Health economic outcomes of switching to alemtuzumab from other disease-modifying therapies in people with multiple sclerosis in the USA
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Describe demographics, clinical characteristics, healthcare resource utilization (HCRU) and costs in people with multiple sclerosis (pwMS) switching to alemtuzumab from other disease-modifying therapies (DMTs). Patients & methods: Retrospective, observational study of IBM®MarketScan® claims database. PwMS previously treated with DMTs and initiating alemtuzumab (1 January 2013 to 31 December 2019) were identified. “Index” was date of alemtuzumab initiation (prescription filled). Results: The study cohort (n = 341) was primarily female (72%) with (mean ± standard deviation) age 45.1 ± 9.5 years. At index, duration of MS was 5.3 ± 2.8 years. HCRU (inpatient/outpatient services), outpatient costs (including MS-specific MRI and emergency room visits) and annualized relapse rate significantly reduced over the 2 years following initiation of alemtuzumab. DMT costs reduced over the same period. Conclusion: Health economic and clinical benefits were seen following switching to alemtuzumab from other DMTs for treatment of MS, in this cohort from the USA.
Tweetable abstract
Switching to alemtuzumab from existing disease-modifying therapy was associated with significant reduction in healthcare resource utilization and economic outlay over 2-year follow-up in people with relapsing #multiplesclerosis in the USA.
Multiple sclerosis (MS) is an immune-mediated disease characterized by an unpredictable course and a broad clinical spectrum [1,2]. MS is, to date, incurable, and the resulting chronic neurodegeneration leads to disease progression in many individuals [2,3]. Of the MS phenotypes (relapsing remitting multiple sclerosis [RRMS], primary progressive MS [PPMS] and secondary progressive MS [SPMS]), RRMS is the most common and accounts for approximately 85% of the MS population [4]. In 2020, it was estimated that 2.8 million people (35.9 per 100,000) were living with MS worldwide [5,6]. Within the USA alone, MS cases almost doubled from about 470,000 in 2010 to about 900,000 in 2017 [5,7]. The increase in MS prevalence is reflected in other areas of the world, but the absolute prevalence increase reported was largest in the Americas (including Latin America) [5]. At least 50% of people with RRMS progress over approximately 10 years to SPMS [8,9], diagnosed based on a combination of history, a clinical exam, regular magnetic resonance imaging (MRI) and other evaluations [1,4]. The need for ongoing and expensive assessments contributes to the economic burden of MS on society.
Disease-modifying therapies (DMTs) can reduce the number or frequencies of relapses and delay the progression of MS [10–12]; however, persistence with DMTs and adherence to treatment regimens are essential for achieving optimal outcomes [13,14]. Indeed, many people with MS (pwMS) require a change of DMT over the course of their disease due to efficacy or lack of efficacy reasons [14–16]. Alemtuzumab, a humanized monoclonal antibody that targets the CD52 surface proteins on B and T cells, is a highly effective DMT approved for people with relapsing forms of MS (RMS). In two, 2-year, phase III clinical trials (CARE-MS I and II), alemtuzumab demonstrated significantly greater efficacy versus subcutaneous interferon beta-1a and a consistent safety profile in patients with RRMS [17]. Moreover, extension trials of these phase III trials demonstrated that the efficacy of alemtuzumab was maintained over 4 years of additional follow-up [18]. Alemtuzumab requires less frequent administration (five intravenous infusions over five consecutive days followed by a second course after 12 months of three infusions over three consecutive days [19]) than most intravenous DMTs and, therefore, may be associated with improved patient compliance. HCRU and economic outcomes are important factors in treatment decisions that should be considered alongside efficacy and safety benefits. Claims data facilitate assessment over a longer term, given that MS has an unpredictable disease course and prolonged remission is the primary aim of treatment with currently available DMTs [20]. At present, however, there is a lack of data on the health economic value of pwMS changing their therapy regimen to alemtuzumab from existing therapy with other DMTs. This retrospective study of claims data from the USA assessed characteristics, healthcare resource utilization (HCRU) and annual relapses in pwMS who switched to alemtuzumab treatment from other existing DMTs for RMS.
Population & methods
Study design & data source
This was a retrospective, observational study of pwMS who were treated with a DMT before switching to alemtuzumab therapy between 1 January 2013 and 31 December 2019 (Supplementary Figure 1). Switching was defined as initiation of alemtuzumab after any prior DMT. Data were extracted from IBM® MarketScan®, a USA claims database that includes data from a selection of large employers, health plans, government and public organizations and captures person-specific clinical utilization, expenditures and enrollment across inpatient, outpatient, prescription drug and carveout services. Eligible individuals were followed for 2 years after the index date (i.e., after initiation of alemtuzumab) due to the dosing schedule of alemtuzumab (Supplementary Figure 1).
Sample selection
Eligible individuals were aged ≥18 years; had a diagnosis of MS (International Classification of Diseases 9th/10th revision [ICD-9, ICD-10] codes: 340 or G35, respectively); received ≥1 DMT before switching to alemtuzumab; and had ≥12 months of continuous enrollment before and after the index date (allowing for a 30-day gap in enrollment). PwMS were excluded if they had <1 year of continuous enrollment prior to or after index date and if they had not received any DMTs before switching to alemtuzumab.
Outcome measures
Study outcomes of interest included demographics and clinical characteristics (comorbidities and MS symptoms), DMTs and concomitant medications (longitudinal prescription claims), inpatient and emergency room (ER) claims coinciding with a primary or secondary diagnosis of MS, and hospitalization or outpatient claims coinciding with a primary or secondary diagnosis of MS to determine the number of relapses. MS-related healthcare costs were captured based on pharmacy, inpatient, or procedure claims for DMTs or concomitant medications for MS treatments, using National Drug Code directory and/or J-code (i.e., for therapies administered in office) and infusion procedures via current procedural terminology codes. For baseline demographics, clinical characteristics, HCRU and relapse rate, a lookback period of 1 year prior to index was used. For prior DMT use, a lookback period of 2 years was used to ensure that the assessment was as comprehensive as possible. For clinical characteristics, HCRU and relapse rate, follow-up was reported at 1 year and 2 years after index.
Surrogate parameters, described previously in the literature [21–24], were used to indirectly measure relapses from the claims data. A relapse was assumed if at least one of the following criteria were met: hospitalization with MS as the main discharge diagnosis (if a urinary tract infection, cystitis, or pneumonia was documented as a secondary diagnosis, a pseudo-relapse was assumed and not considered as a relapse); hospitalization associated with MS as secondary diagnosis and use of corticosteroid therapy during the hospital stay; outpatient diagnosis of MS and a pharmacy claim for corticosteroid therapy within 7 days or a medical claim for intravenous methylprednisolone or injection of adrenocorticotropic hormone.
Statistical analyses
Categorical variables were summarized by frequency and percentage; continuous variables were summarized by mean (standard deviation [SD]) and median (range or interquartile range [IQR]). Descriptive analyses were conducted to summarize the number of pwMS in each DMT and sequence of DMTs.
Total healthcare costs included pharmacy, medical, inpatient and outpatient costs. Per person per year (PPPY) costs (mean costs/mean year of follow-up) were estimated by dividing the mean cost for each individual in the cohort (total cost/total number of patients) by the mean number of years that each individual in the cohort contributed to follow-up, i.e., 1-year pre-index versus 1 or 2 years post-index, (total patient-years/total number of patients). HCRU event rates were calculated by dividing the mean number of events for the cohort by the mean number of years of follow-up for the cohort, i.e., 1-year pre-index versus 1 or 2 years post-index. Event rates were expressed as the number of events per 100 patient-years. Mean cost per event (mean costs/mean year of follow-up) was calculated by dividing the cumulative costs of all events (total cost/total number of events) by the total number of events occurring during follow-up (total events/total patient-years of follow-up). All costs were adjusted for inflation to 2020 US$ using the annual medical care component of the Consumer Price Index [25].
Annualized relapse rate (ARR) 1-year pre-index date and for cumulative years after the index date was compared using Poisson or negative binomial regression models. The total number of relapses was the dependent variable and treatment period (pre-index or post-index) was the covariate. The log of time (in years) of follow-up to 1-year prior to index date and post-index date was the offset variable.
Results
Demographics & clinical characteristics
Of individuals in the database with an MS diagnosis, the final eligible study sample included 341 pwMS who had continuous enrollment and received ≥1 DMT before initiating alemtuzumab (Figure 1). The majority were female (72% [n = 247]; Table 1). At initiation of alemtuzumab, mean ± SD age of the study population was 45.1 ± 9.5 years and average length of MS diagnosis was 5.3 ± 2.8 years (Table 1).
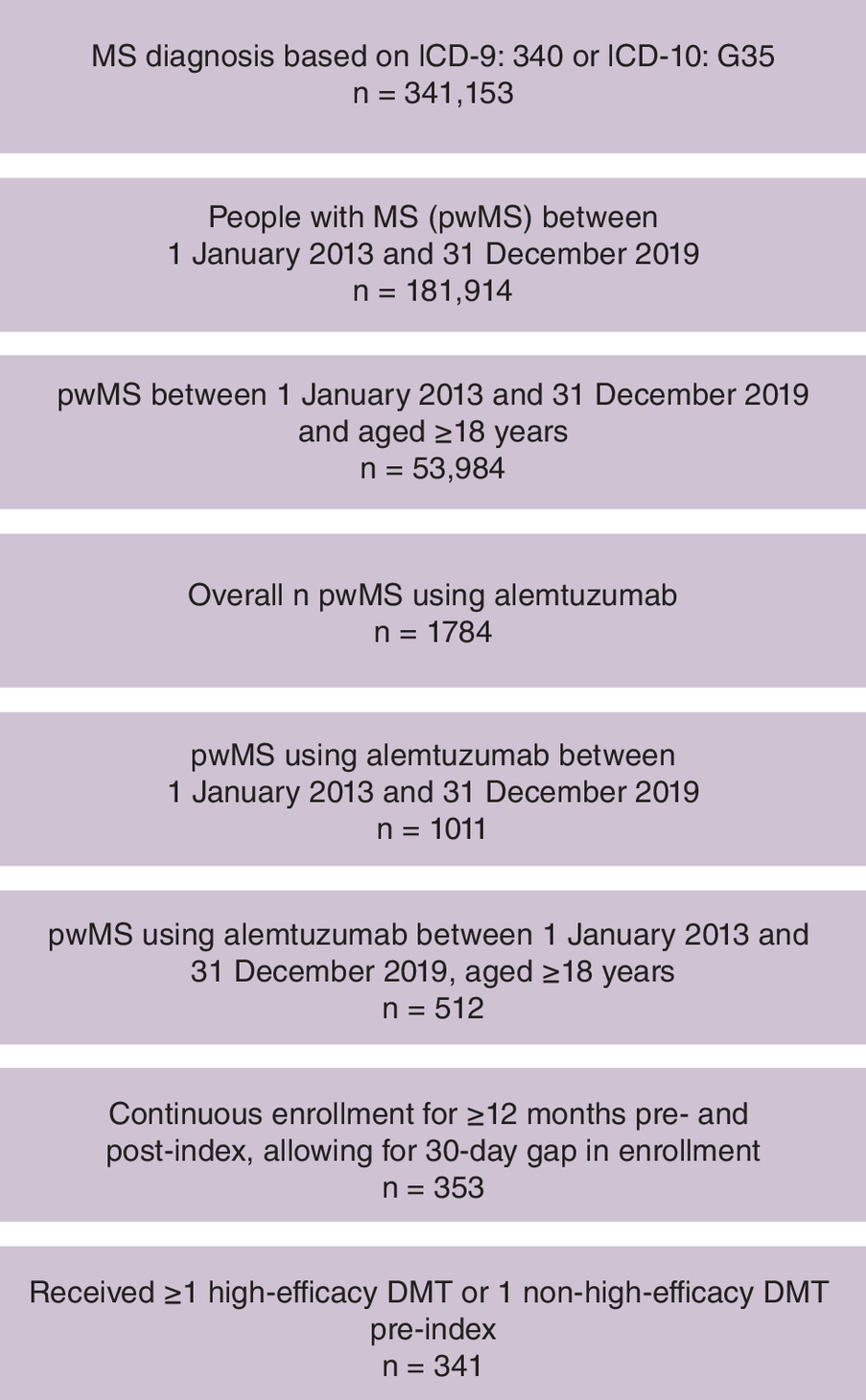
Figure 1. Subject attrition from IBM® MarketScan® database.
DMT: Disease-modifying therapy; ICD-9: International Classification of Diseases 9th revision; ICD-10: International Classification of Diseases 10th revision; MS: Multiple sclerosis; pwMS: People with multiple sclerosis.
| Characteristic | Patients, n = 341 |
|---|---|
| Age at index, years, mean ± SD | 45.1 ± 9.5 |
| Age group, years, n (%) | |
| 18–34 | 56 (16.4) |
| 35–44 | 107 (31.4) |
| 45–54 | 116 (34.0) |
| 55–64 | 60 (17.6) |
| 65+ | 2 (0.6) |
| Age at MS diagnosis, years, mean ± SD | 40.5 ± 9.2 |
| Duration of disease, years, mean ± SD | 5.3 ± 2.8 |
| Sex, n (%) | |
| Female | 247 (72) |
| USA geographic region, n (%) | |
| North Central | 62 (18.2) |
| Northeast | 47 (13.8) |
| South | 186 (54.5) |
| West | 46 (13.5) |
| Insurance coverage plan, n (%) | |
| PPO | 192 (56.3) |
| CDHP | 55 (16.1) |
| HDHP | 32 (9.4) |
| HMO | 21 (6.2) |
| Other† | 41 (12.0) |
| Comorbid conditions in 1-year pre-index period, n (%)‡ | |
| Hypertension | 89 (26.2) |
| Urinary tract infections | 61 (17.9) |
| Hyperlipidemia | 42 (12.4) |
| Unspecified acquired hypothyroidism | 34 (10.0) |
| Diabetes | 25 (7.4) |
| Neuropathic pain | 14 (4.1) |
| Fibromyalgia/myalgia and myositis | 12 (3.5) |
| Arthritis§ | 7 (2.1) |
| Charlson Comorbidity Index, mean ± SD | 0.4 ± 0.93 |
| Common Symptoms, n (%)‡ | |
| Muscle weakness | 67 (19.7) |
| Spasticity | 50 (14.7) |
| Headache (migraine) | 47 (13.8) |
| Malaise and fatigue | 42 (12.4) |
| Urinary incontinence | 40 (11.8) |
| Anxiety | 35 (10.3) |
| Dizziness | 21 (6.2) |
| Diplopia | 13 (3.8) |
| Optic neuritis | 11 (3.2) |
| MDD and depressive disorders | 7 (2.1) |
| Trigeminal neuralgia | 5 (1.5) |
| Ataxia | 4 (1.2) |
| Cognitive impairment | 3 (0.9) |
| Tremor | 2 (0.6) |
Data are mean ± SD or n (%).
†
Exclusive Provider Organization, comprehensive, POS plan with capitation, POS plan or other.
‡
n = 341 for pre-index comorbidities and symptoms.
§
Includes rheumatoid arthritis and osteoarthritis.
CDHP: Consumer-driven health plan; HDHP: High-deductible health plan; HMO: Health Maintenance Organization; POS: Point of service; PPO: Preferred-provider organization; SD: Standard deviation.
Treatment patterns prior to switching to alemtuzumab
Most of the study population who were treated with a DMT within both the 1-year and 2-year pre-index periods were treated with only 1 DMT before switching to alemtuzumab (n = 248/278 [89.2%] and n = 277/336 [82.4%], respectively). Of the remainder, prior to initiating alemtuzumab, 10.1% (n = 28; 1-year pre-index) and 26.8% (n = 90; 2-year pre-index) were prescribed 2 DMTs and 0.7% (n = 2; 1-year pre-index) and 5.7% (n = 19; 2-year pre-index) were prescribed ≥3 DMTs. For the analysis of DMTs 1 year prior to index (i.e., prior to initiation of alemtuzumab), the total number of patients did not total 341, as some patients stopped their DMT for more than 1 year prior to initiating alemtuzumab. Therefore, these patients were not captured within the 1-year pre-index period; however, they were still eligible for the primary analysis, as they used a DMT within the pre-index period (to 1 January 2013).
During the 2-year follow-up period, 69.5% (n = 237/341) of the study population received 2 courses of alemtuzumab treatment, as per the dosing schedule on the prescribing label [19]. In total, 91/341 (26.7%) received only 1 course of treatment and the remainder (3.8% [n = 13/341]) received a third course of treatment at 2 years follow-up.
Most commonly used DMTs prior to switching to alemtuzumab were natalizumab and dimethyl fumarate. Natalizumab was also the DMT used for the longest time prior to switching to alemtuzumab (mean ± SD treatment duration) 1-year pre-index (250 ± 81 days) and 2-year pre-index (457 ± 180 days), followed by fingolimod (249 ± 74 days and 347 ± 188 days, respectively) and dimethyl fumarate (195 ± 110 days and 354 ± 222 days, respectively; Supplementary Table 1).
Healthcare resource utilization & costs following switching to alemtuzumab
All-cause length of hospital stay was reduced by a median of 1 day from 1-year pre-index to 2-years post-index (median [IQR 25–75]: 4 [3–11] days vs 3 [2–10] days, respectively). Similar observations were seen for MS-specific length of hospital stay (1-year pre-index: 5 [3–11] days; 2-years post-index: 4 [2–11]), although significance was not assessed. Utilization of outpatient services and inpatient visits were also generally reduced from 1-year pre-index to 2-years post-index for both all-cause and MS-specific healthcare services (Table 2). For all-cause services, utilization of ER visits, MRI visits and laboratory tests were significantly reduced from 1-year pre-index to 2-years post-index (p < 0.001); similarly, for MS-specific services: MS therapy visits and MRI visits were significantly reduced from 1-year pre-index to 2-years post-index (p < 0.001 and p < 0.0001, respectively; Table 2).
| Healthcare resource utilization | 1-year pre-index | 1-year post-index | p-value | 2-year post-index | p-value |
|---|---|---|---|---|---|
| All-cause services (event rate per 100 person-year) | |||||
| Outpatient visits per person | 0.300 | 0.280 | 0.079 | 0.277 | 0.003 |
| ER visits | 0.0056 | 0.0060 | 0.367 | 0.0057 | <0.0001 |
| Therapy visits‡ | 0.059 | 0.051 | 0.952 | 0.052 | <0.0001 |
| MRI visits | 0.018 | 0.012 | <0.0001 | 0.012 | <0.0001 |
| Laboratory services | 0.072 | 0.061 | 0.003 | 0.060 | <0.0001 |
| Inpatient visits | 0.011 | 0.009 | 0.752 | 0.010 | 0.014 |
| MS-specific services (event rate per 100 person-year) | |||||
| Outpatient visits per person | 0.159 | 0.139 | 0.005 | 0.131 | <0.0001 |
| ER visits | 0.0024 | 0.0025 | 0.738 | 0.0023 | 0.762 |
| Therapy visits‡ | 0.0260 | 0.0260 | 0.474 | 0.0244 | <0.001 |
| MRI visits | 0.016 | 0.010 | <0.0001 | 0.010 | <0.0001 |
| Laboratory services | 0.035 | 0.023 | <0.0001 | 0.021 | 0.257 |
| Inpatient visits | 0.009 | 0.0048 | 0.152 | 0.006 | 0.297 |
| Healthcare costs† | |||||
|---|---|---|---|---|---|
| All-cause services, $ PPPY | |||||
| Outpatient visits | 10,792 | 9844 | 0.052 | 9560 | 0.010 |
| ER visits | 687 | 881 | 0.550 | 832 | <0.001 |
| Therapy visits‡ | 930 | 623 | 0.840 | 701 | <0.001 |
| MRI visits | 2739 | 1907 | <0.0001 | 1660 | < 0.0001 |
| Laboratory services | 906 | 684 | <0.0001 | 714 | 0.005 |
| Inpatient visits | 2909 | 3312 | 0.994 | 3909 | 0.002 |
| MS-specific services, $ PPPY | |||||
| Outpatient visits | 5876 | 5278 | 0.553 | 4851 | <0.0001 |
| ER visits | 236 | 376 | 0.678 | 324 | 0.466 |
| Therapy visits‡ | 411 | 380 | 0.813 | 406 | 0.002 |
| MRI visits | 2451 | 1701 | <0.0001 | 1463 | < 0.0001 |
| Laboratory services | 479 | 241 | <0.0001 | 254 | 0.001 |
| Inpatient visits | 1999 | 1017 | 0.190 | 1356 | 0.413 |
All costs were adjusted to 2020 USA$ using the healthcare component of the Consumer Price Index.
†
Total amount paid by insurance.
‡
Includes physical, occupational, speech, and rehabilitation therapies, and some therapies may have been claimed as an inpatient visit.
ER: Emergency room; MRI: Magnetic resonance imaging; MS: Multiple sclerosis; PPPY: Per person per year.
The average healthcare cost per person at index was $26,022, with costs for alemtuzumab (over the 5-day course of administration and including any administrative costs) at $23,490 (Supplementary Table 2). All-cause PPPY costs were significantly decreased from 1-year pre-index to 2-years post-index for outpatient visits, including MS therapy visits, MRIs and laboratory tests (p = 0.01) but were significantly increased for ER visits (p < 0.001) and inpatient visits over the same period (p = 0.002; Table 2). PPPY costs for MS specific outpatient visits significantly reduced over the same period, alongside therapy visits, laboratory services and costs for MRI visits (Table 2). There was no change in MS-specific PPPY costs for inpatient visits.
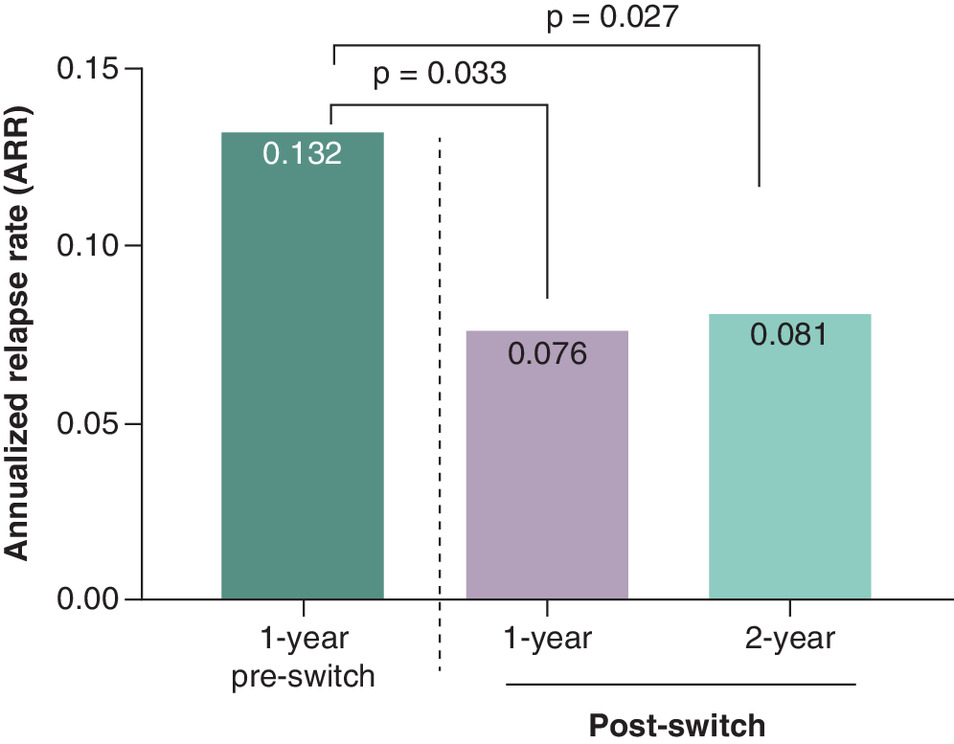
Total PPPY DMT costs (including pharmacy claims and medical prescription claims in the outpatient and inpatient setting) and the overall PPPY costs of treating MS were reduced 2 years after switching to alemtuzumab (Figure 2). For example, PPPY total prescription costs reduced by $12,632 (from $64,294 1-year prior to switching to $51,662 2-years post-index). A similar pattern was observed for MS-specific prescription costs (from $49,015 to $41,292; Figure 2). Overall, ARR significantly reduced from 1-year pre-index to 1- and 2-year post-index periods (p = 0.033 and 0.027, respectively; Figure 3).
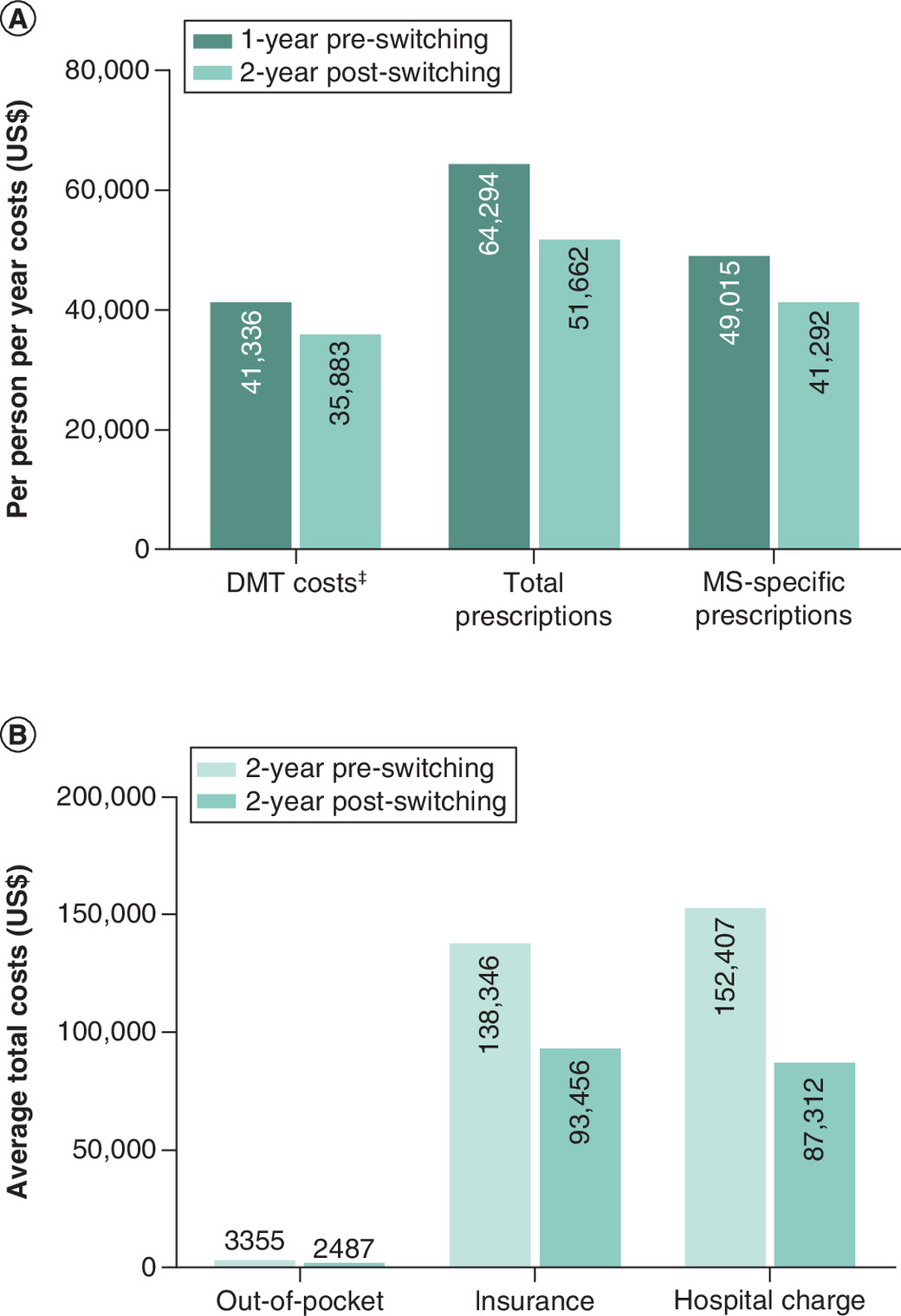
Figure 2. Multiple sclerosis treatment costs.
(A) Cost of multiple sclerosis treatments per person per year*. (B) Average total cost of treating multiple sclerosis, as paid by payers, in 2-years pre- and post-switching to alemtuzumab†.
*Costs do not include the first course of alemtuzumab; this was considered at index date. †All costs adjusted to 2020 USA$ using the healthcare component of the Consumer Price Index [25]. ‡DMT costs include pharmacy claims and medical prescription claims in the outpatient and inpatient setting.
DMT: Disease-modifying therapy; MS: Multiple sclerosis.
Discussion
Using data from commercially insured population from the USA, we found that MS-specific HCRU for outpatient and inpatient services were significantly reduced for the 2-year period after pwMS initiated alemtuzumab treatment. A reduction in healthcare costs was also seen, for both all-cause and MS-specific services (particularly MRI and laboratory services), although costs associated with all-cause inpatient visits/services increased. The increase in costs associated with inpatient visits/services could potentially include the infusion costs of alemtuzumab itself considering that the infusion must be performed in a hospital or infusion center setting. Short-term (1-year) reductions in average PPPY costs, including out-of-pocket costs and hospital charges, were also seen, including reduced PPPY total costs over the longer (2-year) term. Collectively, our observations demonstrate that switching to alemtuzumab therapy was generally associated with favorable economic reductions in both MS-related and overall HCRU and in total and PPPY costs for these pwMS.
As MS is a life-long disease, it is associated with a considerable economic burden and additional HCRU and costs are incurred every time a patient switches from one DMT to another [26,27]. Therefore, ensuring that pwMS find a well-tolerated and cost-effective DMT early in their treatment trajectory is a priority, not only for the individual but also for the healthcare providers and the healthcare system as a whole. In this real-world analysis, HCRU and other costs were reduced over the 2-year period after the pwMS initiated alemtuzumab. These reductions in cost were likely due to the infrequent dosing regimen of alemtuzumab and the reduction in relapses leading to reduced need for acute visits. Of note, natalizumab was the most commonly used DMT prior to switching (41% were prescribed natalizumab during the 1-year pre-index period) and the treatment regimen for natalizumab involves a monthly, not yearly, infusion, as is the case for alemtuzumab. Although we did not specifically compare drug versus drug, this change in treatment regimen may have been a key driver behind the reduction in HCRU and laboratory visits (and associated costs) seen post-switching, due to the change in frequency of infusion visits and associated tests. However, other key factors were also driving costs; for example, costs associated with MRI visits reduced by $750 PPPY within 1-year of switching to alemtuzumab. Most of the study population (70%) remained on alemtuzumab throughout the 2-year follow-up period, and received the standard, pre-defined two courses [19], with 27% receiving one course and the remainder (4%) receiving a third dose during the 2-year post-index period. This suggests that the efficacy of alemtuzumab was maintained over the 2-year post-index period as those pwMS not achieving a sufficient response to treatment would be expected to discontinue from treatment or request a further course of treatment. These findings add to those of a previous 8-year post-hoc analysis of the randomized phase III CARE-MS studies showing that 48–53% of pwMS across age cohorts (ranging from 18 to 55 years) received no additional alemtuzumab or DMT beyond the 2-year core study period, and approximately 70% of pwMS remained in the study and received alemtuzumab throughout 8-years of follow-up [28].
In the present study, most pwMS (89.2%) had used only one other DMT prior to initiating alemtuzumab and the DMT used most frequently was natalizumab, as noted above. The importance of the number of DMTs used prior to switching to alemtuzumab (and in which sequence) has been highlighted in previous literature [29], because the therapeutic response and susceptibility for developing secondary autoimmunity in pwMS initiating alemtuzumab is associated with the number and sequence of previous DMTs. Moreover, there is a risk for outcomes potentially being greater with increasing numbers of previous DMTs, such as with previous use of fingolimod [29]. Findings from the current study indicate that healthcare professionals were following contemporary practice guidelines in the USA and prescribing alemtuzumab after only one previous DMT [20]. Furthermore, the observation that pwMS were switching from 1 high efficacy DMT to another high efficacy DMT suggests that the switch was most likely due to efficacy or safety reasons. Overall, initiating treatment with a high efficacy DMT, such as alemtuzumab, early in the disease trajectory may prevent the need to switch DMT so frequently, thereby reducing overall HCRU and healthcare costs, as indicated by the economic observations in the current study.
People with MS have a broad range of disease presentations and traditional assessment of efficacy in clinical trials is through monitoring of relapses (ARR) and/or changes in the Expanded Disability Status Scale (EDSS) [30]. Unfortunately, no EDSS data were available in the current dataset to indicate disease activity. Clinical outcomes are not reported in claims data and therefore proxy assessments, as the ones used in the current study, are often used to evaluate relapses rather than assessments commonly used in clinical trials. By assessing relapses we demonstrated that switching to alemtuzumab was associated with a significant reduction in ARR and this provided a comparative assessment in the real world with efficacy trials of alemtuzumab versus other DMTs for the treatment of MS [17,18,31,32]. The importance of reducing relapse rates in MS has been highlighted previously [22,33,34]. High relapse rates are associated with higher HCRU and are predictive of treatment-experienced pwMS switching DMT [22,35]. The reduction in ARR following initiation with alemtuzumab may explain the reduction in HCRU observed during the 2-year post-index period in this study. Indeed, with fewer relapses, pwMS receiving alemtuzumab may be more likely to remain compliant with their treatment and less likely to switch to other DMTs, thereby reducing future costs and allowing them to remain on stable therapy.
Some additional considerations should be highlighted when interpreting our study. First, as with all claims-data studies, individuals may have been misclassified due to misdiagnosis or miscoding; therefore, it is possible that not all pwMS switching to alemtuzumab were captured in our dataset. Not all disease entities and variables have their own billing codes; therefore, information on points of interest can be limited when conducting claims-data research. For example, information on MS phenotype and race or ethnicity were not available in the database and therefore not included in this analysis. Some pwMS were lost to follow-up due to noncontinuous enrollment between 1 year pre- and 1-year post-index. Unlike other biologics with different treatment schedules, alemtuzumab has a 2-year administration period. The first course of study drug is administered over five consecutive days, followed by no treatment for 12 months and then a three-day course of drug. This study was designed to include a 2-year post-index period, given the dosing schedule of alemtuzumab as outlined above [19]. Of further note, since pwMS were included up to December 2019 only, the study was not impacted by the COVID-19 pandemic. This is particularly relevant for pwMS receiving alemtuzumab, as they are required to visit an infusion center or hospital for treatment administration, and this may have been disrupted during the COVID-19 pandemic period from March 2020 onward. Finally, as hospitalization and corticosteroid use were used as proxies to determine number of relapses and calculate ARR, only moderate-to-severe relapses (and not mild) were included in the calculation of ARR. Despite the lack of data on mild relapses, our study did demonstrate that alemtuzumab reduced moderate-to-severe MS relapses and these are obviously of greater burden to pwMS, healthcare providers and the healthcare system. Due to the nature of data collection in this study, EDSS scores were not available to assess disability progression as a measure of MS disease status. Despite these limitations, our study demonstrates that significant reductions in HCRU and some costs are associated with switching to alemtuzumab therapy, particularly from other high-efficacy DMTs (e.g., fingolimod, ocrelizumab and natalizumab) for individuals with RMS.
Conclusion
This retrospective analysis of claims data from the USA demonstrate the economic benefits of switching to alemtuzumab from other DMTs in the treatment of RMS. Moreover, the efficacy of alemtuzumab demonstrated in clinical trials has been translated into real-world effectiveness, with corresponding reductions in MS-related HCRU and cost savings associated with MS relapses when people with MS switch to an alemtuzumab treatment regimen.
•
Switching to alemtuzumab from existing disease-modifying therapy (DMT) was associated with significant reduction in healthcare resource utilization and economic outlay in people with multiple sclerosis (pwMS).
•
pwMS who switched to alemtuzumab from existing DMTs also experienced a significant reduction in annualized relapse rate over the 2 years following a switch in treatment regimen.
•
Given the long-term nature of MS and the economic burden it places on individuals and healthcare providers, this study demonstrates the overall economic benefits of alemtuzumab therapy for relapsing MS in the USA.
Author contributions
All authors were involved in the design and conduct of the study, and in interpreting the data. All authors were involved in drafting the manuscript and revising it critically for intellectual content. All authors had access to the study data.
Acknowledgments
The authors are grateful to N Roesch (Medical Director Neurology of Sanofi) for her contributions to aspects of the study design and feedback on measure of relapses.
Financial & competing interests disclosure
This study was funded by Sanofi. L Araujo, K Higuchi and N Greene are employees of Sanofi and may hold stock or stock options. KG Bzdek was an employee of Sanofi at the time of the study. S Kyatham was an employee of Axtria at the time of the study. Axtria were paid consultants to Sanofi in relation to this project. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was provided by K Burrows of CURO (part of Envision Pharma Group) and was funded by Sanofi.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 205.51 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Lublin FD, Coetzee T, Cohen JA, Marrie RA, Thompson AJ. The 2013 clinical course descriptors for multiple sclerosis: a clarification. Neurology 94(24), 1088–1092 (2020).
2.
Lublin FD, Reingold SC, Cohen JA et al. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology 83(3), 278–286 (2014).
3.
Thompson AJ, Banwell BL, Barkhof F et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 17(2), 162–173 (2018).
4.
Klineova S, Lublin FD. Clinical Course of Multiple Sclerosis. Cold Spring Harb. Perspect. Med. 8(9), a028928 (2018).
5.
Walton C, King R, Rechtman L et al. Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS, third edition. Mult. Scler. 26(14), 1816–1821 (2020).
6.
Multiple Sclerosis International Federation. Atlas of MS (3rd Edition): mapping multiple sclerosis around the world key epidemiology findings (2021). www.msif.org/wp-content/uploads/2020/10/Atlas-3rd-Edition-Epidemiology-report-EN-updated-30-9-20.pdf
7.
Wallin MT, Culpepper WJ, Campbell JD et al; Us Multiple Sclerosis Prevalence Workgroup. The prevalence of MS in the United States: a population-based estimate using health claims data. Neurology 92(10), e1029–e1040 (2019).
8.
Cree BaC, Arnold DL, Chataway J et al. Secondary Progressive Multiple Sclerosis: New Insights. Neurology 97(8), 378–388 (2021).
9.
Weinshenker BG, Bass B, Rice GP et al. The natural history of multiple sclerosis: a geographically based study. I. Clinical course and disability. Brain 112(Pt 1), 133–146 (1989).
10.
Beiki O, Frumento P, Bottai M, Manouchehrinia A, Hillert J. Changes in the risk of reaching multiple sclerosis disability milestones in recent decades: a nationwide population-based cohort study in Sweden. JAMA Neurol. 76(6), 665–671 (2019).
11.
Goodin DS, Reder AT, Ebers GC et al. Survival in MS: a randomized cohort study 21 years after the start of the pivotal IFNβ-1b trial. Neurology 78(17), 1315–1322 (2012).
12.
Smith AL, Cohen JA, Hua LH. Therapeutic targets for multiple sclerosis: current treatment goals and future directions. Neurotherapeutics 14(4), 952–960 (2017).
13.
Bergvall N, Makin C, Lahoz R et al. Relapse rates in patients with multiple sclerosis switching from interferon to fingolimod or glatiramer acetate: a US claims database study. PLOS ONE 9(2), e88472 (2014).
14.
Bergvall N, Petrilla AA, Karkare SU et al. Persistence with and adherence to fingolimod compared with other disease-modifying therapies for the treatment of multiple sclerosis: a retrospective US claims database analysis. J. Med. Econ. 17(10), 696–707 (2014).
15.
Grand'maison F, Yeung M, Morrow SA et al. Sequencing of high-efficacy disease-modifying therapies in multiple sclerosis: perspectives and approaches. Neural. Regen. Res. 13(11), 1871–1874 (2018).
16.
Alroughani R, Van Wijmeersch B, Al Khaboori J et al. The use of alemtuzumab in patients with relapsing-remitting multiple sclerosis: the Gulf perspective. Ther. Adv. Neurol. Disord. 13, 1756286420954119 (2020).
17.
Cohen JA, Coles AJ, Arnold DL et al. Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis: a randomised controlled phase 3 trial. Lancet 380(9856), 1819–1828 (2012).
18.
Coles AJ, Arnold DL, Bass AD et al. Efficacy and safety of alemtuzumab over 6 years: final results of the 4-year CARE-MS extension trial. Ther. Adv. Neurol. Disord. 14, 1756286420982134 (2021).
19.
Sanofi. LEMTRADA®(alemtuzumab) injection, for intravenous use [prescribing information] (2022). https://products.sanofi.us/lemtrada/lemtrada.pdf
20.
Rae-Grant A, Day GS, Marrie RA et al. Practice guideline recommendations summary: disease-modifying therapies for adults with multiple sclerosis: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 90(17), 777–788 (2018).
21.
Ohlmeier C, Gothe H, Haas J et al. Epidemiology, characteristics and treatment of patients with relapsing remitting multiple sclerosis and incidence of high disease activity: real world evidence based on German claims data. PLOS One 15(5), e0231846 (2020).
22.
Raimundo K, Tian H, Zhou H et al. Resource utilization, costs and treatment patterns of switching and discontinuing treatment of MS patients with high relapse activity. BMC Health Serv. Res. 13, 131 (2013).
23.
Ollendorf DA, Jilinskaia E, Oleen-Burkey M. Clinical and economic impact of glatiramer acetate versus beta interferon therapy among patients with multiple sclerosis in a managed care population. J. Manag. Care Pharm. 8(6), 469–476 (2002).
24.
Chastek BJ, Oleen-Burkey M, Lopez-Bresnahan MV. Medical chart validation of an algorithm for identifying multiple sclerosis relapse in healthcare claims. J. Med. Econ. 13(4), 618–625 (2010).
25.
U.S. Bureau of Labor Statistics. CPI Medical care services (2013–2020)(2021). www.bls.gov/cpi/data.html
26.
Paz-Zulueta M, Parás-Bravo P, Cantarero-Prieto D, Blázquez-Fernández C, Oterino-Durán A. A literature review of cost-of-illness studies on the economic burden of multiple sclerosis. Mult. Scler. Relat. Disord. 43, 102162 (2020).
• This literature review focusing on the cost of illness in multiple sclerosis (MS) highlights the main cost determinants for patients with less severe MS as due to the costs of drugs, with costs incurred from informal care or production losses being more attributable in severe cases of MS.
27.
Freeman L, Kee A, Tian M, Mehta R. Retrospective claims analysis of treatment patterns, relapse, utilization, and cost among patients with multiple sclerosis initiating second-line disease-modifying therapy. Drugs Real World Outcomes 8(4), 497–508 (2021).
•• This study highlighted poor adherence and non-persistence of patients with MS switching to a second disease-modifying therapy, and one-third of patients relapsed within 12-months of switching.
28.
Bass AD, Arroyo R, Boster AL et al; Care-Ms I C-MI, CAMMS03409, and TOPAZ Investigators. Alemtuzumab outcomes by age: post hoc analysis from the randomized CARE-MS studies over 8 years. Mult. Scler. Relat. Disord. 49, 102717 (2021).
29.
Pfeuffer S, Ruck T, Pul R et al. Impact of previous disease-modifying treatment on effectiveness and safety outcomes, among patients with multiple sclerosis treated with alemtuzumab. J. Neurol. Neurosurg. Psychiatry 92(9), 1007–1013 (2021).
30.
Zhang Y, Salter A, Wallström E, Cutter G, Stüve O. Evolution of clinical trials in multiple sclerosis. Ther. Adv. Neurol. Disord. 12, 1756286419826547 (2019).
31.
Arnold DL, Fisher E, Brinar VV et al. Superior MRI outcomes with alemtuzumab compared with subcutaneous interferon β-1a in MS. Neurology 87(14), 1464–1472 (2016).
32.
Zhang J, Shi S, Zhang Y et al. Alemtuzumab versus interferon beta 1a for relapsing-remitting multiple sclerosis. Cochrane Database Syst. Rev. 11(11), CD010968 (2017).
33.
Bonafede MM, Johnson BH, Watson C. Health care-resource utilization before and after natalizumab initiation in multiple sclerosis patients in the US. Clinicoecon. Outcomes Res. 6, 11–20 (2013).
34.
Nicholas J, Boster A, Wu N et al. Comparison of disease-modifying therapies for the management of multiple sclerosis: analysis of healthcare resource utilization and relapse rates from US insurance claims data. Pharmacoecon. Open 2(1), 31–41 (2018).
•• This study sought to provide a more accurate representation of cost burden associated with MS relapse, and found that cost drastically increased with the severity of relapse underscoring the need to manage relapses with high-efficacy treatments.
35.
Nicholas J, Zhou H, Deshpande C. Annual cost burden by level of relapse severity in patients with multiple sclerosis. Adv. Ther. 38(1), 758–771 (2021).
• This analysis of patients taking disease-modifying therapies found they were associated with reductions in healthcare utilization and non-prescription costs. Similar to our analysis, cost reductions were largely driven by reductions in the use of outpatient services and inpatient hospital visits.
Information & Authors
Information
Published In
Copyright
© 2022 Sanofi. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 14 July 2022
Accepted: 14 October 2022
Published online: 28 November 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Health economic outcomes of switching to alemtuzumab from other disease-modifying therapies in people with multiple sclerosis in the USA. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0127
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Sophia Woodson, Edward J. Gettings, Chu-Yueh Guo, Sylvia Klineova, Jong-Mi Lee, Rebecca S. Romero, Aljoeson Walker, Kinyee Fong, Jason P. Mendoza, Nicholas Belviso, Boyang Bian, James B. Lewin, Sai L. Shankar, Real-World Treatment Outcomes in Black, Hispanic, Asian, and White People with Multiple Sclerosis Treated with Fumarates in the USA, Neurology and Therapy, 10.1007/s40120-025-00773-3, 14, 4, (1641-1656), (2025).
- Jeremy W. Jacobs, Thomas C. Binns, Danielle Schlafer, Jennifer S. Woo, Garrett S. Booth, Brian D. Adkins, Alemtuzumab and thrombotic thrombocytopenic purpura: Analysis of an international surveillance database and systematic literature review, Transfusion and Apheresis Science, 10.1016/j.transci.2025.104081, 64, 2, (104081), (2025).
- Aliza B Ben-Zacharia, Jenny J Feng, Brandon P Moss, Nicholas Belviso, Filipe Branco, Jason P Mendoza, James B Lewin, Clinical characteristics and treatment outcomes in multiple sclerosis patients treated with anti-CD20s who switched to fumarates: a retrospective analysis of a US healthcare claims database, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0071, 14, 3, (2025).