The societal impact of obinutuzumab in the first-line treatment of patients with follicular lymphoma in Germany
Publication: Journal of Comparative Effectiveness Research
Abstract
In this study, we assessed the productivity gains associated with the use of obinutuzumab in combination with chemoimmunotherapy (G-chemo) in first-line treatment among follicular lymphoma patients. Health benefits, measured as an increase in progression-free survival, were translated into productivity gains in both paid and unpaid work using gross value added as productivity measure. From 2017 to 2030, 11,870 overall progression-free years can be gained by utilizing obinutuzumab. These progression-free years correspond to undiscounted productivity gains of about €187.9 million in paid work and about €535.9 million in unpaid work. Our study shows that the benefits of the use of obinutuzumab in the first-line treatment of follicular lymphoma extend beyond clinical advantages.
Lay abstract
Despite effective treatment options, follicular lymphoma is still incurable and is associated with frequent relapses. Patients with hematological cancers are among those most likely to experience work impairment due to their condition. Novel treatments such as an obinutuzumab-based chemotherapy, however, can improve patients’ progression-free survival considerably and enable them to pursue their everyday activities and participate in the labor market. In this study, we quantify how much work productivity can be generated by treating patients with an obinutuzumab-based therapy instead of with the alternative standard therapy. Our results show that, when taking together all expected new follicular lymphoma patients in Germany from 2017 to 2030, the overall productivity that can potentially be generated amounts to €723.8 million, including productivity from both paid work and unpaid work such as housekeeping or childcare.
Follicular lymphoma (FL) is the most common type of indolent non-Hodgkin lymphoma, a group of blood cancers, in the Western hemisphere. In Germany, about 3000–3500 patients are diagnosed with FL per year [1], with numbers presumably increasing in coming years due to population ageing. Most cancer patients and especially those with hematological cancers, experience significant work incapacity due to severe disease symptoms such as pain and fatigue, as well as side effects of treatment and psychological distress [2,3]. About 47% of FL patients are under the age of 65 [1] The fact that, a large share of patients is active in the workforce at the time of diagnosis underscores the relevance of the condition with respect to economic implications in terms of productivity loss.
At the same time, evidence shows that, even for patients with hematological cancers, work ability improves over time, once a disease remission has been achieved [4]. Naturally, maintaining remission is likely to have a substantial effect on work ability, which in turn affects both participation in the labor market and the ability to perform daily activities. Improving treatment of patients with hematological cancer and increasing duration of remission, thus not only reduces the burden of disease for the individual but also results in socioeconomic benefits in form of increased productivity. The key component of the treatment of patients with advanced stage FL is an immunotherapy, often combined with chemotherapy. While the anti-CD20 antibody rituximab, which was the first monoclonal antibody to be used successfully in the treatment of FL, has already improved outcomes substantially [5–7], novel anti-CD20 antibodies have been shown to bring further improvements.
In this study, we assessed the productivity gains that are associated with a more effective treatment of FL using the example of one recently approved novel drug. More precisely, we assessed the productivity gains associated with the use of obinutuzumab in combination with chemoimmunotherapy (G-chemo) in first-line treatment among FL patients. To this end, we adopted an existing cost–effectiveness model and extrapolated the health effects to the current and future patient population (over the period 2017–2030) in Germany [8]. The cost–effectiveness model is based on the GALLIUM clinical trial, which has shown that obinutuzumab therapy significantly prolongs progression-free survival (PFS) and reduces the risk of an early relapse compared with the current standard of care chemoimmunotherapy with rituximab (R-chemo). The estimated rate of PFS at 3 years was 80.0% under G-chemo versus 73.3% under R-chemo; the hazard ratio for progression, relapse or death was 0.66 (95% CI: 0.51–0.85; p = 0.001) [9]. The aggregated health benefits were further translated into productivity gains in both paid and unpaid work using gross value added (GVA) as a measure of productivity.
While there is clear evidence of the positive effects of a therapy with G-chemo on PFS, evidence about societal effects that go beyond this clinical effect is missing. Indirect costs are not included in the cost–effectiveness model [8]. To our knowledge, neither are there other studies that analyze the economic and societal impact of using obinutuzumab. We aim to fill this research gap by providing an assessment of the potential gain in productivity from paid and unpaid work in Germany based on the additional health benefits of G-chemo compared with R-chemo.
Materials & methods
Patient-level model for health benefits
In a first step, we calculated the health benefits for the average patient who is treated with G-chemo instead of R-chemo. Here, health benefits refer to health gains in terms of additional time that patients spend in a progression-free health state due to the treatment with G-chemo. Therefore, we adopted an existing cost–effectiveness model that compares obinutuzumab-based chemotherapy followed by obinutuzumab monotherapy versus rituximab plus chemotherapy followed by rituximab monotherapy in previously untreated FL patients in the United States [8]. The cost–effectiveness model uses a Markov model with three discrete health states – progression-free, experiencing disease progression and dead. During each 3-months cycle, patients move from one health state to another with a certain transition probability. Data inputs are efficacy data from the GALLIUM clinical trial (ClinicalTrials.gov: NCT01332968), data cut-off September 2016. The trial data show that there are significant differences in PFS between a treatment with G-chemo and R-chemo [9]. A detailed description of the model and underlying assumptions can be found in Guzauskas et al. [8]. The authors provided us with the data and calculations behind their parametrically fitted and extrapolated PFS curves. All model inputs were adopted one-to-one, except the overall mortality inputs, which were adjusted according to current life tables for Germany [10].
Using this model, we simulated the treatment course and treatment outcome, that is time in the progression-free health state, of the average patient in two alternative scenarios: patients are treated with G-chemo and subsequent G maintenance for a maximum of 30 months or until disease progression and patients are treated with R-chemo and R maintenance for a maximum of 30 months or until disease progression. Our analysis is limited to assessing work productivity effects during PFS. The reason for this is that there was a significant effect of an obinutuzumab-based therapy on PFS in the GALLIUM clinical trial, while differences in overall survival were not significant [9].
Population model for health benefits
While the patient-level model provides information on the additional time spent in the progression-free health state for one average patient, it is the aim of this study to assess the accumulated health benefits for the entire target patient population over an extended time period. The target population are all patients for whom a treatment with immunochemotherapy, in other words, G-chemo or R-chemo, is indicated. These patients are newly diagnosed, with untreated FL in an advanced disease stage and in need of treatment [11].
Therefore, as a second step, we constructed a dynamic population model based on the patient-level model as described above. Starting in 2017, a new cohort of incident patients enters the model at the beginning of every 1-month cycle while the existing cohorts remain progression-free, experience a disease progression or die, according to the patient-level Markov model.
The size of the patient cohorts entering the model in each cycle is based on assumptions regarding population development, incidence rates and therapy options as derived and presented in the value dossier on obinutuzumab-based therapy in untreated FL submitted to G-BA (German HTA agency) [12]. While the forecasts of incident patients in the value dossier are limited until the year 2022, our calculations are further extended until 2030. We assumed that both incidence rates and the possible choice of therapy options remain constant through 2030. According to these estimations, the absolute yearly number of patients who are candidate for a first-line treatment with anti-CD20 antibody (+chemotherapy) ranges from 1724 in 2017 to 1885 in 2030 [1,12]. The patient cohorts are further divided into gender and 10-year age groups according to data from the German population-based cancer registry [1]. All patient cohorts in the model are followed until the end of 2030. The period was chosen to approximate the likely life cycle or a pharmaceutical product as obinutuzumab (similar to Himmler et al. [13]). Main input parameters for the calculation can also be found in Table A1 in the Supplementary data.
For both scenarios, we finally added up the time in months spent in the progression-free health state for the entire patient population from 2017 to 2030. The difference of this accumulated progression-free health state time between the two treatment scenarios provides us with the incremental overall health benefit of G-chemo.
Socioeconomic benefits
To calculate the socioeconomic benefits associated with G-chemo, we translate the estimated incremental progression-free time into meaningful measures such as paid and unpaid work hours. The assumption is that more time spent in a progression-free health state implies not only a higher quality of life for patients but also higher capability to keep their job or to perform daily activities, including household tasks (housekeeping, childcare, etc.) and voluntary service [14].
Both paid and unpaid work contribute to a society’s prosperity by generating value added, one of the most widely used welfare measures. While formal national accounts systems only consider the value added that is generated within paid work, in other words, work that produces goods or services that are traded for money in the economy, unpaid work also generates value added [15,16]. Unpaid work includes household tasks such as housekeeping, childcare, other informal care as well as voluntary activities.
Socioeconomic benefits are thus depicted in terms of the potential to generate value added, comprising value added from both paid and unpaid work. In the following we describe how we assigned value added from paid and unpaid work to the health benefits, measured in additional PFS months, that are generated by using obinutuzumab.
Paid work
We started by determining the overall time that patients use for paid work, that is how much of their progression-free time they in fact spend working. We assumed that this depends on actual employment, return to work probabilities and possible work impairments due to the severity of the condition.
To our knowledge, there is no evidence that FL patients differ from the average population in terms of their employment pattern before the onset of the disease. We thus assume that employment patterns of FL patients equal those of the overall population. According to data from the German Statistical Office for 2016, the average employment rate for people at ages 20–59 is about 80% (ranging from 71% in the age group 20–29 to 86% in the age group 40–49). At higher age groups, the employment rate drops to on average 35% in the age group 60–69 and 6% in the age group 70–79 [17,18].
Assumptions on return to work rates are based on two studies assessing return to work rates among different cancer patients. Spelten et al. observed patients who were treated in hospitals in the Netherlands for different types of cancer over a time period of up to 18 months after the first day of sick leave [19]. They report that 24% of patients return at 6 months, 50% return at 12 months and 64% return at 18 months after initial diagnoses. Similarly, Horsboel et al. studied return to work rates for different subtypes of hematological cancers and reported return to work rates very similar to these numbers [20]. We therefore apply the numbers reported in Spelten et al. and assume that the initial patients return 6 months after the start of the treatment. As for the remaining 36% of patients in working age, we assumed that they retire with the onset of the disease.
Still, many cancer patients, although experiencing disease remission and being able to return to work, suffer from impaired health as a result of their condition and/or treatment that translates into a certain degree of work and activity impairment [21,22].
Several studies analyze quality of life as well as work and activity impairment of FL patients during different treatment stages by use of the WPAI (Work Productivity and Activity Impairment) and the EORTC QLQ-30 (European Organization for Research and Treatment of Cancer – Core Quality of Life Questionnaire) questionnaire. According to these studies, work impairment is estimated to range between 20 and 40% after a first disease remission [14,23,24]. We thus assumed that patients who return to work after induction therapy and remain progression-free experience an average reduction of work capacity by about 30% during the whole progression-free period.
To summarize, we applied the following formula to determine the time (in months) that FL patients of one cohort spend on paid work:
where paid workage, gender denotes the additional overall time that an age-gender cohort spends on paid work, measured in months.
FPS6 months denotes the time spent in the progression-free health state during the first 6 months after the diagnosis and p(return)6 months is the rate of return to work during these first 6 months (analogously for 12 and 18 months). Employment rateage, gender is the age- and gender-specific employment rate.
In order to further value this potential time of paid work with the value added it contributes, we drew on data from the 2016 national accounts on GVA per labor input, in other words, labor productivity, in the German economy [25]. That is, the time for unpaid work accumulated over age-gender cohorts, , is multiplied with average monthly GVA per employee.
Our study differs from most health economic evaluations by using GVA as a measure of productivity instead of gross or net income which is typically used. It allows us to capture not only productivity gains for patients, measured by income, but also productivity gains that accrue to employers (earnings) and the state (taxes on income and earnings), thereby taking a truly societal perspective. It further allows us to distinguish between direct, indirect and induced GVA effects, which were calculated using Leontief multipliers following the input-output literature [26,27].
Unpaid work
Besides employment, individuals also perform productive activities outside of the labor market for which they receive no payment. These activities, including housekeeping, childcare, informal care and so on, are generally referred to as unpaid work. In valuing the additional time spent in a progression-free health state, we therefore not only account for paid work but also for contributions of value added through unpaid work.
In a first step, we derived the amount of time that an average person from an age-gender cohort typically spends on different unpaid work activities from the German time use survey [28]. This survey measures how people, divided by gender and age group, precisely allocate their time across different day-to-day activities across a total duration of 24 h. In order to distinguish unpaid work from leisure time and other activities, we followed the third person criterion defining unpaid work as activities that may also be performed by another person [29].
In accordance with our valuation approach regarding paid work, benefits of unpaid work were valued according to the potential to generate value added. Therefore, all unpaid work activities were assigned to their equivalent market substitute, following the approach by Hofmann [30]. This proxy good method (also known as the replacement cost approach) assumes that each activity is worth what it would cost to purchase the same service on the free market [31]. Unpaid work was then valued with its respective age- and gender-specific GVA per capita equivalent. The level of work impairment in performing unpaid work in our model population is assumed to be equivalent to the level of work impairment in paid work. Analogously to the outlined approach on paid work, we also calculated indirect and induced value added contributions for unpaid work. While the direct GVA effect of unpaid work is not considered in the system of national accounts, indirect and induced effects are. Goods and services that are used in performing unpaid work (tools, ingredients for cooking, etc.) are purchased and are thus included in official statistics.
Aggregating the potential value added that can be generated from both paid and unpaid work yields the overall societal impact of using obinutuzumab in the first-line treatment of FL patients.
Results
Between 2017 and 2030, 25,419 newly diagnosed patients who are candidates for a treatment with G-chemo enter the population model. Figure 1 displays the results of the dynamic population model, in other words, the number of patients in progression-free, progressive disease or dead health states respectively in each treatment scenario over time. The share of progression-free patients is comparatively higher in the G-chemo as compared with the R-chemo scenario. Overall, the years that patients spend in a progression-free health state amount to 123,736 years in the G-chemo scenario and to 111,865 years the R-chemo scenario, resulting in a difference of additional 11,870 years of PFS for patients in G-chemo treatment, which corresponds to 5.6 months per patient entering the model.
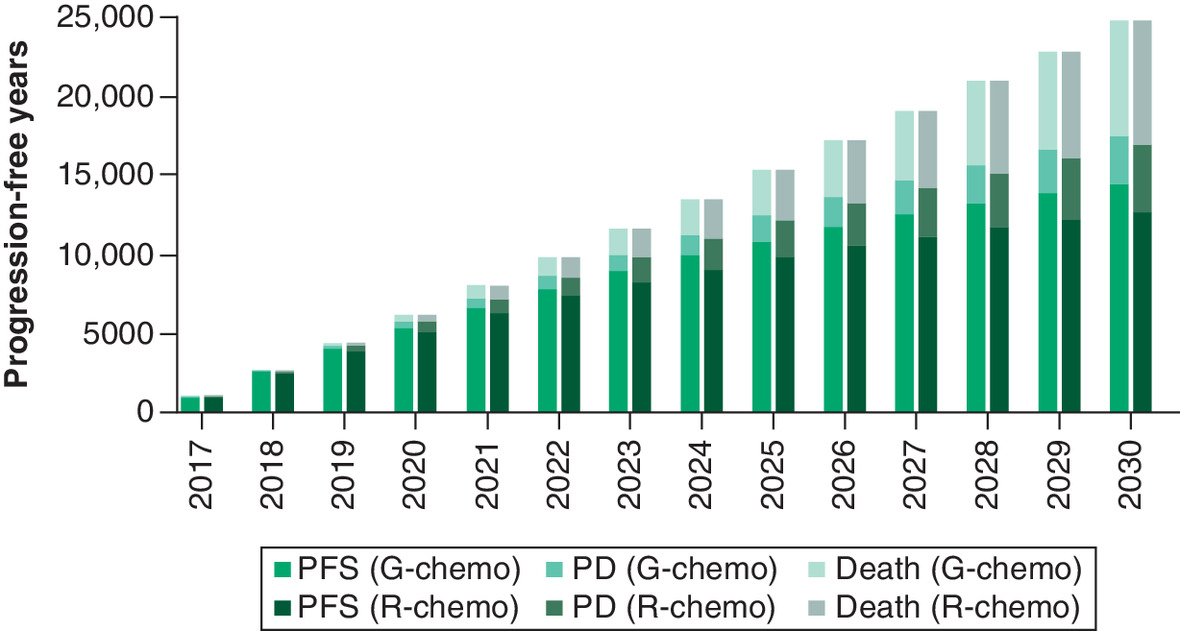
Figure 1. Health footprint – years spent in progression-free survival, progressive disease and dead health state with G-chemo and R-chemo therapy, respectively.
Bars represent the number of patients in progression free, PD or dead health states, respectively, in each treatment scenario over time.
PD: Progressive disease; PFS: Progression-free survival.
These additional 11,870 years of PFS translate into a total of about 11.2 million h for both paid and unpaid work (Table 1). Assuming average labor force participation rates between 4 and 90% for the respective age and gender cells and a work impairment rate of 30%, the additional progression-free years can be translated into a potential gain of 2.3 million hours of paid work. These hours correspond to approximately 1654 full-time employment years. Using current GVA per capita figures, this equals a potential value added of €90.1 million of direct effects. In addition, indirect and induced effects amount to €97.8 million, resulting in a total of €187.9 million in potential GVA effects from paid work.
| Type of work | Hours gained | Potential gains in value added (GVA effects) | ||
|---|---|---|---|---|
| Direct effects (in €) | Indirect & induced effects (in €) | Total GVA effects (in €) | ||
| Paid work | 2.3 million | 90.1 million | 97.8 million | 187.9 million |
| Unpaid work | 8.9 million | 267.1 million | 268.8 million | 535.9 million |
| Total | 723.8 million | |||
GVA: Gross value added.
Further, taking the age and gender distribution of the patient population into account and applying a constant post-treatment work impairment rate of 30%, the number of estimated years of PFS translate into 8.9 million h of unpaid work. This corresponds to an average of around 1400 hours of unpaid work per person and year. Valuing these hours with the GVA per hour of the closest market substitutes of unpaid work activities, results in an additional potential value-added effect of about €267.1 million. These direct effects correspond to additional €268.6 million of indirect and induced GVA effects from unpaid work.
Sensitivity analysis
All parameters in our model are based on assumptions or derived from statistical estimations (survival parameters in the Markov model), both of which are subject to uncertainty. To address this uncertainty, we conducted univariate sensitivity analyses, in other words, we changed each input variable at a time while keeping all other variables constant. This is a straightforward way to assess the sensitivity of the model to changes in input parameters and at the same time it permits identifying those input parameters that have the strongest impact on model results.
For the survival curve parameters, we applied 95% confidence limits of the estimated treatment effect as upper and lower values. For the other parameters, which were derived from the literature and for input parameters based on administrative statistics, we applied a range of variability of ± 20% of the baseline value.
The results of the sensitivity analysis are shown in Figure 2. Each bar represents the change in the direct social impact (paid and unpaid work) in million Euros if the input parameter listed on the left-hand side is changed to its upper or lower bound value. At baseline, the social impact sums up to around €257 million.
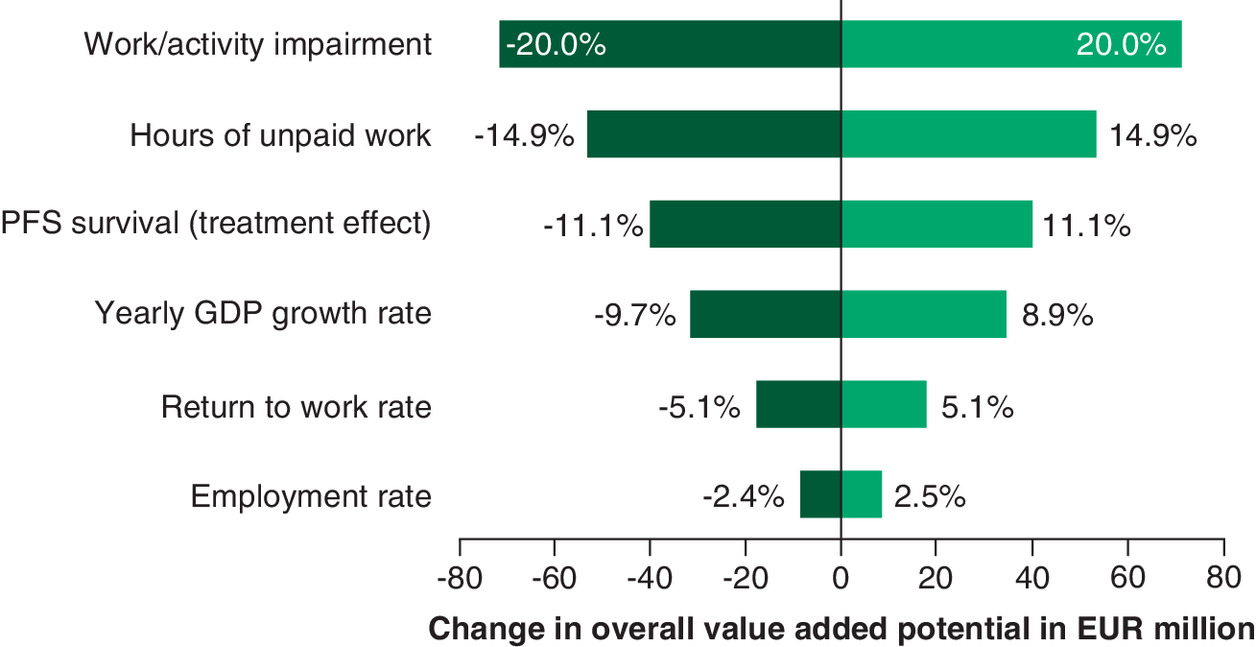
Figure 2. Sensitivity analysis – impact of changes in input parameters on change in overall value added potential in Euro million.
Each bar represents the change in the direct social impact (paid and unpaid work) in million Euros if the input parameter listed on the left-hand side is changed to its upper or lower bound value.
GDP: Gross domestic product; PFS: Progression-free survival.
The variable with the largest effect on the estimated social impact is the work and activity impairment. Labor market assumptions (employment rate and return to work rate) show the lowest impact on results. Overall, changes in the outcome due to (one-way) changes in input parameters do not exceed 20%, bolstering confidence in the reliability of our results.
Discussion
In this study, we used an extended approach to assess the societal value that can be created using obinutuzumab for the first-line treatment of FL. To our knowledge, this is the first study that quantifies the productivity effects obinutuzumab. Regarding the first-line treatment of FL, the study by Guzauskas and colleagues that provides the basis for our calculations, is the only cost–effectiveness study we have found. However, they only focus on direct medical costs but do not consider indirect productivity costs [8]. Also, regarding the use of obinutuzumab in later line treatment, cost–effectiveness studies exclusively consider costs from the perspective of the healthcare system, that is direct medical costs, but not from a societal perspective [32,33]. In general, while it is known that the economic and societal burden of FL is significant, there is very little information available regarding the societal cost of the illness. Due to lack of data availability, most studies are generally limited to hospital-based direct treatment costs [34].
Therefore, we aim to fill this void by explicitly assessing the positive economic and societal effects of effectively treating FL. A novelty of our study also lies in the chosen approach for monetizing the health-related productivity effects. Valuing averted losses of productive time in terms of GVA based on the national accounts and considering possible indirect and induced economic effects presents a new way of estimating productivity effects. It allows us to capture not only productivity gains for patients, measured by income, but also productivity gains that accrue to employers (earnings) and the state (taxes on income and earnings), thereby taking a truly societal perspective.
By also including unpaid work, which has been applied and discussed before [35], we are providing a more comprehensive picture of the broader economic effects of improvements in productivity impairment.
Besides adding to the literature discussing the inclusion of indirect costs in health economic evaluation, our analysis, first and foremost, provides valuable insights by illustrating the socioeconomic effects of a medical innovation. We add to the discussion on value-based pricing by showing that the benefits and the value of an innovative medicine may go far beyond the clinical advantages. While the focus can and should be on the benefits that a treatment can have on the patients themselves, effects on the economy and society as a whole are often neglected. However, these may be substantial once we consider how longer periods without disease progression enable patients to continue contributing to society by pursuing their every-day activities and participating in the labor market.
Limitations
It is important to note that the economic benefits we presented in the previous section display an economic potential – based on current economic figures for Germany – rather than a micro simulation of actual economic effects that might happen in the economy. Economic outcomes such as value creation are generally influenced by many factors that go beyond the supply of a healthy labor force. Our goal in this study is to show associations and not necessarily causality.
In order to assess overall economic implications, one would further have to model possible indirect productivity effects such as compensation mechanisms by co-workers or changes in patients’ consumption patterns, which might go in different directions and are generally hard to capture. Also, we do not consider changes in the healthcare providers’ productivity due to changes in demand for healthcare services. A further important socioeconomic aspect not considered here is the effect on patients’ informal caregivers [36]. While the listed aspects are important from an economic point of view and should receive further attention in future research, they would go beyond the scope of this study.
It is further important to note that data on employment, GVA per employee and unpaid work activities applied throughout the model refer to the year 2016. That means that future changes of employment rates or worker productivity are not displayed in our calculations. Instead, we assume that the average potential of value added contribution remains constant over time.
Further, the socioeconomic benefit depicted in this study is based only on the benefit that can be derived from differences in the duration of PFS due to first-line treatment. We assume that once patients experience a disease progression, further treatment lines, progression-free periods and overall survival do not differ by treatment group (G-chemo or R-chemo). We acknowledge that patients do not necessarily stop being productive once their disease progresses or they regain a progression-free health state at a later point of time. But we assume they do so to the same degree in both treatment regimes, which is why it does not contribute to incremental benefits of G-chemo. Similarly, we do not account for differences in adverse event rates unless they also result in changes in PFS. Evidence shows that adverse events occur slightly more often under a treatment with G-chemo as compared with a treatment with R-chemo [9]. Still, we assume that these do not have a noticeable effect on work capacity beyond the critical period of induction therapy. Since any positive effects of obinutuzumab that go beyond the direct PFS effects are not considered, the socioeconomic benefits in this study display a conservative estimate.
Another important limitation concerns the static assumptions regarding future developments and the uncertainty that we face around predictions. First, we simulate the model as if there will be no other first-line treatment options other than G-chemo and R-chemo until 2030, which is questionable given the current speed of medical innovations. Second, assumptions on labor market parameters as well as age and gender distribution are based on current figures. Future structural changes are thus not considered. Limitations inherent to the underlying Markov model are discussed in [8].
By incorporating productivity effects generated by unpaid work, we address a frequent argument used against the inclusion of indirect costs in health economic evaluations: wider economic benefits of innovative medicines are usually ignored as these apply only to working-age patients who are active in the labor market and are thus not relevant for the patient population in question [37]. However, evidence shows that including unpaid work loss as indirect costs in health economic evaluation has a substantial effect on results [38].
Conclusion
In this study, we analyzed the health effects and socioeconomic effects of a first-line treatment of FL with obinutuzumab-based chemoimmunotherapy as compared with the current standard therapy based on rituximab. We simulated two treatment scenarios, G-chemo or R-chemo for newly diagnosed patients from 2017 to 2030.
We show that among the 25,429 patients entering the model, 11,870 additional progression-free years can be gained when G-chemo is used instead of R-chemo. Further, these progression-free years results in an additional potential of value added (GVA) creation of about €187.9 million from paid work and another €535.9 million from unpaid work. These GVA gains occur in addition to clinical benefits in terms of longer PFS and represent an economic benefit of G-chemo treatment from a societal perspective.
Our study shows the extent to which a reduction in the disease burden of FL patients in Germany is associated with avoided productivity losses and subsequently economic and societal benefits. It emphasizes that the burden of FL is not limited to poor health and the associated healthcare resource use but that it also includes considerable productivity effects. This also implies that the benefits of an effective treatment of FL with obinutuzumab clearly extend beyond clinical advantages. Due to longer PFS, this treatment also results in positive economic effects in terms of increased productivity. The explicit consideration of unpaid work in our study further adds to the existing literature by including a broader perspective on productivity to inform decision-making.
•
In this study, we quantify the aggregate productivity gains in both paid and unpaid work of follicular lymphoma patients in Germany when obinutuzumab-based therapy is used as opposed to rituximab-based therapy.
•
To calculate the socioeconomic benefits associated with G-chemo, we translate the estimated incremental progression-free time into meaningful measures such as paid and unpaid work hours. These are further translated into the patients' potential to generate value added.
•
While often only paid work is considered in health economic evaluations, we take into account the patients’ potential to generate value added from both paid and unpaid work. Unpaid work includes household tasks such as housekeeping, childcare, other informal care as well as voluntary activities and contributes to a society’s prosperity too.
•
From 2017 to 2030, 11,870 overall progression-free years can be gained by utilizing obinutuzumab as compared with rituximab-based therapy. These progression-free years correspond to undiscounted productivity gains of about €187.9 million in paid work and about €535.9 million in unpaid work.
•
Our study shows that the advantages of the use of obinutuzumab in the first-line treatment of follicular lymphoma extend beyond clinical benefits. Due to longer progression-free survival, this treatment also results in positive economic effects in form of increased productivity.
Financial & competing interests disclosure
This study was funded by Roche Pharma. A Launonen and PO Thuresson are current employees of Roche Pharma. U Dünzinger is a former employee of Roche Pharma. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_data.zip)
- Download
- 42.49 KB
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Robert Koch Institute. Follikuläres non-hodgkin-lymphom (ICD-10 Code C82). Zentrum Für Krebsregisterdaten (2018). http://www.krebsdaten.de/abfrage
2.
Short PF, Vasey JJ, BeLue R. Work disability associated with cancer survivorship and other chronic conditions. Psychooncology 17(1), 91–97 (2008).
3.
Kessler RC, Greenberg PE, Mickelson KD, Meneades LM, Wang PS. The effects of chronic medical conditions on work loss and work cutback. J. Occup. Environ. Med. 43(3), 218 (2001).
4.
Munir F, Yarker J, McDermott H. Employment and the common cancers: correlates of work ability during or following cancer treatment. Occup. Med. 59(6), 381–389 (2009).
5.
Marcus R, Imrie K, Belch A et al. CVP chemotherapy plus rituximab compared with CVP as first-line treatment for advanced follicular lymphoma. Blood 105(4), 1417–1423 (2005).
6.
Marcus R, Imrie K, Solal-Celigny P et al. Phase III study of R-CVP compared with cyclophosphamide, vincristine, and prednisone alone in patients with previously untreated advanced follicular lymphoma. J. Clin. Oncol. 26(28), 4579–4586 (2008).
7.
Hiddemann W, Kneba M, Dreyling M et al. Frontline therapy with rituximab added to the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) significantly improves the outcome for patients with advanced-stage follicular lymphoma compared with therapy with CHOP alone: results of a prospective randomized study of the German Low-Grade Lymphoma Study Group. Blood 106(12), 3725–3732 (2005).
8.
Guzauskas GF, Masaquel A, Thuresson P-O, Dawson K, Veenstra DL. Obinutuzumab plus chemotherapy followed by obinutuzumab monotherapy is cost-effective vs. rituximab plus chemotherapy followed by rituximab monotherapy for previously untreated follicular lymphoma patients in the United States. Leuk. Lymphoma 60(7), 1668–1676 (2019).
•• Cost–effectiveness model that forms the basis for our calculations of the health footprint.
9.
Marcus R, Davies A, Ando K et al. Obinutuzumab for the first-line treatment of follicular lymphoma. N. Engl. J. Med. 377(14), 1331–1344 (2017).
•• Main evaluation of the clinical trial that compares obinutuzmab-based chemotherapy to rituximab-based chemotherapy in patients with follicular lymphoma.
10.
Destatis. Allgemeine Sterbetafel 2010/12. Statistisches Bundesamt, Wiesbaden, Germany (2015).
11.
EMA. European Public Assessment Report (EPAR) for Gazyvaro, Annex I – Summary of Product Characteristics. (2018). https://www.ema.europa.eu/en/medicines/human/EPAR/gazyvaro
12.
Roche Pharma AG. Dossier zur Nutzenbewertung gemäß § 35a SGB V – Obinutuzumab (Gazyvaro) – Modul 3 A. (2017). https://www.g-ba.de/downloads/92-975-2137/2017-09-21_Modul1_Obinutuzumab.pdf
13.
Himmler S, Müller M, Ostwald D, Seddik A, Basic E, Hradetzky E. Long-term health benefits of stroke prevention with apixaban versus vitamin K antagonist warfarin in patients with non-valvular atrial fibrillation in Germany: a population-based modelling study. Expert Rev. Pharmacoecon. Outcomes Res. 19(2), 223–230 (2019).
14.
Pettengell R, Donatti C, Hoskin P et al. The impact of follicular lymphoma on health-related quality of life. Ann. Oncol. 19(3), 570–576 (2008).
15.
Miranda V. Cooking, caring and volunteering: unpaid work around the world. OECD Soc. Employ. Migr. Work. Pap. No. 116 (2011) (Online).
16.
Krol M, Brouwer W. Unpaid work in health economic evaluations. Soc. Sci. Med. 144, 127–137 (2015).
17.
Destatis. Statistisches Jahrbuch 2016 – Kapitel 13 – Arbeitsmarkt. Statistisches Bundesamt, Wiesbaden, Germany (2016).
18.
Destatis. Die Generation 65+ in Deutschland. Statistisches Bundesamt, Wiesbaden, Germany (2015).
19.
Spelten ER, Verbeek JHAM, Uitterhoeve ALJ et al. Cancer, fatigue and the return of patients to work – a prospective cohort study. Eur. J. Cancer 39(11), 1562–1567 (2003).
20.
Horsboel TA, Nielsen CV, Nielsen B, Jensen C, Andersen NT, de Thurah A. Type of hematological malignancy is crucial for the return to work prognosis: a register-based cohort study. J. Cancer Surviv. 7(4), 614–623 (2013).
21.
Short PF, Vasey JJ, Tunceli K. Employment pathways in a large cohort of adult cancer survivors. Cancer 103(6), 1292–1301 (2005).
22.
Yabroff KR, Lawrence WF, Clauser S, Davis WW, Brown ML. Burden of illness in cancer survivors: findings from a population-based national sample. J. Natl Cancer Inst. 96(17), 1322–1330 (2004).
23.
Cheung MC, Imrie KR, Friedlich J, Buckstein R, Lathia N, Mittmann N. The impact of follicular (FL) and other indolent non-Hodgkin's lymphomas (NHL) on work productivity – a preliminary analysis. Psychooncology 18(5), 554–559 (2009).
24.
Andresen S, Brandt J, Dietrich S, Memmer M-L, Ho AD, Witzens-Harig M. The impact of high-dose chemotherapy, autologous stem cell transplant and conventional chemotherapy on quality of life of long-term survivors with follicular lymphoma. Leuk. Lymphoma 53(3), 386–393 (2012).
25.
Destatis. Volkswirtschaftliche Gesamtrechnung: Inlandsproduktberechnung Detaillierte Jahresergebnisse 2015. Chapter: Fachserie 18, Reihe 1.4. Statistisches Bundesamt, Wiesbaden Germany (2016).
26.
Leontief WW. Quantitative input and output relations in the economic systems of the United States. Rev. Econ. Stat. 18(3), 105 (1936).
27.
Miller RE, Blair PD. Input–Output Analysis: Foundations and Extensions (2nd Edition). Cambridge University Press, Cambridge, UK (2012). http://ebooks.cambridge.org/ref/id/CBO9780511626982
28.
Destatis. Zeitverwendungserhebung - Aktivitäten in Stunden und Minuten für ausgewählte Personengruppen - 2012/2013. Statistisches Bundesamt, Wiesbaden, Germany (2015).
29.
Reid MG. Economics of Household Production. J. Wiley & Sons, NY, USA (1934). http://archive.org/details/economicsofhouse00reid
•• Very fundamental work on valuing household production that provides the basis for our approach to monetarize unpaid work.
30.
Hofmann S. Einfluss nicht-marktlicher Tätigkeiten auf den materiellen Wohlstand und die Einkommensverteilung in Deutschland. Peter Lang International Academic Publishers, Bern, Switzerland (2015). https://www.econstor.eu/handle/10419/178485
31.
van den Berg B, Brouwer W, van Exel J, Koopmanschap M, van den Bos GAM, Rutten F. Economic valuation of informal care: lessons from the application of the opportunity costs and proxy good methods. Soc. Sci. Med. 62(4), 835–845 (2006).
32.
Guzauskas GF, Masaquel A, Reyes C, Wilhelm K, Krivasi T, Veenstra DL. What is the cost–effectiveness of obinutuzumab plus bendamustine followed by obinutuzumab monotherapy for the treatment of follicular lymphoma patients who relapse after or are refractory to a rituximab-containing regimen in the US? Blood 128(22), 3605–3605 (2016).
33.
Haukaas FS, Ohna A, Krivasi T. Cost–effectiveness of obinutuzumab in combination with bendamustine followed by obinutuzumab maintenance versus bendamustine alone in treatment of patients with rituximab-refractory follicular lymphoma in Norway. Appl. Health Econ. Health Policy 16(4), 569–577 (2018).
34.
Foster T, Miller JD, Boye ME, Russell MW. Economic burden of follicular non-hodgkin’s lymphoma. Pharmacoeconomics 27(8), 657–679 (2009).
35.
Krol M, Brouwer W. Unpaid work in health economic evaluations. Soc. Sci. Med. 144, 127–137 (2015).
•• Comprehensive review of how unpaid work is currently included in health economic evaluations. The review shows that despite its importance, unpaid work is only rarely included. It underlines the importance of studies like the present one.
36.
Mazanec SR, Daly BJ, Douglas SL, Lipson AR. Work productivity and health of informal caregivers of persons with advanced cancer. Res. Nurs. Health 34(6), 483–495 (2011).
37.
Paris V, Belloni A. Value in pharmaceutical pricing (2013). https://www.oecd-ilibrary.org/social-issues-migration-health/value-in-pharmaceutical-pricing_5k43jc9v6knx-en
38.
Krol M, Papenburg J, Tan SS, Brouwer W, Hakkaart L. A noticeable difference? Productivity costs related to paid and unpaid work in economic evaluations on expensive drugs. Eur. J. Health Econ. 17(4), 391–402 (2016).
Information & Authors
Information
Published In
Pages: 1017 - 1026
PubMed: 33016109
Copyright
© 2020 Future Medicine Ltd.
History
Received: 30 June 2020
Accepted: 19 August 2020
Published online: 5 October 2020
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The societal impact of obinutuzumab in the first-line treatment of patients with follicular lymphoma in Germany. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0131
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Foteini Tsotra, Kyle Dunton, Mats Rosenlund, Lena Steinbeck, Sukhvinder Johal, Estimating the societal impact of medical interventions: a case study in metastatic breast cancer, Journal of Comparative Effectiveness Research, 10.57264/cer-2026-0005, 15, 6, (2026).
- Ahmed H. Seddik, Jeroen Paulissen, Ramesh Marapin, Sebastiaan Fuhler, Sukhvinder Johal, Mats Rosenlund, Kyle Dunton, Maarten Postma, Roel Freriks, A Comprehensive View of the Methods Used to Measure the Societal Impact of Healthcare Interventions: A Systematic Review, Value in Health, 10.1016/j.jval.2025.02.009, 28, 8, (1288-1299), (2025).
- Marco Bellone, Lorenzo Pradelli, Stefano Molica, Adele Emanuela De Francesco, Daniela Ghislieri, Emanuele Guardalben, Antonietta Caputo, Obinutuzumab Plus Chemotherapy Compared with Rituximab Plus Chemotherapy in Previously Untreated Italian Patients with Advanced Follicular Lymphoma at Intermediate–High Risk: A Cost-Effectiveness Analysis, ClinicoEconomics and Outcomes Research, 10.2147/CEOR.S317885, Volume 13, (661-671), (2021).