The acute effects of action observation training on upper extremity functions, cognitive processes and reaction times: a randomized controlled trial
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To investigate the acute effects of action observation training on upper extremity functions, cognitive functions and response time in healthy, young adults. Materials & methods: A total of 60 participants were randomly divided into five groups: the self-action observation group, action observation group, action practice group, non-action observation group and control group. The Jebsen–Taylor hand function test (JTHFT), nine-hole peg test, serial reaction time task and d2 test of attention were applied to the participants before and after the interventions. Results: JTHFT performance with both non-dominant and dominant hands improved significantly compared with baseline in all groups (p < 0.001). JTHFT performance with non-dominant and dominant hands differed between the groups (p < 0.001). Conclusion: Action observation training seems to enhance the performance of upper extremity-related functions. Observing self-actions resulted in statistically significant positive changes in more variables compared with other methods. However, its clinical effectiveness over the other methods should be investigated in future long-term studies.
Clinical Trial Registration: NCT04932057 (ClinicalTrials.gov)
Observing the activities of others engages an extended parieto-premotor brain network known as the action observation network, which overlaps somewhat with the cortical network recruited for action preparation and execution [1,2]. Sensorimotor activity during action observation may enhance action-related perception [3]. Predictive coding is a computational model of cognition and an effort to explain human behaviors and thoughts in terms of calculations performed by the brain [4]. According to the predictive coding hypothesis, other people's action sensory results are compared with sensory predictions created by the same hierarchical neuronal machinery for movement planning and execution [5,6]. Action observation training can be used to create complementary responses in a turn-taking way (for example, in sports) or to synchronize our movements with those of others at the same time (e.g., when handling an object) [7].
The role of attention seems to be a critical issue in converting observation into action. Activation in the brain during action observation is, in a way, automatic; in other words, even if an individual has no intention of acting on the perceived stimuli, this process occurs. On the other hand, when we engage with complicated surroundings to achieve specific activities, our actions must be directed toward the correct task at the right time. Consequently, selection mechanisms have developed to allow goal-directed behavior sequentially [8]. It has been found that diverting attention from an action observation task to a second cognitive task affects different parameters of the resonant response, preserving time course and muscle selection while drastically reducing the excitability of spinal and cortical motor neurons, as well as the kinematic specificity of the response [9]. At the same time, it could be argued that watching goal-directed videos, which is the basis of action observation training, may enhance attention, an essential cognitive function. Evidence suggests that action observation training can be an effective type of cognitive training to complement physical practice to facilitate desired behavior outcomes [10].
To accomplish everyday functional activities, skilled arm and hand mobility is essential [11], requiring high cognitive processing [12,13]. Most people with neurological conditions have varying degrees of disability related to the upper extremities [14]. Therefore, most rehabilitation programs target improving upper extremity functions. Recent evidence suggests that action observation training is a promising tool for this goal [15,16]. However, the optimal program is not known. Additionally, what should be observed and how the movement should be observed have rarely been studied. While some studies show that it is more effective if people watch their videos [17,18], it is also reported that this is not the case [19]. In addition, even though action observation training can improve upper extremity function [20–21], there is limited evidence of its effects on cognitive functions. Since upper extremity and cognitive functions are associated with each other, and while performing action observation training high cognitive resources are used, the authors speculate that action observation training would improve cognitive functions in parallel with upper extremity function.
Overall, the present study aimed to investigate the acute effects of action observation training on upper extremity functions, cognitive functions and response time in healthy, young adults. It was hypothesized that action observation treatments would improve upper extremity functions compared with watching natural images and controls. The study's second hypothesis was that observing self-videos could improve performance better than observing someone else. The authors thought that if these hypotheses are confirmed even in healthy, young adults, these results will form the basis for full-scale randomized controlled trials in people with different neurological conditions with upper extremity dysfunction.
Materials & methods
Study design & ethical considerations
This study was a randomized controlled trial, and Dokuz Eylul University Ethical Committee approved its protocol (No.: 5845-GOA, Date: 21/12/2020, Clinical Trials ID: NCT04932057). Written informed consent was obtained prior to participation.
Participants
Healthy, young individuals were recruited for this study, which was advertised at three classes at Izmir Katip Celebi University. The researchers explained the study to the students in a course, and the volunteers and eligible students were invited to the laboratory to perform the assessments. Hand dominance was assessed by a modified version of the Edinburgh handedness questionnaire [22]. To minimize the effects of hand dominance, strongly right-handed (>laterality of 80%) healthy adults were included. Exclusion criteria included any neurological, orthopedic or systemic diseases that may affect upper extremity functionality and vision disorders.
Due to a lack of similar research previously, it was planned to include 12 participants per group, for a total of 60 participants, as was recommended by Julious [23].
Procedure
Participants were randomly divided into five groups – the self-action observation group, action observation group, action practice group, non-action observation group and control group – using a simple single sequence randomization method by a researcher (T Kahraman) who did not engage in assessment and intervention procedures. Participants were allocated to the groups according to the numbers 1–5, which they drew. They were allocated to the self-action observation group if they drew 1, the action practice group if they drew 2 and so on. Participants and outcome assessors were blinded to group allocation. Before the assignment, demographic information was gathered, and upper extremity functionality was assessed using the Jebsen-Taylor hand function test (JTHFT) and the nine-hole peg test (NHPT). Reaction time was measured using the serial reaction time task, and cognitive performance was assessed using the d2 test of attention (d2). Tests were administered in random order by using four sealed envelopes. Participants in the self-action observation group watched a video recording that was taken while they were performing JTHFT. The video was watched four times. The JTHFT performance of a third person was shown to participants in the action observation group. Similarly, they watched the video recording four times. Participants in the action practice group performed the JTHFT four more times after the baseline examination. Participants in the non-action observation group watched a slide show of landscape and nature pictures (i.e., motionless images), while participants in the control group waited in a silent and well-lighted room. Table 1 presents the procedure applied to the study groups. All interventions, including the slide show in the non-action observation group and the waiting time of the control group, lasted approximately 25–30 min. After the interventions, the JTHFT, NHPT, serial reaction time task and d2 were applied to all participants. Previously, Schaefer et al. [24] investigated the within-session practice effects of JTHFT and indicated that four trials were required to achieve steady-state performance. Therefore, the amount of practice was designated according to their findings.
Outcomes
Upper extremity functions
The study's primary outcomes were upper extremity-related functions evaluated with JTHFT and NHPT. Jebsen et al. developed the JTHFT to objectively assess manual dexterity in activities of daily living [25]. The test can be administered quickly and requires only easily available items [26]. Previous research has shown the reliability of the test [27]. JTHFT has seven subtests: handwriting; turning over cards; picking up small, common objects; feeding simulation; stacking checkers; moving large, light objects; and moving large, heavy objects. Due to the large task execution differences between non-dominant and dominant hands, a low reliability writing subtest is commonly excluded [24,28]. Therefore, JTHFT performance was measured as the total completion time of the other six subtests [11]. Subtests were performed first with a non-dominant hand, followed by the dominant hand. A chronometer was used to track task completion.
The NHPT is one of the most commonly used assessment tools to evaluate hand dexterity, and it is found to be reliable and valid in young adults [29]. Nine small pegs are grasped from a container, inserted into a nine-hole grid and replaced in the container during the test. The test is performed first with the non-dominant hand, followed by the dominant hand as rapidly as possible, and a shorter test period implies greater dexterity [30]. A test procedure that was previously used by Oxford Grice et al. [30] was implemented.
Cognitive performance
A standard version of the d2 was used to assess some aspects of cognitive function. It examines sustained attention, visual scanning and speed of processing [31]. It is administered with a piece of paper and a pencil; the paper covers 14 rows with 47 ‘d’ and ‘p’ characters with surrounding vertical dashes placed below or above the character. The target is the cancelation of ‘d’ characters with two dashes. Both dashes may be placed above, both dashes below, or one dash below and another above. The participant has 20 s for each line and is supposed to cancel the greatest number of target items possible within that time. The test evaluates the performance of the number of items processed, commission errors (canceled non-target items), omission errors (non-canceled target items), overall errors, percentage of errors (given by dividing the number of total errors by the total number of processed characters), total correct cancelation (given by the total number of processed characters – total errors) and fluctuation (the difference between the most character processed line and the least character processed line). The rationale for choosing the d2 was the possible effect of attention on action observation training performance. The test was found to be valid and reliable [32].
Reaction time
A serial reaction time task assesses participants' response times [33]. Four gray squares appear horizontally over a black background on a computer screen during the test. One of the squares becomes red for each trial, which indicates that it is the target square for the response. Participants placed four fingers of their right hands (starting from index to little finger) on the ‘V’, ‘B’, ‘N’, and ‘M’ letters of a keyboard. They were instructed to press the corresponding button when they saw the square turn red. Overall, mean reaction times were recorded [34].
Statistical analyses
The statistical analyses were performed using IBM SPSS Statistics for Windows (version 25.0, IBM Corp., NY, USA). The distribution of the collected data was checked by the Shapiro–Wilk test and by investigating distribution graphs. Due to the normal distribution, parametric tests were applied. Descriptive statistics were presented with mean and standard deviation. The paired-samples t-test was used to assess the difference between the baseline performance and the performance after the intervention within the groups. Delta values were calculated to analyze the difference by subtracting the baseline assessment value from the final assessment value. Continuous baseline variables and delta values were compared using one-way analysis of variance with a Bonferroni correction between the groups. The gender difference was analyzed using the chi-square test. The significance level was set at p < 0.05, and adjusted p-values are presented.
| Study groups | Intervention |
|---|---|
| Self-action observation group | They watched a video recording that was taken while they were performing JTHFT. The video was watched four times. |
| Action observation group | The participants in the action observation group watched the video recording of a third person’s JTHFT performance four times. |
| Action practice group | They practiced JTHFT four times after the baseline assessment. |
| Non-action observation group | They watched a slide show of landscape and nature pictures (i.e., motionless images). |
| Control group | They waited in a silence in a well-lightened room after the baseline assessment. |
JTHFT: Jebsen–Taylor hand function test.
Results
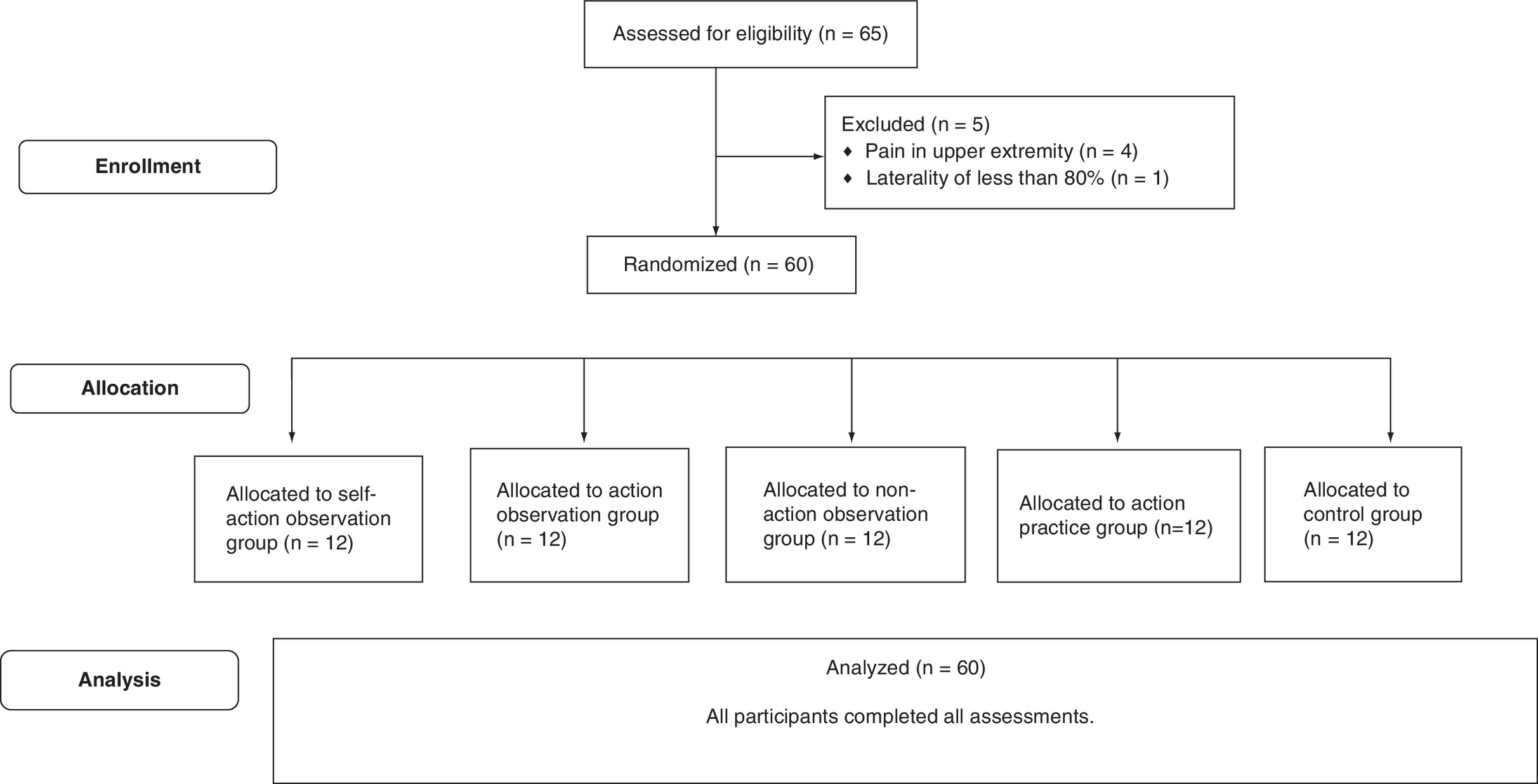
A total of 60 healthy right-handed participants (32 female and 28 male; mean age: 21.32 ± 1.07 years) were included in the study (Figure 1). No significant difference was found in age, gender, height, weight and baseline test performances between the groups (p > 0.05). The demographic characteristics of the participants of the groups and baseline test performances are shown in Table 2.
| sAOG | AOG | APG | nAOG | CG | F/χ2 | p-value | |
|---|---|---|---|---|---|---|---|
| Age (years) | 21.42 ± 1.00 | 21.58 ± 1.17 | 21.59 ± 1.00 | 21.33 ± 1.07 | 21.17 ± 1.19 | 0.401 | 0.807 |
| Height (m) | 1.67 ± 1.05 | 1.72 ± 0.96 | 1.73 ± 0.88 | 1.69 ± 0.59 | 1.71 ± 0.91 | 0.766 | 0.552 |
| Weight (kg) | 61.58 ± 13.29 | 67.54 ± 13.17 | 70.92 ± 14.37 | 62.00 ± 9.81 | 66.33 ± 11.63 | 1.173 | 0.333 |
| BMI (kg/m2) | 21.75 ± 2.79 | 22.75 ± 3.09 | 23.43 ± 2.98 | 21.51 ± 2.28 | 22.70 ± 3.16 | 0.898 | 0.472 |
| Sex, n (%) Female Male | 9 (75) 3 (25) | 5 (42) 7 (58) | 4 (33) 8 (67) | 8 (67) 4 (33) | 6 (50) 6 (50) | 5.76 | 0.218 |
| Upper extremity functionality | |||||||
| JTHFT_Left (s) | 31.57 ± 3.57 | 30.75 ± 2.36 | 30.91 ± 3.55 | 31.01 ± 2.80 | 31.94 ± 3.57 | 0.295 | 0.880 |
| JTHFT_Right (s) | 35.67 ± 3.63 | 32.96 ± 2.76 | 32.60 ± 2.19 | 33.08 ± 2.39 | 33.95 ± 2.19 | 2.527 | 0.051 |
| NHPT_Right (s) | 17.52 ± 2.03 | 17.32 ± 1.57 | 16.61 ± 1.34 | 17.02 ± 1.41 | 17.15 ± 1.49 | 0.567 | 0.687 |
| NHPT_Left (s) | 18.33 ± 1.50 | 18.94 ± 1.79 | 18.94 ± 2.32 | 18.97 ± 1.63 | 18.98 ± 1.58 | 0.301 | 0.876 |
| d2 test of attention variables | |||||||
| Total characters processed | 555.58 ± 67.21 | 563.75 ± 32.02 | 540.50 ± 71.72 | 557.42 ± 60.14 | 531.75 ± 59.11 | 0.589 | 0.672 |
| Errors of commission | 3.25 ± 2.26 | 5.67 ± 4.54 | 5.75 ± 4.05 | 4.33 ± 3.68 | 7.58 ± 4.10 | 2.213 | 0.079 |
| Errors of omission | 27.33 ± 16.00 | 35.50 ± 21.65 | 30.17 ± 18.70 | 32.50 ± 24.03 | 27.67 ± 16.65 | 0.366 | 0.832 |
| Total errors | 30.58 ± 16.14 | 41.17 ± 23.26 | 35.92 ± 20.63 | 36.83 ± 25.50 | 35.25 ± 17.43 | 0.394 | 0.812 |
| Percentage of errors | 5.50 ± 2.83 | 7.36 ± 4.46 | 6.68 ± 3.5 | 6.41 ± 4.09 | 6.50 ± 2.65 | 0.416 | 0.797 |
| Total correct | 525.00 ± 65.68 | 522.42 ± 43.69 | 504.58 ± 70.81 | 520.58 ± 50.61 | 496.50 ± 48.97 | 0.583 | 0.676 |
| Fluctuation | 12.42 ± 6.88 | 13.67 ± 4.58 | 13.00 ± 4.33 | 11.75 ± 3.41 | 15.75 ± 4.96 | 1.145 | 0.345 |
| Reaction time | |||||||
| Serial reaction time task (milliseconds) | 419.15 ± 59.99 | 440.44 ± 44.33 | 418.89 ± 56.14 | 426.09 ± 68.89 | 439.58 ± 74.82 | 0.355 | 0.840 |
Values are presented as mean ± standard deviation unless specified.
AOG: Action observation group; APG: Action practice group; CG: Control group; F: F-value; JTHFT: Jebsen–Taylor hand function test; nAOG: Non-action observation group; NHPT: Nine-hole peg test; sAOG: Self-action observation group; χ2: Chi-square value.
The JTHFT performance with non-dominant and dominant hands improved significantly compared with baseline in all groups (p < 0.001). While there were significant decreases in the NHPT completion time with dominant and non-dominant hands in the self-action observation group (sAOG), the action observation group (AOG) and the action practice group (APG; p < 0.05), no significant difference was observed in the non-action observation group (nAOG) and control group (CG; p > 0.05). Significant improvements were observed in all variables of the d2 test of attention except errors of commission (p = 0.809) in the sAOG. Only the total correct variables significantly increased in the nAOG and CG (Table 3).
| sAOG | AOG | APG | nAOG | CG | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before (mean ± SD) | After (mean ± SD) | p-value | Before (mean ± SD) | After (mean ± SD) | p-value | Before (mean ± SD) | After (mean ± SD) | p-value | Before (mean ± SD) | After (mean ± SD) | p-value | Before (mean ± SD) | After (mean ± SD) | p-value | |
| JTHFT_Left (s) | 31.57 ± 3.57 | 25.14 ± 3.31 | <0.001† | 30.75 ± 2.36 | 25.08 ± 1.72 | <0.001† | 30.91 ± 3.55 | 24.43 ± 2.07 | <0.001† | 31.01 ± 2.80 | 29.11 ± 2.95 | 0.040† | 31.94 ± 3.57 | 28.74 ± 3.27 | <0.001† |
| JTHFT_Right (s) | 35.67 ± 3.63 | 21.74 ± 2.16 | <0.001† | 32.96 ± 2.76 | 22.50 ± 2.24 | <0.001† | 32.60 ± 2.19 | 21.70 ± 1.61 | <0.001† | 33.08 ± 2.39 | 24.90 ± 2.38 | <0.001† | 33.95 ± 2.19 | 25.23 ± 2.11 | <0.001† |
| NHPT_Right (s) | 17.52 ± 2.03 | 15.56 ± 1.90 | <0.001† | 17.32 ± 1.57 | 15.72 ± 0.82 | 0.002† | 16.61 ± 1.34 | 15.49 ± 1.39 | <0.001† | 17.02 ± 1.41 | 16.60 ± 1.48 | 0.228 | 17.15 ± 1.49 | 16.62 ± 1.09 | 0.233 |
| NHPT_Left (s) | 18.33 ± 1.50 | 17.07 ± 1.75 | 0.001† | 18.94 ± 1.79 | 17.44 ± 1.16 | 0.002† | 18.94 ± 2.32 | 17.13 ± 1.75 | <0.001† | 18.97 ± 1.63 | 18.24 ± 1.37 | 0.182 | 18.98 ± 1.58 | 19.08 ± 3.17 | 0.868 |
| Total characters processed | 555.58 ± 67.21 | 601.08 ± 53.91 | 0.017† | 563.75 ± 32.02 | 612.92 ± 19.23 | <0.001† | 540.50 ± 71.72 | 592.17 ± 56.79 | <0.001† | 557.42 ± 60.14 | 595.00 ± 62.29 | <0.001† | 531.75 ± 59.11 | 600.08 ± 37.93 | <0.001† |
| Errors of commission | 3.25 ± 2.26 | 3.00 ± 2.22 | 0.809 | 5.67 ± 4.54 | 5.67 ± 4.31 | 1.000 | 5.75 ± 4.05 | 6.83 ± 2.98 | 0.285 | 4.33 ± 3.68 | 7.42 ± 8.43 | 0.084 | 7.58 ± 4.10 | 8.33 ± 4.62 | 0.616 |
| Errors of omission | 27.33 ± 16.00 | 18.08 ± 12.16 | 0.017† | 35.50 ± 21.65 | 26.25 ± 27.81 | 0.057 | 30.17 ± 18.70 | 20.67 ± 15.27 | 0.025† | 32.50 ± 24.03 | 26.37 ± 23.82 | 0.147 | 27.67 ± 16.65 | 25.67 ± 10.27 | 0.575 |
| Total errors | 30.58 ± 16.14 | 21.08 ± 12.59 | 0.033† | 41.17 ± 23.26 | 31.92 ± 28.38 | 0.070 | 35.92 ± 20.63 | 27.50 ± 16.10 | 0.061 | 36.83 ± 25.50 | 33.78 ± 28.01 | 0.480 | 35.25 ± 17.43 | 34.00 ± 11.79 | 0.780 |
| Percentage of errors | 5.50 ± 2.83 | 3.60 ± 2.22 | 0.013† | 7.36 ± 4.46 | 5.21 ± 4.60 | 0.008† | 6.68 ± 3.5 | 4.66 ± 2.64 | 0.018† | 6.41 ± 4.09 | 5.53 ± 4.20 | 0.215 | 6.50 ± 2.65 | 5.71 ± 2.06 | 0.298 |
| Total correct | 525.00 ± 65.68 | 580.00 ± 58.96 | 0.003† | 522.42 ± 43.69 | 581.00 ± 33.72 | <0.001† | 504.58 ± 70.81 | 564.50 ± 57.72 | <0.001† | 520.58 ± 50.61 | 561.33 ± 57.48 | <0.001† | 496.50 ± 48.97 | 566.08 ± 42.14 | <0.001† |
| Fluctuation | 12.42 ± 6.88 | 7.83 ± 6.26 | 0.008† | 13.67 ± 4.58 | 8.92 ± 2.23 | 0.007† | 13.00 ± 4.33 | 8.83 ± 2.41 | 0.005† | 11.75 ± 3.41 | 8.50 ± 4.12 | 0.001† | 15.75 ± 4.96 | 11.00 ± 4.82 | 0.026† |
| Serial reaction time task (milliseconds) | 419.15 ± 59.99 | 341.56 ± 61.87 | <0.001† | 440.44 ± 44.33 | 347.00 ± 36.40 | <0.001† | 418.89 ± 56.14 | 324.66 ± 57.10 | <0.001† | 426.09 ± 68.89 | 346.02 ± 59.69 | <0.001† | 439.58 ± 74.82 | 349.19 ± 61.91 | <0.001† |
Values are presented as mean ± SD.
†
p < 0.05.
AOG: Action observation group; APG: Action practice group; CG: Control group; JTHFT: Jebsen–Taylor hand function test; nAOG: Non-action observation group; NHPT: Nine-hole peg test; sAOG: Self-action observation group; SD: Standard deviation.
Delta values differed considerably between the groups in JTHFT performance with non-dominant and dominant hands (p < 0.001). In the non-dominant hand, significant differences were observed between the sAOG and nAOG (p < 0.001), the sAOG and CG (p = 0.022), the AOG and nAOG (p = 0.004), the APG and nAOG (p < 0.001) and the APG and CG (p < 0.001). While the JTHFT was performed with the dominant hand, delta values varied significantly between the sAOG and AOG, nAOG and CG (p = 0.004; p < 0.001; p = 0.020; respectively). Additionally, while there were significant differences in delta values of the NHPT completion time with the dominant hand between the sAOG and nAOG (p = 0.048), significant differences were observed in the non-dominant hand between the APG and CG (p = 0.024). No significant difference was observed in any variable of the d2 test of attention and reaction time between the groups (p > 0.05) (Table 4).
| sAOG | AOG | APG | nAOG | CG | ηp2 | F | p-value | Post hoc comparisons with Bonferroni corrections | |
|---|---|---|---|---|---|---|---|---|---|
| Δ JTHFT_Right (s) | -7.51 (-8.65, -6.37) | -5.04 (-7.02, -3.06) | -5.39 (-7.09, -3.69) | -2.55 (-4.56, -0.54) | -2.05 (-2.99, -1.12) | 0.381 | 8.466 | <0.001† | sAOG>nAOG (p < 0.001†), sAOG>CG (p = 0.022†), AOG>nAOG (p = 0.004†), APG>nAOG (p < 0.001†), APG>CG (p = 0.020†) |
| Δ JTHFT_Left (s) | -13.74 (-15.64, -11.83) | -14.27 (-19.17, -9.37) | -14.94 (-18.21, -11.68) | -6.26 (-9.72, -2.79) | -5.61 (-7.40, -3.82) | 0.357 | 7.624 | <0.001† | sAOG>AOG (p = 0.04†), sAOG>nAOG (p < 0.001†), sAOG>CG (p < 0.001†) |
| Δ NHPT_Right (s) | -1.96 (-2.78, -1.152) | -1.60 (-2.48, -0.71) | -1.12 (-1.84, -0.40) | -0.421 (-1.15, 0.30) | -0.53 (-1.45, 0.39) | 0.190 | 3.230 | 0.019† | sAOG>nAOG (p = 0.048†) |
| Δ NHPT_Left (s) | -1.26 (-1.88, -0.64) | -1.51 (-2.33, -0.69) | -1.81 (-2.49, -1.13) | -0.73 (-1.86, 0.40) | 0.09 (-1.14, 1.33) | 0.186 | 3.135 | 0.022† | APG>CG (p = 0.024†) |
| Δ Total characters processed | 45.50 (9.83, 81.17) | 49.17 (28.06, 70.27) | 51.67 (31.53, 71.80) | 51.67 (31.53, 71.80) | 68.33 (42.80, 93.87) | 0.071 | 1.048 | 0.391 | – |
| Δ Errors of commission | -0.25 (-2.47, 1.97) | 0.00 (-2.39, 2.39) | 1.08 (-1.04, 3.21) | 1.08 (-1.04, 3.21) | 0.75 (-2.45, 3.95) | 0.074 | 1.102 | 0.365 | – |
| Δ Errors of omission | -9.25 (-16.46, -2.03) | -9.25 (-18.82, 0.32) | -9.50 (-17.56, -1.44) | -9.50 (-17.56, -1.44) | -2.00 (-9.62, 5.62) | 0.051 | 0.742 | 0.568 | – |
| Δ Total errors | -9.50 (-18.06, -0.94) | -9.25 (-19.38, 0.88) | -8.42 (-17.31, 0.47) | -8.42 (-17.30, 0.47) | -1.25 (-10.86, 8.36) | 0.057 | 0.835 | 0.509 | – |
| Δ Percentage of errors | -1.90 (-3.30, -0.48) | -2.16 (-3.61, -0.70) | -2.02 (-3.63, 0-.41) | -2.02 (-3.63, -0.41) | -0.79 (-2.37, 0.80) | 0.063 | 0.932 | 0.452 | – |
| Δ Total correct | 55.00 (22.61, 87.39) | 58.58 (40.92, 76.24) | 59.92 (42.64, 77.19) | 59.92 (42.64, 77.19) | 69.58 (46.45, 92.71) | 0.075 | 1.107 | 0.363 | – |
| Δ Fluctuation | -4.58 (-7.68, -1.49) | -4.75 (-7.95, -1.55) | -4.17 (-6.76, -1.57) | -4.17 (-6.76, -1.57) | -4.75 (-8.82, -0.68) | 0.015 | 0.213 | 0.930 | – |
| Δ Serial reaction time task (milliseconds) | -76.79 (-92.18, -61.40) | -91.17 (-109.65, -72.68) | -91.50 (-111.89, -71.11) | -80.75 (-96.58, -64.92) | -85.79 (-105.84, -65.74) | 0.058 | 0.844 | 0.503 | – |
†
p < 0.05
Values are presented as means (95% CI).
AOG: Action observation group; APG: Action practice group; CG: Control group; Δ: Delta; F: Test statistic for F-test; JTHFT: Jebsen–Taylor hand function test; ηp2: Partial eta squared; nAOG: Non-action observation group; NHPT: Nine-hole peg test; sAOG: Self-action observation group.
Discussion
This study aimed to examine the acute effects of action observation training on upper extremity functions, cognitive processes and response times in young, healthy adults. It was hypothesized that action observation interventions would enhance upper extremity functions compared with natural image watching and controls. The second hypothesis was that observing self-actions would be more effective than watching another person. While all participants improved the total JTHFT performance, only participants in the action observation groups (the self-action observation group and action observation group) and participants who practiced the test four more times (the action practice group) decreased the nine-hole peg test completion time significantly compared with the baseline. Also, there was no statistically significant difference between the groups, but the d2 test of attention (d2) showed that the people in the self-action observation group had better cognitive performance.
Previously, several studies examined the effects of action observation training on upper extremity functions (reaching, grasping, object manipulation etc.) in both healthy participants [35–38] and people with various diseases [15,20,21]. Sakaguchi and Yamasaki combined action observation with motor imagery and compared the effectiveness of this method with the physical training group [38]. Sport stacking, an upper extremity functionality test, was chosen as the main outcome, and both groups completed 20 min of practice per day for 3 days. After the training, both groups improved their test completion performance, and there was no significant difference between them. Although the researchers did not include any neurophysiological tests in the research design, they have attributed that performance improvement to the activation of greater motor areas and the corticospinal tract based on previous findings. Romano Smith et al. [39] investigated the effects of motor imagery, action observation and a combination of motor imagery and action observation on dart-throwing performance. The groups practiced the interventions three times a week for 6 weeks, and pre-training and post-training dart-throwing performances were compared. After the interventions, it was found that while there was no improvement in the control group, participants in the action observation, motor imagery and a combination of motor imagery and action observation groups improved their performance significantly. Moreover, improvement in the combination of motor imagery and action observation was greater than in the action observation and motor imagery groups. The researchers argued that the difference had arisen from the production of more effective visuomotor command encoding by adding motor imagery to action observation. In the current study, the authors did not add any motor imagery practice, and they observed that the observation of action alone is an effective way to improve upper extremity functions, even with a single 20 min session. Similarly, Adhikari et al. [16] examined the impact of a single session of action observation training on improving upper extremity functions in subacute stroke patients. The study's primary outcomes included hand performance-related subtests of the Wolf motor function test and Stroke Impact Scale. They reported significant improvements in action observation training, including group compared with usual care. Furthermore, improvements were sustained for 7 days after the intervention. Even though the authors of the current study did not reassess the participants to report long-term effects, which was not in the scope of this study, the findings are in parallel with theirs. Additionally, participants in action observation groups only watched the JTHFT in the videos; however, their nine-hole peg test performance was significantly enhanced compared with baseline. So, after action observation training, an improvement in performance on a specific task that was observed could be transferred to another task involving the upper extremities.
One main concern regarding the effects of action observation training is focus and attention issues. Emerson et al. argued that practitioners seldom teach participants how to observe the desired activity or what elements to focus on, which is a drawback in the present delivery technique for action observation training [40]. In the present study, participants in the action observation groups were instructed to “focus on the nature of movement in the video and try to find cues on how to perform faster when you practice the test” to eliminate the disadvantage of the action observation technique. Furthermore, the authors evaluated sustained attention and working memory, which are essential elements of cognitive functions [41], using the d2. Although the difference between the groups was not statistically significant, participants scored better in almost all the d2 variables.
Additionally, while participants in the self-action observation group and action practice group significantly reduced the number of errors in the d2 at the final assessment, there was no significant difference in the final assessment compared with baseline in the remaining three groups. An increase in attention level may be one possible cause of better performance in both upper extremity-related tasks. In a recent study by Kemmerer, the literature was reviewed, and it has been concluded that mirror neuron system responses are enhanced when people's attention is drawn to the mechanical components of observed actions [42]. The findings of the present study are thereby in parallel with previous conclusions.
One interesting finding of the present study was that participants watched their videos and performed observed actions better than those who watched someone else's actions. Several mechanisms could be suggested in that regard. First, the participants may have focused more on the actor on the screen, which greatly impacts action observation performance [42]. Ste-Marie et al. discussed the issue in depth and stated that there is insufficient evidence to decide which observation technique (self-action or a model's actions) is more effective, and both observation procedures have different benefits for the observers [43]. Holmes and Calmels have indicated that when viewing self-generated actions as opposed to other people's actions, there may be a stronger functional resemblance of brain activity to that during motor execution [18]. Second, another reason might be the impact of different perspectives. As studied by Ge et al., the first-person perspective causes more massive and greater activation compared with the third-person perspective [44]. In that regard, Nagai and Tanaka investigated event-related desynchronization responses under three conditions: motor imagery + self-action observation, motor imagery + observation of another person's action and motor imagery only; like the findings of the present study, they found that participants who observed their hand movements with motor imagery had greater event-related desynchronization [36]. In the present study, the authors also say that observing one's own actions improves performance on a simple hand-opening-and-closing task and on the JTHFT, which is a much more difficult hand-functioning test.
There are some limitations to the present study. First, the sample size per group seems too small; however, post-analysis revealed that the study achieved a power of at least 0.97 for the main outcomes. Therefore, the authors believe that these findings have not been found by chance, which is supported by the evidence in the literature. Second, the data of any high-tech devices could not be included as an outcome. Nevertheless, using easily applicable outcome measurements such as JTHFT and the nine-hole peg test is valuable for researchers and may be used in daily practice by clinicians. Third, the learning effect is generally a problem in acute effect studies. Even though the authors tried to decrease the learning effect by applying a literature-recommended number of trials before each test, it is obvious that the learning effect and/or placebo effect might still be present, as significant improvements were observed in the control groups (i.e., the non-action observation group and control group). This point should indicate cautiousness when interpreting the results of this study. Finally, the hypotheses were tested only on a healthy population. However, the study's results from a group of people who were healthy could have a big effect on neuroscience research.
Conclusion
In conclusion, action observation training seems to enhance the performance of upper extremity-related functions. Moreover, observing self-actions resulted in statistically significant positive changes in more variables compared with other methods. However, future long-term studies should investigate its clinical effectiveness over the other methods. This study's observed performance improvements might be attributed to both neurophysiological and behavioral mechanisms.
Future perspective
In the future, researchers should use high-tech outcome measures to find out more about these mechanisms and look at how different action observation techniques affect people with neurological conditions.
•
Action observation training can be used to create complementary responses in a turn-taking way or to synchronize movements with those of others at the same time.
•
Activation in the brain during action observation is, in a way, automatic; in other words, even if an individual has no intention of acting on the perceived stimuli, this process occurs.
•
A single-session action observation training may enhance upper extremity functions.
•
After action observation training, an improvement in performance on a specific task that was observed could be transferred to another task involving the upper extremities.
•
Observing self-videos may improve performance to a greater extent compared with observing another person.
•
Performance improvements might be attributed to both neurophysiological and behavioral mechanisms.
Author contributions
Y Emuk, T Kahraman and Y Sengul contributed to the design and implementation of the research, the analysis of the results and the writing of the manuscript.
Acknowledgments
The authors sincerely thank the participants of the study.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. Individual participant data that underlie the results reported in this article after deidentification (text, tables and figures) will be shared immediately following the publication. Proposals should be directed to [email protected]. To gain access, data requesters will need to sign a data access agreement. Clinical trial identifier: NCT04932057.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Giese MA, Rizzolatti G. Neural and computational mechanisms of action processing: interaction between visual and motor representations. Neuron 88(1), 167–180 (2015).
2.
Hardwick RM, Caspers S, Eickhoff SB, Swinnen SP. Neural correlates of action: comparing meta-analyses of imagery, observation, and execution. Neurosci Biobehav Rev 94, 31–44 (2018).
3.
Avenanti A, Annella L, Candidi M, Urgesi C, Aglioti SM. Compensatory plasticity in the action observation network: virtual lesions of STS enhance anticipatory simulation of seen actions. Cereb Cortex 23(3), 570–580 (2013).
4.
Rao RP, Ballard DH. Predictive coding in the visual cortex: a functional interpretation of some extra-classical receptive-field effects. Nat Neurosci 2(1), 79–87 (1999).
5.
Friston K, Mattout J, Kilner J. Action understanding and active inference. Biol Cybern 104(1), 137–160 (2011).
6.
Donnarumma F, Costantini M, Ambrosini E, Friston K, Pezzulo G. Action perception as hypothesis testing. Cortex 89, 45–60 (2017).
7.
Cardellicchio P, Dolfini E, Hilt PM, Fadiga L, D'ausilio A. Motor cortical inhibition during concurrent action execution and action observation. Neuroimage 208, 116445 (2020).
8.
Tipper SP. From observation to action simulation: the role of attention, eye-gaze, emotion, and body state. Q J Exp Psychol 63(11), 2081–2105 (2010).
9.
Puglisi G, Leonetti A, Landau A, Fornia L, Cerri G, Borroni P. The role of attention in human motor resonance. PLOS ONE 12(5), e0177457 (2017).
10.
Kim T, Frank C, Schack T. A systematic investigation of the effect of action observation training and motor imagery training on the development of mental representation structure and skill performance. Front Hum Neurosci 11, 499 (2017).
11.
Stewart JC, Saba A, Baird JF, Kolar MB, O'Donnell M, Schaefer SY. Effect of standing on a standardized measure of upper extremity function. OTJR 41(1), 32–39 (2020).
12.
Van De Winckel A, De Patre D, Rigoni M et al. Exploratory study of how cognitive multisensory rehabilitation restores parietal operculum connectivity and improves upper limb movements in chronic stroke. Sci Rep 10(1), 1–11 (2020).
13.
Hooyman A, Malek-Ahmadi M, Fauth EB, Schaefer SY. Challenging the relationship of grip strength with cognitive status in older adults. Int J Geriatr Psychiatry 36(3), 433–442 (2021).
14.
Burridge J, Alt Murphy M, Buurke J et al. A systematic review of international clinical guidelines for rehabilitation of people with neurological conditions: what recommendations are made for upper limb assessment? Front Neurol 10, 567 (2019).
15.
Borges LR, Fernandes AB, Melo LP, Guerra RO, Campos TF. Action observation for upper limb rehabilitation after stroke. Cochrane Database Syst Rev 10(10), CD011887 (2018).
16.
Adhikari SP, Tretriluxana J, Chaiyawat P, Jalayondeja C. Enhanced upper extremity functions with a single session of action-observation-execution and accelerated skill acquisition program in subacute stroke. Stroke Res Treat 2018, 1490692 (2018).
• A pioneering study showing that even a single-session action observation training may be effective.
17.
Oñate JA, Guskiewicz KM, Marshall SW, Giuliani C, Yu B, Garrett WE. Instruction of jump-landing technique using videotape feedback: altering lower extremity motion patterns. Am J Sports Med 33(6), 831–842 (2005).
18.
Holmes P, Calmels C. A neuroscientific review of imagery and observation use in sport. J Mot Behav 40(5), 433–445 (2008).
19.
Ghobadi N, Daneshfar A, Shojaei M, Ghobadi N. Comparing the effects of self and expert models observation on performance and learning of futsal side foot pass. Euro J Exp Biol 3(1), 508–512 (2013).
20.
Alamer A, Melese H, Adugna B. Effectiveness of action observation training on upper limb motor function in children with hemiplegic cerebral palsy: a systematic review of randomized controlled trials. Pediatric Health Med Ther 11, 335 (2020).
21.
Rocca MA, Meani A, Fumagalli S et al. Functional and structural plasticity following action observation training in multiple sclerosis. Mult Scler J 25(11), 1472–1487 (2019).
22.
Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9(1), 97–113 (1971).
23.
Julious SA. Sample size of 12 per group rule of thumb for a pilot study. Pharm Stat 4(4), 287–291 (2005).
24.
Schaefer SY, Saba A, Baird JF, Kolar MB, Duff K, Stewart JC. Within-session practice effects in the Jebsen hand function test (JHFT). Am J Occup Ther 72(6), 7206345010p7206345011–7206345010p7206345015 (2018).
•• A pioneering study investigating with-in session practice effects of a commonly used clinical tool.
25.
Jebsen R, Taylor N, Trieschmann R, Trotter M, Howard L. An objective and standardized test of hand function. Arch Phys Med Rehabil 50(6), 311–319 (1969).
26.
Fabbri B, Berardi A, Tofani M et al. A systematic review of the psychometric properties of the Jebsen–Taylor hand function test (JTHFT). Hand Surg Rehabil 40(5), 560–567 (2021).
27.
Sığırtmaç İC, Öksüz Ç. Investigation of reliability, validity, and cutoff value of the Jebsen–Taylor hand function test. J Hand Ther 34(3), 396–403 (2021).
28.
Sears ED, Chung KC. Validity and responsiveness of the Jebsen–Taylor hand function test. J Hand Surg Am 35(1), 30–37 (2010).
29.
Temporiti F, Mandaresu S, Calcagno A et al. Kinematic evaluation and reliability assessment of the nine hole peg test for manual dexterity. J Hand Ther (2022) (Epub ahead of print).
30.
Oxford Grice K, Vogel KA, Le V, Mitchell A, Muniz S, Vollmer MA. Adult norms for a commercially available nine hole peg test for finger dexterity. Am J Occup Ther 57(5), 570–573 (2003).
31.
Da Silva-Sauer L, Garcia RB, Ehrich De Moura A, Fernández-Calvo B. Does the d2 test of attention only assess sustained attention? Evidence of working memory processes involved. ApplNeuropsycholAdult (2022). (Epub ahead of print)
32.
Caglar E, Koruc Z. Reliability and validity of d2 test of attention for athletes. Hacettepe Journal of Sport Sciences 17(2), 58–80 (2006).
33.
Nissen MJ, Bullemer P. Attentional requirements of learning: evidence from performance measures. Cogn Psychol 19(1), 1–32 (1987).
34.
Trofimova O, Mottaz A, Allaman L, Chauvigné LAS, Guggisberg AG. The “implicit” serial reaction time task induces rapid and temporary adaptation rather than implicit motor learning. Neurobiol Learn Mem 175, 107297 (2020).
35.
Brihmat N, Tarri M, Quidé Y et al. Action, observation or imitation of virtual hand movement affect differently regions of the mirror neuron system and the default mode network. Brain Imaging Behav 12(5), 1363–1378 (2018).
36.
Nagai H, Tanaka T. Action observation of own hand movement enhances event-related desynchronization. IEEE Trans Neural Syst Rehabilitation Eng 27(7), 1407–1415 (2019).
37.
Chen J, Kan W, Liu Y et al. Frequency-specific equivalence of brain activity on motor imagery during action observation and action execution. Int J Neurosci 131(6), 599–608 (2021).
38.
Sakaguchi Y, Yamasaki S. The effects of physical training versus combined action observation and motor imagery in conjunction with physical training on upper-extremity performance. Somatosens Mot Res 38(4), 366–372 (2021).
39.
Romano Smith S, Wood G, Coyles G, Roberts JW, Wakefield CJ. The effect of action observation and motor imagery combinations on upper limb kinematics and EMG during dart-throwing. Scand J Med Sci Sports 29(12), 1917–1929 (2019).
40.
Emerson JR, Binks JA, Scott MW, Kenny RP, Eaves DL. Combined action observation and motor imagery therapy: a novel method for post-stroke motor rehabilitation. AIMS Neurosci 5(4), 236 (2018).
41.
Wilke J, Giesche F, Klier K, Vogt L, Herrmann E, Banzer W. Acute effects of resistance exercise on cognitive function in healthy adults: a systematic review with multilevel meta-analysis. Sports Med 49(6), 905–916 (2019).
42.
Kemmerer D. What modulates the mirror neuron system during action observation? multiple factors involving the action, the actor, the observer, the relationship between actor and observer, and the context. Prog Neurobiol 205, 102128 (2021).
•• A comprehensive review investigating the action observation-related factors.
43.
Ste-Marie DM, Lelievre N, St Germain L. Revisiting the applied model for the use of observation: a review of articles spanning 2011–2018. Res Q Exerc Sport 91(4), 594–617 (2020).
• An updated study reviewing recent articles.
44.
Ge S, Liu H, Lin P, Gao J, Xiao C, Li Z. Neural basis of action observation and understanding from first- and third-person perspectives: an fMRI study. Front Behav Neurosci 12, 283 (2018).
Information & Authors
Information
Published In
Pages: 987 - 998
PubMed: 35770659
Copyright
© 2022 Future Medicine Ltd.
History
Received: 22 April 2022
Accepted: 17 June 2022
Published online: 30 June 2022
Keywords:
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The acute effects of action observation training on upper extremity functions, cognitive processes and reaction times: a randomized controlled trial. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0079
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Tania López Hernández, Marina Caparó Ferré, Albert Salas-Huetos, Isabel Salvat Salvat, Cristina Adillón Camón, Influence of referent selection on balance in action observation: A randomized controlled trial, Complementary Therapies in Medicine, 10.1016/j.ctim.2025.103150, 90, (103150), (2025).
- Yange Wei, Shanyuan He, Peng Luo, Hanshuo Su, Yuanle Chen, Shisen Qin, Zhongguo Zhang, Rongxun Liu, Dongshuai Wei, Juan Wang, Fei Wang, Chuansheng Wang, Combining transcranial direct current stimulation with music therapy improves cognitive function in schizophrenia: study protocol for a randomized, double-blind, sham-controlled clinical trial, Frontiers in Psychiatry, 10.3389/fpsyt.2025.1543789, 16, (2025).
- Almudena Cerezo-Zarzuelo, Marcos Rios-Lago, Francisco Jose Sanchez-Cuesta, Beatriz Gavilan-Agusti, Alfonso Hurtado-Martinez, Juan Pablo Romero-Muñoz, Effects of transcranial direct current stimulation on motor and cognitive function in paediatric brain damage: a systematic review and meta-analysis, Disability and Rehabilitation, 10.1080/09638288.2025.2496783, (1-19), (2025).
- Kevser Sevik Kacmaz, Bayram Unver, The efficacy of taping on elbow proprioception in healthy individuals: A single-blinded randomized placebo-controlled study, Journal of Hand Therapy, 10.1016/j.jht.2024.02.014, 37, 2, (201-208), (2024).
- Katsuya Sakai, Tsubasa Kawasaki, Yumi Ikeda, Junpei Tanabe, Akari Matsumoto, Kazu Amimoto, Differences in the early stages of motor learning between visual-motor illusion and action observation, Scientific Reports, 10.1038/s41598-023-47435-8, 13, 1, (2023).
- Yusuf Emuk, Turhan Kahraman, Yesim Sengul, Effects of a single session action observation training on hand function in healthy young adults: a randomised controlled assessor and participants-blinded trial, Somatosensory & Motor Research, 10.1080/08990220.2023.2165055, 41, 1, (18-25), (2023).