Reducing preoperative blood orders and costs for radical prostatectomy
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: A maximum surgical blood order schedule (MSBOS) was implemented at our institution to optimize preoperative blood ordering and reduce unnecessary blood preparation for patients undergoing radical prostatectomy (RP), a common urologic procedure. Materials & methods: We conducted a retrospective review of patients who underwent RP from 2010 to 2016 and categorized patients by date of RP (pre- or post-MSBOS) and compared preoperative blood-ordering practices. Results: After MSBOS implementation, preoperative blood orders changed from predominantly type and cross-match 2 units (53%) to no sample (56%) for robot-assisted laparoscopic RP, and from mostly type and cross-match 2 units (62%) to type and screen (75%) for open RP with resultant cost savings. Conclusion: MSBOS implementation and compliance decreases unnecessary preoperative blood orders.
Radical prostatectomy (RP) for prostate cancer constitutes a significant proportion of urologic healthcare volume and costs in the USA [1,2]. Prior studies have demonstrated that the cost of RP varies significantly between centers, with variation driven by multiple patient, surgeon and hospital factors [3–6]. Since RP is a high-volume procedure for Medicare patients, it may be one of the first urologic procedures to be subjected to future bundled payment models, which would incentivize standardization to achieve cost containment on a national scale [3,7]. In order to improve efficiency and prepare for these potential payment changes, it is important to identify areas within the RP pathway where value can be optimized.
The optimization of preoperative blood preparation and ordering practices represents a potential area for improvement, as both open RP (ORP) and robot-assisted laparoscopic RP (RALRP) have been associated with relatively low transfusion rates – although RALRP may be associated with relatively lower morbidity and hospital length of stay overall than ORP [8–10]. To promote efficient preoperative blood preparation and reduce the potential wastage of blood, an updated maximum surgical blood order schedule (MSBOS) – an institution-specific preoperative blood ordering protocol – was devised and implemented at our institution in 2012 [11]. This updated MSBOS was the first protocol in the USA to provide comprehensive recommendations for various surgical procedures based on institution-specific blood utilization data, including percent of patients transfused, estimated blood loss (EBL), transfusion index (mean number of units transfused per patient) and the risk of major bleeding for various surgical procedures [11]. Since RALRP is associated with less EBL and a lower rate of packed red blood cell (pRBC) transfusions than ORP, our MSBOS guidelines recommend that surgeons order a preoperative type and screen (T/S) for patients undergoing ORP and no preoperative blood orders (i.e., ‘no sample’ [NS]) for patients undergoing RALRP [12–14].
Given that the impact of MSBOS guidelines on preoperative blood preparation and blood utilization for ORP and RALRP has not been previously described, we assessed temporal trends in preoperative blood ordering practices before and after MSBOS implementation at our institution. We also quantified costs associated with preoperative blood ordering before and after MSBOS implementation, as well as MSBOS compliance.
Materials & methods
Study population
We performed a retrospective review of men who underwent RP for prostate cancer between 1 February 2010 and 29 April 2016 at our institution using data from our institutional blood management and RP databases. The sources of data for transfusions and the database quality control methods have been previously described [15]. We excluded six patients who were listed as Jehovah’s Witnesses, since they did not undergo any preoperative blood testing or receive any pRBC transfusions. We also excluded 751 patients who underwent RP in 2012 (the MSBOS transition year) from statistical analyses, but data from 2012 are depicted in our graphical displays of temporal trends for the purposes of continuity (Figures 1 & 2).
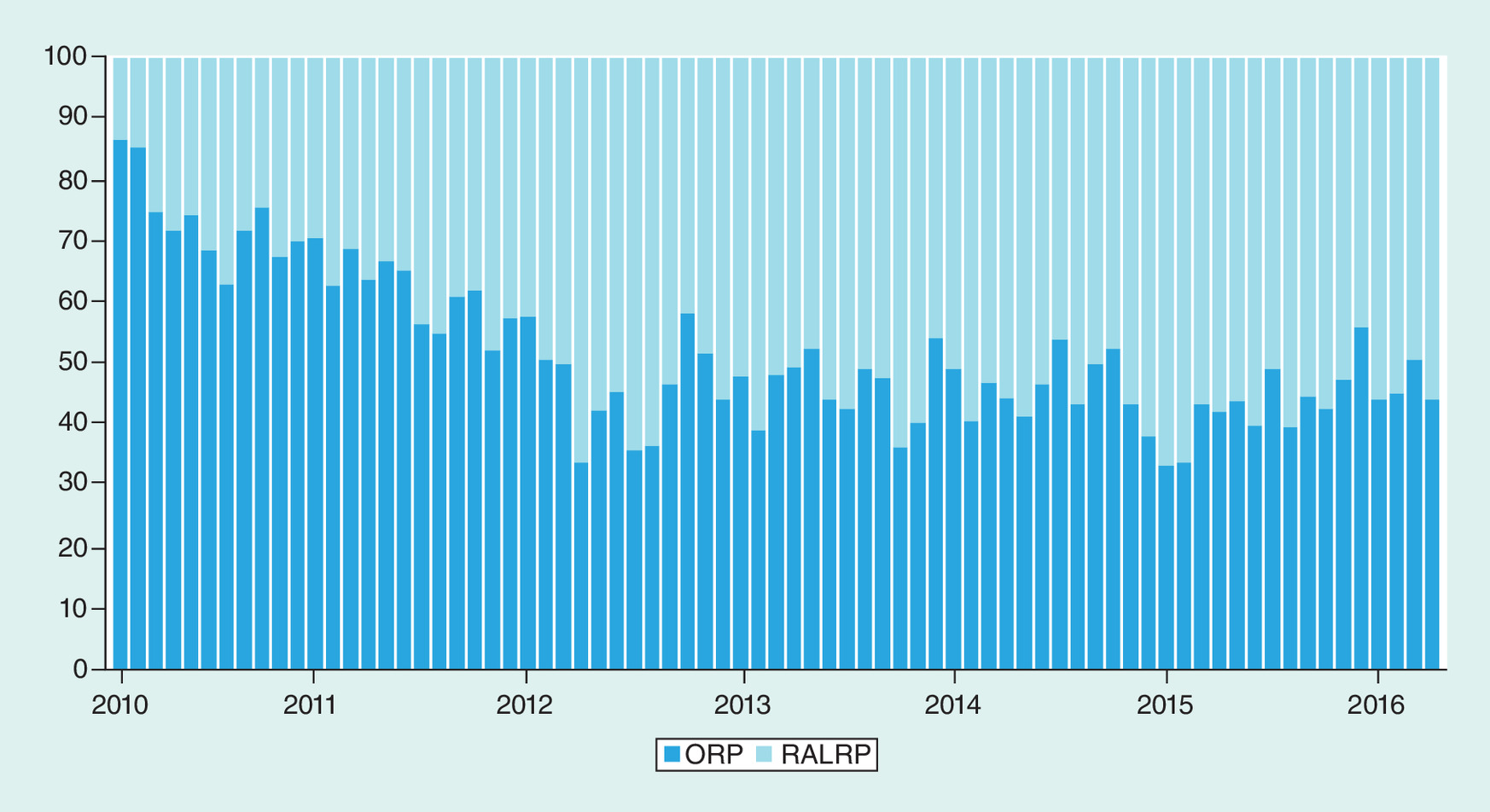
Figure 1. Relative distribution of type of radical prostatectomy performed over time.
Bars represent the percent of total prostatectomy cases that were performed in either an open or robotic fashion for each month of our study period. Patients who underwent radical prostatectomy in 2012 are shown, but were not included in the study population to account for the transition phase during implementation of new preoperative blood ordering guidelines.
ORP: Open radical prostatectomy, RALRP: Robot-assisted laparoscopic radical prostatectomy.

Figure 2. Comparison of preoperative blood orders over time before and after MSBOS implementation for (A) robot-assisted laparoscopic radical prostatectomy and (B) open radical prostatectomy.
Patients who underwent radical prostatectomy in 2012 are shown, but were not included in the study population to account for the transition phase during implementation of new preoperative blood ordering guidelines.
MSBOS: Maximum surgical blood order schedule; T/C: Type and cross-match (2 units); T/S: Type and screen.
Patient and disease characteristics assessed included patient age, race, BMI, Charlson Comorbidity Index (CCI), preoperative serum prostate-specific antigen (PSA), clinical stage, diagnostic biopsy Gleason grade group (GG) and presence of nonorgan-confined (NOC) disease on surgical pathology. We also assessed type of RP performed, surgical operating room (OR) time, intraoperative EBL, rates of intraoperative and whole-hospital pRBC transfusions, the whole-hospital nadir hemoglobin, preoperative blood orders for preparing pRBCs (T/S, type and cross-match [T/C] 2 units and NS), the cost associated with each type of preoperative blood order, and MSBOS compliance.
Intervention
Prior to 2012, there were no established blood ordering guidelines at our institution and blood ordering was dependent on surgeon preference. In 2012, a first-of-its-kind institution-specific preoperative blood ordering protocol was created via an algorithm that has been previously described [11] and implemented across our institution. Specifically, for ORP, this recommended changing the common ordering practice of T/C 2 units to T/S. For RALRP, this recommended changing the predominant ordering practice of T/C 2 units to NS.
Statistical analysis
Patient and disease characteristics, surgical outcomes and blood-related outcomes between patients who underwent ORP versus RALRP were compared in the pre- and post-MSBOS eras using Fisher's exact tests, Chi-squared tests, Wilcoxon tests or Student’s t-tests, as appropriate. Univariate logistic regression was used to assess patient, disease and surgical factors associated with the likelihood of receipt of whole-hospital pRBC transfusions (during the whole-hospital stay) among patients who underwent RALRP and ORP. Univariate logistic regression was also used to assess patient, disease and surgical factors associated with MSBOS noncompliance among patients who underwent RALRP. Analyses were generated using JMP version 12.1.0. (SAS Institute, NC, USA), with a two-sided p-value <0.05 considered statistically significant.
Results
Overall, 3994 men underwent RP at our institution during the pre-MSBOS era (2010–2011) and post-MSBOS era (2013–2016) and met study inclusion criteria. Of these, 2413 (60%) underwent RP in the post-MSBOS period. Patient and disease characteristics stratified by type of RP and whether RP was performed in the pre- or post-MSBOS time period are shown in Table 1. In the pre-MSBOS period, significant differences in BMI and Gleason GG at diagnostic biopsy were found among patients who underwent ORP versus RALRP. In the post-MSBOS period, significant differences in age, CCI, preoperative PSA, clinical stage and Gleason GG at diagnostic biopsy were found among patients who underwent ORP versus RALRP. However, the statistical significance likely reflects the large sample size as the differences were small and likely not clinically significant.
| Characteristic | Pre-MSBOS (2010–2011) n = 1581 (40%) | p-value | Post-MSBOS (2013–2016) n = 2413 (60%) | p-value | ||
|---|---|---|---|---|---|---|
| ORP n = 1060 (67%) | RALRP n = 521 (33%) | ORP n = 1091 (45%) | RALRP n = 1322 (55%) | |||
| Age in years, median (IQR) | 59 (54–64) | 59 (54–63) | 0.54 | 62 (56–66) | 60 (55–65) | <0.001 |
| African-American race, n (%) | 139 (13.1) | 61 (11.7) | 0.98 | 160 (14.7) | 165 (12.5) | 0.19 |
| BMI (kg/m2), median (IQR) | 27.1 (25.1–29.1) | 27.3 (25.1–30.0) | 0.03 | 27.4 (25.1–30.1) | 27.3 (25.1–30.0) | 0.36 |
| CCI ≥3, n (%) | 249 (23.5) | 140 (26.9) | 0.14 | 231 (21.1) | 226 (17.1) | 0.01 |
| PSA (ng/ml), median (IQR) | 4.9 (3.7–6.7) | 5.0 (3.9–6.6) | 0.39 | 5.8 (4.4–8.5) | 5.5 (4.3–7.6) | 0.001 |
| Clinical stage, n (%) | 0.16 | <0.001 | ||||
| – T1 (a–c) | 818 (77.2) | 419 (80.4) | 793 (72.7) | 986 (74.6) | ||
| – T2 (a–c) | 231 (21.8) | 95 (18.2) | 262 (24.0) | 297 (22.5) | ||
| – T3 (a–c) | 3 (0.3) | 0 (0.0) | 19 (1.7) | 3 (0.2) | ||
| Gleason GG, n (%) | 0.01 | <0.001 | ||||
| – 1 | 568 (53.6) | 303 (58.2) | 380 (34.8) | 551 (41.7) | ||
| – 2 | 276 (26.0) | 147 (28.2) | 328 (30.0) | 439 (33.2) | ||
| – 3 | 134 (12.6) | 48 (9.2) | 167 (15.3) | 181 (13.7) | ||
| – 4 | 51 (4.8) | 11 (2.1) | 107 (9.8) | 93 (7.0) | ||
| – 5 | 30 (2.8) | 12 (2.3) | 109 (10.0) | 58 (4.4) | ||
| NOC disease, n (%) | 291 (27.5) | 123 (23.6) | 0.09 | 384 (35.2) | 422 (31.9) | 0.09 |
CCI: Charlson comorbidity index; GG: Grade group; IQR: Interquartile range; MSBOS: Maximum surgical blood order schedule; NOC: Non organ-confined; ORP: Open radical prostatectomy; PSA: Prostate-specific antigen; RALRP: Robot-assisted laparoscopic radical prostatectomy.
Type of RP
The relative frequency of each type of RP also changed significantly between the pre-MSBOS and post-MSBOS periods. In the pre-MSBOS era, ORP represented 67% of all RPs performed; in the post-MSBOS era, ORP represented 45% of all RPs performed (Table 1). RALRP became increasingly more common over time, representing 14% of all RPs in February 2010 and 56% of all RPs in April 2016 (Figure 1).
Surgeon
In the pre-MSBOS period, there were nine surgeons who performed the majority of RPs at our institution. There were four surgeons who performed ORP only, one surgeon who performed RALRP only, and four surgeons who performed both types of RP. In the post-MSBOS period, there were nine surgeons (eight from the pre-MSBOS period and one new surgeon). There were three surgeons who performed ORP only, three surgeons who performed RALRP only and three surgeons who performed both types of RP.
EBL & pRBC transfusions
The median intraoperative EBL for RALRP was significantly less than that of ORP in the pre-MSBOS period (200 ml [interquartile range {IQR}: 100–300] vs 600 ml (IQR: 400–800), respectively, p < 0.001] and in the post-MSBOS period (150 ml [IQR: 100–200] vs 500 ml [350–750], respectively, p < 0.001; Table 2). Additionally, the median whole-hospital nadir hemoglobin was significantly lower for patients who underwent ORP compared with RALRP in both the pre-MSBOS period (10.9 g/dl [IQR: 10.0–11.7] vs 11.9 g/dl [IQR: 11.1–12.7], respectively, p < 0.001) and the post-MSBOS period (10.9 g/dl [IQR: 9.9–11.7] vs 11.9 [IQR: 11.1–12.7], respectively, p < 0.001; Table 2). RALRP was associated with significantly lower rates of intraoperative pRBC transfusions than ORP in both the pre-MSBOS period (0.2 vs 1.5%, respectively, p = 0.02) and post-MSBOS period (0.0 vs 1.0%, respectively, p < 0.001); however, the rates of whole-hospital pRBC transfusions for RALRP were significantly lower than ORP in the post-MSBOS period only (1.2 vs 2.7%, respectively, p = 0.006; Table 2). When comparing the pre-MSBOS and post-MSBOS time periods, there was a decrease in the overall rate of intraoperative and whole-hospital pRBC transfusions for ORP (1.5–1.0% and 3.2–2.7%, respectively) and RALRP (0.2–0.0% and 2.1–1.2%, respectively).
| Outcome | Pre-MSBOS (2010–2011) (n = 1581; 40%) | p-value | Post-MSBOS (2013–2016) (n = 2413; 60%) | p-value | ||
|---|---|---|---|---|---|---|
| ORP n = 1060 (67%) | RALRP n = 521 (33%) | ORP n = 1091 (45%) | RALRP n = 1322 (55%) | |||
| OR time (minutes), median (IQR) | 110 (88–133) | 177 (151–201) | <0.001 | 108 (84–135) | 153 (131–174) | <0.001 |
| EBL (ml), median (IQR) | 600 (400–800) | 200 (100–300) | <0.001 | 500 (350–750) | 150 (100–200) | <0.001 |
| pRBC transfusion (intraoperative), n (%) | 16 (1.5) | 1 (0.2) | 0.02 | 11 (1.0) | 0 (0.0) | <0.001 |
| pRBC transfusion (whole hospital), n (%) | 34 (3.2) | 11 (2.1) | 0.21 | 30 (2.7) | 16 (1.2) | 0.006 |
| Nadir Hb (g/dl), median (IQR) | 10.9 (10.0–11.7) | 11.9 (11.1–12.7) | <0.001 | 10.9 (9.9–11.7) | 11.9 (11.1–12.7) | <0.001 |
EBL: Estimated blood loss; Hb: Hemoglobin; IQR: Interquartile range; MSBOS: Maximum surgical blood order schedule; OR: Operating room; ORP: Open radical prostatectomy; pRBC: Packed red blood cell; RALRP: Robot-assisted laparoscopic radical prostatectomy.
On univariate analysis, patient age, BMI, CCI, Gleason GG at diagnostic biopsy, clinical stage, the presence of NOC disease and operating room time were not associated with an increased probability of receiving a whole-hospital pRBC transfusion for patients who underwent RALRP (Table 3). However, preoperative PSA above the overall median (≥ 5.3 ng/ml) was associated with an increased probability of receiving a whole-hospital pRBC transfusion for patients who underwent RALRP (odds ratio [OR]: 2.34 [95% CI: 1.01–5.37]; p = 0.045). For patients who underwent ORP, CCI ≥3 (OR: 1.82 [95% CI: 1.08–3.07]; p = 0.03] and OR time above the overall median (≥123 min; OR: 2.34 [95% CI: 1.42–3.83]; p < 0.001) were associated with an increased probability of receiving a whole-hospital pRBC transfusion (Table 3). However, patient age, BMI, PSA, Gleason GG at diagnostic biopsy, clinical stage, and the presence of NOC disease were not associated with an increased probability of receiving a whole-hospital pRBC transfusion for patients who underwent ORP.
| Characteristic | RALRP n = 1843 (46%) | ORP n = 2151 (54%) | ||
|---|---|---|---|---|
| Odds ratio (95% CI) | p-value | Odds ratio (95% CI) | p-value | |
| Age ≥60 years† | 1.40 (0.65–3.04) | 0.39 | 1.01 (0.62–1.67) | 0.96 |
| BMI ≥30 kg/m2 † | 1.86 (0.84–4.08) | 0.12 | 1.05 (0.58–1.88) | 0.88 |
| CCI ≥3 | 1.71 (0.74–3.95) | 0.21 | 1.82 (1.08–3.07) | 0.03 |
| PSA ≥5.3 ng/ml† | 2.34 (1.01–5.37) | 0.045 | 1.63 (0.98–2.72) | 0.06 |
| Gleason GG ≥3 | 0.62 (0.21–1.80) | 0.38 | 1.15 (0.68–1.98) | 0.60 |
| cT2/T3 (a-c) | 1.26 (0.68–2.34) | 0.46 | 2.19 (0.65–7.28) | 0.21 |
| NOC disease | 1.20 (0.51–2.86) | 0.68 | 1.06 (0.63–1.80) | 0.82 |
| OR time ≥123 min† | 0.99 (0.41–2.35) | 1.00 | 2.34 (1.42–3.83) | <0.001 |
†
Values indicate 50th percentile for the entire cohort.
CCI: Charlson comorbidity index; GG: Grade group; NOC: Nonorgan-confined; OR: Operating room; ORP: Open radical prostatectomy; PSA: Prostate-specific antigen; RALRP: Robot-assisted laparoscopic radical prostatectomy.
Preoperative blood ordering & MSBOS compliance
After MSBOS implementation, the preoperative blood ordering practices at our institution changed from predominantly T/C 2 units (62%) to T/S (75%) for ORP and from T/C 2 units (53%) to NS (56%) for RALRP (Figure 2). The MSBOS noncompliance rates for RALRP and ORP were 44 and 25%, respectively. For RALRP, 95% of MSBOS noncompliance was attributable to ordering preoperative T/S; for ORP, 48% of MSBOS noncompliance was attributable to ordering preoperative T/C 2 units. In terms of MSBOS noncompliance, providers tended to be more likely to order a T/S for patients ≥60 years old who underwent RALRP (OR: 1.18; 95% CI: 1.00–1.38; p = 0.048), even though older age was not significantly associated with an increased likelihood of receiving a whole-hospital pRBC transfusion. The average preoperative blood order cost-per-case for ORP decreased from US$47.31 to US$35.36; the average preoperative blood order cost-per-case for RALRP decreased from US$45.89 to US$17.21, although there would be no blood order costs for RALRP if 100% MSBOS compliance was achieved.
Discussion
In this study of 3994 men who underwent RP at our institution, we found that MSBOS implementation corresponded with a subsequent overall decrease in preoperative blood orders and preparation for both ORP and RALRP with resultant cost-savings. Throughout the duration of our study, the surgeons performing RP were relatively constant, although there was one new replacement in the post-MSOBS period. It is important to note that MSBOS implementation occurred within the context of decreasing rates of RP-associated pRBC transfusions for both ORP and RALRP and a progressive increase in prevalence of RALRP relative to ORP. However, despite the lower rates of EBL and pRBC transfusion associated with RALRP, over 40% of preoperative blood orders for RALRP cases were not compliant with the MSBOS guideline. Furthermore, this noncompliance reflected an age bias, as providers were more likely to order an unnecessary preoperative T/S for older patients undergoing RALRP, even though age was not associated with an increased probability of pRBC transfusion.
Our temporal and comparative results are consistent with studies demonstrating that EBL decreases over time with surgical experience, as well as that RALRP has become more prevalent than ORP and is associated with comparatively less EBL and pRBC transfusions [8,9,12,16–21]. Although there is variation in reports of RP-associated EBL and pRBC transfusion rates in the literature, our results are comparable to other series. In a comparison of RALRP and ORP, Kordan et al. reported a median EBL of 100 versus 450 ml and overall transfusion rates of 0.8 versus 3.4%, respectively [8]. In a recent German study comparing 7007 men who underwent ORP and 3783 men who underwent RALRP, the pRBC transfusion rates were 3.5% and 0.75%, respectively [21].
Of note, RALRP has consistently been shown to be associated with significantly higher cost than ORP: a difference that is largely driven by fixed OR supply costs [9,19,22–25]. Since RALRP is the predominant type of RP performed and may be included in future bundled payment reform in urologic surgery, improving value in modifiable areas of the RP pathway is paramount. The persistent ordering of unnecessary preoperative blood orders and associated unnecessary laboratory costs represents an area of potential improvement in the RP pathway that would promote value-driven care, as even small cost-savings can have an impact on a national scale. We estimate that with 100% compliance to the MSBOS, our institution could have an annual operations cost savings of approximately US$3955 for ORP and US$11586 for RALRP. Therefore, provider education about MSBOS guidelines and RP costs should be increased to promote MSBOS compliance and cost savings. To this end, MSBOS compliance is supported by the American Society of Anesthesiologists' Task Force on Perioperative Blood Management's recommendation that an MSBOS should be utilized ‘when available and in accordance with (your) institutional policy, as a strategy to improve the efficiency of blood ordering practices’ [26].
Our study has several limitations that must be considered. This was a retrospective study of men who underwent RP at a high-volume tertiary academic hospital, which may limit the generalizability of our findings. While our EBL and rates of pRBC transfusions are similar to other published series, EBL and the need for pRBC transfusions may differ based on surgeon experience or the patient population at other centers, and this could impact MSBOS recommendations for RP-associated preoperative blood orders at other institutions. We also did not survey providers to assess reasons for MSBOS noncompliance at our institution. For example, additional reasons for the residual MSBOS noncompliance for RALRP may be clinicians’ reluctance to use universal donor (type-O) emergency release blood as a backup for the rare cases with unexpected bleeding, since the MSBOS recommends no preoperative blood orders for RALRP cases. However, only one out of 1843 RALRP patients in the current study received an intraoperative pRBC transfusion, whereas 27 patients received a pRBC transfusion during their hospital stay. Since postoperative transfusions are usually not emergent, this suggests there would be sufficient time to order a cross-match and avoid emergency release blood for postoperative transfusions. Nonetheless, even if type-O emergency release blood is required, it is much safer than many clinicians understand it to be. In trauma patients, it is used frequently, with a chance of a minor delayed hemolytic reaction between 0.2 and 0.4% and essentially no chance of a life-threatening ABO incompatibility reaction [27–29]. Therefore, additional inquiry regarding reasons for MSBOS noncompliance represents a future area of research.
To our knowledge, this is the first study to examine optimization of preoperative blood ordering practices and MSBOS compliance for RP, a common urological procedure. In our retrospective study of 3994 men who underwent RP, we found that implementation of MSBOS guidelines resulted in a decrease in unnecessary preoperative blood orders for both ORP and RALRP with resultant cost savings. However, over 40% of preoperative blood orders for RALRP cases were not compliant with the MSBOS guidelines, so potential cost savings could be greater than our estimates. Noncompliance was associated with older patient age, even though older patients were not more likely to need transfusions. Therefore, further provider-oriented educational efforts to reduce unnecessary preoperative blood orders are needed to optimize value-driven care for RP.
Conclusion
Overall, our retrospective study revealed that the use of an MSBOS for ORP and RALRP decreased unnecessary preoperative blood ordering at our institution, with resultant cost savings. However, MSBOS compliance can be improved. We aim to increase compliance through continued provider educational efforts.
•
Radical prostatectomy (RP) for prostate cancer constitutes a significant proportion of urologic healthcare volume and cost, with cost variation driven by multiple patient, surgeon and hospital factors.
•
A maximum surgical blood order schedule (MSBOS) was implemented at our institution to standardize and optimize preoperative blood ordering and reduce unnecessary blood preparation for patients undergoing RP.
•
The MSBOS recommended preoperative type and screen (T/S) for open RP (ORP) and no preoperative blood orders or ‘no sample’ for robot-assisted laparoscopic RP (RALRP). The impact of the MSBOS on change in RP practice has never been investigated.
•
In our study of 3994 men, we compared preoperative blood ordering and associated costs in the pre- and post-MSBOS time periods for patients undergoing ORP and RALRP from 2010 to 2016 and categorized patients by date of RP (pre- or post-MSBOS).
•
After MSBOS implementation, preoperative blood orders changed from predominantly type and cross-match (T/C) 2 units (53%) to no sample (56%) for RALRP.
•
After MSBOS implementation, preoperative blood orders changed from predominantly T/C 2 units (62%) to T/S (75%) for ORP.
•
Compared with the pre-MSBOS era, post-MSBOS average preoperative blood order cost-per-case for ORP and RALRP decreased from US$47.31 to US$35.36 and US$45.89 to US$17.21, respectively.
•
The MSBOS noncompliance rates for RALRP and ORP were 44% and 25%, respectively.
•
Our findings demonstrate that MSBOS adherence can decrease unnecessary preoperative blood ordering and associated costs, thereby improving value.
•
Further reduction of unnecessary preoperative blood orders can be achieved with increased provider education to improve MSBOS compliance.
Financial & competing interests disclosure
SM Frank has been on scientific advisory boards for Medtronic, Haemonetics and Baxter, which do not have products relevant to this study. B Trock has research grant funding from Myriad Genetics, Inc. and MDxHealth, neither of which has products relevant to this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Roehrborn CG, Black LK. The economic burden of prostate cancer. BJU Int. 108(6), 806–813 (2011).
2.
Crawford ED, Black L, Eaddy M, Kruep EJ. A retrospective analysis illustrating the substantial clinical and economic burden of prostate cancer. Prostate Cancer Prostatic Dis. 13(2), 162–167 (2010).
3.
Herrel LA, Syrjamaki JD, Linsell SM, Miller DC, Dupree JM. Identifying drivers of episode cost variation with radical prostatectomy. Urology 97, 105–110 (2016).
4.
Cole AP, Leow JJ, Chang SL et al. Surgeon and hospital level variation in the costs of robot-assisted radical prostatectomy. J. Urol. 196(4), 1090–1095 (2016).
5.
Ellimoottil C, Li J, Ye Z et al. Episode-based payment variation for urologic cancer surgery. Urology 111, 78–85 (2018).
6.
Makarov DV, Loeb S, Landman AB et al. Regional variation in total cost per radical prostatectomy in the healthcare cost and utilization project nationwide inpatient sample database. J. Urol. 183(4), 1504–1509 (2010).
7.
Skinner EC, Tang N, Stevenson K et al. Preparing for bundled payments in urology: defining episodes, evaluating variations in care, and demonstrating improved value. J. Clin. Oncol. 35(8), 11–11 (2017).
8.
Kordan Y, Barocas DA, Altamar HO et al. Comparison of transfusion requirements between open and robotic-assisted laparoscopic radical prostatectomy. BJU Int. 106(7), 1036–1040 (2010).
• Describes the differences in transfusion rates between open and robotic-assisted laparoscopic radical prostatectomy, which supports the preoperative blood ordering recommendations of the maximum surgical blood order schedule (MSBOS) described in this paper.
9.
Leow JJ, Chang SL, Meyer CP et al. Robot-assisted versus open radical prostatectomy: a contemporary analysis of an all-payer discharge database. Eur. Urol. 70(5), 837–845 (2016).
10.
Wallerstedt A, Tyritzis SI, Thorsteinsdottir T et al. Short-term results after robot-assisted laparoscopic radical prostatectomy compared to open radical prostatectomy. Eur. Urol. 67(4), 660–670 (2015).
11.
Frank SM, Rothschild JA, Masear CG et al. Optimizing preoperative blood ordering with data acquired from an anesthesia information management system. Anesthesiology 118(6), 1286–1297 (2013).
•• Describes how we created our MSBOS via an algorithm that incorporated past blood usage data to make our current preoperative blood ordering recommendations.
12.
Ilic D, Evans SM, Allan CA, Jung JH, Murphy D, Frydenberg M. Laparoscopic and robotic-assisted versus open radical prostatectomy for the treatment of localised prostate cancer. Cochrane Database Syst. Rev. 9, 1–17 (2017).
13.
Yaxley JW, Coughlin GD, Chambers SK et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: early outcomes from a randomised controlled phase 3 study. Lancet 388(10049), 1057–1066 (2016).
14.
McAlpine K, Forster Md AJ, Breau RH et al. Robotic surgery improves transfusion rate and perioperative outcomes using a broad implementation process and multiple surgeon learning curves. Can. Urol. Assoc. 13(6), 184 (2018).
15.
Frank SM, Savage WJ, Rothschild JA et al. Variability in blood and blood component utilization as assessed by an anesthesia information management system. Anesthesiology 117(1), 99–106 (2012).
•• Describes our institutional blood management database.
16.
Novara G, Ficarra V, Rosen RC et al. Systematic review and meta-analysis of perioperative outcomes and complications after robot-assisted radical prostatectomy. Eur. Urol. 62(3), 431–452 (2012).
17.
Tang K, Jiang K, Chen H, Chen Z, Xu H, Ye Z. Robotic vs. retropubic radical prostatectomy in prostate cancer: a systematic review and a meta-analysis update. Oncotarget 8(19), 32237–32257 (2017).
18.
Schiffmann J, Larcher A, Sun M et al. Differences in patient characteristics among men choosing open or robot-assisted radical prostatectomy in contemporary practice. Urol. Int. 98(1), 40–48 (2017).
19.
Basiri A, de la Rosette JJ, Tabatabaei S, Woo HH, Laguna MP, Shemshaki H. Comparison of retropubic, laparoscopic and robotic radical prostatectomy: who is the winner? World J. Urol. 36(4), 609–621 (2018).
20.
Moul JW, Sun L, Wu H et al. Factors associated with blood loss during radical prostatectomy for localized prostate cancer in the prostate-specific antigen (PSA)-era: an overview of the Department of Defense (DOD) Center for Prostate Disease Research (CPDR) national database. Urol. Oncol. 21(6), 447–455 (2003).
21.
Haese A, Knipper S, Isbarn H et al. A comparative study of robot-assisted and open radical prostatectomy in 10,790 men treated by highly trained surgeons for both procedures. BJU Int. 123(6), 1031–1040 (2019).
• Demonstrates the low transfusion rates for radical prostatectomies and further validates our current preoperative blood ordering recommendations.
22.
Hyams ES, Mullins JK, Pierorazio PM, Partin AW, Allaf ME, Matlaga BR. Impact of robotic technique and surgical volume on the cost of radical prostatectomy. J. Endourol. 27(3), 298–303 (2013).
23.
Bolenz C, Freedland SJ, Hollenbeck BK et al. Costs of radical prostatectomy for prostate cancer: a systematic review. Eur. Urol. 65(2), 316–324 (2014).
24.
Schroeck FR, Jacobs BL, Bhayani SB, Nguyen PL, Penson D, Hu J. Cost of new technologies in prostate cancer treatment: systematic review of costs and cost–effectiveness of robotic-assisted laparoscopic prostatectomy, intensity-modulated radiotherapy, and proton beam therapy. Eur. Urol. 72(5), 712–735 (2017).
25.
Mukherjee K, Kamal KM. Variation in prostate surgery costs and outcomes in the USA: robot-assisted versus open radical prostatectomy. J. Comp. Eff. Res. 8(3), 143–155 (2019).
26.
(. American Society of Anesthesiologists Task Force on Perioperative Blood M. Practice guidelines for perioperative blood management: an updated report. Anesthesiology 122(2), 241–275 (2015).
27.
Goodell PP, Uhl L, Mohammed M, Powers AA. Risk of hemolytic transfusion reactions following emergency-release RBC transfusion. Am. J. Clin. Path. 134(2), 202–206 (2010).
28.
Dutton RP, Shih D, Edelman BB, Hess J, Scalea TM. Safety of uncrossmatched type-O red cells for resuscitation from hemorrhagic shock. J. Traum. 59(6), 1445–1449 (2005).
29.
White MJ, Hazard SW, Frank SM et al. The evolution of perioperative transfusion testing and blood ordering. Anesth. Analg. 120(6), 1196–1203 (2015).
Information & Authors
Information
Published In
Pages: 219 - 226
PubMed: 32043362
Copyright
© 2020 Future Medicine Ltd.
History
Received: 21 August 2019
Accepted: 17 December 2019
Published online: 11 February 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Reducing preoperative blood orders and costs for radical prostatectomy. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0126
Export citation
Select the citation format you wish to export for this article or chapter.