Impact of osteosynthesis in fracture care: a cost comparison study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To estimate the health economic impact of osteosynthesis (OS) in fracture care over six decades in 17 high-income countries. Patients & methods: Applying a decision tree model, we assumed a hypothetical absence of OS and compared OS (intervention) with conservative treatment (CONS; comparator). We included patients with femur, tibia and radius fractures (age <65 years) and for proximal femur fractures also elderly patients (≥70 years). Results: We estimated savings in direct and indirect costs of 855 billion Swiss francs in the working age population in addition to 4.6 million years of life gained. In the elderly population, 69 billion Swiss francs were saved in direct costs of proximal femur fractures in addition to 73 million years of life gained. Conclusion: OS contributed to maximize health gains of society.
Background
The “Arbeitsgemeinschaft für Osteosynthesefragen” (AO) was established in 1958 in Switzerland to improve patient care in musculoskeletal disorders. At that time, the treatment of long bone fractures would mostly consist of cast and extension treatment and patients would stay in hospital for an extended period of time, as is often the case today in low income countries [1].
The AO established the concept of osteosynthesis (OS) on a broader scale. The objectives were to improve patient outcome and reduce the patients’ pain, but also to reduce time in hospital and time until return to work. Four main principles of OS were established to reach these aims: anatomical reduction, stable fixation, preservation of blood supply and early mobilization. The AO pioneers and their followers chose a holistic approach with standardized surgical methods and products, educational programs and surgeon training as well as applied research. As a result, they revolutionized fracture care worldwide.
Surprisingly, this medical innovation has never been formally evaluated for its health economic impact on patients and society. Several books exist but they are more anecdotal, dealing with historical developments and people as well as medical developments [1,2]. To better understand the different steps of this technology penetration, we developed a conceptual framework. We distinguished between input (i.e., a new concept of fracture care), output (e.g., number of surgeons trained and OS procedures performed), outcome (improved individual patient care) and health-economic impact at the society level (e.g., years of life gained; impact on costs). We were not interested in the number of surgical procedures according to AO principles in fracture care, as they represent an output rather than the final impact on patients and society.
To estimate the health economic impact of the technological innovation of OS in fracture care, we performed a health economic evaluation for three index bones over a period of 60 years in 17 high-income countries.
Methods
Advisory board
An advisory board was established in advance. This committee comprised experts who had intimate knowledge about the historical development of the AO, as well as about the spread of OS as a technology over time. In addition, management, medical, health-economic and epidemiologic expertise was covered by the committee.
Design
We aimed to estimate the impact of osteosynthesis in fracture care over six decades (time span from its invention in 1958 to 2017). For our estimation, we assumed a hypothetical absence of this technology. This strategy has been used by other research groups [3–6].
We applied a modeling approach using a three-stage decision tree as a pragmatic simplification of fracture care in our cost comparison study (Figure 1). In brief, we compared OS with conservative treatment (CONS; i.e., plaster or extension treatment for many weeks) for fractures of three index bones (femur; tibia; radius). We included acute care as well as rehabilitation. The three index bones were selected as they include frequent fracture locations of the upper and lower extremities and have specifically profited from OS innovations. To provide best possible robust estimates of the impact of OS, we have selected fractures where OS is the standard of care (femur fractures; tibia fractures). Historically, these fractures resulted in high invalidity rates with CONS and today OS is performed in nearly all patients with these fracture types. To broaden the scope of our study, we decided to also include radius fractures. This is a very common fracture type which is not life threatening and possible benefits of OA may only emerge as productivity gains. Conservative treatment can be a common and valuable treatment option in radius fractures and we wanted to include this in our model. As the decision about the optimal fracture treatment in, for example, shoulder and vertebral fractures is not always straightforward and may also be influenced by specific guidance within the healthcare system, we have not included such fractures in our model. Three anatomical locations (proximal, shaft and distal fractures) were modeled separately for each index bone, as they comprise distinct clinical entities. We assigned probabilities of complication-free healing, bone-related complications (e.g., device infection for OS needing a second operation or nonunion for CONS resulting in prolonged rehabilitation and higher invalidity rates) and venous thromboembolism as another typical complication (higher rates with CONS compared with OS). We assessed direct medical costs, productivity losses and years of life gained (YLG) for both treatment options. For Switzerland, we used a bottom-up approach, as we had detailed data for many input variables (probability inputs in the model: Table 1; costs used in the model: Supplementary Material 1A). To estimate the impact in 16 other high-income countries, we used a top-down approach and applied the findings from Switzerland to these countries, taking a variety of country specific features into account (see below). Finally, outcomes from 17 countries over a period of 60 years were summed up and compared.

Figure 1. Decision tree.
We used a pragmatic simplification of fracture care. 1st stage: Decision of therapeutic approach: OP treatment or CONS for fractures of each index bone (femur, tibia and radius) and all fracture locations (promixal, shaft and distal) separately; 2nd stage: assignment of probabilities of complication-free fracture healing and bone related complications; 3rd stage: assignment of probabilities of another typical complication (venous thromboembolism).
CONS: Conservative treatment; OP: Osteosynthesis; VTE: Venous thromboembolism.
| Stage of model | Age group | Stage 1 | Stage 2 | Stage 3 | Stage 3 | Overall | Overall | Stage 2 | Stage 2 | Stage 3 | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial therapy | Compli-cations† | VTE‡ (without complication in stage 2) | VTE‡ (after complication in stage 2) | Mortality§ (model year 1958) | Mortality§ (model year 2017) | Total absence from work¶ (without complication † in stage 2) | Total absence from work¶ (after complication † in stage 2) | Additional absence from work# (after VTE3) | |||
| Type of model parameter | Years | p-event | p-event | p-event | p-event | p-event | Months | Months | Months | ||
| Femur fracture prox. | <65 | OS | 0.06 | 0.05 | 0.08 | 0.05 | 0.003 | 4 | 9 | 2 | [7–11] |
| CONS | 0.05 | 0.10 | 0.20 | 0.10 | 0.03 | 8 | 155 | 2 | |||
| >70 | OS | 0.06 | 0.05 | 0.08 | 0.40 | 0.27 | |||||
| CONS | 0.05 | 0.10 | 0.20 | 0.60 | 0.60 | ||||||
| Femur fracture shaft | <65 | OS | 0.05 | 0.05 | 0.08 | 0.08 | 0.003 | 8 | 17 | 2 | [7] |
| CONS | 0.05 | 0.10 | 0.20 | 0.15 | 0.03 | 8 | 373 | 2 | |||
| Femur fracture distal | <65 | OS | 0.05 | 0.05 | 0.08 | 0.06 | 0.003 | 3 | 7 | 2 | [7,12] |
| CONS | 0.05 | 0.10 | 0.20 | 0.12 | 0.03 | 7 | 376 | 2 | |||
| Tibia fracture proximal | <65 | OS | 0.05 | 0.05 | 0.08 | 0.02 | 0.001 | 3 | 6 | 2 | [7,13,14] |
| CONS | 0.05 | 0.10 | 0.20 | 0.03 | 0.01 | 6 | 274 | 2 | |||
| Tibia fracture shaft | <65 | OS | 0.05 | 0.05 | 0.08 | 0.02 | 0.001 | 5 | 9 | 2 | [7,14,15] |
| CONS | 0.05 | 0.10 | 0.20 | 0.04 | 0.01 | 6 | 299 | 2 | |||
| Tibia fracture distal | <65 | OS | 0.05 | 0.05 | 0.08 | 0.02 | 0.001 | 6 | 12 | 2 | [7,14,16] |
| CONS | 0.05 | 0.10 | 0.20 | 0.04 | 0.01 | 9 | 279 | 2 | |||
| Radius fracture proximal | <65 | OS | 0.13 | 0 | 0 | 0 | 0 | 2 | 3 | 0 | [7,17] |
| CONS | 0.05 | 0 | 0 | 0 | 0 | 2 | 60 | 0 | |||
| Radius fracture shaft | <65 | OS | 0.05 | 0 | 0 | 0 | 0 | 2 | 4 | 0 | [7] |
| CONS | 0.05 | 0 | 0 | 0 | 0 | 5 | 61 | 0 | |||
| Radius fracture distal | <65 | OS | 0.05 | 0 | 0 | 0 | 0 | 2 | 4 | 0 | [7] |
| CONS | 0.05 | 0 | 0 | 0 | 0 | 2 | 52 | 0 |
Bold figures are subject to sensitivity analyses. For cost figures: Supplementary Material 1A.
†
Complications: complications of OS in stage 2 include: device infection, device dislocation, nonunion; complications of CONS in stage 2 include: nonunion; mal-union. We applied the following assumption in case of lacking data: probabilities of complications for OP and CONS were assumed to be identical and unchanged over all time periods to ensure a conservative estimate of the benefit of OP compared with CONS.
‡
VTE: in case of lacking data, we used the following assumptions (based on clinical expert knowledge) for the two modeled scenarios over all time periods: probability of VTE without prior complications in stage 2 (OP: 5%; CONS 10%) and probability of VTE after prior complications in stage 2 (OP: 8%; CONS 20%). Complications of OS in stage 2 include: device infection, device dislocation, nonunion; complications of CONS in stage 2 include: nonunion; mal-union (for example: patient with femur shaft fracture [mean age 34 years] with OS treatment and second OS due to device infection: probability of VTE is assumed to be 8% compared with 5% in case of complication free fracture healing without second surgery).
§
Mortality: in the working-age population, probabilities of mortality from 1958 to 2017 for OS and CONS are based on available historical and current data. In case of lacking mortality data, we assumed a linear secular trend of improvement, also for CONS. Femur fracture proximal: in the elderly population of 70+ years, mortality data were used for ‘mortality after 365’ days, to account for nonsurgical complications due to polymorbidity. Such complications arrive later after proximal femur fracture and are of utmost importance for the very bad prognosis in this age group. Thus, probability of mortality for CONS after proximal femur fracture was set to be 60% (clinical expert opinion) for absence of surgery in this vulnerable group and unchanged over all time periods; mortality of 50% after 365 days was assumed in the sensitivity analysis [10]. For radius fractures, mortality was set at 0%, as mortality is not a relevant issue for this fracture type.
¶
Absence from work: absence from work for OS and CONS comprises intermediate (e.g., due to rehabilitation) or permanent absence (e.g., due to invalidity) from work. Data taken from [7] and on clinical expert knowledge. Invalidity rates are subject to sensitivity analyses to account for changes in working environment over years. Applied Swiss median wage (2015; age-specific; adjusted for level of employment): CHF 5329.
Example 1: patient with femur shaft fracture (mean age 34 years) with OS treatment and complication nonunion: assumed revision surgery with new implant and overall 17 month-absence from work after injury. Example 2: same 34-year old patient with femur shaft fracture with CONS treatment and permanent non-union: assumed 373-month absence from work for the residual period until age 65, corresponding to 100% invalidity.
#
Additional absence from work after VTE: assumptions based on clinical expert knowledge: 2 months of additional absence from work due to VTE after OP or CONS; the estimates were assumed to be identical and unchanged over all time periods to ensure a conservative estimate of the benefit of OP compared with CONS. Applied Swiss median wage (2015; age-specific; adjusted for level of employment): CHF 5329.
CHF: Swiss franc; CONS: Conservative therapy; OP: Osteosynthesis; OS: Osteosynthesis; p: Probability; VTE: Venous thromboembolism (includes deep vein thrombosis; pulmonary embolism).
Data sources
We used claims data of the Swiss Statistics in Accident Insurance (SSUV) [7]. This database covers about 60% of the Swiss population and extrapolation of the caseload to the full Swiss population is possible. There are two independent social insurance systems for healthcare in Switzerland [18]. First, there is compulsory health insurance for illness for all inhabitants. Second, there is accident insurance that is compulsory for all people in salaried employment. For others, such as the elderly, children, students or the self-employed, their health insurer also covers the costs of treatment in the case of accidents via additional accident insurance. Accident insurance for the employed has more generous benefits than health insurance. For instance, it also covers loss of working hours. The two parallel systems have evolved historically. The compulsory accident insurance scheme is operated by one large national insurance company (SUVA, with a partial monopoly for the manufacturing sector) and several private insurance companies that cover mainly employees from the service sector [18]. Both kinds of accident insurances contribute to the SSUV database.
In addition, we used data from the Swiss MedStat database that covers all in-patient treatments and includes patients beyond working age [19]. For example, all patients aged ≥70 years with femur fractures and in-patient treatment can be identified for specific treatment years. As age groups in the Medstat database are grouped in fixed age classes of ‘40–69’ and ‘70+’, we were not able to include patients from 65 to 69 years for analysis of patients beyond working age. For estimation of the impact in 16 example high-income countries, we used Organisation of Economic Cooperation and Development (OECD) [20] and World Bank data to adjust for country specific features [21].
Patient population
We included the employed Swiss population (aged <65 years), as documented in the SSUV database. Nonemployed people in working age (e.g., students or persons with unpaid work at home) were excluded. For proximal femur fractures, we also included elderly patients (≥70 years) from the MedStat database because proximal femur fractures of elderly people are a considerable and increasing disease burden for healthcare systems of high-income countries [8,22,23]. Included patients had to have as a main diagnosis a fracture of one of the three index bones: femur, tibia and radius (ICD codes: Supplementary Material 1B; distribution of patients across anatomical fracture locations: Supplementary Material 2; change of fracture case load over time: Supplementary Material 3). Patients with other main diagnoses or concomitant index fractures (i.e., non-main diagnosis index fractures) were excluded. Without this distinction, one may be estimating costs of unrelated care or unrelated invalidity, which could be high if fractures are comorbidity of other expensive conditions.
Intervention
OS of fractures of the three index bones (femur; tibia, radius).
Comparator
Conservative treatment (CONS) of fractures of the three index bones (femur; tibia, radius).
Costs
Fracture-related direct medical costs (Swiss francs [CHF]) for acute care treatment and rehabilitation (comprising all inpatient and outpatient after-care) of index bone fractures in patients <65 years were taken as calculated in the SSUV database (number of used resource units multiplied by current Swiss prices). Direct medical costs for treatment and rehabilitation of proximal femur fractures in the elderly population (≥70 years) were derived from the Swiss MedStat database, which covers all inpatient treatments (number of hospitalizations multiplied by current Swiss prices).
Production losses of all index bone fractures in patients <65 years were derived from the SSUV database using the human capital approach. We multiplied: months of temporary absence from work due to injury; months of permanent absence due to invalidity; or months of permanent absence due to premature death before age 65 by current average Swiss wages. Wages were age-specific and took mode and level of employment into account [24]. Different levels of participation in the labor market among men and women were also accounted for, as we only used data of employed persons.
Clinical outcome
We calculated YLG using mortality rates after index bone fractures for OS compared with CONS. We relied on published country-specific life expectancies to take other sources of mortality into account [20]. Relevant clinical data was taken from literature on complications [9,12,13,15–17,25], venous thromboembolism [13] and mortality [10,11,14] as well as from the SSUV database for mortality (Table 1) [7]. Literature was retrieved via focused searches in electronic databases. Discrepancies between publications were resolved via discussion among the clinical experts in the advisory board. In case of missing data for some time periods, we assumed a linear trend of change.
Selection of 17 high-income countries
We defined a sample of 17 countries to estimate the impact of OS on fracture care worldwide: 11 countries from Europe (Switzerland, Germany, Austria, Belgium, the Netherlands, Luxemburg, UK, Denmark, Norway, Sweden and Finland), two from North America (USA and Canada) and four from Asia/Pacific (Japan, Korea, Australia and New Zealand). We only included selected high-income countries to obtain a group of sufficiently homogeneous countries regarding economic conditions, medical technology penetration, population patterns and life-style factors. A ‘naive’ extrapolation of Swiss data to these high-income countries would not be a valid approach without application of further adjustments. In our model, we adjusted for the following five country-specific features [20,21]: population size; healthcare expenditures; life expectancy; gross domestic product per capita; a country-specific ‘technology penetration factor’ to account for historical differences in the technology penetration speed of OS compared with Switzerland (Supplementary Material 4 and 5). This technology penetration factor was estimated based on historical knowledge of interviewees as well as on sale rates of Synthes OS products and the AO’s local educational activities (Germany, Austria: 5-year delay; other included European countries: 10-year delay; included Northern America and Asia/Pacific countries: 25-year delay; from 2000 onwards, technology penetration rate was assumed to be 100% for all included countries) [26,27].
Analysis
With our approach, we finally derived an estimate of the accumulated difference in YLG, in addition to direct and indirect costs of fracture care with OS compared with CONS for three index bones (modeled for nine anatomical locations) in 17 high-income countries over a period of 60 years.
For our cost-analysis, the time horizon for extrapolation of future productivity losses/gains in the SSUV population was from injury to end of working age (65 years). We used a fixed discount rate of 3% for indirect costs. For example, if the mean age of femur shaft fractures in the SSUV population was 45 years, we discounted future productivity gains of OS compared with CONS for the next 20 years until age 65 with a discount rate of 3%. Direct medical costs were not discounted, as they are incurred usually close to the time of fracture. The few historical cost data that were available went more or less in parallel with the 2015 Health Component of the Swiss consumer price index over the last 60 years. Thus, we applied 2015 Swiss costs for all modeled years (1958–2017; inflation rate from 2015 to 2017 in Switzerland is negligible; official 2017 conversion rate: 1 CHF = 1.026 $US).
For our analysis of YLG, the time horizon was from injury to statistically expected end of life for the SSUV and the elderly population aged ≥70 years. We discounted the YLG in the working age and in the elderly population using a fixed discount rate of 3%.
Finally, we performed a series of one-way sensitivity analyses on key parameters (assumed invalidity rates, discount rates, ratio between Swiss and international wages; mortality of elderly patients) to assess the magnitude of influence on outcomes. Analyses were performed using the Microsoft Excel software package (MS Office Professional Plus 2016, USA).
Results
Femur fractures (working-age population)
In the Swiss working-age population, we analyzed 72,360 femur fracture cases (all locations) from 1958 to 2017 with 1.7 million modeled person years (mean age at fracture: 33.5–51.8 years, depending on location; Supplementary Material 2). In patients with femur fractures, modeled average direct medical costs in Switzerland in 2015 are a fifth lower for OS (CHF 19,600) compared with (hypothetical) CONS treatment (CHF 24,200). While the acute care hospital costs for OS are higher than for CONS treatment (e.g., femur shaft fracture without complications: CHF 15,500 vs 10,720), a shorter and less costly rehabilitation period for patients with OS (CHF 3000 vs 12,540), finally leads to higher direct medical costs for CONS treatment according to our model assumptions. The difference in indirect costs is more pronounced. Average indirect costs in Switzerland for OS are only a fifth (CHF 31,000) of the costs for CONS treatment (CHF 158,000) in this patient group. This is mainly due to a shorter period of absence from work compared with CONS and higher return-to-work rates. In addition, lower mortality rates for OS lead to 28,000 YLG until age 65 (40,000 YLG until end of life) which in turn results in decreased productivity losses due to premature death before age 65 (spread of OS and decrease of mortality: Supplementary Material 6). In summary, savings due to OS compared with CONS in patients with femur fractures in this age group are CHF 131,000 per patient, which is mainly due to savings of indirect costs (CHF 127,000).
Annual savings in total costs for femur fracture treatment due to OS increased from 1958 to 2017, due to an increase in technology penetration and a change in epidemiology of fractures. Estimation of the impact in 17 high-income countries resulted in total savings of CHF 272 billion for femur fracture treatment (all locations) in the modeled population (age <65; Table 2). Across 17 high-income countries, we estimated 2.5 million YLG (about 2/3 of these life years are gained before age 65 and included in productivity gains, i.e., indirect cost savings; Table 3).
| Fracture location | Savings in Switzerland direct costs (CHF) (per patient) | Savings in Switzerland indirect costs (CHF) (per patient) | Savings in Switzerland total costs (CHF) (per patient) | Savings in Switzerland total costs (CHF) (1958–2017) | Savings in 17 HICs† total costs (CHF) (1958–2017) |
|---|---|---|---|---|---|
| Femur, age <65 | 4000 | 127,000 | 131,000 | 5 billion | 272 billion |
| Proximal femur, age ≥70 | 3000 | Not included in calculation (retired) | 3000 | 1.1 billion | 69 billion |
| Tibia, age <65 | 2000 | 102,000 | 104,000 | 9.8 billion | 507 billion |
| Radius, age <65 | -4500 | 18,200 | 13,700 | 1.5 billion | 77 billion |
†
‡
Federal Republic of Germany and German Democratic Republic combined for the time before 1989.
§
Korea only since 2000, when it became an Organisation of Economic Cooperation and Development high-income country.
Costs are in Swiss francs (CHF; official 2017 conversion rate: 1 CHF = $US1.026; source: www.exchange-rates.org/Rate/USD/CHF/12-31-2017).
HIC: High-income country.
| Fracture location | Life years gained in Switzerland, total | Life years gained in 17 HICs† total |
|---|---|---|
| Femur, age <65 | 40,000 | 2.5 million |
| Proximal femur, age ≥70 | 0.9 million | 73 million |
| Tibia, age <65 | 37,000 | 2.1 million |
| Radius, age <65 | Mortality is not a relevant issue | Mortality is not a relevant issue |
†
‡
Federal Republic of Germany and German Democratic Republic combined for the time before 1989.
§
Korea only since 2000, when it became an Organisation of Economic Cooperation and Development high-income country.
YLG are calculated until expected end of life for each population according to published life expectancy.
HIC: High-income countries; YLG: Years of life gained.
Proximal femur fractures (elderly population)
In the Swiss elderly population, we analyzed 508,000 proximal femur fracture cases from 1958 to 2017 with 5.8 million modeled person years (mean age at fracture: 75.5 years; Supplementary Material 2). For elderly patients, we modeled only the impact of OS on proximal femur fractures, as this fracture type represents about 85% of femur fractures in this age group [19]. Our modeled incidence of low-impact hip fractures was 154 cases/100,000 inhabitants per year, which was derived from Swiss hospital statistics [19]. This incidence rate was in the range of several other high-income countries [28–31].
For an estimate of direct medical costs, we used the same cost input variables as for the working population but applied an age-specific caseload per year and higher age specific complication rates [8,10,11,29]. For the period 1958–2017, total savings in direct medical costs for treatment of proximal femur fractures in 17 high-income countries resulted in CHF 69 billion (Table 2). In addition, we estimated 73 million YLG (Table 3; pattern across countries: Figure 2).
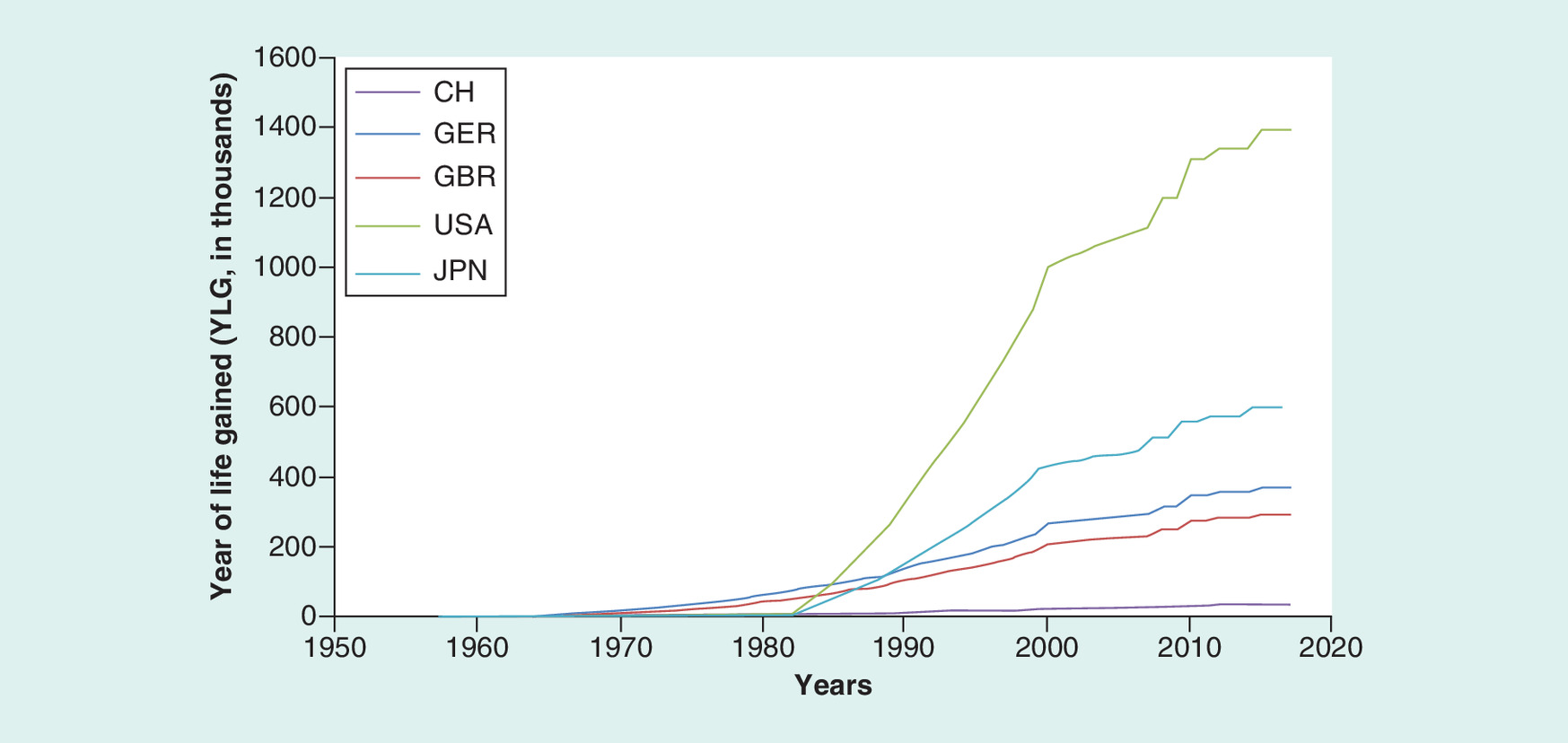
Figure 2. Years of life gained in proximal femur fractures of the elderly across five countries.
Change of annual YLG (in thousands) of the elderly population (‘age 70+’) for each of five modeled high-income countries is depicted from 1958 to 2017. Increase of YLG over time is mainly driven by OS technology penetration and the growing share of elderly persons in high-income countries.
OS: Osteosynthesis; YLG: Years of life gained.
Tibia fractures (working-age population)
In the Swiss working-age population, we analyzed 210,974 tibia fracture cases (all locations) from 1958 to 2017 with 5.1 million modeled person years (mean age at baseline: 39.9–41.7 years; Supplementary Material 2). Similar distributions of direct and indirect costs for OS and CONS were found for tibia fractures as for femur fractures in this age group. Savings due to OS compared with CONS in patients with tibia fractures are CHF 104,000 per patient (direct and indirect costs), which is mainly due to savings of indirect costs (CHF 102,000).
Estimation of the impact in 17 high-income countries resulted in total savings of CHF 507 billion for tibia fracture treatment (Table 2; share of savings across countries: Figure 3). Across 17 high-income countries, we estimated 2.1 million YLG (again, about 2/3 of these YLG before age 65 are included in productivity gains, i.e., indirect cost savings; Table 3).
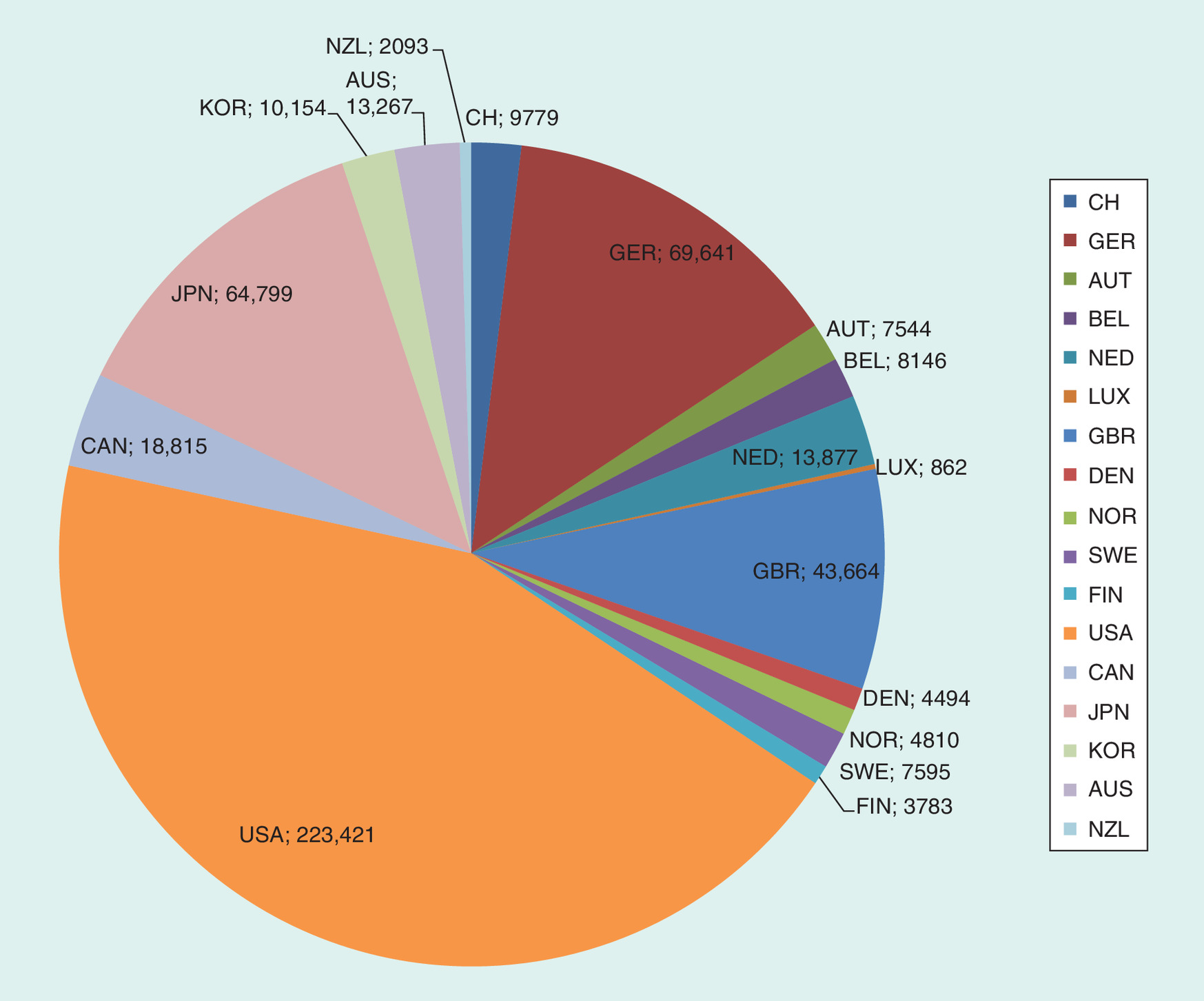
Figure 3. Estimated savings for tibia fractures across 17 high-income countries.
Savings in total costs in patients with tibia fractures (all anatomic locations: osteosynthesis vs conservative treatment) in 17 high-income countries from 1958 to 2017. Savings in million 2015 Swiss francs (CHF); discount rate 3%.
Radius fractures (working-age population)
For radius fractures, we included in our model only the rate of fracture cases, where an indication for OS is given according to current practice for each fracture location (age <65 years: radius proximal: 65%; radius shaft: 100%; radius distal: 90%) [17,32]. This is in contrast to femur and tibia fractures, where the number of patients with a fracture diagnosis is today almost identical with the number of patients with clear indication for OS. We finally analyzed 312,000 radius fracture cases with indication for OS (all locations; thereof 80% distal radius fractures) from 1958 to 2017 with 7 million modeled person years (mean age at baseline: 39.3–42.7 years; Supplementary Material 2).
Savings due to OS compared with CONS in patients with radius fractures are CHF 13,700 per patient (higher direct costs: CHF 4500; lower indirect costs: CHF -18,200). For the period 1958–2017, estimation of the impact in 17 high-income countries resulted in CHF 77 billion (Table 2; pattern across fracture types in Switzerland: Supplementary Material 7). We have not calculated YLG, as mortality is not a relevant issue for these fractures.
Overall impact & sensitivity analyses
Taking the three index bones together for the working-age population, we estimated savings of total costs over a period of 60 years in the 17 selected high-income countries of CHF 856 billion (base-case ‘best guess’ at discount rate 3%; currency: 2015 Swiss francs). The minimum-to-maximum range in our sensitivity analysis was from CHF 360 billion (most conservative case) to 1213 billion (Figure 4; for detailed figures: Supplementary Material 8).
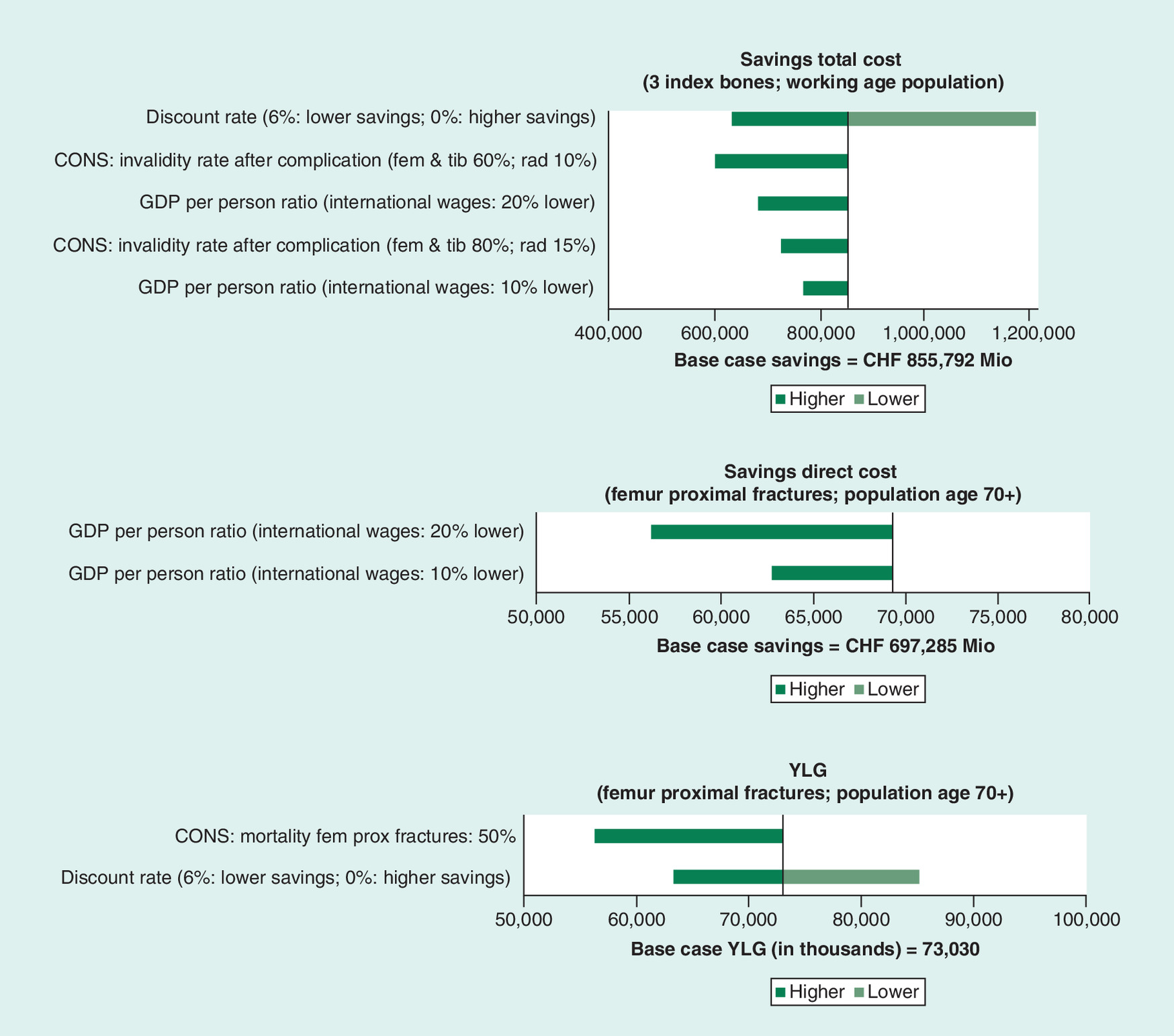
Figure 4. Summary of sensitivity analyses.
Tornado diagram of sensitivity analyses for three outcomes: savings in total costs (three index bones; working age population); savings in direct costs (proximal femur fractures; population age ≥70 years); years of life gained (YLG [proximal femur fractures; population age ≥70 years]).
CONS: Conservative therapy; YLG: Years of life gained.
For the working-age population, a change in the discount rate has the biggest absolute effect on savings in total costs (scenario 0%: CHF 1213 billion; scenario 6%: CHF 635 billion). Assumed invalidity rates after complications with CONS have the next strongest effect on indirect costs (high degree of invalidity [base-case scenario]: savings of CHF 856 billion; intermediate invalidity: CHF 728 billion; low invalidity: CHF 602 billion). Changes in the relationship between Swiss and international wages lead to less pronounced effects on outcomes.
For the elderly population, the range of YLG (base-case: 73 million) is between 85 million (discount rate 0%) and 63 million (discount rate 6%) or 56 million (at an assumed mortality of CONS after proximal femur fracture of 50%; base-case: 60%).
Discussion
In our bottom-up approach, we modeled the clinical course of 595,000 fracture patients from the Swiss working-age population (13.8 million person years from 1958 to 2017) and of 507,000 patients from the Swiss elderly population (5.8 million person years). Furthermore, we estimated the impact of OS in 17 selected high-income countries. The impact of osteosynthesis in fracture care for femur, tibia and radius fractures is substantial for both individual patients and for society as a whole: savings of total costs in the working-age population are mainly due to productivity gains. Compared with OS, CONS treatment for long bone fractures is linked with considerable productivity losses due to long absence from work and often sub-optimal functional outcome. For the elderly population and the working-age population alike, OS leads to a substantial number of life years gained due to lower mortality after long bone fractures. Together with better functional results, this leads to improved quality of life of patients and their relatives, although we had no data to quantify that.
Results in context
The magnitude of estimated savings is difficult to interpret, as cognitive references are often made to a specific country, a specific time window (often 1 year) or a benchmark (e.g., gross domestic product [GDP] of a country).
To break our figures down, we provide some comparisons (Supplementary Material 9). A US research group assessed the impact of better controlled blood pressure on cardiovascular disease (myocardial infarction and stroke), calculating savings in direct medical costs and the number of deaths avoided [3]. In terms of excess deaths avoided, the annual impact of osteosynthesis on femur and tibia fracture care in the USA is of a similar size as the annual impact of antihypertensive care in the USA (osteosynthesis: 2600 lives saved [population age: <65 years] plus 126,000 lives saved [population age: ≥70 years; proximal femur fractures only]; antihypertensive drugs for cardiovascular disease: 86,000 lives saved [population age: 30–79 years]).
For comparison of cost savings, we used our combined estimates (femur, tibia and radius fractures; all locations; direct and indirect costs; population age <65 and ≥70 years). The impact of osteosynthesis in the USA in the year 2016 is of a similar size to the annual impact of antihypertensive care in the USA (osteosynthesis: US$15.3 billion saved; antihypertensive drugs for coronary heart disease and cerebrovascular disease combined: US$16.5 billion saved; population age: 30–79 years). However, the savings due to antihypertensive drugs in the USA may be substantially underestimated, as no indirect costs were included by the US researchers [3]. A comparison of savings with the GDP provides additional information. The estimated cost savings for osteosynthesis and for antihypertensive drugs are in a comparable range of 0.05–0.09% of GDP in three example countries (USA, Germany and Switzerland).
Study strengths & limitations
Our analysis has several strengths: we used real-world patient-care data from a large Swiss accident insurance company and had access to historical treatment data for Switzerland. We cross-checked the plausibility of the annual caseload of high impact fractures [33] as well as direct medical costs using results of a Swiss study on non-communicable diseases (NCD) that included injuries [34]. In addition, we validated our model input by cross-comparison with other results (e.g., number of OS teaching events in some countries; international sale rates of OS devices; specific fracture data in the USA and New Zealand).
In summary, our results represent conservative estimates as we applied conservative assumptions for the input parameters of our model. First, we included only cases with a fracture of an index bone as the main diagnosis, as we wanted to isolate the impact on fracture care of the index bone (e.g., no cases were included with fracture of an index bone as a secondary diagnosis in multi-trauma patients with brain injury, which would have contaminated cost-analysis). Second, in working-age patients, we used YLG before age 65 years for calculation of productivity gains. Additional YLG in this population (from end of working age until end of life expectancy) were not used for calculation of indirect costs in our human capital approach. This approach, however, leads to an underestimate of total benefits over the entire expected life span. Third, possible effects in other (excluded) high- or middle-income countries (e.g., BRIC-countries: Brazil, Russia, India and China) are not covered. These effects are potentially huge according to the Global Burden of Disease study [35]. During the transition process, these middle-income countries have a high burden of injury-related morbidity and mortality, for example, via road injuries with high-impact bone fractures [35].
Our modelling approach also has several limitations as it is based on critical assumptions. First, the workforce of high-income countries has changed over time (changing sector mix with decreasing proportion of blue collar and increasing proportion of white collar workers). While this has implications for injury patterns during work time, which are included in the SSUV data, it also has implications for calculation of invalidity rates and success of occupational redeployment. In our sensitivity analysis, we have varied invalidity rates toward lower values, which reflects a higher proportion of white collar workers. Second, we used fracture-specific cost data for Switzerland, but no such national data was available in the same granularity for the other high-income countries. Third, from the year 2000 onward, we assumed a technology penetration rate of 100% in all included high-income countries. This may not always and in all regions be the case, as studies about regional variations in healthcare systems have shown empirically [36]. Comparing a policy with OS for all fractures (where OS is indicated) with CONS for all fracture patients may, thus, sometimes be an overestimation. Fourth, complication rates may differ substantially depending on regional case mix and surgeon caseload [37]. We had no data to take these factors into account in our study. Fifth, for some high-income country features, we assumed similar conditions over time to those in Switzerland (i.e., change of age structure of population; epidemiology of changes in fracture incidence over time). Finally, organizational and financial responsibilities in a healthcare system may differ across countries. For example, our approach is derived from the perspective of a social insurance-based healthcare system. Such a perspective is not valid for the whole observation period for all countries (e.g., mostly private health insurance system in the USA, until the Affordable Care Act in 2012). Furthermore, in National Health Service (NHS) countries the indication for operative treatment of radius fractures may be different compared with the treatment decisions in Switzerland as an example of a non-NHS country.
Implications for decision makers
The technology of osteosynthesis is well established in state-of-the-art fracture care. However, as with any technology, new questions arise and old problems have to be resolved. For example, re-evaluation of the evidence base is an issue. Clinical studies should continue to evaluate: if osteosynthesis leads to better results compared with conservative therapy in some fracture types, where indication for surgery is under debate; or which approach of osteosynthesis is more effective, where the indication for surgery is non-controversial [9]. In addition, device infection and device failure are still complications with high impact on patients’ quality of life. Despite the great improvements made in the development of high-tech implants in recent years, evolution of technical progress may further provide useful innovations (e.g., concerning bone regeneration, polymers, stem cells) and even more effective strategies to prevent device infection.
From a population health perspective, the knowledge base for evidence-based decisions has to be improved [38]. Examples are improved availability of real-world data in fracture care; registries with complete data for standardized patient reported outcome measures, complications and mortality; combination of patient benefit data and costs to assess real world cost–effectiveness of OS (‘value of healthcare’) [39]. These actions may allow an implementation and continuous monitoring of impact indicators in fracture care in high-income countries. Furthermore, this issue is of specific relevance for the success of the recently launched Global Emergency and Trauma Care Initiative of the WHO in cooperation with the AO Alliance to transform trauma care systems in low- and middle-income countries and improve outcomes for patients [40]. First, a thorough adaption of our model for structure and input parameters in close contact with local experts of low- and middle-income countries is needed. Thereafter, the estimated impact of OS could be used for comparison with projected benefits of, for example, interventions for non-communicable diseases or improved maternal care as derived from other data sources.
Conclusion
Based on the data available, we found that the technology of OS had a significant impact on patient care after bone fractures over the last 60 years, which is relevant to decision makers. Improved functional results with higher return to work rates as well as decreased mortality rates after long bone fractures had a substantial impact: OS led to significant productivity gains for society and saved a substantial number of life years.
Why impact evaluations matter
•
Osteosynthesis (OS) has revolutionized fracture care.
•
A formal impact evaluation of OS as a medical innovation can estimate the impact on health and productivity in populations.
Our aim
•
To estimate the health economic impact of OS in fracture care for three index bones over six decades in 17 example high-income countries.
How we proceeded
•
We assumed a hypothetical absence of the technology of OS and compared OS (intervention) with conservative treatment (CONS; comparator) from a societal perspective.
•
We applied a decision tree model for our cost comparison study. We included fracture patients with femur, tibia and radius fractures (age <65 years); for proximal femur fractures also elderly patients (≥70 years) were included.
•
Outcomes were differences between OS and CONS in years of life gained (YLG) as well as in direct and indirect costs (2015 Swiss francs [CHF] for all modeled years; discount rate 3%).
•
We estimated the impact in 17 example high-income countries (e.g., Switzerland, Germany, USA, Japan and Australia).
Our findings
•
We modeled the clinical course of 595,000 fracture patients from the Swiss working-age population (13.8 million person years from 1958 to 2017) and of 507,000 patients from the Swiss elderly population (5.8 million person years).
•
Estimation of the impact in 17 high-income countries showed savings in direct and indirect costs of CHF 855 billion (minimum 360 to maximum 1213) over six decades in the working-age population.
•
A total of 4.6 million YLG resulted in this age group (2/3 of them before age 65 and incorporated in indirect costs).
•
In the elderly population, CHF 69 billion were saved in direct costs of proximal femur fractures in addition to 73 million YLG.
Potential implications of the findings
•
The health economic impact of OS was substantial over six decades.
•
After a thorough adaption of our model for structure and input parameters in close contact with local experts, the findings may have implications for transforming trauma care systems in low- and middle-income countries to improve outcomes for patients.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Financial & competing interests disclosure
K Eichler reports personal fees from AO Foundation (expert meeting); F Gutzwiller reports personal fees from AO Foundation (advisory board); E Denk and A Joeris are employees of the AO Foundation; J Prein reports being the Vice President of the AO Alliance; N Renner reports being the immediate Past President of the AO Foundation. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
According to the Human Research Act in Switzerland, approval from a local Ethics committee was not required for studies using an anonymized database.
Availability of data and materials
Decision tree model structure, as well as key input parameters of decision tree model and parameters of sensitivity analyses are included in this published article.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 186.12 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Schlich T. Surgery, Science and Industry: A Revolution in Fracture Care, 1950s–1990s. Palgrave Macmillan UK, London, UK (2002).
• Provides a deeper understanding of the impact of osteosynthesis on patients, teaching, industry and science.
2.
Schlich T. Osteosynthese: geschichte einer schwierigen therapiemethode. In: Geschichte operativer Verfahren an den Bewegungsorganen. Rauschmann MA, Thomann K-D, Zichner L (Eds). Steinkopff Heidelberg, Heidelberg, Germany, 55–72 (2000).
3.
Cutler DM, Long G, Berndt ER et al. The value of antihypertensive drugs: a perspective on medical innovation. Health Aff. 26(1), 97–110 (2007).
4.
Turner S, Bhurke S, Cook A. Impact of NIHR HTA programme funded research on NICE clinical guidelines: a retrospective cohort. Health Res. Policy Syst. 13, 37 (2015).
5.
Guthrie S, Bienkowska-Gibbs T, Manville C, Pollitt A, Kirtley A, Wooding S. The impact of the National Institute for Health Research Health Technology programme, 2003–13: a multimethod evaluation. Health Technol. Assess. 19(67), 1–291 (2015).
6.
Guthrie S, Hafner M, Bienkowska-Gibbs T, Wooding S. Returns on research funded under the NIHR Health Technology Assessment (HTA) Programme. RAND Europe 1–83 (2015).
7.
Central Office for Statistics in Accident Insurance. SSUV Statistik der Unfallversicherung UVG: medizinische Statistik (2017). www.unfallstatistik.ch/d/neuza/med_stat/med_stat_d.htm
8.
Flikweert ER, Wendt KW, Diercks RL et al. Complications after hip fracture surgery: are they preventable? Eur. J. Trauma Emerg. Surg. 44(4), 573–580 (2018).
• Provides historical data on hip fracture mortality of the elderly population.
9.
Fixation Using Alternative Implants for the Treatment of Hip Fractures Investigators. Fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet 389(10078), 1519–1527 (2017).
10.
Roberts SE, Goldacre MJ. Time trends and demography of mortality after fractured neck of femur in an English population, 1968–98: database study. BMJ 327(7418), 771–775 (2003).
• Provides historical data on hip fracture mortality of the elderly population.
11.
Dahl E. Mortality and life expectancy after hip fractures. Acta Orthop. Scand. 51(1), 163–170 (1980).
12.
Smith T, Hedges C, Macnair R, Schankat K, Wimhurst J. The clinical and radiological outcomes of the LISS plate for distal femoral fractures: a systematic review. Injury 40(10), 1049–1063 (2009).
13.
Mcnamara IR, Smith TO, Shepherd KL et al. Surgical fixation methods for tibial plateau fractures. Cochrane Database Syst. Rev. (9), CD009679 (2015).
14.
Scholz-Odermatt S. Veränderung der Unfallpyramide. Unfallstatistik UVG 2008-2012 Suva, Luzern, Switzerland, 71–79 (2012).
15.
Clement ND, Beauchamp NJ, Duckworth AD, Mcqueen MM, Court-Brown CM. The outcome of tibial diaphyseal fractures in the elderly. Bone Joint J. 95-B(9), 1255–1262 (2013).
16.
Kuo LT, Chi C-C, Chuang C-H. Surgical interventions for treating distal tibial metaphyseal fractures in adults. Cochrane Database Syst. Rev. (3), CD010261 (2015).
17.
Kupperman ES, Kupperman AI, Mitchell SA. Treatment of radial head fractures and need for revision procedures at 1 and 2 years. J. Hand Surg. (Am.) 43(3), 241–247 (2018).
18.
Brugger U, Plessow R, Hess S et al. The health technology assessment of the compulsory accident insurance scheme of hand transplantation in Switzerland. J. Hand Surg. Eur. Vol. 40(9), 914–923 (2015).
19.
Bundesamt für Statistik, Medizinische Statistik der Krankenhäuser (2016). www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/erhebungen/ms.html
20.
OECD Data (2018). https://data.oecd.org/
• Provides country-specific data for estimation of international impact.
21.
World Bank How does the World Bank classify countries? (2018). https://datahelpdesk.worldbank.org/knowledgebase/articles/378834-how-does-the-world-bank-classify-countries
22.
Lyles KW, Colon-Emeric CS, Magaziner JS et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N. Engl. J. Med. 357(18), 1799–1809 (2007).
23.
Suhm N, Kaelin R, Studer P et al. Orthogeriatric care pathway: a prospective survey of impact on length of stay, mortality and institutionalisation. Arch. Orthop. Trauma Surg. 134(9), 1261–1269 (2014).
24.
Bundesamt für Statistik Lohnniveau Schweiz (2018). www.bfs.admin.ch/bfs/de/home/statistiken/arbeit-erwerb/loehne-erwerbseinkommen-arbeitskosten/lohnniveau-schweiz.html
25.
Gillespie WJ, Walenkamp GH. Antibiotic prophylaxis for surgery for proximal femoral and other closed long bone fractures. Cochrane Database Syst. Rev. (3), CD000244 (2010).
26.
Joeris A, Hoglinger M, Meier F et al. The impact of the AO Foundation on fracture care: an evaluation of 60 years AO Foundation. Injury 50(11), 1868–1875 (2019).
•• Provides a deeper understanding of the impact of osteosynthesis on patients, teaching, industry and science.
27.
Jeanneret J-P. Leading a Surgical Revolution. Springer Nature Switzerland AG, Cham, Switzerland (2019).
28.
Piscitelli P, Brandi ML, Chitano G et al. Epidemiology of fragility fractures in Italy. Clin. Cases Miner. Bone Metab. 8(2), 29–34 (2011).
29.
Kannegaard PN, Van Der Mark S, Eiken P, Abrahamsen B. Excess mortality in men compared with women following a hip fracture. National analysis of comedications, comorbidity and survival. Age Ageing 39(2), 203–209 (2010).
• Provides recent data on hip fracture mortality of the elderly population.
30.
Page PR, Lord R, Jawad A et al. Changing trends in the management of intertrochanteric hip fractures – a single centre experience. Injury 47(7), 1525–1529 (2016).
31.
Imai N, Endo N, Shobugawa Y et al. A decrease in the number and incidence of osteoporotic hip fractures among elderly individuals in Niigata, Japan, from 2010 to 2015. J. Bone Miner. Metab. (2017) (Epub ahead of print).
32.
Motisi M, Kurowicki J, Berglund DD et al. Trends in management of radial head and olecranon fractures. Open Orthop J 11, 239–247 (2017).
33.
Wieser S, Kauer L, Brügger U. Cost-benefit analysis of road accident prevention programmes in Switzerland from 1975 to 2007. (2009). file:///C:/Users/l.dormer/Downloads/01-2009-bericht-cba-road-accidents-e.pdf
34.
Wieser S, Tomonaga Y, Riguzzi M et al. The cost of non-communicable diseases in Switzerland. (2014). www.zora.uzh.ch/id/eprint/103453/
35.
Murray CJ, Barber RM, Foreman KJ. Global Burden of Disease Dalys Hale Collaborators. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. Lancet 386(10009), 2145–2191 (2015).
• Provides data on burden of disease due to injuries in countries of transition.
36.
Wennberg J, Gittelsohn A. Small area variations in health care delivery. Science 182(4117), 1102–1108 (1973).
37.
Caputo LM, Salottolo KM, Slone DS, Mains CW, Bar-Or D. The relationship between patient volume and mortality in American trauma centres: a systematic review of the evidence. Injury 45(3), 478–486 (2014).
38.
Schweizerische Akademie Der Medizinischen Wissenschaften. Stärkung der Versorgungsforschung in der Schweiz. Swiss Academic Reports 9(1), 1–59 (2014).
39.
Porter M, Teisberg E. Redefining Health Care. Creating Value-Based Competition on Results. Harvard Business School Press, MA, USA (2006).
40.
World Health Organization Global emergency and trauma care initiative (2019). www.who.int/emergencycare/global-initiative/en/
• A recent WHO initiative to tackle burden of disease due to injuries in countries of transition.
Information & Authors
Information
Published In
Pages: 483 - 496
PubMed: 32301332
Copyright
© 2020 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 December 2019
Accepted: 15 February 2020
Published online: 17 April 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact of osteosynthesis in fracture care: a cost comparison study. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0194
Export citation
Select the citation format you wish to export for this article or chapter.