A Delphi panel on treatment of high disease activity relapsing remitting multiple sclerosis in the Netherlands
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To gain insight into current treatment and barriers to optimal treatment for high disease activity relapsing remitting multiple sclerosis (MS) in the Netherlands. Materials & methods: A two-round Delphi panel using an online questionnaire was conducted. Seven MS neurologists from diverse locations in the Netherlands were invited to participate. Result: Out of the seven MS neurologists, five completed both questionnaire rounds. Conclusion: Effectiveness and side effects along with patient’s lesion load were the most important factors for choosing a disease modifying therapy (DMTs). Respondents felt restricted to optimally treat their patients due to reimbursement restrictions for certain disease modifying therapies, although agreed that satisfactory treatment options are currently available. The answers show consensus between the participating MS neurologists with high certainty of answers.
Multiple sclerosis (MS) is a chronic and debilitating autoimmune disorder of the central nervous system (CNS), in which T and B cells are believed to play a major pathophysiological role. It can result in neurological impairment and severe disability [1–3]. In most MS patients, the first symptoms appear around the age of 20–40 years. Overall, women are affected approximately twice as often as men, except in the primary-progressive form of the disease, where no sex difference appears. Most patients (~85%) first present with relapsing remitting MS (RRMS), which later progresses into secondary-progressive MS. Within 10 years, without treatment, more than 50% of patients who suffer from RRMS eventually develop secondary-progressive MS, which is characterized by gradual progression of disability with or without superimposed relapses [4]. A subset of the RRMS population can be categorized as high disease activity (HDA) defined as RRMS with two or more relapses within 1 year regardless of received treatment with disease modifying therapies (DMTs) or with one relapse in the previous year and at least one T1 Gd+ lesion or nine or more T2 lesions, while on therapy with other DMTs [5].
Currently, there is no cure for MS, however, the aberrant activity of T and B cells observed in MS has been shown to be affected by immunomodulatory treatments referred to as DMTs, which can favorably alter the course of the disease. The goal of treatment of MS is to reduce the rate and severity of relapses to delay disease progression by preventing accumulation of disability and to reduce brain lesions identified with MRI [6].
The Dutch treatment guidelines at the time of writing of the article for MS date from 2012 and, therefore, do not cover treatments that have been introduced after 2012 [6]. The guidelines do no longer reflect the current general MS treatment landscape in the Netherlands, nor the treatment landscape specifically for (HDA) RRMS. Furthermore, in the Netherlands, there are reimbursement restrictions in place for the DMTs cladribine tablets and fingolimod. These restrictions limit the use of these treatments to patients with HDA RRMS that have not responded to at least one DMT, while their registered indications include treatment of HDA RRMS regardless of prior treatment status [5,7–9]. In addition, the reimbursement of natalizumab and alemtuzumab is also limited in the Netherlands to treatment of patients with HDA RRMS that have not responded to interferon β or glatiramer, while its registered indication does include treatment of HDA RRMS, regardless of prior treatment status if MS is rapidly evolving and severe [10,11].
The objective of this study was to set up a Delphi study with panel experts to provide insight into the current treatment pathway of HDA RRMS and any barriers for optimal treatment in the Netherlands.
Materials & methods
In general, a Delphi study aims to reach consensus between experts on a specific topic. The panel participants reply in several ‘rounds’ to a variety of questions on the topic of interest. After each round, participants receive feedback from the overall group. These rounds repeat themselves to reduce the number of responses until ‘consensus’ is achieved. There is no guidance in the scientific literature on what constitutes a robust panel size for a Delphi study, nor are there clear criteria how a sample size choice should be judged. Therefore, Delphi studies have been performed with a wide variety of panel sizes. However, the criteria for selecting the panellists are important (e.g., expertise and geographic spread) [12–16].
A two-round Delphi study was conducted using an anonymous online questionnaire to reduce the number of responses until ‘consensus’ was achieved. In this study, seven MS neurologists, with a representative geography spread over the Netherlands, were approached for participation. An invitation e-mail was sent describing the background, objectives and timelines of the process. The first-round’s questionnaire was shared with all seven MS neurologists. For the second round of the Delphi study, only the MS neurologists that completed the first-round questionnaire were invited for the second round. The findings of the MS neurologists that completed the first and second round of the questionnaire were included in the analysis. The first- and second-round questionnaires were administered through an online portal, copies (in Dutch) of the questionnaire are included in the online Supplementary data.
First-round questionnaire
In the first-round questionnaire, the following topics relating to the Dutch current treatment pathway in (HDA) RRMS were included:
•
Characteristics of the treatment practice of the respondents;
•
Percentage of HDA RRMS patients per line of treatment (naive for DMTs, previously treated with one DMT, previously treated with two or more DMTs);
•
The treatments that would be given in a situation in which there would be no reimbursement restrictions to DMT-naive patients, and patients previously treated with one DMT;
•
The criteria that are most important in choosing the treatment for HDA RRMS patients;
•
Whether the current situation with reimbursement restrictions on certain DMTs allows for optimal treatment of HDA RRMS patients;
•
The satisfaction of the respondents with the current treatment options available in the Netherlands for DMT-naive patients with HDA RRMS;
•
The proportion of DMT-naive HDA RRMS patients in which treatment switching occurs due to lack of efficacy or side effects within 12 months of treatment initiation, and the proportion of patients in which this could have been prevented, if certain DMTs would have been reimbursed;
•
A case study describing a patient for which respondents were asked to indicate how they would treat this patient, the reasons for choosing this treatment, and if they experience any treatment limitations.
Second-round questionnaire
After the first-round questionnaire, the results were analyzed and a second-round of questionnaires was sent out. The second-round questionnaire contained two additional elements. First, the average and the 90% CI of the results from the first round were presented. The respondents were requested to answer again the questions from the first round keeping these group results in mind. Second, for all questions except those relating to the characteristics of the respondents and their treatment practice, the respondents were also asked to rank how certain they were of their answer on a four-point scale, with the following levels: certain, low risk of being wrong (±10% deviation possible); fairly certain, some risk of being wrong (±20% deviation possible); not very certain, substantial risk of being wrong (±40% deviation possible); uncertain, high risk of being wrong (>40% deviation possible). For the certainty scores, the average certainty score and the range in scores (minimum–maximum score) is presented. The lower the average score is for a question, the more certain the respondents were of their answer.
Results
Out of seven MS neurologists, five completed both the first and second round of the questionnaire.
Respondent characteristics
In their treatment practice, respondents treat on average 60 (90% CI: 50–70) MS patients per month, of which 72% (90% CI: 55–89%) are treated with DMTs and 26% (90% CI: 15–37%) are characterized as HDA RRMS. Of these HDA RRMS patients, 31% (90% CI: 19–43%) have not been previously treated with DMTs, 47% (90% CI: 40–54%) have been previously treated with 1 DMT and 22% (90% CI: 16–28%) have been previously treated with ≥2 DMTs. Respondents reported an average certainty score of 1.8 (range 1–2) for the patients’ treatment history with DMTs, indicating respondents that were fairly certain of their answer (some risk of being wrong [±20% deviation possible]).
Ideal treatment for patients with HDA RRMS
Respondents were asked to describe their ideal treatment for HDA RRMS patients (i.e., if reimbursement would not play a role), for patients who have not been previously treated with DMTs and for patients who have been previously treated with one DMT. The top three choices were natalizumab, alemtuzumab and cladribine tablets for patients not previously treated with DMTs, and natalizumab, ocrelizumab and alemtuzumab for patients previously treated with one DMT (Figure 1; error bars indicate a standard error). Respondents reported an average certainty score of 1.2 (range 1–2), indicating that respondents were certain of their answer (low risk of being wrong [±10% deviation possible]).
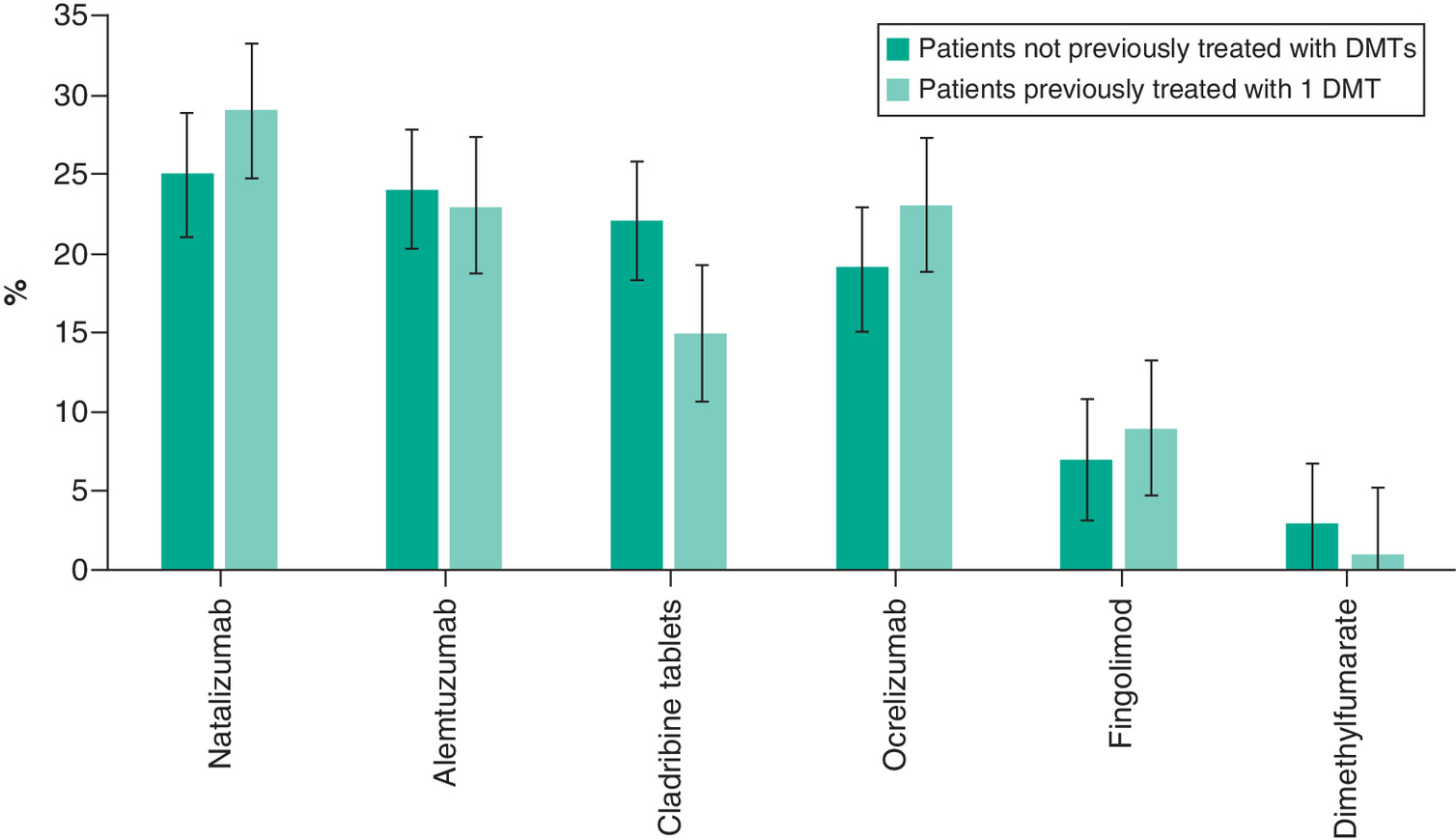
Figure 1. Preferred treatment options for high disease activity relapsing remitting multiple sclerosis patients in an ideal situation where reimbursement status does not play a role (error bars indicate a standard error).
DMT: Disease modifying therapy.
Criteria for choosing treatment
The most important criteria for choosing a treatment for HDA RRMS patients were effectiveness, side-effects profile and the lesion load. These criteria and the average ranking by the respondents are presented in Table 1. Respondents reported an average certainty score of 1.2 (range 1–2), indicating that, on an average, respondents were certain of their answer (low risk of being wrong [±10% deviation possible]).
| Rank | Criterion | Average score (range) |
|---|---|---|
| 1 | Effectiveness | 1.0 (1–1) |
| 2 | Side effects profile | 2.4 (2–3) |
| 3 | Lesion load | 3.4 (2–7) |
| 4 | Wish to have children | 4.6 (4–7) |
| 5 | Monitoring | 5.0 (3–6) |
| 6 | Ease of use | 5.6 (4–7) |
| 7 | Age | 6.6 (5–8) |
| 8 | Gender | 7.8 (5–9) |
| 9 | Dosage | 8.6 (8–9) |
A rank of 1 represents the most important criterion and a rank of 9 represents the least important criterion.
Limitations in & satisfaction with current treatment options
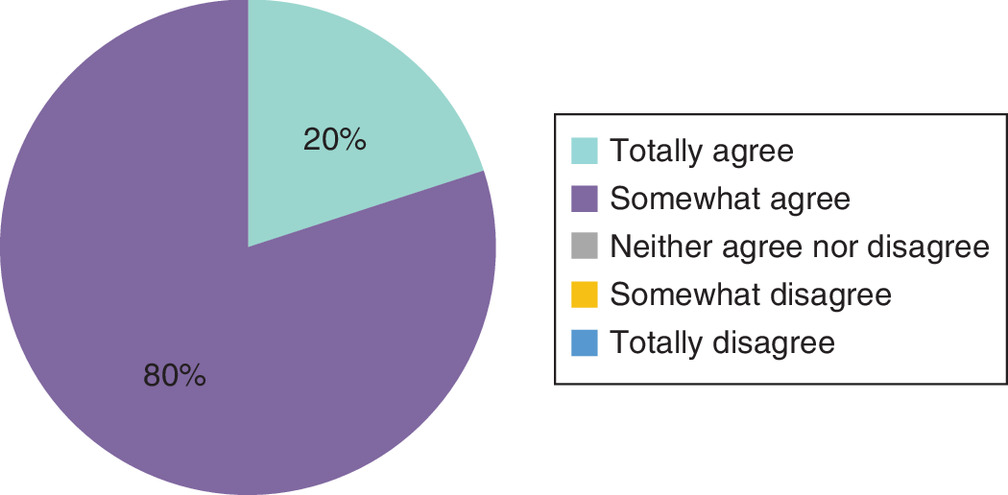
In the Netherlands, there are currently restrictions in the reimbursement of certain DMTs. Respondents were asked whether these reimbursement restrictions prevent them from optimally treating their patients. One of the five respondents totally agreed, and four of the five somewhat agreed with this statement (Figure 2). Motivations for these answers included that reimbursement restrictions should never impede optimal treatment of patients; that reimbursement status is considered as little as possible; that ideally all treatment options should be available especially in light of personalized medicine and shared decision making; and that restrictions sometimes differ between insurance companies and treatment options. Respondents reported an average certainty score of 1.4 (range 1–2), indicating that, on an average, respondents were certain of their answer (low risk of being wrong [±10% deviation possible]).
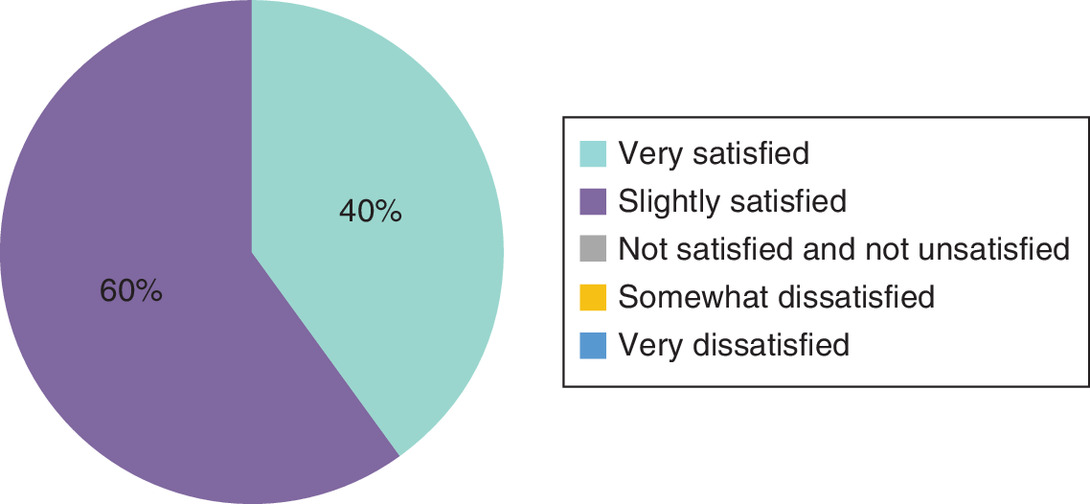
Respondents were also asked how satisfied they were with the currently available treatment options for patients with HDA RRMS that have not been previously treated with DMTs in the Netherlands. Two of the five respondents indicated that they were very satisfied and three of the five indicated that they were satisfied (Figure 3). Motivations for these answers included that although the reimbursement restrictions and conditional funding lead to dissatisfaction, in practice, a solution can usually be found for the individual patient. Because there are relatively few reimbursement restrictions in the Netherlands compared with other countries. Further, the reimbursement restrictions that prevent the use of certain DMTs in first-line treatment should be abolished as it does not make sense that certain DMTs cannot be given as first-line treatment while this is not the case for others, such as ocrelizumab. Respondents reported an average certainty score of 1.2 (range 1–2), indicating that, on an average, respondents were certain of their answer (low risk of being wrong [±10% deviation possible]).
Treatment switching
Respondents reported that in 23% (90% CI: 19–27%) of HDA RRMS patients, it was necessary to switch to another DMT due to insufficiency or side effects of the medication within 12 months after initiation of the first DMT. This could have been prevented in 20% (90% CI: 4–36%) of patients, if certain DMTs would be reimbursed for the first-line treatment of these patients (optional question, answered by four out of five respondents). Respondents reported average certainty scores of 1.8 (range 1–2) and 2.3 (range 2–3), indicating that, on an average, respondents were fairly certain of their answer (some risk of being wrong [±20% deviation possible]).
Case study
At the end of the questionnaire respondents were presented with a fictitious case study about a young DMT-naive woman, with one prior relapse in March that was successfully treated with methylprednisolone. In October of the same year, she had another serious polysymptomatic episode which was again treated with methylprednisolone. Remission of symptoms was incomplete (the full case description is available in Dutch in the questionnaire copies included in the online Supplementary Material).
Three out of five respondents would treat this patient with peginterferon bèta-1a, one out of five would treat this patient with teriflunomide and one out of five would treat this patient with natalizumab. Respondents reported an average certainty score of 1.6 (range 1–2), indicating that, on an average, respondents were certain of their answer (low risk of being wrong [±10% deviation possible]).
When asked to rank the reasons for choosing this specific treatment for this patient the number of exacerbations (average rank 1.8, range 1–3), the effectiveness of the treatment (average rank 2.2, range 1–4) and the lesion load (average rank 2.6, range 2–4) were ranked as the three most important criteria, while the reimbursement status was reported as the least important. Respondents reported an average certainty score of 1.2 (range 1–2), indicating that, on an average, respondents were certain of their answer (low risk of being wrong [±10% deviation possible]).
At Last, respondents were asked whether they experienced limitations in the treatment options for such a patient. In both rounds of the Delphi study, three out of five respondents indicated that they experienced limitations in the treatment options for such a patient, while two out of five respondents indicated that they do not experience limitations. Motivations for these answers in the first round included that ocrelizumab or cladribine tablets would be difficult to prescribe for such a patient; that cladribine tablets or fingolimod should also be potential treatment options for such a patient (which they currently are not), but that prescribing natalizumab is usually not an issue; and that limitations occur due to a multitude of reasons, including reimbursement status, limitations in logistics and business operations, but also due to limited knowledge and experience on the part of both physicians and patients – patients are additionally expected to participate in shared decision making, while they only have limited insight and do not always have a sufficiently critical attitude. Respondents reported an average certainty score of 1.2 (range 1–2), indicating that, on an average, respondents were certain of their answer (low risk of being wrong [±10% deviation possible]).
Discussion
This Delphi study was conducted to gain insights into the current treatment pathway of HDA RRMS patients in the Netherlands and to identify whether MS neurologists experience any barriers for optimal treatment, such as reimbursement restrictions.
As far as epidemiological traits are concerned, out of the average 60 RRMS patients that the respondents treat in their practice on a monthly basis, they indicated that 26% falls into the HDA category and 72% of them is treated with DMTs. Furthermore, our findings from the Delphi study suggest that almost half of the HDA RRMS patients (47%) have been treated with one DMT and almost a quarter (22%) of them have been treated with two or more DMTs.
From a MS neurologist's point of view, effectiveness and side effects of the DMT along with the patient’s lesion load were the most important contributing factors to their treatment decision for choosing a particular DMT. These findings align with the findings among neurologists and nurses from Kremer et al. who assessed which attributes were most important in choosing a particular DMT according to neurologists, nurses and patients. However, patients rated the importance of the attribute safety significantly lower than neurologists and nurses [17].
The majority (three out of five) of the respondents is slightly satisfied with the current treatment options in the Netherlands for patients with HDA RRMS while the remaining two respondents are very satisfied. All of them either totally agree (one out of five) or somewhat agree (four out of five) that the reimbursement restrictions for certain DMTs prevent them from optimally treating their patients. Three of the five respondents provided their interpretation of these findings. They reported that in general, good treatment options exist for HDA RRMS patients in the Netherlands, but that the reimbursement restrictions and indication rules avoid that patients can be treated with the preferred treatment. As an example, they mentioned that ‘several so called second-line DMTs cannot be used until a patient has first failed on another DMT. This is particularly undesirable in case of aggressive MS.’ Furthermore, they mentioned that these issues cannot be solved without a revision of the Dutch MS guideline.
These findings indicate some satisfaction with the treatment options available for (HDA) RRMS patients. Although respondents are satisfied with the treatment options available, they do feel restricted by reimbursement conditions. The respondents indicated that a solution can be found in daily practice, but still there are patients for which the ideal treatment is not directly available due to reimbursement and indication restrictions, for instance patients with aggressive MS.
The finding that the current reimbursement landscape presents a restriction is also highlighted in the MS neurologists’ treatment choices in a hypothetical situation where reimbursement status is not a factor (i.e., when the reimbursement restrictions for certain DMTs would not be in effect). MS neurologists would then treat almost a third of DMT-naive patients with cladribine tablets or fingolimod, which is currently prevented due to reimbursement restrictions limiting their use to patients with HDA RRMS that have not responded to at least one DMT.
It was estimated by the respondents that almost a quarter of the DMT-naive HDA RRMS patients are likely to change to another DMT within 12 months due to insufficient effectiveness or serious side effects. Moreover, the respondents indicate that this switch could have been prevented in up to one-fifth of the cases if certain DMTs (such as fingolimod and cladribine tablets) would be reimbursed for use in these patients.
Effectiveness of the treatment, the number of exacerbations and the lesion load were the most important criteria for choosing a particular treatment, as reported in the case study. The reimbursement status is rated as the least important criterion for their decision. Interestingly, although three out of five experts state that they experience reimbursement restrictions, when presented with the case study in which no restrictions apply, they do opt for those drugs that are currently reimbursed. It is likely that reimbursement has inadvertently played a role in the decision of the experts.
This study carried strengths and limitations. A main strength is that the use of the Delphi panel allows for analysis of the subjective experience and judgment of MS neurologists of the treatment landscape of (HDA) RRMS, and to capture whether they experience restrictions through the reimbursement scheme. A Delphi panel is particularly useful in analyzing subjective experiences of respondents regarding certain situations [12]. Furthermore, the certainty scores and CIs from the second-round questionnaire results indicate that the included experts are quite sure of their answers and are aligned, mostly giving a certainty score of between 1 and 2, indicating low to some (10–20%) risk of being wrong.
Although no clear guidance is given in the scientific literature on what constitutes a robust panel size for a Delphi panel study or on the criteria against which a sample size choice should be judged [12–14], the low number of respondents (five MS neurologists) in the Delphi panel could be seen as a limitation of this study. However, the level of expertise of the respondents and geographical spread between the respondents are considered more important [12–14], which were carefully taken into account in this study.
Conclusion
The findings of this Delphi panel indicate that MS neurologists are satisfied with the current treatment options for patients with DMT-naive HDA RRMS, although they feel that they are prevented from optimally treating their patients due to reimbursement restrictions for certain DMTs. Furthermore, the findings highlight that in an ideal situation, MS neurologists would also treat DMT-naive HDA RRMS patients with medications that are currently restricted to patients that have not responded to at least one DMT. The answers show consensus between the participants and high certainty of answers.
•
At the time of writing, the Dutch treatment guidelines date from 2012 and, therefore, do not cover treatments that have been introduced after 2012.
•
In the Netherlands, there are reimbursement restrictions in place for the disease modifying therapies (DMTs) including cladribine tablets, natalizumab, alemtuzumab and fingolimod. These restrictions limit the use of these treatments to patients with high disease activity (HDA) relapsing remitting multiple sclerosis (RRMS) that have not responded to at least one DMT, while their registered indications do include treatment of HDA RRMS regardless of prior treatment status.
•
A two-round Delphi panel using an online questionnaire was conducted among MS neurologists to gain insights into the current treatment pathway of HDA RRMS patients in the Netherlands and to identify if multiple sclerosis (MS) neurologists experience any barriers for optimal treatment, such as reimbursement restrictions.
•
Effectiveness and side effects of the DMT along with the patient’s lesion load were the most important contributing factors to MS neurologists’ treatment decision for choosing a particular DMT.
•
All respondents either totally (one) or somewhat agree (four) that the reimbursement restrictions for certain DMTs prevent them from optimally treating their patients.
•
In a hypothetical situation where reimbursement status is not a factor, MS neurologists would treat almost a third of DMT-naive patients with cladribine tablets and fingolimod, which is currently prevented due to reimbursement restrictions.
•
Almost a quarter of the DMT-naive HDA RRMS patients are likely to change to another DMT within 12 months due to insufficient effectiveness or serious side effects, which could have been prevented in up to one-fifth of the cases, if certain DMTs would be reimbursed for use in these patients.
•
The results show consensus between the participants and high certainty of answers.
Author contributions
Design of the study was contributed to by RE Michels, ML Peters, KMH Schiffers, G De Voer and M Krol. Conducting the Delphi panel was contributed to by RE Michels, ML Peters, PA Bouma, GID Hengstman, CEP van Munster and E Zeinstra. Analysis was contributed to by RE Michels and ML Peters. Drafting the manuscript was contributed to by RE Michels and ML Peters. Reviewing the manuscript was contributed to by KMH Schiffers, PA Bouma, GID Hengstman, CEP van Munster, E Zeinstra, G De Voer and M Krol.
Financial & competing interests disclosure
Merck B.V., Amsterdam, the Netherlands, an affiliate of Merck KGaA, Darmstadt, Germany, provided funding to IQVIA, the Netherlands for the conduct of this study. KMH Schiffers and G De Voer are employees of Merck B.V., Amsterdam, the Netherlands, an affiliate of Merck KGaA, Darmstadt, Germany. ML Peters, RE Michels and M Krol are employees of IQVIA, Amsterdam, the Netherlands. E Zeinstra has received sponsoring or grant support for clinical studies from Biogen, Sanofi Genzyme, Merck KGaA, Novartis, Roche and Teva. CEP van Munster has received travel support from Novartis, Sanofi Genzyme, Teva Pharmaceuticals and Merck KGaA; and honoraria for lecturing and consulting from Novartis, Biogen-Idec and Merck KGaA; and compensation for serving in a scientific advisory board from Biogen-Idec, Roche, Merck KGaA and Sanofi Genzyme. GID Hengstman has received consultancy fees and grants from Biogen, Sanofi Genzyme, Merck KGaA, Novartis and Roche. PA Bouma provided paid educational and scientific services to Biogen, Sanofi Genzyme, Merck KGaA and Novartis. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_data.zip)
- Download
- 404.36 KB
References
Papers of special note have been highlighted as: • of interest
1.
Franciotta D, Salvetti M, Lolli F, Serafini B, Aloisi F. B cells and multiple sclerosis. Lancet Neurol. 7(9), 852–858 (2008).
2.
Kleinschnitz C, Meuth SG, Kieseier BC, Wiendl H. Immunotherapeutic approaches in MS: update on pathophysiology and emerging agents or strategies 2006. Endocr. Metab. Immune Disord. Drug Targets 7(1), 35–63 (2007).
3.
Chitnis T. The role of CD4 T cells in the pathogenesis of multiple sclerosis. Int. Rev. Neurobiol. 79, 43–72 (2007).
4.
Lublin FD, Reingold SC, Cohen JA et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology 83(3), 278–286 (2014).
5.
European Medicines Agency. Mavenclad – summary of product characteristics (2017). Last revision of text in 2018. https://www.ema.europa.eu/en/medicines/human/EPAR/mavenclad
6.
Richtlijn Multiple Sclerose. https://richtlijnendatabase.nl/richtlijn/multipele_sclerose/multipele_sclerose_-_startpagina.html
• Dutch guideline for multiple sclerosis.
7.
Zorginstituut Nederland. GVS beoordeling cladribine (mavenclad®) (2018). https://www.zorginstituutnederland.nl/publicaties/adviezen/2018/01/24/gvs-advies-cladribine-mavenclad
• Dutch Health Technology Assessment (HTA) assessment report for cladribine tablets listing the reimbursement restrictions.
8.
European Medicines Agency. Gilenya – summary of product characteristics (2011). Last revision of text in 2018. https://www.ema.europa.eu/en/medicines/human/EPAR/gilenya
9.
Zorginstituut Nederland. Wijziging bijlage 2 voorwaarde fingolimod (gilenya). (2016). https://www.zorginstituutnederland.nl/publicaties/adviezen/2016/07/12/wijziging-bijlage-2-voorwaarde-fingolimod-gilenya-bij-actieve-relapse-remitting-multiple-sclerose-rrms
• Dutch HTA assessment report for fingolimod listing the reimbursement restrictions.
10.
European Medicines Agency. Tysabri – summary of product characteristics. (2006). Last revision of the text in 2018. https://www.ema.europa.eu/en/medicines/human/EPAR/tysabri
11.
Zorginstituut Nederland. Herbeoordeling en duiding van natalizumab tysabri®. (2014). https://www.zorginstituutnederland.nl/binaries/zinl/documenten/adviezen/2014/07/14/natalizumab-tysabri-bij-zeer-actieve-relapsing-remitting-multiple-sclerose/Natalizumab+Tysabri+bij+zeer+actieve+relapsing+remitting+multiple+sclerose.pdf
12.
Avella JR. Delphi panels: research design, procedures, advantages, and challenges. J. Doctoral Studies 11, 305–321 (2016).
13.
Akins RB, Tolson H, Cole BR. Stability of response characteristics of a Delphi panel: application of bootstrap data expansion. BMC Med. Res. Methodol. 5, 37 (2005).
14.
Iqbal S, Pipon-Young L. The Delphi method. Psychologist 22(7), 598–601 (2009).
15.
Simoens S. Using the Delphi technique in economic evaluation: time to revisit the oracle? J. Clin. Pharm. Ther. 31(6), 519–522 (2006).
16.
Powell C. The Delphi technique: myths and realities. J. Adv. Nurs. 41(4), 376–382 (2003).
17.
Kremer IEH, Evers S, Jongen PJ, Hiligsmann M. Comparison of preferences of healthcare professionals and MS patients for attributes of disease-modifying drugs: a best-worst scaling. Health Expect. 21(1), 171–180 (2018).
Information & Authors
Information
Published In
Pages: 93 - 100
PubMed: 33275036
Copyright
© 2020 Renée Michels. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 6 July 2020
Accepted: 4 November 2020
Published online: 4 December 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A Delphi panel on treatment of high disease activity relapsing remitting multiple sclerosis in the Netherlands. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0140
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Craig M. Zaidman, Natalie L. Goedeker, Amal A. Aqul, Russell J. Butterfield, Anne M. Connolly, Ronald G. Crystal, Kara E. Godwin, Kan N. Hor, Katherine D. Mathews, Crystal M. Proud, Elizabeth Kula Smyth, Aravindhan Veerapandiyan, Paul B. Watkins, Jerry R. Mendell, Management of Select Adverse Events Following Delandistrogene Moxeparvovec Gene Therapy for Patients With Duchenne Muscular Dystrophy, Journal of Neuromuscular Diseases, 10.3233/JND-230185, 11, 3, (687-699), (2024).