Cost–effectiveness analysis of intravitreal aflibercept in the treatment of diabetic macular edema in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate the cost–effectiveness of intravitreal aflibercept compared with macular laser photocoagulation and ranibizumab for diabetic macular edema (DME) in China. Methods: A Markov model was developed to reflect the vision changes in DME patients. Parameters were estimated from VIVID-EAST trial data, published literature and physician surveys. Results: In a 20-year horizon, intravitreal aflibercept was associated with 7.825 quality-adjusted life years (QALYs) and 217,841 Chinese Yuan Renminbi (CNY), laser photocoagulation was associated with 7.189 QALYs and 135,489 CNY, and ranibizumab was associated with 7.462 QALYs and 222,477 CNY. The incremental cost–effectiveness ratios were 129,397 CNY/QALY and -12,774 CNY/QALY for intravitreal aflibercept versus laser photocoagulation and ranibizumab, respectively. Conclusion: Intravitreal aflibercept was considered as a cost-effective strategy for DME when compared with laser photocoagulation; it was considered as a dominant strategy when compared with ranibizumab.
Diabetic macular edema (DME) is a common microvascular complication of diabetes mellitus (DM) that develops in a subset of patients with diabetic retinopathy. It is characterized by vascular leakage, tissue edema and angiogenesis in the central retina [1,2], and it may have a sudden and debilitating impact on visual acuity (VA) [3]. DME is the leading cause of visual impairment and blindness among working-age individuals worldwide and in China [4–6].
China faces the world’s largest epidemic of DM, ranking at the top with 114.4 million of the total diabetic population in 2017; according to the survey conducted by the China CDC [7], DM prevalence reached 9.7% in the population above 18 years old in 2010. Among the diabetic population, approximately one in three have retinopathy [1], and the prevalence of diabetic retinopathy (DR) in China was reported as high as 34.08% in a recent large-scale, cross-sectional survey [8]. As DM and DR patients keep expanding and aging, more and more patients are living with the threat of vision impairment from DME. The age-standardized prevalence of DME in adult diabetic patients was 5% in China [4,5]. Untreated DME can cause progressive visual decline [9] and reduce the quality of life [10]. Moreover, diabetes patients with DME are associated with more healthcare resources consumption [10,11], and the medical costs of that are 29% higher than those for unaffected patients [11].
Before the advent of anti-VEGF medications, focal/grid laser coagulation was regarded as standard DME treatment for several decades, and its therapeutic value was demonstrated in the Early Treatment Diabetic Retinopathy Study (ETDRS) [12]. However, since 2010, intravitreal anti-VEGF agents, such as ranibizumab and intravitreal aflibercept, have demonstrated benefits to DME patients through a series of clinical trials and have shifted the treatment paradigms. Nowadays, anti-VEGF agents were recommended as the first-line treatment for DME by the European Association of Retinal Experts Guideline [13], the American Diabetes Association Guideline [14], the International Council of Ophthalmology Guideline for Diabetic Eye Care [15] and the Asian Ophthalmologists Collaboration Group [5].
Aflibercept is a recombined fusion protein that binds to all isoforms of VEGF-A, VEGF-B and PIGF, which may have a 100-fold higher binding affinity to VEGF-A than other anti-VEGF medications [16]. Based on the results of VISTADME and VIVIDDME studies [17], it was approved by the US FDA for the treatment of DME in 2015. In China, intravitreal aflibercept is the first anti-VEGF agent that was approved by National Medical Products Administration (formerly China’s FDA) for the treatment of DME, as it has demonstrated clinically meaningful superiority over macular laser photocoagulation for functional and anatomic end points in the Chinese population in the VIVID-EAST study (NCT01783886) [18].
Three treatment options are currently licensed for the treatment of visual impairment due to DME in China: macular laser photocoagulation, intravitreal aflibercept and ranibizumab. Each strategy is well studied in terms of clinical efficacy and safety, and the value for money issues are well discussed in international settings. However, to our knowledge, no studies address the cost–effectiveness of DME treatment in China.
For this reason, our study aims to conduct a cost–effectiveness analysis (CEA) to enable a comprehensive evaluation of the long-term economic benefits of intravitreal aflibercept compared with macular laser photocoagulation and ranibizumab in the treatment of DME from a Chinese societal perspective.
Methods
Model design
The Chinese societal perspective was adopted (accordingly) with both direct and indirect costs included. The time horizon for the base-case modeling was set at 20 years to reflect the lifetime benefit; life expectancy at birth for the Chinese population was 76.7 years in 2017 [19]. The intervention of interest was administered intravitreal aflibercept (Eylea®) 2 mg q8w (2 mg intravitreal aflibercept every 8 weeks after five initial monthly doses), and the comparators of interest included macular laser photocoagulation and ranibizumab 0.5 mg pro re nata (PRN) after three initial monthly doses. Macular laser photocoagulation (hereinafter referred to as ‘laser’) in this study refers to surgical procedures consisting of a high-energy light beam focused on the retinal tissue to be treated, and coagulation occurs when the energy is absorbed and converted by the retinal tissue into thermal energy. Ranibizumab 0.5 mg PRN is the recommended dosage and administration on the Chinese label and represents the current practice of ranibizumab in China. The outcome measure was quality-adjusted life years (QALYs). Consistent with Chinese pharmacoeconomic evaluation guidelines [20], both costs and utilities were discounted at 5% each year and tripled the Chinese gross domestic product per capita (¥178,980 in 2017) and was referenced as a willingness-to-pay threshold in this study according to common practice and WHO’s recommendation.
Three-phase model structure
A state transition Markov model was developed in Microsoft Excel 2007 to project the long-term outcomes of DME patients treated with intravitreal aflibercept, laser and ranibizumab. This economic model was originally developed for Health Technology Assessment Submissions to regulatory agencies in Europe, including the National Institute for Health and Care Excellence (NICE), subsequently, it was further adapted to fit China’s current situation in 2018. In this model, a three-phase approach based on the efficacy, maintenance and nonintervention phases was adopted (Figure 1). This approach had been validated by an experienced ophthalmologists and China’s clinical key opinion leaders (KOLs). The length of each phase followed the settings in the model submitted to NICE, and it was also validated by clinical KOLs to reflect the best consistency to the clinical practice in China. Year 1 as efficacy phase was consistent with treatment length in clinical trial VIVIDDME/VISTADME and also followed the Asian guideline for DME treatment [5].

Efficacy phase
The model started with the efficacy phase. In the model, it was assumed that after the initial efficacy phase (year 1) of an intensive treatment aiming to resolve macular edema, all visual gains could be observed. This was the only phase in which patient vision (measured by best-corrected-visual-acuity [BCVA]) may improve in response to treatment. All of the study eyes in the model received treatment during the efficacy phase. However, only a proportion of the fellow eyes involved were eligible to receive the assigned treatment, and they would follow the same pathway as the study eyes. The possible transitions for patients on treatment during the efficacy phase are shown in Figure 1.
Maintenance phase
In the subsequent maintenance phase (years 2–5), patients still received occasional injections to maintain VA. An assumption that there would be no vision gain or loss (transition probability was 0) in the maintenance phase was used in the model based on clinical expert consultations, which means patients would stay in the same status during the whole maintenance phase. Patient status at the end of the efficacy phase would represent the overall status of the maintenance phase. During the maintenance phase, patients may remain on the treatment they were receiving at the end of the efficacy phase and maintain vision, discontinue treatment or die. Patients who discontinued treatment would jump to nonintervention phase. In the base case, blind patients were not treated during the maintenance phase; therefore, the cost of treatments would not be applied.
Nonintervention phase
Finally, 5 years after treatment initiation, patients would enter the nonintervention phase, in which it was assumed that patients no longer received active treatment and their VA would slightly decrease as per the natural history of VA in aging patients. Any untreated eye affected by DME was assumed to lose vision at a monthly rate in line with natural progression. This assumption was demonstrated in a clinical study [9], and it was adopted in previously published CEA study [21] and the model submitted to NICE. The value used in the model was obtained from the ETDRS group and the Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR) [22]. To calculate the monthly probability of losing ten letters in the current model, the probability was normalized to 1 month and adjusted for the rate of improvement based upon WESDR/ETDRS data, given a 1% rate.
Model health states
Because the quality of life is a function of both eyes, model health states were defined by VA using a two-eye approach. At any given point in the model, both the study eye and nonstudy eye (fellow eye) fall into one of eight mutually exclusive VA health states, as defined by ETDRS letters read (Figure 1). As mentioned earlier, all of the study eyes received treatment during the efficacy phase, whereas only a portion of the fellow eyes involved were eligible to receive the assigned treatment. VA1 is the best health state, representing normal vision, and VA8 is the worst health state, representing blindness. A change in the vision of ten ETDRS letters (two lines of vision) or more was considered in the model, as it is a commonly used end point within ophthalmology clinical trials, including VIVID-EAST, where it is considered clinically significant. Health state ranges were therefore defined as 10-letter increments (with the exception of VA1) to be adequately sensitive to changes in vision associated with the treatment of DME. Therefore, the model featured a total of 65 health states: 64 for every combination of study eye and nonstudy eye, and one absorbing health state representing death.
Mortality
Background mortality rates were taken from the China national life tables [19]. However, clinical experts suggested that severe visual impairment was associated with a higher risk of mortality. Consequently, a relative risk of mortality associated with poor vision was also applied to patients who were blind in both eyes (e.g., health state VA8). According to a previous study [23], the hazard ratios of the total effect of visual impairment and severe visual impairment on mortality relative to no visual impairment are 1.23 (95% CI: 1.16–1.31) and 1.54 (95% CI: 1.26–1.86), respectively.
External clinical validation & physician surveys
An external validation by clinical experts was conducted via in-depth interviews of five KOLs from five tertiary hospitals in four cities in China: Peking University People’s Hospital; EYE & ENT Hospital of Fudan University; Center South University; AIER School of Ophthalmology, Beijing Union Medical College Hospital; and Eye Hospital, Wenzhou Medical University. The KOL interviews were aimed at better understanding of the disease background, validating the model framework and confirming key assumptions.
In addition, 15 ophthalmologists from 15 tertiary hospitals in 12 cities were enrolled to finish a questionnaire-based survey verifying literature review-identified data inputs and closing data gaps in terms of resource utilization and cost items. The 12 cities were Harbin, Shenyang, Beijing, Jinan, Taiyuan, Tianjin, Shanghai, Guangzhou, Hangzhou, Xi’an, Wuhan and Chengdu.
In total, 18 clinical experts from 18 different hospitals (from 14 cities) were involved in the interviews or surveys of this study, with all 18 sites being major, top-tier hospitals in the cities or provinces. These collected data inputs could fairly represent the situation in China, since the selected sites cover the majority of DME treatments in the country.
Model inputs
Clinical inputs
Baseline characteristics of patients
The baseline characteristics of patients entering the model were based on the information from all 301 Chinese patients in the VIVID-EAST trial. Hence, the baseline age was set at 57.6 years old and the proportion of females was 47.5%. At the beginning of the model, an initial distribution of VA was assumed and also obtained from the VIVID-EAST trial. The starting distribution of health states were 0.00% study eye and 3.65% fellow eye, 0.33% study eye and 21.93% fellow eye, 20.93% study eye and 37.21% fellow eye, 29.57% study eye and 22.26% fellow eye, 20.93% study eye and 7.64% fellow eye, 15.28% study eye and 5.32% fellow eye, 9.63% study eye and 1.99% fellow eye, 3.32% study eye and 0.00% fellow eye for VA1 (ETDRS letter 86–100), VA2 (ETDRS letter 76–85), VA3 (ETDRS letter 66–75), VA4 (ETDRS letter 56–65), VA5 (ETDRS letter 46–55), VA6 (ETDRS letter 36–45), VA7 (ETDRS letter 26–35), VA8 (ETDRS letter 0–25) state, respectively.
Fellow eye involvement
All fellow eyes (nonstudy eyes) were either at risk of DME or already affected by DME when patients entered the model. The proportion of fellow eye involvement at baseline was set at 63.7% according to a cross-sectional study conducted in China [24]. For patients without an affected fellow eye at baseline, an annual incidence rate was used to estimate the proportion of fellow eyes becoming affected with DME between model entry and year 4. The annual incidence of the fellow eye was set to 33% according to the incidence of DME in DM patients [25]. Also, all fellow eyes that were affected with DME were assumed to be treated. In the model, to minimize complexity, the BCVA in one eye evolved independently of the other.
Transition probabilities
The transition probabilities of intravitreal aflibercept and laser treatment were derived from individual patient-level data of the VIVID-EAST trial using multistate models (MSM) package in R [26] (Supplementary Table A). This package allows a general MSM to be fitted to longitudinal data to model transition intensities. In the VIVID-EAST trial, 37.4% of Chinese patients randomized to laser received intravitreal aflibercept as a rescue treatment, while less than 4% of Chinese patients in the intravitreal aflibercept group received laser as a rescue treatment. Due to the low incidence and cost of laser as a rescue treatment in aflibercept group, its impact on CEA results is very small and negligible. Therefore, in this case, only the transformation from the laser to intravitreal aflibercept was included in the model as a base-case consideration.
For ranibizumab, the transition probabilities were calculated based on the mean log odds ratios compared with intravitreal aflibercept using results from the most updated network meta-analysis (NMA) [27]. This study conducted a systematic review and identified 75 studies that satisfied the PICOS criteria, and 11 studies were included since they provided data that could inform the indirect analysis of interest; of these, four Phase III studies (VIVID-DME, VISTA-DME [17], RESTORE [28], REVEAL [29]) involved the intervention of laser and intravitreal aflibercept 2 mg q8w or ranibizumab 0.5 mg PRN.
In Korobelnik et al.’s study, indirect comparisons of the random and fixed effects of intravitreal aflibercept 2 mg q8w versus ranibizumab 0.5 mg PRN on 12-month visual outcomes using mixed treatment comparison (MTC) and Bucher analyses were reported, of which, the random effects using MTC analysis were selected as a base case in our study and others were tested in scenario analyses. The base-case mean log odds ratios of intravitreal aflibercept versus ranibizumab 0.5 mg PRN were -0.464 (random effects) for gaining 10–14 letters and -0.626 (random effects) for gaining ≥15 letters.
In order to avoid the probability of overestimating intravitreal aflibercept’s efficacy and to try to enable a more reliable cost–effectiveness conclusion, we assumed no difference in losing letters between intravitreal aflibercept-treated patients and ranibizumab-treated patients, and thus the mean log odds ratio of losing 10–14 letters and losing ≥15 letters of intravitreal aflibercept and ranibizumab were both assumed to be 0.000.
Resources use & cost inputs
Resources use per year per eye and the corresponding unit cost inputs are presented in Tables 1 & 2.
| Treatment | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | Source (year 1)† | Source (years 2–5)‡ |
|---|---|---|---|---|---|---|---|
| Intravitreal aflibercept group | |||||||
| Injections | 8.6 | 3.5 | 2.6 | 2.0 | 2.0 | A | a |
| Outpatient visits | 8.6 | 5.5 | 4.0 | 3.0 | 2.4 | A | a |
| Fundus photography tests | 8.6 | 5.5 | 4.0 | 3.0 | 2.4 | A | a |
| Eye tests | 8.6 | 5.5 | 4.0 | 3.0 | 2.4 | A | a |
| Optical coherence tomography test | 8.6 | 4.9 | 3.1 | 2.3 | 2.1 | A | a |
| Intraocular pressure tests | 8.6 | 5.5 | 4.0 | 3.0 | 2.4 | A | a |
| Fluorescein angiography tests | 8.6 | 1.7 | 1.6 | 1.3 | 1.4 | A | a |
| Slit lamp examination | 8.6 | 5.5 | 4.0 | 3.0 | 2.4 | A | a |
| Optometry tests | 8.6 | 5.5 | 4.0 | 3.0 | 2.4 | A | a |
| Indirect ophthalmoscopy tests | 8.6 | 5.5 | 4.0 | 3.0 | 2.4 | A | a |
| Laser group | |||||||
| Laser treatment | 2.4 | 0.3 | 0.3 | 0.1 | 0.1 | A | a |
| Intravitreal aflibercept injections as rescue treatment | 1.7 | 1.3 | 1.3 | 1.1 | 1.0 | A | a,b |
| Outpatient visits | 6.4 | 3.6 | 3.0 | 2.7 | 2.6 | A | a |
| Fundus photography tests | 6.4 | 3.6 | 3.0 | 2.7 | 2.6 | A | a |
| Eye tests | 6.4 | 3.6 | 3.0 | 2.7 | 2.6 | A | a |
| Optical coherence tomography test | 6.4 | 3.3 | 2.9 | 2.5 | 2.1 | A | a |
| Intraocular pressure tests | 6.4 | 3.3 | 3.0 | 2.7 | 2.6 | A | a |
| Fluorescein angiography tests | 6.4 | 0.8 | 1.2 | 0.8 | 0.9 | A | a |
| Slit lamp examination | 6.4 | 3.6 | 2.9 | 2.5 | 2.6 | A | a |
| Optometry tests | 6.4 | 3.6 | 2.9 | 2.5 | 2.6 | A | a |
| Indirect ophthalmoscopy tests | 6.4 | 3.6 | 2.9 | 2.5 | 2.6 | A | a |
| Ranibizumab group | |||||||
| Injections | 7.8 | 3.5 | 2.6 | 2.0 | 2.0 | B | a |
| Outpatient visits | 12.0 | 5.5 | 4.0 | 3.0 | 2.4 | C | a |
| Fundus photography tests | 12.0 | 5.5 | 4.0 | 3.0 | 2.4 | C | a |
| Eye tests | 12.0 | 5.5 | 4.0 | 3.0 | 2.4 | C | a |
| Optical coherence tomography test | 12.0 | 4.9 | 3.1 | 2.3 | 2.1 | C | a |
| Intraocular pressure tests | 12.0 | 5.5 | 4.0 | 3.0 | 2.4 | C | a |
| Fluorescein angiography tests | 12.0 | 1.7 | 1.6 | 1.3 | 1.4 | C | a |
| Slit lamp examination | 12.0 | 1.7 | 1.6 | 1.3 | 1.4 | C | a |
| Optometry tests | 12.0 | 5.5 | 4.0 | 3.0 | 2.4 | C | a |
| Indirect ophthalmoscopy tests | 12.0 | 5.5 | 4.0 | 3.0 | 2.4 | C | a |
†
Source (year 1): A, VIVID-EAST trial; B, REVEAL trial; C, Estimated based on the indication.
‡
Source (years 2–5): a, China physician survey; b, VIVID-EAST.
| Items | Unit drug cost (¥) | Unit cost (others) (¥) | Source† |
|---|---|---|---|
| Anti-VEGF Injections | |||
| Intravitreal aflibercept 2 mg | 5850 | 819.72 (administration cost) | A, C |
| ranibizumab10 mg/ml 0.2 ml/vial | 5700 | 819.72 (administration cost) | B, C |
| Treatment/monitoring visit | |||
| Laser | 388.16 | C | |
| Outpatient visit | 17.09 | D | |
| Fundus photography | 29.88 | D | |
| Eye test | 3.17 | D | |
| Optical coherence tomography | 121.06 | D | |
| Intraocular pressure test | 11.48 | D | |
| Fluorescein angiography | 163.59 | D | |
| Slit lamp examination | 13.86 | D | |
| Optometry | 11.64 | D | |
| Indirect ophthalmoscopy | 15.10 | D | |
| Adverse event treatment | |||
| Cataract | 5935.98 | C | |
| Vitreous hemorrhage | 12,346.40 | C | |
| Ocular hypertension (IOP) | 927.69 | C | |
| Arterial thromboembolic events‡ | 3452.22 | C | |
†
Source: A: retail price in China’s market; B: negotiated price with Ministry of Human Resource and Social Security in 2017; C: China physician survey, average weighted by 2017 total medical visits in the surveyed 12 cities; D: government report, average weighted by 2017 total medical visits in the surveyed 12 cities.
‡
Antiplatelet Trialists’ collaboration-defined arterial thromboembolic events.
Number of treatments/injections
The numbers of treatments in the efficacy phase (year 1) were taken from the VIVID-EAST trial for intravitreal aflibercept and laser, and from the REVEAL trial for ranibizumab. In the maintenance phase, the numbers of treatments for all comparators were collected through the China physician survey. This model followed an assumption proposed by China clinical KOLs that the numbers of treatments were the same for all anti-VEGFs (intravitreal aflibercept and ranibizumab) in the maintenance phase. The discontinuation rates were obtained from VIVID-EAST trial for intravitreal aflibercept group (12-month rate: 8.91%) and laser group (12-month rate: 8.91%), and the discontinuation rate for ranibizumab was assumed to equal to intravitreal aflibercept due to their similar mechanism of action and administration.
Monitoring visits
Based on the feedback from the physician surveys, each monitoring visit included an eye test, an optical coherence tomography, a fundus photography, an intraocular pressure test, a fluorescein angiography, a slit lamp examination, an optometry and an indirect ophthalmoscopy. The numbers of monitoring visits were derived from the VIVID-EAST trial for intravitreal aflibercept and laser treatment (year 1), and were estimated from the prescribing information of ranibizumab in China for ranibizumab (year 1), since the specific numbers were not reported in the REVEAL study publication. In the maintenance phase (years 2–5), the numbers of monitoring visits were estimated from China’s physician surveys.
Adverse events
Frequent ocular adverse events in the VIVID-EAST trial were obtained for the model analyses. Adverse events that are transient, self-resolving or symptoms of DME were not included in the analyses. According to results reported in the VIVID-EAST trial, 12-month cataract rates of 0.99 and 1.01%, 12-month vitreous hemorrhage rates of 0.00 and 8.08%, 12-month ocular hypertension (IOP) rates of 0.99 and 3.03%, and 12-month Antiplatelet Trialists’ collaboration-defined arterial thromboembolic events rates of 1.98 and 2.02% were used for the intravitreal aflibercept group and laser group, respectively. We assumed that ranibizumab has the same safety profile as aflibercept.
Indirect costs
Indirect costs were included in the base-case analyses for low vision states (VA4, VA5, VA6 and VA7) and blindness state (VA8) to better capture the full costs associated with each intervention. Low vision and blindness in this study were defined based on the visual disability standard published by the Central People’s Government of the People’s Republic of China [30] and verified by clinical experts. The days off for patients and caregivers were derived from the China physician survey, and values used in the model were 124, 350, 57 and 151 days for low-vision patients, blind patients, caregivers for low-vision patients and caregivers for blind patients, respectively. The average daily wage (196 Chinese Yuan Renminbi [CNY]) was calculated using the average national annual salary (67,569 CNY, 2016) divided by 365 days and accounting for the Consumer Price Index [31] difference in 2016 and 2018. The ages of retirement (60 years old for males and 55 years old for females) were also considered in this analysis. Annual allowance (2700 CNY) for blindness (VA8) published in Shanghai regulation document [32] was used in calculating the blindness-related cost.
Utility inputs
Because quality of life is a function of both eyes, a two-eye utility approach was adopted in the base-case analyses. In this study, utilities from a published study based on the two-eye model [33] were used. This source was accepted by NICE as more representative of patients affected by an eye condition. In Czoski-Murray et al.’s study, three age-related macular degeneration (AMD) vision states were produced by simulating the visual impairment associated with AMD through the use of custom-made contact lenses. Participants were randomly recruited from the healthy UK population. The time trade-off (TTO) was anchored at full health and immediate death. After the insertion of each lens, participants undertook five activities of daily living and completed five VF-14, HUI3 and TTO items for the new simulated vision state. TTO values for simulated states regression coefficient reported in the study were 0.869 for constant and -0.368 for VA logarithm as the minimal angle of resolution (VA logMAR). The health state utility base used in the model analysis is presented in Supplementary Table B.
In addition to the health state utilities, disutilities were incorporated for specific adverse events. In this study, the disutility is set as 0.14 [34] for cataract, 0.31 [35] for vitreous hemorrhage and 0.42 [36,37] for Antiplatelet Trialists’ collaboration-defined arterial thromboembolic events based on published relevant literature. The disutilities of ocular hypertension (IOP) were assumed to be zero as no published data are available. Decrements associated with each adverse event were applied to the proportion of the patients experiencing an adverse event in each cycle.
Sensitivity analyses
In order to understand the sensitivity of model outputs to changes in the values of model parameters, a series of structured and comprehensive one-way sensitivity analyses (OWSA) were adopted including all parameters. According to the 2015 China Guidelines for Pharmacoeconomic Evaluations and Manual [20], the variance was set as ±20% for all parameters except for the discount rate, which was set as 3 and 8%.
In addition, a probabilistic sensitivity analysis was conducted with Monte Carlo simulation to simultaneously take into account the uncertainty associated with parameter values. Sampling was based on point estimates used in the deterministic analyses, and standard error equal to 20% of the mean (point estimate) was used as a default. A total of 1000 different samples were taken from all distributions. Beta distribution was assigned for event rates; gamma distribution was assigned for costs and resource use estimates; log-normal distribution was assigned for continuous outcomes; and multivariate normal distribution was assigned for utility values.
To further explore the impact of difference efficacy sources on the results of intravitreal aflibercept versus ranibizumab, the indirect comparisons of the fixed effects using MTC analysis, random effects using Bucher analysis and fixed effects using Bucher analysis reported in Korobelnik et al.’s study were tested as scenario analyses. A further scenario analysis was conducted that considered the difference of losing letters (reported in Korobelnik et al.’s study) between these two groups.
Patient & public involvement
Patients and the public were not involved in this study.
Results
Intravitreal aflibercept versus laser
Base-case results
In the base-case analyses of a 20-year lifetime horizon, a DME patient treated with intravitreal aflibercept was associated with a gain of 7.825 QALYs and a total treatment cost of 217,841 CNY (32,264 USD, exchange rate 2017: 1 USD = 6.75 CNY), while a laser-treated patient was associated with a gain of 7.189 QALYs and a treatment cost of 135,489 CNY (20,067 USD; Table 3 & Supplementary Figure A). In comparison with the laser group, the intravitreal aflibercept group was associated with better health outcomes (incremental gain of 0.636 QALYs) and higher total costs (incremental cost of 82,352 CNY). The analyses resulted in the incremental cost–effectiveness ratio (ICER) of 129,397 CNY (19,165 USD) per QALY, which is lower than the willingness-to-pay (WTP) threshold (178,980 CNY) and therefore, the intravitreal aflibercept strategy will be considered as cost-effective for DME patients in China compared with laser.
| Treatment (efficacy source) | Costs (CNY, ¥) | QALYs | ICER (95% CI) (CNY per QALY) | ||
|---|---|---|---|---|---|
| Direct | Indirect | Total | |||
| Intravitreal aflibercept (VIVID-EAST) | 198,602 | 19,239 | 217,841 | 7.825 | - |
| Laser (VIVID-EAST) | 85,065 | 50,424 | 135,489 | 7.189 | Intravitreal aflibercept vs laser: 129,397, cost-effective (95% CI: -715,758–790,947) |
| Ranibizumab (Korobelnik et al., 2015) | 187,439 | 35,037 | 222,477 | 7.462 | Intravitreal aflibercept vs ranibizumab: -12,774, dominant (95% CI: -245,860–326,833) |
CNY: Chinese Yuan Renminbi; ICER: incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
Sensitivity analyses results
A tornado diagram for the 15 most sensitive parameters based on the ICER measure in OWSA for intravitreal aflibercept versus laser is displayed in Supplementary Figure B1. As it shows, the ICER was most sensitive to variations due to starting age of cohort, intravitreal aflibercept drug costs, number of intravitreal aflibercept injections and discontinuation rates.
A probabilistic sensitivity analysis was run on the base-case data to simultaneously assess the impact of input value uncertainties. The results are summarized in a scatter plot in Figure 2A, which shows the consistent finding that intravitreal aflibercept is a cost-effective strategy compared with a laser in most of the scenarios. Intravitreal aflibercept had a high chance (>50%) of being cost-effective over laser under the WTP threshold of tripled 2017 China per capita GDP (178,980 CNY). In addition, the chance of intravitreal aflibercept being cost-effective over laser increased to 84.5% when using the WTP threshold of tripled-weighted average per capita GDP of 12 cities (333,677 CNY, weighted by the 2017 population size), where the physician surveys were conducted (Supplementary Figure C1).
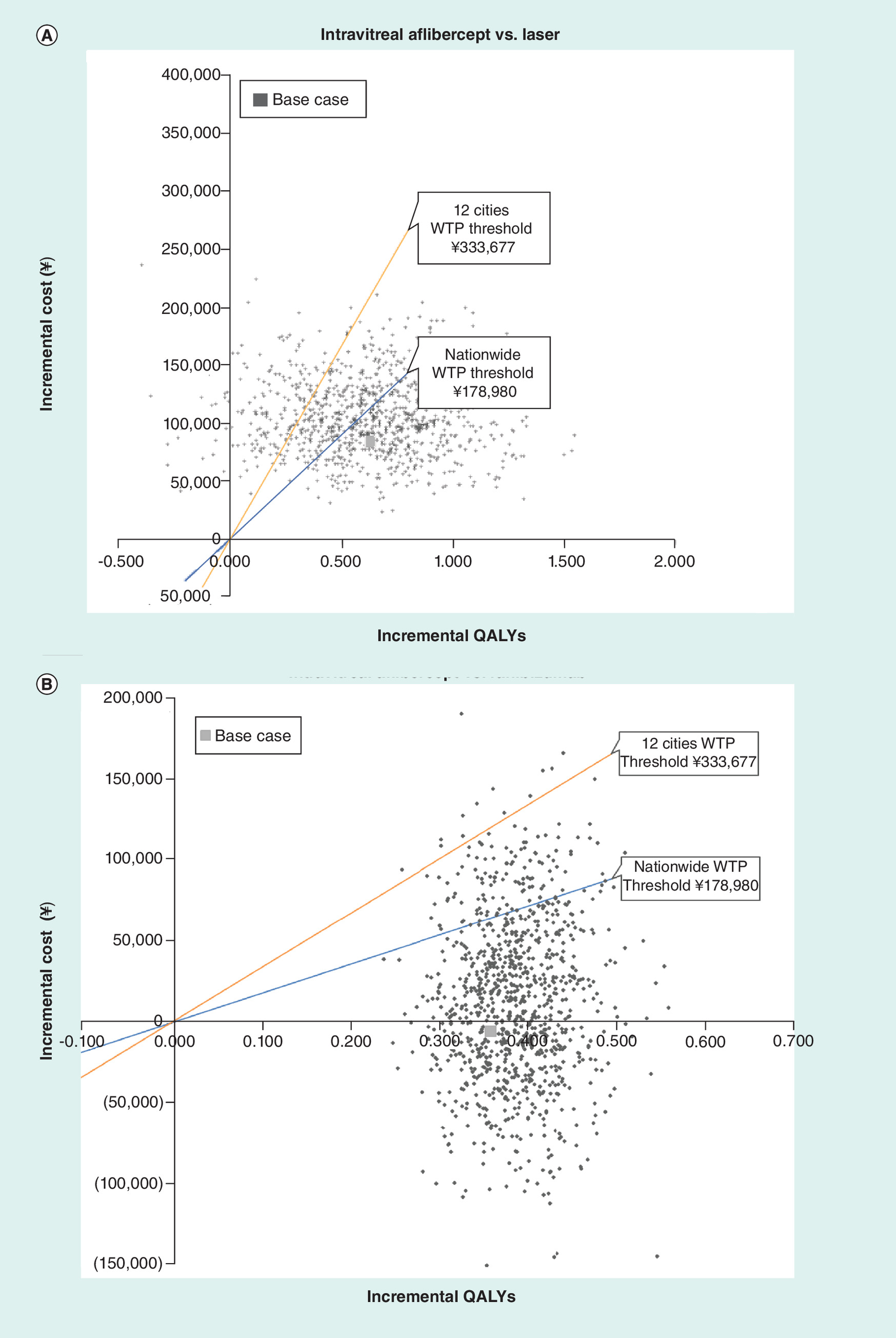
Figure 2. Scatter plot of probabilistic sensitivity analysis.
Nationwide WTP threshold: tripled 2017 China percapita GDP (¥178,980); 12 cities WPT threshold: tripled weighted average of 2017 per capita GDP in the surveyed 12 cities (weighted by 2017 population size, ¥333,677).
Intravitreal aflibercept versus ranibizumab
Base-case results
In the base-case analyses of a 20-year lifetime horizon, a ranibizumab-treated patient was associated with a gain of 7.462 QALYs and a total treatment cost of 222,477 CNY (32,951 USD; Table 3 & Supplementary Figure A), thus resulting in an ICER of -12,774 CNY (-1892 USD) per QALY for intravitreal aflibercept versus ranibizumab. Therefore, when compared with ranibizumab, intravitreal aflibercept can be considered to be a dominant strategy for DME patients in China that is associated with better health outcomes (incremental gain of 0.363 QALY) and lower treatment costs (a difference of -4636 CNY).
Sensitivity analyses & scenario analyses results
OWSA results are presented in the tornado diagram in Supplementary Figure 2B. The results showed that ranibizumab and intravitreal aflibercept drug costs had the largest impact on the CEA results, followed by the number of injections of intravitreal aflibercept and ranibizumab during years 1 and 2.
Probabilistic sensitivity analyses results are summarized in a scatter plot in Figure 2B, which shows the probability of intravitreal aflibercept being considered to be cost-effective or dominant over ranibizumab is 87.9%, under the WTP threshold of tripled 2017 China per capita GDP (178,980 CNY). The chance of intravitreal aflibercept being cost-effective over ranibizumab was determined to be 97.5% under the WTP threshold of tripled weighted average per capita GDP of 12 cities (333,677 CNY, weighted by 2017 population size), where the physician surveys were conducted (Supplementary Figure C2).
The scenario analyses of applying different indirect comparisons results reported in Korobelnik et al.’s study revealed a consistent finding of dominance (fixed effects using MTC analysis) or cost-effective (random or fixed effects using Bucher analysis) for intravitreal aflibercept versus ranibizumab. In addition, when we included the consideration of the difference of losing letters in these two groups, intravitreal aflibercept was associated with much higher QALYs and even lower costs.
Discussion
Health economic evidence is increasingly being recognized as an important and helpful guide for reimbursement decision-making in China ever since the implementation of China’s health reform in 2009, and in particular since the 2017 pricing negotiation of innovative medicines [38]. On the other hand, DME-caused disease burden is increasing due to the expanding diabetic population in China and the emerging treatment options for DME in recent years. In the current setting, this analysis provides the first evidence on the cost–effectiveness of treatment for DME causing visual impairment in China.
Our economic model, which was validated by China clinical experts, employed clinical trial efficacy data and local costs data to assess the economic value of intravitreal aflibercept 2 mg q8w versus laser and ranibizumab 0.5 mg PRN in treating visual impairment due to DME. At this point, it should be noted that bevacizumab and conbercept (also anti-VEGF drugs) were not included in our analyses. Although conbercept is seeking to expand its indication of DME in China, no efficacy data were published for its treatment of DME; an updated economic analysis may be needed once conbercept is approved for the treatment of DME and the relative efficacy data are available in the future. bevacizumab has not been approved for the treatment of any eye-related disease in any nations/regions, thus it was not included as a comparator in our study.
The CEA of intravitreal aflibercept versus laser was mainly conducted based on the efficacy data reported in the VIVID-EAST trial. The VIVID-EAST study was a Phase III, multicenter trial that studied intravitreal aflibercept for the treatment of visual impairment due to DME in an Asian population (recruited 301 Chinese patients, 79.63% of the total study population). We believe that this head-to-head trial-based CEA could examine well the economic value of intravitreal aflibercept compared with laser treatment. The main findings of this study indicate that, when compared with traditional laser treatment, intravitreal aflibercept 2 mg q8w has the potential to be a cost-effective strategy for the treatment of DME in China. Although the intravitreal aflibercept group’s costs were higher for anti-VEGF drugs (laser group also incurred anti-VEGF drug costs due to rescue treatment observed in the trial), monotherapy with intravitreal aflibercept could reduce the central retinal thickness and improve patients’ vision states to gain more QALYs, and further reduce the indirect costs and adverse event costs due to visual impairment. The indirect cost savings from the intravitreal aflibercept group is the main reason the starting age of the cohort has a considerable impact on the ICER. These results are stable in the variance of all other variables and in the majority of scenarios tested via sensitivity analyses.
For the comparison of intravitreal aflibercept versus ranibizumab, relative efficacy was derived from an NMA study published by Korobelnik et al. included 11 studies in an indirect analysis of intravitreal aflibercept 2 mg q8w compared with ranibizumab 0.5 mg PRN, including VIVID-DME, VISTA-DME, RESTORE, REVEAL, etc. [17,28,29]. This study is a major NMA study that concerns the odds ratio of intravitreal aflibercept versus ranibizumab and its findings were further confirmed by an updated NMA using patient level data in 2018 [39]. Our findings revealed that intravitreal aflibercept 2 mg q8w should be considered to be a dominant strategy for the treatment of DME in China when compared with ranibizumab 0.5 mg PRN. For both groups, the costs were mainly driven by the anti-VEGF drug costs. However, the intravitreal aflibercept group could bring higher QALYs for patients because of better efficacy in improving BCVA compared with the ranibizumab group; at the same time, it also saved indirect costs. This is a conservative estimation, since we assumed no difference in losing letters between these two groups, as the scenario analyses showed that the results would be much more in favor of the intravitreal aflibercept group if we considered this difference. Also, sensitivity analyses revealed that the model results were robust to reasonable alterations in inputs and assumptions.
Compared with other retinal conditions like AMD, there are few cost-effective analyses that focus on assessing the cost–effectiveness of anti-VEGF in the management of DME, which are limited to a few analyses from the payer or healthcare system perspective in the USA, UK and Greece. In the USA, the cost–effectiveness of anti-VEGF in DME was assessed using the Diabetic Retinopathy Clinical Research Network Comparative Effectiveness Trial. Treatment with intravitreal aflibercept was found to be associated with the highest gain in QALY, but from the perspective of the US payer, neither intravitreal aflibercept (2.0 mg) nor ranibizumab (0.3 mg) was cost-effective relative to Bevacizumab. Based on the efficacy from a previously published NMA study [40], Régnier et al. assessed the cost–effectiveness of ranibizumab (0.5 mg PRN and 0.5 mg treat and extend) compared with intravitreal aflibercept 2 mg q8w and found that from a UK perspective, ranibizumab was associated with a marginal incremental gain of 0.05 QALYs and slightly lower costs [41]. In Greece, a cost-utility analysis, which was also based on the relative efficacy (odds ratios) reported in Régnier et al.’s NMA [40], reached similar results and concluded that ranibizumab PRN and treat and extend regimens were cost-effective from the Greek payer perspective when compared with intravitreal aflibercept [42]. A more recent study conducted by Priaulx found that intravitreal aflibercept, while generating a higher number of QALYs, also reduced costs per patient per year by £1485 compared with ranibizumab at NHS list prices [43]. It also reported that the probability of intravitreal aflibercept being cost-effective was 83.7% when compared with laser treatment at a threshold of £30,000.
Our findings were consistent with most previous studies of comparing intravitreal aflibercept with laser or with ranibizumab. However, previous studies comparing intravitreal aflibercept with ranibizumab, Kourlaba et al. [42] and Regnier et al. [41] resulted in different conclusions, even though both studies referenced relative efficacy from the Regnier et al.’s NMA study. These two exceptions may be due to a few reasons. As it was discussed in Korobelnik et al.’s study [27], intravitreal aflibercept data included in Regnier et al.’s NMA [40] were only from three studies (DA VINC [44], VIVID-DME and VISTA-DME). The study’s analyses were related to only one secondary efficacy outcome (relative risk of ≥10 letter gain at 12 months), not the primary efficacy outcome in any pivotal Phase III study of intravitreal aflibercept or ranibizumab (mean gain in BCVA at 12 months in VIVID-DME/VISTA-DME). The single outcome included in Regnier et al.’s NMA [40] was also rerun by Korobelnik et al.; in this study, the direction of the effect favored the intravitreal aflibercept group, although the differences were still not significant [27]. The different results presented in these two NMA studies may be the essential reason the results for incremental QALYs of intravitreal aflibercept treatment reported in previous studies [41,42] were different from our study.
Other strengths of our study include the adoption of the societal perspective and the attempt to estimate the indirect costs based on the best available data. In a Chinese disease burden study conducted for another vision-threatening disease, the indirect cost of wet-AMD constituted 68.58% of the total costs [45]. In our study, the indirect costs included not only the productivity loss and caregiver costs, but also the vision costs of blindness, which were estimated by the allowance of blindness from the government. These indirect costs accounted for 8.83, 37.22, 15.75% of the total costs in the intravitreal aflibercept group, laser group and ranibizumab group, respectively. Although these proportions were lower than the previously reported numbers (as we may have underestimated the indirect costs), our results still indicate a significant burden of indirect costs caused by visual impairment and blindness.
There are, however, some limitations that should be considered. First, because there were no data available regarding the efficacy and resources used in the subsequent years, we assumed there were no vision state changes for patients in the maintenance phases (years 2–5), having acquired related data inputs only from physician estimation. This can be considered a limitation because the results need to be updated once any long-term trial data or real-world data become available. Second, given that limited empirical data were available for model testing, we attempted to close the data gaps by relying on recommendations from the KOL interviews and physician surveys that were conducted in 12 tier-1 or tier-2 cities in China. This can also be viewed as a limitation, although we did perform sensitivity analyses for the related parameters. Lastly, we used the allowance of blindness documented by the government as a surrogate for the cost of blindness, since it is difficult to estimate the true cost. The model may not capture all costs due to blindness and subsequently, may underestimate the cost of blindness and the indirect cost of visual impairment, thereby causing the results to favor the comparators (i.e., the laser and ranibizumab groups).
Conclusion
The VIVID-EAST trial-based CEA demonstrated that when compared with laser, intravitreal aflibercept has the potential to be a cost-effective strategy for the treatment of visual impairment due to DME in China, providing more QALYs and further saving on indirect costs. When compared with ranibizumab PRN, with the relative efficacy data derived from an NMA study, intravitreal aflibercept is considered to be a dominant strategy. This study provides the first evidence of the cost–effectiveness of treatment for DME causing visual impairment in China, and can be used as a valuable reference for clinical and reimbursement decision-making.
•
The VIVID-EAST study was a head-to-head trial for the Asian/Chinese population, and this trial-based cost–effectiveness analysis well examined the economic value of intravitreal aflibercept compared with laser treatment.
•
In the base case of a 20-year lifetime horizon, an intravitreal aflibercept-treated patient was associated with 7.825 quality-adjusted life years (QALYs) and 217,841 CNY, and a laser-treated patient was associated with 7.189 QALYs and 135,489 CNY. The incremental cost–effectiveness ratio for intravitreal aflibercept versus laser was 129,397 CNY/QALY, which was lower than the willingness-to-pay threshold of triple GDP per capita in China in 2017.
•
A ranibizumab pro re nata-treated patient was associated with 7.462 QALYs and 222,477 CNY. When comparing with ranibizumab pro re nata, intravitreal aflibercept was associated with better outcomes with lower treatment cost, resulting the incremental cost–effectiveness ratio of -12,774 CNY/QALY.
•
The adoption of a societal perspective incorporated the substantial indirect costs induced by diabetic macular edema-causing visual impairment based on best available data, which helped in generating a more comprehensively conclusion.
•
This study demonstrated the cost–effectiveness of aflibercept versus laser and ranibizumab for diabetic macular edema in China mainly based on local trial and cost data, which may provide important references for clinical and reimbursement decision-making.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
J Ming, Y Zhang, S Hu, X Xu, M Zhao, Y Wang and R Han developed the study objective and CEA model strategy; J Ming, Y Zhang, J Liu, X Zhao and R Han developed/adapted the CEA model and collected inputs. S Hu, X Xu, M Zhao, Y Wang, Y Chen, F Zhang and J Wang validated the model setting and data inputs. J Ming, Y Zhang, S Hu and X Zhao conducted the modeling analyses and manuscript writing. X Xu, M Zhao, Y Wang, Y Chen and F Zhang provided expert consultations on the contents of the manuscript. The manuscript was reviewed and agreed by all the coauthors. All the authors approved the final version of the manuscript.
Financial & competing interests disclosure
This project was sponsored by Bayer Healthcare Company Ltd., Beijing, China. Funding was not contingent upon publication of the manuscript. J Ming, J Liu and X Zhao are current employees of IQVIA, which received funds from Bayer Healthcare Company for this study. R Han is an employee of Bayer Healthcare Company Ltd. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of this shared data is in accordance with the terms (if any) agreed upon their receipt. The source of this data is: VIVID-EAST trial (clinicaltrials.gov identifier: NCT01783886).
Supplementary Material
File (suppl_data.zip)
- Download
- 339.09 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Yau JW, Rogers SL, Kawasaki R et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 35(3), 556–564 (2012).
2.
Cheung N, Mitchell P, Wong TY. Diabetic retinopathy. Lancet 376(9735), 124–136 (2010).
3.
Ciulla TA, Amador AG, Zinman B. Diabetic retinopathy and diabetic macular edema: pathophysiology, screening, and novel therapies. Diabetes Care 26(9), 2653–2664 (2003).
4.
Lim LS, Liew G, Cheung N, Mitchell P, Wong TY. Mixed messages on systemic therapies for diabetic retinopathy. Lancet 376(9751), 1461; author reply 1462 (2010).
5.
Cheung GC, Yoon YH, Chen LJ et al. Diabetic macular oedema: evidence-based treatment recommendations for Asian countries. Clin. Exp. Ophthalmol. 46(1), 75–86 (2018).
6.
Williams R, Airey M, Baxter H et al. Epidemiology of diabetic retinopathy and macular oedema: a systematic review. Eye 18(10), 963 (2004).
7.
Wang L, Gao P, Zhang M et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA 317(24), 2515–2523 (2017).
8.
Liu Y, Song Y, Tao L et al. Prevalence of diabetic retinopathy among 13473 patients with diabetes mellitus in China: a cross-sectional epidemiological survey in six provinces. BMJ Open 7(1), e013199 (2017).
9.
Gangnon RE, Davis MD, Hubbard LD et al. A severity scale for diabetic macular edema developed from ETDRS data. Invest. Ophthalmol. Vis. Sci. 49(11), 5041–5047 (2008).
10.
Lamoureux EL, Tai ES, Thumboo J et al. Impact of diabetic retinopathy on vision-specific function. Ophthalmology 117(4), 757–765 (2010).
11.
Shea AM, Curtis LH, Hammill BG et al. Resource use and costs associated with diabetic macular edema in elderly persons. Arch. Ophthalmol. 126(12), 1748–1754 (2008).
12.
Group ETDRSR. Photocoagulation for diabetic macular edema: early treatment diabetic retinopathy study report no. 4. Int. Ophthalmol. Clinics 27(4), 265–272 (1987).
13.
Schmidt-Erfurth U, Garcia-Arumi J, Bandello F et al. Guidelines for the management of diabetic macular edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica 237(4), 185–222 (2017).
14.
Solomon SD, Chew E, Duh EJ et al. Diabetic retinopathy: a position statement by the American Diabetes Association. Diabetes Care 40(3), 412–418 (2017).
15.
Ophthalmology ICO. Updated 2017 ICO Guidelines for Diabetic Eye Care (2016). http://www.icoph.org/enhancing_eyecare/diabetic_eyecare.html
16.
De Oliveira Dias JR, Andrade GC, Novais EA, Farah ME, Rodrigues EB. Fusion proteins for treatment of retinal diseases: aflibercept, ziv-aflibercept, and conbercept. Int. J. Retina Vitreous 2(1), 3 (2016).
17.
Korobelnik JF, Do DV, Schmidt-Erfurth U et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology 121(11), 2247–2254 (2014).
18.
Chen Y. Intravitreal aflibercept is effecttive in the treatment of patients with diabetic macular edema from asia and russia: results from the VIVID-EAST Study. Presented at: The 9th Congress of Asia Pacific Vitreo-retina Society. Sydney, Australia, 31 July–2 August 2015.
•• This head-to-head Phase III clinical trial study provided important comparative effectiveness data of intravitreal aflibercept versus laser in the treatment of diabetic macular edema in China.
19.
National Bureau of Statistics of China. China Statistical Yearbook-2017. China Statistics Press (2017). http://www.stats.gov.cn/tjsj/ndsj/2017/indexeh.htm
20.
Liu GB. China guidelines for pharmacoeconomic evaluations and manual (2015).
21.
Pershing S, Enns EA, Matesic B, Owens DK, Goldhaber-Fiebert JD. Cost-effectiveness of treatment of diabetic macular edema. Ann. Intern. Med. 160(1), 18–29 (2014).
22.
Klein R, Klein BE, Moss SE, Davis MD, Demets DL. The Wisconsin epidemiologic study of diabetic retinopathy. III. Prevalence and risk of diabetic retinopathy when age at diagnosis is 30 or more years. Arch. Ophthalmol. 102(4), 527–532 (1984).
23.
Christ SL, Lee DJ, Lam BL, Zheng DD, Arheart KL. Assessment of the effect of visual impairment on mortality through multiple health pathways: structural equation modeling. Invest. Ophthalmol. Vis. Sci. 49(8), 3318–3323 (2008).
24.
Jin Peiyao, Peng Jinjuan, Zou Haidong et al. A 5-year prospective study of type 2 diabetes patients in Shanghai Xinjing Community 1. The incidence and risk factors of diabetic retinopathy and diabetic macular edema in Chinese type 2 diabetes residents. Chin. J. Exp. Ophthalmol. 34(4), 363–367 (2016).
25.
Xu Xun, Zheng Ying. Focusing on the treatment of diabetic macular edema. Chin. J. Ocul. Fundus Dis. 32(2), 119–121 (2016).
26.
Jackson CH. Multi-state models for panel data: the msm package for R. J. Stat. Software 38(8), 1–29 (2011).
• Provided the R code to derive the transition probabilities of intravitreal aflibercept and laser treatment from individual patient-level data.
27.
Korobelnik JF, Kleijnen J, Lang SH et al. Systematic review and mixed treatment comparison of intravitreal aflibercept with other therapies for diabetic macular edema (DME). BMC Ophthalmol. 15, 52 (2015).
•• The transition probabilities for ranibizumab (a main comparator in this study) were calculated based on the mean log odds ratios compared with intravitreal aflibercept using results from this network-meta analysis.
28.
Mitchell P, Bandello F, Schmidt-Erfurth U et al. The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology 118(4), 615–625 (2011).
29.
Ohji M, Ishibashi Sr T, Group RS. Efficacy and safety of ranibizumab 0.5 mg as monotherapy or adjunctive to laser versus laser monotherapy in Asian patients with visual impairment due to diabetic macular edema: 12-month results of the REVEAL study. Invest. Ophthalmol. Visual Sci. 53(14), 4664–4664 (2012).
30.
China Disabled Persons’ Federatopm. China’s practical assessment standards for disabled people (2006). http://www.gov.cn/ztzl/gacjr/content_459939.htm
31.
National Bureau of Statistics of China. Consumer Price Index (2018). http://data.stats.gov.cn/english/easyquery.htm?cn=A01
32.
Shanghai Disabled Persons’ Federation. Measures for the administration of living subsidies for difficult persons with disabilities and nursing subsidy for severely disabled persons (2016). http://www.shanghai.gov.cn/nw2/nw2314/nw2319/nw12344/u26aw46410.html
33.
Czoski-Murray C, Carlton J, Brazier J, Young T, Papo NL, Kang HK. Valuing condition-specific health states using simulation contact lenses. Value Health 12(5), 793–799 (2009).
•• Provided utilities based on the two-eye model and is accepted by NICE.
34.
Brown GC, Brown MM, Brown HC, Kindermann S, Sharma S. A value-based medicine comparison of interventions for subfoveal neovascular macular degeneration. Ophthalmology 114(6), 1170–1178 (2007).
35.
Brändle M, Azoulay M, Greiner R. Cost-effectiveness and cost-utility of insulin glargine compared with NPH insulin based on a 10-year simulation of long-term complications with the Diabetes Mellitus Model in patients with type 2 diabetes in Switzerland. Int. J. Clin. Pharmacol. Ther. 45(4), 203–220 (2007).
36.
Pershing S, Enns EA, Matesic B, Owens DK, Goldhaber-Fiebert JD. Cost-effectiveness of treatment of diabetic macular edema. Ann. Intern. Med. 160(1), 18–29 (2014).
37.
Sorensen SV, Kansal AR, Connolly S et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation: a Canadian payer perspective. Thrombosis Haemostasis 105(05), 908–919 (2011).
38.
Li H, Liu GG, Wu J, Wu J-H, Dong C-H, Hu S-L. Recent pricing negotiations on innovative medicines pilot in China: experiences, implications, and suggestions. Value Health Reg. Issues 15, 133–137 (2018).
39.
Muston D, Korobelnik JF, Reason T et al. An efficacy comparison of anti-vascular growth factor agents and laser photocoagulation in diabetic macular edema: a network meta-analysis incorporating individual patient-level data. BMC Ophthalmol. 18(1), 340 (2018).
40.
Régnier S, Malcolm W, Allen F, Wright J, Bezlyak V. Efficacy of anti-VEGF and laser photocoagulation in the treatment of visual impairment due to diabetic macular edema: a systematic review and network meta-analysis. PLoS ONE 9(7), e102309 (2014).
41.
Régnier SA, Malcolm W, Haig J, Xue W. Cost-effectiveness of ranibizumab versus aflibercept in the treatment of visual impairment due to diabetic macular edema: a UK healthcare perspective. Clinicoecon. Outcomes Res. 7, 235 (2015).
42.
Kourlaba G, Relakis J, Mahon R et al. Cost-utility of ranibizumab versus aflibercept for treating Greek patients with visual impairment due to diabetic macular edema. Cost Eff. Resour. Alloc. 14(1), 7 (2016).
43.
Priaulx J, Napier J, Barzey V, Lovato E. The cost effectiveness of aflibercept compared to ranibizumab and laser in the management of diabetic macular oedema (DMO). Presented at: The Royal College of Ophthalmologists Annual Congress 2015. London, UK, 17 March 2015.
44.
Do DV, Nguyen QD, Boyer D et al. One-year outcomes of the da Vinci Study of VEGF Trap-Eye in eyes with diabetic macular edema. Ophthalmology 119(8), 1658–1665 (2012).
45.
Zhang Yabing, Hu Shanlian, Chang Jinghua. Analysis on the disease burden of wet age-related macular degeneration in China. Chin. Health Econ. 34(1), 63–65 (2015).
Information & Authors
Information
Published In
Pages: 161 - 175
PubMed: 31904267
Copyright
© 2020 Future Medicine Ltd.
History
Received: 18 November 2019
Accepted: 10 December 2019
Published online: 6 January 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness analysis of intravitreal aflibercept in the treatment of diabetic macular edema in China. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0174
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Fenghao Shi, Shuhua Tan, Yamin Shu, Tianyi Liu, Yan Xia, Christian Buehrer, Sheng Han, Cost-effectiveness analysis of the use of faricimab in diabetic macular edema in China, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0190, 15, 4, (2026).
- Mojtaba Hasoumi, Vahid Alipour, Hamid Ahmadieh, Jalal Arabloo, Reza Jahangiri, Cost-effectiveness analysis of anti-VEGF drugs in the treatment of visual impairment due to diabetic macular edema: A systematic review, European Journal of Clinical Pharmacology, 10.1007/s00228-026-03995-y, 82, 3, (2026).
- Mari Pesonen, Virpi Jylhä, Eila Kankaanpää, Adverse drug events in cost-effectiveness models of pharmacological interventions for diabetes, diabetic retinopathy, and diabetic macular edema: a scoping review, JBI Evidence Synthesis, 10.11124/JBIES-23-00511, 22, 11, (2194-2266), (2024).
- Tara Li, Vladislav Berdunov, Robin Hamilton, Yaneth Gil Rojas, Christian Bührer, Oliver Cox, Roelien Postema, Marloes Bagijn, Economic Assessment in Resource-Constrained Systems: Individual-Level Simulation Model in Wet Age-Related Macular Degeneration and Diabetic Macular Oedema, Ophthalmology and Therapy, 10.1007/s40123-024-00999-8, 13, 10, (2577-2597), (2024).
- Xin Mao, Zhanjing Dai, Jing Yang, Yuhang Wu, Fan Xie, Yun Lu, Jie Yu, Feng Chang, Yuqiong Lu, Cost-Effectiveness Analysis of Fluocinolone Acetonide Intravitreal (FAI) Implant for Chronic Noninfectious Uveitis Affecting the Posterior Segment of the Eye (NIU-PS) in China, Ophthalmology and Therapy, 10.1007/s40123-024-00939-6, 13, 6, (1757-1772), (2024).
- Zixuan He, Xianqin Huang, Dingyi Chen, Guoan Wang, Yuezhen Zhu, Huangqianyu Li, Sheng Han, Luwen Shi, Xiaodong Guan, Sponsorship bias in published pharmacoeconomic evaluations of national reimbursement negotiation drugs in China: a systematic review, BMJ Global Health, 10.1136/bmjgh-2023-012780, 8, 11, (e012780), (2023).