Comparison of conservative treatment with appendectomy for acute uncomplicated pediatric appendicitis: a meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: We aimed to compare conservative treatment with surgery for uncomplicated pediatric appendicitis to estimate effectiveness and safety. Methods: Data recorded until September 2018 were searched, and relevant academic articles from PubMed, EMBASE, the Cochrane Library and other libraries were selected. STATA version 13.0 (Stata Corporation, TX, USA) was used for statistical analysis. Results: We identified nine eligible papers. The study reported a significant difference in the success rate of treatment in 1 month and in 1 year, and no difference in the incidence of complications. The patients with fecaliths showed low treatment efficacy in conservative treatment group (p < 0.05). Conclusion: Standardized conservative treatment as inpatients for pediatric appendicitis is safe and feasible. Appendectomy was the better choice for patients with fecaliths.
In children, acute appendicitis is the most prevalent gastrointestinal disease [1]. Approximately 1–4 children in 1000 undergo appendectomy per year [2]. Although surgery has been the gold standard in the treatment of pediatric appendicitis, it is an intra-abdominal intervention that requires general anesthesia. The incidence rate of complications of surgery or anesthesia is about 10% within 30 postoperative days [3]. In addition, even with current imaging methods, a normal appendix may be found during appendectomy.
Conservative treatment of appendicitis can be a viable alternative. Several clinical trials and meta-analyses in adults have demonstrated conservative management to be an effective treatment for acute uncomplicated appendicitis [4–10]. However, the conclusions reached in the case of adults may not be applicable to pediatric patients owing to the difference in the clinical scenario as well as development of acute appendicitis in them. There are some studies on the conservative treatment of acute simple appendicitis in children. Recent studies have shown a 75–80% success rate for conservative management in simple pediatric appendicitis [11–19]. However, the treatment of the uncomplicated appendicitis is still a debatable point.
The purpose of our study was to perform meta-analysis comparing conservative treatment with surgery for uncomplicated pediatric appendicitis to estimate the effectiveness and safety of conservative treatment.
Materials & methods
We conducted a meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement standards.
Literature & search strategy
Two independent researchers performed a systematic search of the electronic databases including EMBASE, PubMed and the Cochrane Library, and in other databases to identify randomized controlled trials (RCTs) and randomized cohort studies (RCS) on conservative treatment for acute uncomplicated appendicitis recorded from the initial establishment of electronic databases to September 2018. We used a structured search strategy in combination with Boolean logic: (child OR children OR pediatric patients) AND (uncomplicated appendicitis) AND (nonoperation OR conservative treatment OR antibiotic treatment) AND (appendectomy OR operation). In addition, we checked the reference list of the studies to identify other trials that might potentially qualify for inclusion in the meta-analysis. The process was completed when no further studies could be determined. In case of more than one publication available for a study, we used either the most recent publication or the one with the most relevant information.
Inclusion & exclusion criteria
We included all RCTs and RCS which matched the following inclusion criteria: population: children with acute uncomplicated appendicitis; intervention: conservative treatment; comparison intervention: appendectomy; and outcomes, including more than one of the following outcomes. Exclusion criteria were as follows: non-English language studies; animal studies; studies including complicated appendicitis (abscess, perforation); studies that involved adults and patients with other diseases such as appendix tumor. Two independent authors evaluated all the articles of all recognized studies according to the criteria.
Data extraction & risk of bias assessment
We created an electronic data extraction spreadsheet that included the following information: general trial parameters, demographic characteristics, diagnostic measurements, treatment regimens and outcomes. Two independent authors conducted data collection and disagreements were resolved by discussion. We have presented all the data in Table 1.
| Study (year) | Design | Setting | Simple size | No. of NOM | Patients | Gender (M) | Ref. |
|---|---|---|---|---|---|---|---|
| Svensson et al. (2015) | Randomized pilot trial | Single center | 50 | 24 | Age 5–15 y, diagnosis of acute nonperforated appendicitis, diagnosis made by history, inflammatory markers (WBC count and CRP level) and imaging | 26 | [17] |
| Minneci et al. (2016) | Prospective nonrandomized controlled trial | Single center | 102 | 37 | Age 7–17 y, diagnosis of acute uncomplicated appendicitis, diagnosis made by history, inflammatory markers (WBC count), and imaging; without appendicolith | 69 | [18] |
| Mudri et al. (2017) | Retrospective choice cohort | Multicenter | 52 | 26 | Mean age 6–17 y, diagnosis of acute uncomplicated appendicitis, diagnosis made by history, and imaging (US) | 25 | [20] |
| Hartwich et al. (2016) | Prospective nonrandomized controlled trial | Single center | 74 | 24 | Aged 5–18 y; diagnosis of acute uncomplicated appendicitis, diagnosis made by history, physical examination, inflammatory markers and imaging (US or/and MRI) findings | 34 | [14] |
| Tanaka et al. (2015) | Prospective nonrandomized controlled trial | Single center | 164 | 78 | Aged 6–15 y; diagnosis of acute uncomplicated appendicitis, diagnosis made by physical examination, blood test and imaging findings | 113 | [19] |
| Mahida et al. (2016) | Prospective nonrandomized controlled trial | Single center | 14 | 5 | Aged 9–15 y; diagnosis of acute uncomplicated appendicitis with appendicolith, diagnosis made by clinical history and examination (US, CT and blood test) findings | 6 | [21] |
| Gorter et al. (2017) | Prospective cohort study | Multicenter | 44 | 25 | Aged 7–17 y; diagnosis of acute uncomplicated appendicitis; excluded signs of severe general illness, faecalith, complex appendicitis, significant co-morbidity, allergy for the antibiotics | 29 | [22] |
| Hall et al. (2017) | Randomized pilot trial | Multicenter | 102 | 52 | Aged 3–15 y, acute appendicitis and an appendix mass, successfully treated nonoperatively during the acute stage of the illness; excluded coexisting gastrointestinal disease, a substantial coexisting medical condition or immune defect | 51 | [23] |
| Bachur et al. (2017) | Retrospective study | Multicenter | 63938 | 2416 | Aged <19 y, diagnosis of acute uncomplicated appendicitis; excluded chronic comorbidities | NR | [24] |
| Intervention | Comparator | Outcomes | Follow-up (average) | ||||
| Intravenous meropenem (10 mg/kg × 3 per 24 h) and metronidazole (20 mg/kg × 1 per 24 h) for at least 48 h; keep nil by mouth for the first 24 h | Preoperative antibiotic prophylaxis with 20 mg/kg of metronidazole then appendectomy | Time to discharge; complications; recurrent appendicitis within 1 year | 12 m | ||||
| Intravenous piperacillin sodium–tazobactam sodium ≥24 h, keep nil by mouth for the first 12 h | Prompt initiation of intravenous antibiotics and laparoscopic appendectomy within 12 h | Not having undergone an appendectomy; complicated appendicitis; disability days for the child and parents; appendicitis-related total health care costs; HRQOL | 12 m | ||||
| Received IV ceftriaxone and Flagyl in hospital; within a 7 days of amoxicillin/Clavulin | 1 preop dose of IV ceftriaxone and Flagyl and appendectomy | Interval appendectomy; readmitted to hospital | 12 m | ||||
| A dose of intravenous piperacillin–tazobactam at 100 mg/kg; intravenous pain medication; diet was advanced ad libitum; ampicillin–clavulanate at 50 mg/kg/d TID with a 1-week course | Appendectomy | Initial success/failure of the treatment; recurrence; interval appendectomy | 14 m | ||||
| Cefmetazole 100 mg/kg/d for 48 h, then sulbactam/ampicillin, 200 mg/kg/g + ceftazidime, 150 mg/kg/d | Appendectomy and prophylactic antibiotics until 48 h after surgery | Interval appendectomy; readmitted to hospital | 4.3 y | ||||
| Intravenous piperacillin–tazobactam with 24 h and amoxicillin–clavulanate with 7 days; keep nil by mouth for the first 12 h | Intravenous piperacillin–tazobactam and underwent urgent appendectomy | Not undergoing appendectomy by 1 year after discharge; complicated appendicitis | 4.7 m | ||||
| intravenous antibiotics; diet restriction; pain medication | Pre-, peri- and postoperative care and appendectomy | Allergy to antibiotics, recurrent appendicitis and other complications related appendicitis, appendectomy, fecalith | 25 m | ||||
| NR | NR | The proportion of recurrent acute appendicitis; hospital admission, days off school or normal daily activities, cost | 12 m | ||||
| NR | NR | ED visits, subsequent hospitalizations, advanced imaging studies, complicated appendicitis perforation; recurrent appendectomy | 12 m | ||||
CT: Computed tomography; ED: Emergence department; HRQOL: Health-related quality of life; IV: Intravenous; NOM: No-operative management; NR: No reported; TID: Three-times per day; US: Ultrasonography; WBC: White blood cell.
Two independent authors evaluated the methodological quality and risk of bias of the included RCTs and RCS, respectively, using the Cochrane Tools and the methodological index for nonrandomized studies (MINORS).
Outcomes
The first outcome of interest in the treatment was the success rate of the initial intervention, which we defined as improvement of symptoms with no need for appendectomy and without recurrence within 1 month to 1 year. Efficacy of surgery was considered as an operation without negative appendectomy findings and/or reoperation. If an interval surgery was performed because of parental wish instead of recurrence, we considered the intervention to be successful. On the contrary, if surgery was performed because of recurrence, even in the case of a normal appendix, we considered the intervention to have failed.
The secondary outcomes relating to the treatment were the rate of associated fecaliths, length of hospital stay, total cost, Health-Related Quality of Life (HRQOL) and complications including perforation, abscess, gangrene and/or postoperative complications after the appendectomy.
Data synthesis & analysis
The results of continuous data (length of hospital stay, length of disability, total cost) were calculated as the MD with 95% CIs. For dichotomous outcome variables, we used an odds ratio (OR) with 95% CIs. All analyses were performed using Stata V13. The difference was considered as statistically significant if p < 0.05. When there was evidence of significant heterogeneity (I2 >50%), random-effects models were used; otherwise, fixed-effects models were used for analysis in accordance with the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0).
Results
Results of search
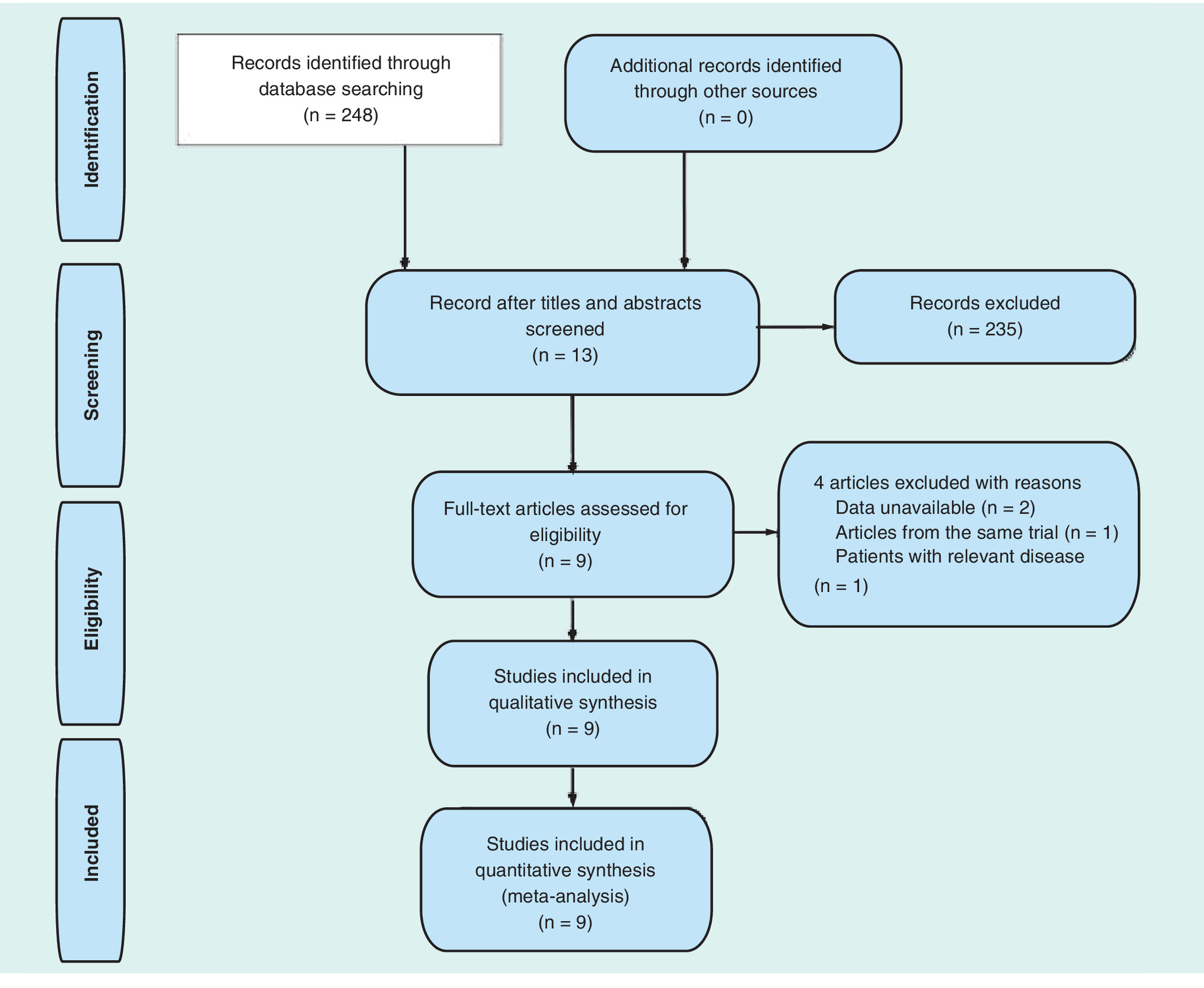
We obtained 248 records from the three databases (PubMed n = 132, EMBASE n = 92 and Cochrane Library n = 92) for the first screening (Figure 1). Glancing over titles and abstracts of the articles, we excluded 235 articles which were clearly not relevant to our criteria. We excluded another four articles after reading the full-text for various reasons (data unavailable, article from the same trial or patients with other relevant disease). Finally, we included nine trials in the meta-analysis [14,17–24].
We summarized the characteristics of the nine included studies as follows: eight studies were performed in hospitals [14,17–23] and one in an emergency department (ED) [24] and 64,540 individuals were incorporated into our trial of whom 61,853 underwent an appendectomy and 2687 underwent conservative treatment. The general trial parameters, demographic characteristics, diagnostic measurements, treatment regimens and outcomes are shown in Table 1. The two RCTs were implemented by Svensson et al. and Hall et al. [17,23].
Study quality & risk of bias
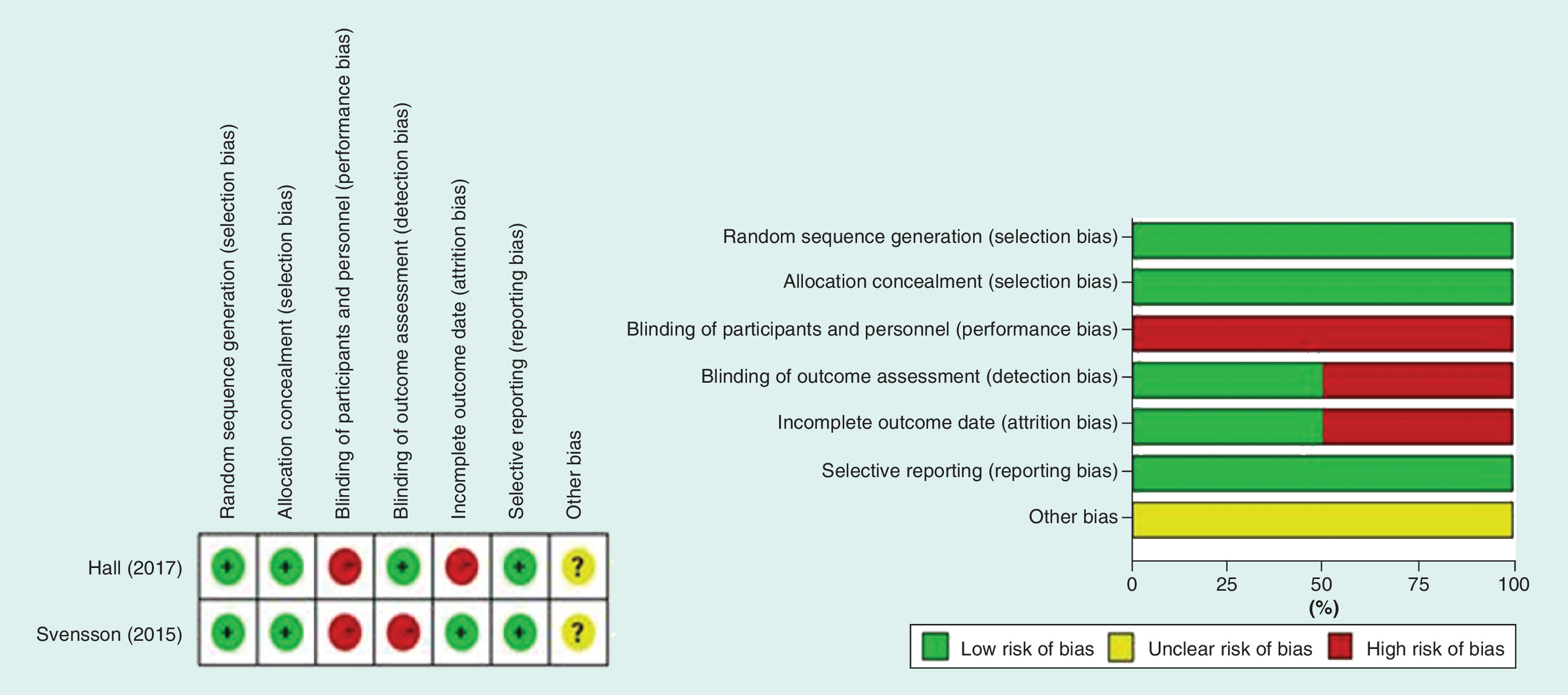
The quality of the included RCTs was evaluated by the scale of Cochrane Tools. The details are showed in Figure 2. The scores of the RCS accessed by MINOR were 18. The details of the quality assessment are summarized in Table 2. Only one study utilized blinded outcome assessment [23].
| Quality assessment for nonrandomized trials | Minneci et al. (2016)† | Mudri et al. (2017)† | Hartwich et al. (2016)† | Tanaka et al. (2015)† | Mahida et al. (2016)† | Gorter et al. (2017)† | Bachur et al. (2017)† |
|---|---|---|---|---|---|---|---|
| A clearly stated aim | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Prospective data collection | 1 | 1 | 2 | 0 | 1 | 2 | 0 |
| End points appropriate to the aim of the study | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Unbiased assessment of the study end point | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| A follow-up period appropriate to the aim of study | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Less than 5% loss to follow-up | 1 | 0 | 0 | 2 | 0 | 0 | 1 |
| Prospective calculation of the sample size | 0 | 0 | 0 | 0 | 2 | 0 | 0 |
| An adequate control group | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Contemporary groups | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Baseline equivalence of groups | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Adequate statistical analyses | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
Outcomes synthesis
Success rate of treatment at 1 month
The success rate of treatment at 1-month follow-up was assessed in six studies [14,17–21]. We found a significant heterogeneity (I2 = 0%; p = 0.959), so that a fixed-effect model was used in the analysis. The success rate was 99% (260/262) in the appendectomy group and 90% (175/194) in the conservative management group (OR: 0.122; 95% CI: 0.041–0.376; p < 0.001, Figure 3). The study by Gorter et al. reported the success rate of treatment at 8-week follow-up, and suggested that it was 100% at 8-week postsurgery in the conservative treatment group [22]. The other two studies did not report the success rate of treatment after the 1-month follow-up [23,24].
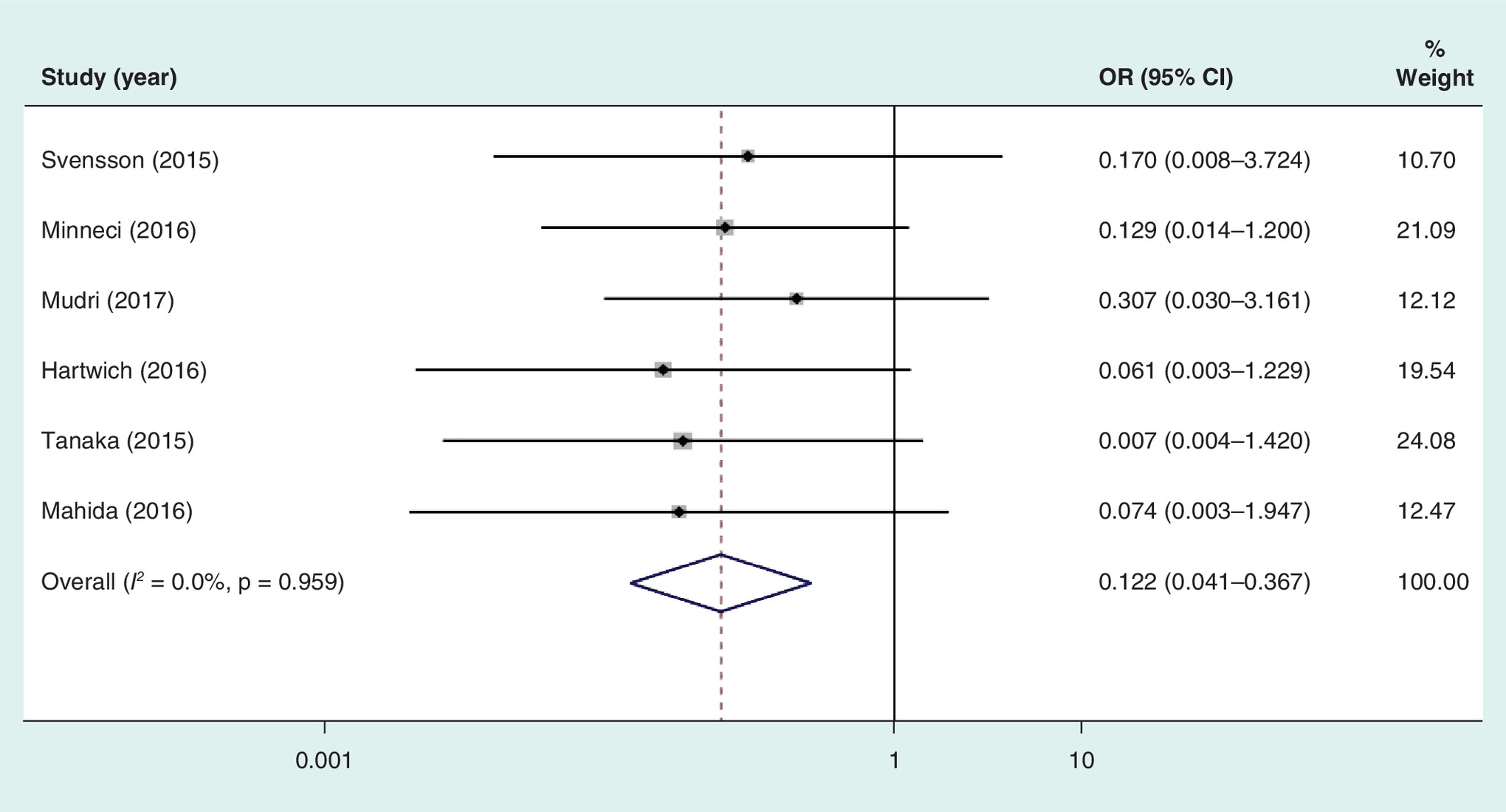
Figure 3. Forest plot showing odds ratio of the success rate in 1 month in the conservative treatment versus appendectomy groups.
OR: Odds ratio.
In the conservative treatment group, 19 of 194 patients (10%) presented with initial failure of conservative treatment; and 16 patients were diagnosed with appendicitis following histopathological examination, with three of them having perforated appendicitis [14,17–19,21]. Mudri et al. could not explain the recurrence of symptoms within 48 h in the three patients who were diagnosed on pathological examination as appendicitis [20]. In their study, nine patients had a recurrence in the 1-year follow-up, of whom only five were diagnosed on pathological examination as appendicitis and four were normal [20]. No one was confirmed to have perforated appendicitis [20]. In the appendectomy group, negative appendectomy findings were observed, except for one (one of 262) patient who experienced a major complication that needed reoperation.
Success rate of treatment within 1 year
Of the 2498 patients allocated to the conservative treatment group, 1098 patients (44.0%) underwent appendectomy within the 1-year follow-up. A significant heterogeneity was observed (I2 = 95.6%; p < 0.001), and we used a randomized-effect model. There was a significant difference in the success rate between the conservative treatment (1400/2498) and appendectomy groups (61,829/61,847; OR: 0.028, 95% CI: 0.001–0.980; p = 0.049, Figure 4) for children with acute uncomplicated appendicitis. Using histopathalogic findings, 43 patients (78.1%, 43/55) were diagnosed with appendicitis in six studies [14,18–20,23,24] and 315 patients (29.5%, 315/1067) were diagnosed with complicated appendicitis in four studies [18–20,24]. Svensson et al. and Hartwich et al. did not report their findings on histological examination [17,21]. Moreover, eight of 46 patients were diagnosed as having a normal appendix based on histopathologic findings.
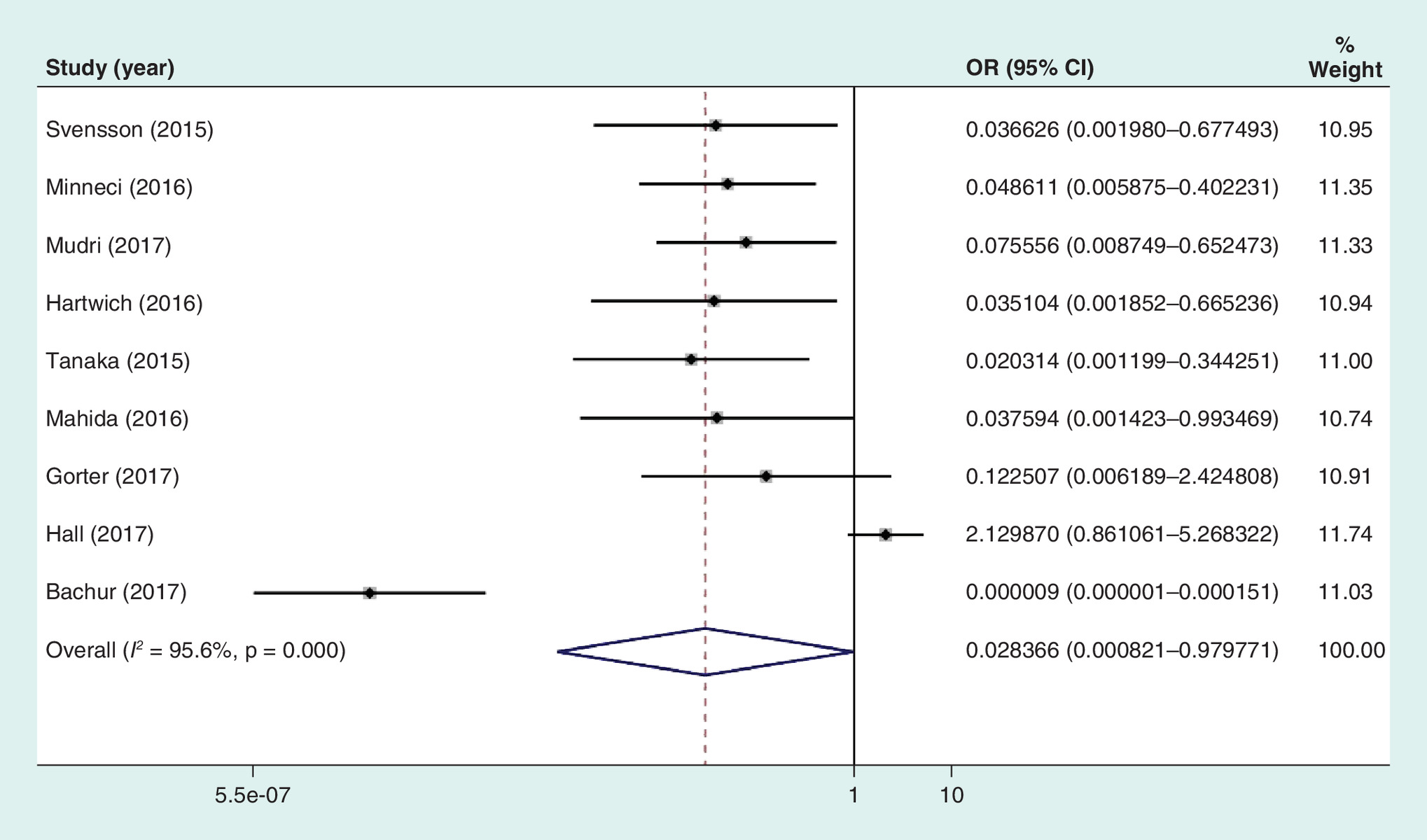
Figure 4. Forest plot showing odds ratio of success rate in 1 year in the conservative treatment versus appendectomy groups.
OR: Odds ratio.
As Bachur et al. had included patients seen in the ED [24], we performed the meta-analysis using the other studies. Conservative treatment was successful in 205 of 271 (75.6%) patients (OR: 0.087; 95% CI: 0.015–0.493; p = 0.006; heterogeneity, I2 = 78.9%; p < 0.001).
Incidence rate of complications
We found no significant difference in the incidence of complications between the conservative treatment group (18/265) and the appendicectomy group (25/316; OR: 0.567; 95% CI: 0.273–1.176; p = 0.127, Figure 5) [14,17–20,22,23]. A low level of heterogeneity existed (I2 = 24.9%; p = 0.239) and we used a fixed-effect model. However, in the operation group, there was a patient who developed laryngospasm during extubation and required reintubation and ICU admission for 4 days [22].
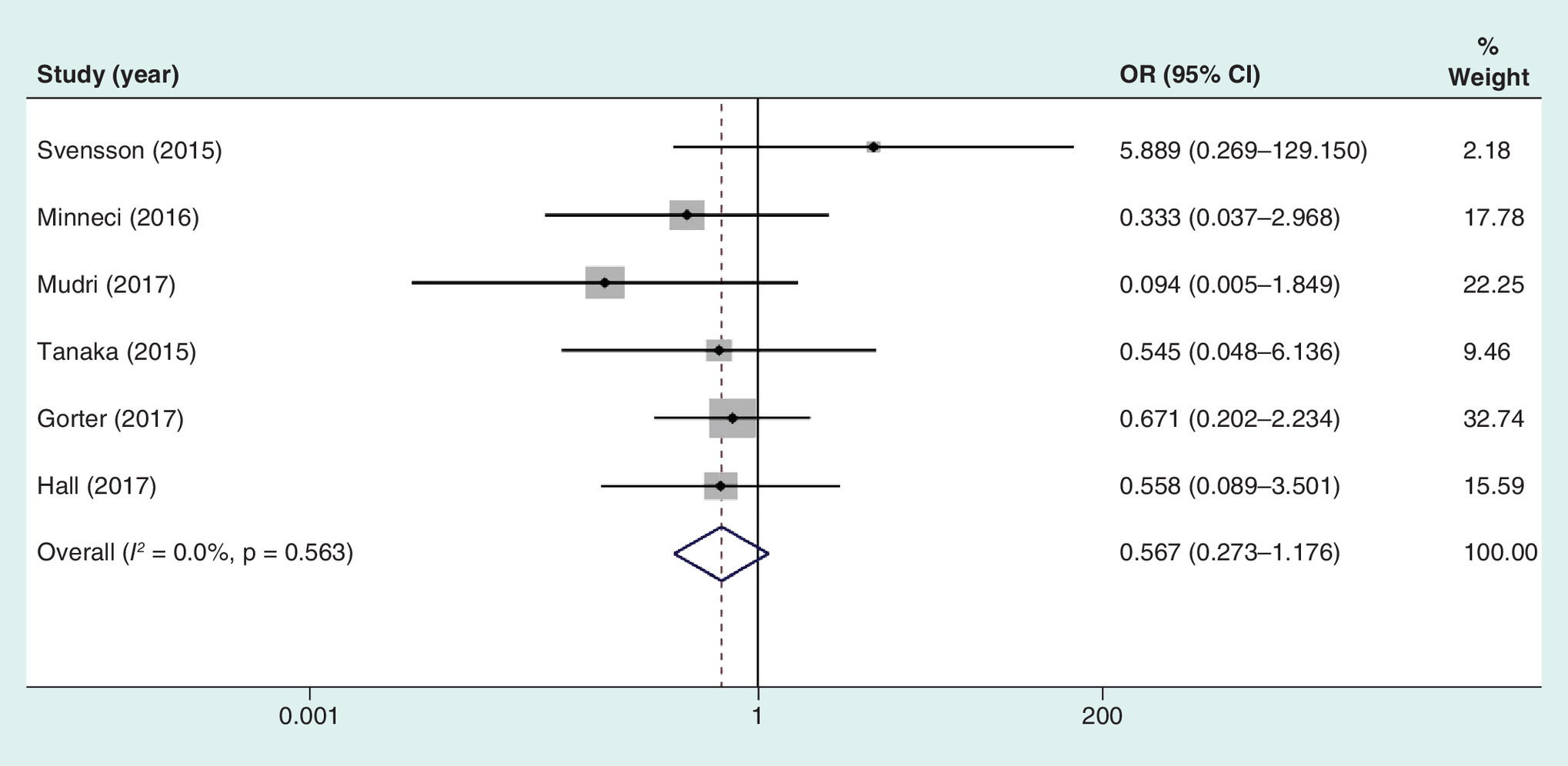
Figure 5. Forest plot showing odds ratio for incidence rate of complications in the conservative treatment versus appendectomy groups.
OR: Odds ratio.
Success rate of appendicolith
We performed a subgroup analysis to show that the success rate of treatment differs in the presence of fecaliths. Of the 11 included studies, six reported the presence of fecaliths [14,17,19–21,23], it was excluded in two [18,22], and Bachur et al. did not report the presence of fecaliths [24]. Compared with that of conservative treatment (25/45), appendectomy (29/29) showed a higher success rate in patients with an appendicolith (OR: 0.073; 95% CI: 0.013–0.400; p = 0.003; heterogeneity, I2 = 0%; p = 0.778, Figure 6). However, we found no statistically significant difference in treatment efficacy between conservative treatment (131/164) and appendectomy (195/212) in patients without a fecalith (OR: 0.475, 95% CI: 0.015–1.699; p = 0.128; heterogeneity, I2 = 82.5%; p < 0.001, Figure 7).
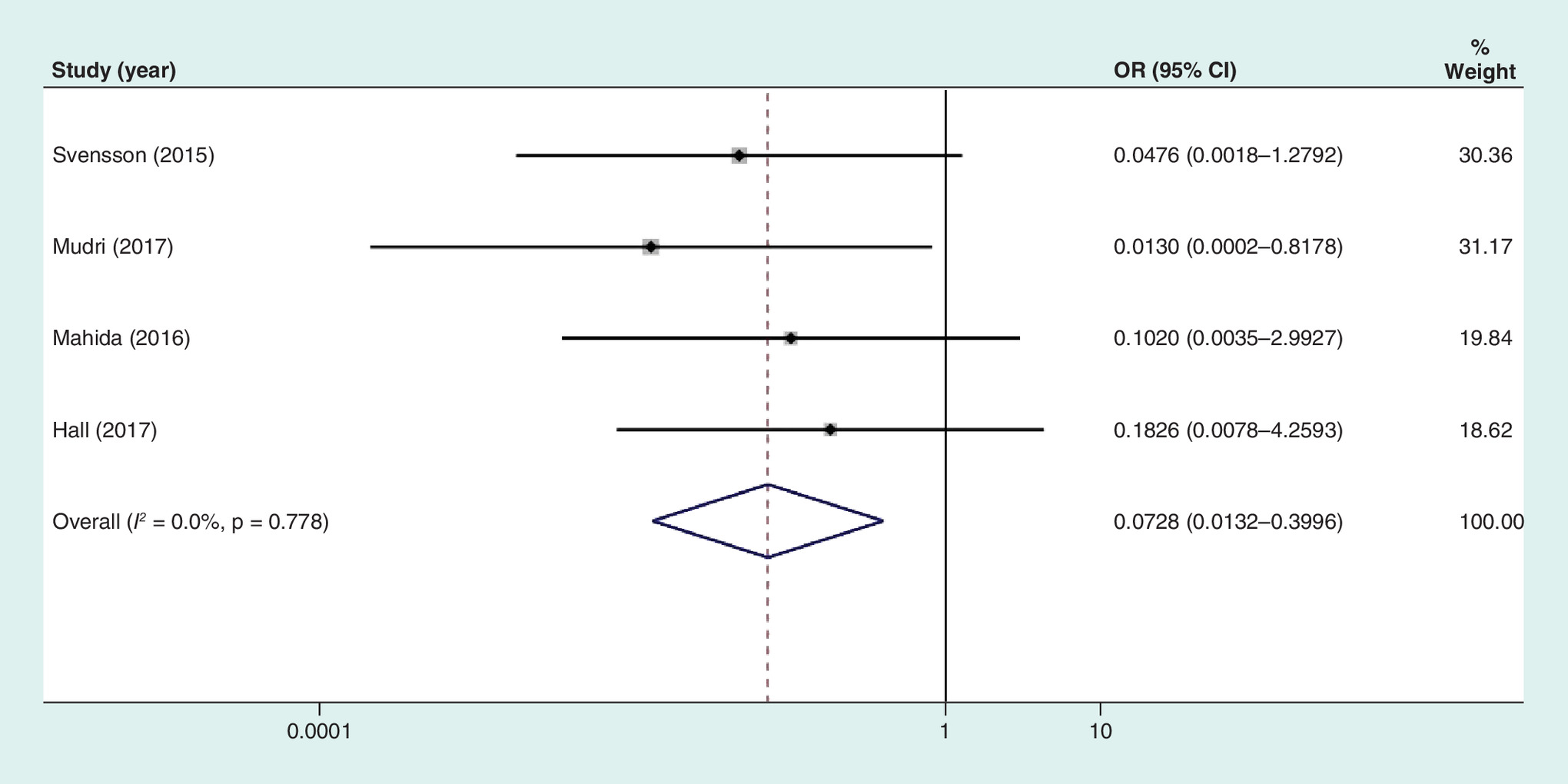
Figure 6. Subgroup forest plot showing odds ratio of the success rate in patients with fecaliths in the conservative treatment versus appendectomy groups.
OR: Odds ratio.

Figure 7. Subgroup forest plot showing odds ratio of the success rate in patients without fecaliths in the conservative treatment versus appendectomy groups.
OR: Odds ratio.
Length of hospital stay
The mean length of hospital stay for conservative treatment of uncomplicated appendicitis ranged from 4.4 to 13.4 h in six studies [17–20,23,24]. However, Mudri et al. only reported the mean of the total length, which was excluded from the meta-analysis [20]. The forest plot showed a longer hospital stay in the conservative treatment group than in the appendectomy group, with a mean difference of 3.293 h, but did not show statistical significance (95% CI: -23.569–16.983 h; p = 0.75; heterogeneity, I2 = 97.4%; p < 0.001).
Furthermore, the mean difference between the two groups in length of disability was 6.767 days with the conservative treatment group having a longer disability period (95% CI: -19.496–5.962 days; p = 0.297; heterogeneity, I 2 = 94.7%; p < 0.001). There was no statistical difference.
Cost
The difference in total appendicitis-associated costs was reported in five studies [14,17,18,20,23], of which four could be included in the meta-analysis. The meta-analysis including the four studies showed that total appendicitis-associated costs increased by US$1.744 in the appendectomy group (95% CI: US$-6.976 to US$3.488; p = 0.514; heterogeneity, I2 = 97.6%; p < 0.001). There was no statistical difference.
Health-related quality of life
Three studies reported on the HRQOL between conservative treatment group and appendectomy group [18,19,22]. However, we could not include them in our meta-analysis owing to some problems with the results, such as strong subjectivity, low follow-up rate and inconsistent assessment methods. Minneci et al. reported on similar quality of life following both treatments by using Quality of Life Inventory instruments in both patients and parents [18]. Conversely, Tanaka et al. found higher patient satisfaction in the appendectomy group [19]. Unfortunately, Gorter et al. failed to obtain the responses to the HRQOL questionnaire in the appendectomy group [22].
Discussion
Surgery has been the standard treatment in acute simple appendicitis owing to concerns of perforation. However, recent trials reveal that conservative treatment might help avoid appendectomy in 83–99% patients with uncomplicated appendicitis in the short-term [11–14,17–19,25,26]. Successful conservative management of acute simple appendicitis helps avoid general anesthesia as well as appendectomy.
We performed a meta-analysis of the reported outcomes between conservative treatment and appendectomy in children with acute uncomplicated appendicitis. Our results revealed no statistical difference between conservative treatment and appendectomy in the incidence of complications, length of hospital stay and total cost associated with appendicitis.
Our study reported the initial success rate of conservative treatment as 90%, whereas the success rate was only 56% in the 1-year follow-up. It should be noted that Bachur et al. included patients with appendicitis from the ED in their study [24]. Bachur et al. reported that differences in patient selection at the onset of treatment, inadequate antibiotic treatment regimens, patient noncompliance or limitations in measuring treatment outcomes by using administrative data led to the increase in the reported fail rate [24]. On excluding the data from the study by Bachur et al., the success rate of conservative treatment was 75.6%, which was similar to the success rate of nonoperative treatment for uncomplicated appendicitis (68–95%) within 1 year according to a meta-analysis in adults [4–10,27]. In addition, although the success rate of treatment in the appendectomy group was 94.5%, it is desirable that the incidence of normal appendix should be lower than the present 4–5% [24,28–31]. Moreover, the consequence of treating a patient with suspected (but unproven) appendicitis with antibiotics would likely be considered more acceptable than undergoing a needless surgery.
We found the incidence rate of complications to be similar with both conservative treatment and appendectomy. Postappendectomy complications have been reported in up to 17% of cases with acute uncomplicated pediatric appendicitis [4,5,7,32]. Gorter et al. reported that one patient experienced a serious complication (re-intubation and ICU admission) after appendectomy [22,31,33,34]. On the contrary, the incidence of complications with conservative management ranges from 0 to -8% in uncomplicated pediatric appendicitis [11–14,17–19,26]. Moreover, all complications were not serious. Furthermore, recent articles have reported no differences in the incidence of perforated appendicitis between those who had undergone surgery following the failure of conservative treatment and those who underwent appendectomy at the outset, which means that appendectomy did not become a more difficult procedure following conservative management for simple pediatric appendicitis [18,35]. There were different pathophysiological characteristics and a lack of linear relationship between simple appendicitis and complex appendicitis, and the delay in surgery was not related to the increased incidence of perforations in children [36–38]. Simple appendicitis can be regarded as an emergency disease different from complex appendicitis. Emergency surgery is not the best way to prevent perforation of the appendix, and an individual management plan should be made according to the clinical characteristics [39–41].
However, we found in our meta-analysis that the success rate of conservative treatment was lower than that for appendectomy in patients with appendicoliths; the success rate of conservative treatment was similar to that of appendectomy in patients without appendicoliths. Similarly, recent articles have reported that the presence of a fecaliths was a risk factor for failure of conservative treatment of simple pediatric appendicitis. The investigative trial had to be terminated in the study by Mahida et al. because the failure rate of the conservative treatment for appendicitis with fecaliths in children was so high that it was unacceptable to both the patients and surgeons [21]. Taken together, it is obviously unreasonable to use conservative treatment for patients with fecaliths. The success rate of conservative management may increase on excluding patients with fecaliths. Therefore, imaging for the presence of appendicoliths is crucial.
No significant difference was noted in the total length of hospital stay in our study. Svensson et al. reported the total length of hospital stay to be longer in the conservative management group than that in the surgery group [17]. A reasonable explanation could be that Svensson et al. requested a minimum of 48 h of intravenous antibiotics [17]. However, Mudri et al. have suggested that the total length of stay in the conservative treatment group is longer than that in the appendectomy group because the conservative treatment group had a high readmission rate due to recurrence [20].
In addition, surgeons differed in their suggestions about the number days required to recuperate, and this might lead to differences in the number of disability days.
We also did not find a significant difference between the two groups for total cost associated with the treatment of appendicitis. Mudri et al. reported that the initial cost of treatment incurred by the appendectomy group was almost double that incurred by the conservative treatment group, but the high recurrence rates led to similar total costs finally [20]. On the contrary, Hartwich et al. found that even considering recurrence and secondary surgery, attempted conservative management of simple appendicitis was still more than US$1000 cheaper than the cost of initial surgery, not considering the surgeon’s and anesthetist’s fees [14]. Similarly, Wu et al. established a model to demonstrate that conservative treatment was more cost-effective than appendectomy for acute simple appendicitis in children [42]. The difference in the results may be explained by the different treatment strategies and charging standards in different centers or regions.
In addition to the defined outcomes, we also evaluated the HRQOL after both treatments as we considered these real-life concerns to be important in establishing the true effectiveness of a treatment. The HRQOL was influenced by several factors. On the one hand, in the conservative management group, HRQOL might be influenced by fear of recurrence, while in the appendectomy group, a few children might suffer from postoperative pain or complications [40]. Tanaka et al. reported that children who underwent appendectomy were more satisfied than the children who received conservative therapy [19]. However, Gorter et al. noted low response rates for HRQOL in the pediatric population [22]. Moreover, the study requires further examination to explore whether there is a statistical difference in the HRQOL between both the treatments because the present satisfaction survey is not a standardized tool and the missing data for 30% of the patients can limit the results.
Huang et al. performed a recent meta-analysis of the related topic and reported similar results of antibiotic therapy being recommended in pediatric patients with uncomplicated appendicitis [43]. However, according to Kessler et al., conservative treatment was not superior to appendectomy because conservative treatment had a higher readmission rate [44]. They explained that many parents tended to opt for interval appendectomy due to worry of relapse. Gorter et al. also reported in their systematic review that conservative treatment could help avoid appendectomy in children, and those who needed a delayed appendectomy had no more postoperative complications than those who underwent an immediate appendectomy [45]. In a systematic review that focused on complicated appendicitis [46], the risk for recurrence in patients who did not undergo interval appendectomy was similar to the risk for morbidity associated with interval appendectomy. Therefore, the key point to be noted from the studies is that uncomplicated appendicitis must be accurately diagnosed, because the development and treatment of the two diseases (uncomplicated appendicitis and complicated appendicitis) are different. Further studies should focus on patient characteristics (such as biomarkers and imaging) to accurately identify uncomplicated appendicitis and predict the failure of conservative management of early uncomplicated appendicitis.
Limitations
The limitations of our study are mentioned in the following points: the follow-up period was only 1 year, while the risk of recurrence is for lifetime; Mahida et al. ended their study within only 4.7 months of the follow-up period; and the included studies were short of some data.
Conclusion
This review provides a detailed and systematically analyzed comparison between conservative treatment and appendectomy for pediatric patients with uncomplicated appendicitis. Standardized conservative treatment as an inpatient for pediatric appendicitis has a high rate of success with a risk for complications comparable to that for appendectomy so it is feasible and effective. However, for patients with appendicoliths, appendectomy is the better choice. We should interpret the quantitative effects with caution because of the large heterogeneity.
Future perspective
Further studies should focus on patient characteristics (such as biomarkers and imaging) to accurately identify uncomplicated appendicitis and predict the failure of conservative management of early uncomplicated appendicitis.
•
In children, acute appendicitis is the most prevalent gastrointestinal disease. Approximately, 1–4 children in 1000 undergo appendectomy per year.
•
Surgery requires general anesthesia and intra-abdominal intervention, and the incidence rate of complications is as high as 10% within 30 postoperative days.
•
It is important to identify whether conservative treatment is effective and safe for acute uncomplicated pediatric appendicitis.
•
The purpose of our study was to perform meta-analysis comparing conservative treatment with surgery for uncomplicated pediatric appendicitis to estimate the effectiveness and safety of conservative treatment.
•
There were no statistically significant differences in the length of stay, total cost and health-related quality of life on comparing the two groups. The study reported a significant difference in the initial success rate of treatment (odds ratio [OR]: 0.122; 95% CI: 0.041–0.367; p < 0.05) and in 1 year (OR: 0.087; 95% CI: 0.015–0.493; p < 0.05).
•
The patients with fecaliths showed low treatment efficacy in the conservative treatment group with a significant difference (OR: 0.073; 95% CI: 0.013–0.004; p < 0.05). For the patients with appendicoliths, appendectomy is the better choice.
•
Conservative treatment was found to be safe and feasible and many patients with acute uncomplicated appendicitis can avoid the risks of the operation and general anesthesia.
•
Our meta-analysis, depending on the existing data, does not provide strong evidence for definite conclusions, while may hint that conservative treatment may be an effective way to treat acute simple appendicitis in children.
Acknowledgements
The authors would like to thank Tianjin Medical University for providing the database.
Authors contributions
LW Bi contributed the most to the study and should be considered first author. BL Yan contributed the same as the first author. LW Bi and BL Yan had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis; study concept and design: all authors. Acquisition, analysis or interpretation of data: LW Bi. Drafting of the manuscript: LW Bi and BL Yan. Critical revision of the manuscript for important intellectual content: QY Yang, HL Cui; statistical analysis: LW Bi; obtained funding: HL Cui; administrative, technical or material support: all authors.
Financial & competing interests disclosure
This work was supported by funding from standardization of endoscopic treatment of acute abdomen in children (no: 14RCGFSY00150). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Gorter RR, Eker HH, Gorter-Stam MA et al. Diagnosis and management of acute appendicitis. EAES consensus development conference 2015. Surg. Endosc. 30(11), 4668–4690 (2016).
2.
Kutasy B, Puri P. Appendicitis in obese children. Pediatr. Surg. Int. 29(6), 537–544 (2013).
3.
Rentea RM, St Peter SD. Pediatric appendicitis. Surg. Clin. North Am. 97(1), 93–112 (2017).
4.
Di Saverio S, Sibilio A, Giorgini E et al. The NOTA Study (Non Operative Treatment for Acute Appendicitis): prospective study on the efficacy and safety of antibiotics (amoxicillin and clavulanic acid) for treating patients with right lower quadrant abdominal pain and long-term follow-up of conservatively treated suspected appendicitis. Ann. Surg. 260(1), 109–117 (2014).
5.
Hansson J, Körner U, Khorram-Manesh A, Solberg A, Lundholm K. Randomized clinical trial of antibiotic therapy versus appendicectomy as primary treatment of acute appendicitis in unselected patients. Br. J. Surg. 96(5), 473–481 (2009).
6.
Hansson J, Körner U, Ludwigs K, Johnsson E, Jönsson C, Lundholm K. Antibiotics as first-line therapy for acute appendicitis: evidence for a change in clinical practice. World J. Surg. 36(9), 2028–2036 (2012).
7.
Salminen P, Paajanen H, Rautio T et al. Antibiotic therapy vs appendectomy for treatment of uncomplicated acute appendicitis: the APPAC Randomized Clinical Trial. JAMA 313(23), 2340–2348 (2015).
8.
Shindoh J, Niwa H, Kawai K et al. Predictive factors for negative outcomes in initial non-operative management of suspected appendicitis. J. Gastrointest. Surg. 14(2), 309–314 (2010).
9.
Styrud J, Eriksson S, Nilsson I et al. Appendectomy versus antibiotic treatment in acute appendicitis. A prospective multicenter randomized controlled trial. World J. Surg. 30(6), 1033–1037 (2006).
10.
Vons C, Barry C, Maitre S et al. Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomised controlled trial. Lancet 377(9777), 1573–1579 (2011).
11.
Abeş M, Petik B, Kazil S. Nonoperative treatment of acute appendicitis in children. J. Pediatr. Surg. 42(8), 1439–1442 (2007).
12.
Armstrong J, Merritt N, Jones S, Scott L, Bütter A. Non-operative management of early, acute appendicitis in children: is it safe and effective? J. Pediatr. Surg. 49(5), 782–785 (2014).
13.
Gorter RR, van der Lee JH, Cense HA et al. Initial antibiotic treatment for acute simple appendicitis in children is safe: short-term results from a multicenter, prospective cohort study. Surgery 157(5), 916–923 (2015).
14.
Hartwich J, Luks FI, Watson-Smith D et al. Nonoperative treatment of acute appendicitis in children: a feasibility study. J. Pediatr. Surg. 51(1), 111–116 (2016).
• Important reference source for conducting meta-analyses.
15.
Kaneko K, Tsuda M. Ultrasound-based decision making in the treatment of acute appendicitis in children. J. Pediatr. Surg. 39(9), 1316–1320 (2004).
16.
Koike Y, Uchida K, Matsushita K et al. Intraluminal appendiceal fluid is a predictive factor for recurrent appendicitis after initial successful non-operative management of uncomplicated appendicitis in pediatric patients. J. Pediatr. Surg. 49(7), 1116–1121 (2014).
17.
Svensson JF, Patkova B, Almström M et al. Nonoperative treatment with antibiotics versus surgery for acute nonperforated appendicitis in children: a pilot randomized controlled trial. Ann. Surg. 261(1), 67–71 (2015).
• Important reference source for conducting meta-analyses.
18.
Minneci PC, Mahida JB, Lodwick DL et al. Effectiveness of patient choice in nonoperative vs surgical management of pediatric uncomplicated acute appendicitis. JAMA Surg. 151(5), 408–415 (2016).
• Important reference source for conducting meta-analyses.
19.
Tanaka Y, Uchida H, Kawashima H et al. Long-term outcomes of operative versus nonoperative treatment for uncomplicated appendicitis. J. Pediatr. Surg. 50(11), 1893–1897 (2015).
• Important reference source for conducting meta-analyses.
20.
Mudri M, Coriolano K, Bütter A. Cost analysis of nonoperative management of acute appendicitis in children. J. Pediatr. Surg. 52(5), 791–794 (2017).
• Important reference source for conducting meta-analyses.
21.
Mahida JB, Lodwick DL, Nacion KM et al. High failure rate of nonoperative management of acute appendicitis with an appendicolith in children. J. Pediatr. Surg. 51(6), 908–911 (2016).
• Important reference source for conducting meta-analyses.
22.
Gorter RR, van der Lee JH, Heijsters FACJ et al. Outcome of initially nonoperative treatment for acute simple appendicitis in children. J. Pediatr. Surg. 53(9), 1849–1854 (2018).
• Important reference source for conducting meta-analyses.
23.
Hall NJ, Eaton S, Stanton MP, Pierro A, Burge DM, CHINA study collaborators and the Paediatric Surgery Trainees Research Network. Active observation versus interval appendicectomy after successful non-operative treatment of an appendix mass in children (CHINA study): an open-label, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2(4), 253–260 (2017).
• Important reference source for conducting meta-analyses.
24.
Bachur RG, Lipsett SC, Monuteaux MC. Outcomes of nonoperative management of uncomplicated appendicitis. Pediatrics 140(1), e20170048 (2017).
• Important reference source for conducting meta-analyses.
25.
Minneci PC, Sulkowski JP, Nacion KM et al. Feasibility of a nonoperative management strategy for uncomplicated acute appendicitis in children. J. Am. Coll. Surg. 219(2), 272–279 (2014).
26.
Steiner Z, Buklan G, Stackievicz R, Gutermacher M, Erez I. A role for conservative antibiotic treatment in early appendicitis in children. J. Pediatr. Surg. 50(9), 1566–1568 (2015).
27.
Eriksson S, Granstrom L. Randomized controlled trial of appendicectomy versus antibiotic therapy for acute appendicitis. Br. J. Surg. 82(2), 166–169 (1995).
28.
Bates MF, Khander A, Steigman SA, Tracy TF Jr, Luks FI. Use of white blood cell count and negative appendectomy rate. Pediatrics 133(1), e39–e44 (2014).
29.
Bachur RG, Hennelly K, Callahan MJ, Chen C, Monuteaux MC. Diagnostic imaging and negative appendectomy rates in children: effects of age and gender. Pediatrics 129(5), 877–884 (2012).
30.
Mariadason JG, Wang WN, Wallack MK, Belmonte A, Matari H. Negative appendicectomy rate as a quality metric in the management of appendicitis: impact of computed tomography, Alvarado score and the definition of negative appendicectomy. Ann. R. Coll. Surg. Engl. 94(6), 395–401 (2012).
31.
Markar SR, Blackburn S, Cobb R et al. Laparoscopic versus open appendectomy for complicated and uncomplicated appendicitis in children. J. Gastrointest. Surg. 16(10), 1993–2004 (2012).
32.
Paudel GR, Agrawal CS, Regmi R, Agrawal S. Conservative treatment in acute appendicitis. JNMA J. Nepal Med. Assoc. 50(180), 295–299 (2010).
33.
Masoomi H, Nguyen NT, Dolich MO et al. Comparison of laparoscopic versus open appendectomy for acute nonperforated and perforated appendicitis in the obese population. Am. J. Surg. 202(6), 733–738 (2011).
34.
Boomer LA, Cooper JN, Anandalwar S et al. Delaying appendectomy does not lead to higher rates of surgical site infections: a multi-institutional analysis of children with appendicitis. Ann. Surg. 264(1), 164–168 (2016).
35.
Podda M, Gerardi C, Cillara N et al. Antibiotic treatment and appendectomy for uncomplicated acute appendicitis in adults and children: a systematic review and meta-analysis. Ann. Surg. (2019) (Epub ahead of print).
36.
Livingston EH, Woodward WA, Sarosi GA, Haley RW. Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management. Ann. Surg. 245(6), 886–892 (2007).
37.
Gurien LA, Wyrick DL, Smith SD, Dassinger MS. Optimal timing of appendectomy in the pediatric population. J. Surg. Res. 202(1), 126–131 (2016).
38.
Serres SK, Cameron DB, Glass CC et al. Time to appendectomy and risk of complicated appendicitis and adverse outcomes in children. JAMA Pediatr. 171(8), 740–746 (2017).
39.
Xu J, Adams S, Liu YC, Karpelowsky J. Nonoperative management in children with early acute appendicitis: a systematic review. J. Pediatr. Surg. 52(9), 1409–1415 (2017).
40.
Caruso AM, Pane A, Garau R et al. Acute appendicitis in children: not only surgical treatment. J. Pediatr. Surg. 52(3), 444–448 (2017).
41.
Lopez JJ, Deans KJ, Minneci PC. Nonoperative management of appendicitis in children. Curr. Opin. Pediatrics 29(3), 358–362 (2017).
42.
Wu JX, Sacks GD, Dawes AJ, DeUgarte D, Lee SL. The cost-effectiveness of nonoperative management versus laparoscopic appendectomy for the treatment of acute, uncomplicated appendicitis in children. J. Pediatr. Surg. 52(7), 1135–1140 (2017).
43.
Huang L, Yin Y, Yang L, Wang C, Li Y, Zhou Z. Comparison of antibiotic therapy and appendectomy for acute uncomplicated appendicitis in children. JAMA Pediatr. 171(5), 426–434 (2017).
•• Important to complement our knowledge of the disease.
44.
Kessler U, Mosbahi S, Walker B et al. Conservative treatment versus surgery for uncomplicated appendicitis in children: a systematic review and meta-analysis. Arch. Dis. Child. 102(12), 1118–1124 (2017).
•• Important to complement our knowledge of the disease.
45.
Gorter RR, The SML, Gorter-Stam MAW et al. Systematic review of nonoperative versus operative treatment of uncomplicated appendicitis. J. Pediatr. Surg. 52(8), 1219–1227 (2017).
•• Important to complement our knowledge of the disease.
46.
Andersson RE, Petzold MG. Nonsurgical treatment of appendiceal abscess or phlegmon: a systematic review and meta-analysis. Ann. Surg. 246(5), 741–748 (2007).
Information & Authors
Information
Published In
Pages: 767 - 780
PubMed: 31137951
Copyright
© 2019 Future Medicine Ltd.
History
Received: 14 March 2019
Accepted: 14 May 2019
Published online: 29 May 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparison of conservative treatment with appendectomy for acute uncomplicated pediatric appendicitis: a meta-analysis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0036
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Toru Futami, Yudai Goto, Miki Toma, Yohei Sanmoto, Torajiro Osada, Takashi Fujimoto, Bin Yamaoka, Takayuki Masuko, Nobuyoshi Asai, Toshihiro Yanai, Ultrasonographic classification for predicting conservative treatment success in children with non-perforated appendicitis: A retrospective single-center study, Journal of Pediatric Surgery, 10.1016/j.jpedsurg.2026.163115, 61, 7, (163115), (2026).
- Simeon Barth, Markus Hufnagel, Lennard Forßmann, Susanne Lagrèze, Stefan Fichtner-Feigl, Dorian Marckmann, Bacterial Pathogens and Antibiotic Resistance Patterns in Pediatric Appendicitis: Implications for Antibiotic Choice, Pediatric Infectious Disease Journal, 10.1097/INF.0000000000005190, 45, 8, (692-698), (2026).
- 东然 于, The Latest Application Progress of Endoscopic Retrograde Appendicitis Treatment in the Treatment of Appendicitis in Children, Advances in Clinical Medicine, 10.12677/acm.2026.1662353, 16, 06, (1407-1416), (2026).
- Yan Lu, Yingzhe Zhang, Letter to the editor regarding: Pediatric complicated appendicitis: Results of a standardized antibiotic protocol in a tertiary center, Journal of Pediatric Surgery, 10.1016/j.jpedsurg.2026.162930, (162930), (2026).
- Amer Al-Ani, Wafa Ibrahim, Kowthar Forsat, Yara Walid Elsherbiny, Mesk Alhammadi, Nada Khaled Matar, Elaf MO Suliman, Haya Elastal, Ahmad Al Amour, Bashir Saddig, Sanjida Afrin, Fethiya Abdu, Systematic Review Comparing Nonoperative Management to Surgical Treatment of Acute Appendicitis in the Presence of a Retained Faecolith, Arab Board Medical Journal, 10.4103/abmj.abmj_47_24, 26, 2, (104-110), (2025).
- Qiuyue Tu, Saif Ullah, Deliang Li, Lingjian Kong, Dan Liu, Ting Wei, Yajuan Li, Qingfen Zheng, Lixia Zhao, Hongwu Xin, Bingrong Liu, Safety and Efficacy of Endoscopic Retrograde Appendicitis Therapy for Pediatric Patients: A Single-Center Retrospective Study in Chinese Children, American Journal of Gastroenterology, 10.14309/ajg.0000000000003428, 120, 12, (2929-2934), (2025).
- Sunjay S. Kumar, Amelia T. Collings, Ryan Lamm, Ivy N. Haskins, Stefan Scholz, Pramod Nepal, Arianne T. Train, Dimitrios I. Athanasiadis, Philip H. Pucher, Joel F. Bradley, Nader M. Hanna, Francisco Quinteros, Nisha Narula, Bethany J. Slater, SAGES guideline for the diagnosis and treatment of appendicitis, Surgical Endoscopy, 10.1007/s00464-024-10813-y, 38, 6, (2974-2994), (2024).
- Mohamed Zarog, Peter O’Leary, Miranda Kiernan, Jarlath Bolger, Paul Tibbitts, Stephen Coffey, Gerard Byrnes, Colin Peirce, Colum Dunne, Calvin Coffey, Circulating fibrocyte percentage and neutrophil-lymphocyte ratio are accurate biomarkers of uncomplicated and complicated appendicitis: a prospective cohort study, International Journal of Surgery, 10.1097/JS9.0000000000000234, 109, 3, (343-351), (2023).
- Jussi Haijanen, Suvi Sippola, Ville Tammilehto, Juha Grönroos, Siiri Mäntyoja, Eliisa Löyttyniemi, Hannele Niiniviita, Paulina Salminen, Diagnostic accuracy using low-dose versus standard radiation dose CT in suspected acute appendicitis: prospective cohort study , British Journal of Surgery, 10.1093/bjs/znab383, 108, 12, (1483-1490), (2021).