provided patients with consultations with highly specialized healthcare professionals.
Active monitoring of geriatric health revealed a catastrophic lack of resources for clinical rehabilitation of disabled pensioners in the outpatient setting. In addition, there was a shortage of healthcare workers able to provide healthcare and social care services at home, including home nursing and home care for seriously ill and disabled patients. In order to improve the organization of healthcare and social care for elderly and senile people living in a large city, it is necessary to monitor demographics as well as morbidity and disability rates among this age category of the population [11]. For the purpose of monitoring, the vital functions of persons aged 65 years and older should be coupled with data on their social profile, lifestyle and quality of life. Information on the satisfaction of elderly and senile individuals with healthcare and social care services can be used when choosing the healthcare and social care priorities offered to this age group [14].
In order to coordinate the work of healthcare and social welfare institutions, coordinating councils for pensioner healthcare and social care should be created at regional administrations. It is recommended to introduce into the practice of healthcare and social care organizations the register of elderly and senile persons and maintain the appropriate integrated database based on the register of patients assigned. It would also be reasonable for SWCs to cooperate with primary care physicians at local polyclinics in choosing elderly and senile candidates for rehabilitation and day hospitals. In addition, it seems appropriate to include in the job description of social workers the responsibility of accompanying elderly and senile persons to day hospitals at polyclinics and day stay units and rehabilitation units at SWCs. Furthermore, it would be prudent to assign social workers to general practitioners (with unions between them formed on a local basis) and bring information about the elderly and senile individuals receiving home-based services to primary care physicians. Eventually, local polyclinics are recommended to organize day hospitals and arrange home care for their elderly and senile patients.
Conclusion
To optimize healthcare and social care of elderly and senile people living in a large city, the focus must be on monitoring the need for various types of healthcare and social care services, founding and maintaining city geriatric centers, finding alternatives to inpatient care, training geriatricians and integrating them into the healthcare system, developing palliative care and nursing care, engaging in active case work and maintaining better control over healthcare and social care access and quality. The existing healthcare system does not meet the needs of the aging population. The proposed model for optimization of outpatient healthcare and social care services provided to elderly and senile individuals ensures cooperation between clinical and social welfare units at the hospital and non-hospital level. Implementation of the authors' model enables a range of healthcare and social care services and allows for management of a patient's health based on individual characteristics. The clinical and social efficacy of the model has been demonstrated, which is indicative of its feasibility.
•
The purpose of this study was to optimize the healthcare and social care model of elderly and senile individuals.
•
The authors created a scale for assessing health and social isolation risk in individuals receiving home-based social welfare services.
•
The results showed that the proportion of elderly and senile people increased from 15.3% in 2011 to 18.6% in 2020.
•
The authors found that the dynamics of clinical and demographic processes are characterized by population aging and a significant number of seniors with disabilities.
•
The results of the study form a methodological basis for planning and improving the organization of healthcare and social care for elderly and senile individuals.
•
The methods for improving the organization of healthcare and social care services offered to the urban population aged 65 and older are substantiated from a scientific point of view.
•
The proposed model for optimization of outpatient healthcare and social care services ensures cooperation between clinical and social welfare units at a hospital and non-hospital level.
•
Implementation of the authors' model enables a range of healthcare and social care services and allows for management of a patient's health based on individual characteristics.
Author contributions
Conceptualization, methodology and software: I Poleshchuk. Data curation, project administration and writing: N Shustikova. Original draft preparation: N Kasimovskaya. Visualization and investigation: O Malkina. Resources and supervision: V Ermilova. Formal analysis and writing: E Egorova. Reviewing and editing: K Khvostunov.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. The study was approved by the local ethics committees of Sechenov First Moscow State Medical University (Sechenov University).
Data sharing statement
Data are available on request.
References
Papers of special note have been highlighted as: • of interest
1.
United Nations. World Population Ageing 2019 (2019). www.un.org/development/desa/pd/news/world-population-ageing-2019-0
2.
United Nations. World Population Prospects 2019 (2019). https://population.un.org/wpp/
3.
Beard JR, Officer A, De Carvalho IA et al. The world report on ageing and health: a policy framework for healthy ageing. Lancet 387(10033), 2145–2154 (2016).
4.
Seals DR, Justice JN, LaRocca TJ. Physiological geroscience: targeting function to increase healthspan and achieve optimal longevity. J. Physiol. 594(8), 2001–2024 (2016).
5.
Sadana R, Blas E, Budhwani S, Koller T, Paraje G. Healthy ageing: raising awareness of inequalities, determinants, and what could be done to improve health equity. Gerontologist 56(Suppl. 2), S178–S193 (2016).
6.
Rowe JM, Rizzo VM, Kang SY et al. Time contribution of social workers in care management: value for older adults. Prof. Case Manag. 24(6), 306–316 (2019).
7.
Donelan K, Chang Y, Berrett-Abebe J et al. Care management for older adults: the roles of nurses, social workers, and physicians. Health Aff. (Millwood) 38(6), 941–949 (2019).
8.
Buerhaus PI, Chang Y, DesRoches C, Guzikowski S, Norman L, Donelan K. The roles and clinical activities of registered nurses and nurse practitioners in practices caring for older adults. Nurs. Outlook 69(3), 380–388 (2021).
9.
WHO. Global strategy and action plan on ag ing and health (2017). www.who.int/publications/i/item/9789241513500
• Describes the growing needs of older people and promotes their inclusion in society as well as healthcare system adaptation.
10.
Kuzmicheva RA, Malay A. The main features of the demographic situation in modern Russia. Stud. Science Issues 5–2(33), 474–480 (2019).
• Analyzes the current demographic situation in Russia.
11.
Bratkova VV, Kochesokov AK, Kochesokova MK. Analysis of demographic situation in modern Russia. Exp. Council Bull. 1(24), 76–81 (2021).
12.
Korolev MA. Medical and social assistance to the elderly (literature review). Cons. Med. 22(12), 77–80 (2020).
13.
Beidina TE, Sapozhnikova TI, Gordeeva TN, Popov YuA. Approaches and directions of social policy in conditions of population aging: specificity of Russia, China, USA. Bull. Tran. Baik. State Uni. 23(7), 74–85 (2017).
• Outlines social and economic problems of the elderly.
14.
Karpikova IS, Kanunnikova AA. Development of social technologies for senior citizens: problems of implementation and assessment (on the example of hospital-replacing technology ‘foster family for an elderly person’). Sociodynamics 6, 19–32 (2020).
15.
Memetov SS, Sharkunov NP. Social problems of elderly and senile people at the present stage. Colloq. J. 5(29), 63–66 (2019).
16.
Bykovskaya TY, Zakharchenko Y, Kim VV. Some features of the provision of medical care to elderly and senile citizens. Colloq. J. 16(40), 69–72 (2019).
17.
Veretennikova AA, Kamyshnikov AI. Interdepartmental interaction in the healthcare system. Reg. System Econ. Manage. 2(45), 31–35 (2019).
• Describes coordination between healthcare and social welfare institutions.
18.
Znachkova EA, Grishina NK, Serdyukovskiy SM, Solovyova NB, Belostotskiy AV, Gridnev OV. Provision of medical care to people over 60 years old with multiple chronic diseases in Moscow. Prob. Soc. Hygiene Pub. Health His. Med. 25(3), 163–167 (2017).
19.
Ellansky YuG, Ilyukhin RG, Ayvazyan ShG. Models of geriatric aid in Russia and Europe: prerequisites for formation, modern stage, prospects. Health Manage. 3, 54–59 (2019).
20.
Larina VN, Kudina EV, Golovko MG, Shcherbakova ES, Ershov NS, Ushakova NA. The incidence of geriatric syndromes in older outpatients. Medicine 2, 13–20 (2019).
21.
Edeleva AN, Fedotkin MA. Improvement of inpatient medical care for elderly and senile people. Med. Almanac 4(44), 18–23 (2016).
• Outlines a model for optimization of outpatient healthcare and social care services provided to elderly and senile people.
22.
Puzin SN, Memetov SS, Sharkunov NP, Kim VV, Litvinova YuV. Problematic issues of medical and social rehabilitation of elderly and senile people at the present stage. Phys. Rehab. Med. Med. Rehab. 1(4), 42–44 (2019).
• Discusses certain aspects of the health status of elderly and senile individuals in Russia.
23.
Aniyozova DZh. The results of a comprehensive assessment of the quality of life of elderly people with chronic diseases. Herald Emerg. Med. 4, 85–87 (2016).
24.
Barsukov VN, Kalachikova ON. Study of the quality of life of the older generation: regional experience. Econ. Soc. Change 4(46), 88–107 (2016).
25.
Bistyaikina D, Palibina A, Pankova E, Soloveva T. Sociological analysis of social well-being of elderly people in the Republic of Mordovia. Kaz. Pedag J. 3(128), 194–198 (2018).
26.
Vechorko VI, Shikina IB. A five-year analysis of the medical and demographic structure of the elderly population served in the hospital center of Moscow and its relationship with disability. Clin. Gerontol. 23(9–10), 11–12 (2017).
27.
Kleeva LP. General demographic situation in Russia and its regions. Bull. Mos. Uni. Fin. Law 1, 38–49 (2020).
Information & Authors
Information
Published In
Pages: 1263 - 1276
PubMed: 36197003
Copyright
© 2022 Future Medicine Ltd.
History
Received: 20 July 2022
Accepted: 12 September 2022
Published online: 5 October 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Development of healthcare and social care services for the elderly population. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0133
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yanru Xiang, Mingyue Xia, Chunhu Zhang, Puwei Chen, Mei Huang, Xingping Dai, Exploring the links between sleep quality and stroke risk in older adults, Scientific Reports, 10.1038/s41598-025-26150-6, 15, 1, (2025).
- Alberto Costantiello, Lucio Laureti, Angelo Quarto, Angelo Leogrande, Methane Emissions in the ESG Framework at the World Level, Methane, 10.3390/methane4010003, 4, 1, (3), (2025).
- Chao Mei, Baoli Xu, Xuefeng Cai, Min Wan, Zhigang Zhao, Yongning Lv, Yu Zhang, Ruxu You, Factors affecting the medication literacy of older adults and targeted initiatives for improvement: a cross-sectional study in central China, Frontiers in Public Health, 10.3389/fpubh.2023.1249022, 11, (2024).