Effects of clinical Pilates on the fitness in people with children with disabilities: a randomized controlled trial
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study aimed to examine the effects of Clinical Pilates Exercises (CPE) on Health-Related Physical Fitness in Primary Caregivers. Patients & methods: Fifty-five participants were randomly divided into the CPE group and the Control group. Individuals in the CPE group performed CPE two-times a week for 8 weeks. Results: The intergroup comparisons showed that there were significant differences in favor of the CPE group in the sit-up test, body extension endurance, body flexion endurance, side bridge (right), squat test and flexibility tests (p < 0.05). The intragroup comparisons revealed significant differences in the CPE group in the sit-up test, body flexion endurance, side bridge (both sides), squat test and flexibility tests (p < 0.05). Conclusion: CPEs are effective on improvement of health-related fitness parameters in the primary caregivers of children with disabilities.
Clinical trial registration number: NCT03729466.
The trial: background & rationale
In the context of this trial, children with disabilities were defined as children diagnosed with cerebral palsy, autism, Down syndrome, metabolic diseases, muscle disorders, language and speech, vision or hearing problems, or other neuromuscular disorders [1]. Tonus changes, muscle coordination problems, balance problems, emotional disorders and cognitive problems on various levels may be observed in these children [2].
In addition to problems that people with disabilities encounter, there are various problems that the caregivers of people with disabilities encounter, and these problems also have a set of consequences. Bringing up a disabled child is accepted as a significant source of burden and stress in caregivers [3–5]. Although the care provided by the caregivers of disabled children provides benefits for both the disabled individual and the society, their high care load may lead to physical and mental health problems [4]. Several problems experienced by these individuals such as physical, psychological, emotional, financial and social problems are named as ‘care burden’ [3]. Care burden affects especially the social environment, occupational and personal roles of caregivers negatively, and it may lead to burnout and other negative outcomes by potentially affecting their capacity to provide care [4]. Physical stresses in caregivers emerge as a result of long-term performance of tasks such as heavy lifting, turning, bathing, helping the child use the toilet and their transfers, putting the child to sleep, dressing and helping the child move [2,6–8]. As the child, especially with physical disabilities, gets older, their body weight increases, thus, causing an increase in the physical stress of the caregivers. Situations that require transportation of children during daily activities lead to an unbalanced load on the caregivers’ body and disruption of the body mechanics, thus, causing musculoskeletal problems such as muscle aches [9]. The primary pains are spinal [10]. Problems increase by the extension of the duration of care, and this leads to poor sleep quality, problems in family relationships, anxiety, depression, financial stress and lower quality of life in caregivers [8]. In addition, it has been reported that mothers caring for disabled children do not have access to assistive technology devices [11] and low rates of physical activity (PA) increase fatigue and physical burden [2,7]. Studies have shown that the distribution of the roles of the parents of children with disabilities changes, and mothers usually take care of the child. This increases the workload on mothers [11–15]. In this regard, the level of fatigue and body weight is higher in mothers in comparison to fathers [16]. It is known that the workload of mothers who continue to work increases even more than the mothers of children without disabilities [15]. Whether the caregivers of children with disabilities are women or men, they should provide care for their children by using their bodies carefully and safely. Caregivers should improve their physical parameters such as muscle strength, muscular endurance and flexibility to provide the personal care of the child with disabilities and meet their primary needs such as transportation, transfer, nutrition and hygiene [2].
According to some studies, social support provided to caregivers affects the health outcomes of the caregivers positively on the optimal level, is related to lower depression levels and better physical health [3], reduced the care burden of the caregivers and improves their quality of life [5,17,18]. Several intervention studies have been conducted to help caregivers cope with the problems they encounter, support them and improve their quality of life. Although most studies have focused on psycho-education or self-management interventions, this shows that these interventions refer to the needs of caregivers regarding the psychosocial effect of a chronic disease, but they do not discuss the preventive health behaviors that caregivers may adopt to reduce the potential negative psychological and physical outcomes regarding their roles [5,19]. With its physical and psychological benefits, PA is one of the most important self-management strategies that will probably help caregivers protect their health on a sufficient level for them to successfully perform their vital roles [5,20].
PA choices are also important. Especially, strengthening core area muscles that are known as the main source of the strength of the human body and improving muscular endurance will decrease the risk of musculoskeletal injury and help with carrying weights [21,22]. While studies in the literature on the effects of PA in caregivers are limited, there are studies reporting that PA is an important method with its physical and psychological benefits that is helpful in caregivers’ protection of their health on a level sufficient for their successful performance of their roles [5,23]. This is why there is a need for supportive interventions to alleviate the excessive burden on caregivers, improve them physically, socially and emotionally and increase their quality of life. A study where a 14-day yoga training was applied showed that the yoga training had positive effects of the anxiety and subjective well-being levels of caregivers. It was also reported that the breathing techniques, relaxation techniques and meditation practices in the yoga sessions also helped caregivers feel better in the physical, psychological, mental and social aspects and perceive and know themselves [24]. Another exercise method that uses breathing exercises and relaxation techniques, Clinical Pilates Exercises (CPE) with proven effectiveness of strengthening the core area is an approach that educates the mind, so that the body can control movement and posture consciously [25,26]. It is a biopsychosocial exercise model that aims to improve the harmony between mind and body with the active participation of patients [18,27]. Therefore, it is an effective model that increases the flexibility, muscle strength and muscle endurance of both healthy and sick individuals [28].
There are various studies on treatment of children with disabilities in the literature, while there are limited numbers of studies on the types of treatments that optimize problems encountered by the caregivers of children with disabilities. Relevant studies have generally focused on stress management and assessment and improvement of the psychosocial status of individuals with children with disabilities [17,18,29,30]. Strategies that may be applied to improve the physical fitness of these individuals have not been investigated. Therefore, the primary goal of our study was to examine the effects of CPE performed by the primary caregivers of children with disabilities on muscle strength, and secondarily, on muscular endurance and flexibility.
Design
This randomized controlled study was conducted at the exercise laboratory of the Physiotherapy and Rehabilitation Department of the Eastern Mediterranean University after ethical approval was obtained with the decision of the Eastern Mediterranean University Scientific Research and Publication Ethics Committee dated 2 April 2018 and numbered 2018/57-05. The participants were given written and verbal information, and their written informed consent was obtained before conducting the study.
This study is registered at the Clinical Trials website with the clinical trial number NCT03729466.
The study was carried out with the primary caregivers of children with disabilities who were brought to the Nicosia Special Education Center and Vocational Education Center for treatment.
Participants
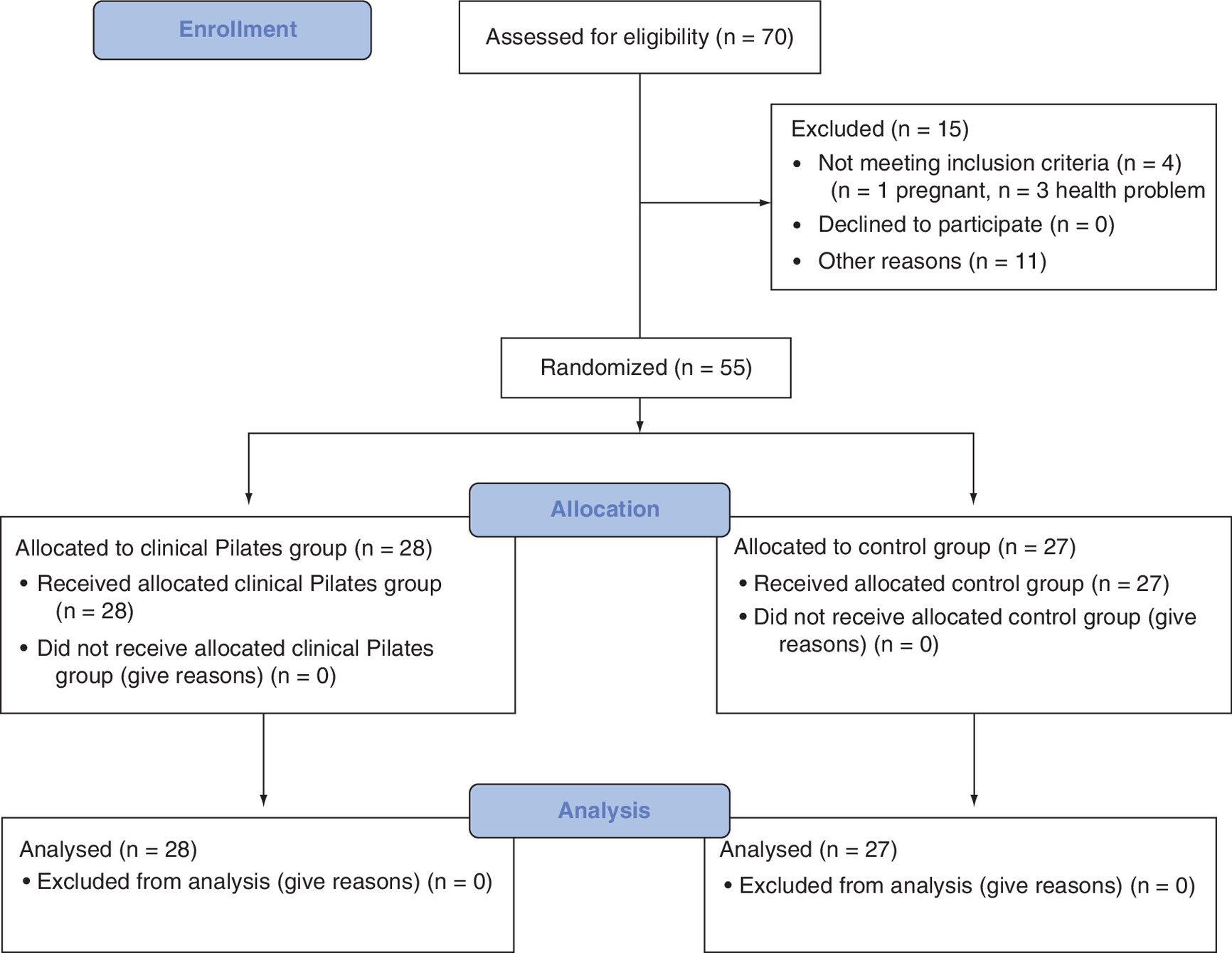
A prior sample size calculation for the study was carried out by conducting statistical tests with the G Power software (version 3.1.9.2) and taking the conventional effect size values recommended by Cohen into account [31]. Accordingly, the required sample size was calculated as 54 (assumptions of α = 0.05, β = 0.20 and effect size below d = 0.8). In the case of potential dropouts, the estimated number of the participants was increased by 30%, and the study was decided to be conducted with 70 individuals including 35 people in each group. Among the primary caregivers of 70 children with disabilities who came for the preinterview, 15 were excluded as they did not meet the inclusion criteria and did not have enough time to participate in the study. After the preinterviews, 55 individuals who met the inclusion criteria were divided into the exercise (n = 28) and control (n = 27) groups with one-block randomization using a randomized allocation software (Figure 1).
Inclusion criteria
Individuals who had not been doing regular exercise in the last 6 months, and who provided care for only one child (older than 3) with special needs for at least 6 months were included in the study.
Exclusion criteria
Pregnant women and those with serious orthopedic, psychiatric and neurological problems and those who had musculoskeletal system injuries in the last 6 months that would prevent them from performing CPE were excluded from the study.
Outcome measures
•
Muscle strength: The muscle strength of the participants, which was our primary outcome, was evaluated with three different tests as described below.
Sit-up test
This test that is used to assess rectus abdominis muscle strength determines the number of repetitions within 30 min. Diener et al. conducted the validity and reliability study of the test. The test–retest reliability was very high (r = 0.98), and the concurrent validity was moderately high (r = 0.38–0.66; p < 0.001) [32]. For the starting position, the individuals were positioned in the supine position with their hands in front, knees flexed at 90° and feet in full contact with the mat. The individuals were asked to perform body flexion with their head until their scapula lower angles were removed from the bed, and then, return to the starting position until their shoulders touched the mat. The number of completed body flexions was recorded.
Back-leg strength
A Takei digital back-leg dynamometer (TKK 5402 model, Takei Scientific Instruments Co. Ltd., Tokyo, Japan) was used to assess back and leg strength. To test back strength, the individuals were positioned on the dynamometer stand with their knees extended, back straight and body slightly flexed, and they were told to hold the dynamometer bar while their arms were stretched. The individuals were asked to pull the dynamometer bar upwards with maximum force.
To test leg strength, the individuals were positioned on the dynamometer stand with their back straight, body slightly flexed and knees flexed, and they were asked to pull the dynamometer bar and hold with stretched arms upward with maximum force. Both assessments were repeated three-times, and the average value of these three repetitions was obtained [33].
Grip strength
Grip test, which is a valid measurement instrument, was used to assess upper extremity strength. Grip strength was measured using a Takei digital grip dynamometer (TKK 5401 model, Grip-D, Takei Scientific Instruments Co. Ltd.). The participants’ grip strengths were assessed with a grip dynamometer whose reliability (for inter-rater reliability, the ICC value was 0.96; for test–retest reliability, the intraclass corelation coefficient [ICC] value was 0.82) test was performed by Mathiowetz et al. [34]. Grip strength was assessed in two positions. As the first position, the standard of the American Society of Hand Therapists (ASHT) which is in the sitting position, back neutral, shoulder adduction, elbow flexed at 90°, forearm supported on the chair and wrist at the neutral position was used [35]. Unlike the first position, the measurement was made with the elbows in full extension and in the standing position as the second position. The individuals were given one tryout before starting the test. The measurement was repeated three-times, and a 1-min rest period was given between each measurement. The test score was found by taking the average of the three measurements [36].
• Muscular endurance:
Body flexion endurance test
The body flexion endurance (BFE) test, one of the McGill endurance tests, was used to evaluate the abdominal muscle endurance of the participants. The BFE test is valid, where, in the study using receiver operating characteristic (ROC) analysis to evaluate the predictive validity of BFE, it was seen that ROC curve analysis revealed areas under the curve that were very close to or exceeded 0.70. Moreover, the intraclass coefficient correlations of the test were 0.90, and the Kappa indices were excellent [37]. The individuals were positioned with their knees flexed at 90°, the soles of their feet in full contact with the test table and their hands crossed in front of their chest. The angle between the body and test table was fixed at 45–60°, and the feet were fixed to the test table with a mobilization belt. Once the position was achieved, the clock was started and the individuals were asked to hold this position. Once the angle between the upper body and thigh changed, the clock was stopped and the test was ended. The period for which they maintained the position was recorded in seconds [38].
Body extension endurance test (Bering–Sorensen test)
The test that was developed by McGill was used to assess the endurance of the body extensor muscles. According to Latimer et al. who conducted the test, the test had good discriminant validity and was reliable (ICC: 0.83) [39]. The individuals were laid face down on the test table with their bodies’ idle and crystal iliacs on the tableside. Their ankles, knees and pelvises were fixed on the test table with a mobilization belt, and they were told to put their arms crossed in front of their chest. When the individuals were ready, they were asked to lift their upper body upward and keep their body and pelvis in a neutral position on the sagittal plane. The clock was started once they lifted their body upward, and when the body angle fell down by 10° from the starting position, or when the person left the test voluntarily, the clock was stopped and the test was ended. The period for which they maintained the position was recorded in seconds [38,40].
Side bridge test
One of the McGill tests, the side bridge (SB) test was used to assess the quadratus lumborum and anterolateral flat muscles among the lateral body muscles. Fax et al. conducted the validity and reliability study of the test [41]. The individuals were positioned on their forearms in the side-lying position with their lower elbow at 90°. Their feet were placed flat with the top leg resting in front of the other foot. The upper arm was fixed on the lower shoulder, and the pelvis was lifted from the floor. A straight line was formed from the head to the toe. The clock was started in this position, and it was stopped when the individuals were unable the hold this position or they lowered their pelvis to the floor. The test was conducted for both the right and left sides, and 5–7 min of break was given between the sides. The period for which they maintained the position was recorded in seconds [42].
Wall squat test
The squat test measures the muscular strength and endurance of the lower body, specifically the hips, quadriceps and hamstrings [43]. For this test, the individuals started in a standing position with their feet slightly forward and their backs against the wall and were asked to come to a sitting position with their knees not passing their feet. The clock was started once they squatted, and it was stopped when they changed the position. The period for which they maintained the position was recorded in seconds.
• Flexibility:
Sit & reach test
It was used to measure the flexibility of the hamstring and spine muscles. Ayala et al. showed acceptable reproducibility measures for the test with a 8.74% coefficient of variation and a 0.92 ICC. The criterion-related validity of the test was moderate [44]. The test material used in the study consists of a wooden attachment with a 55-cm length, 45-cm width and 35-cm height, a tape measure of 0–50 cm where the individual will reach with their arms, and a wooden box with a 35-cm length, 45-cm width and 32-cm height where the individual will place their feet. The individuals were positioned in a long sitting position with their soles in full contact with the wooden box. They were asked to perform an optimal body flexion, so that they could reach without lifting their knees off the ground and wait for 1–2 s at the last point. The test was conducted three-times, and the best score was recorded in centimeters [45].
Trunk lateral flexion test
Atya conducted the reliability and validity study of the test. The reliability of lateral flexion was good (ICC range: 0.81–0.82), but the validity results were weak [46]. For the test of lateral flexion, the individuals stood leaning back against the wall with their feet slightly open and parallel, and their arms stood next to their body. The distal points of the right and left third fingers were marked on the thigh. Then, they were asked to perform body lateral flexion as long as they could bend, and the distal point of the third finger was remarked on the last point reached at the thigh. The distance between the two marked points was measured with a tape and recorded in centimeters. The test was conducted bilaterally. Three repetitions were made for each side. The best score at the end of the test was recorded in centimeters [47].
Intervention
While the individuals in the CPE group received CPE training for 45–60 min twice a week for 8 weeks, no intervention was performed in the Control group (CG). The participants in the CG were warned not to perform sports other than their daily routine during this process. After the initial evaluations, the individuals in the CPE group were informed about the definition, goals and benefits of clinical Pilates, were familiarized with the exercises and how to use the five key elements of clinical Pilates (head–neck location – shoulder location – chest cage location – central focus [neutral position] – how they should preserve and maintain breathing). Two days after familiarization, the CPE training group sessions started in three phases (5 min of warm-up, 35–50 min of exercising and 5 min of cool-down). During the training, the exercises were performed in the standing, supine, side, sitting and face-down positions. CPEs were determined by the physiotherapist who had received CPE training, and the resistances of the elastic bands used during the exercises were individually adjusted. The exercises and the amounts of resistance were progressively increased in the 3rd and 6th weeks. All exercises were performed with ten repetitions and one set accompanied by a physiotherapist. An exercise mat, elastic resistance band and exercise ball were used during the training sessions with music. The exercises performed by the CPE group included the following in order:
•
Warm-up phase: Roll down, upper extremity proprioceptive neuromuscular facilitation (PNF) patterns, toy soldier and minisquat exercises.
•
Exercise phase:
○
Stage 1 (between 0th and 3rd weeks): Abdominal preparation, one leg stretch [2], double leg stretch [2,3], shoulder bridge, hip twist, arm opening, clam, lift lower, mermaid, biceps curl, triceps pull, cobra, stretching exercises (butterfly, hamstring-lumbar extension stretching) and breathing exercises.
○
Stage 2 (between 3rd and 6th weeks): Hundreds [3], oblique preparation, double leg stretch [4], shoulder bridge [2], scissors [4], side kick press, leg lifts, diamond press with arm openings, roll up with obliques, side bend, swimming [2], breaststroke preparation, stretching exercises (butterfly, hamstring-lumbar extension stretching) and breathing exercises.
○
Stage 3 (between 6th and 8th weeks): Hundreds [4], point and flex, one leg circle [2], criss-cross, heels together toes apart, side circle, sidekick in kneeling, open book, roll up with biceps, cleopatra, breaststroke, swimming [2], stretching exercises (butterfly, hamstring-lumbar extension stretching) and breathing exercises.
•
Cool-down phase: the saw, cat stretch, shell, swinging exercises.
Statistical analysis
The data were analyzed using the IBM SPSS Statistics V.20.0.0 program. Shapiro–Wilk test was used to determine whether the data showed a normal distribution. Nonparametric statistical tests were used as the data did not show normal distribution. Mann–Whitney U test was used for the intergroup comparisons of the continuous variables, while Wilcoxon paired-samples test was used for the intragroup comparisons. Fisher’s exact Chi-squared test was used for the intergroup comparisons of the categorical variables. The statistical significance level was determined as p < 0.05. The variables used in the study are expressed in frequencies, percentages (%), mean ± standard deviation (x ± SD), medians and interquartile range.
Effect sizes were calculated to test clinical significance. For the effect size calculation, the formula was used. The effect was interpreted as large when r ≥ 0.5, as moderate when r = 0.3 and as small when r ≤ 0.1 [48].
Data analysis
The sociodemographic characteristics of the participants other than their BMI values were similar (for all p-values: p < 0.05). All the participants in the CPE group were female, and 88.9% (female = 24, male = 3) of CG were female. The mean age of the children who were given care in the CPE group was 10.1 ± 5.2 years, while it was 9.3 ± 4.9 years in the CG. No significant differences were found between the mean ages of the children and the caregivers in both groups, maintenance time and the disability types of these children (for all p-values: p < 0.05; Table 1).
| Variables | Clinical Pilates group N = 28 | Control group N = 27 | p-value |
|---|---|---|---|
| Age (y) x ± SD | 36.8 ± 9.6 | 41.1 ± 9.7 | 0.13† |
| BMI (kg/m2), x ± SD | 24.4 ± 5.4 (22.3–26.5) | 26.6 ± 4.5 (24.8–28.4) | 0.031† |
| Sex, n (%) – Male – Female | – 28 (100.0) | 3 (11.1) 24 (88.9) | 0.11§ |
| Age of disabled children (y) x ± SD | 10.1 ± 5.2 | 9.3 ± 4.9 | 0.543† |
| Care duration (y) x ± SD | 10.1 ± 5.2 | 9.3 ± 5.00 | 0.566† |
| Types of disabilities, n (%) Physical disability Intellectual disability Vision impairment – Mixed | 4 (14.3) 10 (35.7) – 14 (50.0) | 5 (18.5) 9 (33.3) 1 (3.7) 12 (44.4) | 0.905§ |
†
Mann–Whitney U test.
‡
Chi-squared test.
§
Fisher’s exact test.
SD: Standard deviation.
According to the intergroup comparisons, the pretest results of all muscle strength tests were statistically similar, while a statistically significant difference was found between the post-test results of only the sit-up test (p = 0.00; Table 2).
| Variables | Group | Pretest | Post-test | p3 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M-IQR | p1 | x ± SD | M-IQR | p2 | R | |||||
| Muscle strength | Back muscle strength, kg | CPE | 48.3 ± 19 | 48.1–30.3 | 0.381 | 56.4 ± 16.9 | 58.2–25.6 | 0.359 | <0.000‡ | 0.796 |
| Control | 54.2 ± 22.4 | 50.2–36 | 52.9 ± 22.3 | 54–26.7 | 0.280 | 0.204 | ||||
| Leg muscle strength, kg | CPE | 46.3 ± 16.7 | 42.7–27.7 | 0.788 | 53.5 ± 15.1 | 52.7–20.1 | 0.070 | <0.000‡ | 0.770 | |
| Control | 49.6 ± 23.8 | 48.3–26.2 | 48.1 ± 22.8 | 46–25.3 | 0.127 | 0.288 | ||||
| Grip strength (WFP) (right), kg | CPE | 20.3 ± 5.8 | 19.7–7.2 | 0.900 | 22.1 ± 5.8 | 21.6–8.5 | 0.141 | <0.000‡ | 0.792 | |
| Control | 21.3 ± 9.4 | 17.7–13.2 | 20.2 ± 8.6 | 17.2–12.7 | 0.002† | 0.577 | ||||
| Grip strength (WFP) (left), kg | CPE | 19.5 ± 5.3 | 19.8–6.8 | 0.886 | 21.7 ± 4.7 | 22.5–5.9 | 0.083 | <0.000‡ | 0.762 | |
| Control | 20.8 ± 9.2 | 19.9–11.8 | 19.6 ± 7.9 | 18.4–8.9 | 0.031† | 0.409 | ||||
| Grip strength (WEP) (right), kg | CPE | 20.8 ± 5.7 | 19.9–7.8 | 0.827 | 22 ± 5.4 | 22.2–5.4 | 0.096 | 0.024† | 0.426 | |
| Control | 21.7 ± 8.2 | 19–12.2 | 20.5 ± 7.5 | 18.3–10.4 | 0.041† | 0.386 | ||||
| Grip strength (WEP) (left), kg | CPE | 20.1 ± 5.4 | 20–8.6 | 0.711 | 21.1 ± 4.8 | 21.3–5.8 | 0.333 | 0.025† | 0.424 | |
| Control | 21 ± 8.1 | 21.5–9.7 | 20.2 ± 7.5 | 18.9–8.9 | 0.029† | 0.413 | ||||
| Sit-up test, the number of repetitions | CPE | 14.8 ± 4.7 | 14.5–5.8 | 0.251 | 18.6 ± 4.1 | 18–3.8 | 0.000‡ | <0.000‡ | 0.865 | |
| Control | 13.3 ± 5.7 | 12–9 | 11.6 ± 5.1 | 11–5 | 0.006† | 0.523 | ||||
| Muscular endurance | Trunk flexion endurance test, s | CPE | 24.9 ± 16.9 | 20.5–18.8 | 0.893 | 36.1 ± 20.1 | 28.9–26.9 | 0.000‡ | <0.000‡ | 0.826 |
| Control | 25.8 ± 18.1 | 19.9–28.8 | 19.9 ± 14.6 | 16.3–11.4 | 0.007† | 0.509 | ||||
| Trunk extension endurance test, s | CPE | 16.8 ± 14.1 | 14.8–15.1 | 0.833 | 31.3 ± 18.8 | 26.1–23.8 | 0.002‡ | <0.000‡ | 0.865 | |
| Control | 18.4 ± 19.3 | 10.9–28.7 | 16.3 ± 15.2 | 12.1–27.5 | 0.715 | 0.069 | ||||
| Side bridge test (right), s | CPE | 17.5 ± 12 | 15.3–16.1 | 0.686 | 26.9 ± 16 | 22.6–30.9 | 0.010† | <0.000‡ | 0.822 | |
| Control | 18.1 ± 16.6 | 11.7–24.8 | 16.9 ± 15.1 | 11–20.2 | 0.290 | 0.200 | ||||
| Side bridge test (left), s | CPE | 16.4 ± 10.8 | 14.5–15 | 0.762 | 25.9 ± 15.5 | 21.7–22.9 | 0.009‡ | <0.000‡ | 0.869 | |
| Control | 18.6 ± 17.9 | 11.3–17.7 | 17.3 ± 17.7 | 10.9–19.4 | 0.046† | 0.377 | ||||
| Squat test, s | CPE | 38.6 ± 22.7 | 42.6–29 | 0.860 | 55.3 ± 35 | 51.6–29.4 | 0.003‡ | <0.000‡ | 0.740 | |
| Control | 43.5 ± 42.4 | 28–37.8 | 34.9 ± 30 | 22.8–30.1 | 0.003† | 0.563 | ||||
| Flexibility | Sit and reach test | CPE | 12.4 ± 6.7 | 12.3–6.9 | 0.209 | 17.3 ± 6.3 | 16.5–6.6 | 0.000‡ | <0.000‡ | 0.875 |
| Control | 10.3 ± 5.6 | 10–7.5 | 10 ± 5.3 | 10–8 | 0.251 | 0.217 | ||||
| Trunk lateral flexion test (right) | CPE | 18.6 ± 3.5 | 18.8–5 | 0.619 | 18.5 ± 3.6 | 18.5–4.6 | 0.000‡ | <0.000‡ | 0.823 | |
| Control | 18.2 ± 4.2 | 18–7.5 | 17.9 ± 3.8 | 18–6.5 | 0.213 | 0.235 | ||||
| Trunk lateral flexion test (left) | CPE | 21.8 ± 3.2 | 21.5–3.9 | 0.590 | 21.7 ± 3 | 21.8–4 | 0.000‡ | <0.000‡ | 0.843 | |
| Control | 17.7 ± 3.9 | 17.5–5.5 | 17.4 ± 3.2 | 17.5–5 | 0.194 | 0.245 | ||||
†
p < 0.05.
‡
p < 0.01.
CPE: Clinical Pilates Exercise; IQR: Interquartile range; p1: Mann–Whitney U test between the groups’ pretest results; p2: Mann–Whitney U test between the groups post-test results; p3: Wilcoxon test between the pretest and post-test results for each group; SD: Standard deviation; WEP: Wrist extension position; WFP: Wrist flexion position.
The study found a large effect size in all of the assessment results of the CPE group, back and leg strength, right and left flexion grip strength and sit-up test due to the CPE training (r ≥0.5), and it found a moderate effect size in the right and left extension grip strengths (r = 3; Table 2).
According to the intragroup comparisons of the CG, a statistically significant decrease was found in all strength parameters apart from the back and left strengths (p > 0.05) at the end of the 8 weeks (p < 0.05; Table 2).
The fact that individuals in the CG did not perform any PA for 8 weeks negatively affected their handgrip strength (left) in elbow flexion position and handgrip strength (right and left) in elbow extension position on clinically medium and high levels (5 < r ≥ 0.3), and flexion grip strength (right) and sit-up test results were negatively affected on high levels (r ≥ 0.5; Table 2).
The intergroup comparisons of the muscular endurance tests showed that there were statistically significant differences between the post-test results of the BFE, body extension endurance test, SB (right and left) and wall squat tests (p < 0.05; Table 2).
According to the intragroup comparisons in the CPE group, there were significant differences between the pretest and post-test values of all endurance tests (for all p-values: p < 0.05). When the intragroup clinical effect sizes were examined, the study found that the parameters with significant differences had high effect sizes (for all p-values: p < 0.05; Table 2).
Comparing the pretest and post-test assessment results of the CG, there was a significant difference between the pretest and post-test values of the BFE and wall squat test (p < 0.05), while there were no significant differences in all other parameters (for all p-values: p < 0.05). A statistically significant decrease was found in the BFE and wall squat values (Table 2). This decrease had a clinical effect size on medium and high levels (r ≥ 0.5; Table 2).
The intergroup comparisons of the flexibility (post-test) results showed that there were significant differences between the results of all flexibility tests (for all p-values: p < 0.05; Table 2). Comparing the test results of the CPE group before and after the 8-week-long training, a statistically significant difference was found (for all p-values: p < 0.05; Table 2). The clinical effect sizes in all flexibility parameters were found to be high (r ≥ 0.5; Table 2).
There were no statistically significant differences in the intergroup comparisons of the flexibility measurements of CG (for all p-values: p > 0.05; Table 2).
The clinical effect sizes in all flexibility parameters were found to be between low and moderate (0.3 > r >0.1; Table 2).
Discussion
According to the results of this study that examined the effect of CPE performed with the primary caregivers of children with disabilities on their physical parameters, in the sit-up test, there were statistically significant differences in the muscular endurance and flexibility tests in favor of the CPE group. According to intergroup comparisons of the CPE group, the 8-week-long training program caused a statistically significant increase in the abdominal muscle strength, muscular endurance and flexibility and a statistically significant decrease in the muscle strength and muscular endurance in CG. Additionally, the 8-week-long CPE program was found to have a clinically large effect size on strength, which was the primary measurement, muscular endurance and flexibility.
Studies have shown that the distribution of the roles of parents of children with disabilities changes, and mothers usually take care of the child, thus, increasing the workload on mothers [11–14,49]. Individuals are recommended to participate in PA or regular exercise programs that increase their physical fitness to meet the requirements of increased workload [50]. The study found that CPE performed two-times a week for 8 weeks improved abdominal muscle strength, as well as increasing back and leg muscle strength. However, this increase was not significant. When the literature on treatment methods applied for caregivers was examined, it was observed that studies have been rather on the psychosocial problems of individuals. Very few studies discussing caregivers holistically and applying exercise models toward their physical problems have been encountered. In a study where the physical and psychological effects of a 6-month PA program applied on the caregivers of elderly individuals were examined, the caregivers were divided into groups for yoga, strength training and Tai Chi training. As a result of the study, it was reported that there were significant improvements in all groups in terms of the individuals’ physical function, leg strength, balance and walking endurance [51]. In another study that provided 8 weeks of yoga training to caregivers, physical health and coping attitudes were investigated. As a result of the study, it was found that there was a significant increase in lower extremity muscle strength, and although not statistically significant, there were individual improvements in the coping, upper extremity muscle strength, flexibility, balance and aerobic endurance parameters in the caregivers [52]. While there are no studies on CPE in caregivers, in studies conducted with healthy individuals, CPE training had a clinically large effect size on all body and lower extremity muscle strength and body endurance measurements. The movements in CPE include exercises with approved effectiveness in electromyography studies on target muscles [53,54]. Previous studies have shown that bridge and unilateral bridge exercises in CPEs stretch the multifidus and longissimus thoracis muscles in the most active way. The same studies also showed that swimming exercises do not affect muscle activation of the core area as well as bridge exercises, but they have an effective role in correcting balance [53,54]. Studies which examined the effects of anterior and posterior pelvic tilt performed on the sagittal plane on the multifidus, transversus abdominus, rectus abdominus, external abdominal obliques, erector spinae and rectus femoris muscles found that transversus abdominus activation was high during posterior pelvic tilt that is the basis of clinical Pilates [55,56]. Srivastav et al. conducted a study evaluating effects on abdominal muscle strength on different surfaces and reported that bridge exercise performed on an exercise ball caused greater gravity center control and better spinal muscle stabilization due to its limited support base than that performed on a cushion [55]. Studies have shown that using an elastic-resistant band in Pilates exercises is more effective in improving muscle strength on the grounds that it provides external power [57,58]. Additionally, Anderson et al. reported that performing Pilates exercises with breathing exercises activates the deep muscles on the core area [59]. As a result of the study, the reason for the improvement of the body and lower extremity muscle strength and body endurance in the CPE group was that the exercises used in this study were the most effective exercises proven by electromyography (EMG) studies in developing specific muscular activation as reported in the studies mentioned above. Combining exercises with accurate breathing training in the treatment sessions may have increased the activation of the core muscles while using unstable surfaces, and the resistant bands may have contributed to the improvement of strength and endurance by causing external loads.
Upper extremity mobility is associated with grip ability, and grip has an important role in increasing the quality of extremity mobility. Therefore, grip is important to be able to perform daily life activities in good quality [60]. Additionally, grip strength is a health marker that is commonly used to estimate whole-body strength [61,62]. Various authors have stated that grip strength is a determinant of the general body strength, postoperative complications, mortality and functional decrease [61,62]. The primary caregivers of children with disabilities need core and lower extremity strength and endurance while meeting the care needs of children with every type of disability. However, they experience difficulties while meeting the transportation, transfer, nutrition and hygiene needs of such children. Thus, they also need upper extremity strength [63]. Therefore, this study assessed both general muscle strength and grip strength to determine the functional status of the upper extremities. The study found that CPE increased grip strength. However, this increase was not statistically significant. The CPE training had clinically large effect sizes on all grip strength parameters. In one study examining grip strength in caregivers, it was found that 8 weeks of yoga training did not significantly increase the upper extremity strength of these individuals, but it improved their grip strength and affected their activities positively [52]. Moreover, many studies in the literature have shown that improvement in core muscle strength affects the distal joints and increases the quality of mobility [21,25]. Similarly, a study where core strength training was performed with swimming training for 8 weeks by sedentary women found that grip strength improved along with the other assessed muscles in the group that got core training compared with the control group which only got swimming training [62]. The same study reported that including sedentary individuals in the exercise group that got core training may contribute positively to development of motor skills [62]. Another study conducted with sedentary women showed that a 12-week-long aerobic exercise program increased dominant handgrip strength. The authors reported that the increase in general strength might increase grip strength [62]. This study determined the core exercises that included CPEs performed with sedentary individuals might have increased their body muscle strength and endurance, as well as improving grip strength by showing distal spread of strength increase.
For daily life activities, performance needs to be continued for long periods for numerous activities. Therefore, muscular endurance is an important aspect of physical performance and should be taken into consideration while assessing musculoskeletal functions [61]. The lower extremity muscular endurance in caregivers who need to resist increased physical stress is significant for the continuity of daily activities of themselves and the children they take care of. Katayifçi et al. examined the effects of CPEs that they performed with healthy individuals for 8 weeks on physical fitness and carried out assessments before and after Pilates training, and in the 6th and 12th weeks after training. Significant improvements were found in all parameters (body, upper and lower extremity muscle strengths, muscular endurance and flexibility, balance and cardiovascular) assessed at the end of the study. They reported that the CPEs maintained their effects on muscle strength, flexibility, endurance (squat test), balance and walking distance even at the end of the 12th week [28]. The authors attributed the positive effect of CPE on muscular endurance to the fact that the exercises were composed of multiple muscle synergies including isometric, eccentric and concentric muscle contractions and co-contractions, as well as their ability to be adapted into daily life activities. Moreover, a study conducted with healthy individuals reported that an increase in muscular endurance occurred after an 8-week-long Pilates training [64]. Another study assessing the effects of CPE showed that CPE had positive results on improving lower extremity endurance [65]. The results of the wall squat test that was used to assess quadriceps endurance were similar to the results of the study by Katayifçi et al. We are of the opinion that the 8-week-long exercise program contributed to improving the muscle strength, as well as improving the lower extremity muscular endurance of multiple muscle synergies including different contraction types.
Flexibility enables daily life activities to be performed effectively and sufficiently by maintaining the normal opening of the joints in the body. Increasing age, hormonal changes and sedentary life cause the range of motion to decrease gradually [66]. Therefore, flexibility training is recommended as an important part of performance- or health-related exercise trainings and should be included in exercise programs. The literature argues that flexibility exercises should be performed with exercise methods rather than training alone [66]. The study found that the body and hamstring flexibility significantly increased and had a high clinical effect in the CPE group. A study providing 8 weeks of yoga training for caregivers observed that flexibility was increased. In the study, it was reported that especially the presence of breathing technique and unique stances within the yoga training provided positive effects on the flexibility parameter [52]. While there have been no studies on CPE training applied with caregivers, various studies investigating the effects of exercise methods like reformer Pilates and clinical Pilates applied with sedentary individuals on flexibility and functionality stated that static stretching taking place between warming up and cooling down may be useful for increasing flexibility [50–54]. Additionally, performing stretching exercises such as ‘the saw, leg stretch, roll down, swan dive,’ which were included in the exercises slowly, in a controlled manner and with breathing was stated to improve both flexibility and body awareness [66–70]. The fact that the program included stretching exercises, warm-up and cool-down phases, and all movements were combined with breathing might have caused an increase in flexibility. Performing exercises slowly, in a controlled manner and rhythmically might have increased stretching.
Limitation
The CPE program was performed for 2 days a week for 8 weeks in this study. In studies in the literature, it was performed 3 days a week for at least 8 weeks [28,65]. However, the fact that the participants had children with disabilities brought a lot of responsibility with it. Therefore, it was necessary to decrease the number of days in this study because the participants did not have enough time. This was the limitation of the study.
Conclusion
The study found that CPEs performed for 8 weeks are a biopsychosocial exercise method that is effective on improving flexibility, muscle strength and muscular endurance among the health-related physical fitness parameters of individuals who provide care for children with disabilities.
•
In addition to problems that people with disabilities encounter, there are various problems that their caregivers encounter.
•
Physical stresses in caregivers emerge as a result of long-term performance of tasks such as heavy lifting, turning, bathing and other tasks.
•
This randomized controlled study was carried out to examine the effects of clinical Pilates exercises on the health-related physical fitness in caregivers of children with disabilities.
•
Clinical Pilates exercises were found to be an effective method of improving physical fitness parameters such as muscular strength, muscular endurance and flexibility.
Author contributions
Y Senturk, B Kirmizigil, EH Tuzun contributed to the literature review and topic identification. B Kirmizigil and EH Tuzun were responsible for the screening of people to be included in the research. Application phase of the study was done by Y Senturk. Writing phase of the article was completed by EH Tuzun, B Kirmizigil and Y Senturk.
Acknowledgments
The authors express their thanks to Spec. Özlem Akşit for their assistance.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This randomized controlled study was conducted at the exercise laboratory of the Physiotherapy and Rehabilitation Department of the Eastern Mediterranean University after the ethical approval was obtained with the decision of Eastern Mediterranean University Scientific Research and Publication Ethics Committee dated 2 April 2018 and numbered 2018/57-05. The participants were given written and verbal information, and their written informed consent was obtained before conducting the study.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. Deidentified, individual data that underlie the results reported in this article will be available from the authors on request. Clinical trial registration number: NCT03729466.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Schuster MA, Chung PJ, Elliott MN, Garfield CF, Vestal KD, Klein DJ. Perceived effects of leave from work and the role of paid leave among parents of children with special health care needs. Am. J. Public Health 99(4), 698–705 (2009).
2.
Sharan D, Ajeesh P, Rameshkumar R, Manjula M. Musculoskeletal disorders in caregivers of children with cerebral palsy following a multilevel surgery. Work 41(Suppl. 1), 1891–1895 (2012).
3.
Oh H, Lee EKO. Caregiver burden and social support among mothers raising children with developmental disabilities in South Korea. Int. J. Disabil. Devel. Educ. 56(2), 149–167 (2009).
4.
Cohen SA, Cook S, Kelley L, Sando T, Bell AE. Psychosocial factors of caregiver burden in child caregivers: results from the new national study of caregiving. Health Qual. Life Outcomes 13(1), 1–6 (2015).
5.
Lambert SD, Duncan LR, Kapellas S et al. A descriptive systematic review of physical activity interventions for caregivers: effects on caregivers’ and care recipients’ psychosocial outcomes, physical activity levels, and physical health. Ann. Behav. Med. 50(6), 907–919 (2016).
6.
Eker L, Tüzün EH. An evaluation of quality of life of mothers of children with cerebral palsy. Disabil. Rehabil. 26(23), 1354–1359 (2004).
7.
Whiting M. Children with disability and complex health needs: the impact on family life. Nurs. Child. Young People 26(3), 26–30 (2014).
8.
Javalkar K, Rak E, Phillips A, Haberman C, Ferris M, Van Tilburg M. Predictors of caregiver burden among mothers of children with chronic conditions. Children 4(5), 39 (2017).
9.
Geere J, Gona J, Omondi F, Kifalu M, Newton C, Hartley S. Caring for children with physical disability in Kenya: potential links between caregiving and carers’ physical health. Child Care Health Dev. 39(3), 381–392 (2013).
10.
Kaya K, Unsal-Delialioglu S, Ordu-Gokkaya NK et al. Musculo-skeletal pain, quality of life and depression in mothers of children with cerebral palsy. Disabil. Rehabil. 32(20), 1666–1672 (2010).
11.
Barnett WS, Boyce GC. Effects of children with Down syndrome on parents’ activities. Am. J. Ment. Retard. 100(2), 115–127 (1995).
12.
Hedov G, Annerén G, Wikblad K. Self-perceived health in Swedish parents of children with Down’s syndrome. Qual. Life Res. 9(4), 415–422 (2000).
13.
Lukemeyer A, Meyers MK, Smeeding T. Expensive children in poor families: out-of-pocket expenditures for the care of disabled and chronically ill children in welfare families. J. Marriage Fam. 62(2), 399–415 (2000).
14.
Powers ET. New estimates of the impact of child disability on maternal employment. Am. Econ. Rev. 91(2), 135–139 (2001).
15.
Westbom L. Impact of chronic illness in children on parental living conditions. A population-based study in a Swedish primary care district. Scand. J. Prim. Health Care 10(2), 83–90 (1992).
16.
Sahida K, Allenidekania A. The relationship between characteristics of parent-child and level fatigue of parents with autism spectrum disorder. UI Proc. Health Med. 2, (2017).
17.
Jackson AC, Liang RPT, Frydenberg E, Higgins RO, Murphy BM. Parent education programmes for special health care needs children: a systematic review. J. Clin. Nursing 25(11–12), 1528–1547 (2016).
18.
Whittingham K, Wee D, Boyd R. Systematic review of the efficacy of parenting interventions for children with cerebral palsy. Child Care Health Dev. 37(4), 475–483 (2011).
• Evaluates the effects of exercise (especially clinical Pilates exercises) on physical performance.
19.
Northouse LL, Katapodi MC, Song L, Zhang L, Mood DW. Interventions with family caregivers of cancer patients: meta-analysis of randomized trials. CA Cancer J. Clin. 60(5), 317–339 (2010).
• Evaluates the effects of exercise (especially clinical Pilates exercises) on physical performance.
20.
Reiner M, Niermann C, Jekauc D, Woll A. Long-term health benefits of physical activity – a systematic review of longitudinal studies. BMC Public Health 13(1), 1–9 (2013).
• Evaluates the effects of exercise (especially clinical Pilates exercises) on physical performance.
21.
Saeterbakken AH, Fimland M, Navarsete J, Kroken T, van der Tillaar R. Muscle activity, and the association between core strength, core endurance and core stability. J. Novel. Physiother. Phys. Rehabil. 2(2), 028–034 (2015).
22.
Shami PA, Mughal AW, Khizar A. Relationship of upper and lower body muscular strength with cardio-respiratory endurance among school going children. SPARK 3(1), 163–172 (2019).
23.
Martin AC, Keats MR. The impact of yoga on quality of life and psychological distress in caregivers for patients with cancer. Oncol Nurs. Forum 41(3), 257–264 (2014).
24.
Bernardi MLD, Amorim MHC, Salaroli LB, Zandonade E. Effects of Hatha Yoga on caregivers of children and adolescents with cancer: a randomized controlled trial. Escola Anna Nery 24, 1 (2020).
25.
Atılgan E, Aytar A, Çağlar A et al. The effects of clinical Pilates exercises on patients with shoulder pain: a randomised clinical trial. J. Bodyw. Mov. Ther. 21(4), 847–851 (2017).
• Evaluates the effects of exercise (especially clinical Pilates exercises) on physical performance.
26.
Katayifçi N, Düger T, Edibe Ü. Sağlıklı bireylerde klinik Pilates egzersizlerinin fiziksel uygunluk üzerine etkisi. J. Exercise Ther. Rehabil. 1(1), 17–25 (2014).
•• Evaluates the effects of exercise (especially clinical Pilates exercises) on physical performance.
27.
Oksuz S, Unal E. The effect of the clinical pilates exercises on kinesiophobia and other symptoms related to osteoporosis: randomised controlled trial. Complement. Ther. Clin. Pract. 26, 68–72 (2017).
28.
Küçük F, Livanelioglu A. Impact of the clinical Pilates exercises and verbal education on exercise beliefs and psychosocial factors in healthy women. J. Phys. Ther. Sci. 27(11), 3437–3443 (2015).
29.
Bunting L. Parenting programmes: the best available evidence. Child Care Pract. 10(4), 327–343 (2004).
30.
Sanders MR, Markie-Dadds C, Tully LA, Bor W. The triple P-positive parenting program: a comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. J. Consult. Clin. Psychol. 68(4), 624 (2000).
31.
Cohen J. Statistical power analysis. Curr. Dir. Psychol. Sci. 1(3), 98–101 (1992).
32.
Diener MH, Golding LA, Diener D. Validity and reliability of a one-minute half sit-up test of abdominal strength and endurance. Res. Sports Med. 6(2), 105–119 (1995).
33.
Ozcan A, Donat H, Gelecek N, Ozdirenc M, Karadibak D. The relationship between risk factors for falling and the quality of life in older adults. BMC Public Health 5(1), 90 (2005).
34.
Mathiowetz V, Weber K, Volland G, Kashman N. Reliability and validity of grip and pinch strength evaluations. J. Hand Surg. 9(2), 222–226 (1984).
35.
Peolsson A, Hedlund R, Öberg B. Intra-and inter-tester reliability and reference values for hand strength. J. Rehabil. Med. 33(1), 36–41 (2001).
36.
Gerodimos V. Reliability of handgrip strength test in basketball players. J. Hum. Kinet. 31(1), 25–36 (2012).
37.
del Pozo-Cruz B, Mocholi MH, del Pozo-Cruz J, Parraca JA, Adsuar JC, Gusi N. Reliability and validity of lumbar and abdominal trunk muscle endurance tests in office workers with nonspecific subacute low back pain. J. Back Musculoskel. Rehabil. 27(4), 399–408 (2014).
38.
Watson T, Graning J, McPherson S et al. Dance, balance and core muscle performance measures are improved following a 9-week core stabilization training program among competitive collegiate dancers. Int. J. Sports Phys. Ther. 12(1), 25 (2017).
39.
Latimer J, Maher CG, Refshauge K, Colaco I. The reliability and validity of the Biering–Sorensen test in asymptomatic subjects and subjects reporting current or previous nonspecific low back pain. Spine 24(20), 2085 (1999).
40.
Butowicz CM, Ebaugh DD, Noehren B, Silfies SP. Validation of two clinical measures of core stability. Int. J. Sports Phys. Ther. 11(1), 15 (2016).
41.
Fax E, Holmes T, Bazett-Jones DM. Reliability and validity of the side bridge endurance test with different shoulder support positions. Med. Sci. Sports Exercise 47(5S), 226 (2015).
42.
Barati A, Safarcherati A, Aghayari A, Azizi F, Abbasi H. Evaluation of relationship between trunk muscle endurance and static balance in male students. Asian J. Sports Med. 4(4), 289 (2013).
43.
Lubans DR, Morgan P, Callister R et al. Test–retest reliability of a battery of field-based health-related fitness measures for adolescents. J. Sports Sci. 29(7), 685–693 (2011).
44.
Ayala F, de Baranda PS, Croix MDS, Santonja F. Reproducibility and criterion-related validity of the sit and reach test and toe touch test for estimating hamstring flexibility in recreationally active young adults. Phys. Ther. Sport 13(4), 219–226 (2012).
45.
Kirmizigil B, Ozcaldiran B, Colakoglu M. Effects of three different stretching techniques on vertical jumping performance. J. Strength Cond. Res. 28(5), 1263–1271 (2014).
46.
Atya AM. The validity of spinal mobility for prediction of functional disability in male patients with low back pain. J. Adv. Res. 4(1), 43–49 (2013).
47.
Sertel M, Yümin ET. Yaşlı bireylerde gövde esnekliği ve kısa fiziksel performansın denge ile ilişkisinin incelenmesi. İnsan ve Toplum Bilimleri Araştırmaları Dergisi 6(1), 591–601 (2017).
48.
Lodewijkx HF, Brouwer B, Kuipers H, Van Hezewijk R. Overestimated effect of epo administration on aerobic exercise capacity: a meta-analysis. Am. J. Sports Sci. Med. 1(2), 17–27 (2013).
49.
Garip Y, Ozel S, Tuncer OB, Kilinc G, Seckin F, Arasil T. Fatigue in the mothers of children with cerebral palsy. Disabil. Rehabil. 39(8), 757–762 (2017).
50.
Ebrahimi H, Balouchi R, Eslami R, Shahrokhi M. Effect of 8-week core stabilization exercises on low back pain, abdominal and back muscle endurance in patients with chronic low back pain due to disc herniation. Physical Treatments. 4(1), 25–32 (2014).
51.
Hill K, Smith R, Fearn M, Rydberg M, Oliphant R. Physical and psychological outcomes of a supported physical activity program for older carers. J. Aging Phys. Activity 15(3), 257–271 (2007).
52.
Van Puymbroeck M, Payne LL, Hsieh P-C. A Phase I feasibility study of yoga on the physical health and coping of informal caregivers. Evid. Based Complement. Alternat. Med. 4(4), 519–529 (2007).
53.
Xiao J, Sun J, Gao J, Wang H, Yang X. The activity of surface electromyographic signal of selected muscles during classic rehabilitation exercise. Rehabil. Res. Pract. 2016, 4796875 (2016).
54.
Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J. Orthopaed. Sports Phys. Ther. 37(12), 754–762 (2007).
55.
Srivastav P, Nayak N, Nair S, Sherpa LB, Dsouza D. Swiss ball versus mat exercises for core activation of transverse abdominis in recreational athletes. J. Clin. Diagnost. Res. 10(12), YC01 (2016).
56.
Takaki S, Kaneoka K, Okubo Y et al. Analysis of muscle activity during active pelvic tilting in sagittal plane. Phys. Ther. Res. 19(1), 50–57 (2016).
57.
Plachy J, Kovách M, Bognár J. Improving flexibility and endurance of elderly women through a six-month training programme. Hum. Mov. 13(1), 22–27 (2012).
58.
Irez GB, Ozdemir RA, Evin R, Irez SG, Korkusuz F. Integrating Pilates exercise into an exercise program for 65+ year-old women to reduce falls. J. Sports Sci. Med. 10(1), 105 (2011).
59.
Anderson BD, Spector A. Introduction to Pilates-based rehabilitation. Orthopaed. Phys. Ther. Clin. N. Am. 9(3), 395–410 (2000).
60.
Cetinus E, Buyukbese MA, Uzel M, Ekerbicer H, Karaoguz A. Hand grip strength in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 70(3), 278–286 (2005).
61.
White C, Dixon K, Samuel D, Stokes M. Handgrip and quadriceps muscle endurance testing in young adults. Springerplus 2(1), 451 (2013).
62.
Akyol P, İmamoğlu O. The effects of a three months exercise on physical fitness, body composition and some blood parameters in sedentary middle aged female. J. Educ. Training Studies 7(11), 63–71 (2019).
63.
Bohannon RW. Dynamometer measurements of grip and knee extension strength: are they indicative of overall limb and trunk muscle strength? Percept. Mot. Skills 108(2), 339–342 (2009).
64.
Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance, and posture. J. Strength Cond. Res. 24(3), 661–667 (2010).
65.
Angın E, Erden Z, Can F. The effects of clinical Pilates exercises on bone mineral density, physical performance and quality of life of women with postmenopausal osteoporosis. J. Back Musculoskel. Rehabil. 28(4), 849–858 (2015).
66.
Farinatti P, Rubini E, Silva E, Vanfraechem J. Flexibility of the elderly after one-year practice of yoga and calisthenics. Int. J. Yoga Ther. 24(1), 71–77 (2014).
67.
Bhadauria EA, Gurudut P. Comparative effectiveness of lumbar stabilization, dynamic strengthening, and Pilates on chronic low back pain: randomized clinical trial. J. Exer. Rehabil. 13(4), 477 (2017).
68.
Lee H, Caguicla JMC, Park S et al. Effects of 8-week Pilates exercise program on menopausal symptoms and lumbar strength and flexibility in postmenopausal women. J. Exer. Rehabil. 12(3), 247 (2016).
69.
Baena-Beato PÁ, Artero EG, Arroyo-Morales M, Robles-Fuentes A, Gatto-Cardia MC, Delgado-Fernández M. Aquatic therapy improves pain, disability, quality of life, body composition and fitness in sedentary adults with chronic low back pain. A controlled clinical trial. Clin. Rehabil. 28(4), 350–360 (2014).
70.
Lee C-W, Hyun J, Kim SG. Influence of Pilates mat and apparatus exercises on pain and balance of businesswomen with chronic low back pain. J. Phys. Ther. Sci. 26(4), 475–477 (2014).
Information & Authors
Information
Published In
Pages: 409 - 422
PubMed: 33709771
Copyright
© 2021 Future Medicine Ltd.
History
Received: 13 June 2020
Accepted: 16 December 2020
Published online: 12 March 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Effects of clinical Pilates on the fitness in people with children with disabilities: a randomized controlled trial. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0108
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mustafa Han, Şevval Akaydın, Atike Yılmaz, Serdar Koç, Comparison of The Physical Fitness Parameters of Special Education Vocational School Students and Inclusion High School Students, International Journal of Disabilities Sports and Health Sciences, 10.33438/ijdshs.1436311, 7, 3, (597-607), (2024).