TELEmedicine as an intervention for sepsis in emergency departments: a multicenter, comparative effectiveness study (TELEvISED Study)
Publication: Journal of Comparative Effectiveness Research
Abstract
Sepsis is a life-threatening infection that affects over 1.7 million Americans annually. Low-volume rural hospitals have worse sepsis outcomes, and emergency department (ED)-based telemedicine (tele-ED) has been one promising strategy for improving rural sepsis care. The objective of this study is to evaluate the impact of tele-ED consultation on sepsis care and outcomes in rural ED patients. The TELEvISED study is a multicenter (n = 25) retrospective propensity-matched comparative effectiveness study of tele-ED care for rural sepsis patients in a mature tele-ED network. Telemedicine-exposed patients will be matched with non telemedicine patients using a propensity score to predict tele-ED use. The primary outcome is 28-day hospital free days, and secondary outcomes include adherence with guidelines, mortality and organ failure.
ClinicalTrials.gov: NCT04441944.
Lay abstract
Sepsis is a life-threatening infection that affects over 1.7 million Americans annually. Sepsis patients in low-volume rural hospitals die more often, and emergency department-based real-time video telemedicine has been one promising strategy for improving rural sepsis care. This study evaluates the impact of telemedicine consultation on sepsis care and outcomes in rural sepsis patients. The TELEvISED study is conducted in 25 rural hospitals that participate in a mature rural telemedicine network. Patients for whom telemedicine is used will be compared with those for whom it is not used to measure the effect on mortality, hospital length-of-stay and secondary outcomes including quality of care and severity of illness.
Background & rationale
Sepsis is a life-threatening condition that has doubled in incidence over the past decade, and now affects over 1.7 million Americans annually [1]. As an advanced form of infection-related organ failure, sepsis now constitutes 17% of all in-hospital deaths in the USA at a cost of almost US$24 billion, making it the most expensive acute condition treated in US hospitals [2]. Most sepsis patients are admitted from the emergency department (ED), and aggressive early ED care has been shown to improve sepsis survival [3–6]. The Surviving Sepsis Campaign (SSC) publishes recommendations for sepsis care, consisting of early recognition, early appropriate antibiotics and early resuscitation [5,7–11]. The Centers for Medicare and Medicaid Services, a federal agency that administers the nation’s public healthcare programs, also report a quality metric for patients with sepsis or septic shock (SEP-1) [12]. These facts suggest that the quality of sepsis care is recognized by clinicians, researchers and policy-makers as an important area for improving patient outcomes, and ED is as impactful area to target.
Currently, 19% of Americans live in rural areas, and rural sepsis patients are at particularly high risk of poor outcomes [13–15]. Rural patients prefer to receive care close to home, but they are less likely to receive guideline-adherent sepsis care, and low-volume EDs have 38% higher sepsis mortality [16–24]. Rural EDs are also less likely to be staffed by board-certified emergency physicians, and sepsis is a condition infrequently managed in many low-volume centers [25]. Consequently, rural EDs often rely on inter-hospital transfer to relocate sepsis patients to tertiary hospitals, but even transferred rural sepsis patients have higher mortality than their urban counterparts [26–28]. Patients who bypass rural hospitals to seek care directly in larger centers also have worse outcomes, with an estimated 5.6% increase in mortality compared with those who seek care in their local communities [29]. Early, high-quality care is critical to improve rural sepsis survival, and delays in early care are common and are associated with significantly worse outcomes [30]. This observation suggests that novel strategies are needed to improve outcome in this vulnerable cohort.
Telemedicine has been one promising strategy adopted in many rural EDs to improve both the quality of early emergency care and access to high-quality tertiary networks [31–34]. Telemedicine networks provide a real-time, high-definition, on-demand video connection between a rural hospital and a tertiary hub. A survey of New England hospitals showed that telemedicine services were available in 49% of hospital EDs, with low-volume rural hospitals comprising the majority of tele-ED users [33]. Other rural areas have even higher penetration, with telemedicine being used in over 80% of North Dakota critical access hospital EDs [32]. Telemedicine can maintain access to care despite rural staffing challenges and can increase access to services not typically available in rural centers [35]. Our research group has previously shown that rural telemedicine availability shortens ED door-to-provider times and length-of-stay for trauma patients and shortens the time-to-arrival to a tertiary care center among transferred patients [36,37].
Telemedicine has been used to supplement sepsis care since its inception [38], including improved monitoring and adherence with protocolized sepsis care [39–42]. ED-based telemedicine has also been associated with increased adherence to sepsis guidelines and reduced sepsis-associated transfers between hospitals [43–46]. Each of these reports suggested that telemedicine improved care, but all were preliminary reports of pilot programs that had not yet expanded to scale.
Avera eCARE, a telemedicine network based in Sioux Falls, South Dakota, serves as a telemedicine hub for a network of over 190 EDs in 13 states, and it is the largest rural ED-based telemedicine network in North America. Rural clinicians or nursing staff activate the telemedicine network by depressing a button installed in the ED, and on-demand high-definition video consultation (tele-ED) are provided by a board-certified emergency physician and experienced ED nurse via a video monitor in the patient’s room. This network has been functioning since 2009 and now conducts over 7500 tele-ED video consultations annually. The hub staff have access to the electronic medical record for each participating hospital and can review radiography and EKGs, enter nursing documentation, and enter physician orders. As a telemedicine hub, the network disseminates quality improvement activities across their multiple centers, and sepsis has been one of the focus areas [47]. Therefore, this network provides a unique platform in which to study the impact of telemedicine on sepsis outcomes, which has not rigorously done before.
The objective of this study is to evaluate the impact of tele-ED care on rural sepsis patients. Our goal is to understand what role tele-ED plays in improving guideline adherence and clinical outcomes. Our hypothesis is that telemedicine increases 28-day hospital-free days, through its effect on improving adherence with SSC guidelines.
Methods & analysis
Study design
This study is a multicenter (n = 25) retrospective propensity-matched comparative effectiveness study of tele-ED care for sepsis patients with sepsis. Initially, 30 hospitals were identified for participation, but data use restrictions only permitted 25 to participate. This manuscript is reported in accordance with the Template for Intervention Description and Replication checklist for Population Health and Policy (TIDieR-PHP) and the study was designed using the Strengthening the Reporting of Observational Studies in the Epidemiology (STROBE) statement: Guidelines for Reporting Observational Studies [48,49].
Study population
This study will include all adult (age ≥18 years) sepsis patients who presented to a participating rural ED between 1 August 2016 and 30 June 2019 (Table 1). Data collection/abstraction started on 10 October 2019 and is anticipated to be complete by 30 December 2020. Because of poor sensitivity in diagnosis code-based definitions of sepsis [50], we will use a multistep sepsis definition requiring identification of infection in the ED, organ failure in the ED, at systemic inflammatory response syndrome criteria in the ED and hospital diagnosis of both infection and organ failure (Figure 1). To identify hospital diagnosis of infection and organ failure, we will use the Fleischmann-Struzek approximation of sepsis using International Classification of Diseases, 10th edition, Clinical Modification (ICD-10-CM) discharge diagnoses or an explicit discharge sepsis code (R65.20 or R65.21) [4]. Infection in the ED is defined as the explicit documentation of a source of infection in the ED medical record. Organ failure in the ED is defined based on the Sequential Organ Failure Assessment (SOFA) score of ≥2 points (or a change of two points in those with pre-existing chronic disease) [51]. Systemic inflammatory response syndrome is defined according to the original Bone criteria as at least 2 of the following: body temperature greater than 38°C or less than 36°C; heart rate greater than 90 beats per minute; respiratory rate greater than 22 breaths per minute or pCO2 less than 32 mmHg; or a white blood cell count greater than 12,000 cells/μl, less than 4000 cells/μl or the presence of greater than 10% immature neutrophils [52]. These criteria were selected to parallel the Sepsis-3 definition, but additionally required convincing evidence of recognized infection and objective organ failure in the ED [53]. All records include data on the ED visit and inpatient visits, even when patients are transferred between rural hospitals and tertiary centers. Any patients transferred to a hospital outside the network will be excluded for missing inpatient data.
| Site | Population of city, 2010 (persons) | Annual ED volume, 2019 (visits per year) | ICU | Total inpatient beds (count) | Distance to transfer receiving hospital (miles) | Rurality (Federal Office of Rural Health Policy) | Rurality (rural-urban commuting area) | Rurality (rural-urban continuum code) |
|---|---|---|---|---|---|---|---|---|
| 1 | 1000–1999 | 1500–3499 | No | 23 | 30–59 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 2 | 1000–1999 | 500–1499 | No | 6 | 90–119 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 3 | 2000–4999 | 500–1499 | No | 21 | Less than 30 | Rural | Metropolitan area high commuting with primary commuting flow 30% or more to urbanized area (2.0) | Counties in metropolitan areas of fewer than 250,000 population (3) |
| 4 | 2000–4999 | 500–1499 | No | 18 | 30–59 | Rural | Rural area (10.0) | Less the 2500 urban population, adjacent to a metro area (8) |
| 5 | 1000–1999 | 500–1499 | No | 10 | Over 239 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 6 | 1000–1999 | 3500–7499 | No | 25 | 150–179 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 7 | 1000–1999 | 500–1499 | No | 25 | 150–179 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 8 | 10,000–19,999 | 7500–14,999 | Yes | 25 | 90–119 | Rural | Micropolitan area core (4.0) | Population of 2500–19,999, not adjacent to a metro area (7) |
| 9 | 10,000–19,999 | 7500–14,999 | Yes | 50 | 60–89 | Rural | Micropolitan area core (4.0) | Population of 2500–19,999, not adjacent to a metro area (7) |
| 10 | 10,000–19,999 | 7500–14,999 | Yes | 75 | 60–89 | Rural | Micropolitan area core (4.0) | Population of 2500–19,999, not adjacent to a metro area (7) |
| 11 | 2000–4999 | 1500–3499 | No | 25 | 180–239 | Rural | Small town core (7.0) | Population of 2500–19,999, not adjacent to a metro area (7) |
| 12 | 1000–1999 | 500–1499 | No | 25 | 60–89 | Rural | Rural area with secondary commuting flow (30–49%) to a large urban cluster (10.2) | Less the 2500 urban population, adjacent to a metro area (8) |
| 13 | 20,000–49,999 | 7500–14,999 | Yes | 49 | 180–239 | Rural | Micropolitan area core (4.0) | Population of 20,000 or more, not adjacent to a metro area (5) |
| 14 | 10,000–19,999 | 3500–7499 | Yes | 50 | 180–239 | Rural | Micropolitan area core (4.0) | Population of 2500–19,999, not adjacent to a metro area (7) |
| 15 | 1000–1999 | 500–1499 | No | 25 | 90–89 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 16 | Less than 1000 | Less than 500 | No | 16 | 120–149 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 17 | 2000–4999 | 500–1499 | No | 25 | 30–59 | Rural | Small town core (7.0) | Population of 2500–19,999, not adjacent to a metro area (7) |
| 18 | Less than 1000 | 500–1499 | No | 24 | 60–89 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 19 | 2000–4999 | 7500–14,999 | No | 44 | 90–119 | Rural | Micropolitan area core (4.0) | Population of 2500–19,999, not adjacent to a metro area (7) |
| 20 | Less than 1000 | Less than 500 | No | 25 | 60–89 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 21 | 1000–1999 | 500–1499 | No | 20 | 120–149 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 22 | 2000–4999 | 500–1499 | No | 25 | 30–59 | Rural | Small town core (7.0) | Population of 2500–19,999, not adjacent to a metro area (7) |
| 23 | 1000–1999 | 3500–7499 | No | 17 | 90–119 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
| 24 | 5000–9999 | 1500–3499 | No | 19 | 30–59 | Rural | Small town core (7.0) | Population of 2500–19,999, not adjacent to a metro area (7) |
| 25 | 1000–1999 | 1500–3499 | No | 20 | 90–119 | Rural | Rural area (10.0) | Less the 2500 urban population, not adjacent to a metro area (9) |
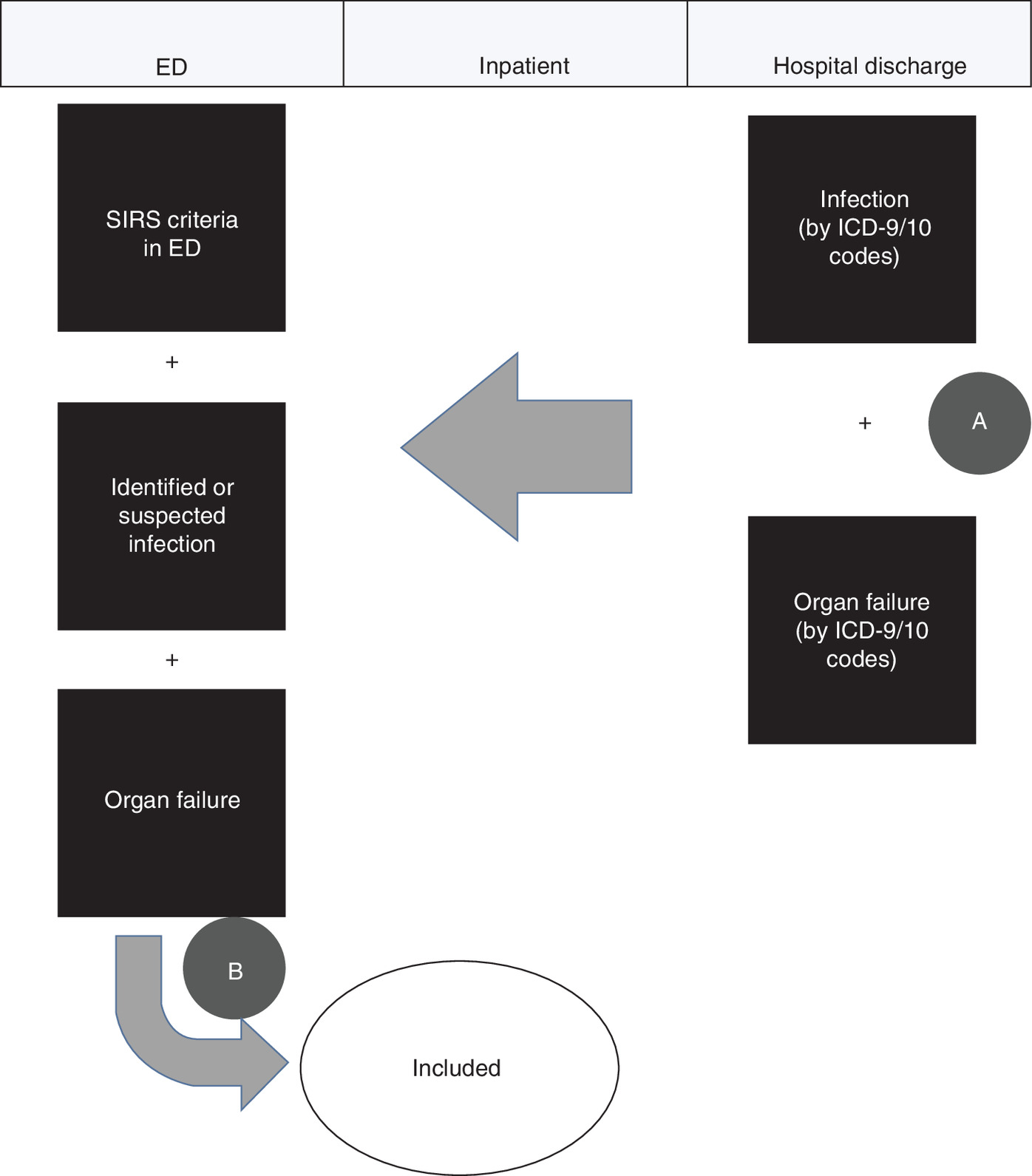
Figure 1. Case selection definition.
(A) First, discharge diagnosis will be screened for sepsis discharge codes. (B) Then the ED electronic medical record will be examined for appropriate clinical criteria to determine the analytic dataset.
ED: Emergency department.
Intervention
As part of standard treatment, Avera eCARE uses established protocols for sepsis management. Standardized nurse-directed sepsis screening is used in all participating rural EDs (Figure 2), and tele-ED consultation is left to the discretion of the local treating clinician. Tele-ED providers are board-certified emergency physicians providing care via remote connection from SD, USA. The telemedicine hub uses computerized decision-support software during tele-ED consultations to guide recommendations for patient care, including fields prompting for sepsis guideline adherence elements (e.g., lactate measurement) and fields for recording completion times for each element of the SSC bundle elements. This real-time checklist aids hub staff in guiding local clinicians through elements of guideline-adherent sepsis care [47]. In addition to real-time clinical support, the telemedicine network sponsors regular continuing education events provided for nurses, advanced practice providers and physicians by remote education. Many clinicians also cite ongoing professional education provided in the context of clinical care as an additional benefit of tele-ED use [54]. The telemedicine service is currently provided in a self-sustaining financial model, and none of the research funding supporting this analysis supports telemedicine clinical operations.

Figure 2. Standardized nurse screening for sepsis for all patients during emergency department triage (prior to telemedicine activation).
ED: Emergency department.
Patient & public involvement
Patients and members of the public were not involved in the development of the research question or study design, and they will not be involved in the conduct of the study.
Data collection
Data collection will be performed using manual chart abstraction in accordance with the methods described by Kaji et al. [55]. Research team members will access the health system electronic medical record in which charts from all participating hospitals are maintained. We will use the original hospital medical record instead of the telemedicine record, because we want to limit ascertainment bias for non telemedicine patients and we have observed previously that telemedicine is rarely referenced in the primary medical record in participating hospitals [56]. Data will be abstracted by three research assistants blinded to the use of telemedicine and details of the study hypothesis, using a standard data collection form with a priori-defined data elements and a coding guide using a Research Electronic Data CAPture (REDCap) secure database (Supplementary Material 1). The case report form was developed by a research team member with significant training in both sepsis data abstraction and sepsis clinical practice, and the case report form was pilot-tested to ensure that data collection aligned with the order in which data could be abstracted efficiently. Real-time error checking and data validation algorithms were built into the database to reduce data entry errors.
All research assistants will have an introductory training to the medical record by a project trainer who has prior experience with sepsis data abstraction and use of the medical record. The trainer will conduct education sessions regarding the data collection tools with each of the three research assistants through one-on-one mentorship over a 4-week dedicated training period. Ten training records will be abstracted by all research assistants, and the trainer will review the data collected for each data element and provide feedback prior to certifying research assistants to abstract additional records. The trainer will continue reviewing portions of data collection until data collection is reliable for every research assistant. After training activities are complete, a 10% sample of all records will be abstracted by both a research assistant and the trainer, and discordance will be reviewed with research assistants on an ongoing basis for training and quality control.
Abstractor inter-rater reliability measurements (Cohen’s kappa) will be conducted on the decision for inclusion in the study cohort and on key data elements (hospital length-of-stay, mortality, timing of each SSC intervention and Acute Physiology and Chronic Health Evaluation Score, 2nd edition [APACHE-II] score). The study team determined a priori that agreement of greater than 90% on cohort inclusion, determination of adherence with the SSC 3-h bundle and outcome variables was acceptable.
Exposure of interest
The primary exposure of interest is tele-ED consultation. Tele-ED use is defined as using video tele-ED during the rural ED visit for sepsis, and it will be defined by identifying the presence of a matching visit in the tele-ED call log maintained by the telemedicine hub. No telemedicine consultations occurring exclusively outside the ED will be included in the tele-ED cohort. Any sepsis case identified in our inclusion criteria for which no tele-ED consultation is identified will comprise a case without tele-ED use.
Outcomes
Primary outcome
The primary clinical outcome is 28-day hospital-free days. This composite outcome is calculated as the hospital length-of-stay subtracted from a total of 28 days, with any in-hospital deaths coded as zero hospital-free days. This outcome has the advantage of incorporating both length-of-stay and the competing outcome of death in the same metric, with larger values always indicating less severe outcomes [57].
Secondary outcomes
Secondary outcomes will include both process-related outcomes and clinical outcomes.
The process outcome of interest is completion of the SSC 3-h bundles from the 2016 guidelines, which requires the following items be completed within 3 h after ED arrival: measure blood lactate level, obtain blood cultures prior to antibiotics, administer appropriate broad-spectrum antibiotics and administer 30 ml/kg crystalloid fluid bolus in the setting of hypotension or elevated lactate. We will also measure completion of the 6-h bundle, requiring documentation of the following elements within 6 h after hospital arrival: vasopressors for hypotension (mean arterial pressure less than 65 mmHg) after fluid resuscitation, and repeat lactate measurement if initial lactate was greater than 2 mmol/l [7,58]. The requirement to reassess resuscitation and volume status was excluded from this metric because of the difficulty in determining completion of this element from the medical record. This primary outcome was determined as a dichotomous outcome of adherent or not adherent with all data elements, but additional outcomes included completion of each of the bundle elements individually. Since the SSC recommendations changed to a 1-h bundle during the data collection period, we will also conduct a sensitivity analysis to measure completion during the more expedited time target [59]. We will analyze the time-to-event data from arrival at the first ED.
Antibiotic appropriateness will be determined based on administration of antibiotics within 3 h of hospital arrival with activity against likely pathogens based on the suspected infection in the initial ED (according to relevant guidelines published by the Infectious Diseases Society of America), or broad-spectrum coverage active against gram-positive and gram-negative bacteria according to the SSC guidelines current at the time of clinical care [7,60–62]. Two emergency medicine clinical pharmacists will review each antibiotic combination from the ED and independently adjudicate antibiotic appropriateness, blinded to the telemedicine status of the case. Discrepancies will be resolved by a third emergency medicine clinical pharmacist. Antibiotic combinations that are broader than recommended by guidelines will be coded as ‘appropriate.’
Additional clinical outcomes of interest will include mortality, mechanical ventilation, 28-day ventilator-free days, vasopressor use, 28-day vasopressor-free days, new renal replacement therapy, inter-hospital transfer, 28-day ICU-free days, ED length-of-stay and time-to-inpatient unit arrival.
Covariates
Additional variables are defined for use in the propensity score and risk-adjustment models. Illness severity will be measured using the APACHE-II score using the worst values of each parameter from the first 24 h of health system contact [63]. Comorbidities will be identified as present from the ED and hospital admission medical record among the following: hypertension, chronic obstructive pulmonary disease, asthma, cirrhosis, history of organ transplant, congestive heart failure, malignancy, HIV infection, diabetes mellitus, end-stage renal disease requiring hemodialysis. Insurance status will be recorded from patient financial records. Shock index will be calculated as (heart rate)/(systolic blood pressure), measured at ED triage [64]. Year will also be recorded to capture temporal trends in sepsis management and outcomes.
Missing data
If data are missing on clinical outcomes, the record will be excluded. Participants not recorded in the call log will be assumed not to have had tele-ED used, and sepsis-related interventions not recorded will be assumed that these interventions did not occur.
Causal model
This study is testing the hypothesis that telemedicine decreases mortality and hospital length of stay by increasing the probability that high-quality sepsis care is delivered, and that the improved quality of care improves clinical outcomes by decreasing organ dysfunction that leads to prolonged hospital stay. The impact of telemedicine is proposed to occur through direct patient care recommendations, training local providers who can provide better care to subsequent patients and improved protocols and standard care elements that improve future care (Figure 3). Because high-quality sepsis care may be delivered without telemedicine and certain patient-level characteristics (e.g., severity of illness, need for transfer) may be associated with telemedicine use, our analytic strategy is designed to reduce the impact of selection bias and confounding.
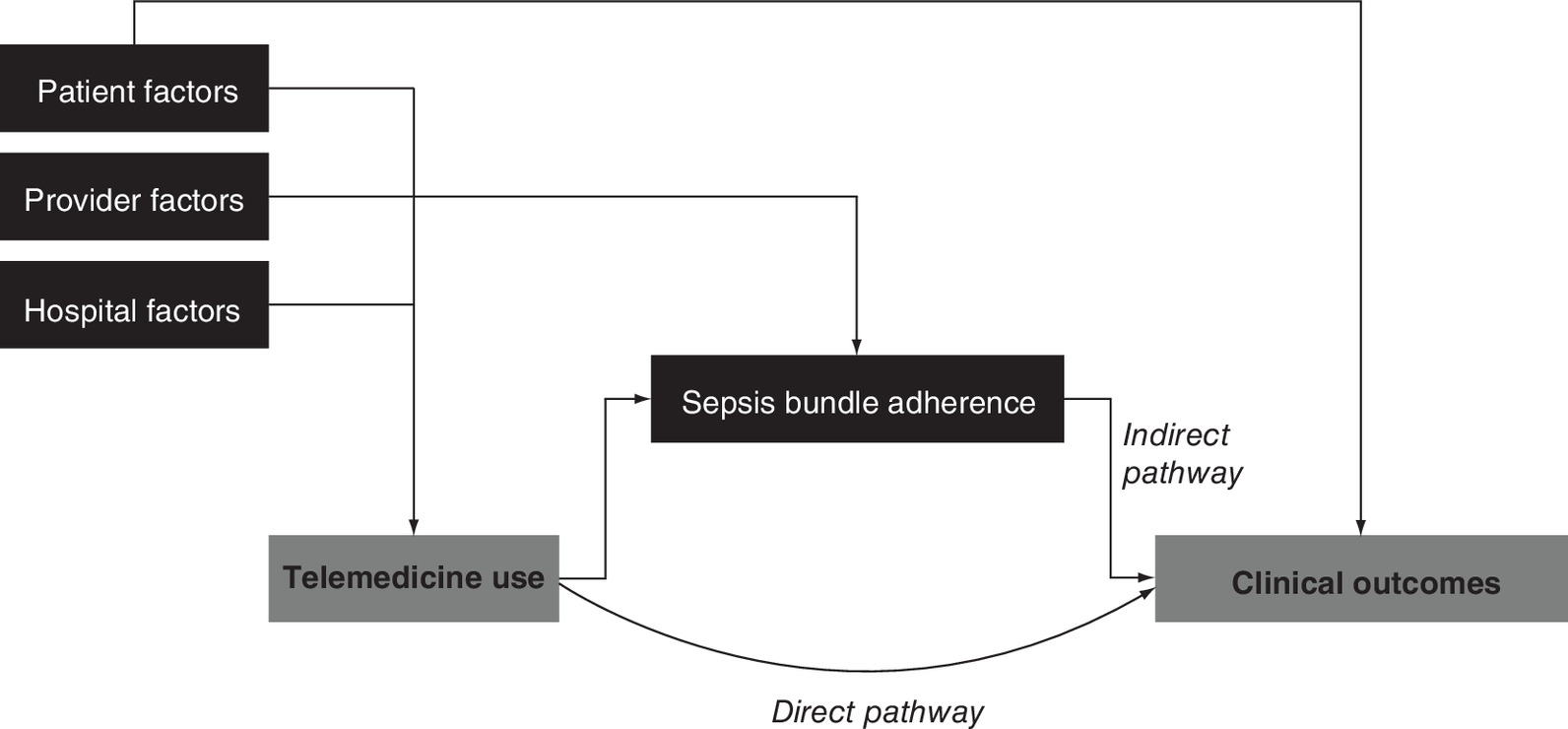
Figure 3. Causal model.
The relationship between telemedicine use and clinical outcomes in rural sepsis patients is complicated and acts through multiple pathways. In addition, patient factors, provider factors and hospital factors confound the causal model.
Proposed statistical methods
Propensity score matching
This study will utilize propensity score matching to pair patients on their likelihood of having telemedicine used. To predict the probability of telemedicine use, a propensity score will be generated using the following patient-oriented candidate variables: illness severity (APACHE-II score), age, comorbidities, shock index, lowest systolic blood pressure in the ED, insurance status, suspected source of infection, procedures performed in the ED (e.g., intubation, central venous line placement), inter-hospital transfer, year and ED provider type (physician vs advanced practice provider).
Initially, we will attempt to match telemedicine-exposed cases to unexposed controls within each hospital. If insufficient unexposed cases within each hospital are available or if the measured covariates are poorly matched between the cohorts, a more broadly defined propensity score will be used, we will add hospital-level covariates to the propensity score to be included in the match: presence of an ICU, rurality (measured using Rural-Urban Commuting Area [RUCA] categories [65]), ED volume and a hospital-specific categorical variable to capture facility-level differences. If this broader score is used, exposed cases will be matched to unexposed cases across the entire cohort.
The predicted probability of telemedicine consultation will be computed for each case (e.g., propensity score) using the described logistic regression model. The distribution of propensity scores for telemedicine-exposed and telemedicine-unexposed cohorts will be analyzed to ensure sufficient overlap in the probability of telemedicine use. Patients for whom telemedicine was used (exposed) will be matched to non telemedicine controls (unexposed) in a 1:1 ratio using an optimal matching algorithm [66]. The distribution of the covariates between the two cohorts will be analyzed with the standardized differences method, with a standardized difference of 0.1 considered significant [67].
Multilevel modeling
Explanatory hierarchical regression models will be built with generalized linear mixed models using a negative binomial distribution in the propensity-matched cohorts. All candidate variables defined for the propensity score will be tested for differences between the propensity-matched cohort. Additionally, organ-specific components of the SOFA score in the ED will be tested for balance across cohorts. If no imbalances exist, then the primary generalized linear mixed model will include the predictor variable of telemedicine use alone and the primary outcome variable of 28-day hospital-free days with a random intercept of the propensity-matched pair (which will be matched within index hospital). If imbalances exist on any adjustment variables, they will be included as additional predictor variables, and variables will be retained in the model based on the Akaike Information Criterion. The model will be examined for interactions and multicollinearity. Similar models will be built for all hypothesis-driven primary and secondary clinical and process-oriented outcomes.
Mediation analysis
If telemedicine is associated with better clinical outcomes and greater adherence with the SSC bundle, mediation analysis will be used to determine what proportion of the clinical effect is attributable to adherence with the bundle. In this model, telemedicine may improve bundle adherence through the indirect pathway, which could improve clinical outcomes, but there may be other non bundle effects of telemedicine (direct pathway, Figure 3). We will use the product of coefficients approach to mediation analysis using standardized coefficients to maintain the same scale in dichotomous predictors and outcomes [68–72]. Because parametric assumptions are violated with this approach, confidence intervals will be estimated using bootstrap resampling for testing significance [73,74]. This analysis is planned using the mediator of the 3-h SSC bundle and its subcomponents, with all defined clinical outcomes.
Sample size
Since the analysis will be conducted using propensity-matched pairs, we propose a power calculation using the paired samples t-test. While hospital-free days is unlikely to be normally distributed, the difference in the outcomes for propensity-matched pairs is expected to be parametric. We defined a clinically meaningful difference in our primary outcome of length-of-stay as 10% based on prior reports [75,76]. We conducted a pilot study of sepsis patients in a smaller cohort of rural hospitals from the same network in February 2016 that reported mean 28-day hospital-free days to be 18.5 days [56]. We calculate that 234 pairs will provide 80% power and 312 pairs will provide 90% power to detect a difference of ≥10% in 28-day hospital-free days between the paired cohorts, assuming α = 0.05; ρ = 0.25 and mean 28-day hospital-free days of 18.5 days (SD 8.2; Figure 4).
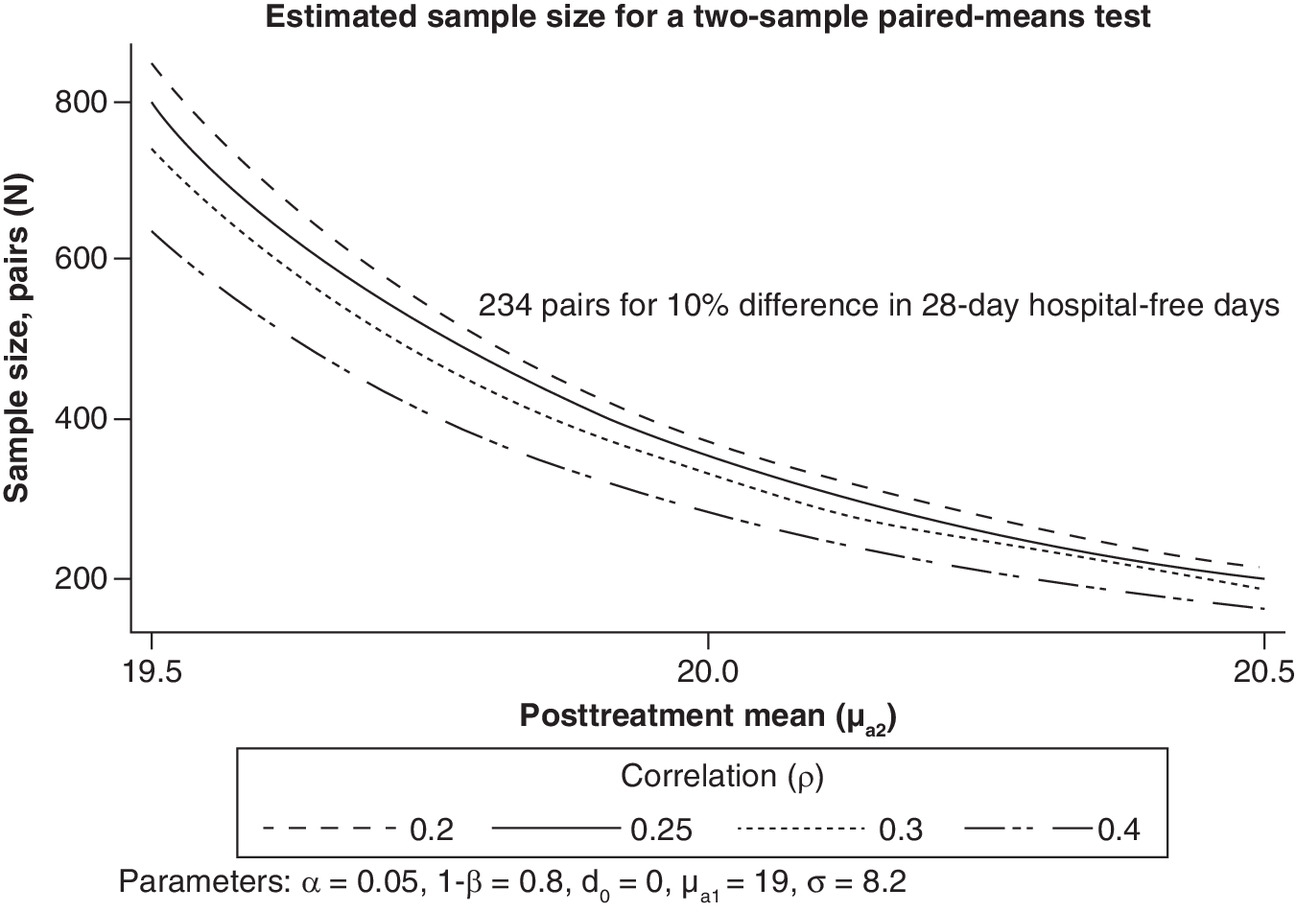
Figure 4. Sample size estimate.
An estimated 234 pairs of propensity-matched cases are required to detect a 10% difference in 28-day hospital-free days with 80% power.
In our 2016 pilot study, 40% of cases identified by ICD-9-CM codes met all inclusion criteria (Figure 1), and 34% used telemedicine [56]. Preliminary query of the medical record of participating hospitals suggests a total available sample of 4,240 records based on discharge diagnoses alone. This sample would predict approximately 576 qualifying sepsis cases for which telemedicine was used.
Anticipated results
Based on prior related analyses, we expect to observe that tele-ED use is associated with improved adherence to SSC guidelines, and that this improvement in adherence will be associated with increased 28-day hospital free days [44,56]. We believe that is reasonable because of the strong published data that SSC bundle adherence is associated with improved outcomes [77–79], but directly demonstrating the causal model involving tele-ED is important, and mediation analysis will help clarify the pathway.
In our mediation analysis, we expect that our effect will be both through the causal pathway of SSC guideline adherence and also through the direct pathway (e.g., through a pathway other than through guideline adherence).
Data storage & management
All data will be entered into a secure password-protected REDCap database accessible only to the study team. For each data element, values will be summarized to identify missingness, outliers and discrepancies. Prior to analysis, data will be deidentified, and protected health information will only be accessed on password-protected computers using a secure encrypted server. The study PI will have access to the final dataset and will take ultimate responsibility for its integrity.
Ethics & dissemination
Ethics approval
The study protocol was reviewed and approved by the institutional review board (IRB) at both the University of Iowa and at Avera eCARE under waiver of informed consent.
Dissemination & data sharing
The results of this study will be disseminated via publication in peer-reviewed journals, presentations at scientific meetings and dissemination of research briefs to participating rural hospitals. Aggregate data will be shared with investigators who make a written request to the study team, and cross-institution collaborations are encouraged. Because of the sparsely populated region where this study is being conducted, hospital-identifiable data could permit identification of individuals, so patient-level data will not be released. The study team will, however, collaborate with investigators to conduct additional analyses while maintaining the security of the dataset.
Strengths & limitations
Strengths
The main strength of this study design is that we are measuring real-world pragmatic impact of tele-ED consultation in a mature telemedicine network. Many telemedicine studies report the results of small single-center pilot programs, or they report the findings from demonstration projects that are not scalable [40,43,45]. The intervention we are testing is operating in a sustainable network at scale.
The second strength is our use of a multicenter network. Rural hospitals vary considerably, so including 25 rural hospitals of different sizes, ownership structures and in different states increases our external validity.
The third strength is our use of propensity score matching and mediation analysis to both account for selection in who received telemedicine and also to test a causal pathway for how patients might be impacted by tele-ED consultation. Testing the hypothesis that tele-ED is associated with clinical outcomes while also measuring the pathway of that proposed effect is robust, because it both adds credibility to any effect on the primary outcome and it allows for subsequent theories on how the relationship between a hub and a rural center might function.
Finally, our use of a clinical outcome is a strength. Our goal in this analysis is to prioritize patient-oriented clinical outcomes over process outcomes, because those clinical outcomes are most relevant to patients, providers and policymakers.
Limitations
The main limitation of our study is its observational design. Because our primary data source is an electronic medical record, we are limited by the quantity and quality of the data recorded in the medical record. Despite our use of propensity score methods, there may be residual confounding by indication not adjusted by the statistical methods we propose. We are limited by our method of data collection, in that a group of data abstractors will be abstracting charts manually. We have designed robust quality control checks into this process, but some data collection errors may be unrecognized. Another limitation is the fact that participating hospitals subscribe to a single tele-ED network. The impact of that network may be different in structure, process and outcomes from other tele-ED networks [80]. All participating hospitals are in the Midwest, which may mean they are different from hospitals in other US regions.
Conclusion
The TELEvISED study is the first large-scale evaluation of the use of tele-ED care to improve the outcomes of sepsis patients in rural hospitals. Identifying alternative strategies for implementation and dissemination of high-quality care in the treatment of critically ill patients in rural EDs is important. Future work will focus on optimizing implementation strategies and better elucidating the mechanisms of impact for those providing rural healthcare.
Strengths and limitations of this study:
•
This study will evaluate the impact of telemedicine in rural emergency departments (EDs) to measure its association with improved quality of ED sepsis care and improved clinical outcomes.
•
The study will use mediation analysis to understand the mechanism by which any improvements in clinical outcomes are observed.
•
The use of a propensity-matched cohort design in a multicenter (n = 25) study of rural EDs is a strength to enhance external validity and limit selection bias.
•
Conducting a study in a mature network where providers choose whether to consult telemedicine may retain some residual confounding.
Author contributions
NM Mohr: conception and study design, acquisition of data, analysis and interpretation of data, drafting and revising the manuscript; KK Harland, MP Jones: conception and study design, analysis and interpretation of data, critically revising the manuscript for important intellectual content; UE Okoro: analysis and interpretation of data, critically revising the manuscript for important intellectual content; BM Fuller: conception and study design, interpretation of data, critically revising the manuscript for important intellectual content; K Campbell: study design; acquisition of data, interpretation of data, critically revising the manuscript for important intellectual content; MB Swanson: analysis and interpretation of data, critically revising the manuscript for important intellectual content; SQ Simpson, EA Parker, K Mueller, E Chrischilles, CR Carpenter: conception and study design, interpretation of data, critically revising the manuscript for important intellectual content; EA Parker: conception and study design, interpretation of data, critically revising the manuscript for important intellectual content; LJ Mack, A Bell, K DeJong: study design, acquisition of data, interpretation of data, critically revising the manuscript for important intellectual content; B Faine, A Zepeski: analysis and interpretation of data, critically revising the manuscript for important intellectual content; MM Ward: conception and study design, acquisition of data, analysis and interpretation of data, critically revising the manuscript for important intellectual content.
Acknowledgments
The authors would like to acknowledge H McKay, M Shaffer and C Wymore (University of Iowa) for their assistance with data collection; K Wallace, MS (University of Iowa) for her assistance with database programming and development; M Schmidt (Avera eCARE) for her expertise in interpreting medical records and her assistance with training and quality control activities; and W Berg, PhD (Avera eCARE) for his help with data management and medical record queries.
Financial & competing interests disclosure
This study is supported by the Agency for Healthcare Research and Quality (K08HS025753), the Institute for Clinical and Translational Science at the University of Iowa through a grant from the National Center for Advancing Translational Sciences at the NIH (UL1TR002537), and the Rural Telehealth Research Center through a grant from the Federal Office of Rural Health Policy, Health Resources and Services Administration (U1CRH29074). These contents are solely the responsibility of the authors and do not necessarily reflect the views of the Agency for Healthcare Research and Quality, and National Institutes of Health, or the Federal Office of Rural Health Policy. LJM, AB, and KD declare that they are employed by Avera eCARE, an organization that provides tele-ED services to rural hospitals. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval for all human subjects research activities.
Supplementary Material
File (supplementary material.pdf)
- Download
- 510.50 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Rhee C, Dantes R, Epstein L et al. Incidence and trends of sepsis in US hospitals using clinical vs claims data, 2009–2014. JAMA 318(13), 1241–1249 (2017).
2.
Hall MJ, Williams SN, Defrances CJ, Golosinskiy A. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief 62, 1–8 (2011).
3.
Filbin MR, Arias SA, Camargo CA Jr, Barche A, Pallin DJ. Sepsis visits and antibiotic utilization in US Emergency Departments. Crit. Care Med. 42(3), 528–535 (2014).
4.
Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 29(7), 1303–1310 (2001).
5.
Rivers E, Nguyen B, Havstad S et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N. Engl. J. Med. 345(19), 1368–1377 (2001).
• First paper to show the impact of early, aggressive emergency department-based care at improving survival in critically ill patients with sepsis.
6.
Rivers EP. Point: adherence to early goal-directed therapy: does it really matter? Yes. After a decade, the scientific proof speaks for itself. Chest 138(3), 476–480; discussion 484–485 (2010).
7.
Rhodes A, Evans LE, Alhazzani W et al. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Intens. Care Med. 43(3), 304–377 (2017).
8.
Kent N, Fields W. Early recognition of sepsis in the emergency department: an evidence-based project. J. Emerg. Nurs. 38(2), 139–143 (2012).
9.
Gaieski DF, Mikkelsen ME, Band RA et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit. Care Med. 38(4), 1045–1053 (2010).
10.
Kumar A, Roberts D, Wood KE et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 34(6), 1589–1596 (2006).
11.
ProCESS Investigators; Yealy DM, Kellum JA, Huang DT et al. A randomized trial of protocol-based care for early septic shock. N. Engl. J. Med. 370(18), 1683–1693 (2014).
12.
Severe Sepsis and Septic Shock, Sepsis Bundle Project (SEP-1), National Hospital Inpatient Quality Measures. In: Specifications Manual for National Hospital Inpatient Quality Measures. Center for Medicare & Medicaid Services Baltimore, MD, USA, 1–60 (2017).
• The Centers for Medicare and Medicaid Services has designed a quality measure for evaluating the appropriateness of early sepsis care that incorporates elements of the Surviving Sepsis Campaign guidelines, and our data collection is based on this national quality metric.
13.
Gaieski DF, Edwards JM, Kallan MJ, Mikkelsen ME, Goyal M, Carr BG. The relationship between hospital volume and mortality in severe sepsis. Am. J. Respir. Crit. Care Med. 190(6), 665–674 (2014).
14.
Nguyen Y-L, Wallace DJ, Yordanov Y et al. The volume-outcome relationship in critical care: a systematic review and meta-analysis. Chest 148(1), 79–92 (2015).
15.
Urban and Rural Classification and Urban Areas Criteria (2010). www.census.gov/programs-surveys/geography/guidance/geo-areas/urban-rural/2010-urban-rural.html
16.
Glickman SW, Krubert C, Koppenhaver J, Glickman LT, Schulman KA, Cairns CB. Increased rate of central venous catheterization procedures in community EDs. Am. J. Emerg. Med. 28(2), 208–212 (2010).
17.
Djogovic D, Green R, Keyes R et al. Canadian Association of Emergency Physicians Sepsis Treatment Checklist: Optimizing Sepsis Care in Canadian Emergency Departments. CJEM 14(1), 36–39 (2012).
18.
Salhi RA, Edwards JM, Gaieski DF, Band RA, Abella BS, Carr BG. Access to care for patients with time-sensitive conditions in Pennsylvania. Ann. Emerg. Med. 63(5), 572–579 (2014).
19.
Faine BA, Noack JM, Wong T et al. Interhospital transfer delays appropriate treatment for patients with severe sepsis and septic shock: a retrospective cohort study. Crit. Care Med. 43(12), 2589–2596 (2015).
20.
Burenheide K. Developing Disease State Management Guidelines for Rural Health Care (2008). www.mwcritcare.org
21.
Kaukonen K, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA 311(13), 1308–1316 (2014).
22.
Arise, Anzics. The outcome of patients with sepsis and septic shock presenting to emergency departments in Australia and New Zealand. Crit. Care Resus. 9(1), 8–18 (2007).
23.
Kocher KE, Haggins AN, Sabbatini AK, Sauser K, Sharp AL. Emergency department hospitalization volume and mortality in the United States. Ann. Emerg. Med. 64(5), 446–457 (2014).
24.
Mohr NM, Wong TS, Faine B, Schlichting A, Noack J, Ahmed A. Discordance between patient and clinician experiences and priorities in rural interhospital transfer: a mixed methods study. J. Rural Health 32(1), 25–34 (2016).
25.
Groth H, House H, Overton R, Deroo E. Board-certified emergency physicians comprise a minority of the emergency department workforce in iowa. West J. Emerg. Med. 14(2), 186–190 (2013).
26.
Iwashyna TJ. The incomplete infrastructure for interhospital patient transfer. Crit. Care Med. 40(8), 2470–2478 (2012).
27.
Golestanian E, Scruggs JE, Gangnon RE, Mak RP, Wood KE. Effect of interhospital transfer on resource utilization and outcomes at a tertiary care referral center. Crit. Care Med. 35(6), 1470–1476 (2007).
28.
Mohr NM, Harland KK, Shane DM, Ahmed A, Fuller BM, Torner JC. Inter-hospital transfer is associated with increased mortality and costs in severe sepsis and septic shock: an instrumental variables approach. J. Crit. Care 36, 187–194 (2016).
29.
Mohr NM, Harland KK, Shane DM et al. Rural patients with severe sepsis or septic shock who bypass rural hospitals have increased mortality: an instrumental variables approach. Crit. Care Med. 45(1), 85–93 (2017).
30.
Van Zanten AR, Brinkman S, Arbous MS, Abu-Hanna A, Levy MM, De Keizer NF. Guideline bundles adherence and mortality in severe sepsis and septic shock. Crit. Care Med. 42(8), 1890–1898 (2014).
31.
Ward MM, Ullrich F, Mueller K. Extent of telehealth use in rural and urban hospitals. Rural Policy Brief, 1(2014 4), 1–4 (2014).
32.
Mohr N, Harland K, Chrischilles E et al. Telemedicine penetration and consultation among rural trauma patients in critical access hospital emergency departments in North Dakota. Rural Telehealth Res. Center Res. Policy Brief 2016(2), 1–4 (2016).
33.
Zachrison KS, Hayden EM, Schwamm LH et al. Characterizing New England emergency departments by telemedicine use. West J. Emerg. Med. 18(6), 1055–1060 (2017).
34.
Hollander JE, Carr BG. Virtually perfect? Telemedicine for Covid-19. N. Engl. J. Med. 382(18), 1679–1681 (2020).
35.
Potter AJ, Mueller KJ, Mackinney AC, Ward MM. Effect of tele-emergency services on recruitment and retention of US rural physicians. Rural Remote Health 14(3), 2787 (2014).
36.
Mohr NM, Vakkalanka JP, Harland KK et al. Telemedicine use decreases rural emergency department length of stay for transferred North Dakota trauma patients. Telemed. J. E. Health 24(3), 194–202 (2018).
37.
Mohr NM, Young T, Harland KK et al. Emergency department telemedicine shortens rural time-to-provider and emergency department transfer times. Telemed. J. E. Health 24(8), 582–593 (2018).
38.
Mohr NM, Hurst EK, Mackinney AC, Nash EC, Carr BG, Skow B. Telemedicine for Early Treatment of Sepsis. In: Telemedicine in the Intensive Care Unit. Koenig MA (Ed.). Springer International Publishing, NY, USA, 255–280 (2019).
39.
Rincon TA, Manos EL, Pierce JD. Telehealth intensive care unit nurse surveillance of sepsis. Comput. Inform. Nurs. 35(9), 459–464 (2017).
40.
Loyola S, Wilhelm J, Fornos J. An innovative approach to meeting early goal-directed therapy using telemedicine. Crit. Care Nurs. Q. 34(3), 187–199 (2011).
41.
Deisz R, Rademacher S, Gilger K et al. Additional telemedicine rounds as a successful performance-improvement strategy for sepsis management: observational multicenter study. J. Med. Internet Res. 21(1), e11161 (2019).
42.
Rincon TA, Bourke G, Seiver A. Standardizing sepsis screening and management via a tele-ICU program improves patient care. Telemed. J. E. Health 17(7), 560–564 (2011).
43.
Agarwal AK, Gaieski DF, Perman SM et al. Telemedicine REsuscitation and Arrest Trial (TREAT): a feasibility study of real-time provider-to-provider telemedicine for the care of critically ill patients. Heliyon 2(4), e00099 (2016).
44.
Mohr NM, Campbell KD, Swanson MB, Ullrich F, Merchant KA, Ward MM. Provider-to-provider telemedicine improves adherence to sepsis bundle care in community emergency departments. J. Telemed. Telecare (.2020) (Epub ahead of print).
•• Telemedicine in emergency departments has been shown previously to improve adherence with international sepsis care guidelines, in a cohort of multiple telemedicine networks. In the prior paper, however, patient-oriented clinical outcomes were not able to be evaluated.
45.
Machado SM, Wilson EH, Elliott JO, Jordan K. Impact of a telemedicine eICU cart on sepsis management in a community hospital emergency department. J. Telemed. Telecare 24(3), 202–208 (2018).
46.
Ilko SA, Vakkalanka JP, Ahmed A, Harland KK, Mohr NM. Central venous access capability and critical care telemedicine decreases inter-hospital transfer among severe sepsis patients: a mixed methods design. Crit. Care Med. 47(5), 659–667 (2019).
47.
Mohr N, Skow B, Wittrock A et al. Improving access to high quality sepsis care in a South Dakota emergency telemedicine network. Rural Telehealth Res. Center Res. Policy Brief 2017(8), 1–4 (2017).
•• The participating telemedicine network has implemented sepsis quality of care pathways previously, upon which the proposed evaluation is built.
48.
Campbell M, Katikireddi SV, Hoffmann T, Armstrong R, Waters E, Craig P. TIDieR-PHP: a reporting guideline for population health and policy interventions. BMJ 361, k1079 (2018).
49.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370(9596), 1453–1457 (2007).
50.
Iwashyna TJ, Odden A, Rohde J et al. Identifying patients with severe sepsis using administrative claims: patient-level validation of the angus implementation of the international consensus conference definition of severe sepsis. Med. Care 52(6), e39–43 (2014).
51.
Vincent JL, Moreno R, Takala J et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the working group on sepsis-related problems of the European Society of Intensive Care Medicine. Intens. Care Med. 22(7), 707–710 (1996).
52.
Bone RC, Balk RA, Cerra FB et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 101(6), 1644–1655 (1992).
53.
Singer M, Deutschman CS, Seymour C et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 315(8), 801–810 (2016).
54.
Zhu X, Merchant KaS, Mohr NM, Wittrock AJ, Bell AL, Ward MM. Real-time learning through telemedicine enhances professional training in rural emergency departments. Telemed. J. E. Health (2020) (Epub ahead of print).
55.
Kaji AH, Schriger D, Green S. Looking through the retrospectoscope: reducing bias in emergency medicine chart review studies. Ann. Emerg. Med. 64(3), 292–298 (2014).
56.
Campbell K, Vakkalanka P, Wittrock A et al. Telemedicine is associated with improved antibiotic appropriateness in rural emergency departments (oral presentation). Society for Education and Research in Connected Health (SEARCH) (2017).
57.
Yehya N, Harhay MO, Curley MaQ, Schoenfeld DA, Reeder RW. Reappraisal of ventilator-free days in critical care research. Am. J. Respir. Crit. Care Med. 200(7), 828–836 (2019).
58.
Surviving Sepsis Campaign: Updated Bundles in Response to New Evidence (2015). www.survivingsepsis.org/SiteCollectionDocuments/SSC_Bundle.pdf
59.
Levy MM, Evans LE, Rhodes A. The surviving sepsis campaign bundle: 2018 update. Intens. Care Med. 44(6), 925–928 (2018).
60.
Metlay JP, Waterer GW, Long AC et al. Diagnosis and treatment of adults with community-acquired pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 200(7), e45–e67 (2019).
61.
Gupta K, Hooton TM, Naber KG et al. International Clinical Practice Guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 52(5), e103–e120 (2011).
62.
Stevens DL, Bisno AL, Chambers HF et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 59(2), e10–e52 (2014).
63.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit. Care Med. 13(10), 818–829 (1985).
64.
Berger T, Green J, Horeczko T et al. Shock index and early recognition of sepsis in the emergency department: pilot study. West J. Emerg. Med. 14(2), 168–174 (2013).
65.
EconomicResearch Service. Rural-urban commuting area codes (2020). www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx
66.
Austin PC. A comparison of 12 algorithms for matching on the propensity score. Stat. Med. 33(6), 1057–1069 (2014).
67.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 46(3), 399–424 (2011).
68.
Sobel M. Asymptotic confidence intervals for indirect effects in structural equation models. In: Sociological Methodology, Leinhardt S (Ed.). American Sociological Association, Washington DC, USA, 290–312 (1982).
69.
Mackinnon DP, Fairchild AJ, Fritz MS. Mediation analysis. Ann. Rev. Psychol. 58, 593 (2007).
70.
Iacobucci D. Mediation analysis and categorical variables: the final frontier. J. Consumer Psychol. 22(4), 582–594 (2012).
71.
Imai K, Keele L, Tingley D. A general approach to causal mediation analysis. Psychol. Meth. 15(4), 309–334 (2010).
72.
Valeri L, Vanderweele TJ. Mediation analysis allowing for exposure-mediator interactions and causal interpretation: theoretical assumptions and implementation with SAS and SPSS macros. Psychol. Meth. 18(2), 137–150 (2013).
73.
Linden A, Karlson KB. Using mediation analysis to identify causal mechanisms in disease management interventions. Health Serv. Outcomes Res. Meth. 13, 86–108 (2013).
74.
Williams J, Mackinnon DP. Resampling and distribution of the product methods for testing indirect effects in complex models. Struct. Equ. Modeling 15(1), 23–51 (2008).
75.
Weiss AJ, Elixhauser A. Overview of hospital stays in the United States, 2012 (Statistical Brief #180). 1–14 (2014).
76.
Rotter T, Kugler J, Koch R et al. A systematic review and meta-analysis of the effects of clinical pathways on length of stay, hospital costs and patient outcomes. BMC Health Serv. Res. 8(1), 265 (2008).
77.
Rhodes A, Phillips G, Beale R et al. The Surviving Sepsis Campaign bundles and outcome: results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study). Intens. Care Med. 41(9), 1620–1628 (2015).
78.
Levy MM, Dellinger RP, Townsend SR et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intens. Care Med. 36(2), 222–231 (2010).
79.
Levy MM, Rhodes A, Phillips GS et al. Surviving Sepsis Campaign: association between performance metrics and outcomes in a 7.5-year study. Intens. Care Med. 40(11), 1623–1633 (2014).
80.
Donabedian A. The quality of care. How can it be assessed? JAMA 260(12), 1743–1748 (1988).
Information & Authors
Information
Published In
Copyright
© 2021 Future Medicine Ltd.
History
Received: 7 July 2020
Accepted: 20 November 2020
Published online: 20 January 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
TELEmedicine as an intervention for sepsis in emergency departments: a multicenter, comparative effectiveness study (TELEvISED Study). (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0141
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Cole Wymore, Eliezer Santos León, Priyanka Vakkalanka, Uche Okoro, Karisa K. Harland, Brian M. Fuller, Kalyn Campbell, Morgan B. Swanson, Brett Faine, Anne Zepeski, Edith A. Parker, Luke J. Mack, Amanda Bell, Katie DeJong, Keith Mueller, Elizabeth Chrischilles, Christopher R. Carpenter, Kelli Wallace, Michael P. Jones, Marcia M. Ward, Nicholas M. Mohr, The association between interhospital transfer and sepsis guideline adherence among rural emergency department patients, PLOS One, 10.1371/journal.pone.0351133, 21, 7, (e0351133), (2026).
- Al Anoud Abdul, Mohamed Mustaf Ahmed, Elsayed S. Moubarak, Majd Oweidat, Emma Cravo, Farah Deeba, Mohammed Alsabri, Pediatric Shock in Low-Middle-Income Countries: Evidence-Based Strategies for Recognition, Resuscitation, and System-Level Adaptations, Current Treatment Options in Pediatrics, 10.1007/s40746-026-00367-7, 12, 1, (2026).
- Joshua Cunningham, Niklas Bobrovitz, Ajaykumar Shanmugaraj, Dean Giustini, Dylan Collins, Defining emergency physicians’ consultative roles in emergency care: a scoping review, Canadian Journal of Emergency Medicine, 10.1007/s43678-025-01025-x, 28, 2, (129-137), (2025).
- Anna M. Kaldjian, Priyanka Vakkalanka, Uche Okoro, Cole Wymore, Karisa K. Harland, Kalyn Campbell, Morgan B. Swanson, Brian M. Fuller, Brett Faine, Anne Zepeski, Edith A. Parker, Luke Mack, Amanda Bell, Katie DeJong, Kelli Wallace, Keith Mueller, Elizabeth Chrischilles, Christopher R. Carpenter, Michael P. Jones, Marcia M. Ward, Nicholas M. Mohr, The Effect of Sepsis Recognition on Telemedicine Use in Rural Emergency Department Sepsis Treatment, Telemedicine and e-Health, 10.1089/tmj.2024.0281, 31, 7, (848-857), (2025).
- Nicholas M. Mohr, Kimberly A.S. Merchant, Brian M. Fuller, Brett Faine, Luke Mack, Amanda Bell, Katie DeJong, Edith A. Parker, Keith Mueller, Elizabeth Chrischilles, Christopher R. Carpenter, Michael P. Jones, Steven Q. Simpson, Marcia M. Ward, The role of telehealth in sepsis care in rural emergency departments: A qualitative study of emergency department sepsis telehealth user perspectives, PLOS One, 10.1371/journal.pone.0321299, 20, 4, (e0321299), (2025).
- Benjamin Wilkinson, Eliezer Santos León, J. Priyanka Vakkalanka, Azeemuddin Ahmed, Karisa K. Harland, Brian M. Fuller, Kalyn Campbell, Morgan B. Swanson, Brett Faine, Anne Zepeski, Luke Mack, Amanda Bell, Katie DeJong, Kelli Wallace, Edith A. Parker, Keith Mueller, Elizabeth Chrischilles, Christopher R. Carpenter, Michael P. Jones, Steven Q. Simpson, Nicholas M. Mohr, Longer Total Interhospital Transfer Times for Rural Sepsis Patients Not Associated with Increased Mortality, Prehospital Emergency Care, 10.1080/10903127.2024.2447044, 29, 8, (1111-1116), (2025).
- Andreas Edel, Kristina Fuest, George Karlis, Principles and Management of Sepsis, Best 2022 Clinical Cases in Intensive Care Medicine, 10.1007/978-3-031-36398-6_1, (3-14), (2023).
- Nicholas M. Mohr, Uche Okoro, Karisa K. Harland, Brian M. Fuller, Kalyn Campbell, Morgan B. Swanson, Cole Wymore, Brett Faine, Anne Zepeski, Edith A. Parker, Luke Mack, Amanda Bell, Katie DeJong, Keith Mueller, Elizabeth Chrischilles, Christopher R. Carpenter, Kelli Wallace, Michael P. Jones, Marcia M. Ward, Outcomes Associated With Rural Emergency Department Provider-to-Provider Telehealth for Sepsis Care: A Multicenter Cohort Study, Annals of Emergency Medicine, 10.1016/j.annemergmed.2022.07.024, 81, 1, (1-13), (2023).
- Nicholas M Mohr, Allison R Schuette, Fred Ullrich, Luke J Mack, Katie DeJong, Carlos A Camargo Jr, Kori S Zachrison, Krislyn M Boggs, Adam Skibbe, Amanda Bell, Mark Pals, Dan M Shane, Knute D Carter, Kimberly AS Merchant, Marcia M Ward, An economic and health outcome evaluation of telehealth in rural sepsis care: a comparative effectiveness study, Journal of Comparative Effectiveness Research, 10.2217/cer-2022-0019, 11, 10, (703-716), (2022).