Hospital readmission among patients with unruptured intracranial aneurysms undergoing stent-assisted endovascular coiling using the ENTERPRISE® 2 stent versus Neuroform® Atlas stent
Publication: Journal of Comparative Effectiveness Research
Abstract
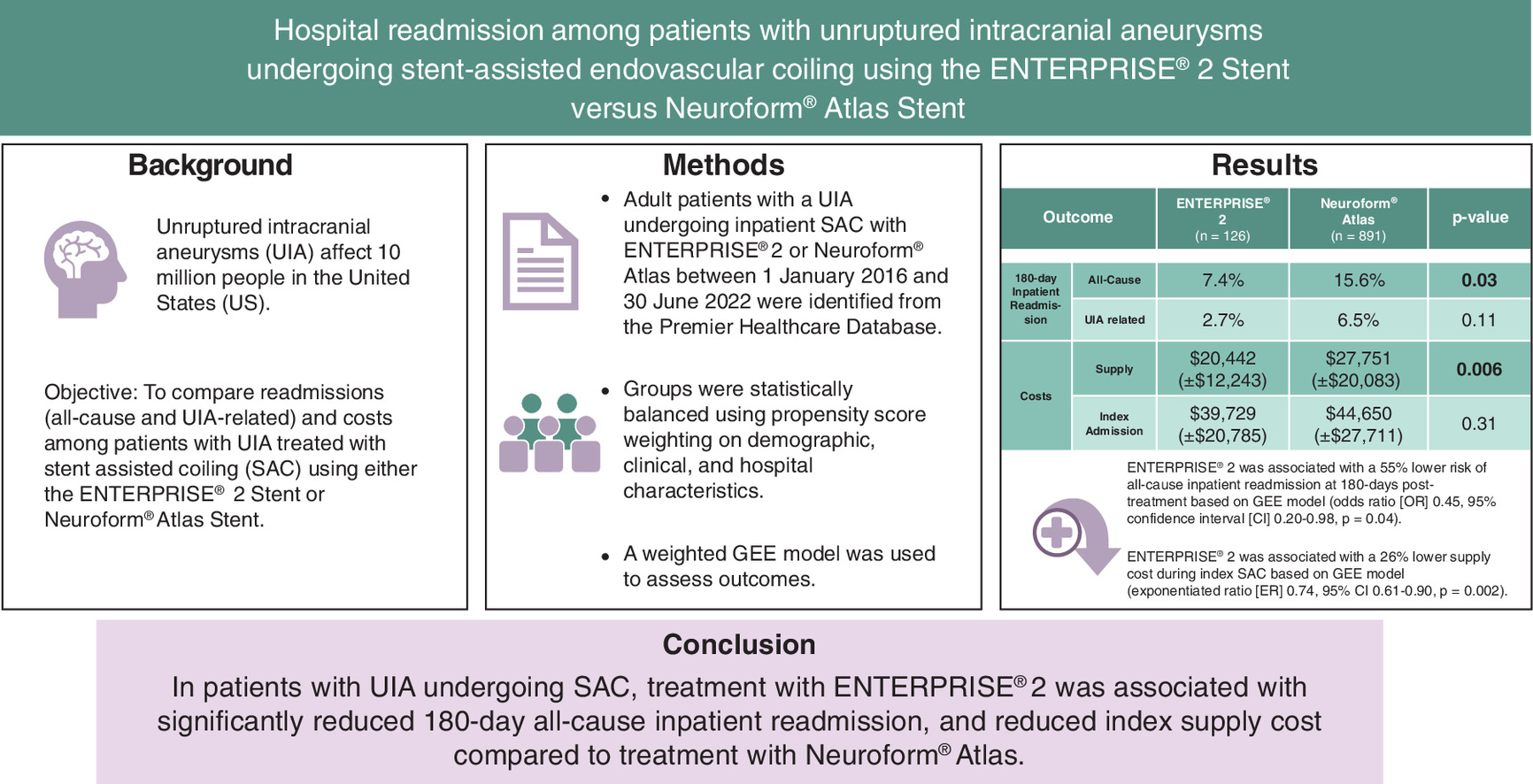
Aim: Stent-assisted endovascular coiling is a safe and effective treatment for unruptured intracranial aneurysms (UIAs). This study compared 180-day inpatient readmission and cost among patients with UIA who underwent stent-assisted coiling (SAC) using the ENTERPRISE® 2 or Neuroform® Atlas stent. Materials & methods: In this retrospective cohort study, adults with UIA undergoing SAC were identified in the Premier Healthcare Database (2016–2022) and grouped based on the stent used: ENTERPRISE 2 or Neuroform Atlas. Outcomes included all-cause and UIA-related inpatient readmission in the 180 days following treatment, index admission and supply cost. Inverse probability of treatment weighting of propensity score method balanced the two cohorts on study covariates. A weighted generalized estimating equation model assessed study outcomes. Results: A total of 1017 patients were included (ENTERPRISE 2, n = 126; Neuroform Atlas, n = 891). Hospital and patient characteristics except race were well-balanced after weighting. Patients treated with ENTERPRISE 2 versus Neuroform Atlas were 55% less likely to have an all-cause inpatient readmission in the 180-day follow-up period (odds ratio 0.45, 95% CI: 0.20–0.98, p = 0.04). Further, the ENTERPRISE 2 cohort had significantly lower index supply cost ($20,442 vs $27,561, exponentiated ratio 0.74, 95% CI: 0.61–0.90, p = 0.002) compared with the Neuroform Atlas cohort. No significant differences were observed in UIA-related inpatient readmission or total index admission cost between cohorts. Conclusion: Among patients with UIA undergoing SAC, the use of ENTERPRISE 2 stent was associated with a significantly reduced risk of all-cause inpatient hospital readmission and significantly lower index supply cost compared with the Neuroform Atlas stent.
Plain language summary
What is this article about?
Unruptured intracranial aneurysms (UIAs) affect about 3% of the population. Stent-assisted endovascular coiling is a common treatment modality for UIA. This study compared readmissions and costs among UIA patients undergoing stent-assisted endovascular coiling using the ENTERPRISE® 2 stent versus Neuroform® Atlas stent.
What were the results?
Patients treated with ENTERPRISE 2 stent had a significantly lower risk of all-cause inpatient hospital readmission and lower cost of supplies during admission for coiling procedure compared with those treated with Neuroform Atlas stent. There were no differences in UIA related inpatient readmission or total admission cost between the two groups.
What do the results mean?
The use of ENTERPRISE 2 stent (vs Neuroform Atlas stent) was associated with lower costs and hospital readmission rates following stent-assisted endovascular coiling for UIA.
Graphical abstract
Unruptured intracranial aneurysms (UIAs) are a significant health concern, affecting 10 million people (∼3% of the general population) in the US [1,2]. Nearly a third of patients with UIA are at risk for rupture during their lifetime [1]. Ruptured intracranial aneurysms carry substantial morbidity and mortality, accounting for nearly 80% of nontraumatic subarachnoid hemorrhages (SAHs) [3] and a fatality rate of 27–44% [4]. With the incidental diagnoses of UIA increasing due to widespread use of cranial imaging [5], it is imperative to identify the most effective and efficient treatments available.
Endovascular coiling is a common treatment approach for UIA [6], and has demonstrated lower rates of neurological complications, cardiovascular complications, disability, and mortality rates compared with surgical clipping [7,8], with occlusion outcomes comparable to flow diverters [9]. Additionally, cost savings have been observed with endovascular coiling compared with surgical clipping due to shorter hospital and ICU stays, lowering overall medical resource consumption [10]. Cost savings have also been observed with endovascular coiling compared with flow diverters when treating aneurysms <0.9 cm3 [11], with long-term cost benefits due to lower staffing requirements, shorter hospital stays [12], and better functional outcomes [13]. However, endovascular coiling alone can be insufficient for treating wide-necked aneurysms [14], defined by a neck of ≥4 mm or dome-to-neck ratio of <2 [15], which generally require stents and balloons for complete occlusion [16]. Therefore, stent-assisted coiling (SAC) was developed as an advanced, safe and effective solution to overcome insufficiencies such as coil prolapse observed with endovascular coiling alone for wide-necked aneurysms, and to promote aneurysm thrombosis. These advancements have improved endovascular treatment for UIA [17]. Two of the most commonly-used stents employed in SAC for UIA are ENTERPRISE® (CERENOVUS, CA, USA) and Neuroform® Atlas (Stryker Neurovascular, MI, USA). Both stents have good safety profiles and studies show similar efficacy results [18–23], with the major differentiating feature being the closed-cell design of ENTERPRISE and open-cell design of Neuroform Atlas.
Studies comparing performance and patient outcomes between the two stents have found that ENTERPRISE stent is easier to deploy, has higher rates of complete occlusion and recanalization, lower mortality rates and better economic outcomes compared with Neuroform Atlas [17,19,24]. Additionally, a recent propensity-score matched cohort study found that patients with UIA treated with ENTERPRISE had significantly lower hospital readmission rates compared with those treated with Neuroform [19], However, the authors included all generations of both ENTERPRISE and Neuroform stents. Several features of ENTERPRISE 2 differ from its previous generation, (ENTERPRISE 1), including a novel geometric design to improve conformability, radiopacity, delivery system, outward force and shelf-life. Studies comparing ENTERPRISE 2 to its earlier generation have found significant improvements in wall apposition in curved vessels [25,26], lower procedure complication rates, and shorter operation times for the treatment of UIA [27]. Several design improvements have also been made to the Neuroform Atlas® stent compared with its previous generation (Neuroform EZ®), including improved trackability, smaller cell size with improved coil support and retention, decreased internal microcatheter diameter for a lower profile, improved recrossing and stability from the closed cell design at the proximal end, and an open-cell design for improved conformability to the vessel wall [28]. SAC with Neuroform Atlas has improved rates of immediate Raymond-Roy Class 1 occlusion and the need for retreatment compared with Neuroform EZ [29]. The differential features offered by ENTERPRISE 2 and Neuroform Atlas may impact patient outcomes including rehospitalization and cost associated with UIA treatment.
As the prevalence and burden of UIA on the healthcare system escalates, there is a need to evaluate patient outcomes and cost associated with different SAC devices. The objective of this study was to examine patient outcomes including all-cause and UIA-related inpatient readmission in the 180 days following treatment among patients with UIA who underwent endovascular coiling using ENTERPRISE 2 versus Neuroform Atlas stent. Further, we compared cost differentials (index admission and supply) associated with treatment using the two devices.
Materials & methods
Data source
Using a retrospective cohort design, we analyzed the Premier Healthcare Database (PHD) from July 2015 to December 2022. The PHD includes billing data from more than 1000 hospitals representing different bed sizes, teaching statuses and geographic regions across the US. Information on billed medications, diagnostic and therapeutic services, and primary and secondary diagnoses associated with hospitalizations detailed from a cost-accounting department is available in the PHD, in addition to patient demographic and payer information. As dictated by Title 45 Code of Federal Regulations (45 CFR 46.101(b)(4))) (https://www.govinfo.gov/content/pkg/CFR-2011-title45-vol1/pdf/CFR-2011-title45-vol1.pdf), Institutional Review Board oversight was not required for our analysis using the PHD. No individuals were identified in the aggregated data.
Study sample
Adult patients with a primary diagnosis of UIA undergoing an elective inpatient SAC procedure with ENTERPRISE 2 or Neuroform Atlas between 1 January 2016 and 30 June 2022 were identified from the PHD. The first observed hospital admission during this period meeting these criteria was designated as the index hospital admission. Patients were required to have undergone their SAC procedure at a hospital that contributed to the PHD during the 180-day pre- and 180-day post-index period and were then classified into the ENTERPRISE 2 or Neuroform Atlas cohort.
Patients who had a diagnosis present on admission of SAH or ruptured aneurysm, or those who had undergone inpatient endovascular coiling or surgical clipping in the 180-day pre-index period with a primary diagnosis of UIA or SAH were not included.
Study covariates
Patient demographics evaluated included age (18–49, 50–59, 60–69 and 70+ years), sex (male, female), race/ethnicity (white, non-white), marital status (married, non-married) and payer type (commercial, Medicare, Medicaid/other). Patient clinical characteristics including the Elixhauser Comorbidity Index score, presence of diabetes, hypertension, congestive heart failure, transient ischemic attack, obesity and depression were also assessed based on diagnoses present during the index admission. Hospital characteristics included size (000–499 beds, 500+ beds), geographic region (Midwest, South, Northeast, West), type (teaching, non-teaching) and 180-day pre-index endovascular coil volume.
Study outcomes
Primary study outcomes were 180-day all-cause inpatient readmission and 180-day UIA-related inpatient readmission (i.e., primary diagnosis of UIA) in the post-index SAC procedure period. Secondary outcomes were index admission cost and index supply cost. We evaluated the secondary outcomes based on a subset of the study cohort in which patients had validated cost information during their index admission.
Statistical analysis
Inverse probability of treatment weighting
The inverse probability of treatment weighting (IPTW) of propensity score approach was used to minimize the effect of potential confounders and balance the cohorts on study covariates [30]. Each patient was assigned a weight using IPTW and an estimation of average treatment effect. A logistic regression model was used to estimate the propensity score of an individual to use ENTERPRISE 2. The inverse of the propensity score was used to generate the weight for each patient. Stabilized IPTW weights were calculated for each patient and applied in the analysis. The absolute standardized mean difference (SMD) was used to determine if the distribution of covariates were well-balanced after weighting, with a value of ≥0.25 to ≤ -0.25 indicating an unbalanced distribution.
Data analysis
Descriptive statistics for the pre- and post- weighted cohorts were reported for all study variables. To examine study outcomes between the cohorts on covariates, bivariate comparisons were conducted post-weighting using chi-square tests. To examine differences in readmission outcomes between cohorts, a weighted generalized estimating equation (GEE) model with logit link and binomial distribution function was used. GEE model with log link and gamma distribution was used to evaluate the cost outcomes between cohorts. The GEE models adjusted for hospital clustering to adjust for correlations in outcomes among patients who underwent treatment in the same hospital. Any covariate that emerged as significant post-weighting (based on the absolute SMD outside of the ≥0.25 to ≤ -0.25 range) was further controlled for in the GEE model. The Benjamini–Hochberg (BH) correction method was used to account for Type I errors caused by multiple comparisons for outcomes assessed in the regression analysis. A p-value of <0.05 was considered statistically significant (for BH corrections, the highest p smaller than the BH critical value was identified [using a false discovery rate of 0.10], with all ps above the highest p-value considered significant). All analyses were conducted using R software (Version 4.1.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
A total of 1017 patients met the study criteria, of whom 126 (12%) were treated with ENTERPRISE 2 and 891 (88%) were treated with Neuroform Atlas. Supplementary Figure 1 shows the study patient attrition.
Prior to IPTW, several covariates were unbalanced between the groups (Table 1). There was a significant difference in age (aSMD = 0.287), where a lower proportion of the ENTERPRISE 2 group were over age 60 years (52.4% [66/126] vs 63.7% [567/891] for Neuroform Atlas). There was a significant difference in payer type (aSMD = 0.394), with a significantly higher proportion of the ENTERPRISE 2 group having commercial insurance (50.8% [64/126] vs 32.2% [287/891]) versus those treated with Neuroform Atlas. Mean Elixhauser score was lower for the ENTERPRISE 2 group (1.87 ± 1.69 vs 2.31 ± 1.60 for Neuroform Atlas, aSMD = 0.268), which had a higher proportion of scores 0–1 (50.8% [64/126] vs 33.5% [298/891] for Neuroform Atlas, aSMD = 0.361). The ENTERPRISE 2 group had a lower proportion of patients with hypertension (59.5% [75/126] vs 74.7% [666/891], aSMD = 0.328), and obesity (5.6% [7/126] vs 16.8% [150/891], aSMD = 0.364) than Neuroform Atlas group. A greater proportion of patients in the ENTERPRISE 2 group were treated in hospitals with 500+ beds (86.5% [109/126] vs 57.0% [508/891] for Neuroform Atlas, aSMD = 0.693), and in hospitals in the South (76.2% [96/126] vs 53.2% [474/891] for Neuroform Atlas, aSMD = 0.497) versus those in Neuroform Atlas group. Mean endovascular coiling volume was higher in the ENTERPRISE 2 group (24.54 ± 13.23 vs 19.96 ± 14.26, aSMD = 0.333) versus the Neuroform Atlas group. After weighting, the study cohorts were well-balanced for all covariates except race (post-weighting aSMD = 0.326). To adjust for any potential impact of race on study outcomes, we controlled for race in the GEE analyses.
| Pre-weighted | Post-weighted | |||||
|---|---|---|---|---|---|---|
| ENTERPRISE® 2, n (%) (n = 126) | Neuroform® Atlas, n (%) (n = 891) | aSMD | ENTERPRISE® 2, % | Neuroform® Atlas, % | aSMD | |
| Age range, years | 0.287 | 0.127 | ||||
| 18–49 | 28 (22.2%) | 118 (13.2%) | 17.0% | 13.4% | ||
| 50–59 | 32 (25.4%) | 206 (23.1%) | 25.8% | 23.6% | ||
| 60–69 | 33 (26.2%) | 323 (36.3%) | 29.4% | 34.9% | ||
| 70+ | 33 (26.2%) | 244 (27.4%) | 27.8% | 27.1% | ||
| Gender | 0.061 | 0.060 | ||||
| Male | 38 (30.2%) | 244 (27.4%) | 30.5% | 27.8% | ||
| Female | 88 (69.8%) | 647 (72.6%) | 69.5% | 72.2% | ||
| Race | 0.113 | 0.326† | ||||
| White | 95 (75.4%) | 627 (70.4%) | 84.7% | 71.3% | ||
| Non-white | 31 (24.6%) | 264 (29.6%) | 15.3% | 28.7% | ||
| Marital status | 0.196 | 0.139 | ||||
| Married | 71 (56.3%) | 415 (46.6%) | 40.9% | 47.8% | ||
| Non-married | 55 (43.7%) | 476 (53.4%) | 59.1% | 52.2% | ||
| Payer type | 0.394 | 0.126 | ||||
| Commercial | 64 (50.8%) | 287 (32.2%) | 29.2% | 34.6% | ||
| Medicare | 48 (38.1%) | 437 (49.0%) | 49.4% | 47.6% | ||
| Medicaid/Other | 14 (11.1%) | 167 (18.8%) | 21.4% | 17.8% | ||
| Elixhauser score | ||||||
| Mean (SD) | 1.87 (1.69) | 2.31 (1.60) | 0.268 | 2.11 (1.61) | 2.25 (1.61) | 0.085 |
| 0–1 | 64 (50.8%) | 298 (33.5%) | 0.361 | 39.3% | 35.6% | 0.162 |
| 2–3 | 45 (35.7%) | 412 (46.2%) | 47.2% | 44.9% | ||
| 4+ | 17 (13.5%) | 181 (20.3%) | 13.5% | 19.5% | ||
| Diabetes | 19 (15.1%) | 173 (19.4%) | 0.115 | 12.9% | 18.8% | 0.164 |
| Hypertension | 75 (59.5%) | 666 (74.7%) | 0.328 | 71.2% | 72.8% | 0.036 |
| Congestive heart failure | 3 (2.4%) | 56 (6.3%) | 0.193 | 4.0% | 5.8% | 0.083 |
| TIA/Stroke | 22 (17.5%) | 106 (11.9%) | 0.158 | 15.0% | 12.8% | 0.064 |
| Obesity | 7 (5.6%) | 150 (16.8%) | 0.364 | 13.6% | 15.4% | 0.052 |
| Depression | 13 (10.3%) | 140 (15.7%) | 0.161 | 22.6% | 15.1% | 0.191 |
| Hospital bed size | 0.693 | 0.036 | ||||
| <500 | 17 (13.5%) | 383 (43.0%) | 41.1% | 39.4% | ||
| 500+ | 109 (86.5%) | 508 (57.0%) | 58.9% | 60.6% | ||
| Hospital region | 0.497 | 0.172 | ||||
| Midwest/West | 21 (16.7%) | 281 (31.5%) | 33.5% | 29.8% | ||
| Northeast | 9 (7.1%) | 136 (15.3%) | 18.8% | 14.3% | ||
| South | 96 (76.2%) | 474 (53.2%) | 47.7% | 55.9% | ||
| Hospital type | 0.211 | 0.175 | ||||
| Teaching | 98 (77.8%) | 610 (68.5%) | 61.2% | 69.5% | ||
| Non-teaching | 28 (22.2%) | 281 (31.5%) | 38.8% | 30.5% | ||
| Endovascular coiling volume (mean, SD) | 24.54 (13.23) | 19.96 (14.26) | 21.74 (14.65) | 20.58 (14.33) | ||
†
Race was controlled in the GEE regression analyses.
Boldface data are aSMD values that exceed the 0.25 cutoff.
aSMD: Absolute standardized mean difference; SD: Standard deviation; TIA: Transient ischemic attack.
Outcomes
All-cause inpatient readmission in the 180-day post-index stent-assisted endovascular coiling period was significantly lower for patients treated with ENTERPRISE 2 compared with Neuroform Atlas in the bivariate analysis after weighting (7.4 vs 15.6%, p = 0.03). No significant difference in 180-day UIA related inpatient readmission was observed among patients treated with ENTERPRISE 2 versus Neuroform Atlas (2.7 vs 6.5%, p = 0.11). Results from the GEE analysis showed that patients treated with ENTERPRISE 2 had a 55% lower risk of all-cause inpatient readmission in the 180-day post-endovascular procedure period versus those treated with Neuroform Atlas (odds ratio [OR]: 0.45 [0.20–0.98], p = 0.04). No significant difference in 180-day UIA related inpatient readmission was observed among the ENTERPRISE 2 versus Neuroform Atlas cohort (OR: 0.39 [0.12–1.26], p = 0.12).
We examined cost outcomes in a subset of patients (n = 887) with 119 patients were treated with ENTERPRISE 2 and 768 were treated with Neuroform Atlas. In the bivariate analysis, no significant difference in index admission cost was observed between the ENTERPRISE 2 versus Neuroform Atlas cohort ($39,729 [$20,785] vs $44,650 [$27,711], p = 0.31); however, the ENTERPRISE 2 cohort had significantly lower index supply cost versus the Neuroform Atlas cohort ($20,442 [($12,243] versus $27,561 [($20,083], p = 0.006). Variables including race, Elixhauser score, presence of depression and hospital region were not well-balanced post weighting, therefore these variables were further controlled in the GEE models. Results from the GEE analysis did not reveal any significant difference in the index admission cost among the ENTERPRISE 2 and Neuroform Atlas cohort (exponentiated ratio [ER]: 0.91 [0.76–1.09], p = 0.29). The use of ENTERPRISE 2 was associated with a 26% lower supply cost versus Neuroform Atlas in the GEE analysis (ER: 0.74 [0.61–0.90], p = 0.002) (Table 2).
| ENTERPRISE® 2† | Neuroform® Atlas† | Chi-square test, p-value | OR | 95% CI | GEE regression model, p-value‡ |
|---|---|---|---|---|---|
| All-cause inpatient readmission | |||||
| 7.4% | 15.6% | 0.03 | 0.45 | 0.20–0.98 | 0.04 |
| UIA related inpatient readmission‡ | |||||
| 2.7% | 6.5% | 0.11 | 0.39 | 0.12–1.26 | 0.12 |
| T-test, p-value | ER | 95% CI | GEE regression model, p-value‡ | ||
| Index admission cost | |||||
| $39,729 ($20,785) | $44,650 ($27,711) | 0.31 | 0.91 | 0.76–1.09 | 0.29 |
| Index supply cost | |||||
| $20,442 ($12,243) | $27,561 ($20,083) | 0.006 | 0.74 | 0.61–0.90 | 0.002 |
†
Rates or costs of weighted cohort.
‡
UIA-related readmission was defined as hospitalization with a primary diagnosis of UIA.
Bold p-values indicate a significant difference.
Benjamini–Hochberg (BH) critical values were: 0.025 for index supply cost; 0.05 for all-cause readmissions; 0.075 for UIA related readmissions; and 0.100 for index admission cost. As such, the results after BH correction remained consistent and indicated significant differences for all-cause inpatient readmissions and index supply cost.
ER: Exponential ratio; OR: Odds ratio; UIA: Unruptured intracranial aneurysm; CI: Confidence interval.
Discussion
In this retrospective cohort study of patients with UIA who underwent stent-assisted endovascular coiling, those treated with the ENTERPRISE 2 stent were 55% less likely to have all-cause inpatient readmission in the 180 days following treatment compared with patients treated with Neuroform Atlas. Further, the use of ENTERPRISE 2 stent was associated with cost savings, as reflected in the significantly lower index supply cost associated with its use versus Neuroform Atlas. No significant difference in other study outcomes were observed between the two cohorts. These findings may have important implications for healthcare utilization and cost when choosing a device for endovascular treatment in patients with UIA.
Though not directly comparable (due to the difference in device generations studied), the results of our investigation are consistent with those of a recent real-world cohort study that found a significant reduction by 28–38% in all-cause, cardiovascular and UIA related readmission, along with a trend toward lower cost among patients who underwent treatment with ENTERPRISE compared with Neuroform stent [19]. Our results may be attributed to the higher physical strength, strut tension strength, compression strength, circumferential radial force and visibility of ENTERPRISE 2 compared with Neuroform Atlas stent [31,32].
Compared with ENTERPRISE 1, the ENTERPRISE 2 stent introduced several design changes such as improved radiopacity with platinum and tungsten markers in the hypotubing, an increased diameter of 0.5 mm, increased efficiency of prepping by adding flushing holes in the introducer, improved robustness of the delivery wire, minimized kink ratio and increased outward force. Improved radiopacity in ENTERPRISE 2’s hypotubing enhances visibility compared with its earlier generation. Optimal visibility enables precise navigation and stent placement and has been associated with lower rates of procedure related complications such as in-stent thrombosis [27], which may be related to lower index supply cost by eliminating the need for management with additional stents or therapy such as thrombectomy, angioplasty or antithrombotic agents.
The minimized kink ratio and increased outward force in ENTERPRISE 2 enhances flexibility, allowing the outer curve to elongate and the inner curve to compress. These modifications may lead to better wall apposition [27] and a smaller gap between the stent and vessel wall [25] compared with ENTERPRISE 1. Apposition is critical for achieving optimal occlusion without coil herniation and in minimizing the potential for thromboembolic complications [33]. Altogether, the improved features introduced in ENTERPRISE 2 may potentially be associated with cost savings through more efficient and accurate procedures and minimizing the need for repeated attempts, and potentially reducing procedure time. Indeed, shorter operation times have been observed when using ENTERPRISE 2 compared with its earlier generation [27].
Although UIA related inpatient readmission was not significantly different between groups, examination of the GEE results suggested a trend favoring lower UIA related inpatient readmission in patients treated with ENTERPRISE 2 versus Neuroform Atlas (OR: 0.39, 95% CI: 0.12–1.26). Additionally, further investigation revealed that around 60–65% of all-cause readmission were aneurysm-related in both study cohorts. Taken together, it is assumed that the design advancements made to ENTERPRISE 2 in terms of improved visibility, navigation precision, stent placement and procedural efficiency could potentially have contributed to the reduced rate of all-cause readmission as observed in the current study among patients treated with ENTERPRISE 2 stent compared with Neuroform Atlas stent.
Limitations
The current study has a few limitations. First, in the PHD, a readmission can only be assessed if the patient were to return to the same hospital. If a patient undergoes readmission in another hospital (other than the one in which they had index procedure), then that readmission cannot be assessed. As such, our rate of readmission may have been an underestimate of the true rate of readmission; however, this limitation is likely to cause non-differential bias and not influence the directionality of our results. Second, the device search strategy was based on a combination of the device name and catalog identifiers. This is a reasonable approach for device identification as unique device identifiers are not universally adopted and listed; however, this may have led to device misidentification. Third, hospitals in the PHD are not federally funded and are based in the US, which may limit the generalizability of our findings. Additionally, the data we collected lacked specificity of diagnosis and procedural codes which prevented us from identifying patients being treated specifically for wide-neck aneurysms or other clinical details about aneurysm-specific features including the precise location, size or neck width of the aneurysm, which could influence both device selection and study outcomes. Finally, data on physician experience level was not available, which could potentially impact patient outcomes and cost.
Conclusion
To the best of our knowledge, this is the first retrospective database study to compare outcomes among patients with UIA who underwent stent-assisted endovascular coiling using ENTERPRISE 2 versus Neuroform Atlas. Study results showed that treatment with ENTERPRISE 2 may potentially be associated with a significant decrease in all-cause inpatient readmission in the 180-day period following treatment, and a significantly reduced index supply cost compared with treatment with Neuroform Atlas. These results should be interpreted in light of limitations typically associated with the use of secondary observational data sources including potential device misclassification, incomplete readmission assessment, and limited generalizability. As the incidence of UIA increases, it is important to compare the impact of different devices on patient outcomes and cost. Our findings may help guide clinical decision-making that could improve patient outcomes and reduce cost for the management of UIA.
Summary points
•
This is a retrospective cohort study assessing admission costs and 180-day inpatient hospital readmissions post stent-assisted endovascular coiling using ENTERPRISE® 2 versus Neuroform® Atlas for the treatment of unruptured intracranial aneurysm.
•
A multihospital nationwide database (PHD) was used for study purposes.
•
After propensity weighting to balance the study cohorts on underlying covariates, results showed a 55% lower risk of 180 day all-cause inpatient readmissions and 26% lower supply cost during the admission for coiling procedure for the ENTERPRISE 2 stent group versus Neuroform Atlas stent group.
•
No statistically significant differences in unruptured intracranial aneurysm related inpatient readmissions and total admission cost were observed between the two groups.
•
Study results highlight lower costs and better outcomes associated with the use of ENTERPRISE 2 stent, which may help guide clinical decision making in stent selection.
Author contributions
RD Leacy, R Khanna, E Kottenmeier, Y Rong: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing – original draft, review and editing.
Acknowledgments
Writing and editorial support were provided by J Touchette and JO Oltmanns of Superior Medical Experts.
Financial disclosure
This work was supported by CERENOVUS, a Johnson & Johnson Company.
Competing interests disclosure
R DeLeacy has received consulting fees and participated on a scientific advisory board for CERENOVUS, and served as the secretary for the Society of Neurointerventional Surgery (2022–2023). R Khanna, E Kottenmeier and Y Rong are employed by Johnson & Johnson. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing and editorial support were provided by Superior Medical Experts.
Ethical conduct of research
The use of PINC AI Healthcare Database was reviewed by the New England Institutional Review Board and was determined to be exempt from broad Institutional Review Board approval, as this study does not involve human subjects’ research. Confidentiality of data subject records were maintained at all times. All study reports contained aggregate data only and did not identify individual data subjects or physicians.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary figure.docx)
- Download
- 37.30 KB
References
Papers of special note have been highlighted as: • of interest
1.
Korja M, Lehto H, Juvela S. Lifelong rupture risk of intracranial aneurysms depends on risk factors: a prospective Finnish cohort study. Stroke 45(7), 1958–1963 (2014).
2.
Wiebers DO, Whisnant JP, Huston J et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 362(9378), 103–110 (2003).
3.
Brown RD. Unruptured intracranial aneurysms. Semin. Neurol. 30(5), 537–544 (2010).
4.
Nieuwkamp DJ, Setz LE, Algra A, Linn FH, de Rooij NK, Rinkel GJ. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol. 8(7), 635–642 (2009).
5.
Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 10(7), 626–636 (2011).
6.
Smith GA, Dagostino P, Maltenfort MG, Dumont AS, Ratliff JK. Geographic variation and regional trends in adoption of endovascular techniques for cerebral aneurysms. J. Neurosurg. 114(6), 1768–1777 (2011).
7.
Hwang JS, Hyun MK, Lee HJ et al. Endovascular coiling versus neurosurgical clipping in patients with unruptured intracranial aneurysm: a systematic review. BMC Neurol. 12, 99 (2012).
8.
Brinjikji W, Rabinstein AA, Lanzino G, Kallmes DF, Cloft HJ. Patient outcomes are better for unruptured cerebral aneurysms treated at centers that preferentially treat with endovascular coiling: a study of the national inpatient sample 2001–2007. Am. J. Neuroradiol. 32(6), 1065–1070 (2011).
9.
Li L, Xu GQ, Gao HL et al. Endovascular treatment of intracranial vertebral artery unruptured dissecting aneurysms: comparison of flow diversion and stent-assisted coiling or stenting alone. Front. Neurol. 13, 919866 (2022).
10.
Lo YL, Bih ZL, Yu YH, Li MC, Chen HM, Wu SY. Long-term medical resource consumption between surgical clipping and endovascular coiling for aneurysmal subarachnoid hemorrhage: a propensity score–matched, nationwide, population-based cohort study. Int. J. Environ. Res. Public Health 18(11), 5989 (2021).
11.
el-Chalouhi N, Jabbour PM, Tjoumakaris SI et al. Treatment of large and giant intracranial aneurysms: cost comparison of flow diversion and traditional embolization strategies. World Neurosurg. 82(5), 696–701 (2014).
12.
Bairstow P, Dodgson A, Linto J, Khangure M. Comparison of cost and outcome of endovascular and neurosurgical procedures in the treatment of ruptured intracranial aneurysms. Australas. Radiol. 46(3), 249–251 (2002).
13.
Maud A, Lakshminarayan K, Suri MF, Vazquez G, Lanzino G, Qureshi AI. Cost-effectiveness analysis of endovascular versus neurosurgical treatment for ruptured intracranial aneurysms in the United States. J. Neurosurg. 110(5), 880–886 (2009).
14.
Armoiry X, Turjman F, Hartmann D et al. Endovascular treatment of intracranial aneurysms with the WEB device: a systematic review of clinical outcomes. Am. J. Neuroradiol. 37(5), 868–872 (2016).
15.
Hendricks BK, Yoon JS, Yaeger K et al. Wide-neck aneurysms: systematic review of the neurosurgical literature with a focus on definition and clinical implications. J. Neurosurg. 133(1), 159–165 (2019).
16.
Park HS, Kwon SC, Park ES, Park JB, Kim MS. A new definition for wide-necked cerebral aneurysms. J. Cerebrovasc. Endovasc. Neurosurg. 21(4), 193–198 (2019).
17.
Kadkhodayan Y, Rhodes N, Blackburn S, Derdeyn CP, Cross DT, Moran CJ. Comparison of Enterprise with Neuroform stent-assisted coiling of intracranial aneurysms. Am. J. Roentgenol. 200(4), 872–878 (2013).
• This study highlights that ENTERPRISE® stent use was associated with statistically significant superior deployment rate and occlusion rate as compared with Neuroform® stent.
18.
Hwang S-K, Hwang G, Bang JS, Oh CW, Kwon OK. Endovascular Enterprise stent-assisted coil embolization for wide-necked unruptured intracranial aneurysms. J. Clin. Neurosci. 20(9), 1276–1279 (2013).
19.
Leacy R, Kottenmeier E, Lee SH, Khanna R, Spiotta AM. Endovascular treatment with the Enterprise stent versus the Neuroform or low-profile visualized intraluminal support stent for unruptured aneurysms. J. Comp. Eff. Res. 10(4), 295–305 (2021).
• This retrospective cohort study suggests that ENTERPRISE stent use was associated with significantly lower risk of readmissions versus other stent including Neuroform stent.
20.
Wang J, Vargas J, Spiotta A et al. Stent-assisted coiling of cerebral aneurysms: a single-center clinical and angiographic analysis. J. Neurointerv. Surg. 10(7), 687–692 (2018).
21.
Gentric JC, Biondi A, Piotin M et al. Safety and efficacy of neuroform for treatment of intracranial aneurysms: a prospective, consecutive, French multicentric study. Am. J. Neuroradiol. 34(6), 1203–1208 (2013).
22.
Dong L, Wang J, Chen X et al. Stent-assisted coiling using the Neuroform Atlas stent for treatment of aneurysms that recur after coil embolization. Front. Neurol. 13, 967942 (2022).
23.
Caragliano AA, Papa R, Pitrone A et al. The low-profile Neuroform Atlas stent in the treatment of wide-necked intracranial aneurysms – immediate and midterm results: an Italian multicenter registry. J. Neuroradiol. 47(6), 421–427 (2020).
24.
King B, Vaziri S, Singla A, Fargen KM, Mocco J. Clinical and angiographic outcomes after stent-assisted coiling of cerebral aneurysms with Enterprise and Neuroform stents: a comparative analysis of the literature. J. Neurointerv. Surg. 7(12), 905–909 (2015).
• This literature review demonstrates that ENTERPRISE use is associated with lower rates of hardware failure at deployment, peri-procedural intracranial hemorrhage and recanalization and higher rates of complete occlusion as compared to Neuroform stent.
25.
Kono K, Terada T. In vitro experiments of vessel wall apposition between the Enterprise and Enterprise 2 stents for treatment of cerebral aneurysms. Acta Neurochir. (Wien) 158(2), 241–245 (2016).
26.
Chihara H, Ishii A, Kikuchi T, Ikeda H, Arai D, Miyamoto S. Deployment technique that takes advantage of the characteristics of Enterprise VRD2: an in vitro study. J. Neurointerv. Surg. 9(10), 969–973 (2017).
27.
Li Z, Xuan J, Fang X et al. Comparison of Enterprise stent 2 with 1 in assisting coiling of ruptured aneurysms: a real-world study. J. Comp. Eff. Res. 11(12), 879–887 (2022).
28.
Jankowitz BT, Hanel R, Jadhav AP et al. Neuroform Atlas Stent System for the treatment of intracranial aneurysm: primary results of the Atlas Humanitarian Device Exemption cohort. J. Neurointerv. Surg. 11(8), 801–806 (2019).
29.
Daou BJ, Palmateer G, Linzey JR et al. Stent-assisted coiling of cerebral aneurysms: head to head comparison between the Neuroform Atlas and EZ stents. Interv. Neuroradiol. 27(3), 353–361 (2021).
30.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
31.
Iwakami T, Fujii N, Son J. Comparison of the physical characteristics of support stents for cerebral aneurysm embolization. J. Neuroendovasc. Ther. 15(12), 778–786 (2021).
32.
Kato N, Yuki I, Otani K et al. Flow Diverter apposition in patients with large or giant intracranial aneurysms evaluated on three-dimensional fusion images acquired by high-resolution cone-beam computed tomography and digital subtraction angiography. World Neurosurg. 147, e388–e395 (2021).
33.
Heller R, Calnan DR, Lanfranchi M, Madan N, Malek AM. Incomplete stent apposition in Enterprise stent-mediated coiling of aneurysms: persistence over time and risk of delayed ischemic events. J. Neurosurg. 118(5), 1014–1022 (2013).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 13 June 2025
Accepted: 18 July 2025
Published online: 1 August 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Hospital readmission among patients with unruptured intracranial aneurysms undergoing stent-assisted endovascular coiling using the ENTERPRISE® 2 stent versus Neuroform® Atlas stent. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0096
Export citation
Select the citation format you wish to export for this article or chapter.