Clinical outcomes of retrievable inferior vena cava filters for venous thromboembolic diseases
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To identify literature evidence assessing retrievable inferior vena cava filter (rIVCF) for venous thromboembolic diseases. Methods: A systematic literature search was conducted to identify relevant references from the mainstay English and Chinese bibliographic databases (search period: January 2003 to October 2019). Results: 80 original studies with 11,413 patients were included in this review. The success rates of deploying the six types of rIVCFs ranged from 98.4 to 100.0%. Denali had the highest retrieval success rate (95.4–97.6%). The incidence rates of fracture and perforation associated with retrieving the six rIVCFs were less than 2%. Conclusion: The approved rIVCF had comparable clinical profiles, except that Denali was easier to be retrieved than other rIVCF.
The early inferior vena cava filters (IVCF) were usually implanted permanently to prevent life-threatening pulmonary embolism (PE) in the patients with venous thromboembolic diseases (VTD) [1,2]. Because the permanent IVCF (pIVCF) were not designed for retrieving from a percutaneous approach, it was challengeable to retrieve pIVCF and the risk of deep vein thrombosis (DVT) increased with the longer indwell time of these permanent IVCF. The landmark PREPIC trial confirmed the increased risk of recurrent DVT associated with pIVCF plus anticoagulation in the comparison with anticoagulation alone [3]. Thus, retrievable IVCF (rIVCF) were developed to address this limitation of pIVCF [4]. Different from pIVCF, the developed rIVCF keep the filter structure for PE prevention and also add the hook structure to facilitate retrieving filter [5].
Günther Tulip filter was the first rIVCF approved by US FDA in 2003. Since then, several types of retrievable IVCF have been developed to further improve operation, filtration efficiency, mechanical stability, and retrievability period [6]. However, the clinical outcomes associated with the approved rIVCFs are rarely compared in randomized trial settings. Thus, this review aimed to identify the existing literature evidence to differentiate the approved rIVCF regarding PE prevention, deploying and retrieving success rates and the complications associated with deploying, indwelling and retrieving rIVCF.
Methods
IVCF was introduced in China in 1995 and over 40,000 patients in China receive the treatments with IVCF per year. IVCF might be well studied in China and the evidence published in Chinese should be an important source for this systematic review. Because the authors of this study have the Chinese language capacity, this study selected the three English bibliographic databases (MEDLINE, EMBASE, Web of Science) and also the three mainstay Chinese bibliographic databases (China National Knowledge Infrastructure [CNKI], WANFANG, and VIP) to conduct literature search from 2003, the year for the approval of first rIVCF in USA (2003), to the date (31 October 2019) when this study started. The literature search strategies were developed by combining the keywords for rIVCF (‘retrievable IVCF’, ‘retrievable inferior vena cava filter’, or ‘rIVCF’) and VTD (‘venous thromboembolic diseases’ or ‘VTD’). The initially identified references from each database were pooled to remove the duplicated references. The titles and abstracts of the identified references were screened to exclude the irrelevant references. The full publications of the identified references from screening were further reviewed for their eligibility using the defined inclusion and exclusion criteria. This review included any original studies, including observational studies, phase I trial, phase II trial, and randomized clinical trials, reporting PE and outcomes (including but not limited to success rate and complications) associated with deploying indwelling, and retrieving rIVCF in patients with VTD or high risk for VTD. The publication languages of the included studies were limited to English and Chinese. This review excluded studies with unspecified IVCF type, case study, non-human study, editorial publications, guidelines, review, and the study with inadequate information for data extraction. The full publication of the original studies meeting both inclusion and exclusion were reviewed to extract the following information. The extracted study information included patient characteristics, rIVCF information, and clinical outcomes were extracted by study groups. The extracted clinical outcomes related to rIVCF deployment (deployment success rate, deployment operation time, deployment fluoroscopy time, and incidences of complications associated with deployment), indwelling rIVCF (incidences of symptomatic PE and complications during rIVCF indwell time), and retrieving rIVCF (retrieving rate, advanced technology utilization rate for retrieving IVCF, and complications associated with retrieving rIVCF). This study used Jadad score [7] to assess the quality of included randomized clinical trials and the Newcastle Ottawa Scale [8] to assess the quality of the included observational studies. The literature search, study eligibility assessment, study quality assessment and data extraction were conducted independently by two research associates for quality control. Any disagreements between the two research associates were resolved by consulting with the project lead.
The extracted outcome measures from the included studies were used to categorize the included studies into three groups to assess clinical outcomes associated with deploying, indwelling and retrieving rIVCF, respectively. The extracted information was synthesized using a single-arm meta-analysis. Continuity correction (0.5 event) was used in the meta-analysis if the included studies reported 0 or all events for the measured outcome [9]. Plogit function was used to transform proportion in the meta-analysis. This study also used the parameter testing method, including one-way ANOVA for continuous data and chi-square tests for categorical data, to compare the pooled estimations of patient characteristics (age, gender and disease indications), rIVCF deployment and retrieval approaches, and clinical outcomes associated with the rIVCF types. This study performed the data analyses using statistical software R (version 4.0.2). The statistical significance in the parameter tests was defined as a two-sided p-value less than 0.05.
Results
The literature search identified 4602 references from the included three English bibliographic databases and 2632 references from the included three Chinese bibliographic databases. After reviewing the titles, abstracts and full publications associated with these references, this study included 80 references (70 English references and ten Chinese references) reported clinical outcomes associated with ALN [10–19], Celect [18–45], Crux [46], Denali [19,44,45,47–53], Günther Tulip [17–19,29,38–42,53–88] and Option [19,43,50,51,53,75,86–89]. The literature search flow charts for English and Chinese bibliographic databases are illustrated in Figure 1.
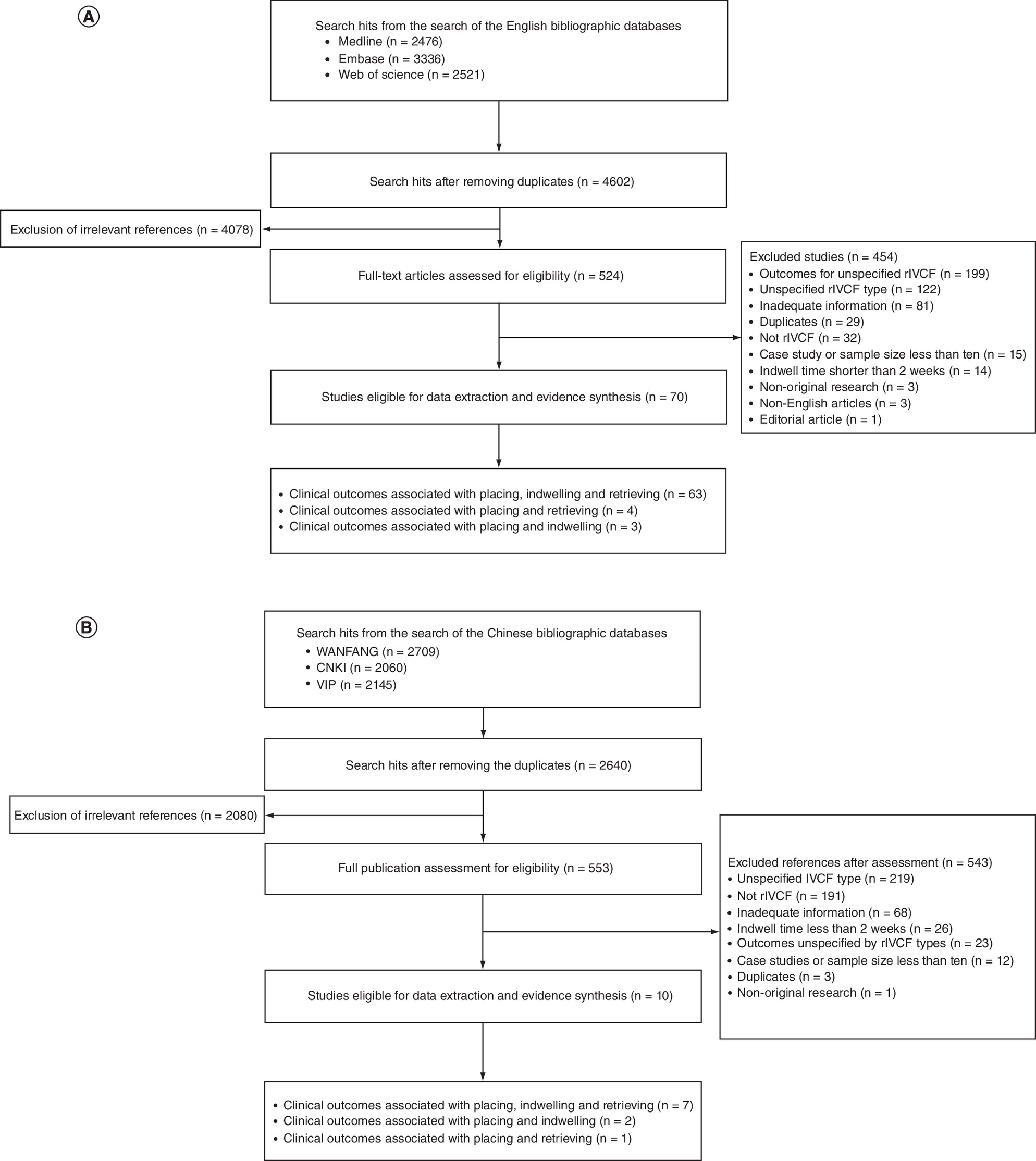
Figure 1. The flowchart of the literature search.
(A) English bibliographic databases; (B) Chinese bibliographic databases.
IVCF: Inferior vena cava filters.
Pooled patient characteristics from the included references
This review pooled the reported patient characteristics from the included studies using the same type of rIVCF. Based on the pooled patient characteristics by the type of rIVCF, the patients receiving the six types of rIVCF had comparable age (ranging from 51.9 to 64.9 years, p = 0.992) but significantly different gender distribution (male gender proportion ranging from 41.6 to 58.4%, p < 0.001). The underlying diseases associated with these patients were also significantly different from the rIVCF types. Based on the summarized distributions of patient indications, ALN, Celect and Denali were mainly used in patients with DVT and/or PE, Crux and Günther Tulip were mainly used in patients with high thromboembolic risk surgery, and Option was mainly used in patients with an active or high risk of bleeding. The profiles of approaches used to deploy and retrieve the six types of rIVCF were also significantly different. The femoral vein was the main insertion approach for Celect and Denali, and jugular vein was the main insertion approach for ALN, Günther Tulip and Option. The included studies didn't provide sufficient information regarding the insertion approaches used for Crux. The right jugular vein was the main retrieving approach for ALN, Celect, Denali, Günther Tulip and Option. Crux was mainly retrieved from the femoral vein. The indwell time associated with the six types of rIVCF ranged from 4.6 to 17.2 months (p = 0.03). The patient characteristics and the profiles of deploying and retrieving approaches associated with the six types of rIVCF are summarized in Table 1.
| Patient characteristics | Denali | Celect | Option | Crux | ALN | Günther Tulip | p-value |
|---|---|---|---|---|---|---|---|
| Sample size | 693 | 1,685 | 429 | 125 | 722 | 2280 | |
| Age (years) | 57.8 (55.2–60.4) | 56.3 (49.6–63.1) | 60.7 (55.9–65.5) | 59.1 (56.1–62.1) | 64.9 (57.7–72.2) | 51.9 (46.8–57.1) | 0.992 |
| Male gender (%) | 57.1% (52.4–61.7%) | 50.4% (47.2–53.7%) | 58.4% (49.6–66.7%) | 58.4% (49.6–66.7%) | 42.0% (31.9–52.8%) | 46.6% (42.0–51.3%) | <0.001 |
| Patient indications | |||||||
| Active or high risk of bleeding | 2.3% | 0.2% | 20.5% | 0.0% | 3.5% | 2.6% | <0.001 |
| Bariatric surgery | 0.0% | 0.6% | 0.0% | 4.8% | 0.0% | 3.8% | <0.001 |
| Burn | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.1% | 0.241 |
| Cancer | 0.0% | 0.1% | 0.0% | 4.0% | 1.6% | 0.1% | <0.001 |
| Cardiopulmonary disease | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.2% | 0.005 |
| DVT | 11.2% | 13.8% | 1.0% | 15.2% | 0.0% | 12.2% | <0.001 |
| DVT and bone fracture | 15.6% | 4.3% | 0.0% | 0.0% | 0.0% | 0.0% | <0.001 |
| DVT and/or PE | 23.6% | 10.1% | 13.7% | 0.0% | 25.7% | 15.3% | <0.001 |
| Free-floating iliocaval thrombus | 0.0% | 0.5% | 0.8% | 0.0% | 9.3% | 0.3% | <0.001 |
| High thromboembolic risk surgery | 1.5% | 1.2% | 13.2% | 31.2% | 1.4% | 31.1% | <0.001 |
| High thromboembolic risk trauma | 0.2% | 4.1% | 0.0% | 14.4% | 1.1% | 0.1% | <0.001 |
| ICU patients with high thromboembolic risk | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.5% | <0.001 |
| Intracranial disease | 0.0% | 0.1% | 0.0% | 0.0% | 0.0% | 2.7% | <0.001 |
| Long-bone and pelvic bone fractures with VTE | 0.0% | 0.8% | 0.0% | 0.0% | 0.0% | 0.0% | <0.001 |
| Non-gastric bypass surgery | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.3% | 0.001 |
| PE | 2.3% | 5.8% | 0.4% | 8.8% | 0.0% | 3.6% | <0.001 |
| Thrombocytopenia | 0.2% | 0.0% | 2.1% | 0.0% | 0.0% | 0.2% | <0.001 |
| Transcatheter therapy | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.1% | 0.241 |
| VTE | 1.0% | 0.0% | 2.9% | 0.0% | 20.9% | 2.7% | <0.001 |
| Unclarified | 42.0% | 58.4% | 45.5% | 21.6% | 36.5% | 24.1% | <0.001 |
| Insertion approach | |||||||
| Unspecified jugular vein | 0.7% | 4.2% | 0.0% | 0.0% | 9.3% | 14.2% | <0.001 |
| Left jugular vein | 0.2% | 0.0% | 0.4% | 0.0% | 0.0% | 0.1% | 0.002 |
| Right jugular vein | 13.4% | 0.7% | 20.5% | 0.0% | 5.2% | 20.3% | <0.001 |
| Unspecified femoral vein | 26.3% | 1.2% | 0.0% | 0.0% | 11.8% | 7.7% | <0.001 |
| Left femoral vein | 4.6% | 2.1% | 1.4% | 0.0% | 0.0% | 2.9% | <0.001 |
| Right femoral vein | 7.5% | 5.0% | 10.0% | 0.0% | 0.0% | 17.5% | <0.001 |
| Non-jugular non-femoral vein | 8.3% | 0.0% | 0.0% | 0.0% | 10.7% | 0.1% | <0.001 |
| Unspecified vein | 38.9% | 86.9% | 67.6% | 100.0% | 63.1% | 37.1% | <0.001 |
| Indwell time (months) | 5.8 | 5.4 | 6.7 | 4.6 | 17.2 | 9.1 | 0.030 |
| Retrieving approach | |||||||
| Jugular vein | 29.4% | 9.2% | 0.0% | 29.6% | 2.7% | 5.3% | <0.001 |
| Left jugular vein | 0.0% | 0.1% | 0.0% | 0.0% | 0.0% | 0.3% | 0.396 |
| Right jugular vein | 37.4% | 18.5% | 48.4% | 0.0% | 11.6% | 31.8% | <0.001 |
| Femoral vein | 0.0% | 0.0% | 0.0% | 70.4% | 0.0% | 0.0% | <0.001 |
| Other | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.1% | 0.597 |
| Unclarified | 33.2% | 72.2% | 51.6% | 0.0% | 85.7% | 62.5% | <0.001 |
Statistical significance: p < 0.05.
DVT: Deep vein thrombosis; PE: Pulmonary embolism; rIVCF: Retrievable inferior vena cava filter; VTE: Venous thromboembolism.
Clinical outcomes associated with deploying the six types of rIVCF
The pooled estimations of the deployment success rates associated with the six types of rIVCF were highly comparable by ranging from 98.4 to 100.0%. The complication profiles associated with deploying the six types of rIVCF were slightly different. The included studies did not report any incidence of dislocation associated with deploying Denali, Celect and Option. However, the incidence of dislocation was reported for deploying ALN (0.4%, 95% CI: 0.0–5.5%), Crux (0.8%, 95% CI: 0.1–4.4%) and Günther Tulip (0.1%, 95% CI: 0.0–0.8%). Four of the six types rIVCF (ALN: 1.1%, 95% CI: 0.2–6.7%; Celect: 0.3%, 95% CI: 0.0–3.9%; Günther Tulip: 0.2%, 95% CI: 0.0–0.6%; Option: 0.1%, 95% CI: 0.0–32.7%) were associated with the incidence of tilt, a common complication associated with deploying rIVCF. The perforation was only reported for deploying Denali (0.9%, 95% CI: 0.3–2.4%) and Günther Tulip (0.1%, 95% CI: 0.0–0.6%) in the included studies. Three studies reported comparable operation time associated with three rIVCF (22.0 min for Crux; 17.8 min for Denali; 23.6 min for Option) and fluoroscopy time associated with two rIVCF (3.6 min for Denali; 3.7 min for Option).
Clinical outcomes associated with indwelling rIVCF
75 out of the included 80 studies reported the incidences of symptomatic PE and complications related to indwelling rIVCF. The included studies did not report any incidence of symptomatic PE associated with indwelling Denali, irrespective of the indwelling time. The incidence rates of symptomatic PE associated with the other five types of rIVCF over the classified indwell time ranged from 0.1–2.4% (Figure 2). Of the reported complications associated with indwelling the six types, tilt and perforation were the main complications associated with indwelling rIVCF. Indwelling Celect was associated with the highest incidence rate of tilt over 2 weeks to 1 month indwell time (31.9%, 95% CI: 24.8–40.0%), 1–3 months indwell time (4.2%, 95% CI: 1.0–16.0%) and 3–6 months indwell time (2.1%, 95% CI: 0.5–7.9%). Indwelling ALN was associated with the highest incidence rate of tilt over 6 to 12 months indwell time (2.9%, 95% CI: 0.1–46.0%) and 12 to 24 months indwell time (6.6%, 95% CI: 2.6–15.7%). Additionally, the pooled estimations of perforation rate associated with indwelling Celect was the highest in all classified indwell times, except 1–3 months in which Option was associated with the highest perforation rate (9.5%, 95% CI: 2.7–28.9%). Migration, fracture and IVC occlusion associated with indwelling the six types rIVCF were much less prevalent. The highest pooled incidence rate of migration was associated with Celect over 12–24 months indwell time (0.4%, 95% CI: 0.0–25.5%). The incidences of fracture and IVC occlusion were only reported for the indwelling with Celect, Günther Tulip and Option. The highest pooled estimations of the incidence rates for the two complications were 0.6% for fracture associated with indwelling Celect over 6–12 months and 0.7% for IVC occlusion associated with indwelling Option over 3–6 months. The pooled incidence rates of tilt and perforation associated with indwelling six types of rIVCF over different times are illustrated in Figure 3.

Figure 2. Pooled incidence rate of symptomatic pulmonary embolism associated with the six rIVCFs by indwell time periods.
IVCF: Inferior vena cava filters.

Figure 3. Pooled incidence rate of tilt and perforation associated with the six rIVCFs by indwell time periods.
(A) Pooled estimations for the tilt rate associated with indwelling six IVCF types. (B) Pooled estimations for the perforation rate associated with indwelling six IVCF types.
IVCF: Inferior vena cava filters.
Clinical outcomes associated with retrieving rIVCF
74 of the included 80 studies reported clinical outcomes associated with retrieving rIVCF. The pooled success rates of retrieving the six types of rIVCF through conventional techniques substantially varied from 75.6% to 98.4% (Figure 4). Retrieving Denali was associated with the highest success rate among the rIVCF types over the indwell time for 2 weeks to 1 month (95.4%, 95% CI: 89.5– 98.1%), 3–6 months (95.8%, 95% CI: 92.4–97.7%) and 6–12 months (97.6%, 95% CI: 93.1–99.2%). Retrieving Celect was associated with the highest advanced technique utilization rate to retrieve rIVCF over the indwell time for 1–3 months (2.3%, 95% CI: 0.4–12.0%) and Option had the highest advanced technique utilization rate to retrieve rIVCF over the indwell time for 3–6 months (15.5%, 95% CI: 11.7–20.2%). According to the reported operation time and fluoroscopic time associated with retrieving IVCF in the included studies, retrieving Denali was associated with the shortest operation time (23.1 min, 95% CI: 19.9–26.3 min) and shortest fluoroscopy time (1.1 min, 95% CI: 1.0–1.2 min). The complications associated with retrieving rIVCF were not common as the two reported complications, fracture and perforation, were only reported for retrieving Celect and Denali with pooled incidence rates less than 2%.
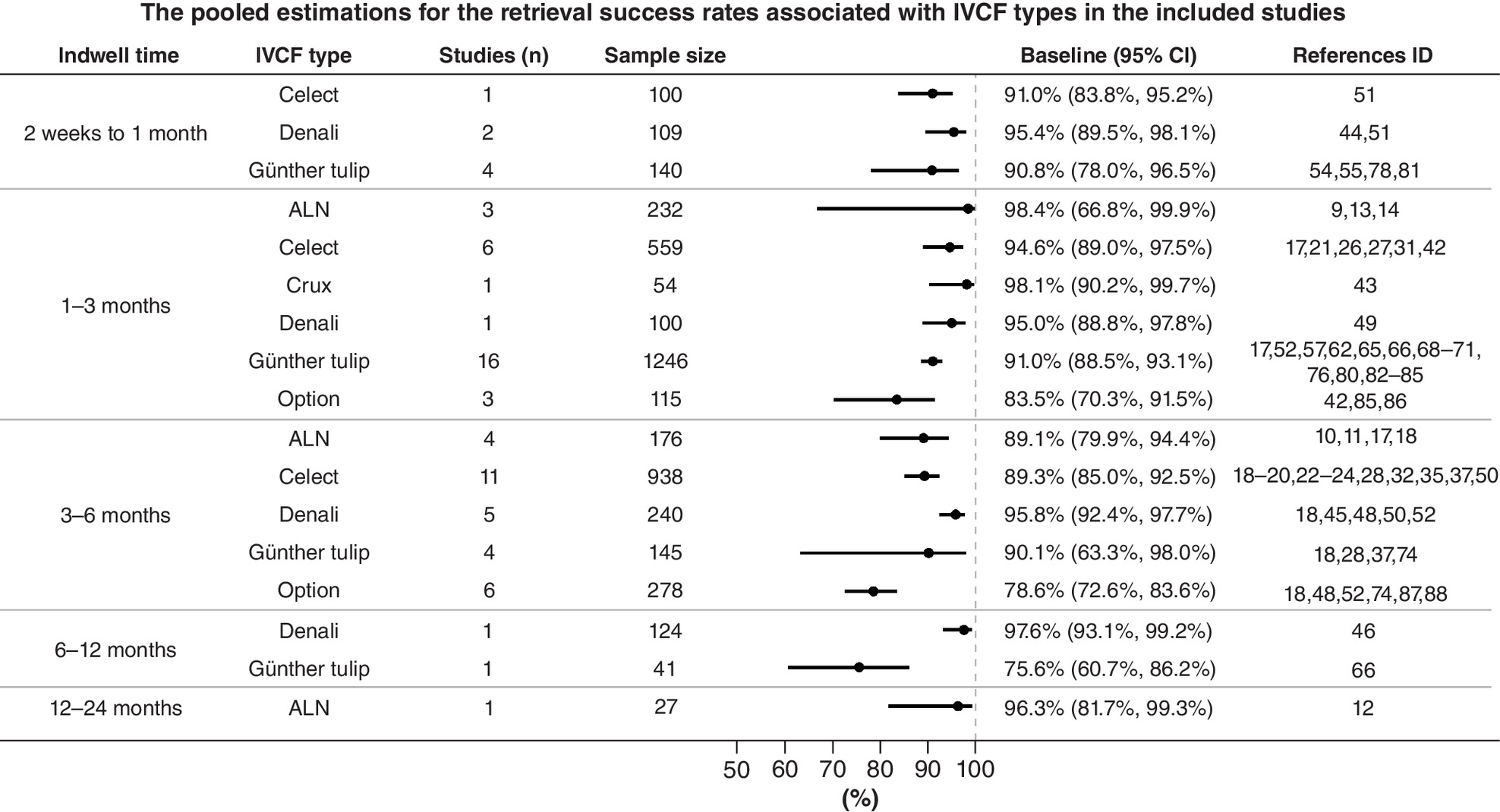
Figure 4. Pooled retrieving success rate associated with the six rIVCFs by indwell time periods.
IVCF: Inferior vena cava filters.
Discussion
To our knowledge, this study could be the most comprehensive literature review as it included the published English and Chinese studies since the first approved rIVCF by FDA in 2003. This review synthesized the identified evidence to comprehensively assess the clinical outcomes associated with deploying, indwelling and retrieving six common types of rIVCF in patients with a high risk of developing PE. Even though most of the included studies used the single-arm observational study design to evaluate rIVCF, the six types of rIVCF had the same indication that could substantially reduce the heterogeneity of patient characteristics across studies. The approaches used to deploy and retrieve these six types of rIVCF were also similar. The confounding effects associated with deployment and retrieving could be minimized. Thus, the pooled evidence based on many studies and a large sample size should be robust for validity and reliability. Since it is challenging to assess rIVCF in randomized trial settings, the pooled evidence in this review could be an alternative evidence source to support clinical decision making and policy making regarding the clinical utilization of rIVCF to control PE risk in patients with VTD.
Many included observational studies in this review provided a large body of real-world evidence to characterize the patients using rIVCF and the approaches used to deploy and retrieve rIVCF. The summarized evidence for patient demographics indicated that the patients receiving the six types of rIVCF had comparable age but significantly different male gender proportions. We believe that the surgeon didn't have a preference to select rIVCF type by patient gender but the skewed gender distribution associated with underline diseases could confound the gender distribution in the patients utilizing rIVCF. The pooled distribution of patient indications by rIVCF types indicated that Denali and Option were likely to be used more often in patients with bone fracture or active bleeding, which were usually related to trauma and occurred more often in males [90,91]. The other rIVCF types were used more often in patients with DVT, PE, or high thromboembolic risk surgery. Even though the six rIVCF were mainly used in the prophylactic patient groups, the differences in the distribution of patient indications could confound the patient characteristics and also the clinical outcomes. Based on the collected information for deploying and retrieving approaches, the six types of rIVCF were mainly deployed and retrieved through the jugular vein. Deploying and retrieving approaches should have limited confounding effects in the pooled evidence. However, the potential impact of gender on certain clinical outcomes, such as PE and complications associated with rIVCF over indwell time, should be taken into account because the risk of venous thrombosis could be doubled in male people above 60 years of age [92].
The pooled evidence in this review suggested that Denali was likely to be superior to the other five types of rIVCF in many aspects related to effects, operation and safety. The pooled evidence for the incidence of symptomatic PE associated with the six types of rIVCF in this review confirmed more effective embolic filtration associated with the two levels of the filter structure. Denali was the only rIVCF without any reported symptomatic PE over indwell time in the included studies. When compared with the other five types of rIVCF, the cranial and caudal anchors of Denali are located at the base of the six lower filter arms [93]. This structure could resist superior and inferior migration and further stabilize the filter by providing points for incorporation into the caval wall. Thus, the risk of tilt associated with Denali is minimized and the middle position of Denali in the caval could maximize the performance for embolic filtration [94]. Of the other five types rIVCF, ALN, Celect, and Günther Tulip have two levels filter. This explained why the pooled incidence rates of symptomatic PE associated with these three rIVCF were relatively lower than that for Option, which has one level filter [95]. Crux has an entirely different structure when compared with the other five types of rIVCF. Crux has two symmetric spiral wire forms connected at the ends with a web of expanded poly-tetrafluoroethylene (ePTFE) in the caudal portion, five tissue anchors, and a sinusoidal retrieval tail at each end [96]. Thus, Crux only has one level filter and the pooled incidence rate of symptomatic PE associated with Crux was comparable with those of the one level filter rIVCF in this review.
The pooled evidence in this review indicated that six types of rIVCF were associated with high and comparable deployment success rates. Additionally, the pooled complication rates of deployment associated with the six types of rIVCF were minimum and less than 1.6%. Thus, the differences in the structures of the six types of rIVCF were unlikely to impact the performance of rIVCF deployment. However, the pooled evidence related to the indwelling and retrieving rIVCF in this review suggested that the structures of these rIVCF had substantially impacted the complications related to rIVCF over indwell time and the performance of retrieving rIVCF. First, this review identified that Celect was associated with much higher rates of tilt and perforation than other types of rIVCF over indwell time. Different from other conical rIVCF, Celect was designed to have anchors on the primary filter legs (first level). The secondary legs of Celect don't have anchors to support fixation on the caval wall. The tilted Celect could further increase the risk of perforation through changing the allocation of the total forces on the primary strut [97]. Thus, the rIVCF with anchors on the two levels of filter legs could reduce the risk of tilt and further reduce the risk of perforation. The pooled evidence in this review confirmed this theory as the rIVCFs with this type of design, such as ALN and Denali, were associated with much lower pooled incidence rates for both tilt and perforation indeed. The pooled evidence for the retrieve rate, advanced technique utilization for retrieving rIVCF, and operation time and fluoroscopic time associated with retrieving the six types IVCF further confirmed that the rIVCF design mattered the retrieving performance. Of the assessed six types of rIVCF, only Crux does not have a conical design that could facilitate the rIVCF retrieving. However, the complications during indwell time, such as tilt and perforation, could substantially increase the difficulty in retrieving rIVCF. In addition, the cranial and caudal anchors of Denali are located at the base of the six lower filter arms. This structure can resist superior and inferior migration that are the main challenges for filter retrieving. That is why ALN and Denali could have much better performance, characterized by higher retrieve rate using normal techniques, lower advanced technique utilization rate than Celect, Günther Tulip and Option. Because the utilization of advanced technique for retrieving rIVCF could reduce the complications associated with retrieving the six rIVCF, the reported incidences of complications associated with the six rIVCF were not common and occurred less than 2% of the patients in the included studies. With this confounding effect associated with advanced technique, the utilization of advanced technique for retrieving rIVCF could be more appropriate outcome measure for assessment than the incidence of complications caused by retrieving. Thus, Denali were more attractive than other types of rIVCF by reducing radiation exposures, improving performance and outcomes associated with retrieving and saving health resources.
As a systematic literature review, this study identified several evidence gaps that should be considered in future research. Even though this review included enormous numbers of studies for evidence synthesis, most of the included studies (78 out of 80 studies) were observational studies and this review was unable to identify enough studies that could be used to conduct indirect comparisons across the six types rIVCF. Thus, the comparisons of the pooled outcomes associated with the six types of rIVCF were not adjusted. The reported differences in the pooled estimations associated with the six types of rIVCF should be further confirmed in future studies that could conduct adjusted analysis using individual patient-level data. This review stratified the included studies by indwell time for the pooled analysis of the incidence of complications. However, the analysis did not observe any trend indicating the relationship between the incidence of complications and indwell time. Instead, some pooled incidence of complications, such as tilt, was even higher in the group with the shortest indwell time. As most of the included studies were observational study, this result might reflect more attention to monitoring complications in the first month after the placement of rIVCF in real-world clinical practices. Another explanation was that the self-center design of the rIVCF could correct tilt over indwell time. Future studies longitudinally and regularly following up the patients for complications after the rIVCF placement are needed to clarify the association between the incidence of complications and indwell time. Additionally, this review had limited capacity of using the secondary data or information collected from the included studies to conduct subgroup analyses by patient indications, patient gender and rIVCF access sites, which could confound PE occurrence and the measured outcomes, including success rate and complications associated with deploying and retrieving rIVCF. Finally, the common limitations associated with retrospective study design could bias the assessment as well. For example, the complications could be under-reported due to incomplete information and lack of standard methods for outcome measurement. Thus, a prospective cohort study with a well-designed data collection and measurement methods could be a more suitable design to assess retrievable rIVCF in the future.
Conclusion
Based on 80 original studies, the pooled evidence in this comprehensive literature review indicated a high and comparable success rate of deploying rIVCF for PE prevention. However, the pooled evidence related to the indwelling and retrieving IVCF suggested that Denali caused fewer complications during indwell time and improved retrieving performance and efficiency, which were characterized by higher retrieve rate using normal techniques and shorter operation time. Since this review was unable to conduct the adjusted analysis to compare clinical outcomes associated with the rIVCF, future prospective cohort studies with a well-designed data collection approach are needed to further differentiate clinical utility of the assessed rICVF in this review.
•
Existing evidence indicated that deploying the six types of retrievable inferior vena cava filter (rIVCF) were associated with high and comparable success rate.
•
The pooled incidences of pulmonary embolism and complications associated with the approved rIVCF during indwell time were relatively low.
•
Denali had the highest success rate for retrieving among the six types of rIVCF in the market.
•
The difficulty in retrieving rIVCF would be the main concern for the utilization of rIVCF to prevent pulmonary embolism in patients with venous thromboembolic diseases.
Author contributions
J Liu and W Chen formulated the research idea and developed the study protocol. P Jiang, X Tian, W Jia and N Huang conducted literature search and data extraction from included literature. H Zhan conducted the study quality assessment and synthesized the extracted data under the guidance of W Chen. J Liu and W Chen drafted the manuscript. All authors have critically reviewed the manuscript and approved the submission of this manuscript.
Financial & competing interests disclosure
An unrestricted grant was provided by Becton, Dickinson and Company. H Zhan and W Chen are employed in a consulting firm which receives industry research funds for real-world studies and health economics research. N Huang is the employee of Becton, Dickinson and Company. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Kaufman JA, Kinney TB, Streiff MB et al. Guidelines for the use of retrievable and convertible vena cava filters: report from the Society of Interventional Radiology multidisciplinary consensus conference. Surg. Obes. Relat. Dis. 2(2), 200–212 (2006).
2.
Young T, Tang H, Hughes R. Vena caval filters for the prevention of pulmonary embolism. Cochrane Database Syst. Rev. 2, CD006212 (2010).
3.
Greenfield LJ. The PREPIC study group. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d'Embolie Pulmonaire par Interruption Cave) randomized study. Perspect. Vasc. Surg. Endovasc. Ther. 18(2), 187–188 (2006).
4.
Kaufman JA, Kinney TB, Streiff MB et al. Guidelines for the use of retrievable and convertible vena cava filters: report from the Society of Interventional Radiology multidisciplinary consensus conference. Surg. Obes. Relat. Dis. 2(2), 200–212 (2006).
5.
Ghatan CE, Ryu RK. Permanent versus retrievable inferior vena cava filters: rethinking the “one-filter-for-all” approach to mechanical thromboembolic prophylaxis. Semin. Intervent. Radiol. 33(2), 75–78 (2016).
6.
Al-Hakim R, Kee ST, Olinger K, Lee EW, Moriarty JM, McWilliams JP. Inferior vena cava filter retrieval: effectiveness and complications of routine and advanced techniques. J. Vasc. Interv. Radiol. 25(6), 933–940 (2014).
7.
Jadad AR, Moore RA, Carroll D et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control. Clin. Trials 17(1), 1–12 (1996).
8.
Peterson J, Welch V, Losos M, Tugwell PJ. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute, Canada, 1–2 (2011).
9.
Efthimiou O. Practical guide to the meta-analysis of rare events. Evid. Based Ment. Health 21(2), 72–76 (2018).
10.
Carrafiello G, Mangini M, Fontana F et al. Suprarenal inferior vena cava filter implantation. Radiol. Med. 117(7), 1190–1198 (2012).
11.
Caronno R, Piffaretti G, Tozzi M et al. Mid-term experience with the ALN retrievable inferior vena cava filter. Eur. J. Vasc. Endovasc. Surg. 32(5), 596–599 (2006).
12.
Imberti D, Bianchi M, Farina A, Siragusa S, Silingardi M, Ageno W. Clinical experience with retrievable vena cava filters: results of a prospective observational multicenter study. J. Thromb. Haemost. 3(7), 1370–1375 (2005).
13.
Laganà D, Carrafiello G, Lumia D et al. Removable vena cava filter: single-centre experience with a single device. Radiol. Med. 118(5), 816–825 (2013).
14.
Mismetti P, Rivron-Guillot K, Quenet S et al. A prospective long-term study of 220 patients with a retrievable vena cava filter for secondary prevention of venous thromboembolism. Chest 131(1), 223–229 (2007).
15.
Mismetti P, Laporte S, Pellerin O et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone on risk of recurrent pulmonary embolism: a randomized clinical trial. JAMA 313(16), 1627–1635 (2015).
16.
Pellerin O, di Primio M, Sanchez O, Meyer G, Sapoval M. Successful retrieval of 29 ALN inferior vena cava filters at a mean of 25.6 months after placement. J. Vasc. Interv. Radiol. 24(2), 284–288 (2013).
17.
Koizumi J, Hara T, Sekiguchi T et al. Multicenter investigation of the incidence of inferior vena cava filter fracture. Jpn J. Radiol. 36(11), 661–668 (2018).
18.
Lee MJ, Valenti D, de Gregorio MA, Minocha J, Rimon U, Pellerin O. The CIRSE Retrievable IVC Filter Registry: Retrieval Success Rates in Practice. Cardiovasc. Intervent. Radiol. 38(6), 1502–1507 (2015).
19.
Dowell JD, Wagner D, Elliott E, Yildiz VO, Pan X. Factors associated with advanced inferior vena cava filter removals: a single-center retrospective study of 203 patients over 7 years. Cardiovasc. Intervent. Radiol. 39(2), 218–226 (2016).
20.
Bos A, Van Ha T, van Beek D et al. Strut penetration: local complications, breakthrough pulmonary embolism, and retrieval failure in patients with Celect vena cava filters. J. Vasc. Interv. Radiol. 26(1), 101–106 (2015).
21.
Doody O, Given MF, Kavnoudias H, Street M, Thomson KR, Lyon SM. Initial experience in 115 patients with the retrievable Cook Celect vena cava filter. J. Med. Imaging Radiat. Oncol. 53(1), 64–68 (2009).
22.
Jinglei DU, Shiping YU, Xiuqin SU et al. The recyclability and safety of Celect retrievable vena cava filter. Chin. J. Radiol. 52(2), 135–139 (2018).
23.
Lyon SM, Riojas GE, Uberoi R et al. Short- and long-term retrievability of the Celect vena cava filter: results from a multi-institutional registry. J. Vasc. Interv. Radiol. 20(11), 1441–1448 (2009).
24.
Sangwaiya MJ, Marentis TC, Walker TG, Stecker M, Wicky ST, Kalva SP. Safety and effectiveness of the celect inferior vena cava filter: preliminary results. J. Vasc. Interv. Radiol. 20(9), 1188–1192 (2009).
25.
Zhou D, Spain J, Moon E, Mclennan G, Sands MJ, Wang W. Retrospective review of 120 celect inferior vena cava filter retrievals: experience at a single institution. J. Vasc. Interv. Radiol. 23(12), 1557–1563 (2012).
26.
Rajasekhar A, Lottenberg L, Lottenberg R et al. A pilot study on the randomization of inferior vena cava filter placement for venous thromboembolism prophylaxis in high-risk trauma patients. J. Trauma 71(2), 323–329 (2011).
27.
Tian X, Liu JL, Jia W. Clinical application of Celect retrievable filters for fracture combined with deep venous thrombosis. Chin. J. Vasc. Surg. 4, 230–234 (2014).
28.
Zhao BX, Gu JP, He X. The safety and effectiveness of Celect inferior vena cava filter evaluated by CT. Chin. J. Radiol. 8, 619–623 (2018).
29.
Rosenthal D, Kochupura PV, Wellons ED, Burkett AB, Methodius-Rayford WC. Günther Tulip and Celect IVC filters in multiple-trauma patients. J. Endovasc. Ther. 16(4), 494–499 (2009).
30.
Dowell JD, Castle JC, Schickel M et al. Celect inferior vena cava wall strut perforation begets additional strut perforation. J. Vasc. Interv. Radiol. 26(10), 1510–1518 (2015).
31.
Dowell JD, Castle JC, Spinner J, Black S. Role of inferior vena cava filters in transplant patients. Clin. Transplant. 31(2), e12865 (2017).
32.
Jiang P, Cheng ZY, Li JY. Effect of indwelling time of Celect filter on inferior vena cava penetration. Shandong Med. J. 20, 100–102 (2018).
33.
Lee BE, Van Allan RJ, Friedman ML, Lipshutz HG. Complications and retrieval characteristics of Celect Platinum inferior vena cava filters. J. Vasc. Surg. Venous Lymphat. Disord. 6(2), 163–172 (2018).
34.
Lee SY, Lee J. Is external compression on the IVC a risk factor for IVC filter abutment? A single center experience of 141 infrarenal celect filter insertions. Eur. J. Radiol. Open 5, 73–78 (2018).
35.
Son J, Bae M, Chung SW, Lee CW, Huh U, Song S. Should we remove the retrievable cook celect inferior vena cava filter? Eight years of experience at a single center. Korean J. Thorac. Cardiovasc. Surg. 50(6), 443–447 (2017).
36.
Wang W, Zhou D, Obuchowski N, Spain J, An T, Moon E. Fracture and migration of Celect inferior vena cava filters: a retrospective review of 741 consecutive implantations. J. Vasc. Interv. Radiol. 24(11), 1719–1722 (2013).
37.
Zhou D, Moon E, Bullen J, Sands M, Levitin A, Wang W. Penetration of Celect inferior vena cava filters: retrospective review of CT scans in 265 patients. AJR Am. J. Roentgenol. 202(3), 643–647 (2014).
38.
Swami U, Annunziata G, Fulger I. Experience with vena cava filters at a large community hospital and level-I trauma center: indications, complications, and compliance barriers. Clin. Appl. Thromb. Hemost. 20(5), 546–552 (2014).
39.
Durack JC, Westphalen AC, Kekulawela S et al. Perforation of the IVC: rule rather than exception after longer indwelling times for the Günther Tulip and Celect retrievable filters. Cardiovasc. Intervent. Radiol. 35(2), 299–308 (2012).
40.
Go MR, Keller-Biehl L, Starr JE. Penetration of the inferior vena cava and adjacent organs after filter placement is associated with retrievable filter type and length of time in place. J. Vasc. Surg. Venous Lymphat. Disord. 2(2), 174–178 (2014).
41.
McLoney ED, Krishnasamy VP, Castle JC, Yang X, Guy G. Complications of Celect, Günther tulip, and Greenfield inferior vena cava filters on CT follow-up: a single-institution experience. J. Vasc. Interv. Radiol. 24(11), 1723–1729 (2013).
42.
Laborda A, Kuo WT, Ioakeim I et al. Respiratory-induced haemodynamic changes: a contributing factor to IVC filter penetration. Cardiovasc. Intervent. Radiol. 38(5), 1192–1197 (2015).
43.
Ryu RK, Desai K, Karp J et al. A comparison of retrievability: Celect versus Option Filter. J. Vasc. Interv. Radiol. 26(6), 865–869 (2015).
44.
Bos AS, Tullius T, Patel M et al. Indwelling and retrieval complications of Denali and Celect infrarenal vena cava filters. J. Vasc. Interv. Radiol. 27(7), 1021–1026 (2016).
•• This is a control study comparing two rIVCF.
45.
Bae JH, Lee SY. Filter tilting and retrievability of the Celect and Denali inferior vena cava filters using propensity score-matching analysis. Eur. J. Radiol. Open 5, 153–158 (2018).
• This study reported adjusted comparisons of the outcomes between two rIVCF.
46.
Smouse HB, Mendes R, Bosiers M, Van Ha TG, Crabtree T. RETRIEVE Investigators. The RETRIEVE trial: safety and effectiveness of the retrievable crux vena cava filter. J. Vasc. Interv. Radiol. 24(5), 609–621 (2013).
• Reported both safety and effectiveness of retrievable inferior vena cava filter (rIVCF).
47.
Choi SJ, Lee SY, Ryeom HK et al. Femoral versus jugular access for Denali Vena Cava Filter placement: analysis of fluoroscopic time, filter tilt and retrieval outcomes. Clin. Imaging 52, 337–342 (2018).
48.
Reis SP, Kovoor J, Sutphin PD et al. Safety and effectiveness of the Denali Inferior vena cava filter: intermediate follow-up results. Vasc. Endovascular Surg. 50(6), 385–390 (2016).
• Reported both effectiveness and safety of Denali.
49.
Stavropoulos SW, Chen JX, Sing RF et al. Analysis of the final DENALI trial data: a prospective, multicenter study of the denali inferior vena cava filter. J. Vasc. Interv. Radiol. 27(10), 1531–1538 (2016).
• The prospective multicenter design and large sample size made the real-world evidence in this study more reliable and valid.
50.
Han K, Kim MD, Kim GM et al. Comparison of retrievability and indwelling complications of Celect and Denali infrarenal vena cava filters: a randomized, controlled trial. Cardiovasc. Intervent. Radiol. 44(10), 1536–1542 (2021).
•• This study was a randomized control trial.
51.
Dowell JD, Semaan D, Makary MS, Ryu J, Khayat M, Pan X. Retrieval characteristics of the Bard Denali and Argon Option inferior vena cava filters. J. Vasc. Surg. Venous Lymphat. Disord. 5(6), 800–804 (2017).
52.
Xie MY, Wang XG. Application of retrievable vena cava filter in patients with lower limb fractures complicated with deep venous thrombosis. Chin. J. Bases Clinics Gen. Surg. 26(3), 312–314 (2019).
53.
Ramaswamy RS, Jun E, van Beek D et al. Denali, Tulip, and Option inferior vena cava filter retrieval: a single center experience. Cardiovasc. Intervent. Radiol. 41(4), 572–577 (2018).
54.
Chen GP, Gu JP, He X. Clinical application of the Gunther Tulip inferior vena cavu filter. J. Med. Imaging 15, 867–869 (2005).
55.
de Gregorio MA, Gamboa P, Gimeno MJ et al. The Günther Tulip retrievable filter: prolonged temporary filtration by repositioning within the inferior vena cava. J. Vasc. Interv. Radiol. 14(10), 1259–1265 (2003).
56.
De Gregorio MA, Gamboa P, Bonilla DL et al. Retrieval of Gunther Tulip optional vena cava filters 30 days after implantation: a prospective clinical study. J. Vasc. Interv. Radiol. 17(11 Pt 1), 1781–1789 (2006).
57.
Ge B, Liu P. Inferior vena cava filter placement for prevention of pulmonary embolism: a report of 57 cases. Orthopedic J. Chin. 6, 1049–1050 (2012).
58.
Hoffer EK, Mueller RJ, Luciano MR, Lee NN, Michaels AT, Gemery JM. Safety and efficacy of the Gunther Tulip retrievable vena cava filter: midterm outcomes. Cardiovasc. Intervent. Radiol. 36(4), 998–1005 (2013).
59.
Hong D, Zhang XT. Comparison on the value of OptEase filter and Tulip filter in endovascular therapy of deep venous thrombosis. Chinese J. Interv. Imaging Ther. 8(3), 193–196 (2011).
60.
Hoppe H, Nutting CW, Smouse HR et al. Günther Tulip filter retrievability multicenter study including CT follow-up: final report. J. Vasc. Interv. Radiol. 17(6), 1017–1023 (2006).
61.
Kaskarelis IS, Koukoulaki M, Chlapoutaki CE et al. Clinical experience with Günther temporary inferior vena cava filters. Clin. Imaging 30(2), 108–113 (2006).
62.
Keller IS, Meier C, Pfiffner R, Keller E, Pfammatter T. Clinical comparison of two optional vena cava filters. J. Vasc. Interv. Radiol. 18(4), 505–511 (2007).
63.
Looby S, Given MF, Geoghegan T, McErlean A, Lee MJ. Gunther Tulip retrievable inferior vena caval filters: indications, efficacy, retrieval, and complications. Cardiovasc. Intervent. Radiol. 30(1), 59–65 (2007).
64.
Offner PJ, Hawkes A, Madayag R, Seale F, Maines C. The role of temporary inferior vena cava filters in critically ill surgical patients. Arch. Surg. 138(6), 591–595 (2003).
65.
Ota S, Yamada N, Tsuji A et al. The Günther-Tulip retrievable IVC filter: clinical experience in 118 consecutive patients. Circ. J. 72(2), 287–292 (2008).
66.
Piano G, Ketteler ER, Prachand V et al. Safety, feasibility, and outcome of retrievable vena cava filters in high-risk surgical patients. J. Vasc. Surg. 45(4), 784–788 (2007).
67.
Rosenthal D, Wellons ED, Hancock SM, Burkett AB. Retrievability of the Günther Tulip vena cava filter after dwell times longer than 180 days in patients with multiple trauma. J. Endovasc. Ther. 14(3), 406–410 (2007).
68.
Schuster R, Hagedorn JC, Curet MJ, Morton JM. Retrievable inferior vena cava filters may be safely applied in gastric bypass surgery. Surg. Endosc. 21(12), 2277–2279 (2007).
69.
Strauss EJ, Egol KA, Alaia M, Hansen D, Bashar M, Steiger D. The use of retrievable inferior vena cava filters in orthopaedic patients. J. Bone Joint Surg. Br. 90(5), 662–667 (2008).
70.
Terhaar OA, Lyon SM, Given MF, Foster AE, Mc Grath F, Lee MJ. Extended interval for retrieval of Günther Tulip filters. J. Vasc. Interv. Radiol. 15(11), 1257–1262 (2004).
71.
Xiao L, Xu K, Shen J, Li H, Tong J, Zhang X. The application of GxA8xB9nther Tulip retrievable inferior vena cava filter in interventional treatment for acute deep venous thrombosis of lower extremity. J. Interv. Radiol. 19(9), 707–711 (2010).
72.
Xiao L, Shen J, Tong J, Li H, Xu K. The initial experience of transjugular retrieval of Geunther Tulip inferior vena cava filters. J. Interv. Radiol. 20(5), 366–371 (2011).
73.
Yamagami T, Kato T, Iida S, Hirota T, Nishimura T. Gunther tulip inferior vena cava filter placement during treatment for deep venous thrombosis of the lower extremity. Cardiovasc. Intervent. Radiol. 28(4), 442–453 (2005).
74.
Yamagami T, Kato T, Hirota T, Yoshimatsu R, Matsumoto T, Nishimura T. Evaluation of retrievability of the Gunther tulip vena cava filter. Cardiovasc. Intervent. Radiol. 30(2), 226–231 (2007).
75.
Geisbüsch P, Benenati JF, Peña CS et al. Retrievable inferior vena cava filters: factors that affect retrieval success. Cardiovasc. Intervent. Radiol. 35(5), 1059–1065 (2012).
76.
Wicky S, Doenz F, Meuwly JY, Portier F, Schnyder P, Denys A. Clinical experience with retrievable Günther Tulip vena cava filters. J. Endovasc. Ther. 10(5), 994–1000 (2003).
77.
Given MF, McDonald BC, Brookfield P et al. Retrievable Gunther Tulip inferior vena cava filter: experience in 317 patients. J. Med. Imaging Radiat. Oncol. 52(5), 452–457 (2008).
78.
Hiromatsu S, Nata S, Ohno T et al. Non-permanent inferior vena cava filters for prophylaxis and treatment of lower limb venous thromboembolism. Vasc. Endovasc. Surg. 44(8), 668–673 (2010).
79.
Ray CE Jr, Mitchell E, Zipser S, Kao EY, Brown CF, Moneta GL. Outcomes with retrievable inferior vena cava filters: a multicenter study. J. Vasc. Interv. Radiol. 17(10), 1595–1604 (2006).
80.
Seshadri T, Tran H, Lau KK, Tan B, Gan TE. Ins and outs of inferior vena cava filters in patients with venous thromboembolism: the experience at Monash Medical Centre and review of the published reports. Intern. Med. J. 38(1), 38–43 (2008).
81.
Smouse HB, Rosenthal D, Thuong VH et al. Long-term retrieval success rate profile for the Günther Tulip vena cava filter. J. Vasc. Interv. Radiol. 20(7), 871–878 (2009).
82.
Gasparis AP, Spentzouris G, Meisner RJ, Elitharp D, Labropoulos N, Tassiopoulos A. Improving retrieval rates of temporary inferior vena cava filters. J. Vasc. Surg. 54(Suppl. 6), S34–S38 (2011).
83.
Karmy-Jones R, Jurkovich GJ, Velmahos GC et al. Practice patterns and outcomes of retrievable vena cava filters in trauma patients: an AAST multicenter study. J. Trauma 62(1), 17–25 (2007).
84.
Sag AA, Stavas JM, Burke CT, Dixon RG, Marquess JS, Mauro MA. Analysis of tilt of the Günther Tulip filter. J. Vasc. Interv. Radiol. 19(5), 669–676 (2008).
85.
Turba UC, Arslan B, Meuse M et al. Günter tulip filter retrieval experience: predictors of successful retrieval. Cardiovasc. Intervent. Radiol. 33(4), 732–738 (2010).
86.
Olorunsola OG, Kohi MP, Fidelman N et al. Caval penetration by retrievable inferior vena cava filters: a retrospective comparison of Option and Günther Tulip filters. J. Vasc. Interv. Radiol. 24(4), 566–571 (2013).
87.
Johnson MS, Nemcek AA Jr, Benenati JF et al. The safety and effectiveness of the retrievable option inferior vena cava filter: a United States prospective multicenter clinical study. J. Vasc. Interv. Radiol. 21(8), 1173–1184 (2010).
88.
Iqbal SI, Elmi A, Hedgire S et al. Preliminary experience with Option inferior vena cava filter. Vasc. Endovasc. Surg. 47(1), 24–29 (2013).
89.
Tsui B, An T, Moon E, King R, Wang W. Retrospective review of 516 implantations of Option inferior vena cava filters at a single health care system. J. Vasc. Interv. Radiol. 27(3), 345–353 (2016).
90.
Soleymanha M, Mobayen M, Asadi K, Adeli A, Haghparast-Ghadim-Limudahi Z. Survey of 2582 cases of acute orthopedic trauma. Trauma Mon. 19(4), e16215 (2014).
91.
Wall PL, Glawe BJ, Sahr SM et al. Gender differences in blood transfusions after trauma related to ages and mechanisms. Am. Surg. 80(5), E141–E143 (2014).
92.
Roach RE, Cannegieter SC, Lijfering WM. Differential risks in men and women for first and recurrent venous thrombosis: the role of genes and environment. J. Thromb. Haemost. 12(10), 1593–1600 (2014).
93.
Bard Denali Vena Cava Filter Instructions for Use [package insert]. Bard Peripheral Vascular, AZ, USA (2013). Revision 4
94.
Singer MA, Wang SL. Modeling blood flow in a tilted inferior vena cava filter: does tilt adversely affect hemodynamics? J. Vasc. Interv. Radiol. 22(2), 229–235 (2011).
95.
Option™ELITE Inferior Vena Cava Filter System. (2020). https://www.argonmedical.com/products/option-elite-inferior-vena-cava-filter-system
96.
Murphy EH, Johnson ED, Kopchok GE, Fogarty TJ, Arko FR. Crux vena cava filter. Expert Rev. Med. Devices 6(5), 477–485 (2009).
97.
Durack JC, Westphalen AC, Kekulawela S et al. Perforation of the IVC: rule rather than exception after longer indwelling times for the Günther Tulip and Celect retrievable filters. Cardiovasc. Intervent. Radiol. 35(2), 299–308 (2012).
Information & Authors
Information
Published In
Pages: 437 - 449
PubMed: 35199584
Copyright
© 2022 Future Medicine Ltd.
History
Received: 22 November 2021
Accepted: 5 February 2022
Published online: 24 February 2022
Keywords:
Topics
Authors
Funding Information
BD (Becton, Dickinson and Company)
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Clinical outcomes of retrievable inferior vena cava filters for venous thromboembolic diseases. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0291
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Pengkai Cao, Xintong Luo, Yunsong Li, Xiang Gao, Xiangdong Liu, Yanrong Zhang, Wei Bi, Anticoagulation Therapy May Reduce Subsegmental Nonocclusive Inferior Vena Cava Filter–Related Thrombus Burden: A Retrospective Study in a Single-Center Institution, Journal of Endovascular Therapy, 10.1177/15266028251384946, (2025).
- Xuan Tian, Jianlong Liu, Jinyong Li, Xiao Liu, Mi Zhou, Yule Tian, Case Report: Endoluminal removal of a conical retrievable superior vena cava filter with a retraction hook attached to the wall, Frontiers in Cardiovascular Medicine, 10.3389/fcvm.2024.1412571, 11, (2024).
- Miguel Angel De Gregorio, Juan Jose Ciampi-Dopazo, Jose Urbano, Roman Bernal, Carolina Serrano-Casorrán, Cristina Bonastre, Jose Maria Abadal, Santiago Mendez, Arturo Fredes, Jose Rodriguez, Sergio Rodriguez, Jose Andres Guirola, Effectiveness, Retrievability, and Safety of Celect vs. ALN Inferior Vena Cava Filters: A Randomized Prospective Multicenter Controlled Study, Journal of Vascular Diseases, 10.3390/jvd2010012, 2, 1, (177-187), (2023).