Real-world weight changes in people with HIV-1 at risk of weight gain (female, Black or Hispanic) switching from integrase strand transfer inhibitors
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Compare weight changes between people living with HIV-1 (PLWH) at high risk of weight gain (females, Blacks or Hispanics) switching from an integrase strand transfer inhibitor (INSTI) to a protease inhibitor (PI) or another INSTI. Materials & methods: Mean weight changes from pre-switch to up-to-12 months post-switch were retrospectively compared between PLWH switching to a PI or INSTI. Results: 356 PLWH were eligible. At 9- and 12-month post-switch, weight increases were observed for INSTI (weight: +1.55 kg and +1.59 kg), while decreases were observed for PI (-0.23 kg and -1.59 kg); differences between cohorts widened over time. Conclusion: These data suggest that switching off an INSTI may be a management tool to mitigate or reverse weight gain.
Tweetable abstract
ART management may be an option to mitigate or reverse weight gain following initial INSTI treatment among female, Black or Hispanic PLWH who have a higher risk of weight gain.
The introduction of antiretroviral therapy (ART) for HIV-1 has significantly improved clinical outcomes and quality of life [1–4]. With life expectancy improving among people living with HIV-1 (PLWH) in the USA, there has been an increase in the prevalence of diseases associated with aging among PLWH [5]. Related to this, weight gain is also now emerging as an important consideration, especially given the link between higher weight and comorbidities such as cardiometabolic conditions in the general population [6,7]. While an increasing trend in BMI (23.8 kg/m2 in 1998 and 24.8 kg/m2 in 2010) and the proportion of obese PLWH initiating ART (9% in 1998 and 18% in 2010) has been observed among PLWH over time [8], ART itself has also been associated with increased weight gain in PLWH [9,10]. It has been reported that factors such as diabetes, multiple comorbidities and low neutrophils/lymphocytes ratio are independent predictors of being overweight or obese in PLWH over 50 years of age receiving ART [11]. Furthermore, certain populations such as females, Blacks or Hispanics have been observed to experience greater ART-related weight gain [12,13] than other populations.
The US Department of Health and Human Services (DHHS) guidelines generally recommend ART regimens containing an integrase strand transfer inhibitor (INSTI) for the majority of PLWH initiating ART [14]. Protease inhibitors (PIs) are also recommended in specific PLWH populations such as those at risk of non-adherence or those who initiate treatment rapidly without baseline laboratory and resistance testing results [14]. Although INSTIs are recommended for most PLWH, guidelines from the US DHHS underline a greater risk of weight gain associated with INSTI-based regimens compared with other approved ART regimens [14]. In addition, INSTI-related weight gain has also been established in previous studies including results from a recent systematic literature review, which have demonstrated that INSTIs are associated with greater weight gain or BMI increase than other ART classes [15]. When compared with PI-based regimens, a majority of studies have suggested that INSTI-based regimens were associated with greater increases in weight/BMI gain after ART initiation in both treatment-naive and treatment-experienced PLWH [16–21].
Although INSTI-experienced PLWH who gain weight may switch to a different ART class to better control weight, switches to another INSTI-based regimen may also occur because of the general preference for this class of ART medication based on DHHS guideline recommendations or because one of the backbone components (e.g., tenofovir alafenamide [TAF]) was believed to be responsible for the observed weight gain. While there is research investigating weight changes in treatment-naive PLWH, overall and for specific regimens, there are little data available to date on switching off an INSTI as a strategy to mitigate or reverse weight gain. More specifically, there has been relatively little investigation into the extent of weight gain or BMI increase among treatment-experienced PLWH who switched ART following initial INSTI treatment, specifically among populations at high risk of weight gain. Therefore, this study aims to describe and compare weight and BMI changes among PLWH at higher risk of weight gain, as defined in the DHHS guidelines (i.e., females, Blacks or Hispanics) [12–14], who were previously treated with an INSTI-based ART regimen and were then switched to a PI-based ART versus another INSTI-based ART.
Materials & methods
Data source
Electronic medical record (EMR) data from the Symphony Health, an ICON plc Company, IDV® database (1 April 2015 to 31 March 2021) was used to identify the study population and address the study objectives. This provider-based EMR database comprises historical clinical information such as medications prescribed and administered, lab results, vital signs including weight and BMI measurements, and clinical diagnoses. The data were de-identified and compliant with the requirements of the Health Insurance Portability and Accountability Act (HIPAA). As such, PLWH did not sign informed consent for enrollment in the provider-based EMR database. As this was an analysis of EMR data, Institutional Review Board approval was not required, for two reasons: it was a retrospective analysis of existing data (and hence, involved no intervention or interaction conducted by the authors); and no personally identifiable information was included in the EMR dataset.
Study design
A retrospective, longitudinal cohort study design was used for this analysis. Adult female, all Black (male or female), or all Hispanic (male or female) PLWH who were initiated on an INSTI as part of a complete ART regimen (defined as ≥2 nucleoside reverse transcriptase inhibitors [NRTIs] or a single NRTI if the regimen was dolutegravir [DTG] + lamivudine, with all NRTI agents being received within 14 days before or after the date of the first INSTI prescription) and who subsequently switched to either a PI-based or another INSTI-based complete ART regimen within 90 days of the last prescription for the initial INSTI regimen were included.
PLWH were assigned to mutually exclusive PI or INSTI cohorts based on the first observed prescription for the agent that they switched to. The index date was defined as the date of the first prescription for the agent to which the PLWH switched (i.e., new PI or different INSTI). Therefore, PLWH were assigned to the PI cohort if they first switched to a PI or to the INSTI cohort if they first switched to another INSTI. PLWH who only had a switch in the NRTI backbone but remained on the same INSTI agent were not considered to have a treatment switch and were not included in the INSTI cohort. To represent the most recent and commonly used ART regimens, only switches to darunavir (DRV) or atazanavir (ATZ) were included for the PI cohort, and switches to DTG, elvitegravir (EVG), or bictegravir (BIC) were included for the INSTI cohort.
Continuous clinical activity in the EMR database was defined as the period from the first to the last record in the database. The baseline period was defined as the 6-month period of continuous clinical activity before the index date, and the follow-up period was defined as the period from the index date until the earliest of initiation of another PI or INSTI agent that was different from the index agent (i.e., a switch of the NRTI backbone was not considered a treatment switch), initiation of a non-nucleoside reverse transcriptase inhibitor (NNRTI) agent, the end of continuous clinical activity, or the end of data availability (i.e., on-treatment approach).
Study population
Adult female, any Black or any Hispanic PLWH who were treated with an INSTI (i.e., raltegravir, DTG, EVG or BIC) used as part of a complete ART regimen (i.e., the initial INSTI regimen), and who were subsequently treated with a PI agent (i.e., DRV or ATZ) or a different INSTI agent (i.e., DTG, EVG or BIC), used as part of a complete ART regimen between 1 October 2015 and 15 November 2020, were included if they were diagnosed with HIV-1 prior to the index date, had ≥6 months of continuous clinical activity before the index date and had ≥1 weight or BMI measurement in both the baseline and follow-up periods (Figure 1).
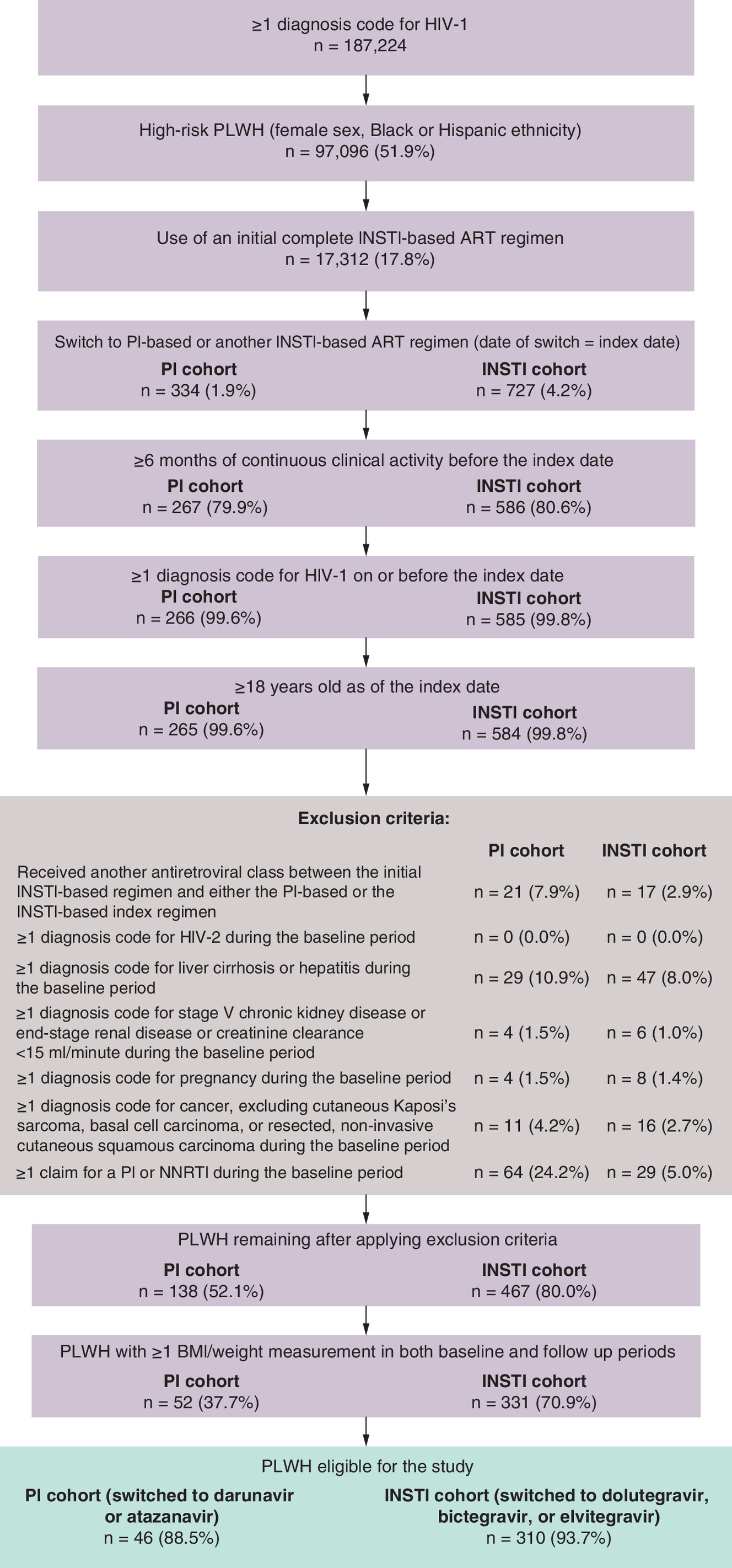
Figure 1. Identification of the study population.
ART: Antiretroviral therapy; INSTI: Integrase strand transfer inhibitor; NNRTI: Non-nucleoside reverse transcriptase inhibitor; PI: Protease inhibitor; PLWH: People living with HIV-1.
PLWH were excluded if they were males of non-Black/non-Hispanic ethnicity, received another ART class between the initial INSTI-based regimen and either the PI-based or the INSTI-based index regimen, had ≥1 diagnosis of HIV-2, liver cirrhosis or hepatitis, stage V chronic kidney disease or end-stage renal disease (or creatinine clearance <15 mL/minute), pregnancy, or cancer (excluding cutaneous Kaposi's sarcoma, basal cell carcinoma, or resected, non-invasive cutaneous squamous carcinoma) during the baseline period, or if they were previously treated with a PI or NNRTI during the baseline period.
Study measures
Demographic and clinical characteristics were described during the 6-month baseline period. To understand weight/BMI trajectories, the mean weight and BMI measurements observed during the period prior to initiating the initial INSTI-based regimen (pre-INSTI period), during their initial INSTI-based ART regimen (during-INSTI period), and after switching from the initial INSTI regimen (post-index period) were evaluated among PLWH with ≥1 measurement in each of these periods.
Differences in weight and BMI between the baseline and follow-up periods were also assessed at 3-, 6-, 9- and 12-month post-index time points. Follow-up weight/BMI measurements were assessed during non-overlapping 3-month intervals at 75, 165, 255 and 345 days, using ± 45-day windows around each time point. If an individual had more than one weight or BMI value during a specific 3-month interval, all values were used to calculate the mean weight or BMI for that interval (Supplementary Figure 1).
For each post-index time point, the absolute and relative differences (i.e., any increase [i.e., >0%] and ≥5% increase) in weight or BMI between the post-index time point and the baseline measurement were assessed among both cohorts.
Statistical analysis
Baseline characteristics were reported using means, standard deviations (SDs), medians for continuous variables and counts and proportions for categorical variables. Inverse probability of treatment weighting (IPTW) was used to account for differences in baseline characteristics between the PI and INSTI cohorts. First, the propensity score (PS) for each individual was estimated using a multivariable logistic regression model, where the dependent variable was the index treatment indicator (i.e., PI or INSTI) and baseline characteristics were independent variables used to predict treatment switch. The following baseline variables were included in the PS model: age, gender, ethnicity, geographic region, insurance plan type, year of the index date, Quan-Charlson Comorbidity index (Quan-CCI; excluding HIV-1 symptoms), hypertension, dyslipidemia, obesity, type II diabetes, BMI and observed duration of initial INSTI treatment. IPTWs for each individual were estimated as follows: 1/PS for PLWH in the PI cohort and 1/(1-PS) for PLWH in the INSTI cohort. In addition, weights were normalized by the mean weight and truncated at the 95th percentile of the IPTW distribution. In the resulting weighted sample, each individual contributed according to their reweighted representation, and the weighted sample size after IPTW for a given cohort represented the sum of each individual's weight in that cohort. Therefore, even though the same individuals contributed to the analysis before and after weighting, the sample size after weighting was different than the original sample size (before weighting) [22]. The resulting differences in weight/BMI changes between the weighted PI and INSTI cohorts reflected the average treatment effect.
Differences in baseline characteristics between the two cohorts were evaluated using standardized differences. Characteristics with a standardized difference <10% were considered well balanced [23]. The mean change in weight and BMI between the baseline and follow-up periods was compared between PI and INSTI cohorts at 3-, 6-, 9- and 12-month post-index using mean differences obtained from weighted ordinary least squares regression models. The proportion of PLWH having any and ≥5% weight or BMI increase between the post- and pre-index periods were also compared between the index treatments at 3-, 6-, 9- and 12-month post-index using odds ratios (ORs) obtained from weighted logistic regression models. All weighted models were further adjusted for the following additional baseline variables that remained imbalanced after IPTW, to obtain doubly-robust estimates: age, gender, ethnicity, baseline Quan-CCI (excluding HIV-1), baseline hypertension, baseline dyslipidemia, baseline type II diabetes, weight gain ≥5% after starting initial INSTI (weight outcomes only) and BMI increase ≥5% after starting initial INSTI (BMI outcomes only). To account for the variability in individual's IPTW, non-parametric bootstrap procedures with 500 iterations were used to calculate 95% confidence intervals (CIs) and p-values for all regression models.
As part of a subgroup analysis, mean weight differences between the baseline and follow-up periods were described among PLWH who switched from their initial TAF-containing INSTI regimen to an index non-TAF-containing INSTI regimen.
Results
Overall, 46 PLWH were eligible for inclusion in the PI cohort and 310 PLWH were eligible for inclusion in the INSTI cohort (Figure 1). After applying IPTW, weighted samples were 153 and 203 PLWH in the PI and INSTI cohorts, respectively (Table 1).
| Weighted population† | |||
|---|---|---|---|
| Demographic characteristics | PI cohort, n = 153 | INSTI cohort, n = 203 | Standardized difference‡ |
| Age at index date (years), mean ± SD [median] | 42.5 ± 12.6 [42.0] | 45.5 ± 13.6 [45.0] | 23.4% |
| Female, n (%) | 92 (60.3) | 106 (52.4) | 16.0% |
| Ethnicity, n (%) | |||
| Black | 75 (49.1) | 109 (53.5) | 8.8% |
| Hispanic | 24 (15.6) | 30 (14.5) | 3.0% |
| White | 10 (6.2) | 18 (8.8) | 9.9% |
| Other | 44 (29.1) | 47 (23.2) | 13.5% |
| US geographic region, n (%) | |||
| South | 117 (76.8) | 154 (76.0) | 1.7% |
| Midwest | 12 (7.8) | 17 (8.4) | 2.2% |
| Northeast | 16 (10.5) | 17 (8.1) | 8.2% |
| West | 8 (4.9) | 14 (6.8) | 8.1% |
| Unknown | 0 (0.0) | 1 (0.6) | 11.0% |
| Insurance plan type, n (%) | |||
| Insurance plan information available (in claims) | 149 (97.3) | 188 (92.6) | 21.6% |
| Commercial | 100 (65.1) | 126 (62.0) | 6.6% |
| Medicaid | 32 (20.9) | 37 (18.4) | 6.4% |
| Medicare | 13 (8.7) | 19 (9.4) | 2.4% |
| Other/unknown | 4 (2.5) | 6 (2.8) | 1.9% |
| Year of index date, n (%) | |||
| 2015 | 7 (4.4) | 12 (6.0) | 7.1% |
| 2016 | 29 (19.2) | 29 (14.3) | 13.0% |
| 2017 | 17 (11.2) | 19 (9.5) | 5.7% |
| 2018 | 35 (22.7) | 48 (23.7) | 2.4% |
| 2019 | 46 (30.1) | 59 (29.0) | 2.3% |
| 2020 | 19 (12.4) | 36 (17.5) | 14.2% |
| Clinical characteristics | |||
|---|---|---|---|
| Quan-CCI (excluding HIV-1 symptoms), mean ± SD [median] | 0.4 ± 0.8 [0.0] | 0.5 ± 1.0 [0.0] | 14.6% |
| Other physical comorbidities, n (%) | |||
| Hypertension | 27 (17.6) | 50 (24.4) | 16.9% |
| Obesity | 19 (12.6) | 26 (12.7) | 0.4% |
| Dyslipidemia/hyperlipidemia | 14 (9.3) | 28 (13.8) | 14.2% |
| Type II diabetes mellitus | 8 (5.5) | 22 (10.9) | 19.9% |
| PLWH with a BMI measurement, n (%) | 153 (100.0) | 202 (99.4) | 11.0% |
| BMI (kg/m2), mean ± SD [median] | 29.5 ± 7.2 [29.0] | 29.8 ± 7.7 [28.7] | 4.2% |
| BMI categories (kg/m2), n (%) | |||
| <25 | 50 (32.5) | 65 (32.3) | 0.5% |
| 25–29 | 34 (22.0) | 47 (23.3) | 3.2% |
| 30–34 | 47 (30.4) | 44 (21.9) | 19.5% |
| ≥35 | 23 (15.1) | 45 (22.5) | 19.1% |
| BMI increase ≥5% after starting initial INSTI, n (%) | 54 (35.1) | 38 (18.9) | 37.1% |
| PLWH with a weight measurement, n (%) | 153 (100.0) | 203 (100.0) | 0.0% |
| Weight (kg), mean ± SD [median] | 83.2 ± 19.0 [83.9] | 85.0 ± 23.7 [81.6] | 8.4% |
| Weight gain ≥5% after starting initial INSTI, n (%) | 54 (35.1) | 38 (18.9) | 37.1% |
| Initial INSTI-based regimen | |||
| Observed duration of INSTI treatment (months), mean ± SD [median] | 14.3 ± 13.8 [10.9] | 16.9 ± 15.8 [13.2] | 17.3% |
| Dolutegravir-based, n (%) | 82 (53.7) | 66 (32.7) | 43.4% |
| Elvitegravir-based, n (%) | 46 (29.8) | 87 (42.8) | 27.2% |
| Raltegravir-based, n (%) | 13 (8.3) | 33 (16.0) | 23.7% |
| Bictegravir/emtricitabine/TAF, n (%) | 12 (8.1) | 17 (8.5) | 1.3% |
| TAF, n (%) | 72 (47.3) | 91 (45.0) | 4.6% |
| TAF 10 mg | 36 (23.3) | 51 (25.3) | 4.6% |
| TAF 25 mg | 37 (24.0) | 40 (19.8) | 10.2% |
| TDF, n (%) | 36 (23.8) | 65 (32.1) | 18.7% |
†
The number of PLWH reported in this weighted population represents the sum of weights for the corresponding PLWH, rounded to the nearest integer. The proportions displayed were calculated prior to the rounding and may be slightly different than if they were calculated based on rounded numbers.
‡
For continuous variables, the standardized difference was calculated by dividing the absolute difference in means of the PI cohort and the INSTI cohort by the pooled standard deviation of both groups. The pooled standard deviation is the square root of the average of the squared standard deviations. For categorical variables with two levels, the standardized difference is calculated using the following equation where P is the respective proportion of participants in each group: (PPI-PINSTI)/√([p1 + p2]/2), where p1 = PPI(1-PPI) and p2 = PINSTI(1-PINSTI).
CCI: Charlson Comorbidity Index; INSTI: Integrase strand transfer inhibitor; PI: Protease inhibitor; PLWH: People living with HIV-1; SD: Standard deviation; TAF: Tenofovir alafenamide; TDF: Tenofovir disoproxil fumarate.
Study population characteristics
Baseline characteristics for each weighted cohort are presented in Table 1. The mean age was 42.5 years (SD = 12.6) and 45.5 years (SD = 13.6) in the PI and INSTI cohorts, respectively, and females accounted for 60.3 and 52.4% of PLWH in the two cohorts, respectively. Most PLWH were Black (PI: 49.1%; INSTI: 53.5%), resided in the South (PI: 76.8%; INSTI: 76.0%) and were covered by commercial insurance plans (PI: 65.1%; INSTI: 62.0%). The mean baseline Quan-CCI score (excluding HIV-1 symptoms) was 0.4 (SD = 0.8) and 0.5 (SD = 1.0) in the PI and INSTI cohorts, respectively. The mean baseline weight was 83.2 kg [183.4 lbs] (SD = 19.0 kg) and 85.0 kg [187.4 lbs] (SD = 23.7 kg), and the mean baseline BMI was 29.5 kg/m2 (SD = 7.2) and 29.8 kg/m2 (SD = 7.7) in the PI and INSTI cohorts, respectively. The mean duration of the initial INSTI-based regimen prior to ART switch was 14.3 months (SD = 13.8) and 16.9 months (SD = 15.8) in the PI and INSTI cohorts, respectively. The most common initial INSTI-based regimen was DTG-based for the PI cohort (53.7%) and EVG-based for the INSTI cohort (42.8%).
In the PI cohort, the most common PI that PLWH switched to was DRV (74.1%; Table 2). In the INSTI cohort, the most common INSTI that PLWH switched to was BIC/emtricitabine (FTC)/TAF (52.3%), followed by a DTG-based ART regimen (40.8%). TAF use was observed among 50.0% and 65.5% of index regimens in the PI and INSTI cohorts, respectively. The mean duration of the index treatment (i.e., on-treatment period) was 14.7 months (SD = 11.8) in the PI cohort and 19.9 months (SD = 14.5) in the INSTI cohort.
| Weighted population† | ||
|---|---|---|
| PI cohort, n = 153 | INSTI cohort, n = 203 | |
| Duration of treatment on the index ART regimen (months), mean ± SD [median] | 14.7 ± 11.8 [11.5] | 19.9 ± 14.5 [18.3] |
| PI-based‡, n (%) | 153 (100.0) | – |
| DRV-based | 113 (74.1) | – |
| Atazanavir-based | 40 (25.9) | – |
| Boosted PI | 144 (94.3) | – |
| PI with boosted c | 101 (66.0) | – |
| PI with boosted ritonavir | 43 (28.3) | – |
| INSTI-based, n (%) | – | 203 (100.0) |
| Bictegravir/FTC/TAF | – | 106 (52.3) |
| Dolutegravir-based | – | 83 (40.8) |
| Elvitegravir-based | – | 23 (11.3) |
| Raltegravir-based | – | 3 (1.7) |
| Non-boosted INSTI | – | 181 (89.0) |
| Boosted INSTI (with c) | – | 22 (11.0) |
| NRTI agents, n (%) | ||
| TAF | 76 (50.0) | 133 (65.5) |
| TDF | 69 (45.0) | 21 (10.3) |
| FTC | 138 (90.2) | 146 (71.7) |
| Lamivudine | 18 (11.6) | 64 (31.3) |
| Abacavir | 14 (9.1) | 60 (29.8) |
†
Of note, the number of PLWH reported in this weighted population represents the sum of weights for the corresponding PLWH, rounded to the nearest integer. The proportions displayed were calculated prior to the rounding and may be slightly different than if they were calculated based on rounded numbers.
‡
Out of all PLWH in the PI cohort, 60 (39.2%) were initiated on DRV/c/FTC/TAF.
ART: Antiretroviral therapy; c: Cobicistat; DRV: Darunavir; FTC: Emtricitabine; INSTI: Integrase strand transfer inhibitor; NRTI: Nucleoside/nucleotide reverse transcriptase inhibitors; PI: Protease inhibitor; PLWH: People living with HIV-1; SD: Standard deviation; TAF: Tenofovir alafenamide; TDF: Tenofovir disoproxil fumarate.
Comparison of weight & BMI change after treatment switch
The analysis of weight/BMI trajectories showed that weight and BMI increases were observed after starting the initial INSTI-based regimen for both cohorts, with a numerically higher gain observed pre-switch in those who later went into the PI cohort (weight: mean increase from 80.8 kg before initiation of the initial INSTI to 84.6 kg while on initial INSTI treatment; BMI: mean increase from 28.6 to 29.9 kg/m2) than into the INSTI cohort (weight: mean increase from 84.1 to 85.0 kg; BMI: mean increase from 29.4 to 29.8 kg/m2). After switching from the initial INSTI regimen to the index regimen, weight and BMI increases were observed to stabilize in the PI cohort (weight: mean increase from 84.6 kg while on initial INSTI treatment to 84.8 kg while on PI treatment; BMI: mean increase from 29.9 to 30.0 kg/m2), while increases continued to be observed in the INSTI cohort (weight: mean increase from 85.0 kg while on initial INSTI treatment to 86.1 kg while on second INSTI treatment; BMI: mean increase from 29.8 to 30.1 kg/m2; Figure 2).
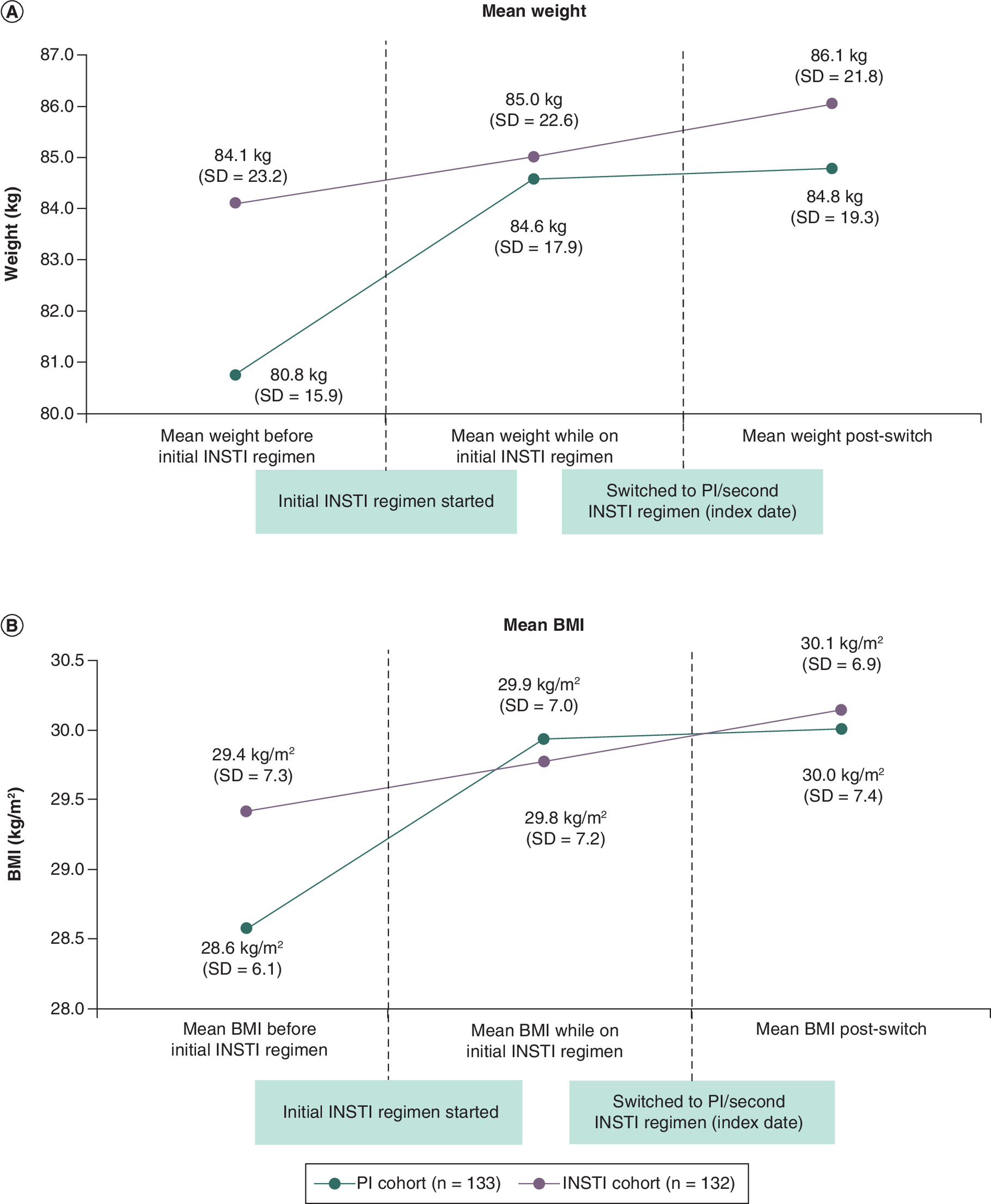
Figure 2. Change in weight and BMI pre-INSTI, during INSTI and post-index*,**,***.
*The period before initial INSTI regimen was defined as the time from beginning of continuous clinical activity to initiation of first INSTI regimen. The period while on INSTI regimen was defined as the time from initiation of first INSTI regimen to index date (i.e., date of switch to another INSTI agent or PI). The post-switch period was defined as the time from the index date to end of follow-up (i.e., earliest of initiation of another PI or INSTI agent different from the index agent, use of an NNRTI agent, end of continuous clinical activity, or end of data availability [31 March 2021]). Mean measurements observed during each period were reported.
**The sample used for this analysis represented a subgroup of the overall study cohort, as only PLWH who had a measurement in each of the periods of interest (i.e., pre-INSTI period, during the INSTI period and the post-index period) were included.
***For weight measurements, the mean (median) duration of observation for each period was as follows: before initial INSTI regimen, PI cohort: 24.4 (24.9) months and INSTI cohort: 23.2 (19.2) months; while on initial INSTI regimen, PI cohort: 15.7 (12.1) months and INSTI cohort: 18.2 (14.9) months; post-switch, PI cohort: 14.9 (11.5) months and INSTI cohort: 19.1 (17.5) months. For BMI measurements, the mean (median) duration of observation for each period was as follows: before initial INSTI regimen, PI cohort: 24.4 (24.9) months and INSTI cohort: 23.2 (18.9) months; while on initial INSTI regimen, PI cohort: 15.7 (12.1) months and INSTI cohort: 18.3 (14.9) months; post-switch, PI cohort: 14.9 (11.5) months and INSTI cohort: 19.2 (17.5) months.
INSTI: Integrase strand transfer inhibitor; PI: Protease inhibitor; SD: Standard deviation.
After treatment switch, PLWH in the INSTI cohort initially experienced slightly smaller (but non-significant) weight and BMI increases at 3- and 6-month time points than PLWH in the PI cohort (Figure 3). However, at 9- and 12-months post-switch, PLWH in the INSTI cohort experienced numerically higher weight and BMI increases than those in the PI cohort, with PLWH in the PI cohort experiencing an overall mean decrease in weight post-index, while those in the INSTI cohort experienced an overall mean increase in weight post-index. More specifically, at 9 months, the weighted doubly robust mean difference in body weight was 1.66 kg [(]3.66 lbs] (mean increase for INSTI cohort: Δ9 months = +1.55 kg [+3.42 lbs ] (SD = 8.27 kg); mean decrease for PI cohort: Δ9 months = -0.23 kg [-0.51 lbs] ( SD = 4.67 kg); p = 0.21) and at 12 months, the weighted mean difference in body weight widened to 3.23 kg [7.12 lbs] (mean increase for INSTI cohort: Δ12 months = +1.59 kg [+3.51 lbs] [SD = 6.87 kg]; mean decrease for PI cohort: Δ12 months = -1.59 kg [-3.51 lbs]( SD = 9.06 kg); p = 0.13).
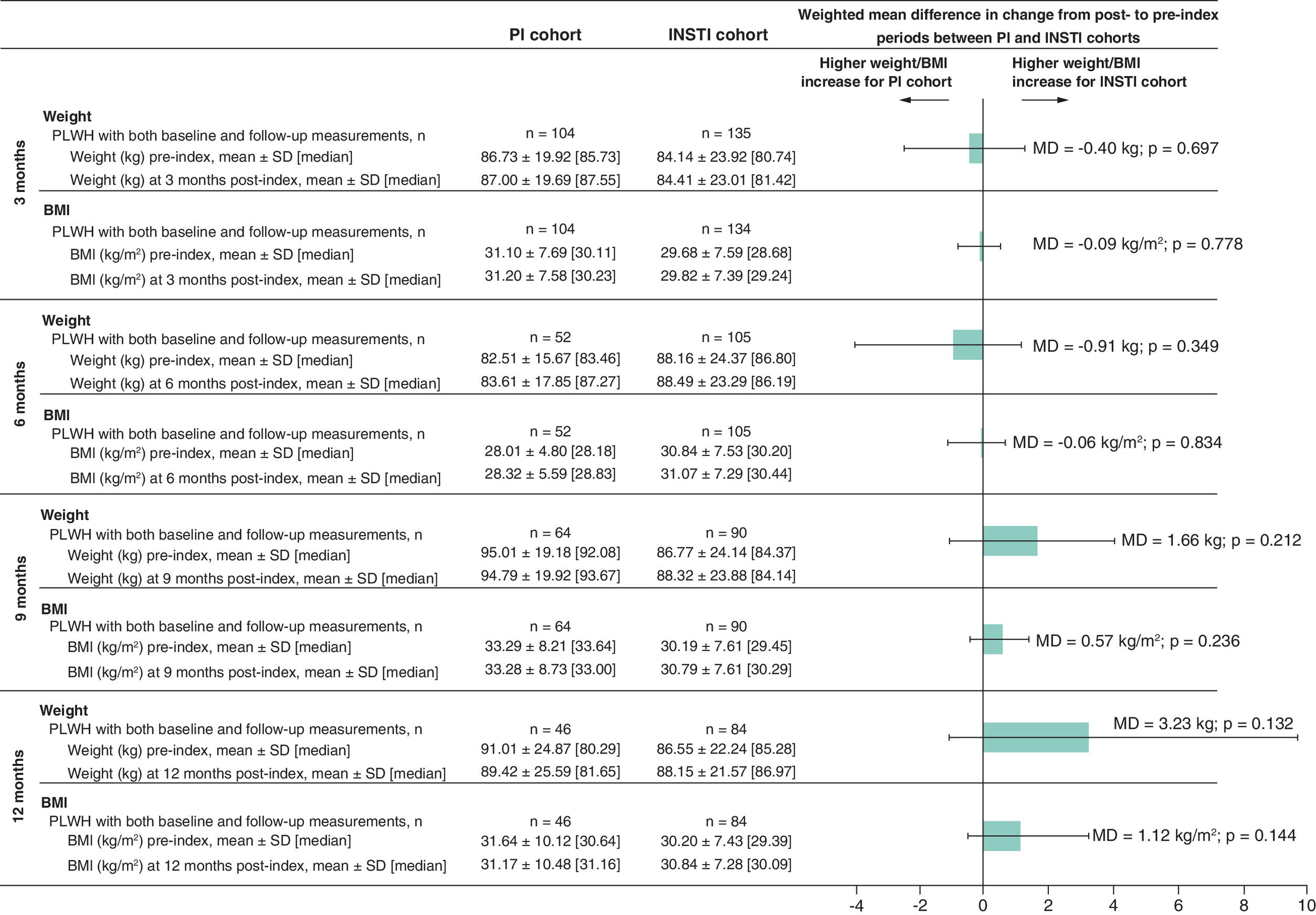
Figure 3. Comparison of mean weight or BMI change between the pre- and post-index periods*.
*Non-parametric 95% CIs and p-values were obtained from 500 bootstrap iterations. At each bootstrap resample, the inverse probability of treatment weights was re-estimated.
INSTI: Integrase strand transfer inhibitor; MD: Mean difference; PI: Protease inhibitor; PLWH: People living with HIV-1.
Similarly, PLWH in the INSTI cohort experienced numerically higher BMI increases than PLWH in the PI cohort at most time points, with widening differences in BMI increase over time, although none of the differences reached statistical significance. More specifically, at 9 months, the weighted doubly robust mean difference in BMI was 0.57 kg/m2 (mean increase for INSTI cohort: Δ9 months = +0.60 kg/m2 (SD = 2.82); no mean change for PI: Δ9 months = 0.00 kg/m2 (SD = 1.66); p = 0.24) and at 12 months, the weighted mean difference in BMI widened to 1.12 kg/m2 (mean increase for INSTI: Δ12 months = +0.64 kg/m2 (SD = 2.36); mean decrease for PI: Δ12 months = -0.46 kg/m2 (SD = 3.02); p = 0.14).
Compared with PLWH in the PI cohort, PLWH in the INSTI cohort also experienced numerically higher relative weight and BMI increases at most time points using relative outcome measures (i.e., weight/BMI increase >0% and ≥5%), although none of the differences reached statistical significance (Figure 4). More specifically, at 9 months, 56.8 and 28.1% of PLWH in the INSTI cohort experienced any weight gain or ≥5% weight gain, respectively, while 32.1 and 13.8% of PLWH in the PI cohort experienced these outcomes, respectively. At 12 months, 68.4 and 33.9% of PLWH in the INSTI cohort experienced any weight gain or ≥5% weight gain, respectively, while 55.9 and 24.8% of PLWH in the PI the cohort experienced these outcomes. Results were similar for BMI increase, with 56.8 and 28.0% of PLWH in the INSTI cohort experienced any BMI increase and ≥5% BMI increase at 9 months, respectively, while 32.1 and 16.8% of PLWH in the PI cohort experienced these outcomes. At 12 months, 67.3 and 35.0% of PLWH in the INSTI cohort experienced any BMI increase and ≥5% BMI increase, respectively, while 55.9 and 24.8% of PLWH in the PI cohort experienced these outcomes.
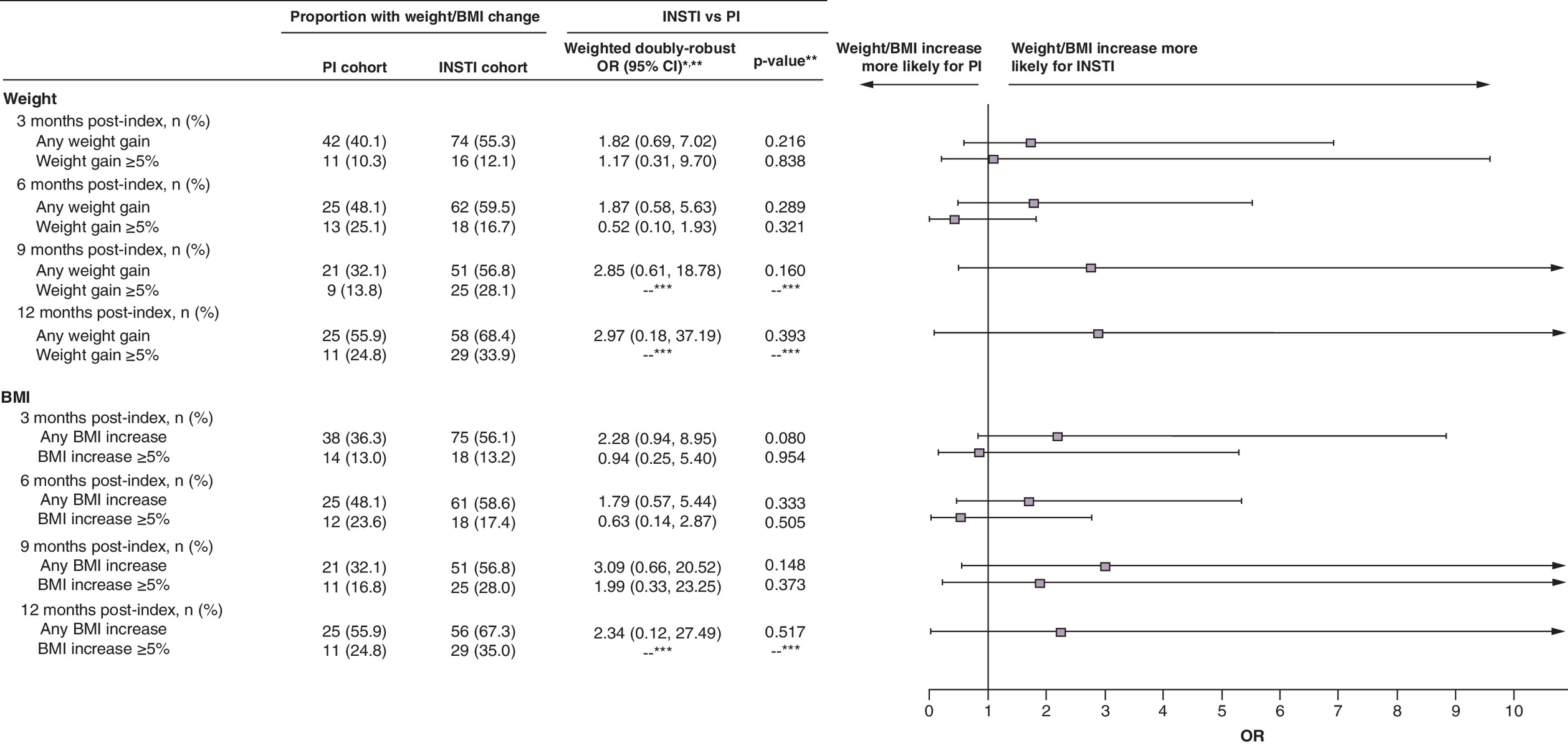
Figure 4. Weight and BMI comparisons by threshold between pre-index and post-index time points.
*An OR >1 indicates that the INSTI cohort had a higher risk of weight or BMI gain than the PI cohort.
**Non-parametric 95% CIs and p-values were obtained from 500 bootstrap iterations. At each bootstrap resample, the inverse probability of treatment weights were re-estimated.
***Data not available, given that logistic regression models for these outcomes did not converge.
CI: Confidence interval; INSTI: Integrase strand transfer inhibitor; OR: Odds ratio; PI: Protease inhibitor.
Although sample sizes were small (n = 12 and n = 11 at 9 and 12 months, respectively), removing TAF from the original INSTI regimen did not change the finding that switching to another INSTI regimen is associated with continued weight increase, as PLWH who switched from a TAF-containing INSTI regimen to a non-TAF-containing INSTI regimen experienced a mean increase in body weight of 3.04 kg [6.70 lbs] at 9 months and 1.79 kg [3.95 lbs] at 12 months.
Discussion
To our knowledge, this is the first retrospective longitudinal study evaluating the weight/BMI changes occurring post-INSTI switch among females, Blacks or Hispanics who switched to one of two different regimens – a PI or another INSTI. It showed that among these PLWH, weight gain and BMI increases were observed after initiation of the initial INSTI regimen, but the weight/BMI trajectories were observed to level off to a greater extent in the longer term for PLWH switching to a PI than for those switching to another INSTI, and the net weight change observed at months 9 and 12 after switching to a PI was a weight loss. Furthermore, this study observed a trend toward greater mean weight/BMI increases in the INSTI cohort compared with the PI cohort, particularly after 9 and 12 months of treatment, with larger increases observed at later time points.
Previous research has noted that initiation of INSTI-based ART in many populations of treatment-naive PLWH leads to higher weight gain [18,24,25]. Other studies have also noted trends toward weight increase upon a switch to an INSTI, including BIC/FTC/TAF [20,26,27]. Furthermore, the DHHS outlines the weight gain potential of INSTIs in its guidelines and notes that further questions about the regional distribution, association with cardiometabolic risk and reversibility of weight gain after discontinuation remain [14]. Although current recommendations for mitigating weight gain focus predominantly on lifestyle measures (which were not evaluable in the current study) [28], many PLWH may experience challenges in adopting changes to these lifestyle measures [29]. The current study suggests however that ART management could be another strategy to mitigate weight gain in this population, as highlighted by the observation that weight gain at later time points was qualitatively less for PIs than INSTIs, combined with the observed leveling-off of weight trajectories in the PI cohort. Furthermore, as weight gain was observed to continue in the INSTI cohort, this suggests that a switch from one INSTI to another, if undertaken as a strategy to manage INSTI-related weight gain, may not yield the intended result. On the other hand, switching to a PI may help over time. Despite the evidence of weight gain after INSTI initiation [15], the mechanism by which INSTIs cause weight gain remains unknown, as does the reversibility and the time needed for reversibility of INSTI-related weight gain. The current study may provide preliminary insights into the latter. More specifically, for PLWH switching to a PI, results showed that the effect of the initial INSTI regimen may have prevented the observation of reversibility of weight gain at earlier time points (i.e., 3 and 6 months), but not at later time points (i.e., 9 and 12 months), where a decrease in weight was observed, thus suggesting that reversibility may occur >6 months post-switch.
An important aspect of this study is the focus on female, Black, or Hispanic PLWH; Black and Hispanic groups in particular are disproportionately affected by HIV-1 [30]. Similar to the results of the current study, previous studies as well as the DHHS guidelines have highlighted that these populations experience significantly higher weight gain upon initiating ART, particularly with INSTI-based regimens [14,31–33]. One study observed an increase in annualized weight gain of greater magnitude among females with BMI ≥30 kg/m2 (post-switch increase of 1.7 kg/year [3.7 lbs/year]) and Black PLWH (post-switch increase of 0.9 kg/year [2.0 lbs/year]) after switching to an INSTI-based ART [31]. Black female PLWH who initiated an INSTI-based regimen also had a significantly greater weight increase (mean difference of 1.5 kg [3.3 lbs], p = 0.003) compared with a PI-based regimen, and female Hispanic PLWH had a trend toward the same result (mean difference of 0.4 kg [0.9 lbs]; p = 0.423) [34]. Although previous studies have addressed weight trajectories after starting ART among treatment-naive PLWH, including finding greater weight gain in high risk patients [32], this study provides further context to research in this area by identifying weight trajectories in a population of PLWH previously exposed to an INSTI who then switched to another INSTI-based or PI-based regimen. Future studies should investigate whether and how weight trajectories may differ between high risk and low risk PLWH after ART switching.
Previous studies have suggested that PLWH experiencing weight gain following ART use are more likely to develop incident diabetes and cardiovascular disease [35–40], although the implications of rapid weight gain associated with INSTI-based regimens remain unclear. One study reported a dose-dependent association between weight gain and the risk of diabetes, with every 5 lbs of weight gained, incident diabetes risk increased by 14% among PLWH treated with ART (HR: 1.14; 95% CI: 1.10–1.17) compared with 8% among uninfected individuals (HR: 1.08; 95% CI: 1.07–1.10) [37]. A recent study evaluating participants in the Data Collection on Adverse Events of Anti-HIV Drugs (D:A:D) Study receiving ART found that a BMI gain of ≥2 kg/m2 was associated with a significantly higher risk of diabetes compared with stable BMI across all baseline BMI categories; for the baseline BMI category 25–29.9 kg/m2, a BMI gain of 1–1.9 kg/m2 also significantly increased the risk of diabetes (HR: 1.33; 95% CI: 1.02–1.74) compared with stable BMI [40]. In the context of growing evidence linking weight gain in PLWH with incident cardiometabolic conditions, results from future clinical trials investigating the impact of a switch from an INSTI to a PI-containing ART regimen (DEFINE study, NCT04442737) [41] or to an NNRTI-containing regimen (The Do IT study, NCT04636437) [42] will be important to help understand the impact of treatment switch on weight trajectory after a rapid weight gain has been observed on the prior ART regimen.
An additional aspect which merits further investigation is the presence of TAF in the ART regimen. The use of TAF has been noted as a risk factor for ART-related weight gain and was associated with greater weight gain in comparison to TDF [32,43,44]. In the current study, 47.3% of the PI cohort and 45.0% of the INSTI cohort had TAF as part of their initial INSTI regimen; during the index regimen 50.0% of the PI cohort and 65.5% of the INSTI cohort had TAF in their respective ART regimens. It is therefore a possibility that the presence of TAF in these regimens contributed to the observed weight trajectories, even if just used as part of the initial INSTI regimen. Indeed, although sample sizes were low, when PLWH in the current study switched from TAF-containing INSTI regimens to a non-TAF-containing INSTI regimens, a mean weight gain of 3.04 kg [6.70 lbs] was observed at 9 months post-index and a mean weight gain of 1.79 kg [3.95 lbs] was observed at 12 months, which represented higher increases than results observed for the overall INSTI cohort. Future studies assessing treatment switch while accounting for the presence of TAF would also be important to help elucidate the contributors to weight gain and determine mitigation strategies, but this small dataset suggests that in the presence of weight gain following initial INSTI use, switching to another INSTI even in the absence of TAF is unlikely to achieve the desired outcome. Of note, the use of a TDF-based regimen was not considered a confounder in this study, as pooled data from eight large phase III HIV comparative clinical trials demonstrated that TDF was not associated with an increased risk of weight gain relative to other backbone agents, including TAF [32].
This study is subject to certain limitations. First, the study was limited by a small sample size, resulting in reduced power to detect smaller effect sizes and the inability to present results separately for female, Black or Hispanic PLWH. In addition, the small sample also prevented the analysis of the impact of switching to specific ART regimens. Future research with a larger sample is needed to confirm the findings. Second, data on waist circumference were not available, and therefore limited the ability to fully capture changes in all adiposity measurements. Third, the validity of IPTW rests on the untestable assumption that all confounders are accounted for, and while a large number of variables were included in this analysis, there remains the possibility of unmeasured confounding and residual imbalances. For example, although observed weight gain and BMI change after the initial INSTI regimen were accounted for, reasons for switching treatment after the use of an initial INSTI could not be ascertained and confounding by indication (i.e., more PLWH switched to a PI-based regimen because of weight change-related reasons) cannot be ruled out. Additional laboratory parameters, such as HIV viral load and CD4+ cell count, which have also been associated with weight change [32] were not available for the majority of included PLWH and therefore could not be included in the PS model for balancing or used to assess virological failure. Furthermore, while doubly-robust adjustment was used to address remaining imbalances after applying IPTW, given the small sample size, only a limited number of variables could be included as part of the statistical adjustment for the remaining imbalances due to the potential for non-convergence of the weighted regression models. Fourth, there remained imbalances, including for the distribution of the initial INSTI-based regimen between the PI and INSTI cohorts, which may have impacted the observed weight gain or BMI change, given that different INSTI agents may impact weight gain differently. Additionally, lifestyle measures, which may play a considerable role in weight changes, were not observable in this study and hence could not be adjusted for. Fifth, claims and EMR data may contain inaccuracies or omissions in diagnoses, billing and other variables. Sixth, as with all EMR databases, the prescription of an ART medication was assumed to indicate its use and that it was taken as indicated. Finally, given the use of a provider-based data source, services and medications PLWH receive from providers outside of the network may not be captured; therefore, the full treatment history of PLWH may not be captured, as PLWH could have been prescribed ARTs outside of the network.
Conclusion
This study is the first containing data post-INSTI switch that supports the idea that ART management may be an option to mitigate or reverse weight gain following initial INSTI use among PLWH with a higher risk of weight gain. More specifically, following initial INSTI treatment, results showed numerically greater increases in weight gain and BMI at 9 and 12 months for PLWH who switched to a different INSTI regimen versus decreases for PLWH who switched to a PI regimen, with differences between the two cohorts widening over time. Future studies with larger sample sizes and additional follow-up are needed to confirm these findings.
•
While there is research investigating weight changes in treatment-naive people living with HIV-1 (PLWH), overall and for specific regimens, there has been relatively little investigation into the extent of weight gain or BMI increase among treatment-experienced PLWH with a higher risk of weight gain who switched antiretroviral therapy (ART) following initial integrase strand transfer inhibitor (INSTI) treatment.
•
This study evaluated the change in weight and BMI among females, Black, or Hispanic PLWH after switching from an INSTI-based ART regimen to a protease inhibitor (PI)-based or another INSTI-based regimen.
•
To address the study objective, inverse probability of treatment weighting (IPTW) was used to account for differences in characteristics between PLWH switching to a PI or INSTI.
•
When on the initial INSTI regimen, weight and BMI increased for both treatment cohorts.
•
Post-INSTI switch, weight and BMI appeared to level off to a greater extent at later time points in the PI cohort than the INSTI cohort.
•
A trend toward overall weight loss was observed for PLWH after switching to a PI-based regimen, while a trend toward weight gain was observed for PLWH after switching to another INSTI-based regimen.
•
The proportion of PLWH having a weight/BMI increase >0% and ≥5% post-switch was also higher in the INSTI cohort than in the PI cohort.
•
This study is the first containing data post-INSTI switch that supports the idea that ART management may be an option to address INSTI-related weight gain among PLWH with a higher risk of weight gain.
•
Future studies with larger sample sizes and additional follow-up are needed to confirm these findings.
Author contributions
B Emond, A Shah, M Vermette-Laforme, C Rossi and M-H Lafeuille contributed to study conception and design, collection and assembly of data and data analysis and interpretation. BK Bookhart, D Anderson and P Donga contributed to study conception and design and data analysis and interpretation. All authors reviewed and approved the final content of this manuscript.
Acknowledgments
Part of the material in this manuscript was presented at the 24th International AIDS Conference (AIDS 2022) held from 29 July to 2 August 2022, as an e-poster presentation.
Financial & competing interests disclosure
This study was funded by Janssen Scientific Affairs, LLC. The study sponsor was involved in several aspects of the research, including the study design, the interpretation of data, the writing of the manuscript and the decision to submit the manuscript for publication. B Emond, A Shah, M Vermette-Laforme, C Rossi and M-H Lafeuille are employees of Analysis Group, Inc., a company that provided consulting services to Janssen Scientific Affairs, LLC for the development and conduct of this study and manuscript. BK Bookhart, D Anderson and P Donga are employees of Janssen Scientific Affairs, LLC and are stockholders of Johnson & Johnson. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing and editorial assistance were provided by K Milbers, a former employee and F Chik, a current employee of Analysis Group, Inc., a consulting company that has provided paid consulting services to Janssen Scientific Affairs, LLC, which funded the development and conduct of this study and manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary figure.docx)
- Download
- 42.37 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Arasteh K, Yeni P, Pozniak A et al. Efficacy and safety of darunavir/ritonavir in treatment-experienced HIV type-1 patients in the POWER 1, 2 and 3 trials at week 96. Antivir. Ther. 14(6), 859–864 (2009).
2.
Farnham PG, Gopalappa C, Sansom SL et al. Updates of lifetime costs of care and quality-of-life estimates for HIV-infected persons in the United States: late versus early diagnosis and entry into care. J. Acquir. Immune Defic. Syndr. 64(2), 183–189 (2013).
3.
Lundgren JD, Babiker AG, Gordin F et al. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N. Engl. J. Med. 373(9), 795–807 (2015).
4.
Lifson AR, Grund B, Gardner EM et al. Improved quality of life with immediate versus deferred initiation of antiretroviral therapy in early asymptomatic HIV infection. AIDS 31(7), 953–963 (2017).
5.
Gallant J, Hsue PY, Shreay S, Meyer N. Comorbidities among US patients with prevalent HIV infection – a trend analysis. J. Infect. Dis. 216(12), 1525–1533 (2017).
• A large cohort study (>64,000 PLWH) which matched PLWH to HIV-negative controls in the US between 2003 and 2013. The reported findings include an increased comorbidity burden among PLWH, with the most common comorbidities being essential hypertension, hyperlipidemia and endocrine disorders.
6.
Narayan KM, Boyle JP, Thompson TJ, Gregg EW, Williamson DF. Effect of BMI on lifetime risk for diabetes in the U.S. Diabetes Care 30(6), 1562–1566 (2007).
7.
Bae YS, Choi S, Lee K et al. Association of concurrent changes in metabolic health and weight on cardiovascular disease risk: a nationally representative cohort study. J. Am. Heart Assoc. 8(17), e011825 (2019).
8.
Koethe JR, Jenkins CA, Lau B et al. Rising obesity prevalence and weight gain among adults starting antiretroviral therapy in the United States and Canada. AIDS Res. Hum. Retroviruses 32(1), 50–58 (2016).
• A large cohort study (>14,000 PLWH) which matched PLWH to HIV-negative controls in North America between 1998 and 2010. The reported findings include an increase in baseline BMI from 23.8 to 24.8 kg/m2 when initiating ART, as well as an increase in the proportion of PLWH who were obese when initiating ART; 18% of normal BMI PLWH became obese after 3 years of ART.
9.
Silverberg M, Leyden W, Alexeef S et al. Changes in body mass index over time in persons with and without HIV. 23rd International AIDS Conference (2020).
10.
Buzón-Martín L. Weight gain in HIV-infected individuals using distinct antiretroviral drugs. AIDS Rev. 22(3), 158–167 (2020).
11.
Mazzitelli M, Isabel Pereira B, Moyle G et al. Factors associated with overweight/obesity in a cohort of people living with HIV over 50 years of age. AIDS Care 34(4), 542–544 (2022).
12.
Asundi A, Olson A, Jiang W et al. Integrase inhibitor use associated with weight gain in women and incident diabetes mellitus. AIDS Res. Hum. Retroviruses 38(3), 208–215 (2022).
13.
Bedimo R, Adams-Huet B, Taylor B, Lake J, Luque A. 538. Integrase inhibitor-based HAART is associated with greater BMI gains in Blacks, Hispanics, and women. Open Forum Infect. Dis. 5(S1), S199 (2018).
14.
Guidelines for the use of antiretroviral agents in adults and adolescents living with HIV (updated September 21, 2022). https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-arv/guidelines-adult-adolescent-arv.pdf (October 5, 2022).
15.
Eckard AR, Mccomsey GA. Weight gain and integrase inhibitors. Curr. Opin. Infect. Dis. 33(1), 10–19 (2020).
16.
Chow W, Donga P, Côté-Sergent A et al. An assessment of weight change associated with the initiation of a protease or integrase strand transfer inhibitor in patients with human immunodeficiency virus. Curr. Med. Res. Opin. 36(8), 1313–1323 (2020).
•• A large, recent cohort study (>20,000 PLWH) which generated balanced cohorts (using IPTW) of PLWH initiating an INSTI or a PI in the US between 2017 and 2019. The PI cohort was significantly less likely to experience ≥5% weight or BMI gain (OR [≥5% weight gain] = 0.61; p = .014; OR [≥5% BMI gain] = 0.51; p < .001), and mean weight/BMI gain was significantly lower in the PI cohort.
17.
Emond B, Rossi C, Cote-Sergent A et al. Body mass index increase and weight gain among people living with HIV-1 initiated on single-tablet darunavir/cobicistat/emtricitabine/tenofovir alafenamide or bictegravir/emtricitabine/tenofovir alafenamide in the United States. Curr. Med. Res. Opin. 38(2), 287–298 (2022).
• Recent cohort study which generated balanced cohorts (>1,000 PLWH per cohort; balanced using IPTW) who were treatment-naïve or virologically suppressed and initiated either single-tablet darunavir/cobicistat/emtricitabine/tenofovir alafenamide (DRV/c/FTC/TAF) or bictegravir/emtricitabine/tenofovir alafenamide (BIC/FTC/TAF) between 2017 and 2020. Reported results included a larger BMI or weight increase at consecutive time points in PLWH initiating BIC/FTC/TAF (12 months: mean difference in BMI = 1.23 kg/m2; p < .001; mean difference in weight = 2.84 kg [6.26 lbs]; p = 0.008) relative to those initiating DRV/c/FTC/TAF.
18.
Bourgi K, Jenkins CA, Rebeiro PF et al. Weight gain among treatment-naïve persons with HIV starting integrase inhibitors compared to non-nucleoside reverse transcriptase inhibitors or protease inhibitors in a large observational cohort in the United States and Canada. J. Int. AIDS Soc. 23(4), e25484 (2020).
19.
Wu KS, Anderson C, Little SJ. Integrase strand transfer inhibitors play the main role in greater weight gain among men with acute and early HIV infection. Open Forum Infect. Dis. 8(1), ofaa619 (2021).
20.
Norwood J, Turner M, Bofill C et al. Weight gain in persons with HIV switched from efavirenz-based to integrase strand transfer inhibitor-based regimens. J. Acquir. Immune. Defic. Syndr. 76(5), 527 (2017).
21.
Pantazis N, Papastamopoulos V, Antoniadou A et al. Changes in body mass index after initiation of antiretroviral treatment: differences by class of core drug. Viruses 14(8), (2022).
22.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
23.
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 28(25), 3083–3107 (2009).
24.
Bourgi K, Rebeiro PF, Turner M et al. Greater weight gain in treatment-naive persons starting dolutegravir-based antiretroviral therapy. Clin. Infect. Dis. 70(7), 1267–1274 (2020).
25.
Chen YW, Hardy H, Pericone CD, Chow W. Real-world assessment of weight change in people with HIV-1 after initiating integrase strand transfer inhibitors or protease inhibitors. J. Health Econ. Outcomes Res. 7(2), 102–110 (2020).
•• A recent cohort study using electronic health records between 2016 and 2018 with matched US cohorts (>1,500 PLWH), half of whom initiated a PI-based ART regimen and half of whom initiated an INSTI-based regimen. The reported findings include a significantly greater mean weight gain among INSTI initiators (1.3 kg) (95% CI: 0.5–2.0), a higher proportion with ≥5% weight gain (OR = 1.3, 95% CI: 1.0–1.6), and a 2.5 kg greater mean weight gain (95% CI: 0.7–4.2) and a higher proportion with ≥5% weight gain in females, relative to PI initiators.
26.
Mounzer K, Brunet L, Hsu R et al. Changes in body mass index associated with antiretroviral regimen switch among treatment-experienced, virologically suppressed people living with HIV in the United States. AIDS Res. Hum. Retroviruses 37(11), 852–861 (2021).
27.
Mazzitelli M, Trunfio M, Putaggio C et al. Viro-immunological, clinical outcomes and costs of switching to BIC/TAF/FTC in a cohort of people living with HIV: a 48-week prospective analysis. Biomedicines 10(8), 1823 (2022).
28.
Venter WDF, Sokhela S, Calmy A et al. Weight gain stopping/switch rules for antiretroviral clinical trials. AIDS 35(Suppl. 2), S183–S188 (2021).
29.
Abbamonte JM, Cristofari NV, Weiss SM, Kumar M, Jayaweera DT, Jones DL. Heart health and behavior change in HIV-infected individuals. AIDS Behav. 25(2), 615–622 (2021).
30.
HIV by Group. www.cdc.gov/hiv/group/index.html (2022).
31.
Lake JE, Wu K, Bares SH et al. Risk factors for weight gain following switch to integrase inhibitor–based antiretroviral therapy. Clin. Infect. Dis. 71(9), e471–e477 (2020).
32.
Sax PE, Erlandson KM, Lake JE et al. Weight gain following initiation of antiretroviral therapy: risk factors in randomized comparative clinical trials. Clin. Infect. Dis. 71(6), 1379–1389 (2020).
33.
Coelho LE, Jenkins CA, Shepherd BE et al. Weight gain post-ART in HIV+ Latinos/as differs in the USA, Haiti, and Latin America. The Lancet Regional Health – Americas 8 (2022).
34.
Chen Y-W, Anderson D, Pericone CD, Donga P. Real-world assessment of weight change in African American females and Hispanics with HIV-1 after initiating integrase strand-transfer inhibitors or protease inhibitors. J. Health Econ. Outcomes Res. 9(1), 1–10 (2022).
•• A recent study which included two cohorts of female African Americans (>3400 PLWH) or Hispanics (>1800 PLWH) who initiated either a PI-based ART regimen or an INSTI-based ART regimen between 2015 and 2018, balanced via IPTW. Main findings include female African American INSTI initiators having 1.5 kg greater mean weight gain (2.1 kg vs 0.6 kg; p = 0.033), and a higher proportion with ≥5% weight gain (odds ratio [OR] = 1.2; 95% CI [1.0–1.4]) compared to PI initiators; among Hispanics, INSTI initiators had a higher proportion with ≥5% weight gain.
35.
Nduka CU, Stranges S, Kimani PK, Sarki AM, Uthman OA. Is there sufficient evidence for a causal association between antiretroviral therapy and diabetes in HIV-infected patients? A meta-analysis. Diabetes Metab. Res. Rev. 33(6), (2017).
36.
Kumar S, Samaras K. The impact of weight gain during HIV treatment on risk of pre-diabetes, diabetes mellitus, cardiovascular disease, and mortality. Front. Endocrinol. (Lausanne) 9, 705 (2018).
37.
Herrin M, Tate JP, Akgun KM et al. Weight gain and incident diabetes among HIV-infected veterans initiating antiretroviral therapy compared with uninfected individuals. J. Acquir. Immune Defic. Syndr. 73(2), 228–236 (2016).
38.
Mccann K, Shah S, Hindley L et al. Implications of weight gain with newer anti-retrovirals: 10-year predictions of cardiovascular disease and diabetes. AIDS 35(10), 1657–1665 (2021).
39.
Mccomsey GA, Emond B, Shah A et al. Association between weight gain and the incidence of cardiometabolic conditions among people living with HIV-1 at high risk of weight gain initiated on antiretroviral therapy. Infect. Dis. Ther. (2022) (Epub ahead of print).
40.
Petoumenos K, Kuwanda L, Ryom L et al. Effect of changes in body mass index on the risk of cardiovascular disease and diabetes mellitus in hiv-positive individuals: results from the D:A:D Study. J. Acquir. Immune Defic. Syndr. 86(5), 579–586 (2021).
41.
A study of darunavir/cobicistat/emtricitabine/tenofovir alafenamide (D/C/F/TAF) evaluated as a fixed dose combination regimen in participants switching from an integrase inhibitor who have experienced rapid weight gain (DEFINE). https://clinicaltrials.gov/ct2/show/NCT04442737 (2022).
42.
Doravirine for persons with excessive weight gain on integrase inhibitors and tenofovir alafenamide. https://clinicaltrials.gov/ct2/show/NCT04636437 (2022).
43.
Venter WDF, Moorhouse M, Sokhela S et al. Dolutegravir plus two different prodrugs of tenofovir to treat HIV. N. Engl. J. Med. 381(9), 803–815 (2019).
44.
Mallon PW, Brunet L, Hsu RK et al. Weight gain before and after switch from TDF to TAF in a U.S. cohort study. J. Int. AIDS Soc. 24(4), e25702–e25702 (2021).
Information & Authors
Information
Published In
Copyright
© 2022 Analysis Group, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 August 2022
Accepted: 10 November 2022
Published online: 29 November 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world weight changes in people with HIV-1 at risk of weight gain (female, Black or Hispanic) switching from integrase strand transfer inhibitors. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0147
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Paula Debroy, Jordan E. Lake, To Switch or not to Switch: are there any Antiretroviral Strategies to Attenuate Weight Gain in People with HIV?, Current HIV/AIDS Reports, 10.1007/s11904-026-00782-3, 23, 1, (2026).
- John R Koethe, Jordan E Lake, Amy Kantor, Laura Smeaton, Kristine Erlandson, Laura Moran, Pablo Belaunzaran-Zamudio, Alan Landay, Rafael E Campo, Paula Debroy, Jaclyn Ann Bennet, Jane O'Halloran, Win Min Han, Oladapo Alli, Michael Leonard, Roy M Gulick, A 48-Week, Randomized Controlled Trial of Doravirine for Individuals With HIV and Obesity on Integrase Inhibitors and Tenofovir Alafenamide: The Do IT Study (ACTG A5391), Clinical Infectious Diseases, 10.1093/cid/ciag196, 83, 1, (e81-e89), (2026).
- XiaoYong Chen, Guijin Liang, Zenglu Zheng, Yun Cao, Association between early prophylactic heparin therapy and mortality in patients with septic shock secondary to respiratory infections: analysis based on MIMIC-IV database, BMC Infectious Diseases, 10.1186/s12879-025-11963-7, 25, 1, (2025).
- Iulia Filip, Strategies for managing weight gain associated with antiretroviral therapy: switch or add?, AIDS, 10.1097/QAD.0000000000004078, 39, 2, (N3-N5), (2024).
- Konstantinos Markakis, Olga Tsachouridou, Eleni Georgianou, Dimitrios Pilalas, Sideris Nanoudis, Symeon Metallidis, Weight Gain in HIV Adults Receiving Antiretroviral Treatment: Current Knowledge and Future Perspectives, Life, 10.3390/life14111367, 14, 11, (1367), (2024).
- David Anderson, Moti Ramgopal, Debbie P Hagins, Johnnie Lee, Richard Bruce Simonson, Tien-Huei Hsu, Ping Xu, Nina Ahmad, William R Short, DEFINE: A Prospective, Randomized, Phase 4 Trial to Assess a Protease Inhibitor–Based Regimen Switch Strategy to Manage Integrase Inhibitor–Related Weight Gain, Clinical Infectious Diseases, 10.1093/cid/ciae449, 80, 3, (602-612), (2024).