Efficacy and safety of PD-1/PD-L1 and CTLA-4 immune checkpoint inhibitors in colorectal cancer: a meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aims: To evaluate the efficacy and safety of PD-1/PD-L1 and/or CTLA-4 inhibitors in the treatment of colorectal cancer (CRC) by meta-analysis. Methods: Electronic databases were searched. Eligible studies included investigations of efficacy and safety of anti-PD-1/PD-L1 or anti-CTLA-4 agents in patients with CRC. Corresponding indicators were calculated. Results: A total of 15 articles were included. The pooled objective response rate, overall survival rate, progression-free survival rate and adverse event rate were 33, 56, 46 and 59%, respectively. The objective response rates for CRC with deficient mismatch repair and CRC with proficient mismatch repair were 43 and 3%, respectively, in patients treated with PD-1 inhibitors. Conclusion: The authors' study indicates that PD-1/PD-L1 inhibitors manifest promising clinical responses in the treatment of CRC with deficient mismatch repair with acceptable treatment-related adverse events.
Colorectal cancer (CRC) is one of the most commonly diagnosed malignant tumors worldwide, with an annual incidence of 19.7 in 100,000 and a mortality of 8.9 in 100,000 [1,2]. It accounts for about 10% of global diagnosed cancers and cancer-related deaths every year [3]. The main causes of the high mortality associated with advanced CRC are malignant cancer progression and metastases. Furthermore, despite advances in the standards of treatment, prognosis remains poor for patients with metastatic CRC, with a median 5-year survival rate of 14% [4]. Environmental risk factors, including alcohol and tobacco use, aging, diet and sedentary lifestyle, contribute to the development of CRC [5–7]. Moreover, genetic instability, including chromosome abnormality, microsatellite instability and CpG island methylator phenotype, is an important cause of CRC [8]. Cases of CRC can be divided into those that involve deficient mismatch repair (dMMR) or high levels of microsatellite instability and those that involve proficient mismatch repair (pMMR) or low levels of microsatellite instability, among which dMMR CRC with high levels of microsatellite instability is associated with high tumor mutation load and immune cell infiltration [9]. Thus, patients with CRC are in urgent need of more effective therapies.
Currently, the standard first-line therapy for local metastatic CRC is adjuvant chemotherapy and a biologic agent, including anti-EGFR and anti-VEGF antibodies; however, the specific regimen depends on cancer characteristics. Several factors may affect therapeutic options in patients with metastatic CRC, including patient characteristics, tumor characteristics, molecular characteristics and patient preference [10–12]. However, most patients progress within 1 year [13]. The human immune system plays a major role in the suppression of tumor initiation and progression [14]. CD8+ T cells can seek out and destroy precancerous and cancerous cells in the human body. However, tumors have the potential to evade immune response through different mechanisms, including upregulation of ligands that synergistically inhibit immune checkpoint receptors, which leads to impotent T cells [1,14,15]. Novel methods of immunotherapy have been attracting attention because of their ability to prime the immune system to attack cancer cells [5,16]. Inhibition of the known interaction between PD-1 and PD-L1 can restore the activity of T cells against tumor cells [17–19]. Over the past decade, monoclonal antibodies that target PD-1/PD-L1 (nivolumab, pembrolizumab, avelumab, atezolizumab and durvalumab) have demonstrated promising clinical responses in patients with CRC [20–31]. Furthermore, CTLA-4 is another checkpoint that has been found to be a reliable target, and antibodies targeting CTLA-4 (ipilimumab and tremelimumab) have manifested profound outcomes in treatment for advanced cancers [32–35]. However, only a fraction of patients have been found to respond to immune checkpoint inhibitor (ICI) monotherapy [33]. In previous clinical trials, outcomes were improved when patients received a combination of anti-PD-1/PD-L1 and anti-CTLA-4 agents [28,36,37].
To the best of the authors' knowledge, several studies with small sample sizes have investigated the efficacy and safety of PD-1/PD-L1 and/or CTLA-4 inhibitors in patients with CRC. The aim of this study was to conduct a meta-analysis by collating the available evidence to generate an accurate and sound assessment of the efficacy and toxicity of anti-PD-1/PD-L1 and/or CTLA-4 agents and to subsequently provide evidence and insight with regard to clinical implementation, decision-making and future research.
Methods
Statement
This meta-analysis was based entirely on previously published studies with declared ethical approval, and no original raw clinical data were collected or utilized; therefore, ethical approval was not required for this study. This review was conducted on the basis of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [38].
Search strategy and selection criteria
The authors conducted a computerized search of the electronic databases PubMed, Web of Science and Embase from inception to April 30, 2021, with articles in English considered. The following search strategy was used: (((((((((Nivolumab[Title/Abstract]) OR Pembrolizumab[Title/Abstract]) OR Durvalumab[Title/Abstract]) OR Tremelimumab[Title/Abstract]) OR Avelumab[Title/Abstract]) OR ((((PD1[Title/Abstract]) OR PDL1[Title/Abstract] OR CTLA-4[Title/Abstract]) OR immune check point[Title/Abstract]) OR immune therapy[Title/Abstract]))))) AND (((((Colon cancer[Title/Abstract]) OR colorectal adenocarcinoma[Title/Abstract]) OR colorectal cancer[Title/Abstract]) OR colorectal carcinoma[Title/Abstract]))))). The references of these articles were also searched to assay any additional studies not previously identified in the initial literature search. The inclusion criterion was clinical trials demonstrating the utility of PD-1/PD-L1 or CTLA-4 inhibitors in patients with CRC. To avoid duplications, if studies recruited participants over the same period of time or in the same study center, only the study with the largest sample size or yielding the most pertinent outcomes was included. Exclusion criteria included case reports, review articles, news and editorials.
Two independent investigators (C Jin and X Zhu) conducted the literature search and process of study inclusion. When disagreement occurred, the investigators discussed their differences, and a third reviewer (X Huang) was involved in cases in which no consensus was achieved. The authors used the Methodological Index for Non-Randomized Studies to evaluate the quality of studies included in this meta-analysis [39].
Data extraction and quality assessments
Two reviewers independently screened the titles and abstracts according to the inclusion criterion. A full-text reading of the literature was performed for the final inclusion. The following information was extracted from each study: name of first author, year of publication, number of patients, name of inhibitors, type of ICI, sex and age of patients, molecular CRC phenotypes and outcome parameters. The primary outcomes were objective response rate (ORR), complete response rate, partial response rate, stable disease rate, disease progression rate, disease control rate, 12-month overall survival (OS) rate, 12-month progression-free survival (PFS) rate and treatment-related adverse event (AE) rate of any grade. Clinical response and disease progression were assessed according to Response Evaluation Criteria in Solid Tumors version 1.1 [40].
Statistical analysis
The authors used R 4.0.2 software for statistical analyses. The efficacy of ICIs in CRC was assessed based on the aforementioned indicators. Cochran's Q test was used to assess heterogeneity between studies, and the I2 statistic was used to investigate the magnitude of the heterogeneity. Pooled indicators and their respective 95% CIs were calculated with a random effects model or fixed effects model. If the I2 value was >50%, a random effects model was used; otherwise, a fixed effects model was used. Egger's tests were performed to assess potential publication bias. Furthermore, the authors conducted a sensitivity analysis to check the stability of pooled outcomes. A probability of p < 0.05 was regarded as statistically significant.
Results
Study selection and characteristics
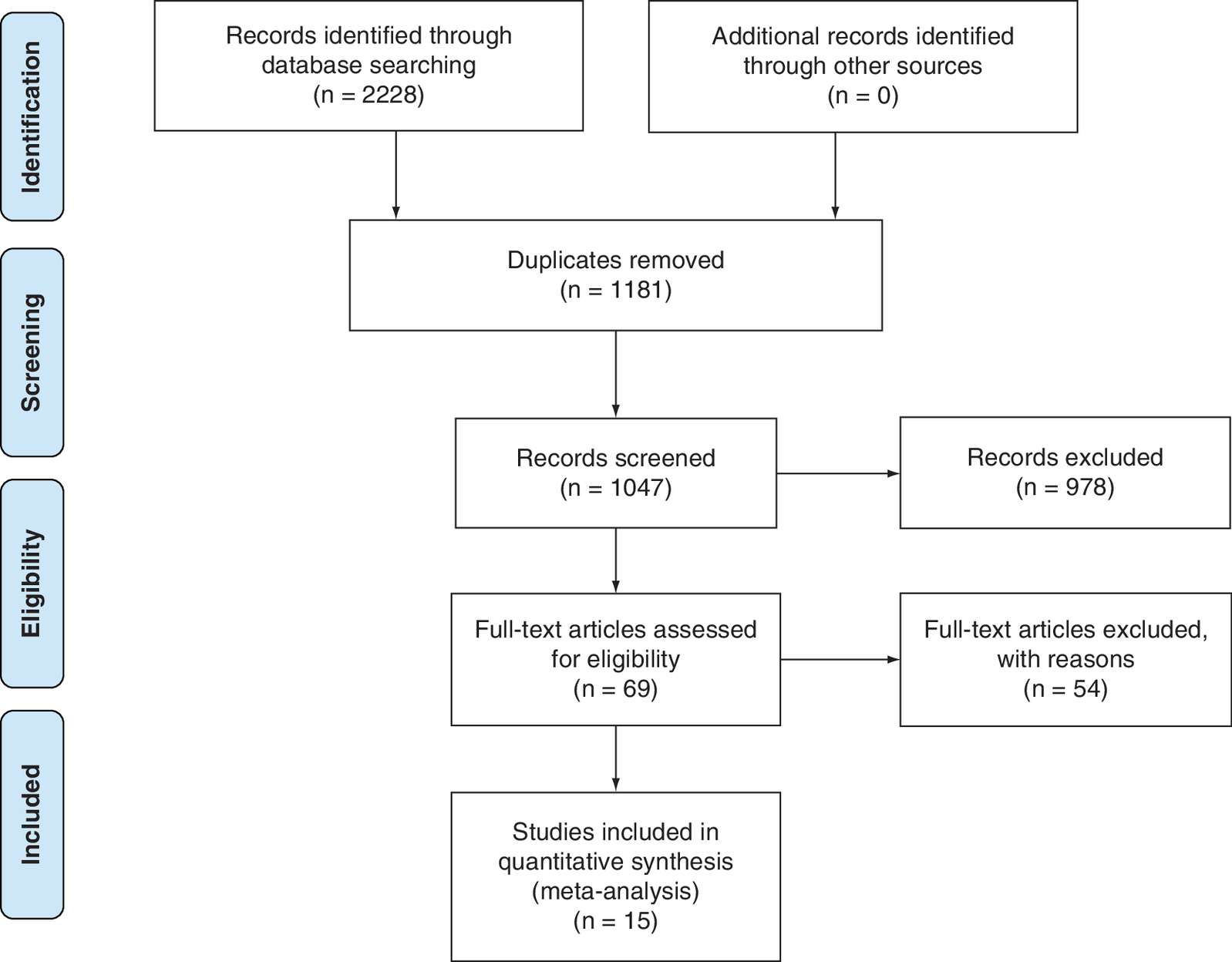
A total of 2228 articles were identified from the databases searched. Of these, 1181 duplicates were removed and 978 studies were excluded through an initial screening. After a full-text assessment of the remaining 69 articles for eligibility, 15 articles were identified for inclusion in this meta-analysis. No additional studies were found through reference screening of the included articles. Figure 1 shows the flow chart and results of the literature search and study selection process. The selected 15 studies, which contained a total of 924 patients diagnosed with CRC, provided the relevant eligible outcomes required for this study. Of note, results of two studies [26,28] originated from the CheckMate 142 cohort and had different indicators. Table 1 shows the details of the studies included.
| Author | Year | Sample size | Sex, M/F | Age, years (range) | Name of ICI | Dose of ICI | Type of ICI | Molecular phenotype | MINORS score | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| Chung | 2010 | 47 | 29/18 | 62 (39–79) | Tremelimumab | 15 mg/kg | CTLA-4 | NR | 15 | [21] |
| Lipson | 2013 | 14 | NR | NR | BMS-936558 | NR | PD-1 | dMMR | 15 | [41] |
| Le | 2015 | 32 | 19/13 | NR | Pembrolizumab | 10 mg/kg | PD-1 | dMMR/pMMR | 13 | [24] |
| Segal | 2016 | 26 | 10/16 | 55 (18–80) | Pembrolizumab | 200 mg every 3 weeks for up to 24 months | PD-1 | pMMR | 14 | [30] |
| Overman | 2017 | 74 | 44/30 | 52.5 (44.0–64.0) | Nivolumab | 3 mg/kg | PD-1 | dMMR | 16 | [29] |
| O'Neil | 2017 | 23 | 13/10 | 57 (40–78) | Pembrolizumab | 10 mg/kg | PD-1 | pMMR | 14 | [27] |
| Overman | 2018 | 119 | 70/49 | 58 (21–88) | Nivolumab + ipilimumab | Nivolumab 3 mg/kg plus ipilimumab 1 mg/kg | PD-1 + CTLA-4 | dMMR | 15 | [28] |
| Sinicrope | 2018 | 24 | NR | NR | Pembrolizumab | 200 mg a day | PD-1 | dMMR | 14 | [31] |
| Le | 2019 | 61 | 36/25 | 53 (21–84) | Pembrolizumab | 200 mg every 3 weeks | PD-1 | dMMR | 15 | [23] |
| Morse | 2019 | 119 | 70/49 | 58 (21–88) | Nivolumab + ipilimumab | Nivolumab 3 mg/kg plus ipilimumab 1 mg/kg | PD-1 + CTLA-4 | dMMR | 14 | [26] |
| Andre | 2020 | 153 | 71/82 | 63 (24–93) | Pembrolizumab | 200 mg every 3 weeks | PD-1 | dMMR | 14 | [42] |
| Chen | 2020 | 119 | 74/45 | 65 (39–87) | Tremelimumab + durvalumab | 75 mg of tremelimumab every 28 days for the first four cycles plus 1,500 mg durvalumab every 28 days | PD-L1 + CTLA-4 | NR | 14 | [37] |
| Cohen | 2020 | 57 | 30/27 | 57 (46–64) | Nivolumab + ipilimumab | Nivolumab 3 mg/kg plus ipilimumab 1 mg/kg | PD-1 | dMMR | 13 | [43] |
| Kim | 2020 | 33 | 44403 | 60 (25–88) | Avelumab | 10 mg/kg | PD-L1 | dMMR | 14 | [44] |
| Kanikarla-Marie | 2020 | 23 | 12/11 | 56 (28–69) | Tremelimumab + durvalumab | 75 mg of tremelimumab every 28 days for the first four cycles plus 1,500 mg durvalumab every 28 days | PD-L1 + CTLA-4 | dMMR/pMMR | 13 | [36] |
dMMR: Deficient mismatch repair; F: Female; ICI: Immune checkpoint inhibitor; M: Male; MINORS: Methodological Index for Non-Randomized Studies; NR: Not reported; pMMR: Proficient mismatch repair.
Efficacy and safety of ICIs
The numbers of articles included in the analysis of ORR, complete response rate, partial response rate, stable disease rate, disease progression rate, disease control rate, OS rate, PFS rate and AE rate were 10, 8, 10, 11, 10, 6, 8, 7 and 10, respectively. The pooled ORR, complete response rate, partial response rate, stable disease rate, disease progression rate, disease control rate, OS rate, PFS rate and AE rate were 33% (95% CI: 23–45; I2 = 86%; p < 0.01), 11% (95% CI: 8–15; I2 = 46%; p = 0.08), 27% (95% CI: 18–36; I2 = 81%; p < 0.01), 30% (95% CI: 23–38; I2 = 74%; p < 0.01), 35% (95% CI: 19–53; I2 = 95%; p < 0.01), 59% (95% CI: 35–81; I2 = 95%; p < 0.01), 56% (95% CI: 32–79; I2 = 97%; p < 0.01), 46% (95% CI: 32–61; I2 = 91%; p < 0.01) and 59% (95% CI: 55–63; I2 = 49%; p = 0.05), respectively (Table 2). Detailed results of the analyses are shown in Supplementary Figures 1–9.
| ICI indicator | % pooled outcome | % LCI | % HCI | % I2 value | p-value |
|---|---|---|---|---|---|
| ORR | 33 | 23 | 45 | 86 | < 0.01 |
| Complete response rate | 11 | 8 | 15 | 46 | 0.08 |
| Partial response rate | 27 | 18 | 36 | 81 | < 0.01 |
| Stable disease rate | 30 | 23 | 38 | 74 | < 0.01 |
| Disease progression rate | 35 | 19 | 53 | 95 | < 0.01 |
| Disease control rate | 59 | 35 | 81 | 95 | < 0.01 |
| OS rate | 56 | 32 | 79 | 97 | < 0.01 |
| PFS rate | 46 | 32 | 61 | 91 | < 0.01 |
| AE rate | 59 | 55 | 63 | 49 | 0.05 |
AE: Adverse event; HCI: Highest CI; ICI: Immune checkpoint inhibitor; LCI: Lowest CI; ORR: Objective response rate; OS: Overall survival; PFS: Progression-free survival.
Efficacy and safety of monotherapy
Eleven articles reported the efficacy and safety of PD-1 antibodies. The pooled ORR, OS rate, PFS rate and AE rate for PD-1 inhibitors were 32% (95% CI: 20–45; I2 = 85%; p < 0.01), 67% (95% CI: 49–83; I2 = 85%; p < 0.01), 43% (95% CI: 25–61; I2 = 68%; p < 0.01) and 61% (95% CI: 48–74; I2 = 84%; p < 0.01), respectively (Figure 2). The ORRs for dMMR CRC and pMMR CRC were 43% (95% CI: 34–54; I2 = 68%; p < 0.01) and 3% (95% CI: 0–10; I2 = 0%; p = 0.42), respectively (Figure 3). The pooled OS and PFS rates for dMMR CRC were 76% (95% CI: 69–82; I2 = 7%; p = 0.34) and 53% (95% CI: 40–66; I2 = 83%; p < 0.01), respectively (Figures 4 & 5). O'Neil et al. reported a 12-month OS rate of 30% and PFS rate of 4% for pMMR CRC [27]. The overall AE rates for dMMR CRC and pMMR CRC were 64% (95% CI: 48–78; I2 = 88%; p < 0.01) and 54% (95% CI: 18–88; I2 = 86%; p < 0.01), respectively (Figure 6).
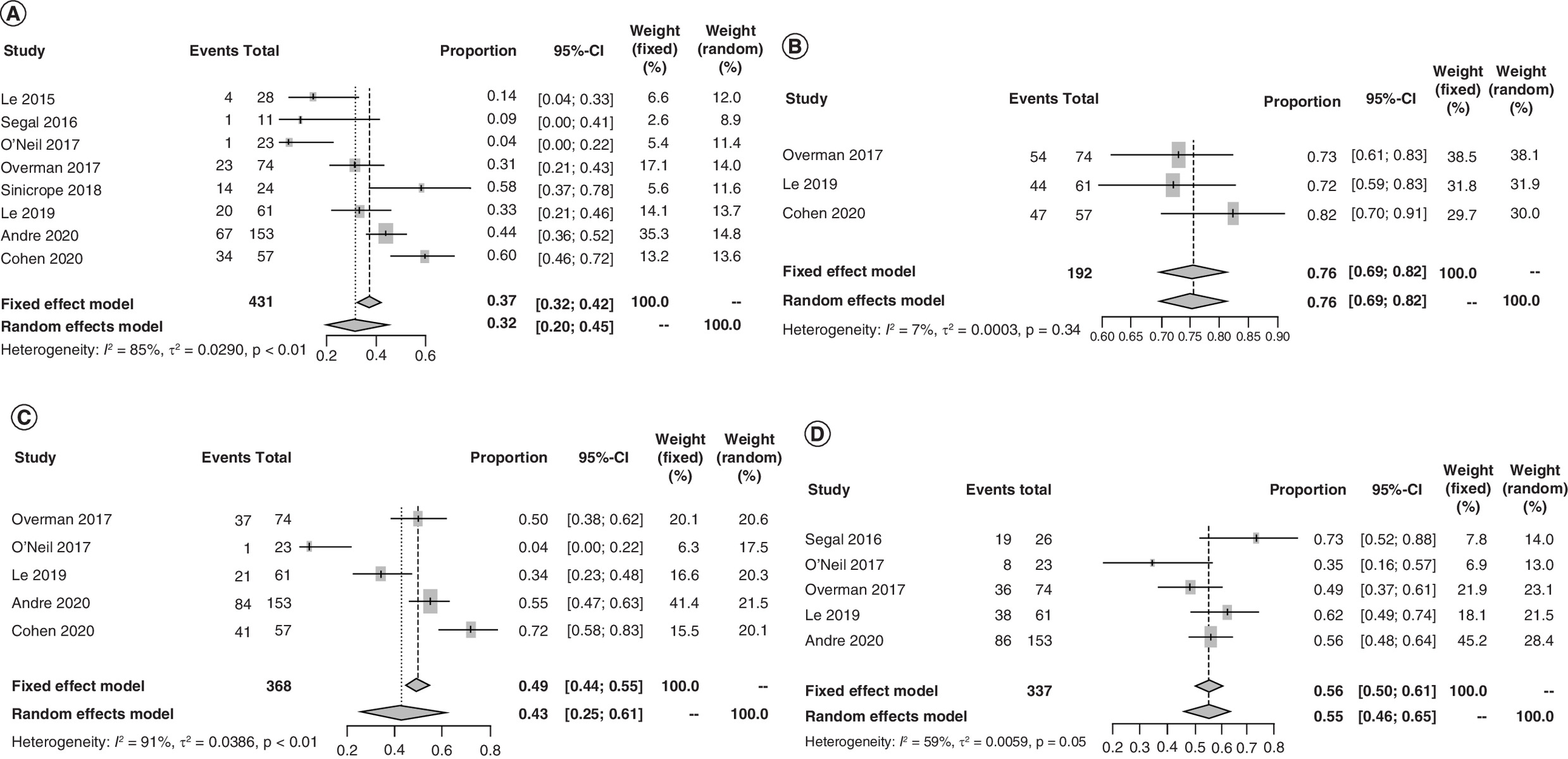
Figure 2. Forest plots of efficacy and adverse event rates in PD-1 subgroup.
(A) Forest plot of ORRs in PD-1 subgroup. (B) Forest plot of 12-month OS rates in PD-1 subgroup. (C) Forest plot of 12-month PFS rates in PD-1 subgroup. (D) Forest plot of treatment-related AE rates in PD-1 subgroup.
AE: Adverse event; ORR: Objective response rate; OS: Overall survival; PFS: Progression-free survival.
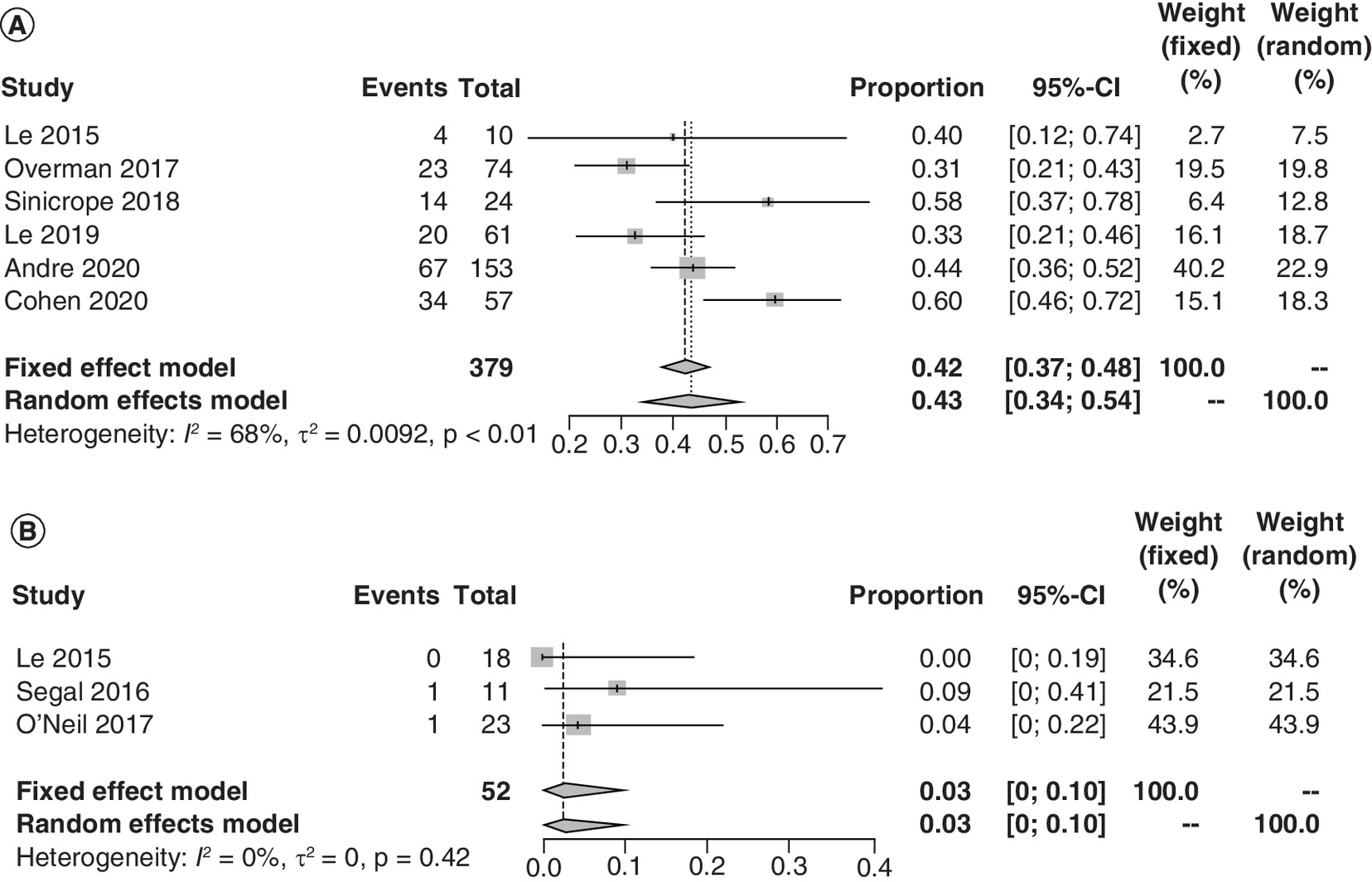
Figure 3. Forest plots of objective response rates in patients with colorectal cancer with deficient and proficient mismatch repair in PD-1 subgroup.
(A) Forest plot of ORRs in patients with dMMR CRC in PD-1 subgroup. (B) Forest plot of ORRs in patients with pMMR CRC in PD-1 subgroup.
CRC: Colorectal cancer; dMMR: Deficient mismatch repair; ORR: Objective response rate; pMMR: Proficient mismatch repair.
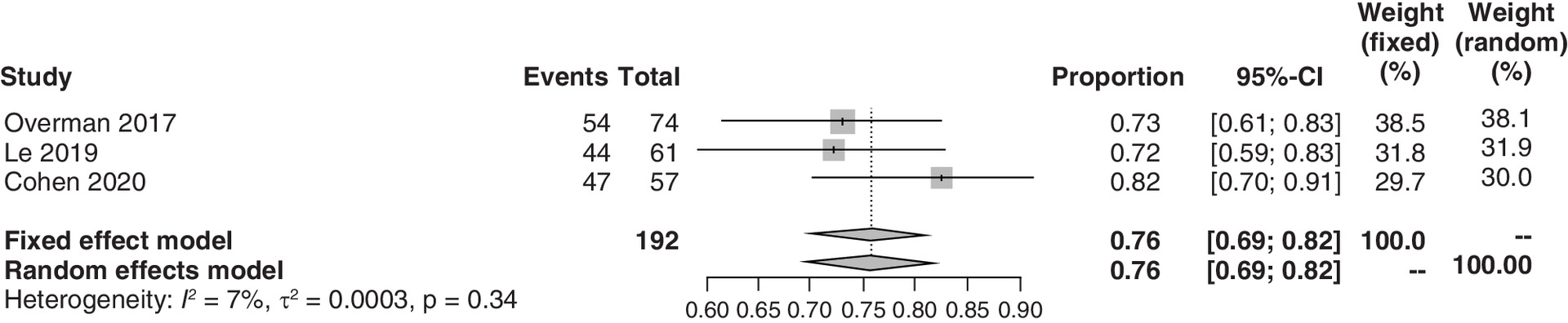
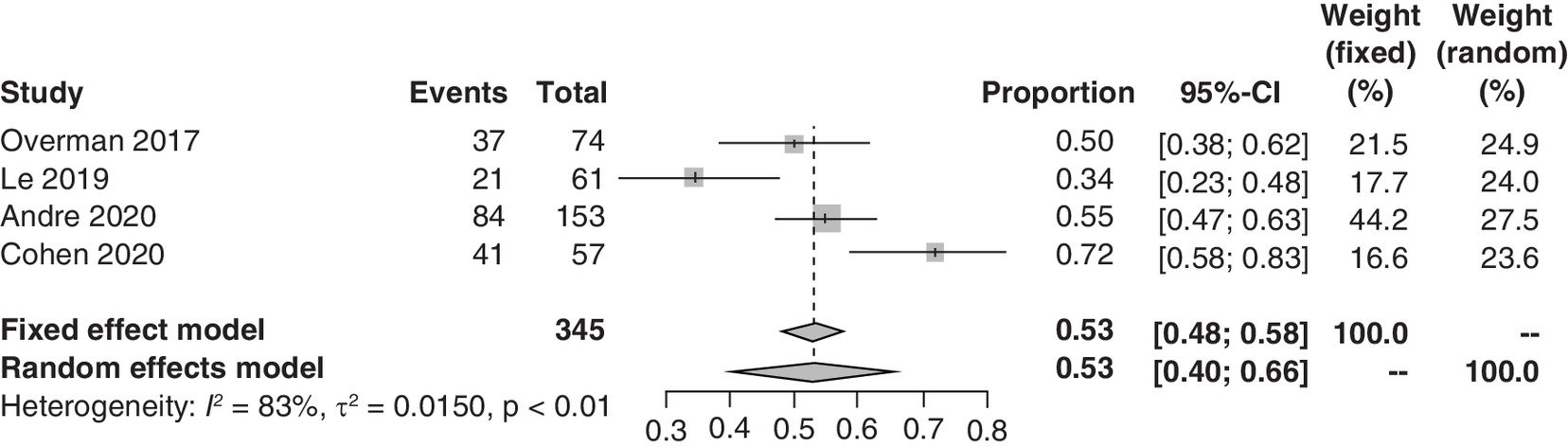
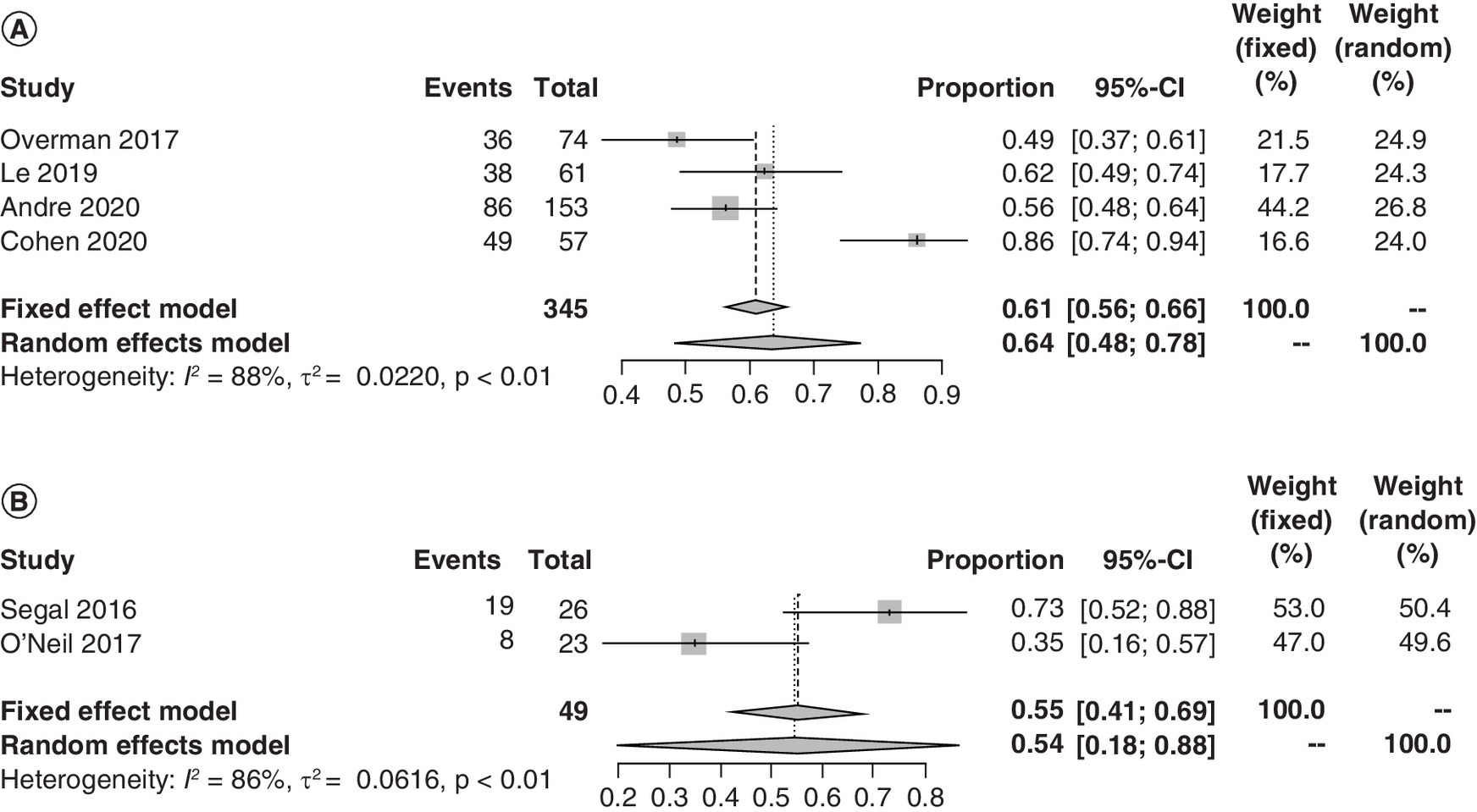
Figure 6. Forest plots of treatment-related adverse event rates in patients with colorectal cancer with deficient and proficient mismatch repair in PD-1 subgroup.
(A) Forest plot of treatment-related AE rates in patients with dMMR CRC in PD-1 subgroup. (B) Forest plot of treatment-related AE rates in patients with pMMR CRC in PD-1 subgroup.
AE: Adverse event; CRC: Colorectal cancer; dMMR: Deficient mismatch repair; pMMR: Proficient mismatch repair.
Results of a study by Kim et al. demonstrated that the ORR, OS rate, PFS rate and AE rate of avelumab monotherapy in 33 dMMR CRC patients were 24, 67, 36 and 73%, respectively [44]. Chung et al. reported a disease progression rate of 96% and OS rate of 11% in 47 CRC patients treated with tremelimumab [21].
Efficacy and safety of combined immunotherapy
Results of the Checkmate 142 study demonstrated that in dMMR CRC patients treated with nivolumab plus ipilimumab, the ORR, 12-month OS rate, 12-month PFS rate and AE rate were 55, 87, 71 and 56%, respectively. Two studies assessed the efficacy and/or safety of combined therapy with durvalumab and tremelimumab. The complete response rate observed in the study by Kanikarla-Marie et al. was 17%, with a stable disease rate of 65% [36]. In the study by Chen et al., the disease control rate was 23%, AE rate was 64% and 12-month OS rate was 20% [37].
Publication bias
Egger's tests for publication bias yielded p-values of 0.0729, 0.2898, 0.0287, 0.1502, 0.3349, 0.3021, 0.7798, 0.0964 and 0.5735 in the pooled analysis of ORR, complete response rate, partial response rate, stable disease rate, disease progression rate, disease control rate, OS rate, PFS rate and AE rate, respectively. The respective p-values for ORR, OS, PFS and AEs in the PD-1 subgroup were 0.2112, 0.1396, 0.2675 and 0.8366.
Sensitivity analysis
The authors performed a sensitivity analysis to assess the impacts of a single study on the overall outcomes. The I2 value was reduced from 66 to 46% by omitting the study by Overman et al. [29] from the meta-analysis of complete response rate, with a pooled rate of 11% (95% CI: 8–15). In the pooled analysis of 12-month OS rate in the PD-1 subgroup, the I2 value was reduced from 85 to 7% when the study by O'Neil et al. was omitted, with a pooled rate of 76% (95% CI: 69–82) [27]. With regard to the analysis of AE rates, results of the sensitivity analysis revealed that the I2 value decreased from 75 to 49% after omitting the study by Cohen et al., with a pooled rate of 59% (95% CI: 55–63) [43]. Likewise, the I2 value decreased from 84 to 59% after omitting the study by Cohen et al. from the analysis of AE rates in the PD-1 subgroup, with a pooled rate of 56% (95% CI: 50–61). Nevertheless, after excluding one study after another, the other pooled results demonstrated the robustness of the results.
Discussion
CRC is one of the most common tumors, with high rates of incidence and mortality worldwide [3]. Recently, immune checkpoint molecules such as PD-1/PD-L1 and CTLA-4 have been identified as possible targets for immunotherapy in CRC [45]. A number of clinical trials assessing PD-1/PD-L1 and/or CTLA-4 inhibitors in the treatment of dMMR CRC and CRC with high levels of microsatellite instability have demonstrated practice-changing results [21–31,36,37,41–44]. In this meta-analysis, 15 published articles containing 924 CRC patients treated with anti-PD-1/PD-L1 and/or CTLA-4 agents were included. Six articles were published within 2 years. The pooled ORR, complete response rate, partial response rate, stable disease rate, disease progression rate, disease control rate, OS rate, PFS rate and AE rate were 33, 11, 27, 30, 35, 59, 56, 46 and 59%, respectively. With regard to ICI monotherapy, only studies using PD-1 inhibitors were pooled analysis, whereas results of studies estimating CTLA-4 agents were not pooled up due to insufficient numbers of studies. Results revealed significant response and survival outcomes with anti-PD-1 agents in patients with dMMR CRC compared with patients with pMMR CRC. Unfortunately, patients with dMMR CRC account for approximately 15% of all cases of CRC [1]. The lack of recruitment of tumor immune cells appears to be the fundamental obstacle to the curative effect of CRC patients with pMMR subtype [9]. As for the dMMR CRC subset, high neoantigen expression and elevated degree of intraepithelial T-cell infiltration make tumor cells especially susceptible to ICIs, which promotes T-cell-mediated antitumor activities [46]. The results of this meta-analysis demonstrated superior efficacy of anti-PD-1 agents compared with PD-L1 and CTLA-4 inhibitor monotherapy. Furthermore, combined anti-PD-1 and CTLA-4 immunotherapy appeared to be even more effective, with a lower AE rate compared with ICI monotherapy. The US FDA has approved combination immunotherapy (nivolumab and ipilimumab) for use in CRC [28].
In this meta-analysis, the authors did a systematic literature search in the English language to enhance the probability of retrieving as many relevant studies as possible. Data extraction was conducted by two independent investigators using a well-designed form. The authors intended to use individual patient data for this meta-analysis. However, as these data were difficult to acquire, the authors eventually decided to conduct this meta-analysis at the study level. In addition, no randomized controlled trials were included in the authors' study. Nevertheless, the authors assessed the quality of studies included using the Methodological Index for Non-Randomized Studies scale. The heterogeneity among studies was statistically evaluated, and there was significant heterogeneity in most indicators. The heterogeneity may be attributed to differences in baseline characteristics of the study participants, study design, drug compliance, median lines of prior therapy in each study and other relevant factors. The authors were unable to conduct meta-regression because of the limited information on covariates provided by each included study. Sensitivity analysis revealed that after omitting studies that affected the pooled results, the degree of heterogeneity decreased in the meta-analysis of complete response rate, 12-month OS rate and AE rate in the PD-1 subgroup as well as overall AE rate. Furthermore, with the exception of the partial response rate analysis, Egger's tests indicated that there were no potential publication bias in the studies included. Because of the heterogeneity of information included in each study, the authors did not meta-analyze specific adverse reactions. Despite the existence of heterogeneity and publication bias, the results of this analysis may provide insight into and assistance with the design of clinical trials with larger sample sizes and longer follow-up periods for the evaluation of the efficacy and safety of PD-1/PD-L1 and/or CTLA-4 inhibitors.
Based on the outcomes of this meta-analysis, the authors can conclude that PD-1 inhibitors and combination immunotherapy demonstrate promising and profound clinical response and OS rates with durable treatment-related AEs in the treatment of dMMR CRC. However, the pathogenesis of treatment-related AEs remains poorly understood [47]. Interestingly, the majority of treatment-related AEs were manageable with and resolved using the recommended evidence-based algorithms for early intervention and treatment [26]. Although immunotherapy is the standard of care for dMMR CRC patients, several questions remain to be addressed, including optimal duration of immunotherapy, combination of agents, drug-resistance mechanisms of unresponsive patients, and the development of new agents targeted to enhance treatment effectiveness in the pMMR subtype. Moreover, the assessment of the long-term outcomes of patients with long survival and those are now undergoing adjuvant clinical trials ought to be focused in the future.
•
Over the past decade, monoclonal antibodies that target PD-1/PD-L1 have demonstrated promising clinical responses in patients with colorectal cancer.
•
Antibodies targeting CTLA-4 manifest profound outcomes in the treatment of advanced cancers.
•
Several studies with small sample sizes have investigated the efficacy and safety of PD-1/PD-L1 and/or CTLA-4 inhibitors in patients with colorectal cancer.
•
The authors conducted a meta-analysis to generate an accurate and sound assessment of the efficacy and toxicity of anti-PD-1/PD-L1 and/or CTLA-4 agents.
•
The results of this meta-analysis demonstrated superior efficacy of anti-PD-1 agents compared with PDL-1 and CTLA-4 inhibitor monotherapy.
•
Combined anti-PD-1 and CTLA-4 immunotherapy appeared to be even more effective, with a lower adverse event rate compared with immune checkpoint inhibitor monotherapy.
•
PD-1 inhibitors and combination immunotherapy demonstrate a promising and profound clinical response and overall survival rate with durable treatment-related adverse events in the treatment of colorectal cancer with deficient mismatch repair.
•
Questions remain to be addressed, including optimal duration of immunotherapy and combination of agents and drug resistance mechanisms of unresponsive patients.
Author contributions
C Jin and X Huang conceived and designed the study. C Jin and X Zhu were responsible for the collection, extraction and analysis of the data. C Jin and T Gong were responsible for writing the manuscript. Z Wei and J You performed the quality evaluation and completed data analysis. J You polished the English language usage. All authors reviewed the manuscript and approved the final version.
Financial & competing interests disclosure
This study was supported by ZDRCPY011 from Wuxi Key Talents Cultivation Objects. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
The data that support the findings of this study are available from the corresponding author on reasonable request.
Supplementary Material
File (supplementary figure 1.tiff)
- Download
- 121.25 KB
File (supplementary figure 2.tiff)
- Download
- 100.96 KB
File (supplementary figure 3.tiff)
- Download
- 124.96 KB
File (supplementary figure 4.tiff)
- Download
- 130.23 KB
File (supplementary figure 5.tiff)
- Download
- 123.83 KB
File (supplementary figure 6.tiff)
- Download
- 95.55 KB
File (supplementary figure 7.tiff)
- Download
- 110.39 KB
File (supplementary figure 8.tiff)
- Download
- 104.03 KB
File (supplementary figure 9.tiff)
- Download
- 117.57 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Kreidieh M, Mukherji D, Temraz S, Shamseddine A. Expanding the scope of immunotherapy in colorectal cancer: current clinical approaches and future directions. Biomed. Res. Int. 2020, 9037217 (2020).
2.
Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 16(12), 713–732 (2019).
• Provides important data regarding the global burden of colorectal cancer (CRC).
3.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 68(6), 394–424 (2018).
4.
Siegel RL, Miller KD, Fedewa SA et al. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 67(3), 177–193 (2017).
5.
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet 394(10207), 1467–1480 (2019).
•• Provides comprehensive information on CRC.
6.
Willett WC. Diet and cancer: an evolving picture. JAMA 293(2), 233–234 (2005).
7.
Martinez-Useros J, Garcia-Foncillas J. Obesity and colorectal cancer: molecular features of adipose tissue. J. Transl. Med. 14, 21 (2016).
8.
Grady WM, Carethers JM. Genomic and epigenetic instability in colorectal cancer pathogenesis. Gastroenterology 135(4), 1079–1099 (2008).
9.
Ganesh K, Stadler ZK, Cercek A et al. Immunotherapy in colorectal cancer: rationale, challenges and potential. Nat. Rev. Gastroenterol. Hepatol. 16(6), 361–375 (2019).
10.
Wrobel P, Ahmed S. Current status of immunotherapy in metastatic colorectal cancer. Int. J. Colorectal Dis. 34(1), 13–25 (2019).
11.
Morse MA, Hochster H, Benson A. Perspectives on treatment of metastatic colorectal cancer with immune checkpoint inhibitor therapy. Oncologist 25(1), 33–45 (2020).
12.
Yiu AJ, Yiu CY. Biomarkers in colorectal cancer. Anticancer Res. 36(3), 1093–1102 (2016).
• Describes advances in CRC biomarkers.
13.
Chau I, Cunningham D. Treatment in advanced colorectal cancer: what, when and how? Br. J. Cancer 100(11), 1704–1719 (2009).
14.
Emambux S, Tachon G, Junca A, Tougeron D. Results and challenges of immune checkpoint inhibitors in colorectal cancer. Expert Opin. Biol. Ther. 18(5), 561–573 (2018).
15.
Salmaninejad A, Valilou SF, Shabgah AG et al. PD-1/PD-L1 pathway: basic biology and role in cancer immunotherapy. J. Cell. Physiol. 234(10), 16824–16837 (2019).
16.
Das S, Ciombor KK, Haraldsdottir S, Goldberg RM. Promising new agents for colorectal cancer. Curr. Treat. Options Oncol. 19(6), 29 (2018).
17.
Sunshine J, Taube JM. PD-1/PD-L1 inhibitors. Curr. Opin. Pharmacol. 23, 32–38 (2015).
18.
Wolf D. Checkpoint-inhibition in oncology. Oncol. Res. Treat. 39, 27 (2016).
19.
Yaghoubi N, Soltani A, Ghazvini K, Hassanian SM, Hashemy SI. PD-1/ PD-L1 blockade as a novel treatment for colorectal cancer. Biomed. Pharmacother. 110, 312–318 (2019).
20.
Cai J, Qi Q, Qian X et al. The role of PD-1/PD-L1 axis and macrophage in the progression and treatment of cancer. J. Cancer Res. Clin. Oncol. 145(6), 1377–1385 (2019).
21.
Chung KY, Gore I, Fong L et al. Phase II study of the anti-cytotoxic T-lymphocyte-associated antigen 4 monoclonal antibody, tremelimumab, in patients with refractory metastatic colorectal cancer. J. Clin. Oncol. 28(21), 3485–3490 (2010).
22.
Hubbard JM, Patel MR, Bekaii-Saab TS et al. A phase II, open label, randomized, noncomparative study of eFT508 (tomivosertib) alone or in combination with avelumab in subjects with relapsed/refractory microsatellite stable colorectal cancer (MSS CRC). J. Clin. Oncol. 37(Suppl. 15), e14145 (2019).
23.
Le DT, Kim TW, Van Cutsem E et al. Phase II open-label study of pembrolizumab in treatment-refractory, microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: KEYNOTE-164. J. Clin. Oncol. 38(1), 11–19 (2020).
•• Reports the results of an important phase II study of pembrolizumab.
24.
Le DT, Uram JN, Wang H et al. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 372(26), 2509–2520 (2015).
25.
Morris VK, Salem ME, Nimeiri H et al. Nivolumab for previously treated unresectable metastatic anal cancer (NCI9673): a multicentre, single-arm, phase 2 study. Lancet Oncol. 18(4), 446–453 (2017).
26.
Morse MA, Overman MJ, Hartman L et al. Safety of nivolumab plus low-dose ipilimumab in previously treated microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer. Oncologist 24(11), 1453–1461 (2019).
27.
O'Neil BH, Wallmark JM, Lorente D et al. Safety and antitumor activity of the anti-PD-1 antibody pembrolizumab in patients with advanced colorectal carcinoma. PLoS One 12(12), e0189848 (2017).
•• Reports the safety and efficacy of pembrolizumab in advanced CRC.
28.
Overman MJ, Lonardi S, Wong KYM et al. Durable clinical benefit with nivolumab plus ipilimumab in DNA mismatch repair-deficient/microsatellite instability-high metastatic colorectal cancer. J. Clin. Oncol. 36(8), 773–779 (2018).
29.
Overman MJ, McDermott R, Leach JL et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol. 18(9), 1182–1191 (2017).
30.
Segal NH, Kemeny NE, Cercek A et al. Non-randomized phase II study to assess the efficacy of pembrolizumab (Pem) plus radiotherapy (RT) or ablation in mismatch repair proficient (pMMR) metastatic colorectal cancer (mCRC) patients. J. Clin. Oncol. 34(Suppl. 15), 3539 (2016).
31.
Sinicrope FA, Chakrabarti S, Eiring R et al. Clinical outcome of patients with microsatellite instability-high (MSI-H) metastatic colorectal cancer (mCRC) treated with pembrolizumab. J. Clin. Oncol. 36(Suppl. 15), e24127 (2018).
32.
Tarhini A. Immune-mediated adverse events associated with ipilimumab CTLA-4 blockade therapy: the underlying mechanisms and clinical management. Scientifica (Cairo) 2013, 857519 (2013).
33.
Rotte A, Jin JY, Lemaire V. Mechanistic overview of immune checkpoints to support the rational design of their combinations in cancer immunotherapy. Ann. Oncol. 29(1), 71–83 (2018).
34.
Rotte A, Bhandaru M, Zhou Y, Mcelwee KJ. Immunotherapy of melanoma: present options and future promises. Cancer Metastasis Rev. 34(1), 115–128 (2015).
35.
Michot JM, Bigenwald C, Champiat S et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur. J. Cancer 54, 139–148 (2016).
36.
Kanikarla-Marie P, Haymaker C, Parra ER et al. Pilot clinical trial of perioperative durvalumab and tremelimumab in the treatment of resectable colorectal cancer liver metastases. Clin. Cancer Res. 27(11), 3039–3049 (2021).
37.
Chen EX, Jonker DJ, Loree JM et al. Effect of combined immune checkpoint inhibition vs best supportive care alone in patients with advanced colorectal cancer: the Canadian Cancer Trials Group CO.26 Study. JAMA Oncol. 6(6), 831–838 (2020).
38.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int. J. Surg. 8(5), 336–341 (2010).
•• Describes a widely used protocol for conducting systematic literature reviews.
39.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J. Surg. 73(9), 712–716 (2003).
40.
Eisenhauer EA, Therasse P, Bogaerts J et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur. J. Cancer 45(2), 228–247 (2009).
41.
Lipson EJ, Sharfman WH, Drake CG et al. Durable cancer regression off-treatment and effective reinduction therapy with an anti-PD-1 antibody. Clin. Cancer Res. 19(2), 462–468 (2013).
42.
André T, Shiu KK, Kim TW et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N. Engl. J. Med. 383(23), 2207–2218 (2020).
43.
Cohen R, Bennouna J, Meurisse A et al. RECIST and iRECIST criteria for the evaluation of nivolumab plus ipilimumab in patients with microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: the GERCOR NIPICOL phase II study. J. Immunother. Cancer 8(2), e001499 (2020).
• Describes Response Evaluation Criteria in Solid Tumors (RECIST) and immune RECIST (iRECIST) in the treatment evaluation of CRC.
44.
Kim JH, Kim SY, Baek JY et al. A phase II study of avelumab monotherapy in patients with mismatch repair-deficient/microsatellite instability-high or POLE-mutated metastatic or unresectable colorectal cancer. Cancer Res. Treat. 52(4), 1135–1144 (2020).
45.
Xiao Y, Freeman GJ. The microsatellite instable subset of colorectal cancer is a particularly good candidate for checkpoint blockade immunotherapy. Cancer Discov. 5(1), 16 (2015).
46.
Roth MT, Das S. Pembrolizumab in unresectable or metastatic MSI-high colorectal cancer: safety and efficacy. Expert Rev. Anticancer Ther. 21(2), 229–238 (2021).
•• Describes the safety and efficacy of pembrolizumab in CRC with high levels of microsatellite instability (MSI).
47.
Smith KM, Desai J. Nivolumab for the treatment of colorectal cancer. Expert Rev. Anticancer Ther. 18(7), 611–618 (2018).
Information & Authors
Information
Published In
Pages: 203 - 212
PubMed: 35023361
Copyright
© 2021 Future Medicine Ltd.
History
Received: 7 June 2021
Accepted: 26 November 2021
Published online: 13 January 2022
Keywords:
Topics
Authors
Funding Information
Wuxi Key Talents Cultivation Objects: ZDRCPY011
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Efficacy and safety of PD-1/PD-L1 and CTLA-4 immune checkpoint inhibitors in colorectal cancer: a meta-analysis. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0134
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Pengcheng Zhu, Anna Han, Chunhua Quan, Nanomedicine delivery systems remodel the immunosuppressive microenvironment of colorectal cancer: synergistic strategies and mechanisms of targeted immune checkpoint inhibitors, Frontiers in Immunology, 10.3389/fimmu.2026.1882956, 17, (2026).
- Bing Han, Qiong Chai, Qian Chen, Min Liu, Ting Wang, Yu-li Zhang, Zan Li, Zhen Chen, Bo-wang Li, Xian Li, Hua Sui, Qingfeng Tang, Sodium butyrate inhibits colorectal cancer development by reducing M2 macrophage polarization and PD-L1 expression, mSystems, 10.1128/msystems.00692-25, (2025).
- Yu Zhang, Haixia Guan, Xixuan Feng, Mengyan Liu, Jinhuan Shao, Mengchi Liu, Jialei He, Yahui Jin, Jinglin Zhu, Chunli Zheng, Emerging strategies in colorectal cancer immunotherapy: enhancing efficacy and survival, Frontiers in Immunology, 10.3389/fimmu.2025.1616414, 16, (2025).
- Cheng Tong, Yue Wu, Renzhao Wu, New dimensions of PD-1/PD-L1 inhibitor combination therapy in cancer treatment: current advances and future perspectives, Frontiers in Immunology, 10.3389/fimmu.2025.1616872, 16, (2025).
- Long Ma, Wentao Zhou, Xizhi Ma, Xiaopo Li, Qian Zhang, Wenting Ma, Nafei Chen, XiaoTao Zhou, XiaoHui Tang, Preparation and property evaluation of oral colon targeted protein delivery system with sodium alginate and chitosan, Scientific Reports, 10.1038/s41598-025-04983-5, 15, 1, (2025).
- Jin Woong Lee, Carter Kim, Michael J. Poellmann, Zixian Zhu, Seungpyo Hong, The Role of Dendrimers in Improving Antibody and Peptide Biologics for Cancer Treatment, Langmuir, 10.1021/acs.langmuir.5c00934, 41, 27, (17322-17334), (2025).
- Ting Tian, Huan Han, Jingtao Huang, Jun’e Ma, Ruoxi Ran, DBI as a Novel Immunotherapeutic Candidate in Colorectal Cancer: Dissecting Genetic Risk and the Immune Landscape via GWAS, eQTL, and pQTL, Biomedicines, 10.3390/biomedicines13051115, 13, 5, (1115), (2025).
- Ali Rahimi, Zeinab Baghernejadan, Ali Hazrati, Kosar Malekpour, Leila Nejatbakhsh Samimi, Alireza Najafi, Reza Falak, Hossein Khorramdelazad, Combination therapy with immune checkpoint inhibitors in colorectal cancer: Challenges, resistance mechanisms, and the role of microbiota, Biomedicine & Pharmacotherapy, 10.1016/j.biopha.2025.118014, 186, (118014), (2025).
- Weigeng Liu, Clinical efficacy and predictive indicators of cindilizumab combined with XELIRI protocol in advanced colorectal carcinoma patients, American Journal of Translational Research, 10.62347/KZDR9031, 17, 8, (6180-6190), (2025).
- Lloyd Mabonga, Rebecca Leony Fourie, Abidemi Paul Kappo, Sylvester Lyantagaye, Zodwa Dlamini, Emerging treatment approaches for colorectal cancer treatment resistance, Colorectal Cancer Treatment Resistance, 10.1016/B978-0-443-33475-7.00001-9, (107-145), (2025).
- See more