Real-world outcomes of long-term prednisone and deflazacort use in patients with Duchenne muscular dystrophy: experience at a single, large care center
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess outcomes among patients with Duchenne muscular dystrophy receiving deflazacort or prednisone in real-world practice. Methods: Clinical data for 435 boys with Duchenne muscular dystrophy from Cincinnati Children’s Hospital Medical Center were studied retrospectively using time-to-event and regression analyses. Results: Median ages at loss of ambulation were 15.6 and 13.5 years among deflazacort- and prednisone-initiated patients, respectively. Deflazacort was also associated with a lower risk of scoliosis and better ambulatory function, greater % lean body mass, shorter stature and lower weight, after adjusting for age and steroid duration. No differences were observed in whole body bone mineral density or left ventricular ejection fraction. Conclusion: This single center study adds to the real-world evidence associating deflazacort with improved clinical outcomes.
Lay abstract
This retrospective study described outcomes for boys with Duchenne muscular dystrophy treated at Cincinnati Children’s Hospital Medical Center with the glucocorticoids deflazacort (∼95% daily dosing) or prednisone (∼68% daily dosing). Patients receiving deflazacort had lower risk of losing ambulation, lost ambulation at older ages than those receiving prednisone, and had lower risk of scoliosis. Across clinic visits, deflazacort was associated with greater preservation of ambulatory and pulmonary function, shorter stature, lower bodyweight and greater % lean body mass. This study adds to the evidence associating real-world dosing of deflazacort with improved outcomes for patients with Duchenne muscular dystrophy.
Duchenne muscular dystrophy (DMD) is an X-linked recessive disorder characterized by progressive deterioration in skeletal and cardiac muscles due to mutations in the dystrophin gene [1]. Globally, DMD affects approximately one in every 3500 newborn males [2]. Initial manifestations of the disorder include progressive declines in ambulatory function during childhood that typically culminate in complete loss of independent ambulation by adolescence [3]. Additional impacts include worsening cardiac and pulmonary function, as well as a deterioration in bone health; over time, these disabling declines collectively contribute to mortality by early adulthood. The median survival for boys with DMD is 21.8 years [4–8].
Corticosteroids are the current standard of care for patients with DMD, and have modified the natural history of the disease by slowing the progression of motor and pulmonary functional decline and extending survival [9–11]. The beneficial effects of corticosteroids are attributed to their anti-inflammatory activity, particularly in muscles with low levels of dystrophin, which can help preserve ambulation by delaying the loss of muscle strength [7,12]. The glucocorticoids in use have been prednisone/prednisolone and deflazacort, an oxazoline derivative of prednisolone. Prolonged glucocorticoid steroid treatment is associated with linear growth failure, excessive weight gain and heightened risk of osteoporosis [12,13].
Comparative studies of prednisone and deflazacort in DMD have been based on randomized trials [14–16], post-hoc analyses of placebo-arm data [17,18] and on longer term analyses of natural history data [9–11]. While clinical trials are the gold standard for assessing the efficacy and safety of therapeutics, data from electronic health records of patients seen in clinics can be used to assess real-world outcomes. We aimed to study the outcomes associated with deflazacort and prednisone/prednisolone treatments, including ambulatory, pulmonary, cardiac, growth and bone-health outcomes, in patients with DMD with the use of real-world data from a large, single center cohort receiving coordinated, collaborative and interdisciplinary patient- and family-centered care consistent with modern guidelines for the management of DMD [19].
Patients
This is a retrospective cohort analysis of clinical data from electronic health records of patients with DMD who attended the Comprehensive Neuromuscular Center at Cincinnati Children’s Hospital Medical Center (CCHMC) from 2004 to March 2017. The de-identified data from an institutional review board (IRB) approved electronic clinic registry (IRB #2010-1881) were curated for the following variables of interest: demographics, vitals, glucocorticoid steroid use, bone density and body composition (via dual-energy x-ray absorptiometry [DEXA] scans), diagnosis of scoliosis and measures of ambulatory, pulmonary and cardiac function. Patients included in the present study were required to have a recorded date of steroid initiation and a recorded steroid type in the CCHMC database. The majority (99%) of clinic visits and follow-up time included in this study occurred prior to the US FDA approval of deflazacort in February 2017; during this period patients took imported deflazacort. The outcomes of interest were ages at clinical events (loss of ambulation and scoliosis); patients’ ambulatory, pulmonary and cardiac function; and weight, lean body mass and bone health.
Statistical methods
Analyses of ages at clinical events
For the analyses of ages at clinical events, included patients were categorized into prednisone- and deflazacort-initiated groups based on their first recorded steroid type. Patient characteristics during the first clinic visit and their dosing regimens (daily vs other) were summarized in these groups. Means and standard deviations (SD) were reported for continuous characteristics; counts and percentages were reported for categorical characteristics.
Loss of ambulation was identified as Functional Mobility Scale (FMS) score >4, which is indicative of patients’ full-time use of a wheelchair for mobility in DMD. The FMS ranges from 1 (mild gait abnormalities) to 8 (unable to sit without support) with FMS 1–4 for ambulatory patients and 5–8 for nonambulatory patients. Patients studied for this outcome were required to have an FMS score of 1–4 at their first clinic visit.
Age at onset of scoliosis was defined as the first recorded clinical diagnosis of scoliosis in the patient’s medical record. Clinical diagnosis of scoliosis at CCHMC is determined based on clinical examination and confirmation with spine radiographic reports finding Cobb’s angle >20 degrees. Patients studied for time to scoliosis were required to be free of scoliosis at their first clinic visit.
Age at first occurrence of FMS >4 and first diagnosis of scoliosis were studied in time-to-event analyses, with age as the time variable, and censoring at the end of data availability. Kaplan-Meier curves and log-rank tests were calculated to compare these outcomes between steroid initiation groups. Cox proportional hazards analyses were used to estimate the association between steroid type and age at event while adjusting for age at steroid initiation, the calendar year during which the patient had initiated steroid use, and whether the patient had initiated steroids prior to or after their first clinic visit at CCHMC. The adjusted analyses thus accounted for differences in the duration of steroid exposure, potential temporal trends that might impact outcomes across groups, and potential differences in care received prior to CCHMC. Sensitivity analyses were conducted distinguishing between patients who received daily versus other regimens of prednisone and, separately, distinguishing those who maintained prednisone versus those who switched to deflazacort after initiation.
Analyses of average outcomes across clinic visits
For the analyses of associations between steroid type and clinical status, patients’ clinic visits were included in the analysis if the patient was ≥4 years of age at the visit and consistently used either prednisone or deflazacort while under care at CCHMC. Patients who switched steroids were excluded from this analysis, as the precise date of switching was not always available. Studied outcomes included: functional outcomes (4 stair climb [4SC] velocity [stairs/second]; 30-ft walk/run velocity [feet/seconds]; timed sit-to-stand velocity [1/seconds]; North Star Ambulatory Assessment [NSAA] total score), forced vital capacity (FVC) %-predicted; left ventricular ejection fraction (LVEF) %; body size and composition (height [cm], total body mass [kg], % lean body mass, % body fat); and bone health assessed as whole body bone mineral density (BMD in g/cm2) using DEXA. Analyses of each outcome included only those visits at which the outcome was measured. For ambulatory function tests, this excluded visits at which the test was not conducted because the patient was not willing or able to complete the test.
Multivariable regression analyses were used to estimate cross-sectional associations between steroid type (deflazacort or prednisone) and each outcome measure across all assessments. These analyses estimated the average differences observed during clinic visits between patients receiving deflazacort and those receiving prednisone. The analyses were adjusted for current age, years since steroid initiation, whether the patient had begun taking steroids prior to or after their first clinic visit at CCHMC, and current visit year, as well as the interaction between current age and years since steroid initiation. The inclusion of the interaction term allows the effect of duration of steroid exposure to potentially vary by current age. Adjustment for visit year (i.e., the calendar year of the visit) accounts for potential temporal factors that might have influenced outcomes. Adjusting for whether the patient had initiated steroids prior to or after their first clinic visit at CCHMC accounts for potential differences in care received prior to CCHMC. Generalized estimating equations with an exchangeable correlation structure were used to account for the use of multiple clinic visits per patient.
Results
Patient characteristics
Among n = 600 total boys in the CCHMC database, n = 559 had their date of steroid initiation recorded and n = 500 had a steroid type recorded at some point during their follow-up history at CCHMC. A further n = 435 of these patients had at least one assessment of FMS or an assessment for scoliosis. Among these patients, at their first clinic visit at CCHMC, those treated with prednisone (n = 105; 68% daily) had a mean (±SD) age of 8.1 (±3.1) years, while patients treated with deflazacort (n = 330; 95% daily) had a mean age of 6.5 (±3.1) years (Table 1). A little over half of the patients had initiated steroids prior to their first clinic visit at CCHMC, and the proportion doing so differed by steroid type (75% for prednisone and 48% for deflazacort); for these patients the average time between steroid initiation and first clinic visit was similar between steroid groups at 2.5 and 2.3 years, respectively. The overall average follow-up included in the time-to-event analyses was 11.2 years in the FMS analyses and 11.9 years in the scoliosis analyses. The follow-up time was similar across prednisone- and deflazacort-initiated patients (<6 months difference in mean follow-up time).
| PRED (N = 105) | DFZ (N = 330) | |
|---|---|---|
| Demographics and body size/composition | ||
| Age at first clinic visit at CCHMC (years): | 8.1 ± 3.1 | 6.5 ± 3.1 |
| – Median (IQR) | 7.9 (5.8–9.7) | 6.0 (4.5–8.0) |
| – Range | 0.3 – 19.5 | 0.2 – 25.3 |
| Age at first clinic visit at CCHMC with FMS (years) | 8.7 ± 3.3 | 7.1 ± 3.4 |
| Height (cm) | 125.4 ± 17.1 | 113.2 ± 15.4 |
| Weight (kg) | 33.0 ± 16.2 | 24.2 ± 11.1 |
| BMI (kg/m2) | 19.7 ± 4.5 | 18.1 ± 3.8 |
| % lean body mass (DEXA) | 64.1 ± 10.3 | 70.0 ± 9.0 |
| Steroid use | ||
| Age at steroid initiation (years) | 6.4 ± 2.5 | 5.7 ± 2.1 |
| Initiation prior to first clinic visit at CCHMC, n (%): | 79 (75.2) | 157 (47.6) |
| – Years from initiation to first clinic visit at CCHMC | 2.5 ± 2.3 | 2.3 ± 2.4 |
| Dosing frequency at first recorded steroid, n (%):‡ | ||
| – Daily | 69 (67.7%) | 310 (95.1%) |
| – Other | 33 (32.4%) | 16 (4.9%) |
| Switched steroid type during follow-up at CCHMC, n (%): | ||
| – Deflazacort → prednisone | – | 14 (4.2%) |
| – Prednisone → deflazacort | 44 (41.9%) | – |
| Calendar year of steroid initiation: | ||
| – 1993–2000 | 0 (0.0%) | 7 (2.1%) |
| – 2000–2008 | 42 (40.0%) | 142 (43.0%) |
| – 2009–2016 | 63 (60.0%) | 181 (54.9%) |
| Ambulatory function | ||
| NSAA total score | 17.8 ± 6.8 | 20.7 ± 6.4 |
| FMS | 2.5 ± 1.3 | 1.9 ± 1.0 |
| Timed sit-to-stand (s) | 4.7 ± 4.1 | 2.8 ± 2.0 |
| Timed 30-ft walk/run (s) | 5.8 ± 2.2 | 5.2 ± 2.1 |
| Timed 4-stair climb (s) | 3.6 ± 2.0 | 3.7 ± 2.8 |
| Pulmonary and cardiac function | ||
| FVC (l) | 2.1 ± 0.4 | 1.7 ± 0.5 |
| FVC %-predicted | 95.3 ± 21.8 | 99.6 ± 25.1 |
| LVEF % | 58.6 ± 7.7 | 61.2 ± 8.7 |
†
Patient characteristics are summarized at the time of the first clinic visit at CCHMC with either an FMS or scoliosis assessment recorded unless otherwise noted. Statistics reported are means ± standard deviations unless otherwise noted.
‡
Percentages calculated among the n = 102 and n = 326 patients with nonmissing dosing data for prednisone and deflazacort groups, respectively.
BMI: Body mass index; CCHMC: Cincinnati Children’s Hospital Medical Center; DEXA: Dual-energy x-ray absorptiometry; DFZ: Deflazacort; FMS: Functional mobility scale; FVC: Forced vital capacity; IQR: Interquartile range; LVEF: Left ventricular ejection fraction; NSAA: North Star Ambulatory Assessment; PRED: Prednisone; SD: Standard deviation.
At first clinic visit at CCHMC with functional data recorded, deflazacort-initiated patients were on average younger, shorter and weighed less, compared with prednisone-initiated patients (Table 1). The deflazacort-initiated group was also younger on average at steroid initiation compared with the prednisone-initiated group (5.7 vs 6.4 years, respectively). Across measures of ambulatory, pulmonary and cardiac function at the first clinic visit at CCHMC, deflazacort-treated patients tended to have better or similar function compared with prednisone-treated patients.
Analyses of ages at clinical events
During follow-up at CCHMC, 107 patients lost ambulation (FMS >4; deflazacort-initiated patients: 22.9% [73/319]; prednisone–initiated patients: 35.8% [34/95]) (Figure 1). Loss of ambulation occurred at significantly older ages for deflazacort-initiated patients; the median age at transition was 15.6 years in the deflazacort-initiated group and 13.5 years in the prednisone-initiated group (log-rank p < 0.01). By age 15 years, 56% of prednisone-initiated patients had lost ambulation, compared with 43.7% of deflazacort-initiated patients.

Figure 1. Age at loss of ambulation (functional mobility scale >4) by first recorded steroid type (Kaplan–Meier analysis).
FMS: Functional Mobility Scale.
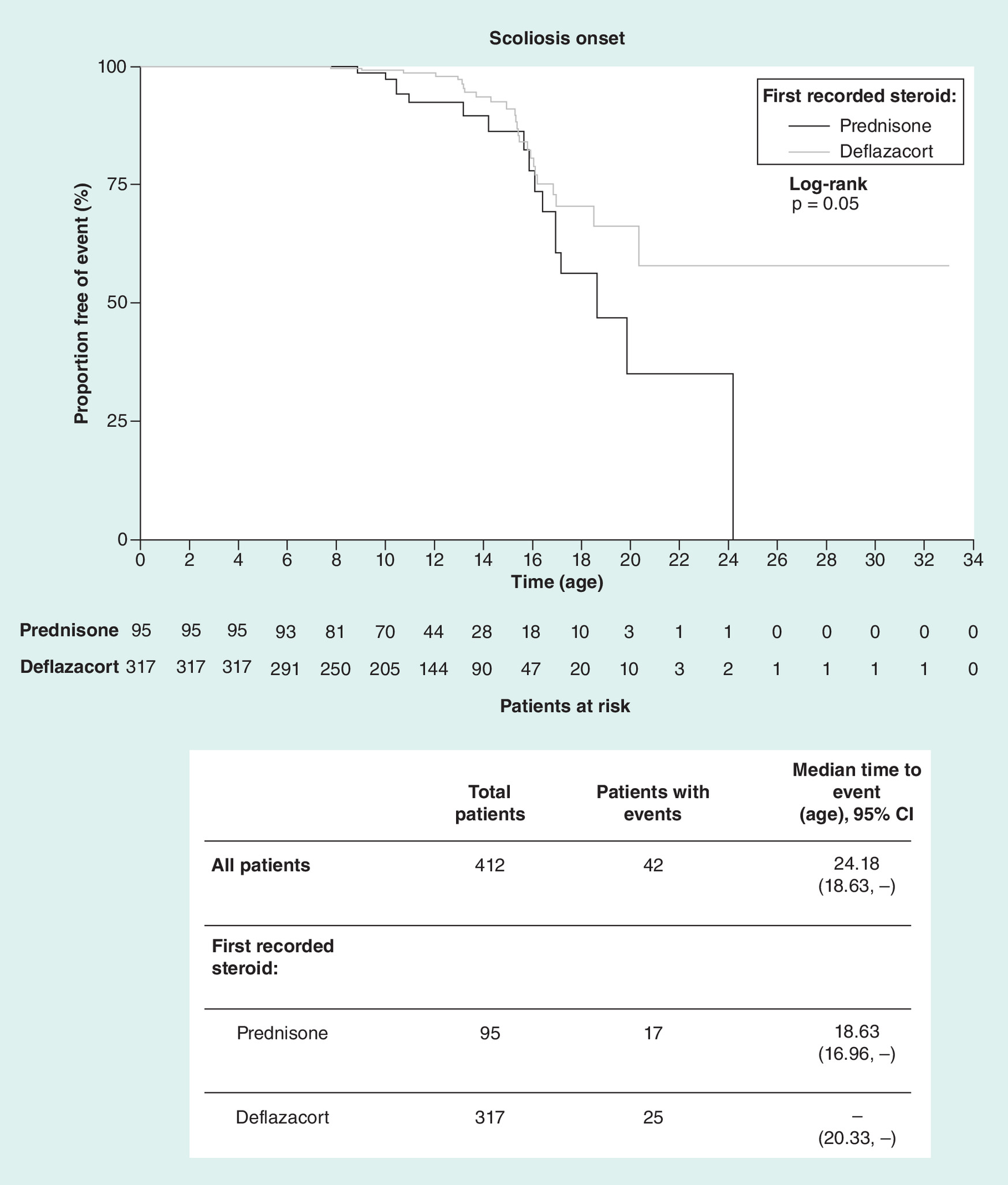
During follow-up at CCHMC, 42 patients developed scoliosis (deflazacort-initiated patients: 7.9% [25/317]; prednisone-initiated patients: 17.9% [17/95]) (Figure 2). Scoliosis occurred at significantly older ages for patients initiating deflazacort compared with prednisone; the median age was not reached in the deflazacort-initiated group, whereas the median age of scoliosis onset was 18.6 years in the prednisone-initiated group (log-rank test p = 0.05). Based on the Kaplan–Meier estimates, by age 15 years, 13.7% of prednisone-initiated patients and 8.9% of deflazacort-initiated patients had scoliosis.
These associations persisted in Cox proportional hazards analyses that adjusted for age at steroid initiation, year of steroid initiation and whether the patient had initiated steroids prior to or after their first clinic visit at CCHMC (Table 3). Relative to treatment with prednisone, treatment with deflazacort was associated with a reduction in the hazard of loss of ambulation by 53% and with a reduction in the hazard of scoliosis by 59%. Hazard ratios were similar in both the adjusted and unadjusted analyses. The age at loss of ambulation findings were robust to a sensitivity analysis that excluded the n = 11 patients who required orthotics or braces to walk at their first assessment (i.e., FMS = 4).
| Outcome †,‡ | Difference between DFZ (N = 330) vs PRED (reference group; N = 105) | 95% CI | p-value |
|---|---|---|---|
| 4SC (velocity) (stairs/seconds) | |||
| Unadjusted | 0.54 | (0.31–0.78) | <0.001§ |
| Adjusted | 0.63 | (0.37–0.88) | <0.001§ |
| 30-ft walk/run (velocity) (feet/seconds) | |||
| Unadjusted | 1.16 | (0.66–1.67) | <0.001§ |
| Adjusted | 1.35 | (0.82–1.87) | <0.001§ |
| Timed sit-to-stand (velocity) (1/seconds) | |||
| Unadjusted | 0.13 | (0.08–0.18) | <0.001§ |
| Adjusted | 0.13 | (0.08–0.17) | <0.001§ |
| NSAA (total score) | |||
| Unadjusted | 4.22 | (2.23–6.22) | <0.001§ |
| Adjusted | 4.65 | (2.63–6.68) | <0.001§ |
| FVC %-predicted (%) | |||
| Unadjusted | 14.74 | (7.55–21.92) | <0.001§ |
| Adjusted | 9.24 | (3.06–15.41) | <0.01§ |
| LVEF (%) | |||
| Unadjusted | 1.69 | (-0.86–4.24) | 0.19 |
| Adjusted | 0.87 | (-1.58–3.32) | 0.49 |
| Height (cm) | |||
| Unadjusted | -12.84 | (-18.18 to -7.50) | <0.001§ |
| Adjusted | -5.96 | (-8.41 to -3.51) | <0.001§ |
| Total body mass (kg) | |||
| Unadjusted | -12.31 | (-17.14 to -7.47) | <0.001§ |
| Adjusted | -6.67 | (-10.21 to -3.13) | <0.001§ |
| % Lean body mass (%) | |||
| Unadjusted | 7.22 | (4.57–9.87) | <0.001§ |
| Adjusted | 4.52 | (2.41–6.64) | <0.001§ |
| % Body fat (%) | |||
| Unadjusted | -7.56 | (-10.37 to -4.75) | <0.001§ |
| Adjusted | -4.73 | (-6.97 to -2.50) | <0.001§ |
| Whole body BMD (g/cm2) | |||
| Unadjusted | -0.03 | (-0.05 to -0.01) | <0.001§ |
| Adjusted | -0.00 | (-0.02–0.01) | 0.76 |
†
Multivariable regressions adjusted for age at visit, visit year, steroid duration, an interaction term between age and steroid duration, and initiation of steroids prior to first clinic visit at Cincinnati Children’s Hospital Medical Center.
‡
For both the unadjusted and adjusted analyses, the reported values reflect the results for deflazacort versus prednisone (reference group) on the outcome of interest. Patients who switched steroids were not included in this analysis.
§
Denotes statistical significance.
4SC: 4-Stair climb; BMD: Bone mineral density; DFZ: Deflazacort; FVC: Forced vital capacity; LVEF: Left ventricular ejection fraction; NSAA: North Star Ambulatory Assessment; PRED: Prednisone.
| Outcome †,‡ | Hazard ratio for DFZ (N = 330) vs PRED (N = 105) | 95% CI | p-value |
|---|---|---|---|
| Loss of ambulation (FMS >4) | |||
| Unadjusted | 0.55 | (0.36–0.83) | <0.01§ |
| Adjusted | 0.47 | (0.30–0.74) | <0.01§ |
| Scoliosis onset | |||
| Unadjusted | 0.54 | (0.29–1.01) | 0.05 |
| Adjusted | 0.41 | (0.21–0.82) | <0.05§ |
†
Adjusted for age at steroid initiation, year at steroid initiation and whether the patient had initiated steroids prior to or after their first clinic visit at Cincinnati Children’s Hospital Medical Center.
‡
For both the unadjusted and adjusted analyses, the reported values reflect the results for deflazacort versus prednisone (reference group) on the outcome of interest.
§
Denotes statistical significance.
DFZ: Deflazacort; FMS: Functional Mobility Scale; PRED: Prednisone.
In sensitivity analyses with dosing frequency data available, comparisons between deflazacort (95% daily) and separated groups receiving daily versus other regimens of prednisone yielded findings consistent with those of the main analyses for ages at loss of ambulation and scoliosis (Supplementary Table 1).
In the separate sensitivity analyses among patients with switching data available, there were n = 44 patients initiated on prednisone who switched to deflazacort (42% out of 105) and n = 14 who initiated on deflazacort and switched to prednisone (4.2% out of 330). Among the subset of switchers from prednisone to deflazacort with duration data available (about 28% of the n = 44), the average duration on prednisone was 3.1 years and the average subsequent duration on deflazacort was 2.5 years. Times to scoliosis and loss of ambulation among prednisone-to-deflazacort switchers were numerically prolonged compared with patients continuing on prednisone, but shorter compared with patients initiated with deflazacort (Supplementary Table 2). Initiation with deflazacort was associated with a reduction in the hazard of loss of ambulation by 64% relative to being treated with prednisone only. Switching from prednisone to deflazacort was numerically associated with a reduction in the hazard of loss of ambulation by 51% relative to being treated with prednisone only. Similarly, initiation with deflazacort was associated with a reduction in the hazard of incurring the onset of scoliosis by 61%, and switching from prednisone to deflazacort was numerically associated with a reduction in the hazard of incurring scoliosis by 13%, relative to being treated with prednisone only.
Analyses of average outcomes across clinic visits
When analyzing associations between steroid type and outcomes across all clinic visits, the sample sizes varied according to the assessment frequency of each outcome as follows: 4SC velocity: 1519 total observations from 285 patients; 30-ft walk/run velocity: 1794 observations from 303 patients; timed sit-to-stand velocity: 1651 observations from 294 patients; NSAA: 1400 total observations from 294 patients; FVC %-predicted: 1193 total observations from 256 patients; LVEF %: 687 total observations from 225 patients; total body mass: 1886 total observations from 314 patients; height: 2237 total observations from 326 patients; % lean body mass and % body fat: 1886 total observations from 314 patients; and whole body BMD: 1886 total observations from 314 patients. On average, patients had clinical visits spanning 4.9 years, with a mean of seven visits per patient. Across all visits used in cross-sectional analyses, patients had a median age of 9.9 years (interquartile range: 7.4–12.9 years). The median age across all visits was higher in the prednisone group (11.3 years) compared with the deflazacort group (9.6 years).
Cross-sectional analyses
Cross-sectional associations between steroid type and patient status across all clinic visits (unadjusted and adjusted) are summarized in Table 2. After adjusting for age at the clinic visit, steroid duration as of the visit, the calendar year of the visit, and whether the patient had initiated steroids prior to or after their first clinic visit at CCHMC in a regression analysis as well as the interaction between age at clinic visit and steroid duration, patients treated with deflazacort, on average, exhibited a significantly greater 4SC velocity compared with patients treated with prednisone (by 0.63 stairs/s) across all clinic visits at which this assessment was conducted (p < 0.001). On average in these adjusted analyses, across all clinic visits with assessments recorded, patients treated with deflazacort also had a greater 30-ft walk/run velocity (by 1.35 feet/s), a greater timed sit-to-stand velocity (by 0.13 1/s), a higher NSAA total score (by 4.7 points), a higher FVC %-predicted (by 9.2 percentage points), a higher % lean body mass (by 4.5 percentage points) and a lower % body fat (by 4.7 percentage points) compared with patients treated with prednisone (all p < 0.05). Patients treated with deflazacort also had a lower mean total body mass (by 6.7 kg) and were shorter on average (by 6.0 cm) compared with patients treated with prednisone (all p < 0.05). Similar results were observed when regression analyses for height and FVC %-predicted were additionally adjusted for the type of height assessment (e.g., standing, wingspan, segmental measurements). No significant differences between steroid types were observed across assessments for LVEF % or whole body BMD.
Discussion
This retrospective analysis of real-world data from a single, large DMD care center identified associations between the use of deflazacort and greater preservation of ambulatory and pulmonary function, and prolonged time to loss of ambulation and scoliosis, compared with the use of prednisone. Deflazacort was also associated with shorter stature, lower total bodyweight and greater % lean body mass.
Loss of ambulation represents a clinically meaningful milestone in DMD progression [9,11,20]. The results of the present study align with prior evidence associating deflazacort with delayed loss of ambulation [9,20–22]. For example, in a 2006 study conducted among 74 boys (ages 10–18 years) with DMD, patients treated with deflazacort (mean treatment duration 5.5 years) were able to rise from supine to standing, climb stairs and walk 10 meters without assistance for 3–5 years longer than those in a placebo group [22]. A 2015 study utilizing the Cooperative International Neuromuscular Research Group (CINRG) natural history database also associated deflazacort with delayed loss of ambulation; participants who received deflazacort treatment for ≥1 year had a median 3-year longer delay in loss of ambulation compared with those receiving prednisone (p < 0.001) [9]. Similarly, results of a 2018 study utilizing the CINRG database found that long-term treatment with deflazacort was associated with an increase in the median ages at the loss of ambulation by approximately 2 years compared with patients treated with prednisone [20]. Our finding of a near similar 2-year delay in the time to loss of ambulation with deflazacort compared with prednisone treatment in a single large care center, with homogenous care recommendations across patients, supports the prior finding, based on a global multi-center study, of a better motor outcome with deflazacort treatment compared with prednisone/prednisolone treatment.
Scoliosis is an important comorbidity of DMD that is closely associated with muscle weakness and loss of ambulation [23–25]. The consequences of scoliosis are significant, and complications associated with surgery to correct spinal deformities can further exacerbate the disease burden in DMD [23]. The lower risk of scoliosis observed among patients receiving deflazacort compared with prednisone in the current study is clinically meaningful, and concordant with the greater preservation of ambulatory function observed among the deflazacort-treated patients.
While there were only a small number of patients switching from prednisone to deflazacort in the present study, this group exhibited hazards of loss of ambulation and scoliosis that were numerically intermediate relative to patients who consistently received prednisone (highest risk) and those who initiated deflazacort (lowest risk).
In addition to studying ages at clinical events, our study assessed differences between deflazacort- and prednisone-treated patients across all clinic visits. Differences in ambulatory function across visits reached magnitudes deemed clinically meaningful in prior research [26–28]. For example, a previous study reported that a difference of 2–4 points in the NSAA total score and a difference of 0.3–0.6 stairs/s in 4SC velocity represent clinically meaningful differences [28]. Across clinic visits, the present study found numerically higher performance on NSAA (by 4.6 points) and 4SC velocity (by 0.59 stairs/s) associated with deflazacort compared with prednisone use, after accounting for the patient’s age and duration of steroid treatment at the clinic visit.
The lower weight and shorter height among patients treated with deflazacort versus prednisone in the present study replicate well-known associations for these treatments [14,29,30]. Underlying these changes in overall body size, deflazacort was associated with a more favorable body composition compared with prednisone in the present study, with higher % lean body mass and lower % body fat. As lean mass largely reflects muscle mass [31], the higher levels of % lean body mass observed among patients using deflazacort versus prednisone align with the observed differences in ambulatory function between the two treatment groups.
This study found no evidence of a difference in whole body BMD between deflazacort- and prednisone-treated patients. This was surprising given that a previous study has associated daily deflazacort with an annualized fracture risk of 1367 per 10,000 person years, an almost twofold higher risk compared with daily prednisone [32]. Fracture data were not available for the current study, and further investigation of this outcome is needed. Other adverse effects of steroids that were not available in the present database but warrant further study include Cushingoid appearance, insulin resistance and behavioral changes.
Declines in respiratory function due to progressive muscle weakening are a significant contributor to the morbidity and mortality in DMD [33]. Patients receiving deflazacort in the present study had, on average, better pulmonary function with higher FVC %-predicted compared with patients receiving prednisone. The higher %-predicted values for deflazacort-treated patients versus prednisone/prednisolone-treated patients may be related to the shorter stature of deflazacort-treated patients since height is the denominator for calculating FVC %-predicted FVC. Greater preservation of pulmonary function with deflazacort was also observed in the aforementioned 2018 study utilizing the CINRG database, which estimated a delay in median age at FVC <1L by approximately 2 years compared with treatment with prednisone [20].
Cardiac disease is the primary cause of mortality in over 20% of patients with DMD due to the dystrophin gene defect causing an absence of the muscle cytoskeletal protein dystrophin and leading to cardiac muscle disease [34–36]. This study found no evidence of a difference in LVEF % between patients treated with deflazacort or prednisone. Patients in both the deflazacort and prednisone groups had an average LVEF % of over 55% (59 and 58%, respectively), indicating that LVEF % was preserved during the majority of follow-up.
Limitations
The principal limitation of this study is that steroid use was not randomized as in a clinical trial. Therefore, differences in outcomes between steroid groups could be confounded by factors that differ between these groups. Some of these factors could be accounted for in our analyses via regression adjustment. For example, the younger average age at steroid initiation for deflazacort-treated patients could impact outcomes, but was accounted for by adjusting for age at steroid initiation. It could also be hypothesized that differences in care received prior to CCHMC, including potential differences in steroid dosing or supportive care, could have impacted outcomes. Indeed, a higher proportion of patients initiating prednisone did so prior to CCHMC compared with those initiating deflazacort. For this reason, our analyses adjusted for whether or not steroids were initiated prior to the first clinic visit at CCHMC, among other factors. However, despite these adjustments for observed differences between groups, it is possible that unobserved differences are present. In particular, it was not possible to identify the extent to which potential differences in socioeconomic status (SES) may have affected the results. Cost has been a factor for most families at CCHMC who opt for prednisone instead of out-of-pocket, imported deflazacort. Prednisone is also cheaper in other countries. Generally, families at CCHMC with higher SES tend to have better adherence to care plans. For example, care plans may include recommendations for self- or family-administered physiotherapy such as stretching, night brace usage and nutritional/weight management; adherence to these recommendations could be impacted by SES through differences in self-efficacy, social support, or anxiety/depression [37,38].
The impact of different dosing regimens is a plausible contributor to the differences in outcomes observed in the present study between patients receiving prednisone and deflazacort. In particular, the impact of excessive weight gain with prednisone/prednisolone [14] could have resulted in lower tolerated doses of prednisone/prednisolone as in the CINRG cohort (cumulative dose of daily prednisone patients was 1729 mg or equivalent deflazacort dose of 2075 mg vs cumulative dose of 2922 mg) [20]. In this way, differences in functional outcomes and scoliosis risk could be explained by better tolerability of deflazacort to enable more optimal dosing of recommended 0.9 mg/kg/day as opposed to a lower dose of prednisone due to its side effect of excessive weight gain. Indeed, a randomized trial of fixed daily doses of prednisone (0.75 mg/kg/day) and deflazacort (0.9 mg/kg/day) identified no significant differences in motor function, but substantially greater weight gain with prednisone [14]. While sensitivity analyses separating out daily and other regimens of prednisone identified results consistent with those of the main analyses, our study is limited by the lack of data on cumulative or time-varying doses of deflazacort and prednisone. It was not possible to compare dose-adjusted outcomes. Rather, the outcomes observed in the present study represent those associated with real-world, individualized dosing for each steroid type at CCHMC. Beyond differences in dosing, other potential differences between deflazacort and prednisone, including greater reduction of interferon gamma levels [39] and potential immunomodulatory effects [39–42], or lower protein binding and nonaffinity for transcortin and potential impacts on bioavailability in muscle fibers [43–46], could be speculated to impact functional outcomes, but were not investigated in the present study.
As a study of real-world data captured in clinical practice, there are also limitations stemming from the data collection process. In particular, ambulatory test results were not available from patients who were unable or unwilling to complete the assessments. Thus, the cross-sectional analyses of ambulatory function represent differences among patients who completed those tests.
Conclusion
This study of real-world data adds to the evidence from other observational studies associating the use of deflazacort with greater preservation of motor and pulmonary function relative to the use of prednisone, and further indicates concurrent preservation of lean body mass and delay of scoliosis.
•
The corticosteroids prednisone and deflazacort represent the standard of care in Duchenne muscular dystrophy (DMD), and real-world evidence is needed to fully characterize their effectiveness.
•
This retrospective cohort study analyzed clinical outcomes (ambulatory, pulmonary, cardiac, bone-health) of 435 patients with DMD from Cincinnati Children’s Hospital Medical Center who received deflazacort only (∼95% daily regimen), prednisone only (∼68% daily regimen), or were switched from prednisone to deflazacort.
•
Treatment with deflazacort was associated with a significant delay in loss of ambulation relative to treatment with prednisone (15.6 vs 13.5 years).
•
The onset of scoliosis was significantly delayed among patients treated with deflazacort (median age of onset not reached) versus prednisone (median age of onset: 18.6 years).
•
On average across clinic visits, and after accounting for current age, duration of steroid treatment, whether the patient had initiated steroids prior to or after their first CCHMC clinic visit, and current visit year, deflazacort-treated patients experienced significantly greater 4-stair climb velocity, 30-ft walk/run velocity, timed sit-to-stand velocity, greater North Star Ambulatory Assessment total score, greater forced vital capacity %-predicted, greater % lean body mass and a greater % body fat compared with patients treated with prednisone. Patients treated with deflazacort also had a lower mean total body mass and were shorter, on average, compared with patients treated with prednisone.
•
No significant differences in whole body bone mineral density or left ventricular ejection fraction were observed among treatment groups.
•
Patients who switched from prednisone to deflazacort experienced a numerically greater delay in their loss of function compared with patients treated with prednisone only, but less of a delay compared with those who were treated with deflazacort.
•
Overall these findings suggest that, with real-world steroid dosing, slower functional decline is associated with deflazacort treatment compared with prednisone. Studies with randomized steroid assignment are necessary to assess treatment effects without confounding by socioeconomic status or other factors, and to identify and compare optimal dosing.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
JR Marden: data analysis and interpretation of results; manuscript writing and editing. J Freimark: data analysis and interpretation of results; manuscript writing and editing. Z Yao: data analysis and interpretation of results; manuscript writing and editing. J Signorovitch: study design; data analysis and interpretation of results; manuscript writing and editing. C Tian: data curation; study design; interpretation of results; manuscript writing and editing. BL Wong: data curation; study design; interpretation of results; manuscript writing and editing.
Acknowledgments
The authors are grateful to the patients for providing informed consent to participate in the Neuromuscular Clinic registry of clinical data to enable outcomes research like this study. We are grateful to members of the Collaborative Trajectory Analysis Project (cTAP) for contributions to the interpretation of this research.
J Bange, systems analyst at Cincinnati Children’s Hospital Medical Center (CCHMC), helped with data curation; and R Hu, research manager and coordinator of the CCHMC study, contributed to data collection and management. We also thank C Santos from PTC Therapeutics, Inc. for providing input on study design.
Financial & competing interests disclosure
This study was facilitated by cTAP with funding from PTC. cTAP is a pre-competitive coalition of academic clinicians, drug developers and patient foundations formed in 2015 to overcome challenges affecting clinical trials in DMD. cTAP has received sponsorship from Astellas Pharma (Mitobridge), BioMarin, Biophytis, Bristol-Myers Squibb, Catabasis, FibroGen, Inc., Italfarmaco SpA, Marathon Pharmaceuticals, Pfizer, Inc., PTC Therapeutics, Roche, Sarepta Therapeutics, Shire plc, Solid Biosciences, Summit Plc., Wave Life Sciences, Parent Project Muscular Dystrophy, Charley’s Fund and CureDuchenne, a founding patient advocacy partner and provider of initial seed funding to cTAP.
JR Marden, J Freimark, Z Yao and J Signorovitch are employees of Analysis Group, Inc., a consulting firm that received funding from PTC Therapeutics to conduct this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by Gloria DeWalt, PhD, and Shelley Batts, PhD, employees of Analysis Group, Inc. Support for this assistance was provided by PTC Therapeutics.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all experimental investigations. In addition, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary_materials.docx)
- Download
- 15.41 KB
References
Papers of special note have been highlighted as: • of interest •• of considerable interest
1.
Genetic and Rare Diseases Information Center. Duchenne muscular dystrophy. https://rarediseases.info.nih.gov/diseases/6291/duchenne-muscular-dystrophy
2.
National Organization for Rare Disorders. Duchenne muscular dystrophy. https://rarediseases.org/rare-diseases/duchenne-muscular-dystrophy/
3.
Emery AE, Muntoni F, Quinlivan RC. Duchenne Muscular Systrophy. Oxford University Press, Oxford, UK (2015).
4.
Birnkrant DJ, Bushby K, Bann CM et al. Diagnosis and management of Duchenne muscular dystrophy, part 2: respiratory, cardiac, bone health, and orthopaedic management. Lancet Neurol. 17(4), 347–361 (2018).
5.
Ishikawa Y, Miura T, Ishikawa Y et al. Duchenne muscular dystrophy: survival by cardio-respiratory interventions. Neuromuscul. Disord. 21(1), 47–51 (2011).
6.
Lomauro A, D’Angelo MG, Aliverti A. Assessment and management of respiratory function in patients with Duchenne muscular dystrophy: current and emerging options. Ther. Clin. Risk. Manag. 11, 1475–1488 (2015).
7.
Morgenroth VH, Hache LP, Clemens PR. Insights into bone health in Duchenne muscular dystrophy. Bonekey Rep. 1, 9 (2012).
8.
Pandya S, James KA, Westfield C et al. Health profile of a cohort of adults with Duchenne muscular dystrophy. Muscle Nerve 58(2), 219–223 (2018).
9.
Bello L, Gordish-Dressman H, Morgenroth LP et al. Prednisone/prednisolone and deflazacort regimens in the CINRG Duchenne Natural History Study. Neurology 85(12), 1048–1055 (2015).
•• Real-world, observational study that provided class 4 evidence regarding the efficacy of prednisone and deflazacort in delaying the loss of ambulation in patients with Duchenne muscular dystrophy (DMD).
10.
Mcdonald CM, Gordish-Dressman H, Henricson EK et al. Longitudinal pulmonary function testing outcome measures in Duchenne muscular dystrophy: long-term natural history with and without glucocorticoids. Neuromuscul. Disord. 28(11), 897–909 (2018).
•• Longitudinal study that compared changes in pulmonary function (10 years follow-up) among patients with DMD who received glucocorticoid treatment (daily prednisone, daily deflazacort, alternative regimens) versus untreated patients with DMD.
11.
Mcdonald CM, Henricson EK, Abresch RT et al. The cooperative international neuromuscular research group Duchenne natural history study--a longitudinal investigation in the era of glucocorticoid therapy: design of protocol and the methods used. Muscle Nerve 48(1), 32–54 (2013).
12.
Buckner JL, Bowden SA, Mahan JD. Optimizing bone health in Duchenne muscular dystrophy. Int. J. Endocrinol. 2015, 928385 (2015).
13.
Hawker GA, Ridout R, Harris VA, Chase CC, Fielding LJ, Biggar WD. Alendronate in the treatment of low bone mass in steroid-treated boys with Duchennes muscular dystrophy. Arch. Phys. Med. Rehabil. 86(2), 284–288 (2005).
14.
Bonifati MD, Ruzza G, Bonometto P et al. A multicenter, double-blind, randomized trial of deflazacort versus prednisone in Duchenne muscular dystrophy. Muscle Nerve 23(9), 1344–1347 (2000).
15.
Griggs RC, Miller JP, Greenberg CR et al. Efficacy and safety of deflazacort vs prednisone and placebo for Duchenne muscular dystrophy. Neurology 87(20), 2123–2131 (2016).
16.
Cunniff T, Wanaski S, Dubow J, Meyer J. Effect of deflazacort and prednisone versus placebo on muscle strength in boys with Duchenne muscular dystrophy who have lost ambulation: results from the Deflazacort Clinical Trial Program (S28.006). Neurology 86(Suppl. 16), S28.006 (2016).
17.
Shieh PB, Mcintosh J, Jin F et al. Deflazacort versus prednisone/prednisolone for maintaining motor function and delaying loss of ambulation: a post hoc analysis from the ACT DMD trial. Muscle Nerve 58(5), 639–645 (2018).
•• A post-hoc analysis that assessed clinical outcomes from the placebo arm (prednisone/prednisolone and deflazacort) of a 48-week Phase III trial.
18.
Mcdonald CM, Sajeev G, Yao Z et al. Deflazacort vs prednisone treatment for Duchenne muscular dystrophy: a meta-analysis of disease progression rates in recent multicenter clinical trials. Muscle Nerve (2019).
19.
Wong BL, Rybalsky I, Shellenbarger KC et al. Long-term outcome of interdisciplinary management of patients with Duchenne muscular dystrophy receiving daily glucocorticoid treatment. J. Pediatr. 182, 296–303 (2017).
• Real-world, retrospective study that evaluated clinical outcomes and side effects associated with daily glucocorticoid treatment (deflazacort or prednisone) among patients with DMD (ages 10 to <16 years for a mean of 8.5 years).
20.
Mcdonald CM, Henricson EK, Abresch RT et al. Long-term effects of glucocorticoids on function, quality of life, and survival in patients with Duchenne muscular dystrophy: a prospective cohort study. Lancet 391(10119), 451–461 (2018).
•• Longitudinal, prospective, cohort study that examined functional outcomes of patients with DMD (ages 2–28 years for 10 years) who were treated with glucocorticoids (prednisone/prednisolone or deflazacort) versus untreated patients with DMD.
21.
Bach JR, Martinez D, Saulat B. Duchenne muscular dystrophy: the effect of glucocorticoids on ventilator use and ambulation. Am. J. Phys. Med. Rehabil. 89(8), 620–624 (2010).
22.
Biggar WD, Harris VA, Eliasoph L, Alman B. Long-term benefits of deflazacort treatment for boys with Duchenne muscular dystrophy in their second decade. Neuromuscul. Disord. 16(4), 249–255 (2006).
23.
Archer JE, Gardner AC, Roper HP, Chikermane AA, Tatman AJ. Duchenne muscular dystrophy: the management of scoliosis. J. Spine Surg. 2(3), 185–194 (2016).
24.
Alman BA, Raza SN, Biggar WD. Steroid treatment and the development of scoliosis in males with duchenne muscular dystrophy. J. Bone Joint Surg. Am. 86(3), 519–524 (2004).
25.
Lebel DE, Corston JA, McAdam LC, Biggar WD, Alman BA. Glucocorticoid treatment for the prevention of scoliosis in children with Duchenne muscular dystrophy: long-term follow-up. J. Bone Joint Surg. Am. 95(12), 1057–1061 (2013).
26.
Mcdonald CM, Henricson EK, Abresch RT et al. The 6-minute walk test and other endpoints in Duchenne muscular dystrophy: longitudinal natural history observations over 48 weeks from a multicenter study. Muscle Nerve 48(3), 343–356 (2013).
27.
Mayhew AG, Cano SJ, Scott E et al. Detecting meaningful change using the North Star Ambulatory Assessment in Duchenne muscular dystrophy. Dev. Med. Child Neurol. 55(11), 1046–1052 (2013).
28.
Wong B, Signorovitch J, Staunton H et al. Estimating clinically meaningful 48-week change thresholds in the north star ambulatory assessment and four-stair climb in Duchenne muscular dystophy. Presented at: Action Duchenne International Conference. Birmingham, UK (2018).
29.
Moxley RT 3rd, Pandya S, Ciafaloni E, Fox DJ, Campbell K. Change in natural history of Duchenne muscular dystrophy with long-term corticosteroid treatment: implications for management. J. Child Neurol. 25(9), 1116–1129 (2010).
• Highlights studies that documented the clinical effects associated with long-term (>3 years) corticosteroid treatment in patients with DMD.
30.
Mcadam LC, Mayo AL, Alman BA, Biggar WD. The Canadian experience with long-term deflazacort treatment in Duchenne muscular dystrophy. Acta Myol. 31(1), 16–20 (2012).
31.
Palmieri GM, Bertorini TE, Griffin JW, Igarashi M, Karas JG. Assessment of whole body composition with dual energy x-ray absorptiometry in Duchenne muscular dystrophy: correlation of lean body mass with muscle function. Muscle Nerve 19(6), 777–779 (1996).
32.
Joseph S, Wang C, Bushby K et al. Fractures and linear growth in a nationwide cohort of boys with Duchenne muscular dystrophy with and without glucocorticoid treatment: results from the UK NorthStar Database. JAMA Neurol. 76(6), 701–709 (2019).
33.
Roberto R, Fritz A, Hagar Y et al. The natural history of cardiac and pulmonary function decline in patients with duchenne muscular dystrophy. Spine (Phila Pa 1976) 36(15), E1009–E1017 (2011).
34.
Hoffman EP, Brown RH Jr, Kunkel LM. Dystrophin: the protein product of the Duchenne muscular dystrophy locus. Cell 51(6), 919–928 (1987).
35.
Eagle M, Baudouin SV, Chandler C, Giddings DR, Bullock R, Bushby K. Survival in Duchenne muscular dystrophy: improvements in life expectancy since 1967 and the impact of home nocturnal ventilation. Neuromuscul. Disord. 12(10), 926–929 (2002).
36.
Spurney C, Shimizu R, Morgenroth LP et al. Cooperative International Neuromuscular Research Group Duchenne Natural History Study demonstrates insufficient diagnosis and treatment of cardiomyopathy in Duchenne muscular dystrophy. Muscle Nerve 50(2), 250–256 (2014).
37.
Berkman LF, Glass T. Social integration, social networks, social support, and health. Social Epidemiol. 1, 137–173 (2000).
38.
Jack K, Mclean SM, Moffett JK, Gardiner E. Barriers to treatment adherence in physiotherapy outpatient clinics: a systematic review. Man. Ther. 15(3), 220–228 (2010).
39.
Flanigan KM, Campbell K, Viollet L et al. Anti-dystrophin T cell responses in Duchenne muscular dystrophy: prevalence and a glucocorticoid treatment effect. Hum. Gene Ther. 24(9), 797–806 (2013).
40.
Liu T, Zhang L, Joo D, Sun SC. NF-kappaB signaling in inflammation. Signal Transduct. Target Ther. 2, pii: 17023 (2017).
41.
Thapa RJ, Basagoudanavar SH, Nogusa S et al. NF-kappaB protects cells from gamma interferon-induced RIP1-dependent necroptosis. Mol. Cell. Biol. 31(14), 2934–2946 (2011).
42.
Wesemann DR, Benveniste EN. STAT-1 alpha and IFN-gamma as modulators of TNF-alpha signaling in macrophages: regulation and functional implications of the TNF receptor 1:STAT-1 alpha complex. J. Immunol. 171(10), 5313–5319 (2003).
43.
Nayak S, Acharjya B. Deflazacort versus other glucocorticoids: a comparison. Indian J. Dermatol. 53(4), 167–170 (2008).
44.
Assandri A, Buniva G, Martinelli E, Perazzi A, Zerilli L. Pharmacokinetics and metabolism of deflazacort in the rat, dog, monkey and man. Adv. Exp. Med. Biol. 171, 9–23 (1984).
45.
Bashar T, Apu MNH, Mostaid MS, Islam MS, Hasnat A. Pharmacokinetics and bioavailability study of a prednisolone tablet as a single oral dose in Bangladeshi healthy volunteers. Dose Response 16(3), 1559325818783932 (2018).
46.
Burakiewicz J, Sinclair CDJ, Fischer D, Walter GA, Kan HE, Hollingsworth KG. Quantifying fat replacement of muscle by quantitative MRI in muscular dystrophy. J. Neurol. 264(10), 2053–2067 (2017).
Information & Authors
Information
Published In
Pages: 177 - 189
PubMed: 31922454
Copyright
© 2020 Analysis Group, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 13 November 2019
Accepted: 16 December 2019
Published online: 10 January 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world outcomes of long-term prednisone and deflazacort use in patients with Duchenne muscular dystrophy: experience at a single, large care center. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0170
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Nadine A. Ikelaar, Louise S. M. Blok, Mees H. P. Stoop, Yvonne D. Krom, Julia Bongers, Petra Dibbets-Schneider, Erik W. van Zwet, Pieter Bas de Witte, Erik H. Niks, Effects of intermittent corticosteroids on scoliosis, bone density, and vertebral fractures in duchenne muscular dystrophy, Journal of Neuromuscular Diseases, 10.1177/22143602261472975, (2026).
- Craig M. McDonald, James Signorovitch, Nathalie Marie Goemans, Eugenio Mercuri, Heather Gordish-Dressman, Krista Vandenborne, Gautam Sajeev, Susan J. Ward, Mirko Fillbrunn, Molly Frean, Laurent Servais, Erik H. Niks, Volker Straub, Imelda J.M. De Groot, Francesco Muntoni, A Validated Prognostic Score for Time to Loss of Ambulation in Patients With Duchenne Muscular Dystrophy, Neurology, 10.1212/WNL.0000000000214705, 106, 12, (2026).
- Jae Hwa Bae, Soyoung Kwak, Emergency department visits among patients with neuromuscular diseases receiving home mechanical ventilation: a nationwide population-based study, Journal of Yeungnam Medical Science, 10.12701/jyms.2026.43.32, 43, (32), (2026).
- Xueqin Gao, Joseph J. Ruzbarsky, Matthieu Huard, S.Amir H. Sajedi, Peter T. Shyu, Zuokui Xiao, Britney S. Force, Sarah White, Jessica Ayers, Bing Wang, X. Edward Guo, Johnny Huard, Targeting cellular senescence in dystrophin-/-/utrophin-/-double knockout mice improves musculoskeletal health and increases lifespan, Pharmacological Research, 10.1016/j.phrs.2025.108016, 222, (108016), (2025).
- Jin Sun, Jie Tang, Lu Wei, Juan Geng, Rui Xiao, Niu Li, Shuyuan Li, Jian Wang, Qihua Fu, Ruen Yao, Tingting Yu, Integrated Genotyping Strategies for Uncovering Detailed Haplotype Structures and Characterization of DMD Duplications , Clinical Chemistry, 10.1093/clinchem/hvaf136, 72, 2, (291-302), (2025).
- Fatima I. Nakhusheva, Artem V. Serov, Oleg L. Lapochkin, The experience of treating patients with Duchenne myodystrophy caused by nonsense mutation, L.O. Badalyan Neurological Journal, 10.46563/2686-8997-2025-6-3-133-139, 6, 3, (133-139), (2025).
- Shiny Thomas, Tahereh Neyaz, Kristin M. Conway, Aida Soim, Paul A. Romitti, Carla Zingariello, Joshua R. Mann, Trends in Corticosteroid Use Among Males With Duchenne Muscular Dystrophy (DMD) During 2000-2015: Data From the MD STAR net , Journal of Child Neurology, 10.1177/08830738251367466, 41, 4, (505-519), (2025).
- D. V. Vlodavets, S. B. Artemyeva, E. V. Tozliyan, A. K. Shulchenko, Vamorolone – a corticosteroid approved by global regulators for the treatment of Duchenne muscular dystrophy. Literature review, Russian Journal of Child Neurology, 10.17650/2073-8803-2025-20-2-40-51, 20, 2, (40-51), (2025).
- Edna Julieth Bobadilla-Quesada, Manuel Huertas Quiñones, Juan David Lasprilla Tovar, Fernando Suárez Obando, Norma Carolina Barajas Viracachá, Paulo César Becerra Ortiz, Carlos Ernesto Bolaños Almeida, José Manuel Cañón Zambrano, Sandra Milena Castellar-Leones, Jenny Libeth Jurado Hernández, Isabel Londoño Ossa, Sergio Alejandro Nossa Almanza, Blair Ortiz Giraldo, Fernando Ortiz-Corredor, Sandra Yaneth Ospina Lagos, Juan Carlos Prieto, Carolina Rivera-Nieto, Edicson Ruiz Ospina, Felipe Ruiz-Botero, Maria Salcedo-Maldonado, Diana Pilar Soto Peña, Lina Marcela Tavera-Saldaña, María Julia Torres-Nieto, Diana Carolina Sánchez-Peñarete, Glucocorticoides y manejo cardíaco en pacientes con distrofia muscular de Duchenne, Revista Ciencias de la Salud, 10.12804/revistas.urosario.edu.co/revsalud/a.13926, 23, Especial, (1-13), (2025).
- Edna Julieth Bobadilla-Quesada, Juan David Lasprilla Tovar, Norma Carolina Barajas Viracachá, Paulo César Becerra Ortiz, Carlos Ernesto Bolaños Almeida, José Manuel Cañón Zambrano, Sandra Milena Castellar-Leones, Manuel Huertas Quiñones, Nicolas J. Laza Gutierrez, Isabel Londoño Ossa, Blair Ortiz Giraldo, Fernando Ortiz-Corredor, Sandra Yaneth Ospina Lagos, Juan Carlos Prieto, Carolina Rivera-Nieto, Edicson Ruiz Ospina, Felipe Ruiz-Botero, Maria Salcedo-Maldonado, Diana Pilar Soto Peña, Fernando Suárez-Obando, Lina Marcela Tavera-Saldaña, María Julia Torres-Nieto, Diana Carolina Sánchez-Peñarete, Uso de glucocorticoides en pacientes con distrofia muscular de Duchenne, Revista Ciencias de la Salud, 10.12804/revistas.urosario.edu.co/revsalud/a.13612, 23, Especial, (1-19), (2025).
- See more