Medical oncology referral and systemic therapy of patients with advanced stage urothelial carcinoma
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To understand physician visit patterns among patients with stage IV (including nonmetastatic [M0] and metastatic [M1] disease) urothelial carcinoma (UC) and understand factors associated with a timely referral to a medical oncologist and systemic treatment. Patients & methods: Retrospective analysis of Surveillance, Epidemiology and End Results-Medicare data. Results: First physician encounter was with a urologist (M0: 69%; M1: 53%) or primary care physician ([PCP]; M0: 19%, M1: 25%) for the majority of patients around UC diagnosis. After the index urologist encounter, most patients had a subsequent medical oncologist visit at a median of 52 days (M0: 69.5 days, M1: 33 days). In an adjusted model, older age, index PCP visit, higher comorbidities and M0 disease were negatively associated with a medical oncologist referral. Among those referred to a medical oncologist, older age, Hispanic or non-Hispanic Black race and not being married were negatively associated with subsequent chemotherapy receipt (p < 0.05). Conclusion: Many patients with advanced UC encounter multiple specialists during their disease course. Older patients or those with a first UC-related encounter with a PCP are less likely to be referred to medical oncology. Once referred to medical oncology, social determinants, including race and marital status, are relevant predictors of receiving chemotherapy.
Approximately 75% of patients with urothelial carcinoma (UC) in the USA are diagnosed after the age of 65 years [1,2]. Patients diagnosed with stage IV UC, which includes patients who have locally advanced/unresectable UC that has grown through the bladder wall into the pelvic or abdominal wall without distant metastasis (M0) or those with distant metastasis (M1) [3], may initially be asymptomatic or present to a primary care physician (PCP) or a urologist with loco-regional (e.g., hematuria, dysuria and pelvic pain) and/or systemic/constitutional symptoms. Typically, if deemed clinically warranted, the urologist would then conduct a cystoscopy, obtain a biopsy, obtain appropriate imaging tests and perform a transurethral resection of bladder tumor (either at the initial visit or on a follow-up visit for diagnostic, and potentially therapeutic purposes). The patient may subsequently be referred by the urologist to a medical oncologist to help complete further staging work up and formulate a treatment plan. Although the urologist is generally the gatekeeper in terms of obtaining relevant tumor tissue to help establish pathologic diagnosis, physician-to-physician referral patterns of patients suspected of having UC can vary, which may impact subsequent management.
According to the current National Comprehensive Cancer Network and American Urological Association guidelines, first-line therapy for stage IV M0 patients can include immune checkpoint inhibitors (ICIs), chemoradiation or chemotherapy that may or may not also incorporate cystectomy; upon recurrence, additional systemic therapy, and in select patients, cystectomy or radiation therapy are recommended [4,5]. In patients with M1 disease, guidelines recommend platinum-based chemotherapy and ICIs for first-line therapy and ICIs or chemotherapy as second-line therapies (depending on first-line treatment) [4,5]. Recent studies, however, report that approximately two-thirds of all stage IV bladder cancer patients [6,7] and 55% of those with metastatic UC [8] are not treated with systemic chemotherapy, despite the survival advantage conferred by chemotherapy [6]. Several factors may contribute to whether or not patients go on to receive systemic chemotherapy, including advanced age, poor performance status [9] or potential issues related to timely access/referral to relevant specialists [10].
Having access to a PCP and urologist may play an important role in establishing diagnosis of UC and appropriate referral for treatment. Similarly, since the medical oncologist is the main prescriber of systemic chemotherapy, not having access to a medical oncologist may be a barrier to receiving chemotherapy. One form of this access barrier is the decision point of the urologist or PCP to make the referral to a medical oncologist in the first place; the relative timing of such a referral then would be relevant to receipt of timely systemic therapy. After evaluation, the medical oncologist, together with the patient, would then decide as to whether the patient is an appropriate candidate for chemotherapy. To investigate the impact of these dynamics of patient referrals and evaluations on subsequent systemic treatment of advanced UC, this study was conducted with two objectives in mind: first, to understand the real-world physician visit patterns of patients in the immediate period leading up to de novo stage IV UC diagnosis, and their subsequent follow-ups after diagnosis; and second for patients seeing a urologist or/and a PCP around the time UC was suspected, to understand the factors associated with a timely referral to a medical oncologist and identify potential factors associated with institution of systemic chemotherapy. Newer therapies (e.g., immunotherapy, antibody drug–conjugates and targeted agents) are being increasingly incorporated into the management of advanced UC. As a result, using chemotherapy as a model treatment to better understand the dynamics of systemic treatment receipt within the patient–physician journal will become increasingly relevant.
Materials & methods
Database
This was a retrospective analysis using data from the linked Surveillance, Epidemiology and End Results (SEER)-Medicare database and the American Medical Association (AMA) Physician Masterfile. The SEER registry consists of 18 state or regional cancer registries, covering 28% of the US population [11,12], while the Medicare database contains covered healthcare service claims and associated costs for all Medicare beneficiaries from time of eligibility until death [13,14]. The AMA Physician Masterfile contains demographic, education, training, specialty and practice information of physicians in the US and US territories [15].
Study population
Medicare patients aged 66 years or older who were newly diagnosed with histologically confirmed stage IV UC from 2004 to 2013 (International Classification of Diseases for Oncology, Third Edition [ICD-O-3] codes 8120/3 - 8124/3) and had associated Medicare claims data from 2003 to 2014 were eligible for inclusion. Stage IV UC was defined as: tumor through the bladder wall into the pelvic or abdominal wall but not spread to regional lymph nodes or metastasized to distant sites (T4b/N0/M0); tumor through the bladder wall into nearby organs and regional lymph nodes but not metastasized (any T/N1–3/M0); or disease metastasized to distant lymph nodes or ome or more distant organs (e.g., bones, liver or lungs) regardless of whether or not the tumor had grown through the bladder wall into nearby organs or spread to regional lymph nodes (any T/any N/M1) [16]. M0 was defined as a disease that had not spread to distant lymph nodes or distant organs, and M1 was defined as a disease that had spread to distant lymph nodes or one or more distant organs [3].
Exclusion criteria
Patients were excluded if they had a postmortem first diagnosis of UC, an unknown diagnosis month/year, had any other cancer (except nonmelanoma skin cancer) in the 5 years prior to UC diagnosis or lacked continuous enrollment in Medicare Part A and B, or were enrolled in a health maintenance organization in the 12 months prior to diagnosis. Additionally, patients with previous UC diagnosis at earlier stages were excluded to define a truly incident cohort of stage IV patients with UC. Patients were followed until death or end of the study period (31 December 2014).
Definition of study index date
Patient–physician interactions affecting UC diagnosis and management typically occur a few weeks to months before receiving a confirmed diagnosis and subsequent staging of UC. Therefore, the study examined physician visit patterns from the 3 months prior to the month of stage IV diagnosis and through the ensuing follow-up. During this period, patients’ UC-related physician encounters were flagged by the presence of an International Classification of Diseases, Ninth Edition, Clinical Modifications (ICD-9-CM) code 188.9 for malignant neoplasm of bladder on an outpatient setting/carrier claim as well as an available National Provider Identifier/Unique Physician Identification Number record.
The first UC-related physician encounter during the study period described above was defined as the study index date for patients (Figure 1). For 90% of patients, the index date of the first UC-related encounter was the same month in which stage IV UC diagnosis was established, or was the immediate month preceding the month of UC diagnosis. By including physician encounters up to 3 months prior to the diagnosis of UC, we captured the real-world nature of patient–physician encounters that may be related to a suspicion of UC, as well as any subsequent physician referrals and patient flow associated with the management of advanced UC. This approach also addressed some of the limitations inherent within the SEER-Medicare database in that: the dataset does not enable the direct identification of the diagnosing physician; since timing of cancer diagnosis from the SEER registry is available on a month/year basis, this does not completely align with the more refined day/month/year time format of the claims information in the Medicare portion of the linked database (from which we derive the timing of specialist encounters). Subsequent visits were captured only at the times when patients were channeled to a new physician specialist post the index physician visit.

Figure 1. Definition of study index date for a hypothetical patient diagnosed in June.
Color of X refers to the specialist (red = PCP, black = urologist, green = medical oncologist, yellow = radiation oncologist).
PCP: Primary care physician; SEER: Surveillance, Epidemiology and End Results; UC: Urothelial carcinoma.
Baseline patient characteristics
Patient demographic characteristics, including age at diagnosis, sex, race/ethnicity, census location and marital status were obtained from the SEER registries. Patient comorbidities that occurred in the 12 months prior to UC diagnosis were extracted from the Medicare claims to calculate the Deyo adaptation of the Charlson Comorbidity Index (CCI) [17]. Performance status was calculated for all patients using a proxy, defined as having a Medicare claim for any of the following in the 12 months prior to UC diagnosis, were the following: wheelchair use, oxygen use, walking aid, hospital bed, hospice, skilled nursing facility or hospitalization.
Index physician characteristics
Physician characteristics were reported only for the index physician (i.e., the first UC-related physician encounter during the study period) to understand those characteristics that could be associated with initial suspicion of UC by M stage. Physician characteristics included age, gender, office location, degree received, training in a US medical school, years since medical school graduation and physician practice setting. Physician practice settings were classified into solo practice; federal government hospital (e.g., Veterans Administration hospital, hospital affiliated with the Armed Forces and US Public Service); local government hospital (i.e., city, county or state-run facilities); and nongovernment practices (e.g., health maintenance organizations, group practices, two-physician practices, medical schools, locum tenens, nongovernment hospitals or other facilities).
Study outcomes
UC-related physician encounters belonging to the following four specialties were retained: urologist, radiation oncologist, medical oncologist and PCP. Study outcomes included describing the physician visit patterns by specialist type post the index date in other words, time from first specialist visit to a medical oncologist visit. If a PCP refers to a urologist and then the urologist refers to a medical oncologist, the time is measured from the initial PCP visit. In addition, determinants of the time to a medical oncologist visit and chemotherapy receipt after an initial visit to a urologist or PCP was examined. Overall survival by first specialty visit was descriptively examined as an exploratory outcome.
Statistical analysis
Descriptive statistics were used to summarize patient and physician characteristics, physician referral patterns and referral patterns from the index visit to subsequent UC-related physician encounters for M0 and M1 patients. Visual Sankey diagrams outlining physician referrals and associated patient flow were constructed from the index physician encounter through subsequent follow-up. No statistical tests were conducted to compare M0 and M1 patients with respect to patterns and timing of referrals, as M1 patients were expected to have poorer survival and therefore shorter follow-up to make fair comparisons to M0 patients.
Cox proportional hazards model with a backward selection procedure (that included covariates with p < 0.10 in the final model) were used to estimate determinants of time to medical oncologist visit after index urologist or PCP visit and time to receiving systemic chemotherapy after index urologist or PCP visit. The covariates that were adjusted in the models included patient clinical characteristics (age, M-stage at diagnosis, Charlson Comorbidity Index (CCI) and performance status at diagnosis), patient demographics (sex, race/ethnicity, marital status, census location, location in an urban vs rural area), receipt of cystectomy and physician characteristics (physician specialty, age, office location and degree received [i.e., MD or DO], US medical school training, years since medical school graduation and practice setting). All analyses were conducted using SAS version 9.4.
Results
Patient characteristics
A total of 2044 stage IV UC patients met inclusion and exclusion criteria (Supplementary Figure 1). The proportion of patients with M0 (49%; n = 1007) or M1 (51%; n = 1037) disease at diagnosis was similar. The mean age at UC diagnosis was 77 years; 64% of patients were male and 85% were non-Hispanic whites. (Table 1). At diagnosis, 71% of patients had a CCI score of 0 or 1 and 25% had a proxy for poor performance status. Patients had a median follow-up of 9 months (interquartile range [IQR]: 4–19 months), which was expectedly shorter for M1 compared with M0 patients (6 [3–13] months vs 14 [7–28] months; p < 0.001), likely related to worse survival for M1 patients.
| Characteristic | All (n = 2044) | M0 (n = 1007) | M1 (n = 1037) | p-value |
|---|---|---|---|---|
| Patient characteristics | ||||
| Age at diagnosis, mean (SD), years | 76.86 (6.88) | 76.21 (6.56) | 77.48 (7.13) | <0.001 |
| Age at diagnosis, n (%) | ||||
| – 66–70 years | 444 (21.7) | 238 (23.6) | 206 (19.9) | 0.013 |
| – 71–75 years | 488 (23.9) | 254 (25.2) | 234 (22.6) | |
| – 76–80 years | 473 (23.1) | 231 (22.9) | 242 (23.3) | |
| – 80+ years | 639 (31.3) | 284 (28.2) | 355 (34.2) | |
| Male, n (%) | 1317 (64.4) | 661 (65.6) | 656 (63.3) | 0.261 |
| Race/ethnicity, n (%) | ||||
| – Non-Hispanic White | 1732 (84.7) | 858 (85.2) | 874 (84.3) | 0.812 |
| – Non-Hispanic Black | 143 (7.0) | 68 (6.8) | 75 (7.2) | |
| – Hispanic | 95 (4.6) | 43 (4.3) | 52 (5.0) | |
| – Other | 74 (3.6) | 38 (3.8) | 36 (3.5) | |
| Marital status at diagnosis, n (%) | ||||
| – Single (never married) | 173 (8.5) | 79 (7.8) | 94 (9.1) | <0.001 |
| – Married | 1114 (54.5) | 597 (59.3) | 517 (49.9) | |
| – Separated/divorced/widowed | 692 (33.9) | 302 (30.0) | 390 (37.6) | |
| – Unknown | 65 (3.2) | 29 (2.9) | 36 (3.5) | |
| Census location, n (%) | ||||
| – West | 868 (42.5) | 428 (42.5) | 440 (42.4) | 0.759 |
| – South | 449 (22.0) | 219 (21.7) | 230 (22.2) | |
| – Northeast | 473 (23.1) | 241 (23.9) | 232 (22.4) | |
| – Midwest | 254 (12.4) | 119 (11.8) | 135 (13.0) | |
| Urban location, n (%) | ||||
| – Rural | 210 (10.3) | 91 (9.0) | 119 (11.5) | 0.069 |
| – Urban | 1834 (89.7) | 916 (91.0) | 918 (88.5) | |
| Charlson Comorbidity Index, n (%) | ||||
| – 0 | 957 (46.8) | 499 (49.6) | 458 (44.2) | <0.001 |
| – 1 | 494 (24.2) | 256 (25.4) | 238 (23.0) | |
| – 2 | 276 (13.5) | 128 (12.7) | 148 (14.3) | |
| – 3+ | 317 (15.5) | 124 (12.3) | 193 (18.6) | |
| Poor performance status, n (%) | ||||
| – Yes | 509 (24.9) | 239 (23.7) | 270 (26.0) | 0.229 |
| Index physician characteristics | ||||
| Age, mean (SD), years | 50.51 (10.41) | 50.57 (10.42) | 50.45 (10.42) | 0.875 |
| Male, n (%) | 1829 (89.5) | 922 (91.6) | 907 (87.5) | 0.003 |
| Office location, n (%) | ||||
| – Northeast | 460 (22.5) | 238 (23.6) | 222 (21.4) | 0.472 |
| – North Central | 267 (13.1) | 123 (12.2) | 144 (13.9) | |
| – South | 470 (23.0) | 226 (22.4) | 244 (23.5) | |
| – West | 847 (41.4) | 420 (41.7) | 427 (41.2) | |
| Degree received, n (%) | ||||
| – DO | 87 (4.3) | 34 (3.4) | 53 (5.1) | 0.052 |
| – MD | 1957 (95.7) | 973 (96.6) | 984 (94.9) | |
| Trained in US medical school, n (%) | 1659 (81.2) | 854 (84.8) | 805 (77.6) | <0.001 |
| Years since medical school graduation, mean (SD) | 23.56 (10.81) | 23.76 (10.85) | 23.36 (10.77) | 0.495 |
| Practice setting, n (%) | ||||
| – Government hospital - federal | 23 (1.1%) | 12 (1.2%) | 11 (1.1%) | 0.542 |
| – Government hospital - city/county/state | 79 (3.9%) | 42 (4.1%) | 37 (3.7%) | |
| – Nongovernment practice | 817 (40.0%) | 407 (39.3%) | 410 (40.6%) | |
| – Not recorded | 922 (45.1%) | 462 (45.8%) | 460 (44.4%) | |
| – Solo practice | 203 (9.9%) | 112 (10.8%) | 91 (9.0%) | |
DO: Doctor of Osteopathic Medicine; M0: Nonmetastatic; M1: Metastatic.
Physician characteristics
The mean age of the index physicians included in the analysis was 50 years; the majority were male (90%) and had a MD degree (96%). Approximately 81% of the index physicians received US medical school training and most practiced in a nongovernment practice (68%). Physicians who suspected UC in M0 patients were more likely to be male and trained in the US compared with M1 patients. No further significant differences in physician characteristics were observed by M stage (Table 1).
Physician referral patterns
Index specialist visit
The most common index UC-related visit was with a urologist (61%), while those with a PCP (22%), medical oncologist (15%) or radiation oncologist (2%) were less common. More patients who saw index PCP were older than 80 years of age (p = 0.003). More patients with CCI score of 3 and greater had an index medical oncologist visit (p = 0.009; Supplementary Table 1). When stratified by M stage, more M0 patients (69%) had index urologist visit compared with M1 patients (53%). However, less M0 patients (19%) had index PCP visit compared with M1 patients (25%). Also, less M0 patients (10%) had index medical oncologist visit compared with M1 patients (20%) (visit 1 in Figure 2).
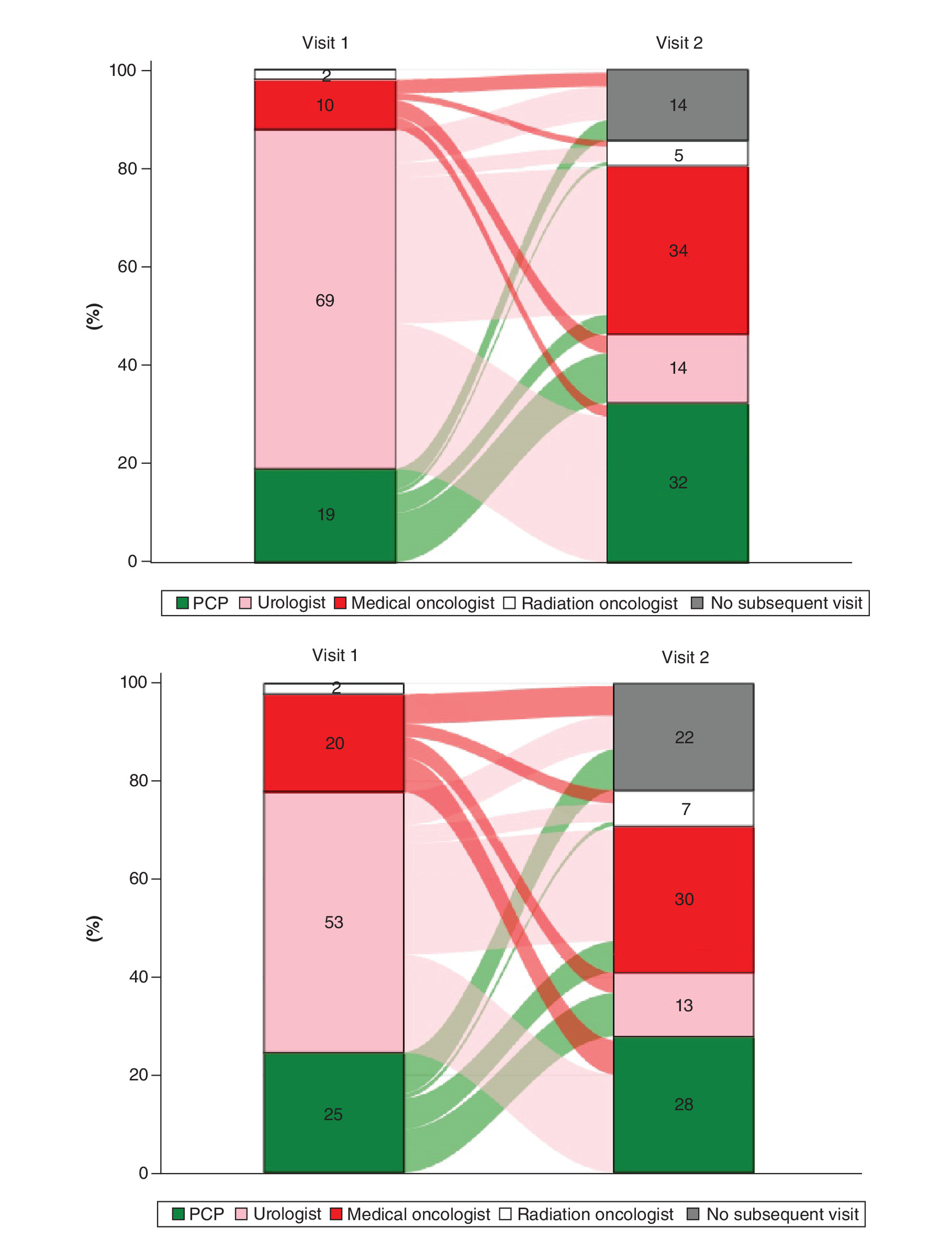
Figure 2. Sankey diagram. Physician referral patterns among nonmetastatic (M0; top panel) and metastatic (M1; bottom panel) patients after index visit.
The relative width of the flow between the bars reflect relative distribution of outflow/inflow by specialist type. The outflow from the 2% radiation oncologists have been masked as they represent patient counts of <11 to be compliant with the NCI data use agreement.
NCI: National Cancer Institute; PCP: Primary care physician.
Referral to a second specialist
The proportions and median (interquartile range) times between referrals are described in Table 2 & Figure 2. The Sankey diagram visually demonstrates that referrals between specialist types are common for both M0 and M1 patients, as designated by the inflow/outflow bands in Figure 2 from one physician specialty to another. Focusing on the referral patterns from the first (index) visit to the immediate next specialist type (visit 2), patients who had their index specialty visit with a PCP had their most common next visit with a urologist (M0: 52.9%; M1: 36.1%; Table 2). For those patients who saw a urologist as the index physician, the next specialist type was a medical oncologist (M0: 43.1%; M1: 42.7%). Index medical oncologists seemed to channel patients to the radiation oncologist (M0: 12.7%; M1: 13.5%) almost three-times as often than index PCP or urologists. Of note, index urologists also had the lowest proportion of not referring patients to any of the other three specialists (M0: 9.8%; M1: 12.8%).
| Specialist visit | M0 patients (n = 1007) | M1 patients (n = 1037) | ||
|---|---|---|---|---|
| n (%) of patients | Days to next specialist type, median (Q1–Q3) | n (%) of patients | Days to next specialist type, median (Q1–Q3) | |
| PCP as index specialist (visit 1) | 191 (19.0) | 255 (24.6) | ||
| Next specialist type (visit 2) | ||||
| – None | 42 (22.0) | NA | 87 (34.1) | NA |
| – PCP | NA | NA | NA | NA |
| – Urologist | 101 (52.9) | 9.0 (3.0–26.0) | 92 (36.1) | 6.0 (1.0–20.0) |
| – Medical oncologist | NR | 20.0 (7.0–107.0) | NR | 14.0 (4.0–34.0) |
| – Radiation oncologist | NR | 7.0 (4.0–46.0) | NR | 6.5 (3.0–132.0) |
| Urologist as index specialist (visit 1) | 694 (68.9) | 553 (53.3) | ||
| Next specialist type (visit 2) | ||||
| – None | 68 (9.8) | NA | 71 (12.8) | NA |
| – PCP | 297 (42.8) | 42.0 (15.0–73.0) | 208 (37.6) | 27.0 (8.0–59.5) |
| – Urologist | NA | NA | NA | NA |
| – Medical oncologist | 299 (43.1) | 51.0 (17.0–97.0) | 236 (42.7) | 22.5 (7.5–49.5) |
| – Radiation oncologist | 30 (4.3) | 40.5 (14.0–83.0) | 38 (6.9) | 12.0 (6.0–56.0) |
| Medical oncologist as index specialist (visit 1) | 102 (10.1) | 207 (20.0) | ||
| Next specialist type (visit 2) | ||||
| – None | 29 (28.4) | NA | 63 (30.4) | NA |
| – PCP | 24 (23.5) | 30.0 (7.5–155.5) | 73 (35.3) | 24.0 (8.0–80.0) |
| – Urologist | 36 (35.3) | 23.0 (5.5–89.0) | 43 (20.8) | 17.0 (6.0–68.0) |
| – Medical oncologist | NA | NA | NA | NA |
| – Radiation oncologist | 13 (12.7) | 5.0 (3.0–30.0) | 28 (13.5) | 7.5 (1.0–28.0) |
NR: Not reported to be compliant with the data use agreement with the NCI. Minority (2%, n = 20) of patients saw a radiation oncologist at index visit; however, these data are not presented because numbers on the subsequent visits are <11 and thus not compliant with the Data Use Agreement with the NCI.
M0: Nonmetastatic; M1: Metastatic; NA: Not applicable; NR: Not reported; PCP: Primary care physician.
With respect to the median time from the index physician specialist to the next specialist type, the time interval was longest for index urologists (varying between 40 and 51 days to next specialist among M0 and 12–27 days among M1 patients) and relatively short for index PCPs (varying between 7 and 20 days to the next specialist among M0 and 6–14 days among M1 patients; Table 2).
Subsequent medical oncologist visit
Seventy four percent of M0 patients and 66% of M1 patients had a subsequent medical oncologist visit at any time since index urologist visit. Approximately 50% of M0 and M1 patients had a subsequent medical oncologist visit at any time since index PCP visit. The median time to visiting a medical oncologist was longer for patients who saw an index urologist (52 days) compared with an index PCP (29 days); this trend was similar when stratified by M stage, with M0 patients, as expected, having longer time intervals than M1 patients (Table 3).
| Referral patterns to medical oncologist | All | M0 patients | M1 patients |
|---|---|---|---|
| Urologist as index specialist, n | 1247 | 694 | 553 |
| Any subsequent medical oncologist visit, n (%) | 877 (70.3) | 512 (73.8) | 365 (66.0) |
| Days from index to first medical oncologist visit | |||
| – Mean (SD) | 102.92 (190.57) | 114.19 (160.01) | 87.11 (225.89) |
| – Median (Q1–Q3) | 52 (20–106) | 69.5 (29–126) | 33 (14–74) |
| PCP as index specialist, n | 446 | 191 | 255 |
| Any subsequent medical oncologist visit, n (%) | 226 (50.7) | 96 (50.3) | 130 (51.0) |
| Days from index to first medical oncologist visit | |||
| – Mean (SD) | 73.5 (183.2) | 117.22 (264.1) | 41.22 (68.6) |
| – Median (Q1–Q3) | 29 (9–77) | 52.0 (16–117.5) | 21.5 (6–42) |
M0: Nonmetastatic; M1: Metastatic; PCP: Primary care physician; SD: Standard Deviation.
Predictors of time from index urologist or PCP visit to first medical oncologist visit
Since patients with UC most often see a urologist or a PCP at initial presentation, predictors of time to seeing a medical oncologist were assessed among patients with an index urologist or PCP visit. In a multivariate Cox regression model, patients whose index specialty visit was with a PCP (hazard ratio [HR]: 0.82 [0.74, 0.97]), were aged 80 years or older (HR: 0.71 [0.60, 0.84]), had CCI score of 3 or greater (HR: 0.78 [0.64, 0.95]), were recipients of cystectomy (HR: 0.80 [0.69, 0.91]) or whose index visit was in a ‘solo practice’ setting (HR: 0.74 [0.60, 0.92]) had lower relative likelihood of seeing a medical oncologist at any time after their index visit compared with the respective reference groups. Overall, M1 patients had a higher relative likelihood of seeing a medical oncologist compared with M0 patients (HR: 1.17 [1.00, 1.36], p = 0.048; Figure 3).
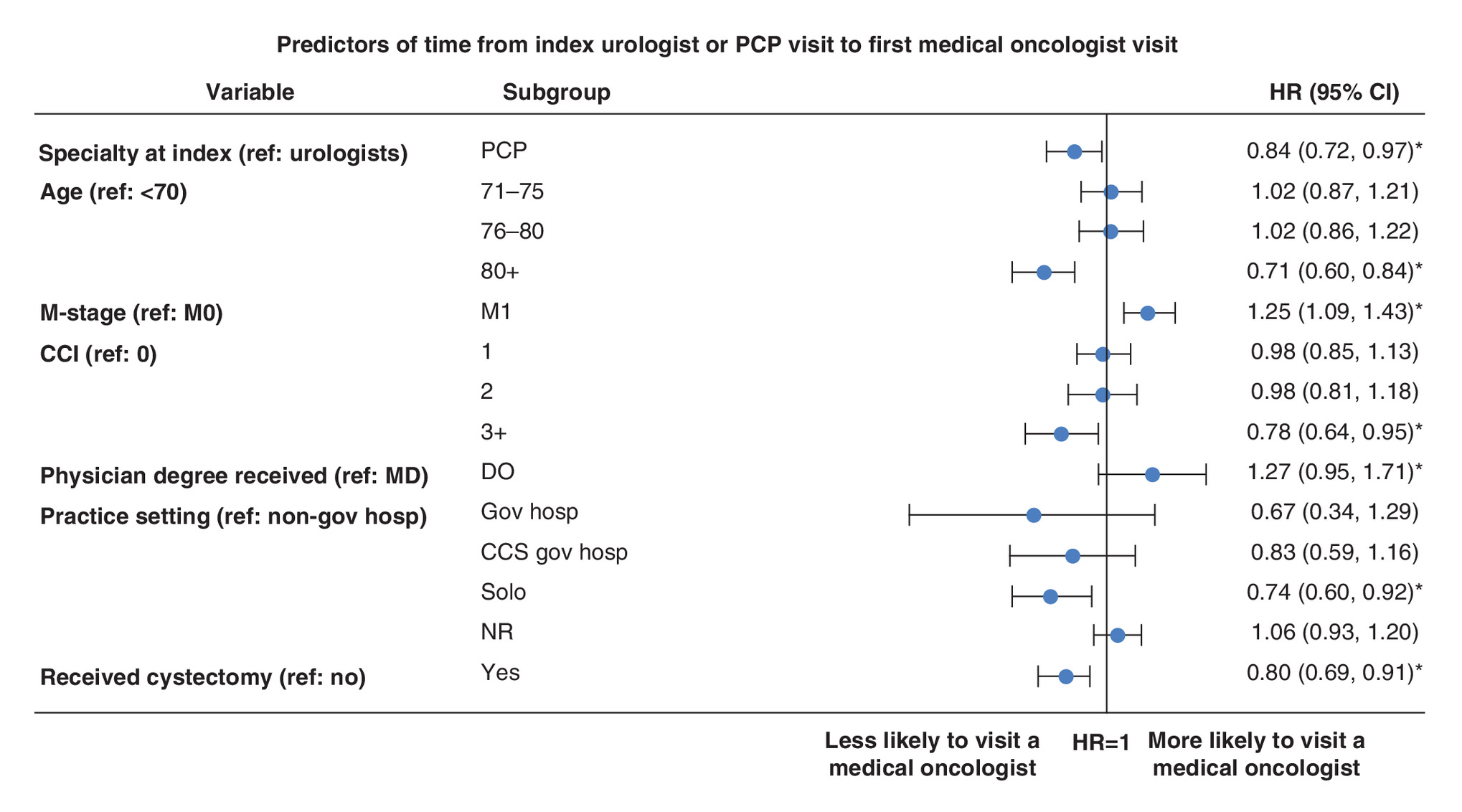
Figure 3. Multivariate Cox model of determinants of time to medical oncologist visit after index urologist visit.
*p < 0.05.
CCI: Charlson Comorbidity Index; CCS: City/county/state; Gov: Government; HR: Hazard ratio; Hosp: Hospital; M0: Nonmetastatic; M1: Metastatic; NR: Not reported; PCP: Primary care physician; Ref: Reference; US: United States.
Predictors of time from index urologist or PCP visit to chemotherapy receipt among patients with subsequent medical oncologist visit
With respect to the predictors of time to systemic chemotherapy receipt post-index urologist or PCP visit and who had subsequent medical oncologist visit, cystectomy recipients (0.63 [0.53, 0.75]), non-Hispanic Black (0.69 [0.49, 0.97]), Hispanic (0.57 [0.38, 0.86]), separated/divorced/widowed (0.79 [0.66, 0.94]) or older patients (gradient of 0.70 [0.58, 0.85], 0.59 [0.48, 0.73] and 0.38 [0.30, 0.47] within the different categories of increasing age) had a significantly lower relative likelihood of receiving a systemic line of chemotherapy (Figure 4). Patients whose physicians were in the Southern US had a 27% lower relative likelihood of receiving a systemic line of chemotherapy compared with patients whose providers were in the West (0.73 [0.59, 0.90]). M stage and whether the patient’s index visit was with a PCP or a urologist did not significantly affect whether the patient received a systemic line of chemotherapy. Stratifying the analysis by M stage confirmed that the initial specialist seen does not have an impact on whether patients receive systemic chemotherapy (had they also seen a subsequent medical oncologist), while some of the characteristics mentioned above were no longer statistically significant. This likely was due to the now smaller sample size in each group (Supplementary Figure 2).
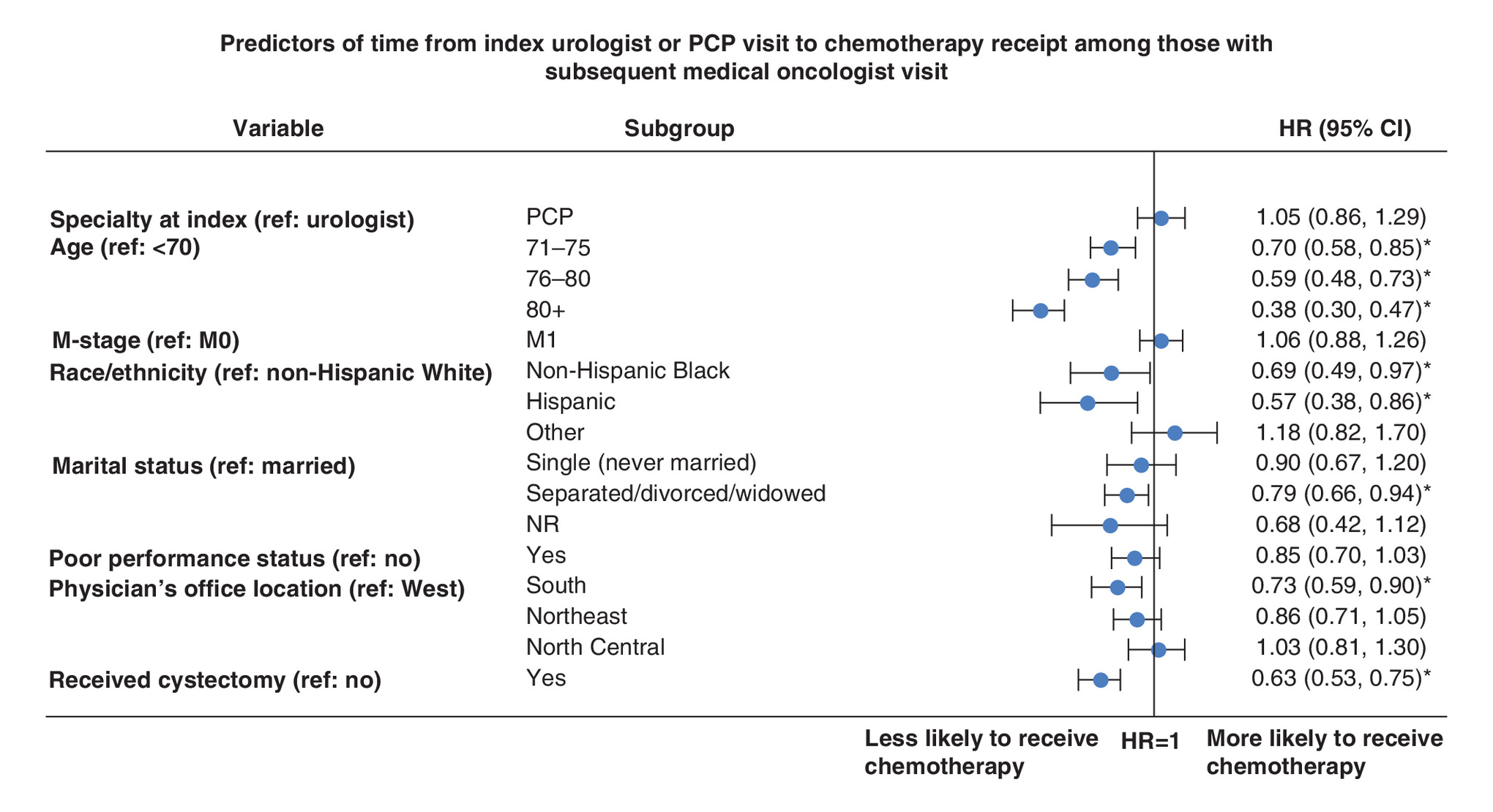
Figure 4. Multivariate Cox model of determinants for time to chemotherapy receipt after index urologist visit.
*p < 0.05.
HR: Hazard ratio; NR: Not reported; PCP: Primary care physician; Ref: Reference.
Discussion
Prior literature has documented the benefits of multidisciplinary management of UC patients, which is associated with improvement in informed and collaborative decision making and possibly earlier initiation of definitive treatments [17–19]. Using the linked SEER-Medicare dataset, we provide a detailed analysis that fills knowledge gaps related to patients with newly diagnosed advanced UC in terms of physician visits, patient referrals and treatment. In this study, we used chemotherapy as the ‘anchor’ to gauge receipt of systemic treatment for the aggregate stage IV UC patient population as well as the M0 and M1 subpopulations that together define stage IV disease. Our aim is to provide more granular information about these aspects of UC management than are generally reported, particularly since such an analysis may help provide a model to further study and understand UC management and outcomes as the treatment landscape continues to evolve with the advent of other systemic therapies beyond the traditional chemotherapy which remains an important backbone of treating advanced UC.
This study found that referral among physician specialties was common, consistent with reported literature [18–20]. An important aspect of the study was to not only look at the urologist but also the relatively understudied specialist, the PCP, within the context of their potential ‘gatekeeper’ role as they may relate to UC. Interestingly, patients who presented to a PCP initially were more likely to be older, have higher comorbidities and poor performance status compared with those presenting to a urologist, suggesting that PCPs may be interacting with the sicker UC population at the index visit (Supplementary Table 1). Although physician referrals varied by the index physician, the role of the PCP in the management of UC patients was prominent. Remarkably, 29% of patients with an index PCP visit were not referred to another specialist, and 50% never saw a medical oncologist over their disease course, which is surprising given that PCPs generally do not provide UC-directed care. Among the patients with index PCP visits who were referred out, the referrals tended to occur rapidly and were predominantly channeled to a urologist, with only a minority of such patients being directly referred to a medical oncologist.
Our descriptive and adjusted models show that urologists were more likely, compared with PCPs, to refer UC patients to a medical oncologist. Interestingly, the median time to visiting a medical oncologist is longer for patients who see an index urologist (52 days) compared with an index PCP (29 days). Seventy percent of the referrals to the medical oncologist stemmed from the urologist, highlighting the prominent role of the latter in channeling patients to systemic treatment. In exploratory descriptive analyses of overall survival by first specialty visits, patients who were initially managed by a urologist had the highest median survival while those initially seen by a PCP had the lowest survival; this trend was observed for both M0 and M1 patients (Supplementary Figure 3). Our results for stage IV UC also mirror findings of a study of muscle invasive bladder cancer, which found that more than 80% of medical oncologists had their patients referred from a urologist, with very few receiving referrals from PCPs or radiation oncologists [21], underscoring the gatekeeper role of the urologist in mediating patient flow and receipt of systemic therapy in both advanced UC and earlier stages of UC. Despite their key role in UC management, our analysis revealed that 30% of stage IV UC patients with index urologist visit did not get any subsequent medical oncologist referral during their entire disease course. However, this is still a lower proportion of patients not being referred out compared with those who had index PCP visit where 50% never had a medical oncology follow-up. Our model also shows that patients had lower relative likelihood of being referred to medical oncology if they were M0, aged 80 years or older, had more comorbidities or underwent cystectomy. It has been shown previously that patients who are older and have comorbidities are less likely to be suitable for chemotherapy [8,22], and hence not referred as quickly to medical oncology. Patients undergoing cystectomy may also be less likely to be referred to medical oncology as they could be receiving peri-operative and postoperative care through the urologist [23].
Looking at patient–physician flow patterns and chemotherapy receipt, certain demographic characteristics emerge that predict for the likelihood of receiving systemic therapy. Consistent with prior studies, older patients have a lower relative likelihood of seeing a medical oncologist or receiving chemotherapy post urologist visit, perhaps in part due to potential comorbidities/relative performance status [6,8,24,25]. Further, being Hispanic, non-Hispanic black, widowed/separated/divorced/never married or being treated by a physician in the Southern US are predictors of lower relative likelihood of receiving chemotherapy. The role of race in the context of delay in chemotherapy receipt or less likelihood of receiving multimodal therapy, or not receiving chemotherapy altogether, as well as poorer survival outcomes, have been well documented by others [26–29]. Better social support, as reflected by marital status, has been shown to lead to greater relative likelihood of UC treatment and overall survival, particularly among males [27,28]. The role of geography also needs further clarification but may reflect physician availability and proximity to treatment centers, keeping in mind that the Southern US houses some of the most socioeconomically deprived counties in the country [26,30,31]. Outlining the referral patterns could be helpful in informing patients, payers and specialists as it provides an understanding around the patient journey, characteristics and the time it takes for a stage IV patient to be referred to medical oncology and to receive systemic chemotherapy. Our analysis suggests that we should educate on the importance of timely referral from PCP/Urologist to medical oncology for timely receipt of systemic chemotherapy.
Strengths of the study include the fact that the SEER-Medicare database is a large nationally representative database that provides relevant longitudinal information on patients. Since the median age at diagnosis for all (not only Medicare) patients with UC is about 73 years, the SEER-Medicare dataset captures most of the UC patients. Further, the availability of tumor, nodes and metastases (TNM) staging within SEER allows for analyzing advanced stage UC patient data, which would not be possible with claims data alone. Finally, linking outpatient and carrier files to the AMA Physician Masterfile allowed us to identify the specialties and demographics of the treating physicians. The integration of these three data sources provide robust insights into patient and provider demographics and treatment patterns.
Our study also has some inherent limitations. As referral patterns were captured over the duration of study follow-up from the time of the index visit, some patients with poor prognosis and shorter overall survival may not have enough time to enable referrals to different specialists. Similarly, patients diagnosed in the last year of the data cut may be administratively censored in other words, they may have seen specialists, but we were not able to capture such data since the most updated data available would be too close to their diagnosis. Further, UC patients may see specialists beyond those identified in this analysis (e.g., physician assistants, oncology nurses, nutrition specialists, pathologists and others). Clinical characteristics, including M stage, CCI score and performance status were measured only at diagnosis, and therefore disease improvement or progression during follow-up that could possibly affect patient treatment or referral patterns was not captured. Although the data used for this analysis was from 2003 through 2014, which precedes the recent integration of ICIs and other newer therapies in advanced UC, our study provides a relevant benchmark to further assess patient–physician dynamics in the context of emerging therapies, keeping in mind that up to very recently, chemotherapy has been the mainstay of systemic management of UC [32,33].
Conclusion
This is one of the few studies to look at physician specialty visits and referral patterns, as well as the determinants of time to medical oncologist visit and chemotherapy receipt among patients diagnosed with incident stage IV UC, including the M0 and M1 subpopulations that define stage IV disease. Future studies should continue to explore which configurations of multispecialists result in the most coordinated, timely and optimal care and improved survival for these patients, particularly as some of the newer therapies become increasingly available for the UC patient. Although younger age, good performance status, social support and race/ethnicity were important determinants of time to seeing a medical oncologist or receiving chemotherapy, it will be relevant in future work to monitor whether the newer therapies can help bridge some of the gaps observed in the management and outcomes of advanced UC patients.
•
Among stage IV urothelial carcinoma (UC) patients, most of initial encounters related to a suspicion of UC are with a urologist (M0: 69%; M1: 53%) followed by a primary care physician (PCP) (M0: 19%; M1: 25%).
•
The median time to visiting a medical oncologist is longer for patients who see an index urologist (52 days) compared with an index PCP (29 days).
•
The descriptive and adjusted models show that urologists are more likely, compared with PCPs, to refer UC patients to a medical oncologist.
•
Patients whose initial encounter related to a suspicion of UC specialty visit is with a PCP, are 80 years of age or older, have Charlson Comorbidity Index score of 3 or greater, have M0 disease, undergo cystectomy or whose index visit is with a ‘solo practitioner’ have lower relative likelihood of being referred to a medical oncologist.
•
Patients who are of Hispanic ethnicity or non-Hispanic Black race/ethnicity, are separated/divorced/widowed, are older, have Charlson Comorbidity Index score of 3 or greater, undergo cystectomy or are being treated by a physician in the Southern part of the United States have lower relative likelihood of receiving chemotherapy once they see a medical oncologist.
•
This study fills knowledge gaps related to physician specialty visits and referral patterns among patients with stage IV UC as well as the effect of referral patterns on chemotherapy receipt.
Author contributions
A Aly, MF Botteman, Y Doleh and R Shenolikar conceptualized the research question and study design. MF Botteman was responsible for data acquisition. A Hussain was the lead clinician reviewing methods and results.
A Aly and C Johnson were responsible for data analysis and C Johnson drafted a first version of the manuscript. All authors reviewed and approved the final version of the manuscript. The authors on this manuscript have no other relevant financial or other relationships to disclose.
Acknowledgments
The authors thanked C Mirvis and V Chirikov for medical writing support and Z Chen and V Chirikov for analytical support.
A Aly was an employee of Pharmerit International during the conduct of this study and is currently an employee of AstraZeneca (200 Orchard Ridge Drive, Gaithersburg, MD 20878).
Financial & competing interests disclosure
AstraZeneca provided funding for this research. A Aly was an employee of Pharmerit International during the conduct of this study; C Johnson and MF Botteman are current employees of Pharmerit International; MF Botteman is a shareholder of Pharmerit International. Y Doleh, A Aly and R Shenolikar are employees of and have stock options in AstraZeneca. Part of A Hussain’s time was supported by a Merit Review Award (I01 BX000545), Medical Research Service, Department of Veterans Affairs. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance was provided by C Mirvis and V Chirikov from Pharmerit.
Ethical conduct of research
This retrospective longitudinal analysis used de-identified data from SEER-Medicare database, and was granted Institutional Review Board exemption. All results were reported per the data use agreement with the National Cancer Institute.
Supplementary Material
File (suppl_file.docx)
- Download
- 165.18 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Erlich A, Zlotta AR. Treatment of bladder cancer in the elderly. Investig. Clin. Urol. 57(Suppl. 1), S26–S35 (2016).
• A comprehensive review of various treatment options for elderly patients with muscle invasive bladder cancer (BC) and nonmuscle invasive BC.
2.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J. Clin. 68(1), 7–30 (2018).
3.
AJCC Cancer Staging Manual. (8th Edition). Amin MB, Edge SB, Greene FLet al. et al. (Eds). Springer, NY, USA (2017).
4.
Flaig TW, Spiess PE, Agarwal N et al. NCCN Guidelines Insights: bladder cancer, version 5.2018. J. Natl Comp. Cancer Netw. 16(9), 1041–1053 (2018).
• Reviews the National Comprehensive Cancer Network guidelines used to treat bladder cancer.
5.
Chang SS, Bochner BH, Chou R et al. Treatment of non-metastatic muscle-invasive bladder cancer: AUA/ASCO/ASTRO/SUO Guideline. J. Urol. 198(3), 552–559 (2017).
6.
Flannery K, Cao X, He J, Zhong Y, Shah AY, Kamat AM. Survival rates and health care costs for patients with advanced bladder cancer treated and untreated with chemotherapy. Clin. Genitourin. Cancer 16(4), e909–e917 (2018).
• Describes the fact that about two-thirds of patients diagnosed with stage IV bladder cancer were not treated with systemic chemotherapy.
7.
Care V-B, Congress A. Costs of care for patients receiving chemotherapy for advanced bladder cancer. J. Clin. Pathways 3(10), 63–70 (2017).
8.
Aly A, Johnson C, Yang S, Botteman MF, Rao S, Hussain A. Overall survival, costs, and healthcare resource use by line of therapy in Medicare patients with newly diagnosed metastatic urothelial carcinoma. J. Med. Econ. 22(7), 662–670 (2019).
9.
Katz H, Wassie E, Alsharedi M. Checkpoint inhibitors: the new treatment paradigm for urothelial bladder cancer. Med. Oncol. 34(10), 170 (2017).
10.
Aiello Bowles EJ, Tuzzio L, Wiese CJ et al. Understanding high-quality cancer care: a summary of expert perspectives. Cancer 112(4), 934–942 (2008).
11.
Noone A-M, Lund JL, Mariotto A et al. Comparison of SEER treatment data with Medicare claims. Med. Care 54(9), e55–e64 (2016).
12.
The National Cancer Institute. Registry Groupings in SEER Data and Statistics (2020). https://seer.cancer.gov/registries/terms.html
13.
Potosky AL, Riley GF, Lubitz JD, Mentnech RM, Kessler LG. Potential for cancer related health services research using a linked Medicare-Tumor Registry Database. Med. Care 31(8), 732–748 (1993).
14.
The National Cancer Institute. SEER-Medicare: brief description of the SEER-Medicare Database (2020). https://healthcaredelivery.cancer.gov/seermedicare/overview/
15.
AMA Physician Masterfile (2019). www.ama-assn.org/practice-management/masterfile/ama-physician-masterfile
16.
Bladder Cancer Stages (2019). www.cancer.org/cancer/bladder-cancer/detection-diagnosis-staging/staging.html
17.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45(6), 613–619 (1992).
18.
Atwell D, Vignarajah DD, Chan BA et al. Referral rates to multidisciplinary team meetings: is there disparity between tumour streams? J. Med. Imaging Radiat. Oncol. 63(3), 378–382 (2019).
19.
Kurpad R, Kim W, Rathmell WK et al. A multidisciplinary approach to the management of urologic malignancies: does it influence diagnostic and treatment decisions? Urol. Oncol. 29(4), 378–382 (2011).
•• Although outdated, this is a real-world single institution study that documents the positive impact of a multidisciplinary team approach on the diagnostic and management decisions for patients with newly diagnosed urologic malignancy.
20.
Harshman LC, Tripathi A, Kaag M et al. Contemporary patterns of multidisciplinary care in patients with muscle-invasive bladder cancer. Clin. Genitourin. Cancer 16(3), 213–218 (2018).
21.
Apolo AB, Kim JW, Bochner BH et al. Examining the management of muscle-invasive bladder cancer by medical oncologists in the United States. Urol. Oncol. 32(5), 637–644 (2014).
22.
Galsky MD, Pal SK, Lin S-W et al. Real-world effectiveness of chemotherapy in elderly patients with metastatic bladder cancer in the United States. Bladder Cancer 4(2), 227–238 (2018).
23.
Kulkarni JN. Perioperative morbidity of radical cystectomy: a review. Indian J. Urol. 27(2), 226 (2011).
24.
Rose TL, Deal AM, Nielsen ME, Smith AB, Milowsky MI. Sex disparities in use of chemotherapy and survival in patients with advanced bladder cancer. Cancer 122(13), 2012–2020 (2016).
25.
Kamat AM, Cao X, He J, Zhong Y, Shah AY, Flannery K. Costs of care for patients receiving chemotherapy for advanced bladder cancer. J. Clin. Pathways 3(10), 63–70 (2017).
26.
Fletcher SA, Gild P, Cole AP et al. The effect of treatment at minority-serving hospitals on outcomes for bladder cancer. Urol. Oncol. 36(5), 238.e237–238.e217 (2018).
27.
Gild P, Wankowicz SA, Sood A et al. Racial disparity in quality of care and overall survival among black vs. white patients with muscle-invasive bladder cancer treated with radical cystectomy: a national cancer database analysis. Urol. Oncol. 36(10), 469.e461–469.e411 (2018).
28.
Prout GR Jr, Wesley MN, Mccarron PG et al. Survival experience of black patients and white patients with bladder carcinoma. Cancer 100(3), 621–630 (2004).
29.
Weiner AB, Keeter M-K, Manjunath A, Meeks JJ. Discrepancies in staging, treatment, and delays to treatment may explain disparities in bladder cancer outcomes: an update from the National Cancer Data Base (2004–2013). Urol. Oncol. 36(5), 237.e239–237.e217 (2018).
•• This is a study using real-world data that documents the heterogeneity and disparities in overall survival for certain groups which may benefit from earlier diagnosis and improved timely access to potentially life prolonging treatment.
30.
Klapheke A, Yap SA, Pan K, Cress RD. Sociodemographic disparities in chemotherapy treatment and impact on survival among patients with metastatic bladder cancer. Urol. Oncol. 36(6), 308.e319–308.e325 (2018).
31.
Konety BR, Joslyn SA. Factors influencing aggressive therapy for bladder cancer: an analysis of data from the SEER program. J. Urol. 170(5), 1765–1771 (2003).
32.
Dietrich B, Srinivas S. Urothelial carcinoma: the evolving landscape of immunotherapy for patients with advanced disease. Res. Rep. Urol. 10, 7–16 (2018).
• Reviews the evolving landsacape of urothelial carcinoma treatment with a focus on immunotherapy.
33.
The National Cancer Institute. FDA alters approved use of two checkpoint inhibitors for bladder cancer (2018). www.cancer.gov/news-events/cancer-currents-blog/2018/bladder-cancer-checkpoint-inhibitor-change
Information & Authors
Information
Published In
Pages: 945 - 957
PubMed: 32964721
Copyright
© 2020 Future Medicine Ltd.
History
Received: 26 May 2020
Accepted: 30 July 2020
Published online: 23 September 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Medical oncology referral and systemic therapy of patients with advanced stage urothelial carcinoma. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0093
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mairead Kearney, Liu Zhang, Elizabeth Hubscher, Mihaela Musat, Sharada Harricharan, Thomas Wilke, Undertreatment in patients with advanced urothelial cancer: systematic literature review and meta-analysis, Future Oncology, 10.2217/fon-2023-0298, 20, 16, (1123-1137), (2023).