The cost–effectiveness, of pegcetacoplan compared with ravulizumab for the treatment of paroxysmal nocturnal hemoglobinuria, in a UK setting
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Paroxysmal nocturnal hemoglobinuria (PNH) is a rare blood disorder characterized by hemolytic anemia, bone marrow failure and thrombosis. We evaluated, the cost–effectiveness of pegcetacoplan, a novel proximal C3 inhibitor, versus ravulizumab in patients with PNH and hemoglobin levels <10.5 g/dl despite eculizumab treatment in the UK healthcare and social services setting. Materials & methods: A Markov cohort framework model, based on the data from the pivotal trial of pegcetacoplan (PEGASUS/NCT03500549), evaluated lifetime costs and outcomes. Patients transitioned through 3 PNH hemoglobin level/red blood cell transfusion health states. Results: Pegcetacoplan provides lower lifetime costs/greater quality-adjusted life years (£6,409,166/14.694QALYs, respectively) versus ravulizumab (£6,660,676/12.942QALYs). Conclusion: Pegcetacoplan is associated with enhanced anemia control, greater QALYs and reduced healthcare costs versus ravulizumab in the UK healthcare and social services setting.
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare, potentially fatal blood disorder [1] characterized by hemolytic anemia, bone marrow failure and thrombosis [2,3]. In PNH, a proportion of hematopoietic stem cells lack various cell surface proteins due to an inability to produce the glycosylphosphatidylinositol anchor that is required for these proteins to be bound to the cell surface [4–6]. This defect is caused by somatic loss-of-function mutations in the PIGA gene [1]. CD59 and CD55 are glycosylphosphatidylinositol-linked complement regulatory proteins that protect blood cells when the complement system is activated [2]. However, in PNH, without these protective proteins, individuals experience complement-mediated destruction of blood cells and the subsequent symptoms of the disease [7].
PNH may present at any age, but it is most frequently diagnosed in people between 30 and 42 years of age [8,9] and affects males and females equally [9]. The global prevalence of the disease is approximately 1–1.5 cases per million [1,10,11]. In the UK, the incidence is estimated to be 1 in 770,000/year [12]. Untreated PNH is associated with considerable disease burden in terms of mortality (with 10-year rate of 24–29%) [13,14] and economic costs [15] especially given its high disease activity [16] and associated systemic complications, including smooth muscle dystonia (presenting as chest and abdominal pain, dysphagia and erectile dysfunction) [1,17], impaired renal function and thrombotic events [18,19]. Disabling anemia-related fatigue is a leading symptom of PNH, and in addition to weakness [1,20–22], contributes to significant impairment in patient health-related quality of life (HRQoL), work productivity and everyday activities [1,23,24]. Thromboembolism is the most common cause of mortality in patients with PNH [14]. Moreover, disease paroxysms can be triggered by events such as physical exertion, vaccinations, infections, pregnancy, or after excessive alcohol consumption. Some patients may also pass dark-colored urine because of the excreted breakdown product of red blood cells (i.e., hemoglobinuria) [25].
Red blood cell transfusions can address anemia in PNH and improve daily functioning [26]; however, recipients face further risks of morbidity and mortality associated with transfusion-related iron overload [27]. The only curative treatment for PNH [19,26], allogeneic bone marrow transplantation, is also associated with considerable morbidity and mortality risk and is not recommended in countries where anti-complement therapy is available [28]. Therefore, therapeutic management of hemolytic disease and/or thromboembolic complications remain the key objectives across international clinical practice. In the UK, current treatment options comprise complement component 5 inhibitors (C5i), including eculizumab and ravulizumab [16,29]. These humanized monoclonal antibodies are specifically designed to target the complement protein C5, prevent its cleavage and thereby prevent the formation of the terminal complement complex, the membrane attack complex [26,30].
Available in Europe since 2007 [31], eculizumab has been the first anti-C5 monoclonal antibody treatment for adults and children that provides sustained inhibition of complement-mediated intravascular hemolysis (IVH) [1]. Eculizumab increases 5-year survival to 95.5% (95% CI: 87.6-98.5%) in the real world compared with survival rates associated with the untreated course of disease (66%; 95% CI: 41.4–85.1%) [32]. Ravulizumab is an eculizumab-like monoclonal antibody that has a half-life four-times longer than eculizumab [33]. Ravulizumab was first licensed by the European Medicines Agency (EMA) in 2019 for treatment in adults and paediatric patients (of body weight ≥40 kg) with PNH who present with hemolysis and clinical symptoms despite treatment with eculizumab for at least the past 6 months [34]. Ravulizumab is now recommended in the UK National Health System (NHS) setting within its marketing authorization as an option for treating PNH in adults [35].
Despite the important benefits that eculizumab provides in the management of PNH [32], the requirement for frequent dosing has limited its clinical utility, and thus been outmoded by ravulizumab given its reduced intravenous infusion frequency (every 8 weeks vs every 2 weeks for eculizumab) [36], facility for dosing individualization via therapeutic drug monitoring approaches and patient preferences [37,38]. However, further limitations remain for C5i due to the emergence of C3-mediated extravascular hemolysis (EVH) and its effect on patient HRQoL [7,39,40].
Pegcetacoplan is a recently available PNH treatment option in the UK. A novel proximal C3 inhibitor (C3i), pegcetacoplan targets the complement cascade, thereby controlling IVH without associated increases in EVH [41]. The self-administered twice weekly 1080 mg dose is delivered with a syringe system infusion pump [42]. Pegcetacoplan is approved by the US FDA for the treatment of adults with PNH [42] based on evidence from PEGASUS (NCT03500549), the pivotal phase 3, prospective, randomized, multicenter, open-label, active-comparator, controlled clinical trial of pegcetacoplan versus eculizumab. For UK prescribing, pegcetacoplan is approved by the European Medicines Agency [43] and the Medicines & Healthcare Products Regulatory Agency [44], and recently recommended by the National Institute for Health and Care Excellence (NICE) for adults with PNH and hemoglobin (Hb) levels <10.5 g/dl after treatment with a C5 inhibitor for at least 3 months.
In PEGASUS, pegcetacoplan provided significant improvement in the primary endpoint, serum Hb levels, and was non-inferior to eculizumab in reducing transfusion requirements and in reducing reticulocyte counts, with comparable safety to eculizumab [41]. In particular, the week 16 Hb levels between the 2 groups were significantly different (3.84 g/dl [95% CI: 2.33–5.34]; p <0.0001) on least-squares mean change from baseline (CFB). Pegcetacoplan also provided substantial and clinically meaningful improvements in patient reported outcomes, including symptoms of fatigue (measured on the Functional Assessment of Chronic Illness Therapy–Fatigue scale), dyspnoea, and HRQoL (measured on the Linear Analog Scale Assessment and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 Scale [EORTC QLQ-C30]) [41,45].
Given the potential lifelong need for treatment and care, the funding of new healthcare technologies for orphan diseases with high unmet needs is as equally crucial as funding diseases with high prevalence; yet allowing patient access to new and highly specialized technologies (HSTs) for rare disease remains a global challenge for healthcare commissioners given ever-constrained budgets [46]. Hence, value assessment frameworks for rare diseases must balance such health policy factors as severity and unmet need with standard efficiency criteria such as cost–effectiveness [47]. Cost–utility analysis (CUA) is a form of cost–effective analysis (CEA) that weighs the incremental health economic benefits, including costs and HRQoL, associated with a new treatment modality in relation to best practice. Some healthcare reimbursement authorities across Europe mandate such analyses to inform health technology assessments for highly specialized technologies for rare diseases as well as non-orphan healthcare technologies [47–50].
This study evaluates the cost–effectiveness, in the UK setting, of pegcetacoplan compared with the newest C5i, ravulizumab, for the treatment of PNH in patients whose anemia was insufficiently controlled despite at least 3 months treatment with eculizumab.
Materials & methods
We conducted the CUA from the perspective of the UK NHS and social services. We developed a de novo Markov model in Microsoft Excel to estimate the long-term cost–effectiveness of the introduction of pegcetacoplan on the UK PNH treatment pathway. The model estimated the lifetime costs and quality-adjusted life years (QALYs) incurred in the pegcetacoplan label population of adults with PNH whose anemia was insufficiently controlled (ie, had Hb levels <10.5 g/dl) despite at least 3 months of treatment with eculizumab and were therefore candidates for switching to pegcetacoplan (Table 1) [41].
| PEGASUS Trial data (n = 80) | ||
|---|---|---|
| Variable | Value (mean/ percentage) | Measurement of uncertainty - distribution (±SE) |
| Baseline patient characteristics | ||
| Age (years) | 48.8 | Normal (±1.79) |
| Sex (female) | 61.3% | Beta |
| Weight (kg) | 75.25 | Normal (±1.97) |
| Time since diagnosis (years) | 10.18 | Normal (±0.96) |
| Treatment outcomes | ||
| Intravenous hemolysis breakthrough and pegcetacoplan treatment discontinuation (at week 16) | 2.44% | Beta |
| Intravenous hemolysis breakthrough requiring a single dose of pegacetacoplan continued thereafter | 1.9% | Beta |
| Percentage of patients receiving chelation therapy (deferoxamine mesilate and deferasirox) | 27.5% | Beta |
| Utilities | ||
| Health states | ||
| No transfusion and Hb ≥10.5 | 0.808 | Beta |
| No transfusion and Hb <10.5 | 0.738 | Beta |
| Transfusion required | 0.695 | Beta |
| Disutilities | ||
| Iron overload | -0.03 | Normal |
| Costs and utilization | ||
| Medication | ||
| Pegcetacoplan 1080 mg PAS price (£) | 3100.00 | Fixed |
| Ravulizumab 300 mg price (£) | 4533.00 | Fixed |
| Prophylactic antibiotic cost (£) | 1.04 | Gamma |
| Chelation therapy cost (per 4-week cycle) (£) | 513.62 | |
| Pegcetacoplan administration cost (£) | 78.67 | Normal |
| Ravulizumab administration cost (£) | 0.00 | Normal |
| Blood transfusion unit cost (£) | 532.51 | Gamma (±5.325a) |
| Mean number of transfusions per cycle | 1.0 | Fixed |
Hb: (Serum) Hemoglobin; IV: Intravenous; SE: Standard error.
A comprehensive systematic literature review (SLR) enabled the identification of models and inputs to the CUA, with searches conducted on 30 July 2020 (updated on 11 March 2021) in MEDLINE, MEDLINE In-Process, Embase, BioScience Information Service of Biological Abstracts, EconLit and Cochrane Library. A single combined search identified existing cost– and clinical– effectiveness, HRQoL/utility and cost/resource use studies in PNH.
Model structure
Informed by clinical data from PEGASUS, the pivotal trial of pegcetacoplan [41], the CUA model was based on a Markov cohort framework whereby patients transitioned between 3 PNH health states representing Hb level at a given trial visit and red blood cell transfusion requirements during the previous 4 weeks. Together, the health states represented different levels of disease status and impacts on PNH healthcare costs and QALYs. The model assumed a cycle length of 4 weeks, based on the length of time between clinical visits in PEGASUS [41]; consequently, health state transitions occurred every 4 weeks.
We stratified transfusion avoidance on patient Hb level above and below a threshold level of 10.5 g/dl; this threshold was consistent with the PEGASUS trial inclusion criteria of Hb <10.5 g/dl and validated by clinical opinion for capturing differences in HRQoL between PNH health states [51,52]. According to clinicians, although anemia is defined as Hb <13.5 g/dl in men and Hb <12 g/dl in women, patients with PNH may have a Hb lower than the general population but feel ‘normal’ because of symptom adaptation [51,52]. Given this, a lower threshold of Hb level of 10.5 g/dl was deemed appropriate for categorising patients as having ‘controlled’ or ‘uncontrolled’ anemia. Hence, the model represented 3 relevant health states including: transfusion-avoidant Hb high (Hb ≥10.5 g/dl); transfusion-avoidant Hb low (Hb <10.5 g/dl); and transfusion dependent (Hb <10.5 g/dl). The model also allowed patients to enter the ‘absorbing’ state of death (Figure 1).
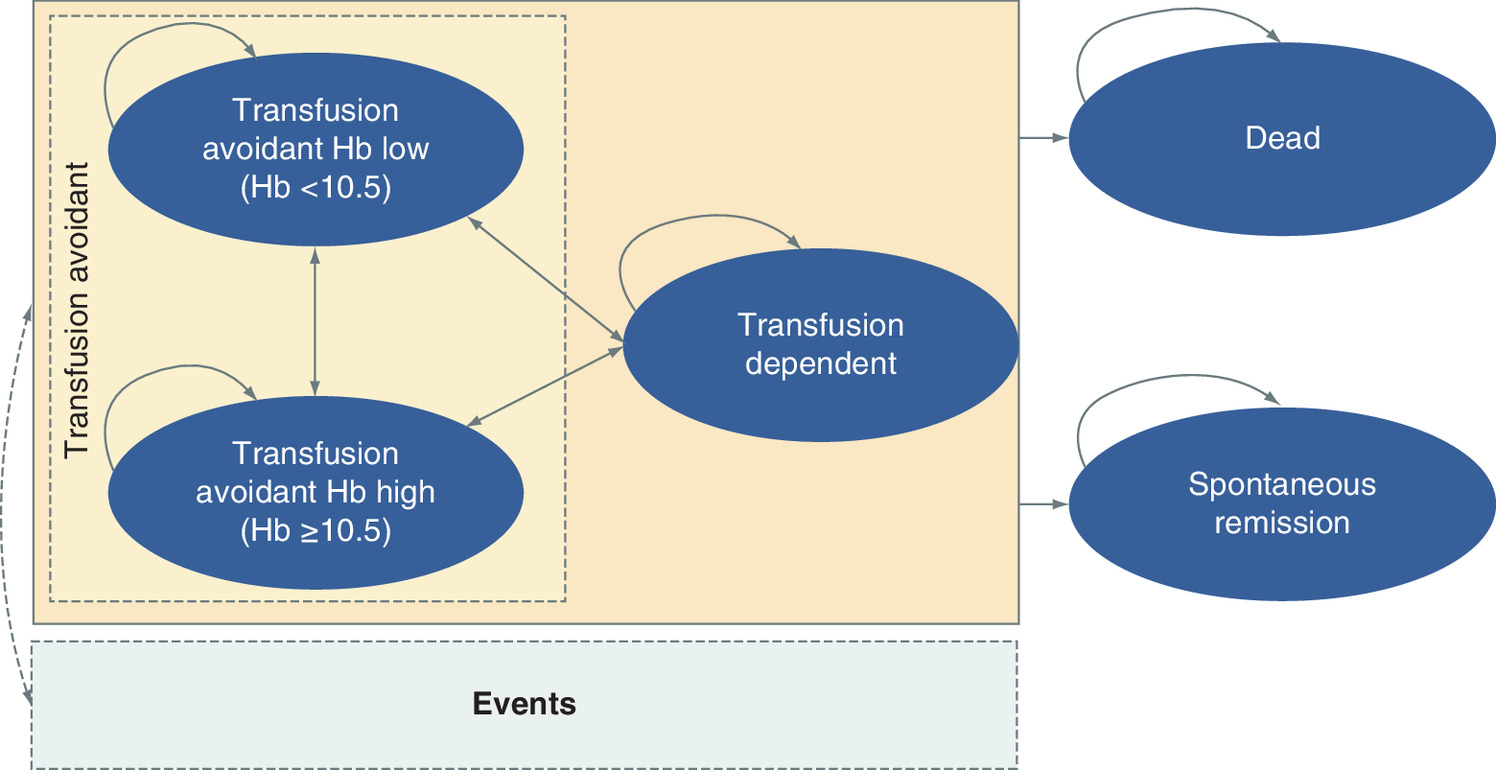
Figure 1. Markov model diagram.
Hb: (Serum) Hemoglobin.
Based on clinical opinion, patients in better health states (ie, the transfusion-avoidant Hb high [Hb ≥10.5 g/dl]) would be expected to accumulate the lowest costs and greatest HRQoL benefits; patients in the transfusion-avoidant Hb low (Hb <10.5 g/dl) state would accumulate relatively higher costs and reduced HRQoL due to anemia, while patients in the transfusion-dependent (Hb <10.5 g/dl) health state would accumulate the highest costs and most impaired HRQoL as most of the negative health effects and costs associated with PNH are due to blood transfusions [3].
Clinical inputs
Treatment response
A post hoc analysis of PEGASUS informed patient baseline clinical status, demographics (Table 1) and transitions between health states for patients treated with pegcetacoplan in the model [41]. The treatment period of PEGASUS comprised a 4-week run-in period during which all patients received pegcetacoplan and concomitant eculizumab treatment; a 16-week controlled period where, after 1:1 randomization, patients received either pegcetacoplan (n = 41) at a dose of 1080 mg subcutaneously twice weekly, or eculizumab (n = 39) administered by intravenous (IV) infusion at the current and stable prescribed dosage [51,52]. A 32-week open-label pegcetacoplan-only period then followed.
PEGASUS trial data from the randomized controlled phase informing the model included, besides the primary efficacy endpoint of mean CFB in Hb level at Week 16: transfusion status, HRQoL based on the EORTC-QLQ-C30 and drug dosage. To inform clinical inputs we first considered anchored matching-adjusted indirect comparison (MAIC) to assess the comparative effectiveness of these treatments among patients previously treated with eculizumab [53,54]. The MAIC used individual patient-level data from PEGASUS and adjusted the trial population to match average aggregate baseline characteristics reported in the ALXN1210-PNH-302 (Study 302) trial for patients receiving ravulizumab [53]. An eculizumab control arm anchored comparisons across both studies [54].
The MAIC showed that, besides equivalent mean CFB in LDH levels, all other clinical, hematological and HRQoL endpoints for patients previously treated with eculizumab were better for patients who received pegcetacoplan compared with those who received ravulizumab [54]. However, there was also evidence to suggest heterogeneity between PEGASUS and the ravulizumab pivotal trial (Study 302), such as in the inclusion criteria (e.g., the 302 study enrolled eculizumab-stable patients), the randomized controlled periods (16 weeks + 4-week run-in phase in PEGASUS versus 26 weeks in Study 302) and the differing dosing of eculizumab between the 2 trials; therefore, we deemed that the results of the MAIC were subject to bias [54]. In lieu, we assigned values for efficacy and safety of ravulizumab based on the head-to-head non-inferiority trial data of ALXN1210-PNH-302 (Study 302) [53,55]. This assumption was also consistent with health technology assessments (HTAs) of ravulizumab conducted by the NICE in England and the Scottish Medicines Agency (SMC) [16,56].
Iron overload
Blood transfusion therapy results in accumulated iron, a key component of Hb present in the red blood cells that the body cannot remove if at an excess level. Therefore, transfused patients can experience iron overload, which can lead to progressive damage of the liver, heart and endocrine system if not removed. Based on iron overload rates in PEGASUS, the model assumed that patients could experience iron overload with a probability of 0.0065 per cycle when in the transfusion dependent health state.
Breakthrough hemoloysis
Patients in the model on pegcetacoplan could experience breakthrough hemolysis at a probability of 0.0315 per cycle if in the transfusion avoidant (Hb <10.5 g/dl health state) or at a probability of 0.1334 per cycle in the transfusion dependent health state, as based on the outcomes in PEGASUS. Moreover, for patients treated with pegcetacoplan, those experiencing breakthrough received a single dose of eculizumab or switched back to eculizumab treatment in PEGASUS [57]; this practice was applied to the model and validated by input from and expert panel of clinicians [57]. For ravulizumab patients, we applied a conservative assumption in the model of no breakthrough hemolysis.
Mortality
In the base-case, we assumed that the background mortality rate among patients receiving any complement inhibitor was comparable with the age- and sex-adjusted general population, as per published evidence [32]. However, we modeled PNH-specific mortality in scenario analyses.
Health state transitions
We calculated transition probabilities between health states for patients receiving pegcetacoplan from the PEGASUS patient-level data from the randomized control period (weeks 4–16) (Table 2). All patients entered the model in the transfusion-avoidant (Hb <10.5 g/dl) health state, with their baseline characteristics reflecting those of patients in PEGASUS. The model assumed a sustained treatment effect, and patients accumulated differential costs and QALYs until death. In the base-case, the model did not consider spontaneous remission, as we would not expect any remission to vary by treatment arm. However, we modeled spontaneous remission in the scenario analyses.
| From | To | ||
|---|---|---|---|
| No transfusion and Hb <10.5 g/dl | No transfusion and Hb ≥10.5 g/dl | Transfusion required | |
| Transition probabilities for patients receiving pegcetacoplan (%) | |||
| No transfusion and Hb <10.5 g/dl | 43.7 | 49.0 | 7.2 |
| No transfusion and Hb ≥10.5 g/dl | 3.1 | 96.6 | 0.3 |
| Transfusion required | 26.6 | 61.2 | 12.2 |
| Transition probabilities for patients receiving ravulizumab (%) | |||
| No transfusion Hb and <10.5 g/dl | 65.2 | 0.1 | 34.7 |
| No transfusion and Hb ≥10.5 g/dl | 74.2 | 3.0 | 22.8 |
| Transfusion required | 40.4 | 0.1 | 59.5 |
Hb: (Serum) hemoglobin.
To estimate transition rates, we first classified patients by health states according to their Hb level and transfusion dependency during the planned visits during the PEGASUS randomized control period. A multinomial logistic regression model that included variables to adjust for the interactions between treatments and visit categories then allowed the calculation of transition probabilities between health states. With current health state as the dependent variable, covariates included the prior 4-weeks' health state, treatment, visit category and age. The regression also included a patient-level random intercept term [58]. Through interviews and an advisory board, clinical experts and health economists validated the final model structure and inputs [51,57].
Utilities
For utilities, we applied the EORTC QLQ-C30 data collected in PEGASUS to map to EQ-5D-3L utility weights (in line with the NICE reference case [59]); this approach addressed the lack of data EQ-5D data collected in the PEGASUS clinical study. A mapping algorithm converted EORTC-QLQ-C30 scores from PEGASUS to EuroQol 5 Dimension 3 Level (EQ-5D-3L) utilities [60], and approach consistent with the UK HTAs for ravulizumab [16,56] and NICE HTA guidance overall [61]. We considered 2 mapping algorithms, by Longworth et al. [60,62] and McKenzie et al. [63], respectively. The Longworth algorithm, based on multinomial logistic regressions, has five separate regressions for the five dimensions of utility on the E5-5D-3L: mobility, self-care, usual activities, pain and anxiety/depression. We applied this algorithm to validate our mapping approach. The utilities applied in the model corresponded to the model health states, as per an analysis conducted to confirm the impact of Hb and transfusion status on utilities. We assumed that utilities remained constant over time; however, we adjusted the estimates for age [60].
IV infusion
Ravulizumab is given as an IV infusion every 8 weeks. A published targeted literature review reported that the frequent regular IV infusion of ravulizumab versus eculizumab was associated with a utility increment of 0.025 [64]. In addition, both NICE and Scottish Medicines Agency HTAs assumed a utility increment of 0.057 associated with the reduced administration frequency of ravulizumab [16,65]. Patients have also reported a preference for subcutaneous over IV delivery in other disease settings [64].
Adverse events
In the base-case, we assumed that the mapped EQ-5D-3L utilities accounted for adverse events. However, in the scenario analyses, we applied disutilities for adverse events as sourced from the SLR, adjusted for the probability of developing the effects per cycle (Supplementary Table 3) and the duration of the event.
Iron overload
To account for disutilities related to iron overloads, targeted literature searches identified a disutility of -0.03 associated with chelation therapy [66]. We applied this value for ravulizumab additively based on the proportion of patients who received chelation therapy in the eculizumab arm in PEGASUS to estimate disutility (-0.00789) (Table 1; Supplementary Table 4).
Costs
Direct costs considered in the model covered PNH treatments, prophylactic antibiotic treatment, blood transfusion, treatment monitoring and adverse events, iron overload and ravulizumab infusion (Table 1). We based dosing assumptions for pegcetacoplan on data from PEGASUS week 4 to week 16 visits.
PNH treatment
For ravulizumab treatment costs, we assumed patients were administered a maintenance weight-based dosing, as per the label [67]. We excluded administration costs in the base-case since the analytic population comprised those who would have been receiving C5i before switching to ravulizumab.
For pegcetacoplan treatment administration costs (Table 3), in the base case we assumed that patients had their first dose administered in a clinic where they also received training in subcutaneous self-administration (£49 assuming 20 min of specialist nurse time based on NHS salary band 6) [68] and self-administered subsequent doses at home. We assumed that nurses also provided support for administering the second and third doses (30 min per home visit; £29.67) [68]. We excluded one-off pump costs for pegcetacoplan at-home infusion in the base-case.
| Treatment | Dosing regimen | Split (%) | ||||
|---|---|---|---|---|---|---|
| Pegcetacoplan | Labeled dosing: • 4-week run-in period: 1080 mg SC administration twice weekly + current dose of eculizumab • Maintenance period: 1080 mg SC administration twice weekly | 100 | ||||
| Dosing units | Cost per administration (£) | |||||
| Initial dose (applied in cycle 1 only): first SC administration includes training for self-administration at home (20 min nurse specialist band 6 £147 per hour of contact time) | £49.00 | |||||
| Dose 2 and 3 (applied in cycle 1 only): at-home care assumed for doses 2 and 3 to check patients administering correctly (30 min community nurse £89 per hour of patient related work) | £29.67 | |||||
| Cost per dose (£) | Doses per week (n) | Drug cost per week (£) | Patients (%) | |||
| 3100 | 2.00 | 6200 | 100% | |||
| Weighted average cost per week (£): | 4600 | |||||
| Ravulizumab | Body weight range (kg) | Loading dose (mg) | Maintenance dose (mg) | |||
| ≥40 to <60 | 2400 | 3000 | ||||
| ≥60 to <100 | 2700 | 3300 | ||||
| ≥100 | 3000 | 3600 | ||||
| Maintenance dose: Weight-based IV infusion every 8 weeks starting 2 weeks after the loading dose | ||||||
| Labeled dosing • 900 mg IV infusion every 14 ± 2 days | 70 | |||||
| Dosing escalation • IV 900 mg IV every 11 days | 1.3 | |||||
| Dosing escalation • IV 1200 mg every 11 days | 26.3 | |||||
| Dose escalation • IV 1500 mg every 11 days | 2.5 | |||||
| Eculizumab | Loading dose | 600 mg IV infusion every week | 6300 | 1 | 6300 | NA |
| Labeled dosing | IV 900 mg every 2 weeks | 9450 | 0.50 | 4725 | 70% | |
| Dose escalation | IV 900 mg every 11 days | 9450 | 0.64 | 6014 | 1.3% | |
| Dose escalation | IV 1200 mg every 2 weeks | 12,600 | 0.50 | 6300 | 26.3% | |
| Dose escalation | IV 1500 mg every 2 weeks | 15,750 | 0.50 | 7875 | 2.5% | |
| Weighted average cost per week (£): | 5233 | |||||
| Weighted average cost per cycle (£): | 20,933 | |||||
IV: Intravenous; PNH: Paroxysmal nocturnal hemoglobinuria; SC: Subcutaneous.
We applied the list price for pegcetacoplan (£3100 per 1080 mg; Table 3) and for ravulizumab based drug price (£4533 per 300 mg) on that assumed in the most recent UK HTAs [16,56]. We did not need to account for wastage costs in the model, as the required dosages for neither pegcetacoplan nor ravulizumab result in any wastage.
Blood transfusion
Monitoring
Monitoring costs, applied at each cycle based on the health state of the patient, stemmed from hematologist visits (£110.61) [16] and blood tests (£32.18) [70]. We estimated these costs based on the number of visits/tests per cycle multiplied by the respective unit costs for each resource per health state, as based on clinical opinion (Table 1 & Supplementary Table 5).
Iron overload
To capture the costs of iron overload in patients administered ravulizumab, we considered the baseline (ie, pre-run in) proportion of patients in the PEGASUS trial receiving chelation therapy [41]. The baseline iron overload medication use (3.8% on deferoxamine mesilate and 23.8% on deferasirox) was multiplied by the cost of the treatments per cycle (Table 1 & Supplementary Table 6) [41].
For pegcetacoplan patients in PEGASUS, given sufficient increases in Hb levels due to the earlier inhibition of the complement cascade provided by treatment [41] blood removal (i.e., venesection), rather than iron chelation, provided a viable option to address iron accumulation at baseline or following any transfusions and for maintenance treatment (average of three venesections per year) [57]. For the cost estimate, we multiplied the unit cost of venesection (i.e., the cost of half an hour at a hematology day unit) [69] by the number of venesections occurring in a 4-week cycle, adjusted by the percentage of patients who received iron chelation therapy at baseline in PEGASUS.
Breakthrough hemolysis
For pegcetacoplan patients, we modeled breakthrough hemolysis costs based on the 1 out of 41 patients (2.4%) in the PEGASUS pegcetacoplan arm who experienced breakthrough [41] and estimated a per-cycle rate of 2.5% based on four episodes in the 16-week treatment period. The event was costed at £9450, the list price of eculizumab, in addition to costs of the associated transfusion-dependent health state [71]. The remaining three patients with breakthrough discontinued pegcetacoplan at week 16 and incurred medical costs of breakthrough treatment, was estimated at £392.86 (Table 1 & Supplementary Table 7).
Adverse events
The model did not include the cost of adverse events in the base-case, but only in the scenario analyses. Per the summaries of product characteristics, the adverse event rates are comparable for ravulizumab [34] and pegcetacoplan. Therefore, we estimated costs based on the probability of developing an event per cycle (Supplementary Table 3) and the corresponding unit cost per adverse event (Supplementary Table 8) per treatment arm. We calculated a sum product of the probabilities of events and their respective unit costs to obtain total adverse event costs per treatment respectively: £48.49 for pegcetacoplan; £46.49 for eculizumab (in those pegcetacoplan patients who revert back to eculizumab) and £6.87 for ravulizumab.
Analysis
We discounted costs and utilities at 3.5% per annum as mandated for the base-case by NICE in England [72] and adjusted costs to 2021 British pounds sterling. Clinically plausible scenarios within the deterministic analyses were characterized by assumptions of non-inferiority between treatments, in terms of breakthrough hemolysis incidence and blood transfusion requirements, various time horizons, discount rates, utilities and clinical effectiveness rates (Supplementary Table 2).
One-way sensitivity analysis (OWSA) demonstrated the level of uncertainty in the model results by varying one parameter at a time and assessing the subsequent impact on the incremental QALYs and incremental costs. We defined the low and high values for each parameter by lower and upper bounds of their 95% CI. In the absence of CI data, we altered the variable by ± 20%; a tornado diagram highlighted the parameters which had the greatest effect on the net monetary benefit (NMB; incremental benefit x threshold – incremental cost), with a positive incremental NMB indicating that the intervention is cost–effective compared with the alternative at the given willingness-to-pay (WTP) threshold. The NMB approach is an alternative to the incremental cost–effectiveness ratio (ICER) that avoids negative ICERs within the OWSA (in such a case that pegcetacoplan costs are lower and QALYs greater than ravulizumab). For this we applied a threshold of £10,000 per QALY, as specified by NICE to allow highly specialized technologies to be made more quickly and widely available within the NHS [73] and capped the upper and lower bounds for clinical plausibility [51,52].
Finally, we used probabilistic sensitivity analyses (PSA) to explore the impact of model parameter uncertainty on the results, performing 1000 simulations with values randomly and simultaneously drawn for each variable from its probability distribution. For event rates and utilities, beta distribution parameters allowed restricting draws to between 0 and 1. The fitted gamma distribution parameters prevented values less than zero for costs, resource use estimates, and hazard ratios. Treatment costs remained fixed. Each iteration gave a distribution of incremental results, and the distributions provided an assessment of the robustness of the cost–effectiveness results. We graphically illustrated uncertainty with an incremental cost–effectiveness plane scatter plot. We conducted all analyses using Excel version 2013 (Microsoft, WA, USA).
Results
Systematic literature review
The searches within the SLR identified no relevant CEA model structures applicable to the given study objectives nor any head-to-head randomized control trial data for comparing pegcetacoplan and ravulizumab in patients previously treated with eculizumab. The SLR also did not identify published data reporting EQ-5D responses in PNH patients. Therefore, a de novo Markov model was developed with health states defined on Hb levels and transfusion status. For comparative effectiveness we aimed to apply data from the previously described MAIC [53,54].
Utility mapping
Estimated utilities at the patient level, using the Longworth algorithm, ranged between -0.14 and 0.97 and mean utilities ranged between 0.72 and 0.86 across the visits (Supplementary Table 1). The McKenzie algorithm, based on a single ordinary least-squares regression, provided individual utilities ranging between -0.21 and 1.06 and mean utilities ranging from 0.55 to 0.89 across the visits. However, at most visits, the McKenzie algorithm resulted in non-interpretable utility values above 1 for some patients. Based on this anomaly, we concluded that the Longworth algorithm was more appropriate for mapping EQ-5D-3L utilities.
Cost–effectiveness analysis
In the base-case CEA, (Table 4), patients receiving ravulizumab accrued 12.942 QALYs at a total cost of £6,660,676. Patients treated with pegcetacoplan accrued 14.694 QALYs at a total cost of £6,409,166. Therefore, pegcetacoplan was economically dominant (i.e., lower total costs, greater number of QALYs) versus ravulizumab in the base case and confirmed through PSA (Table 4).
| Treatment | Total: | Incremental: pegcetacoplan vs comparators | ICER: pegcetacoplan vs ravulizumab | ||||
|---|---|---|---|---|---|---|---|
| Costs (£) | LYG | QALYs | Costs (£) | LYG | QALYs | £/QALY gained | |
| Deterministic analysis | |||||||
| Ravulizumab | 6,660,676 | 19.706 | 12.942 | -251,510 | 0 | 1.75 | Pegcetacoplan dominant |
| Pegcetacoplan | 6,409,166 | 19.706 | 14.694 | – | 0 | – | |
| Probabilistic sensitivity analysis | |||||||
| Ravulizumab | 6,665,853 | 19.706 | 12.999 | -262,127 | 0 | 1.76 | Pegcetacoplan dominant |
| Pegcetacoplan | 6,403,726 | 19.706 | 14.759 | – | 0 | – | |
The bold stresses the results for pegcetacoplan.
ICER: Incremental cost–effectiveness ratio; LYG: Life-years gained; QALY: Quality-adjusted life year.
In the scenario analysis, a variety of scenarios investigating variations in time horizons, discount rates, utilities, and clinical efficacy of pegcetacoplan were consistent with the base case (Supplementary Table 8).
The OWSA for pegcetacoplan versus ravulizumab (Figure 2) showed that the model was most sensitive to: the mean weight of patients, utility values for no transfusion and Hb ≥10.5 g/dl, the cost of blood transfusion and the mean units of blood transfusion. The NMB remained positive across all varied parameters, indicating that pegcetacoplan remained cost–effective compared with ravulizumab at a WTP threshold of £10,000 per QALY (Figure 3; Supplementary Table 10).

Figure 2. One-way sensitivity analysis tornado diagram for pegcetacoplan versus ravulizumab.
Hb: (Serum) Hemoglobin; NMB: Net monetary benefit.
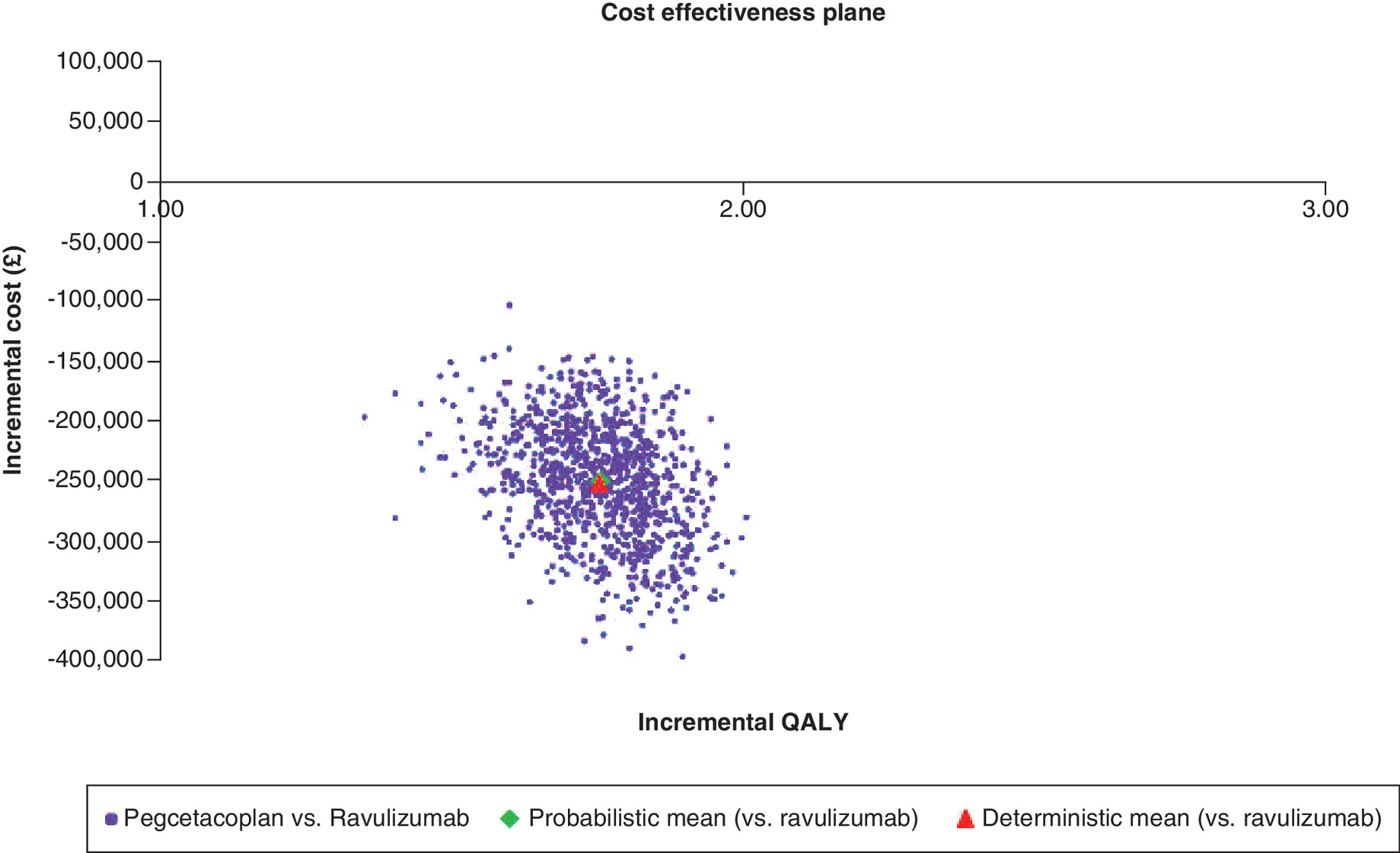
Figure 3. Incremental cost–effectiveness plane.
QALY: Quality-adjusted life year.
The incremental cost–effectiveness plane scatterplot (Figure 3) showed that 100% of results were in the southeast quadrant for pegcetacoplan versus ravulizumab, meaning that pegcetacoplan continued to dominate ravulizumab in each simulation (Figure 3) and was 100% cost–effective at all WTP thresholds.
Discussion
Among patients with PNH and insufficiently controlled anemia despite eculizumab treatment, this CUA showed not only that pegcetacoplan compared with ravulizumab resulted in lower healthcare costs, but also enhanced patient HRQoL. The PSA confirmed 100% of probabilistic iterations remained within all WTP thresholds, including the £10,000 per QALY threshold set by NICE for highly specialized technologies dedicated to drugs for very rare, usually serious conditions. The findings were consistent and robust even after we varied key parameters; pegcetacoplan remained the economically dominant treatment option across scenarios.
Despite the vital therapeutic benefits offered by C5i in preventing IVH and improving patient symptoms and HRQoL outcomes [32,40], some clinical limitations have endured, including the reduced blood transfusion–sparing benefits of C5i, in particular due to C3-mediated EVH [32,33,74]. PEGASUS showed that in patients who had adequately controlled IVH at enrollment (ie., LDH: mean 282.4 [±210.9] U/L), EVH had become the primary mechanism of hemolysis on C5i treatment, which continued to cause severe anemia. While all enrolled patients in PEGASUS had baseline Hb <10.5 g/dl, they also had a high rate of transfusion dependency (i.e., a mean of 6.5 transfusions in the preceding 12 months, with 55% of patients requiring over four transfusions in the preceding 12 months) [41].
Although transfusions may temporarily improve and elevate Hb levels in PNH patients, as the transfused cells express CD59 and CD55 on their cell surface and are resistant to complement-mediated lysis [26], patients may still experience long periods of suboptimal Hb level and resulting fatigue, besides the physiologic impact of iron overload [27]. These negative outcomes of transfusions further exacerbate patient burden because of work absenteeism resulting from transfusion-related hospital visits. As shown by a recent US real-world study, transfusion-dependent patients had significantly higher PNH-related and all-cause higher medical-related, hospital-related and outpatient-related work absenteeism compared with transfusion-free patients [9]. From the healthcare payer's perspective, the economic burden of transfusions is also substantial. A recent US study estimated that healthcare costs associated with hospitalizations and blood transfusions for a breakthrough hemolysis episode amounted to US$51,716 per patient for events due to complement-amplifying conditions, US$152,895 for events due to insufficient C5 inhibition, and US$186,107 for events due to pregnancy [15].
Where prescribing of above-label doses of C5i to address breakthrough hemolysis was common (up to 60%) in PEGASUS enrolled patients at study initiation [41], we also observed alternative findings in the literature. The US real-world study that stratified patients by transfusion-dependency found that transfusion-dependent C5i users were not only more likely to be dosed lower than as recommended on the label but had a shorter median time to treatment discontinuation [9]. The investigators suggested that discontinuation of treatment among transfusion-dependent C5i users may have been attributed to complications resulting in adverse events, the development of comorbid diseases (i.e., aplastic anemia, myelodysplastic syndrome), or the high cost of the therapy, which may have initially contributed to the lower number of infusions (five vs eight infusions) [9].
PEGASUS has provided evidence that, because pegcetacoplan targets the complement cascade earlier than C5i, it achieves improvements across hematological parameters, including Hb, bilirubin, reticulocytes and HRQoL, with almost no/minimal treatment-associated safety issues [41]. Long-term results through week 48 in PEGASUS have further shown clinically meaningful improvements in fatigue among patients continuously administered pegcetacoplan, and in those who switched from eculizumab at week 16. The effect was consistent across all FACIT-F score items, demonstrating that pegcetacoplan significantly reduces fatigue levels and maintains this effect over time by increasing Hb levels and limiting the need for transfusions.
Finally, a feature that is of practical value to patients, providers and payers, the twice-weekly 1080 mg SC dose of pegcetacoplan is self-administered with a syringe system infusion pump that delivers volumes up to 20 ml [42]. While a 30–60 minute time commitment (depending on one versus two infusion sites accessed) is still necessary compared with IV cannulation and infusion [64], the flexibility of SC self-administration of pegcetacoplan may allow patients to feel more in control of their disease management [64] Economically, this reduces the burden on healthcare systems beyond the initial training provided by nurses, compared with the IV infusion of C5i treatment [75]. However, with SC formulations typically needing a higher dosing frequency than IV formulations to enable administration of the relatively higher volume doses required [76], the mechanistic aspects of treatment have been shown across numerous studies to be generally over-ridden by preferences for the features of SC infusions versus IV infusions by patients and healthcare providers [77].
Limitations & strengths
An inherent limitation of this CUA was, because of the rarity of PNH, the small sample size of the PEGASUS clinical trial that informed the clinical and cost parameters. Therefore, some of the more extreme values may have introduced bias into the analysis. Another consideration is that there were no EQ-5D utilities data collected in PEGASUS; therefore, we mapped utilities using data collected on the EORTC-QLQ-30, although the approach was consistent with published NICE guidelines [61] and the HTA of ravulizumab compared with eculizumab [16]. While designed to measure the HRQoL of cancer patients, the EORTC-QLQ-C30 has demonstrated adequate reliability and validity PNH, with some additional items specific to PNH warranted for consideration in future validation studies [78]. Where generic utility instruments may fall short of capturing the specific and important aspects of the condition in question, or when trial-based EQ-5D data are unavailable, validated mapping algorithms can transform disease-specific HRQoL data into patient-level utility values [62]. However, this may have introduced some level of uncertainty into the model as opposed to applying directly elicited EQ-5D-5L values.
For comparative effectiveness inputs, where there was a lack of direct comparison of efficacy for pegcetacoplan versus ravulizumab, given that ravulizumab become available within the NHS only as of May 2021, we filled the evidence gap by assuming identical efficacy between ravulizumab and eculizumab per head-to-head non-inferiority trial data [53,55], which may have only conservatively biased the results. For example, during clinical input [57], the key limitation noted for the ravulizumab versus eculizumab trial design was preclusion of up-dosing [58]. Hence, our assumption of equal efficacy in the model may have underestimated the total costs associated with ravulizumab, as those patients treated with eculizumab who experienced IVH breakthrough in the trial may have required up dosing in actual clinical practice.
Finally, RCT data on which the clinical efficacy inputs were based are considered gold-standard evidence, yet may not fully reflect real-world practice. However, while the UK sites in PEGASUS allowed some level of local clinical practice to be reflected in the analysis, other inputs to the economic analysis were validated with expert input [57]. These inputs included assumptions of Hb thresholds and management of such outcomes as breakthrough hemolysis and iron overload that were representative to UK practice.
According to clinical opinion, a key benefit for pegcetacoplan-treated patients is that they do not require costly life-long chelation therapy (such as deferasirox and deferoxamine mesilate) to treat iron overload as required by those patients on C5i who require regular blood transfusions and accumulate iron in the liver and spleen. Where pegcetacoplan can increase and normalize Hb levels by preventing IVH without an increase in EVH [41], patients do not require continued blood transfusions and as such, do not experience further iron overload [41]. However, prior to the initiation of pegcetacoplan in transfusion dependent patients, built-up iron from prior receipt of regular transfusions would have necessitated venesection to address iron overload in pegcetacoplan patients, as transpired in PEGASUS [57].
In terms of the Hb <10.5 g/dl threshold for anemia within the model health states, although clinical experts confirmed that there is no consensus on an exact Hb level which corresponds to anemia, we applied a threshold that was not only consistent with the inclusion criteria of PEGASUS, but deemed the most appropriate threshold to reflect differences in HRQoL and cost affects in the PNH population. Using a higher threshold (eg, 12 g/dl) as per other anemia thresholds, such as that defined by the WHO [79] for anemia (<13 g/dl in men and <12 g/dl in women) would have led to a wider interval for the anemia health state and which may not have accurately measured the impact of anemia on patient HRQoL. However, while these thresholds are appropriate for the general population, they cannot be generalized to PNH patients who have adjusted to functioning with lower Hb. Therefore, a Hb threshold of 12 g/dl or higher would have misrepresented the reality of uncontrolled anemia in patients with PNH. PNH clinical experts have also confirmed that there is no consensus on an exact Hb level which corresponds to anemia, and that this will vary on a patient-by-patient basis [57].
In the absence of such an accepted threshold, a level of <10.5 g/dl was selected for the PEGASUS trial based on evidence throughout the PNH literature. For example, Risitano et al. proposed a system to classify hematological response in PNH patients on eculizumab [7]. In this trial setting, a complete or major response to eculizumab was associated with Hb levels ≥12 g/dl, a good response with levels ≥10 to <12 g/dl, a partial response with levels ≥8 and <10 g/dl and a minor response with levels <8 g/dl [7]. Earlier, Schrezenmeier et al. also reported that the 1425 patients enrolled in the international PNH registry had a median Hb of 10.6 g/dl, while, McKinley et al. similarly found, from a review of 141 patients referred to the UK National PNH Service, a median Hb level for these patients of 10.9 g/dl. Finally, the pivotal TRIUMPH study, which investigated eculizumab versus placebo, excluded patients with a mean Hb level prior to transfusion over the previous 12 months of above 10.5 g/dl [80].
Conclusion
The base-case results of this CUA, all scenario analyses and sensitivity analyses revealed QALY gains and lifetime cost savings for pegcetacoplan versus ravulizumab in patients with PNH and low Hb levels despite eculizumab therapy. Therefore, by providing enhanced control of anemia, greater improvements in HRQoL and reduced healthcare costs, pegcetacoplan may provide considerable clinical and economic value within the UK PNH treatment pathway.
Future perspective
While curative options for PNH are yet to be developed, treatment with the proximal complement inhibitor pegcetacoplan, as shown in PEGASUS, provides patients with increased disease control through improved Hb levels and overall reduced disease burden gained through independence from transfusions. Real-world evidence will reveal the ongoing humanistic and economic benefits of pegcetacoplan in long-term use and actual practice settings.
•
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare, potentially fatal blood disorder caused by somatic mutations to hematopoietic stem cells.
•
Characterized by hemolytic anemia, bone marrow failure and thrombosis and their clinical manifestations, PNH causes significant disease burden to patients due to chronic hemolysis and its consequences, including thrombotic events and the need for blood transfusions.
•
Curative treatment for PNH is limited to bone marrow transplantation. This is an option in countries where anti-complement therapy is not available, although the procedure is associated with considerable morbidity and mortality risk.
•
Therefore, therapeutic management of hemolytic disease and/or thromboembolic complications remains the key modality in current international and UK clinical practice, with standard of care (SOC) based on treatment with complement component 5 inhibitor (C5i) humanized monoclonal antibodies.
•
Ravulizumab is the newest C5i recommended by National Institute for Health and Care Excellence for the treatment of PNH.
•
Pegcetacoplan is a novel self-administered proximal C3 inhibitor that targets the complement cascade earlier than C5i, controlling intravascular hemolysis without the emergence of C3-mediated extravascular hemolysis.
•
PEGASUS, the pivotal trial of pegcetacoplan, showed that among patients with PNH and insufficiently controlled anemia despite eculizumab treatment, intravascular hemolysis was adequately controlled at enrollment (ie, lactase dehydrogenase [LDH]: mean 282.4 [±210.9] U/l); however, extravascular hemolysis had become the primary mechanism of hemolysis, which continued to cause severe anemia.
•
At baseline, patients in PEGASUS had a mean of 6.5 transfusions in the preceding 12 months, with 55% of patients requiring ≥4 transfusions.
•
Versus ravulizumab, pegcetacoplan provides significant overall improvement across PNH outcomes through increased serum hemoglobin levels, reduced levels of indirect bilirubin, and reticulocytes, and substantial and clinically meaningful improvements in patient fatigue, dyspnoea and health-related quality of life.
•
To inform payer decision-making, we conducted a lifetime cost–utility study based on a Markov model in the UK setting of pegcetacoplan compared with ravulizumab for the treatment with PNH and insufficiently controlled anemia (ie., Hb <10.5 d/l) despite ≥3 months treatment with eculizumab.
•
Results showed that in the base-case, patients receiving ravulizumab accrued 12.942 quality-adjusted life years at a total cost of £6,660,676. Patients treated with pegcetacoplan accrued 14.694 quality-adjusted life years at a total cost of £6,409,166.
•
Therefore, by providing enhanced control of anemia, greater improvements in health-related quality of life and reduced healthcare costs as compared with ravulizumab in patients with PNH, pegcetacoplan may provide considerable clinical and economic value within the UK PNH treatment pathway.
Author contributions
All authors were involved in developing the content of the publication. E McAughey, M Pochopien, P Wojciechowski, and C Knight developed the analytic model and conducted EA conducted analysis for the pegcetacoplan in the UK setting.
Acknowledgments
The investigators of this research wish to thank all the patients, caregivers and family members for their participation in the PEGASUS study.
Financial & competing interests disclosure
This study was funded and reviewed by Apellis Pharmaceuticals, Inc and Swedish Orphan Biovitrum AB, Stockholm, Sweden. Z Hakimi, K Wilson, C Wiseman, N de Castro, and J Nazir are employed by Sobi and hold company shares. S Sarda and N Patel are employed by Apellis and hold company shares. R Kelly discloses advisory boards and lecture fees from Alexion and advisory boards, lecture fees and consultancy for Sobi. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing support, under the guidance of the authors, was provided by Gauri Saal, MA Economics and Michael Kane, ApotheCom, London, UK, and was funded by Swedish Orphan Biovitrum AB, Stockholm, Sweden, in accordance with Good Publication Practice (GPP3) guidelines (Ann. Intern. Med. 2015;163:461–4).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials (5).docx)
- Download
- 30.83 KB
References
Papers of special note have been highlighted as: • of interest
1.
Hill A, Dezern AE, Kinoshita T, Brodsky RA. Paroxysmal nocturnal hemoglobinuria. Nat. Rev. Dis. Primers 3, 17028 (2017).
2.
Parker CJ. Update on the diagnosis and management of paroxysmal nocturnal hemoglobinuria. Hematology Am. Soc. Hematol. Educ. Program 2016(1), 208–216 (2016).
3.
Bektas M, Copley-Merriman C, Khan S, Sarda SP, Shammo JM. Paroxysmal nocturnal hemoglobinuria: patient journey and burden of disease. J. Manag. Care Spec. Pharm. 26(Suppl. 12-b), S8–S14 (2020).
• Revealed that most of the negative health effects and costs associated with paroxysmal nocturnal hemoglobinuria are due to blood transfusions, a key assumption to the present analysis.
4.
Lee SC, Abdel-Wahab O. The mutational landscape of paroxysmal nocturnal hemoglobinuria revealed: new insights into clonal dominance. J. Clin. Invest. 124(10), 4227–4230 (2014).
5.
Mon Pere N, Lenaerts T, Pacheco JM, Dingli D. Evolutionary dynamics of paroxysmal nocturnal hemoglobinuria. PLOS Comput. Biol. 14(6), e1006133 (2018).
6.
Takeda J, Miyata T, Kawagoe K et al. Deficiency of the GPI anchor caused by a somatic mutation of the PIG-A gene in paroxysmal nocturnal hemoglobinuria. Cell 73(4), 703–711 (1993).
7.
Risitano AM, Marotta S, Ricci P et al. Anti-complement treatment for paroxysmal nocturnal hemoglobinuria: Time for Proximal Complement Inhibition? A Position Paper From the SAAWP of the EBMT. Front Immunol. 10, 1157 (2019).
8.
Hillmen P, Lewis SM, Bessler M, Luzzatto L, Dacie JV. Natural history of paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 333(19), 1253–1258 (1995).
9.
Cheng WY, Sarda SP, Mody-Patel N et al. Real-World healthcare resource utilization (HRU) and costs of patients with paroxysmal nocturnal hemoglobinuria (PNH) receiving eculizumab in a US population. Adv. Ther. 38(8), 4461–4479 (2021).
10.
Socié G, Schrezenmeier H, Muus P et al. Changing prognosis in paroxysmal nocturnal hemoglobinuria disease subcategories: an analysis of the International PNH Registry. Intern Med. J. 46(9), 1044–1053 (2016).
11.
Yu F, Du Y, Han B. A comparative analysis of clinical characteristics of patients with paroxysmal nocturnal hemoglobinuria between Asia and Europe/America. Int. J. Hematol. 103(6), 649–654 (2016).
12.
Orphanet. Paroxysmal nocturnal hemoglobinuria [Internet]. Orphanet J. Rare Dis. (2021). www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=GB&Expert=447
13.
Fu R, Li L, Li L et al. Analysis of clinical characteristics of 92 patients with paroxysmal nocturnal hemoglobinuria: a single institution experience in China. J. Clin. Lab Anal. 34(1), e23008 (2020).
14.
Hill A, Kelly RJ, Hillmen P. Thrombosis in paroxysmal nocturnal hemoglobinuria. Blood 121(25), 4985–4996; quiz 5105 (2013).
15.
Tomazos I, Sierra JR, Johnston KM, Cheung A, Brodsky RA, Weitz IC. Cost burden of breakthrough hemolysis in patients with paroxysmal nocturnal hemoglobinuria receiving ravulizumab versus eculizumab. Hematology 25(1), 327–334 (2020).
16.
Single technology appraisal: ravulizumab for treating paroxysmal nocturnal hemoglobinuria [ID1457] (29 September). www.nice.org.uk/guidance/ta698/evidence/committee-papers-pdf-9132078637
• Allowed assumptions of present analysis to be made on precedent health technology assessment assessments.
17.
Berentsen S, Hill A, Hill QA, Tvedt THA, Michel M. Novel insights into the treatment of complement-mediated hemolytic anemias. Ther. Adv. Hematol. 10, 2040620719873321 (2019).
18.
Kokoris SI, Gavriilaki E, Miari A et al. Renal involvement in paroxysmal nocturnal hemoglobinuria: an update on clinical features, pathophysiology and treatment. Hematology 23(8), 558–566 (2018).
19.
Sahin F, Akay OM, Ayer M et al. PESG PNH diagnosis, follow-up and treatment guidelines. Am. J Blood Res. 6(2), 19–27 (2016).
20.
Phillippe HM. Overview of venous thromboembolism. Am. J. Manag. Care 23(Suppl. 20), S376–S382 (2017).
21.
Schrezenmeier H, Röth A, Araten DJ et al. Baseline clinical characteristics and disease burden in patients with paroxysmal nocturnal hemoglobinuria (PNH): updated analysis from the International PNH Registry. Ann. Hematol. 99(7), 1505–1514 (2020).
22.
Devalet B, Mullier F, Chatelain B, Dogné JM, Chatelain C. Pathophysiology, diagnosis, and treatment of paroxysmal nocturnal hemoglobinuria: a review. Eur. J. Hematol. 95(3), 190–198 (2015).
23.
Bektas M, Copley-Merriman C, Khan S, Sarda SP, Shammo JM. Paroxysmal nocturnal hemoglobinuria: current treatments and unmet needs. J. Manag. Care Spec. Pharm. 26(Suppl. 12-b), S14–S20 (2020).
24.
Levy AR, Dysart L, Patel Y et al. Comparison of lost productivity due to eculizumab and ravulizumab treatments for paroxysmal nocturnal hemoglobinuria in France, Germany, Italy, Russia, Spain, the United Kingdom, and the United States. Blood 134, 4803 (2019).
25.
Aamds. PNH—paroxysmal nocturnal hemoglobinuria. (2020).
26.
Young NS, Meyers G, Schrezenmeier H, Hillmen P, Hill A. The management of paroxysmal nocturnal hemoglobinuria: recent advances in diagnosis and treatment and new hope for patients. Semin. Hematol. 46(Suppl. 1), S1–S16 (2009).
27.
Platzbecker U, Hofbauer LC, Ehninger G, Holig K. The clinical, quality of life, and economic consequences of chronic anemia and transfusion support in patients with myelodysplastic syndromes. Leuk. Res. 36(5), 525–536 (2012).
28.
Santarone S, Bacigalupo A, Risitano AM et al. Hematopoietic stem cell transplantation for paroxysmal nocturnal hemoglobinuria: long-term results of a retrospective study on behalf of the Gruppo Italiano Trapianto Midollo Osseo (GITMO). ematologica 95(6), 983–988 (2010).
29.
Ravulizumab for treating paroxysmal nocturnal hemoglobinuria. Technology appraisal guidance [TA698] (15 November). www.nice.org.uk/guidance/ta698/chapter/3-Committee-discussion#treatment-pathway
30.
McKeage K. Eculizumab: a review of its use in paroxysmal nocturnal hemoglobinuria. Drugs 71(17), 2327–2345 (2011).
31.
Alexion. Solirus (eculizumab) [package insert]. US Food and Drug Administration website (2021). www.accessdata.fda.gov/drugsatfda_docs/label/2017/125166s422lbl.pdf
32.
Kelly RJ, Hill A, Arnold LM et al. Long-term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria: sustained efficacy and improved survival. Blood 117(25), 6786–6792 (2011).
33.
Stern RM, Connell NT. Ravulizumab: a novel C5 inhibitor for the treatment of paroxysmal nocturnal hemoglobinuria. Ther. Adv. Hematol. 10, 2040620719874728 (2019).
34.
Ultomiris 300 mg/30 ml concentrate for solution for infusion. Summary of Product Characteristics (SmPC) (15 November). www.medicines.org.uk/emc/product/10457/smpc#gref
35.
Recommendation: Ravulizumab for treating paroxysmal nocturnal hemoglobinuria Technology appraisal guidance [TA698] (15 November). www.nice.org.uk/guidance/ta698/chapter/1-Recommendations
36.
Füreder W, Valent P. Switching from high-dose eculizumab to ravulizumab in paroxysmal nocturnal hemoglobinuria: a case report. HemaSphere 4(4), e455 (2020).
37.
Peipert JD, Kulasekararaj AG, Gaya A et al. Patient preferences and quality of life implications of ravulizumab (every 8 weeks) and eculizumab (every 2 weeks) for the treatment of paroxysmal nocturnal hemoglobinuria. PLOS One 15(9), e0237497 (2020).
38.
Gurnari C, Nautiyal I, Pagliuca S. Current opinions on the clinical utility of ravulizumab for the treatment of paroxysmal nocturnal hemoglobinuria. Ther. Clin. Risk Manag. 17, 1343–1351 (2021).
• Informed the present analysis regarding ravulizumab as the most relevant comparator for a cost–effectiveness analysis of pegcetacoplan.
39.
Risitano AM, Notaro R, Marando L et al. Complement fraction 3 binding on erythrocytes as additional mechanism of disease in paroxysmal nocturnal hemoglobinuria patients treated by eculizumab. Blood 113(17), 4094–4100 (2009).
40.
Schwartz CE, Stark RB, Borowiec K, Nolte S, Myren K-J. Norm-based comparison of the quality-of-life impact of ravulizumab and eculizumab in paroxysmal nocturnal hemoglobinuria. Orphanet J. Rare Dis. 16(1), 389 (2021).
41.
Hillmen P, Szer J, Weitz I et al. Pegcetacoplan versus eculizumab in paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 384(11), 1028–1037 (2021).
• Data from the pivotal trial of pegcetacoplan informed the clinical parameters of the Markov model.
42.
Empavali prescribing information (15 November). www.accessdata.fda.gov/drugsatfda_docs/label/2021/215014s000lbl.pdf
43.
Aspaveli 1 080 mg solution for infusion; Summary of Product Characteristics (SmPC) (2022). www.ema.europa.eu/en/documents/product-information/aspaveli-epar-product-information_en.pdf
44.
ASPAVELI 1 080 mg solution for infusion (29 March). https://mhraproducts4853.blob.core.windows.net/docs/f5c79734c69d0ee30732d383edff42be050e9c90
45.
Röth A, Hoechsmann B, Griffin M et al. Effect of pegcetacoplan on quality of life in patients with paroxysmal nocturnal hemoglobinuria from the pegasus Phase 3 trial comparing pegcetacoplan to eculizumab. Blood 136(Suppl. 1), 10–12 (2020).
46.
Godman B, Bucsics A, Vella Bonanno P et al. Barriers for access to new medicines: searching for the balance between rising costs and limited budgets. Front. in Public Health 6(328), (2018).
47.
Blonda A, Denier Y, Huys I, Simoens S. How to value orphan drugs? A review of European value assessment frameworks. Front. Pharmacol. 12 (2021).
48.
Methodological choices for the economic evaluation at HAS (10 September). www.has-sante.fr/jcms/r_1499251/fr/choix-methodologiques-pour-l-evaluation-economique-a-la-has
49.
The guidelines manual: process and methods [PMG6] (29 September). www.nice.org.uk/process/pmg6/chapter/assessing-cost-effectiveness
50.
Berdud M, Drummond M, Towse A. Establishing a reasonable price for an orphan drug. Cost Eff. Resour. Alloc. 18(1), 31 (2020).
51.
Sobi. Expert survey for collecting data Inputs for the cost–effectiveness model for pegcetacoplan in the treatment of paroxysmal nocturnal hemoglobinuria (PNH) in the US and UK. Data on file.
52.
Sobi. Pegcetacoplan in paroxysmal nocturnal hemoglobinuria (PNH): United Kingdom (UK) health technology assessment virtual advisory board. Data on file. Advisory Board presented at; 2021 Apr 15; Virtual.
53.
Kulasekararaj AG, Hill A, Rottinghaus ST et al. Ravulizumab (ALXN1210) vs eculizumab in C5-inhibitor-experienced adult patients with PNH: the 302 study. Blood 133(6), 540–549 (2019).
• Data were used to match average aggregate baseline characteristics reported in the ALXN1210-PNH-302 (Study 302) trial for patients receiving ravulizumab with the PEGASUS trial population.
54.
Bhak RH, Mody-Patel N, Baver SB et al. Comparative effectiveness of pegcetacoplan versus ravulizumab in patients with paroxysmal nocturnal hemoglobinuria previously treated with eculizumab: a matching-adjusted indirect comparison. Curr. Med. Res. Opin. 37(11), 1913–1923 (2021).
• Data anchored the comparisons of clinical outcomes for pegcetacoplan and ravulizumab.
55.
Wook JL, de Fontbrune FS, Pessoa V et al. Ravulizumab (ALXN1210) vs eculizumab in adult patients with PNH naive to complement inhibitors: the 301 study. Blood 133(6), 530–539 (2019).
56.
Advice: ravulizumab (Ultomiris®) for PNH (15 November). www.scottishmedicines.org.uk/media/5756/ravulizumab-ultomiris-final-jan-2021-for-website.pdf
57.
Sobi. Pegcetacoplan in paroxysmal nocturnal hemoglobinuria: United Kingdom health technology assessment virtual advisory board. Data on file. Advisory Board; 2021 Apr 15; Virtual.
58.
Lee JW, Sicre De Fontbrune F, Wong Lee Lee L et al. Ravulizumab (ALXN1210) vs eculizumab in adult patients with PNH naive to complement inhibitors: the 301 study. Blood 133(6), 530–539 (2019).
59.
Mapping of EQ-5D (24 September). http://nicedsu.org.uk/methods-development/mapping-of-eq-5d/
60.
Longworth L, Yang Y, Young T et al. Use of generic and condition-specific measures of health-related quality of life in NICE decision-making: a systematic review, statistical modelling and survey. Health Technol. Assess 18(9), 1–224 (2014).
• This algorithm was used to validate the mapping approach for the EQ-5D data developed for the present analysis.
61.
Position statement on use of the EQ-5D-5L value set for England (29 September). www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/technology-appraisal-guidance/eq-5d-5l
62.
Longworth L, Rowen D. Mapping to obtain EQ-5D utility values for use in NICE health technology assessments. Value Health 16(1), 202–210 (2013).
63.
Mckenzie L, Van Der Pol M. Mapping the EORTC QLQ C-30 onto the EQ-5D instrument: the potential to estimate QALYs without generic preference data. Value Health 12(1), 167–171 (2009).
64.
Stoner KL, Harder H, Fallowfield LJ, Jenkins VA. Intravenous versus subcutaneous drug administration. Which do patients prefer? A systematic review. Patient (2014).
• This review indicated that patients have reported a preference for subcutaneous over IV delivery in other disease settings, a key treatment benefit of pegcetacoplan.
65.
Advice: eculizumab (Soliris) for PNH (15 November). www.scottishmedicines.org.uk/medicines-advice/eculizumab-soliris-for-pnh-fullsubmission-113016/
66.
Cherry MG, Greenhalgh J, Osipenko L et al. The clinical effectiveness and cost-effectiveness of primary stroke prevention in children with sickle cell disease: a systematic review and economic evaluation. Health Technol Assess 16(43), 1–129 (2012).
67.
Ultomiris (ravulizumab) EPAR (15 November). www.ema.europa.eu/en/medicines/human/EPAR/ultomiris
68.
Unit Costs of Health and Social Care (15 November). www.pssru.ac.uk/project-pages/unit-costs/unit-costs-2019
69.
NHS Reference Costs (15 November). www.england.nhs.uk/publication/2019-20-national-cost-collection-data-publication/
70.
Routine preoperative tests for elective surgery (15 November). www.nice.org.uk/guidance/ng45
71.
Eculizumab (15 November). https://bnf.nice.org.uk/medicinal-forms/eculizumab.html
72.
NICE. 5 The reference case | Guide to the methods of technology appraisal 2013 | Guidance | NICE [Internet]. NICE. NICE; 2013 [cited 2021 May 12] www.nice.org.uk/process/pmg9/resources/guide-to-the-methods-of-technology-appraisal-2013-pdf-2007975843781
73.
Charlton V. NICE and Fair? Health Technology Assessment Policy Under the UK's National Institute for Health and Care Excellence, 1999–2018. Health Care Anal. 28(3), 193–227 (2020).
74.
Debureaux P CF, Silva B, Barone F, De Fontbrune F et al. Hematological response to eculizumab in paroxysmal nocturnal hemoglobinuria: application of a novel classification to identify unmet clinical needs and future clinical goals. Blood 384, 3517 (2021).
75.
Levy AR, Tomazos I, Patel Y, Donato BMK, Briggs A. PSY15 Comparison of lost productivity due to eculizumab and ravulizumab treatments for paroxysmal nocturnal hemoglobinuria in the United States. Value in Health 22, S377 (2019).
76.
Bittner B, Richter W, Schmidt J. Subcutaneous administration of biotherapeutics: an overview of current challenges and opportunities. BioDrugs 32(5), 425–440 (2018).
77.
Abolhassani H, Sadaghiani MS, Aghamohammadi A, Ochs HD, Rezaei N. Home-based subcutaneous immunoglobulin versus hospital-based intravenous immunoglobulin in treatment of primary antibody deficiencies: systematic review and meta analysis. J. Clin. Immunol. 32(6), 1180–1192 (2012).
78.
Weitz I, Meyers G, Lamy T et al. Cross-sectional validation study of patient-reported outcomes in patients with paroxysmal nocturnal hemoglobinuria. Intern Med. J. 43(3), 298–307 (2013).
79.
hemoglobin concentrations for the diagnosis of anemia and assessment of severity (18 January). www.who.int/vmnis/indicators/hemoglobin.pdf
80.
Hillmen P, Young NS, Schubert J et al. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 355(12), 1233–1243 (2006).
Information & Authors
Information
Published In
Pages: 969 - 985
PubMed: 35796199
Copyright
© 2022 Sobi Ab. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 14 April 2022
Accepted: 9 June 2022
Published online: 7 July 2022
Keywords:
Topics
Authors
Funding Information
Swedish Orphan Biovitrum AB
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The cost–effectiveness, of pegcetacoplan compared with ravulizumab for the treatment of paroxysmal nocturnal hemoglobinuria, in a UK setting. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0076
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Shaghayegh Moradi, Yasaman Khajeamiri, Sara Zandi, Mohammadreza Keramati, Ghader Mohammadnezhad, Disease-modifying treatments in paroxysmal nocturnal hemoglobinuria: a systematic review of economic evaluations, Cost Effectiveness and Resource Allocation, 10.1186/s12962-025-00702-z, 24, 1, (2025).
- Coste-efectividad de danicopán, asociado a ravulizumab o eculizumab, para el tratamiento de pacientes adultos con hemoglobinuria paroxística nocturna que presentan anemia hemolítica residual en España, Economía de la Salud, 10.61679/2004040053, 20, (2025).
- Zhixue Li, Defu Zeng, Rong Fu, Xiaohui Zhang, Progress in clinical research on allogeneic hematopoietic stem cell transplantation for the treatment of paroxysmal nocturnal hemoglobinuria, Medicine Plus, 10.1016/j.medp.2025.100070, 2, 1, (100070), (2025).
- Jeremiah Donoghue, Matthew Youngs, Alex Reeve, Krishna Vydyula, Natalia Kunst, Roochi Trikha, Daniel Gallacher, Examining Consistency Across NICE Single Technology Appraisals: A Review of Appraisals for Paroxysmal Nocturnal Haemoglobinuria, PharmacoEconomics, 10.1007/s40273-025-01472-5, 43, 5, (499-508), (2025).
- Satoko Ito, Karthik Chetlapalli, Daniel Wang, Kunal C. Potnis, Rhys Richmond, Harlan M. Krumholz, Alfred I. Lee, Adam Cuker, George Goshua, Cost-effectiveness of iptacopan for paroxysmal nocturnal hemoglobinuria, Blood, 10.1182/blood.2024025176, 145, 1, (127-140), (2025).
- Sergio Di Matteo, Roberto Freilone, Giacomo Bruno, Rosario Notaro, Sabrin Moumene, Nicoletta Martone, Cristina Teruzzi, Antonio Ciccarone, Giorgio Colombo, Cost-Utility Analysis Comparing Pegcetacoplan to Anti-C5 Monoclonal Antibodies in the Treatment of Paroxysmal Nocturnal Hemoglobinuria, ClinicoEconomics and Outcomes Research, 10.2147/CEOR.S442906, Volume 16, (225-232), (2024).
- Mendy ter Avest, Saskia M.C Langemeijer, Nicole M.A. Blijlevens, Nicole C.A.J. van de Kar, Rob ter Heine, Development of a target concentration intervention to individualize paroxysmal nocturnal hemoglobinuria treatment with pegcetacoplan, Annals of Hematology, 10.1007/s00277-024-05699-8, 103, 7, (2267-2272), (2024).
- Anem Waheed, Jamile Shammo, David Dingli, Paroxysmal nocturnal hemoglobinuria: Review of the patient experience and treatment landscape, Blood Reviews, 10.1016/j.blre.2023.101158, 64, (101158), (2024).
- Jesse Fishman, Koo Wilson, Aleksandra Drzewiecka, Michał Pochopień, David Dingli, The cost–effectiveness of pegcetacoplan in complement treatment-naïve adults with paroxysmal nocturnal hemoglobinuria in the USA, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0055, 12, 10, (2023).
- Raymond Wong, Jesse Fishman, Koo Wilson, Michael Yeh, Mohammed Al-Adhami, Abigail Zion, Christopher W. Yee, Lynn Huynh, Mei Sheng Duh, Comparative Effectiveness of Pegcetacoplan Versus Ravulizumab and Eculizumab in Complement Inhibitor-Naïve Patients with Paroxysmal Nocturnal Hemoglobinuria: A Matching-Adjusted Indirect Comparison, Advances in Therapy, 10.1007/s12325-023-02438-9, 40, 4, (1571-1589), (2023).