Comparison of Enterprise stent 2 with 1 in assisting coiling of ruptured aneurysms: a real-world study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To investigate the effectiveness and safety of the Enterprise 2 (E2) stent versus the Enterprise 1 (E1) stent in treating ruptured intracranial aneurysms (RIAs) in China. Materials & methods: The authors conducted an electronic medical record analysis for patients with RIAs who underwent E1/E2 deployment. The main outcomes were immediate complete occlusion (ICO), patient functional outcomes, complications and aneurysm recurrence. Results: Stent deployment was successful in all patients (E2: 90; E1: 270). ICO and patients with good functional outcomes at discharge were similar between E2 and E1 (80.0% vs 75.1% and 78.7% vs 81.1%, respectively). The E2 group had a significantly lower complication rate compared with the E1 group (7.8% vs 16.4%; odds ratio: 0.36; 95% CI: 0.15–0.91; p = 0.031). By 6 months post-discharge, the two groups had comparable patient functional outcomes and aneurysm recurrence (E2 vs E1: 80.2% vs 81.9% and 13.3% vs 14.9%). Conclusion: Compared with the E1 stent, the E2 stent had similar effectiveness but a lower complication risk in treating RIAs.
The introduction of stent-assisted coiling (SAC) for the treatment of intracranial aneurysms (IAs) has brought major advances in the field of cerebrovascular neurosurgery. However, the application of SAC in the setting of subarachnoid hemorrhage has had greater challenges due to stent-associated thromboembolic risks and the need for anti-platelet therapy to counteract thrombogenicity of the stent. Via known mechanism of action, administration of anti-platelet therapy may subject patients to the risk of extra- and intra-cranial bleeding. The 2012 American Heart Association (AHA)/American Stroke Association (ASA) guidelines for the management of aneurysmal subarachnoid hemorrhage recommend SAC only as a last resort for the management of acutely ruptured wide-necked aneurysms [1]. Lack of perceived equipoise in this setting may render the conducting of controlled clinical trials difficult or not feasible. Nevertheless, results from systematic literature reviews of case series or cohorts in treating acutely ruptured IAs found that SAC can be performed with high degrees of technical success but may be associated with higher overall complication rates compared with coiling alone [2,3].
Since the first SAC device was approved for the treatment of IAs in 2002 [4], a number of stents of different designs have been introduced into clinical practice. Over time, the successive generations of devices have continuously evolved to improve the devices and their delivery systems and have made the most distal, complex, wide-necked, irregular lesions amenable to endovascular treatment with significantly lower rates of aneurysm recurrence [5]. The Enterprise vascular reconstruction device and delivery system is a self-expanding nickel–titanium alloy stent system; it is the first closed-cell designed stent and was approved by the Chinese medical device regulatory agency in 2008 and has been broadly used in clinical practice for treating IAs in China. The first-generation Enterprise (E1) is easily navigated and precisely positioned, even in complex IAs [6]. However, one limitation associated with the E1 is the incomplete stent apposition in blood vessels with large diameters and curvatures [7]. In addressing this limitation, the second-generation Enterprise (E2) stent was developed with improved geometry design. The E2 was subsequently introduced in clinical practice in 2018 in China, replacing the earlier generation. Due to its recent availability, to date only two small clinical studies with a total of 34 patients have been reported in the literature and none with ruptured IAs [8,9].
The aim of this study was to compare and analyze the effectiveness and safety of the E2 stent versus the E1 stent in treating ruptured IAs in a real-world setting in China.
Materials & methods
Study populations
The present study is an extension of previous research that evaluated the clinical effectiveness and safety of the first-generation Enterprise (E1) stent in the setting of acute subarachnoid hemorrhage attributable to ruptured intracranial aneurysm (IA). The same study protocol and data collection forms were used in the extension and the data collected from both stages were combined in the analysis. In brief, the study was a single-center, retrospective, observational study based at a tertiary hospital in China. The hospital's electronic medical information system was screened for patients presenting with subarachnoid hemorrhage and treated with E1 (from January 2013 to 2018) or the second-generation Enterprise (E2) stent (from 2018 to November 2020). Patients were included if they had been diagnosed with ruptured IAs and treated with E1 or E2 SAC and had had at least one post-procedural follow-up visit. The Hunt and Hess grading system and Fisher scales were used to rate the severity of subarachnoid hemorrhage [10,11]. Patients were excluded if they met any of the following exclusion criteria: comatose status (Hunt and Hess grade V) attributable to subarachnoid hemorrhage; subarachnoid hemorrhage caused by conditions other than IA such as brain arteriovenous malformation or arteriovenous fistula; and treatment with vascular reconstruction devices other than the Enterprise vascular reconstruction device and delivery system. The numbers of cases and causes of death were described if patients died during hospitalization.
The local institutional ethical review committee approved this study and waived informed consent, as the data were collected from routine patient care and analyzed retrospectively in an anonymous fashion.
Treatment strategy
Interventional embolization was the first choice for the treatment of ruptured aneurysms, including patients with hematoma without obvious space-occupying effect, especially simple coiling at the authors' institute. SAC was used primarily for wide-necked and dissecting aneurysms. Some patients underwent craniotomy due to rebleeding or vasospasm. For patients with multiple aneurysms, the responsible aneurysm was identified by experienced neurointerventional physicians and neurosurgeons according to the clinical and angiographic conditions. The responsible aneurysm was treated first. The rest of the aneurysms were also treated simultaneously if simple coiling could be achieved. Otherwise, they were treated at the second stage. If the responsible aneurysm was difficult to identify, all aneurysms with a high risk of rupture were treated simultaneously.
The anti-platelet regimens entailed several anti-platelet medications administered in the following sequence. A loading dose of aspirin and clopidogrel (300 mg each) are given either orally or by anus for patients with ruptured aneurysms planning stent placement before the procedure. At the beginning of the procedure, 60–80 units/kg of heparin were administered, followed by a half dose every 2 h. Dual anti-platelet drugs (aspirin 100 mg daily and clopidogrel 75 mg daily) were administered for 6 weeks followed by only aspirin, which patients were instructed to use indefinitely. If there was in-stent thrombosis during embolization, tirofiban was given through microcatheter or guiding catheter and pumped intravenously at the same time.
Outcomes measurement
The following effectiveness end points were included in the outcomes evaluation: duration of the procedure, stent placement success rate, immediate embolism rate, patient functional outcomes at discharge and at 3 months and 6 months post-discharge and cumulative aneurysm recurrence at 6 months post-discharge. The degree of aneurysm treatment success was graded based on the digital subtraction angiography (DSA) images according to the revised Raymond–Roy occlusion classification (RROC) criteria [12] immediately after the procedure – class I: complete obliteration; class II: residual neck; class IIIa: residual aneurysm with contrast within coil interstices; and class IIIb: residual aneurysm with contrast along aneurysm wall. The recurrence of aneurysms was defined as at least one level worsening with respect to aneurysm occlusion as determined by the RROC during follow-up compared with that immediately post-surgery, regardless of the need for retreatment [13]. The authors used the Modified Rankin Scale (mRS) score to measure patient functional outcomes. The mRS is a six-point disability scale with possible scores ranging from 0 (no symptoms at all) through 5 (severe disability) [14]. Patients with mRS scores ≤2 were in general considered to have good functional outcomes and those with mRS scores ≥3 were considered to have functional impairment. The safety end point was examined by documented stent-related complications, which were defined as events that occurred during the procedure or hospitalization period such as reruptured aneurysms, hemorrhages associated with external drainage of the brain, in-scaffolding thrombosis and stent disposition. Thromboembolic complications were diagnosed intraoperatively on DSA or CT/MRI scans indicating new infarcts, performed in cases of unexpected neurological compromise.
Statistical analysis
The primary focus of the analysis was to compare the outcomes of interest between patients treated with E2 and those treated with E1. In univariate analysis, for continuous variables, the data were reported as means ± standard deviation (SD), and the two-sample t-test or Wilcoxon rank test was used for the group comparisons as appropriate. For categorical variables, the percentages were calculated with the denominator tabulated from non-missing data unless noted otherwise. The Chi-square or Fisher exact test was used to test the group differences where appropriate. Since the frequency and duration of patient follow-ups were at the discretion of the treating physicians, the cumulative recurrence rate of aneurysms was estimated using the life-table method, which accounts for the duration of follow-ups.
To adjust for the baseline variables that could confound the findings (including age, gender, diabetes, high blood pressure, smoking, Hunt and Hess grade, Glasgow Coma Scale [GCS] score, Fisher scale score, presence of hematoma, aneurysm size, aneurysm width, aneurysm neck width, aneurysm height and stenting technique) in univariate analysis, multivariate logistic regression analysis was fitted by the backward stepwise approach, with all potential confounding factors being included at the initial step. In all analyses, two-tailed p-values were reported for the null hypothesis of no difference between the E1 and E2 stents, and the threshold for statistical significance was p < 0.05. All statistical analyses were conducted using the R version 3.5.3.
Results
Baseline patient characteristics
A total of 360 patients met the study criteria and were included in this analysis; of those, 270 received first-generation Enterprise (E1) and 90 patients were treated with second-generation Enterprise (E2).
Table 1 highlights the patients' demographic characteristics, current smoking and drinking status, notable medical history and clinical presentations at hospital admission. In both E1 and E2 groups, the mean age was near 60 years old, with females accounting for more than two-thirds of the study population; fewer than 10% were current alcohol drinkers or cigarette smokers. When admitted to the hospital, three-quarters of the patients in both groups presented with high blood pressure, and the patients in both groups had nearly identical GCS scores (13.5 ± 2.6 vs 13.5 ± 2.8). However, the patients in the E2 group had significantly higher grades on both the Hunt and Hess scale (p < 0.001) and the Fisher scale (p = 0.002). The presence of intracranial hematomas, acute hydrocephalus and multiple aneurysms was similar between the two groups.
| Characteristics | Enterprise 1 (n = 270) | Enterprise 2 (n = 90) | p-value |
|---|---|---|---|
| Age (years, mean ± SD) | 58.4 ± 11.3 | 60.0 ± 11.5 | 0.259 |
| Male (n, %) | 79 (29.3) | 25 (27.8) | 0.893 |
| Current alcohol drinker (occasional/regular) (n, %) | 16 (20.0) | 6 (21.4) | 1.000 |
| Current tobacco user (n, %) | 18 (6.6) | 3 (3.3) | 0.363 |
| Presence of high blood pressure (>140/90 mmHg) (n, %) | 201 (74.4) | 67 (74.4) | 1.000 |
| Notable medical history (n, %) Diabetes Prior subarachnoid hemorrhages | 12 (4.4) 5 (1.9) | 6 (6.7) 4 (4.4) | 0.599 0.33 |
| Glasgow Coma Scale score (mean + SD) | 13.5 ± 2.6 | 13.5 ± 2.8 | 0.928 |
| Hunt and Hess scale† (n, %) I II III IV | 51 (18.9) 123 (45.6) 76 (28.1) 20 (7.4) | 1 (1.1) 64 (71.1) 16 (17.8) 9 (10.0) | <0.001 |
| Fisher scale‡ (n, %) I II III IV Unknown | 20 (7.4) 94 (34.8) 110 (40.7) 46 (17.0) 1 | 2 (2.2) 16 (17.8) 49 (54.4) 23 (25.6) 0 | 0.002 |
| Combined with hematoma (n, %) None Yes Unknown | 234 (87.0) 35 (13.0) 1 | 85 (94.4) 5 (5.6) 0 | 0.08 |
| Presence of acute hydrocephalus (n, %) | 28 (10.5) | 10 (11.2) | 1 |
| Aneurysm location (n = 322; 110, %) Posterior communicating artery Anterior communicating artery Middle cerebral artery Posterior cerebral artery Anterior cerebral artery Internal carotid artery Others | 107 (33.2) 77 (23.9) 42 (13.0) 27 (8.4) 10 (3.1) 7 (2.2) 52 (16.1) | 37 (33.6) 19 (17.3) 18 (16.4) 7 (6.4) 2 (1.8) 3 (2.7) 24 (21.8) | 0.575 |
| Aneurysm width (mm, mean ± SD) | 4.6 ± 2.8 | 4.8 ± 2.8 | 0.651 |
| Aneurysm height (mm, mean ± SD) | 4.7 ± 2.9 | 4.9 ± 2.7 | 0.682 |
| Aneurysm size (n, %) Small (<5 mm) Medium (5–15 mm) Large (16–25 mm) Unknown | 136 (50.4) 130 (48.1) 4 (1.5) 0 | 44 (50.0) 44 (50.0) 0 (0.0) 2 | 0.509 |
| Presence of multiple aneurysms (n, %) | 48 (17.8) | 20 (22.2) | 0.437 |
†
Hunt and Hess scale: grade I – asymptomatic or minimal headache and slight neck stiffness; grade II – moderate to severe headache, neck stiffness, no neurologic deficit except cranial nerve palsy; grade III – drowsy, minimal neurologic deficit; grade IV – stuporous, moderate to severe hemiparesis, possibly early decerebrate rigidity and vegetative disturbances; grade V – deep coma, decerebrate rigidity, moribund.
‡
Fisher scale: grade I – no subarachnoid or intraventricular hemorrhage detected; grade II – diffuse thin (<1 mm) subarachnoid hemorrage, no clots; grade III – localized clots and/or layers of blood >1 mm in thickness, no intraventricular hemorrhage; grade IV – diffuse or no subarachnoid, intracranial or intraventricular hemorrhage present.
SD: Standard deviation.
The distribution of aneurysm locations was similar, with slightly more than half of all aneurysms located at the posterior or anterior communicating artery in both groups (E1:57.1%; E2:50.9%), followed by the middle cerebral artery (E1:13.0%; E2:16.4%) and posterior cerebral artery (E1:8.4%; E2:6.4%). The measurements of aneurysms were comparable across the two groups as well, with mean aneurysm widths of 4.6 ± 2.8 mm (E1) and 4.8 ± 2.8 mm (E2) and height at 4.7 ± 2.9 mm (E1) and 4.9 ± 2.7 mm (E2), respectively. Tabulated by aneurysm size, about half of the aneurysms were considered small (<5 mm) and the remaining were medium (5–15 mm) in both groups.
Univariate analysis of perioperative outcomes
The univariate perioperative outcomes are displayed in Table 2. The operation time was significantly shorter for the E2 group than for the E1 group (166.3 vs 190.3 min; p = 0.008), and the length of the hospital stay was shorter for the E2 group, but the difference did not reach statistical significance. For both E1 and E2, all stents were successfully deployed during the procedure, with a 100% technical success rate of stent placement. Post-procedural arteriography confirmed that slightly over 75% of the patients achieved complete obliteration (class I) in both groups.
| Characteristics | Enterprise 1 (n = 270) | Enterprise 2 (n = 90) | p-value |
|---|---|---|---|
| Operation time (min, mean ± SD) | 190.3 ± 79.6 | 166.3 ± 51.5 | 0.008 |
| Length of hospital stay (days, mean ± SD) | 19.2 ± 12.6 | 16.7 ± 9.7 | 0.078 |
| Stent placement success (n, %) | 270 (100.0) | 90 (100.0) | NA |
| Updated Raymond–Roy occlusion classification I II IIIa IIIb Missing | 202 (75.1) 38 (14.1) 25 (9.3) 4 (1.5) 1 | 72 (80.0) 11 (12.2) 7 (7.8) 0 (0.0) 0 | 0.593 |
| Procedure-related complications All Hemorrhagic In-stent thrombosis Others | 44 (16.4) 2 (0.7) 32 (11.9) 10 (3.7) | 7 (7.8) 0 (0.0) 7 (7.8) 0 (0.0) | 0.044 |
| Modified Rankin Score 0–2 3–5 Missing | 219 (81.1) 51 (18.9) 0 | 70 (78.7) 19 (21.3) 1 | 0.612 |
NA: Not applicable; SD: Standard deviation.
Overall, 16.4% and 7.8% of the patients in the E1 and E2 groups, respectively, encountered procedure-related complications (p = 0.044). In both groups, in-stent thrombosis was the most common procedure-related complication (E1:11.9%; E2:7.8%), and all but one patient in each group was successfully managed with infusion of thrombolytics. Three patients in the E1 group died during hospitalization due to gastrointestinal bleeding, rerupture of the aneurysm and respiratory and circulatory failure. One patient in the E2 group died due to cerebral herniation secondary to intracranial bleeding.
At discharge, 81.1% and 78.7% of the patients in the E1 and E2 groups, respectively, exhibited good functional outcomes (mRS ≤2; p = 0.612).
Univariate analysis of short & intermediate outcomes
By 3 months post-discharge, six patients from the E1 group and two patients from the E2 group experienced aneurysm recurrence based on RROC. By 6 months post-discharge,an additional ten patients from the E1 group and two patients from the E2 group had aneurysm recurrence, resulting in estimated 6-month cumulative recurrence rates of 14.9% and 13.3%, respectively, after accounting for loss to follow-up using the life-table method.
By 6 months post-discharge, about four of five patients in both groups experienced good functional outcomes (E1:81.9%; E2:80.2%; p = 0.875).
Multivariate analysis of outcomes
The findings from stepwise multivariate logistical regression analysis in assessing the predictors for aneurysm complete obliteration and patient functional outcomes after the procedure indicated that E2 was comparable to E1 after adjusting for potential confounding factors (all p > 0.05). However, the patients treated with E2 had significantly fewer procedure-related complications (Table 3), which is consistent with the results of univariate analysis. After adjusting for the effects of age, the presence of hypertension and aneurysm width and height, the risk of complications associated with E2 was 64% lower compared with E2 (odds ratio [OR]: 0.36; 95% CI: 0.15–0.91). The model also indicates that increased age (OR: 2.48; 95% CI: 1.29–4.77), the presence of hypertension (OR: 2.83; 95% CI: 1.13–7.09) and a large aneurysm width (OR: 1.22; 95% CI: 1.02–1.45) were all independently associated with risk of procedure-related complications.
| Variables | Odds ratio | 95% CI | p-value |
|---|---|---|---|
| Enterprise 2 (vs Enterprise 1) | 0.36 | 0.15–0.91 | 0.031 |
| Age (years) | 2.48 | 1.29–4.77 | 0.007 |
| Presence of hypertension (yes/no) | 2.83 | 1.13–7.09 | 0.026 |
| Aneurysm width (mm) | 1.22 | 1.02–1.45 | 0.026 |
| Aneurysm height (mm) | 0.85 | 0.71–1.03 | 0.099 |
Discussion
In this retrospective, observational study on treating ruptured intracranial aneurysms (RIAs) in a real-world setting, the authors found that, compared with the first-generation Enterprise (E1) stent, the second-generation Enterprise (E2) stent had similar clinical effectiveness with respect to cerebral aneurysm obliteration and patient functional outcomes, as well as comparable aneurysm recurrence by 6 months post-discharge. It was also observed that E2 appeared to have advantages over its earlier generation in terms of significantly shorter operation time and fewer procedure-related complications.
As a self-expandable laser device with a closed-cell design, the Enterprise stent was generally preferred in tortuous and difficult vascular anatomy because of its improved navigability and ease of deployment [15]. In addition, the Enterprise stent can be recaptured and repositioned, including complete withdrawal, if needed. However, it has been observed that the Enterprise stent increasingly tends to have incomplete vessel wall apposition and to cause kinks when it is deployed in vessels with a smaller radius of curvature or a larger diameter of parent vessels (Figure 1) [16,17]. The occurrence of stent vessel wall malposition was found to be associated with radiological as well as clinical signs of cerebral ischemia, both immediately and on follow-up [7,18].
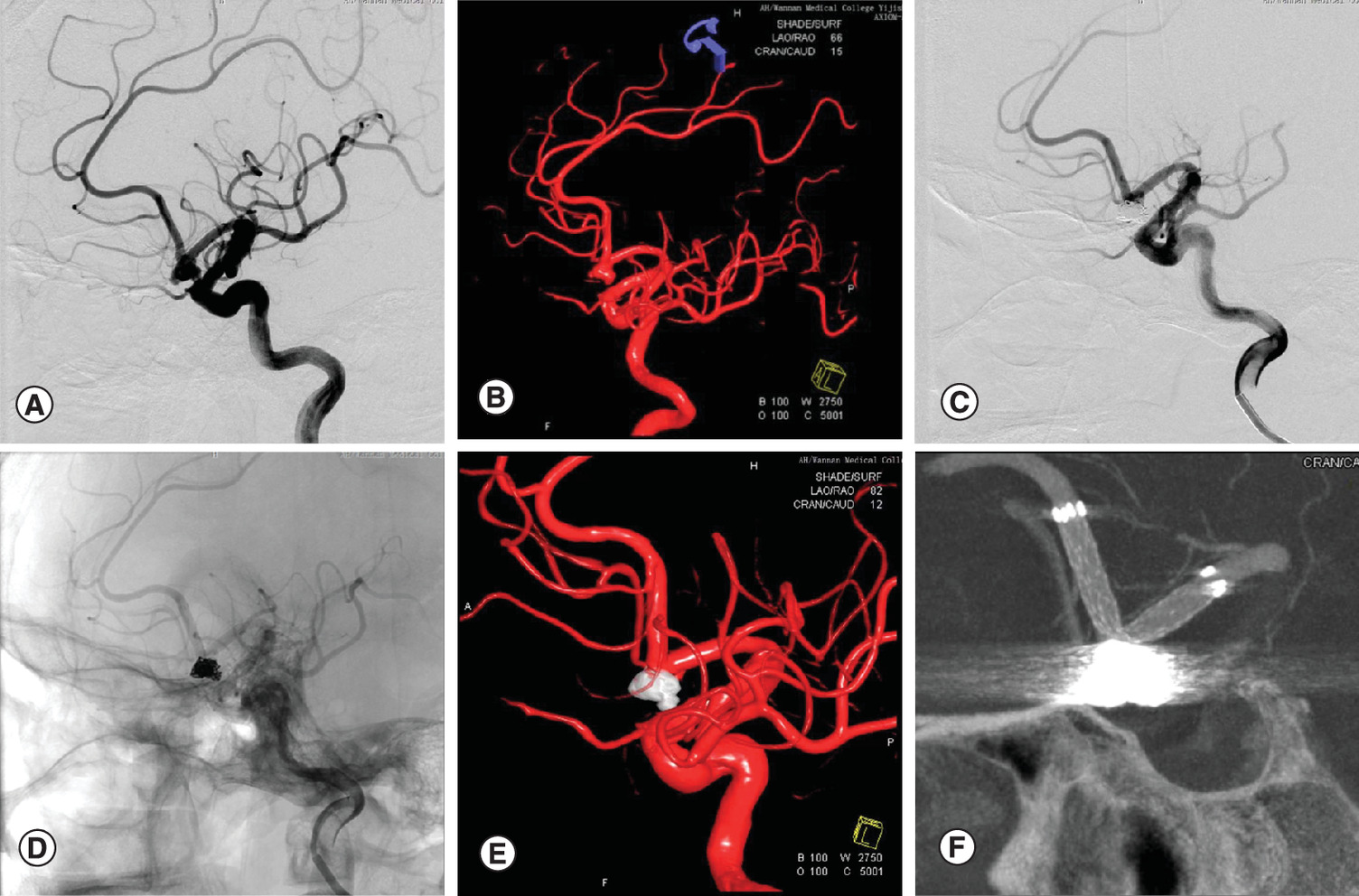
Figure 1. A case from the Enterprise 1 group.
(A & B) The pre-operative angiographic imaging and 3D reconstruction showed an anterior communicating aneurysm. (C & D) The aneurysm was treated with Enterprise 1 assisted coiling. The immediate post-operative angiographic imaging showed the aneurysm was occluded completely. (E) The post-operative 3D reconstruction. (F) The post-operative DynaCTA showed a kink at the neck of the aneurysm.
A few studies compared Enterprise with the Neuroform stent, which is also a self-expanding stent but with an open-cell design, on their risk of procedure-related complications. In one study, the Enterprise stent was shown to be easier to deploy and expanded the number of treatable aneurysms but was associated with increased thromboembolic complications [19]. Another large case series study, with 486 aneurysms treated, found no significant differences in either total or major complication rates between Enterprise and Neuroform stent use [20]. Nevertheless, it is interesting that the data suggested that closed-cell stents may be safer than open-cell stents when an overlapping-stent construct is used. Another large, retrospective study with 435 patients examining in-stent stenosis complications also revealed no difference in risk between Enterprise and Neuroform stents [21].
The successor E2 stent was developed with a changed, closed-cell design of the strut geometry, which is thought to improve its conformity of wall apposition in curved vessels (Figure 2). To achieve this, the geometry of the stent struts was redesigned to enable increased flexibility by allowing the stent to elongate more on the outer curvature and to compress more on the inner curvature [9]. In an in vitro study, E2 exhibited significantly better vessel wall apposition on curved vessels than its predecessor. The gap between the vessel wall and the stent in the E2 stent was approximately half of that in the E1 stent [22]. In another in vitro study, the investigators found that deploying the E2 using the pushing over outer curve technique resulted in a lower incidence of incomplete stent apposition than using the conventional Heller’s push and pull technique of stent deployment. In addition, E2 was shown to have excellent kink resistance than E1. [23].

Figure 2. A case from the Enterprise 2 group.
(A & B) The pre-operative angiographic imaging and 3D reconstruction showed an anterior communicating aneurysm. (C & D) The aneurysm was treated with Enterprise 2 assisted coiling. The immediate post-operative angiographic imaging showed the aneurysm was occluded completely. (E) The post-operative 3D reconstruction. (F) The post-operative DynaCTA showed that the stent was fully open.
Despite the evidence from laboratory evaluations of the stent conformation of E2, little is known about whether the better vessel wall apposition can result in improved clinical outcomes. The findings from the present study indicated that the patients treated with E2 experienced lower risks of procedure-related complications, mostly noticeable in a reduction in in-stent thrombosis. While it is plausible that reduced ischemic complications were attributable to its improved geometry design, the administration of anti-platelet regimens is critical in lowering thrombotic complications with SAC. While dual anti-platelet therapies are routinely used to prevent the occurrence of thromboembolic complications in patients undergoing SAC both pre- and post-operatively, significant heterogeneity in dual anti-platelet regimens exist across different treatment centers [24]. As the present study is a single-center study, the same anti-platelet regimens were used for the study population with similar compliance over the study period.
This study also showed significantly shorter operation time with the E2 stent. One possible reason is that physicians may have needed more time to perform the procedure when the E1 stent was first introduced because of the learning curve. However, there was no trend toward decreased operation time over time being observed when the operation time for the Enterprise stent deployment was analyzed by quintile groups (data not shown). The reduced operation time also cannot be explained by the aneurysm locations or the underlying disease severity. It is likely that fewer in-procedure complications may have contributed to the shorter operation time.
The results of this study should be interpreted in the context of study limitations. First, the study was a non-randomized, retrospective study conducted at a single center. The results reflect the experience of a single center with a specific technique and anti-coagulation protocols and may not be readily generalizable to other centers. On the other hand, a single-center study may have higher interval validity versus a multicenter study, as the findings cannot be distorted because of practice variation (e.g., neurointerventionalists' skills) across the centers. Second, E2 was only recently introduced into clinical practice. As a result, the authors of the present study focused their analysis on outcomes during perioperative and intermediate periods instead of the long term. Finally, the sample size, particularly for the E2 group, was relatively small, which would limit the power of statistical significance testing and increase the likelihood of false-negative findings.
Conclusion
In a real-world setting, we found that, compared with the first-generation Enterprise stent, the second-generation Enterprise stent had similar clinical effectiveness with respect to cerebral aneurysm obliteration and patient functional outcomes immediately after the procedure, as well as comparable patient functional outcomes and aneurysm recurrence by 6 months post-discharge. We also observed that the second-generation Enterprise stent appeared to have advantages over its earlier generation, with fewer procedure-related complications and a significantly shorter operation time.
•
The Enterprise stent is an innovative, self-expandable nitinol stent system used in stent-assisted coiling for treating intracranial aneurysms (IAs).
•
The aim of this study was to compare and analyze the effectiveness and safety of the Enterprise 2 (E2) stent versus the Enterprise 1 (E1) stent in treating ruptured IAs in a real-world setting in China.
•
Compared with the E1 stent, the E2 stent had similar effectiveness but a lower complication risk in treating ruptured IAs.
•
A total of 360 patients (E2 group = 90; E1 group = 270) were included with no differences in demographic characteristics between the E2 and E1 groups (mean age: 60.0 vs 58.4 years; male gender: 27.8% vs 29.3%).
•
Stent deployment was successful in all patients in both groups.
•
Immediate complete occlusion was similar between the two groups (E2 vs E1: 80.0% vs 75.1%; p = 0.593) and most of the patients achieved good functional outcomes (Modified Rankin Scale score ≤2 ) at discharge (E2 vs E1: 78.7% vs 81.1%; p = 0.612).
•
The E2 group had a lower perioperative procedure-related complication rate compared with the E1 group (7.8% vs 16.4%; odds ratio: 0.36; 95% CI: 0.15–0.91; p = 0.031).
•
The operation time was significantly shorter for the E2 group (166.3 vs 190.3 min; p = 0.008), and the length of hospital stay was shorter for the E2 group (16.7 vs 19.2 days) but the difference did not reach statistical significance.
•
By 6 months post-discharge, the patients receiving the E2 stent had good functional outcomes and aneurysm recurrence similar to those of the patients in the E1 group (80.2% vs 81.9% and 13.3% vs 14.9%, respectively).
Author contributions
Z Li contributed to the study design, data collection, analysis and manuscript writing. J Xuan contributed to the conception, design and analysis of the research. X Fang contributed to the literature review and data collection. X Zhao contributed to medical issues communication during data analysis and contributed to the literature review. B Zhang, D Wu, N Lai, J Liu, Z Zhang, J Yuan and F Qin contributed to manuscript writing and data collection.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This study involved data relating to human participants and was approved by the scientific research and new technology institutional review board (IRB) of Wannan Medical College Yijishan Hospital. IRB approval no.: 2019-86.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Connolly ES Jr, Rabinstein AA, Carhuapoma JR et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage. Stroke 43(6), 1711–1737 (2012).
2.
Bodily KD, Cloft HJ, Lanzino G, Fiorella DJ, White PM, Kallmes DF. Stent-assisted coiling in acutely ruptured intracranial aneurysms: a qualitative, systematic review of the literature. AJNR Am. J. Neuroradiol. 32(7), 1232–1236 (2011).
3.
Bsat S, Bsat A, Tamim H et al. Safety of stent-assisted coiling for the treatment of wide-necked ruptured aneurysm: a systematic literature review and meta-analysis of prevalence. Interv. Neuroradiol. 26(5), 547–556 (2020).
4.
Lee KS, Zhang JJY, Nguyen V et al. The evolution of intracranial aneurysm treatment techniques and future directions. Neurosurg. Rev. 45(1), 1–25 (2021).
•• Summarizes the intracranial aneurysm treatment techniques and illustrates the evolution of techniques to overcome the shortfalls of preceding techniques.
5.
Phan K, Huo YR, Jia F et al. Meta-analysis of stent-assisted coiling versus coiling only for the treatment of intracranial aneurysms. J. Clin. Neurosci. 31, 15–22 (2016).
6.
Lubicz B, François O, Levivier M, Brotchi J, Balériaux D. Preliminary experience with the Enterprise stent for endovascular treatment of complex intracranial aneurysms: potential advantages and limiting characteristics. Neurosurgery 62(5), 1063–1069 (2008).
7.
Heller R, Calnan DR, Lanfranchi M, Madan N, Malek AM. Incomplete stent apposition in Enterprise stent-mediated coiling of aneurysms: persistence over time and risk of delayed ischemic events. J. Neurosurg. 118(5), 1014–1022 (2013).
8.
Chen L, Zheng C, Wu J, Gong J, Gao Y, Wan S. The Enterprise2 stent for endovascular treatment of intracranial aneurysms: short-term results from a single center experience. Front. Neurol. 11, 589689 (2020).
• Experiences on the Enterprise 2 stent in the treatment of intracranial and cranial cervical junction aneurysms.
9.
Herweh C, Nagel S, Pfaff J et al. First experiences with the new Enterprise2® stent. Clin. Neuroradiol. 28(2), 201–207 (2018).
• First experiences with the Enterprise 2 stent in the treatment of atherosclerotic stenosis.
10.
Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J. Neurosurg. 28(1), 14–20 (1968).
11.
Fisher CM, Kistler JP, Davis JM. Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery 6(1), 1–9 (1980).
12.
Mascitelli JR, Moyle H, Oermann EK et al. An update to the Raymond–Roy occlusion classification of intracranial aneurysms treated with coil embolization. J. Neurointerv. Surg. 7(7), 496–502 (2016).
• The research proposed the modified Raymond–Roy cassification to further differentiate intracranial aneurysms treated with coil embolization.
13.
Jang CK, Chung J, Lee JW, Huh SK, Son NH, Park KY. Recurrence and retreatment of anterior communicating artery aneurysms after endovascular treatment: a retrospective study. BMC Neurol. 20(1), 287 (2020).
14.
Bonita R, Beaglehole R. Recovery of motor function after stroke. Stroke 19(12), 1497–1500 (1988).
15.
Chalouhi N, Jabbour P, Singhal S et al. Stent-assisted coiling of intracranial aneurysms: predictors of complications, recanalization, and outcome in 508 cases. Stroke 44(5), 1348–1353 (2013).
16.
Heller RS, Malek AM. Parent vessel size and curvature strongly influence risk of incomplete stent apposition in Enterprise intracranial aneurysm stent coiling. AJNR Am. J. Neuroradiol. 32(9), 1714–1720 (2011).
17.
Ebrahimi N, Claus B, Lee CY, Biondi A, Benndorf G. Stent conformity in curved vascular models with simulated aneurysm necks using flat-panel CT: an in vitro study. AJNR Am. J. Neuroradiol. 28(5), 823–829 (2007).
18.
Heller RS, Miele WR, Do-Dai DD, Malek AM. Crescent sign on magnetic resonance angiography revealing incomplete stent apposition: correlation with diffusion-weighted changes in stent-mediated coil embolization of aneurysms. J. Neurosurg. 115(3), 624–632 (2011).
19.
Kadkhodayan Y, Rhodes N, Blackburn S, Derdeyn CP, Cross DT 3rd, Moran CJ. Comparison of Enterprise with Neuroform stent-assisted coiling of intracranial aneurysms. Am. J. Roentgenol. 200(4), 872–878 (2013).
20.
Johnson AK, Munich SA, Tan LA, Heiferman DM, Keigher KM, Lopes DK. Complication analysis in nitinol stent-assisted embolization of 486 intracranial aneurysms. J. Neurosurg. 123(2), 453–459 (2015).
21.
Chalouhi N, Drueding R, Starke RM et al. In-stent stenosis after stent-assisted coiling: incidence, predictors and clinical outcomes of 435 cases. Neurosurgery 72(3), 390–396 (2013).
22.
Kono K, Terada T. In vitro experiments of vessel wall apposition between the Enterprise and Enterprise 2 stents for treatment of cerebral aneurysms. Acta Neurochir. (Wien) 158(2), 241–245 (2016).
23.
Chihara H, Ishii A, Kikuchi T, Ikeda H, Arai D, Miyamoto S. Deployment technique that takes advantage of the characteristics of Enterprise VRD2: an in vitro study. J. Neurointerv. Surg. 9(10), 969–973 (2017).
24.
Gupta R, Moore JM, Griessenauer CJ et al. Assessment of dual-antiplatelet regimen for pipeline embolization device placement: a survey of major academic neurovascular centers in the United States. World Neurosurg. 96, 285–292 (2016).
Information & Authors
Information
Published In
Pages: 879 - 887
PubMed: 35734978
Copyright
© 2022 Future Medicine Ltd.
History
Received: 18 January 2022
Accepted: 6 June 2022
Published online: 23 June 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparison of Enterprise stent 2 with 1 in assisting coiling of ruptured aneurysms: a real-world study. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0005
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Reade De Leacy, Rahul Khanna, Emilie Kottenmeier, Yiran Rong, Readmissions and retreatment among stent-assisted endovascular coiling patients with unruptured intracranial aneurysm using ENTERPRISE® 2 stent versus LVIS™ stent, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0166, 15, 5, (2026).
- Jinlong Yuan, Chenlei Huang, Zhenbao Li, Niansheng Lai, Jiaqiang Liu, Bingbing Zhang, Gang Zhou, Dayong Xia, Xintong Zhao, The EP-VRD2 for endovascular treatment of ophthalmic segment aneurysms: wall apposition and long-term study, Frontiers in Neurology, 10.3389/fneur.2026.1750959, 17, (2026).
- Reade DeLeacy, Zhiqiang Yao, Rahul Khanna, Emilie Kottenmeier, Yiran Rong, Hospital readmission among patients with unruptured intracranial aneurysms undergoing stent-assisted endovascular coiling using the ENTERPRISE® 2 stent versus Neuroform® Atlas stent, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0096, 14, 10, (2025).
- Yichuan Zhang, Jinbo Bai, Fu Kang, Wei Li, Zaixing Xiao, Yong Ma, Erqing Chai, A nomogram to predict the risk of bleeding after discharge from stent-assisted ruptured aneurysm embolization in a Chinese population, Neurosurgical Review, 10.1007/s10143-023-01952-2, 46, 1, (2023).
- Kun Zhang, Wei Ren, Tian-Xiao Li, Zi-Liang Wang, Bu-Lang Gao, Jin-Chao Xia, Hui-Li Gao, Yong-Feng Wang, Jian-Jun Gu, Sub-satisfactory recanalization of severe middle cerebral artery stenoses can significantly improve hemodynamics, Frontiers in Cardiovascular Medicine, 10.3389/fcvm.2022.922616, 9, (2022).