Proximal gastrectomy versus total gastrectomy for adenocarcinoma of the esophagogastric junction: a meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare efficacy between total gastrectomy (TG) and proximal gastrectomy (PG) for upper-third gastric cancer. Materials & methods: PubMed, Embase and Cochrane library were searched to select suitable researches. Stata was used for meta-analysis including 5-year overall survival rate, recurrence rate, complication morbidities and serum nutritional levels. Results: Ten retrospective English researches were contained. Our study showed no significant difference of 5-year overall survival rate, recurrence rate, reflux symptoms and anastomotic leakage. TG experienced longer operation time, more lymph nodes-retrieved number, more estimated blood loss and higher ileus, but less anastomotic stricture. PG showed advantages over TG in terms of serum nutritional levels. Conclusion: PG is more preferable to TG for treatment of upper-third gastric cancer.
Over the past few decades, the incidence of upper-third gastric cancer has increased significantly in the USA [1], with the same trend being observed in Asian countries [2]. Upper-third gastric cancer was considered as adenocarcinoma of the upper third of the stomach with or without inclusion of the esophagogastric junction (EGJ). Due to the difference of the location of tumors’ epicenters, the EGJ was divided into three types according to the Siewert classification [3]. Type I: distal esophagus carcinoma with the center located within 1–5 cm above the EGJ; type II: cardia carcinoma with the center located within 1 cm above to 2 cm below the EGJ; type III: gastric carcinoma with the tumor center between 2 and 5 cm below the EGJ. However, it remains controversial of proximal gastrectomy (PG) or total gastrectomy (TG) for treatment of upper-third gastric cancer.
Usually, a more radical lymphadenectomy along with longer tumor-free distal resection margin can be achieved from TG. Also, Yoshitsugu [4] held a point of view that the number of lymph node metastasis was an independent risk factor affecting the survival rate of gastric cancer, which was proportional to the recurrence rate. However, a Japanese nationwide retrospective study showed prophylactic lymphadenectomy around the distal stomach was not likely to be necessary for EGJ cancer <4 cm in diameter [5]. Additionally, PG was known as function preserving and achieved a survival rate similar with that of TG [6,7], and Katai [8] thought that it was a significant purpose of surgical treatment to reduce the extent of radical gastrectomy, which could protect residual stomach function. That is indeed beneficial for residual stomach after PG. Compared with TG, PG has been found to have advantages in terms of reducing postoperative intrinsic factor secretion and absorption of vitamin B12. Jung [9] held the same view that PG improved postoperative nutritional status and reduced the incidence of dumping syndrome and postoperative anemia. Nonetheless, several short-term follow-up researches have demonstrated that postoperative hemoglobin levels were similar when comparing PG and TG [10,11]. Since there has not been a consensus conclusion, the ongoing Korean multicenter randomized controlled trial (KLASS-05) compared PG with TG in terms of efficacy, which was expected to provide more evidence about the nutritional advantages. Its end point included hemoglobin levels at 2 years and cumulative supplementation of vitamin B12 within 2 years postoperatively.
Although PG has some advantages over TG in retaining residual stomach, it is rarely adopted since the possibility of severe postoperative reflux symptoms and anastomotic stenosis, both of which can lead to quality-of-life deterioration. Several reconstructive procedures have so far been adopted, such as esophagogastrostomy (EGS), jejunal interposition with or without a pouch and double tract. However, it remains controversial to achieve better antireflux effect [12]. While some argued that Roux-en-Y reconstruction after TG was associated with lower incidence of reflux esophagitis [6,13] and the ‘Y’ limb can reduce reflux esophagitis theoretically.
The equivalence or benefit between PG and TG is still a debate. To address these disputes, our study aimed to perform a meta-analysis comparing postoperative prognosis (5-year overall survival rate and recurrence rate), postoperative efficacy (operation time, estimated blood loss and number of lymph node retrieved), postoperative complications (anastomotic stricture, anastomotic leakage, ileus and reflux symptoms) and postoperative nutritional levels (albumin, total protein, cholesterol and hemoglobin) for the radical resection of upper-third gastric cancer.
Methods
Search strategy
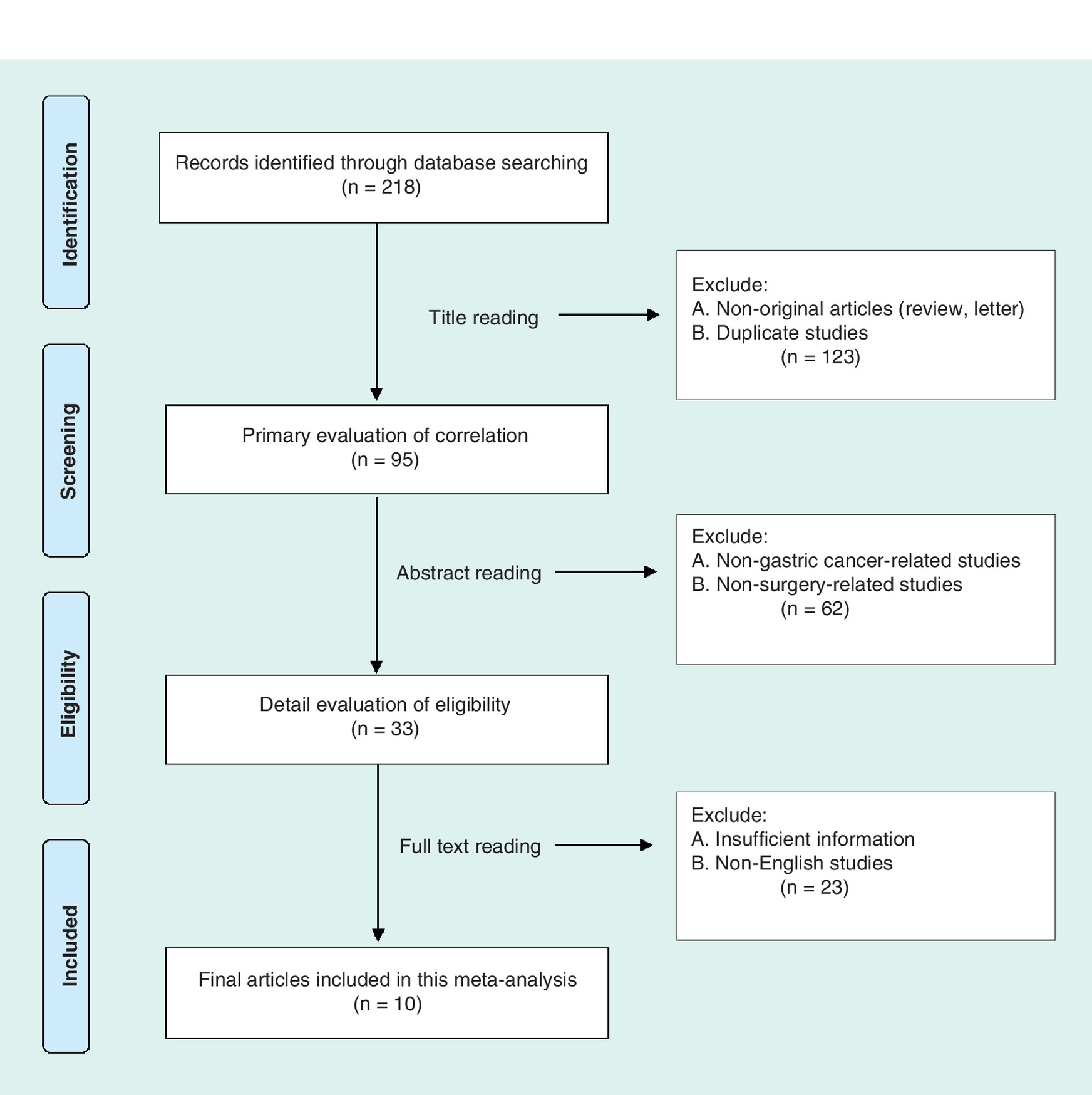
Electronic databases including PubMed (2000–2018.3 [3: March]), Embase (2000–2018.3) and Cochrane library (2000–2018.3) were searched. Language was limited to English. The search progress was conducted as follows in Figure 1. Search strings are ‘proximal gastrectomy’, ‘total gastrectomy’, ‘upper-third gastric cancer’, ‘proximal gastric cancer’, ‘cardia cancer’. Two reviewers carried out the search and assessed independently.
Inclusion criteria
All randomized, prospective and retrospective controlled studies which compared PG with TG for treatment of upper-third gastric cancer were included. Also, patients should be confirmed with pathologic diagnosis and not accepted with preoperative radiotherapy or chemotherapy. In addition, principal outcomes involved 5-year overall survival rate and recurrence rate, subordinate outcomes involved mortality and complication morbidity rates, quality of life (QOL), operation time and nutritional levels, among others.
Exclusion criteria
Proceedings, case reports, comments were not adopted in our study. We excluded studies that had significant differences in tumor stage and reported incomplete baseline information. Also, we excluded small-sized group (<20 patients) or with no long-term follow-up (<12 month) studies.
Data extraction
Two reviewers respectively screened the following of every research: first author, publication year, type of research, inclusion criteria and exclusion criteria.
Data analysis & statistical methods
Stata 15.0 was used to conduct the review. Dichotomous data (5-year overall survival rate, recurrence rate, anastomotic stricture, anastomotic leakage, ileus and reflux symptoms) were presented as odds ratios (ORs) and its 95% CIs. Measurement data (estimated blood loss, operation time, lymph nodes-retrieved number, serum hemoglobin, albumin, total protein and cholesterol level) were presented as weighted mean difference (WMD). Different effect models were selected according to the result of heterogeneity analysis, which was performed using the p-values and I2 values. If the research effect is homogeneous (I2 <50%), then we use the fixed effect model. On the contrary, random effect model was used when there is heterogeneity (I2 >50%). The outcomes were showed by forest plot graphics. The potential publication bias was evaluated by Egger’s tests. Sensitivity analysis was introduced to assess the influence of a single study on the overall assessment. Subgroup analysis was also used to evaluate potential sources of heterogeneity. A p-value < 0.05 was believed as statistically significant.
Results
Search result
First, a total of 218 studies were selected as potentially relevant studies. Afterwards, 123 studies were excluded due to nonoriginal articles (review and letter), and the duplicated researches by browsing the title. The abstracts of the remaining 95 studies were further evaluated and 62 articles among which were ruled out for nongastric cancer-related articles and nonsurgery-related articles. The full texts of the remaining 33 studies were evaluated by two observers, and 23 researches were excluded owing to insufficient data and non-English studies. Eventually, ten retrospective English studies [6,13–21] including 1450 patients (998 by TG vs 452 by PG) were included for analysis (Table 1). Detailed selection process was shown in Figure 1.
| Study (year) | No. | Resection | Reconstruction | n | Stage | Follow-up (month) | Scale NOS | |
|---|---|---|---|---|---|---|---|---|
| EGC | AGC | |||||||
| Shiraishi et al. (2002) | 1 | PG | EGS | 14 | 14 | 0 | 50 | 6/9 |
| TG | R-Y | 20 | 15 | 5 | ||||
| Yoo et al. (2004) | 2 | PG | EGS | 74 | 20 | 54 | 34 | 6/9 |
| TG | R-Y | 185 | 38 | 147 | ||||
| Kim et al. (2006) | 3 | PG | EGS | 43 | 11 | 32 | 47 | 6/9 |
| TG | R-Y | 104 | 16 | 88 | ||||
| Kondh (2007) | 4 | PG | EGS | 10 | 10 | 0 | >60 | 7/9 |
| TG | R-Y | 10 | 10 | 0 | ||||
| An et al. (2008) | 5 | PG | EGS | 89 | 89 | 0 | 40 | 5/9 |
| TG | R-Y | 334 | 334 | 0 | ||||
| Ahn et al. (2013) | 6 | PG | EGS | 50 | 49 | 1 | 44 ± 17 | 7/9 |
| TG | R-Y | 81 | 73 | 8 | 38 ± 22 | |||
| Son et al. (2014) | 7 | PG | EGS | 64 | 64 | 0 | >60 | 6/9 |
| TG | R-Y | 106 | 106 | 0 | ||||
| Kosuga et al. (2015) | 8 | PG | EGS | 25 | 25 | 0 | >36 | 6/9 |
| TG | R-Y | 52 | 52 | 0 | ||||
| Hosoda et al. (2016) | 9 | PG | EGS | 40 | 36 | 4 | 37 | 7/9 |
| TG | R-Y | 59 | 45 | 14 | 42 | |||
| Hayami et al. (2017) | 10 | PG | EGS | 43 | 39 | 4 | 25 | 6/9 |
| TG | R-Y | 47 | 44 | 3 | 49 | |||
| Summary | PG | 452 | 357 | 95 | ||||
| TG | 998 | 733 | 265 | |||||
AGC: Advanced gastric cancer; EGC: Early gastric cancer; EGS: Esophagogastrostomy; NOS: Newcastle–Ottawa scale; PG: Proximal gastrectomy; R-Y: Roux-en-Y esophagojejunostomy; TG: Total gastrectomy.
Study characteristics & quality assessment
The researches included in our study were published between 2000 and 2018. Notably, six involved studies were conducted with open gastrectomy, the rest four studies were all conducted with laparoscopic gastrectomy. The sample size ranged from 20 to 423. The NOS scores varied from 5 to 7, which showed that the qualities of all researches were moderate. More detailed characteristics can be observed in Table 1.
The results of meta-analysis
Association with 5-year overall survival rates & recurrence rate between PG & TG
Our data analysis revealed that PG was comparable with TG on 5-year overall survival rate (OR: 0.95; 95% CI: 0.64–1.40; p = 0.790; Figure 2) and recurrence rate (OR: 3.79; 95% CI: 0.37–38.46; p = 0.260; Figure 3).
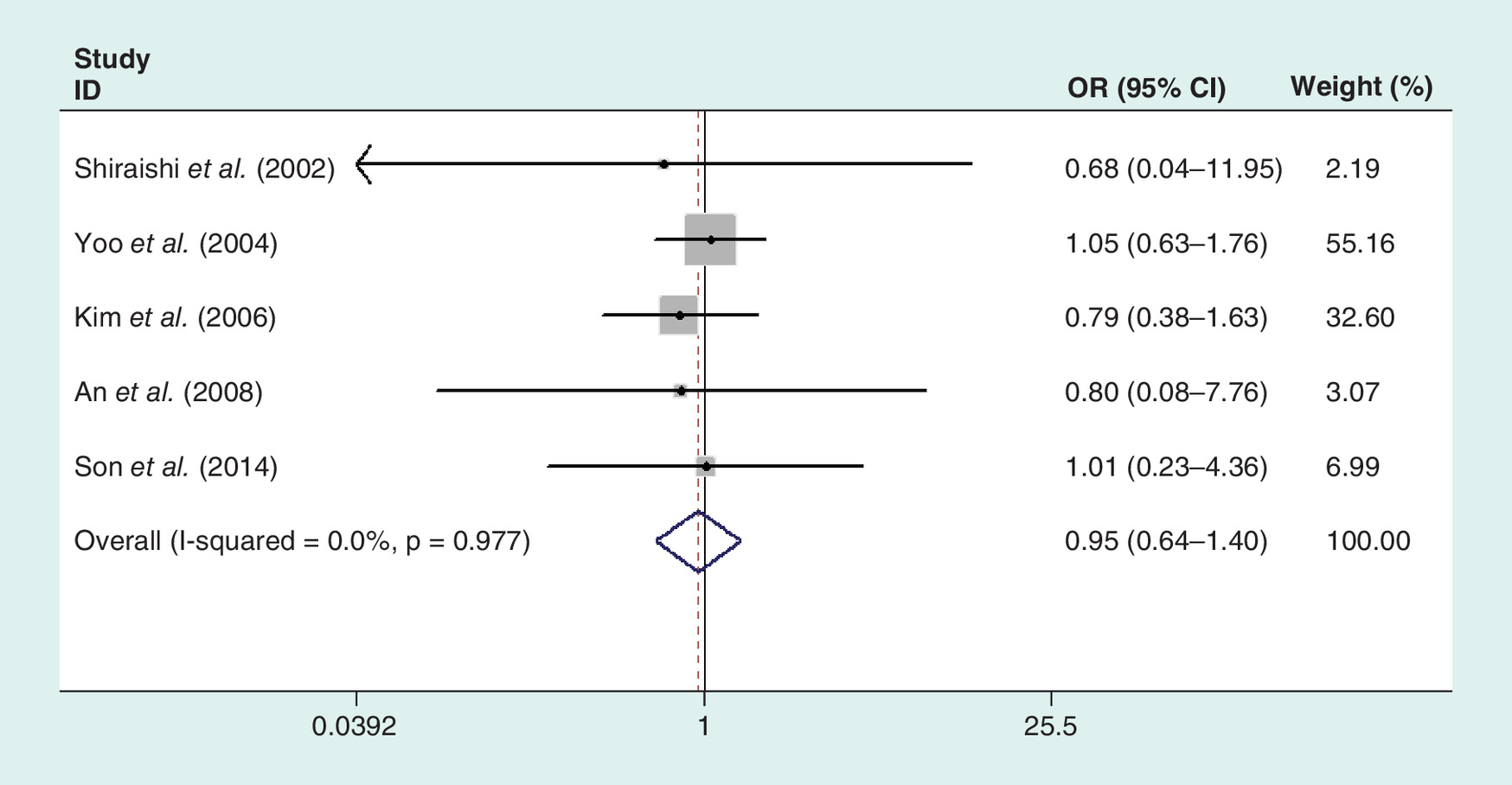
Figure 2. Meta-analysis of 5-year overall survival rate between total and proximal gastrectomies for upper-third gastric cancer.
OR: Odds ratio.
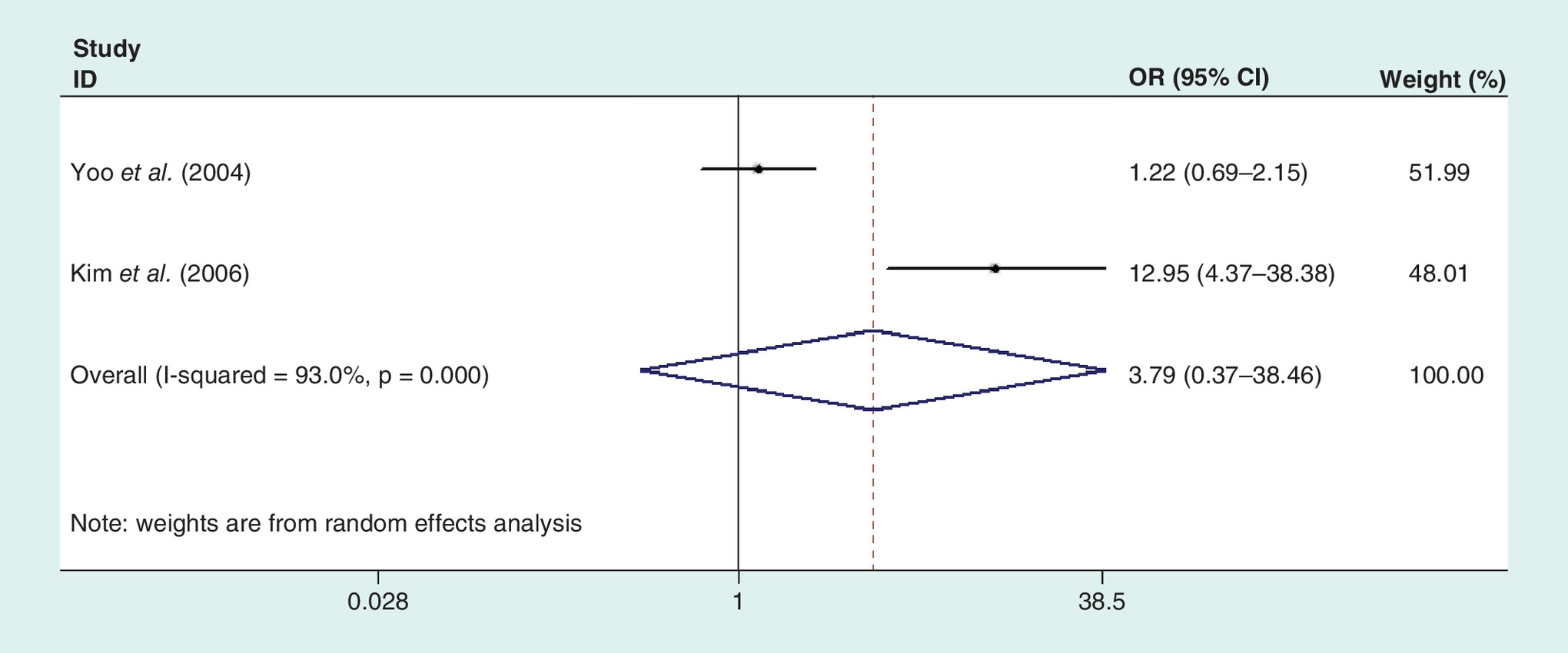
Figure 3. Meta-analysis of recurrence rate between total and proximal gastrectomies for upper-third gastric cancer.
OR: Odds ratio.
Association with intraoperative parameters & postoperative complications between PG & TG
Our data analysis revealed that estimated blood loss could be obviously viewed as lower in PG than TG (WMD = -102.18, 95% CI: -180.41 to -23.94; p = 0.010). Meanwhile, our analysis showed that TG procedure took obviously longer operation time (WMD = -65.47, 95% CI: -103.39 to -27.55; p = 0.001). In addition, PG retrieved less lymph nodes number than TG (WMD = -12.86, 95% CI: -17.44 to -8.28; p = 0.000; Figure 4). Our analysis showed more anastomotic stricture occurred in PG than TG (OR: 3.18; 95% CI: 1.46–6.92; p = 0.004). By the contrary, more ileus occurred among the TG procedure than PG (OR: 0.27; 95% CI: 0.10–0.72; p = 0.010). In addition, our analysis showed no significance in reflux symptoms (OR: 2.69; 95% CI: 0.65–11.11; p = 0.172) and anastomotic leakage (OR: 0.85; 95% CI: 0.38–1.90; p = 0.688; Figure 5).
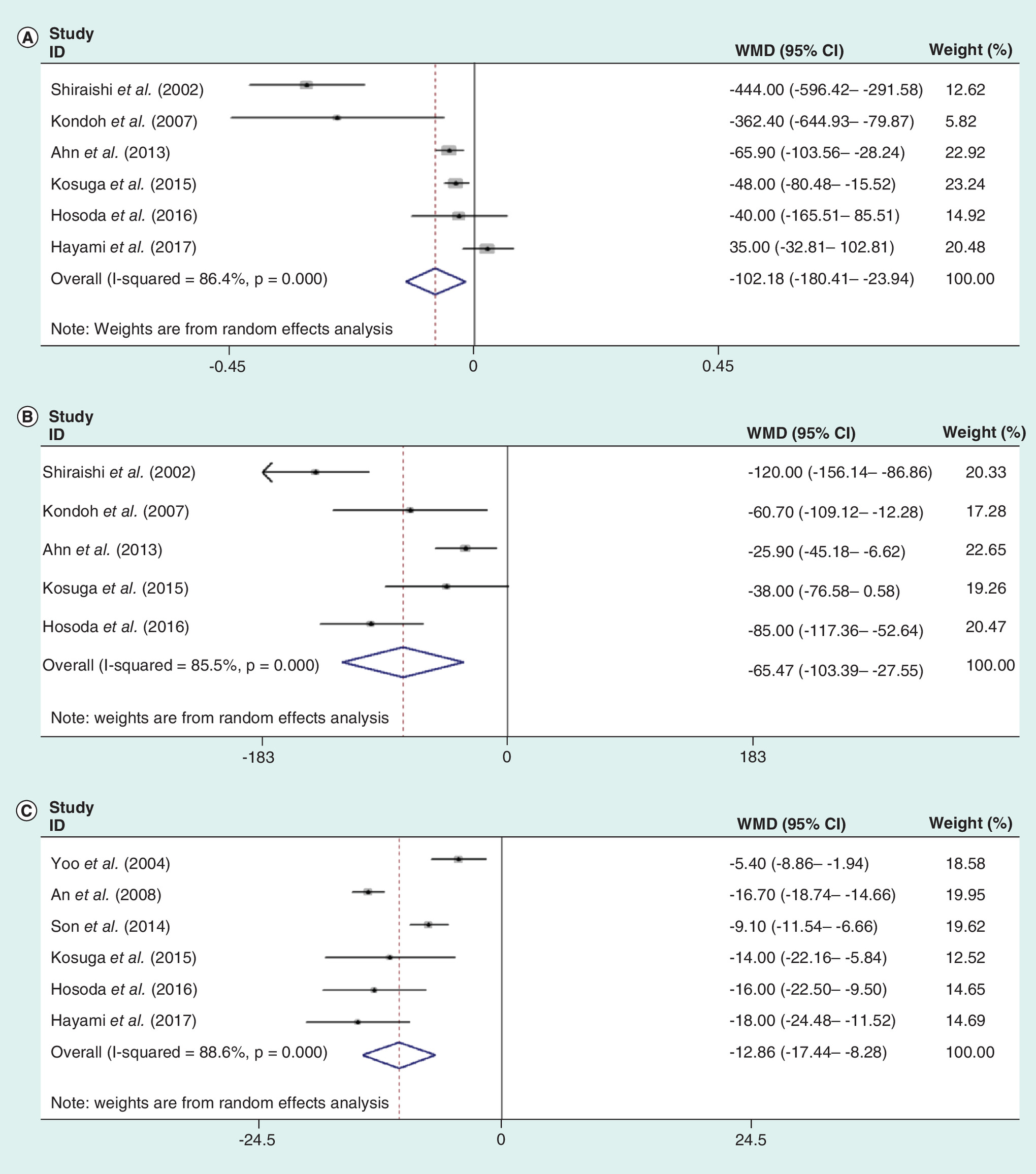
Figure 4. Meta-analysis regarding intraoperative parameters between total and proximal gastrectomies for upper-third gastric cancer.
Meta-analysis regarding estimated blood loss (A), operation time (B), lymph nodes-retrieved number (C) between total and proximal gastrectomies for upper-third gastric cancer.
WMD: Weighted mean difference.
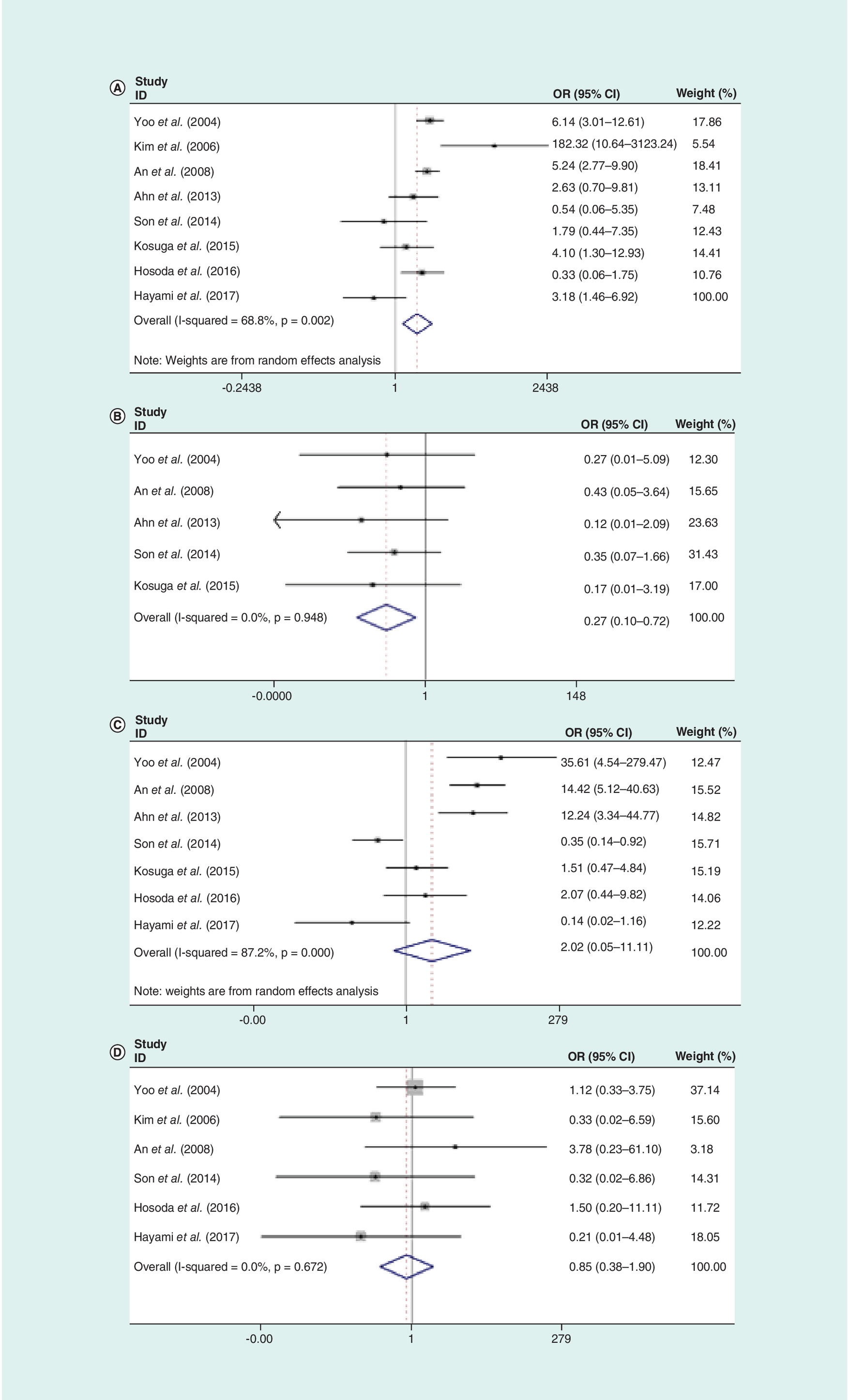
Figure 5. Meta-analysis regarding postoperative complications between total and proximal gastrectomies for upper-third gastric cancer.
Meta-analysis regarding anastomotic stricture (A), ileus (B), reflex symptoms (C), anastomotic leakage (D), between total and proximal gastrectomies for upper-third gastric cancer.
OR: Odds ratio.
Association with postoperative nutritional level between PG & TG
Comparison of nutritional status after PG and TG was conducted. In our study, comparable serum parameters were involved such as albumin, total protein, cholesterol and serum hemoglobin. Higher serum hemoglobin level was observed in the second year follow-up in PG groups (WMD = 0.55, 95% CI: 0.23–0.86; p = 0.004). Furthermore, in the third-year follow-up, PG showed advantages over TG in terms of albumin (WMD = 0.14, 95% CI: 0.044–0.236; p = 0.004), total protein (WMD = 0.25, 95% CI: 0.07–0.42; p = 0.006) and cholesterol (WMD = 6.77, 95% CI: 1.76–11.78; p = 0.08; Figures 6 & 7).

Figure 6. Meta-analysis of serum hemoglobin between total and proximal gastrectomies for upper-third gastric cancer.
2 years follow-up (A); 3 years follow-up (B). Meta-analysis of album between total and proximal gastrectomies for upper-third gastric cancer. 2 years follow-up (C); 3 years follow-up (D).
WMD: Weighted mean difference.
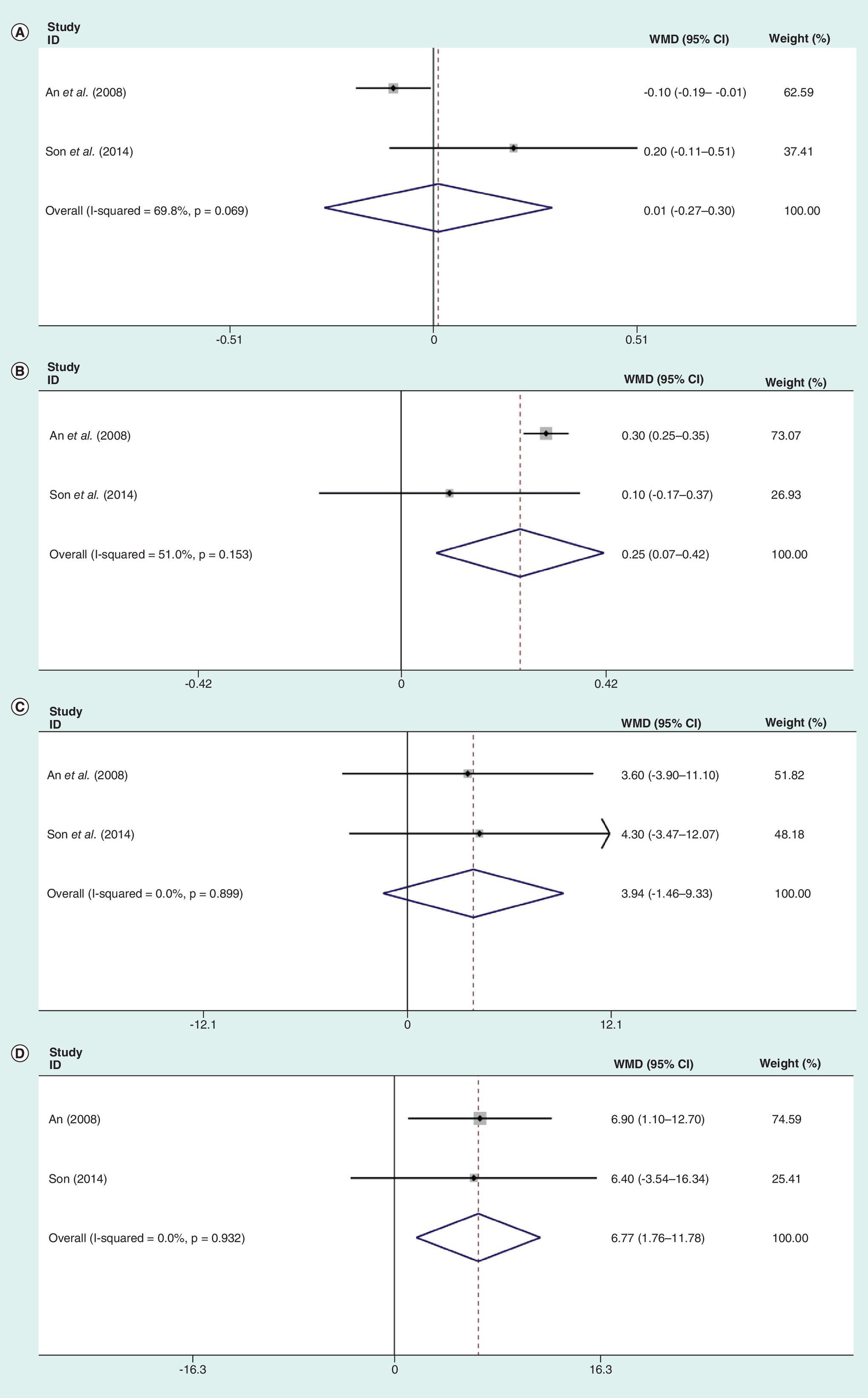
Figure 7. Meta-analysis of total protein between total and proximal gastrectomies for upper-third gastric cancer.
2 years follow-up (A); 3 years follow-up (B). Meta-analysis of cholesterol between total and proximal gastrectomies for upper-third gastric cancer. 2 years follow-up (C); 3 years follow-up (D).
WMD: Weighted mean difference.
Sensitivity analysis & publication bias
Sensitivity analysis was used to assess whether individual research influenced pooled ORs or WMDs by excluding one research in turn. For every meta-analysis, the pooled ORs or WMDs were similar after excluding each study, which verified the stability of meta-analysis.
In our study, Egger’s tests were conducted to detect potential publication bias. According to the outcomes of funnel plot graphics, little publication bias was recognized (Table 2).
| Association between PG and TG | Studies (n) | Overall OR/WMD (95% CI) | Z, POR | Heterogeneity test (I2, Pbias) | Publication bias (Egger’s test) (t, Ppublicationbias) |
|---|---|---|---|---|---|
| 5-year overall survival rate | 1, 2, 3, 5, 7 | 0.95 (0.64–1.40) | 0.31, 0.790 | 0.0%, 0.977 | (-1.13, 0.310) |
| Estimated blood loss | 1, 4, 6, 8, 9, 10 | -102.18 (-180.41 to -23.94) | 3.48, 0.010 | 86.4%, 0.000 | (-1.82, 0.118) |
| Operation time | 1, 4, 6, 8, 9 | -65.47 (-103.39 to -27.55) | 3.93, 0.001 | 85.5%, 0.000 | (-1.92, 0.127) |
| Lymph nodes-retrieved number | 2, 5, 7, 8, 9, 10 | -12.86 (-17.44 to -8.28) | 7.1, 0.000 | 88.6%, 0.000 | (-0.04, 0.966) |
| Anastomotic stricture | 2, 3, 5, 6, 7, 8, 9, 10 | 3.18 (1.46–6.92) | 2.11, 0.004 | 68.8%, 0.002 | (-1.89, 0.091) |
| Reflux symptoms | 2, 5, 6, 7, 8, 9, 10, | 2.69 (0.65–11.11) | 0.99, 0.172 | 87.3%, 0.000 | (-0.36, 0.732) |
| Ileus | 2, 5, 6, 7, 8 | 0.27 (0.10–0.72) | 2.96, 0.010 | 0.0%, 0.948 | (0.45, 0.671) |
| Anastomotic leakage | 2, 3, 4, 6, 7, 9, 11, 13 | 0.85 (0.38–1.90) | 0.82, 0.688 | 0.0%, 0.672 | (-1.50, 0.185) |
OR: Odds ratio; Pbias: P value of heterogeneity test; PG: Proximal gastrectomy; POR: P-value of odds ratio; Ppublication bias: P-value of publication bias; TG: Total gastrectomy; WMD: Weighted mean difference; Z: Z regression coefficient.
Subgroup analysis
Subgroup analysis was mainly conducted on surgical approach, publication year and sample size to explore the potential origins of heterogeneity.
As shown in Table 3, the heterogeneity of estimated blood loss mainly existed in small sample size (n ≤ 90) subgroup (I2 = 91.8%, Pbias = 0.000) and no heterogeneity could be observed in big sample size subgroup (n > 90) (I2 = 0.0%, Pbias = 0.698).
| Subgroup | Studies | OR/WMD (95% CI) | Z | POR/WMD | I2 | Pbias |
|---|---|---|---|---|---|---|
| Estimated blood loss | ||||||
| Surgical approach: | ||||||
| – Open | 2 | -425.60 (-559.75, -291.47) | 6.22 | 0.000 | 0.0% | 0.618 |
| – Laparoscopic | 4 | -36.90 (-75.92, 2.13) | 1.85 | 0.064 | 54.3% | 0.087 |
| Publication year: | ||||||
| – Before 2010 | 2 | -425.60 (-559.75, -291.47) | 6.22 | 0.000 | 0.0% | 0.618 |
| – After 2010 | 4 | -36.90 (-75.92, 2.13) | 1.85 | 0.064 | 54.3% | 0.087 |
| Sample size: | ||||||
| – n >90 | 2 | -63.76 (-99.83, -27.69) | 3.46 | 0.001 | 0.0% | 0.698 |
| – n ≤90 | 4 | -166.57 (-320.36, -12.78) | 2.12 | 0.034 | 91.8% | 0.000 |
| Lymph nodes-retrieved number: | ||||||
| Surgical approach | ||||||
| – Open | 3 | -10.50 (-17.13, -3.88) | 3.11 | 0.002 | 95.0% | 0.000 |
| – Laparoscopic | 3 | -16.28 (-20.28, -12.28) | 7.98 | 0.000 | 0.0% | 0.749 |
| Publication year: | ||||||
| – Before 2010 | 2 | -11.14 (-22.21, -0.07) | 1.97 | 0.049 | 96.7% | 0.000 |
| – After 2010 | 4 | -13.675 (-18.64, -8.70) | 5.40 | 0.000 | 68.8% | 0.022 |
| Sample size: | ||||||
| – n >90 | 4 | -11.64 (-17.30, -5.98) | 4.03 | 0.000 | 92.7% | 0.000 |
| – n ≤90 | 2 | -16.46 (-21.53, -11.38) | 6.36 | 0.000 | 0.0% | 0.452 |
| Operation time: | ||||||
| Surgical approach | ||||||
| – Open | 2 | -93.08 (-150.95, -35.22) | 3.15 | 0.002 | 74.5% | 0.048 |
| – Laparoscopic | 3 | -48.54 (-85.67, -11.42) | 2.56 | 0.010 | 78.9% | 0.009 |
| Publication year: | ||||||
| – Before 2010 | 2 | -93.08 (-150.95, -35.22) | 3.15 | 0.002 | 74.5% | 0.048 |
| – After 2010 | 3 | -48.54 (-85.67, -11.42) | 2.56 | 0.010 | 78.9% | 0.009 |
| Sample size: | ||||||
| – n >90 | 2 | -53.96 (-111.81, 3.88) | 1.83 | 0.067 | 89.4% | 0.002 |
| – n ≤90 | 3 | -74.07 (-127.14, -20.99) | 2.74 | 0.006 | 81.4% | 0.005 |
| Anastomotic structure: | ||||||
| Surgical approach | ||||||
| – Open | 4 | 5.86 (1.94, 17.66) | 3.14 | 0.002 | 71.5% | 0.015 |
| – Laparoscopic | 4 | 1.79 (0.67, 4.78) | 1.16 | 0.248 | 51.7% | 0.102 |
| Publication year: | ||||||
| – Before 2010 | 3 | 8.26 (2.90, 23.50) | 3.95 | 0.000 | 70.4% | 0.034 |
| – After 2010 | 5 | 1.56 (0.63, 3.86) | 0.97 | 0.333 | 45.5% | 0.119 |
| Sample size: | ||||||
| – n >90 | 6 | 4.76 (2.30, 9.83) | 4.21 | 0.000 | 57.2% | 0.039 |
| – n ≤90 | 2 | 0. 82(0.16, 4.27) | 0.24 | 0.812 | 56.7% | 0.129 |
| Reflux symptoms: | ||||||
| Surgical approach | ||||||
| – Open | 3 | 5.24 (0.28, 98.02) | 1.11 | 0.268 | 94.0% | 0.000 |
| – Laparoscopic | 4 | 1.75 (0.36, 8.52) | 0.69 | 0.488 | 78.1% | 0.003 |
| Publication year | ||||||
| – Before 2010 | 2 | 17.31 (6.86, 43.67) | 6.04 | 0.000 | 0.0% | 0.427 |
| – After 2010 | 5 | 1.21 (0.29, 5.13) | 0.26 | 0.792 | 82.8% | 0.000 |
| Sample size | ||||||
| – n >90 | 5 | 5.06 (0.85, 30.04) | 1.78 | 0.075 | 89.5% | 0.000 |
| – n ≤90 | 2 | 0.54 (0.05, 5.86) | 0.51 | 0.608 | 74.6% | 0.047 |
n: Number of sample size; OR: Odds ratio; Pbias: P value of heterogeneity test; POR: P value of odds ratio; WMD: Weighted mean difference; Z: Z regression coefficient.
Similarly, surgical approach, sample size and publication year influenced the results of lymph node-retrieved number (Table 3; POR all < 0.05). When divided by surgical approach, no heterogeneity could be observed in laparoscopic subgroup (I2 = 0.0%, Pbias = 0.749) and high heterogeneity could be observed in open subgroup (I2 = 95.0%, Pbias = 0.000).
Even surgical approach, publication year and sample size were conducted to explore the potential origins of heterogeneity of operation time, we could not find out heterogeneous source.
Also, the heterogeneity of anastomotic stricture mainly existed in before 2010 subgroup (I2 = 70.4%, Pbias = 0.034) and relatively low heterogeneity could be observed in after 2010 subgroup (I2 = 45.5%, Pbias = 0.119).
As shown in Table 3, the heterogeneity of reflux symptoms mainly existed in after 2010 subgroup (I2 = 82.8%, Pbias = 0.000).
Discussion
Surgical resection is currently the main treatment for upper-third gastric cancer. But the extent of optimal gastric resection continues to remain in debate and a final consensus is not yet to be achieved.
Lymph node metastasis was an important factor affecting prognosis [22]. One of the obvious advantages of TG is to reduce positive margin and achieve a more radical lymphadenectomy. Lymph nodes located at the lesser curvature (No.3), right gastroepiploic artery (No.4d), suprapyloric lymph nodes (No.5) and infrapyloric lymph nodes (No.6) are not dissected completely in PG. However, our study showed that PG caused less estimated blood loss, lymph node-retrieved number and shorter operation time. According to our subgroup analysis, the heterogeneity of lymph node-retrieved number mainly existed in open gastrectomy group and small sample size group brought the heterogeneity of estimated blood loss. In open gastrectomy group, the three researches at different times may bring about the heterogeneity. In small sample size group, four researches including half open gastrectomy and half laparoscopic gastrectomy, as different surgical approach, may lead to the heterogeneity. Hosoda [20] held that patients in PG group were expected to be in early stage tumor, so more limited lymph node dissection was adopted, which may shorten operating time and reduce blood loss. Despite the advantage of a more radical lymphadenectomy for TG procedure, there were no statistical significance of 5-year survival and recurrence rate between the two groups according to our study. That may be due to early gastric cancer took the vast majority in our study. Moreover, several studies [23,24] showed that early upper-third gastric cancer was free of metastases to the lymph nodes of preserved sites in the PG group. Additionally, newly published ‘Japanese Gastric Cancer Treatment Guidelines 2014’ recommended that PG was eligible for early cases. Therefore, it seems to be an unnecessary procedure for TG. However, TG is still regarded as the standard surgery for early upper-third gastric cancer in Korea [17].
Current interest can be focused on postoperative complications and improvements in QOL. Our research demonstrated that TG evidently imparted ileus compared with PG. Several studies [25–27] showed that internal hernia was observed only in patients who underwent TG with Roux-en-Y esophagojejunostomy reconstruction. The main reason may be related to abdominal spaces unnaturally created, such as mesenteric defects, jejunojejunostomy-associated mesenteric defects, among others. Besides, internal hernia was a complication known to lead to ileus [28]. Thus, patients with TG may get a higher incidence of ileus.
Reflux symptoms following PG are a primary reason of agony and results in deteriorating the QOL in postoperative patients. Traditionally, PG with EGS is always with high rates of reflux symptoms. As Katsoulis [29] held that 100% of patients suffered reflux symptoms after PG. The main reason is that gastric fluid in the remnant stomach can easily flow back into the esophagus after PG because of absence of the cardia, causing esophageal mucosal damage simultaneously. To overcome the reflux symptoms, various reconstruction methods have been adopted. Hayami [21] reported that severe reflux esophagitis was not observed in PG group with double-flap technique, which preserved the backflow preventer implanted between the submucosa and the serosa flap. Also, Son [18] held that reflux esophagitis following gastric tube reconstruction was observed lower than TG group. Furthermore, Nakane [30] found that patients under PG with pyloroplasty had advantages over those under PG only with food intake, weight recovery and gastric emptying. Recently, a new integrated QOL questionnaire (PGSAS-45) [31,32] has been adopted to assess QOL between different gastrectomies. As Takao [31] indicated that QOL was better in patients with a large remnant stomach, so we considered that PG exceeded TG toward QOL in our research. Moreover, our research showed TG experienced higher incidence of ileus, which may lead to abdominal symptoms included in the questionnaire. Besides, reflux is also one of the items in PGSAS-45. Our research showed that PG was comparable with TG in regard to reflux symptoms. This was due to antireflux measures in PG groups of our incorporated literature, such as EGS (gastric tube), EGS (esophagogastric anterior wall end-to-side anastomosis) and EGS (double-flap technique). Thus, we believe that it is necessary and effective to perform antireflux methods after PG. According to our subgroup analysis, also, these different antireflux measures in after 2010 groups may result in the heterogeneity of reflux symptoms. Besides, when compared with TG, the residual stomach muscle thickened after PG, resulting in scar contracture, which would increase the incidence of anastomotic stricture. Previous findings [6,17] reported that high rates of anastomotic stricture after PG were associated with inflammation caused by reflux. This was consistent with our findings. Furthermore, the occurrence rate of anastomotic leakage in PG was similarly low to that in TG. Deeper understanding of the risk factors, meticulous and experienced surgical techniques may have greatly contributed to the reduced incidence of anastomotic leakage.
Changes in albumin, total protein, cholesterol and hemoglobin levels could be observed in both PG and TG, which are the biochemical markers of the nutritional status of patients. Our study found that long-term outcomes of all the biochemical markers in the PG group were significantly higher than TG. That may be contributed by the preservation of the gastric fundic gland region in PG groups, which contributed to the maintenance of secretion of gastric acid and production of Castle intrinsic factor [19]. Additionally, absorptive function of dietary iron was depended on duodenal passage of food [33]. According to these mechanisms, PG may have the potential advantages over TG with regard to iron and vitamin B12 deficiency anemia [34]. Other nutritional indexes, such as BMIs, triceps skin fold thicknesses and midarm muscle circumferences, were not assessed in our study because of lack of appropriate data. However, generally, our data suggest that PG offers advantage over TG with regard to long-term nutritional levels.
Conclusion
The meta-analysis of current evidence showed that PG was a feasible and safe alternative to TG with 5-year overall survival rate, recurrence rate and reflux symptoms. PG was found to have significant advantages over TG in terms of surgical safety, postoperative long-term nutritional levels and reducing ileus, but more anastomotic stricture. Therefore, PG is more preferable to TG for treatment of upper-third gastric cancer. Furthermore, larger scale cohort studies and more randomized clinical trials are encouraged to evaluate efficacy of surgical procedure for upper-third gastric cancer.
•
Currently, it remains controversial of proximal gastrectomy (PG) or total gastrectomy (TG) for treatment of upper-third gastric cancer.
•
Although a more radical lymphadenectomy along with longer tumor-free distal resection margin can be achieved from TG, PG could achieve a survival rate similar with that of TG.
•
TG seemed to be unnecessary for esophagogastric junction cancer <4 cm in diameter.
•
It has been proved that different antireflux measures are necessary for proximal gastrectomy.
•
There was no difference in 5-year overall survival rate, recurrence rate, reflux symptoms and anastomotic leakage.
•
Our study showed that PG caused less estimated blood loss, lymph node-retrieved number and shorter operation time.
•
Our study showed that TG caused more ileus but less anastomotic stricture.
•
PG showed advantages over TG in terms of serum nutritional levels.
Author contributions
Y Chen designed the study protocol, participated in the data analysis and drafted the manuscript. L Lu, K Fan, D Wang and W Fu participated in the analysis and revision of the manuscript. All authors have read and approved the final manuscript.
Acknowledgment
The authors would like to thank Tianjin Medical University General Hospital for providing the database.
Financial & competing interests disclosure
This research was funded by Tianjin Health Institution Key Projects, grant number ‘15KG148’. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
1.
Buas MF, Vaughan TL. Epidemiology and risk factors for gastroesophageal junction tumors: understanding the rising incidence of this disease. Semin. Radiat. Onc. 23(1), 3–9 (2013).
2.
Hatta W, Tong D, Lee YY, Ichihara S, Uedo N, Gotoda T. Different time trend and management of esophagogastric junction adenocarcinoma in three Asian countries. Dig. Endosc. 29(Suppl. 2), 18–25 (2017).
3.
Siewert JR, Stein HJ. Classification of adenocarcinoma of the oesophagogastric junction. Brit. J. Surg. 85(11), 1457–1459 (1998).
4.
Nakanishi Y, Ohara M, Domen H, Shichinohe T, Hirano S, Ishizaka M. Differences in risk factors between patterns of recurrence in patients after curative resection for advanced gastric carcinoma. World J. Surg. Oncol. 11, 98 (2013).
5.
Yamashita H, Seto Y, Sano T, Makuuchi H, Ando N, Sasako M. Results of a nation-wide retrospective study of lymphadenectomy for esophagogastric junction carcinoma. Gastric Cancer 20(Suppl. 1), 69–83 (2017).
6.
An JY, Youn HG, Choi MG, Noh JH, Sohn TS, Kim S. The difficult choice between total and proximal gastrectomy in proximal early gastric cancer. Am. J. Surg. 196(4), 587–591 (2008).
7.
Sugoor P, Shah S, Dusane R, Desouza A, Goel M, Shrikhande SV. Proximal gastrectomy versus total gastrectomy for proximal third gastric cancer: total gastrectomy is not always necessary. Langenbecks Arch. Surg. 401(5), 687–697 (2016).
8.
Katai H. Function-preserving surgery for gastric cancer. Int. J. Clin. Oncol. 11(5), 357–366 (2006).
9.
Jung DH, Lee Y, Kim DW et al. Laparoscopic proximal gastrectomy with double tract reconstruction is superior to laparoscopic total gastrectomy for proximal early gastric cancer. Surg. Endosc. 31(10), 3961–3969 (2017).
10.
Nozaki I, Hato S, Kobatake T, Ohta K, Kubo Y, Kurita A. Long-term outcome after proximal gastrectomy with jejunal interposition for gastric cancer compared with total gastrectomy. World J. Surg. 37(3), 558–564 (2013).
11.
Zhao P, Xiao SM, Tang LC, Ding Z, Zhou X, Chen XD. Proximal gastrectomy with jejunal interposition and TGRY anastomosis for proximal gastric cancer. World J. Gastroenterol. 20(25), 8268–8273 (2014).
12.
Nakamura M, Yamaue H. Reconstruction after proximal gastrectomy for gastric cancer in the upper third of the stomach: a review of the literature published from 2000 to 2014. Surg. Today 46(5), 517–527 (2016).
13.
Yoo CH, Sohn BH, Han WK, Pae WK. Long-term results of proximal and total gastrectomy for adenocarcinoma of the upper third of the stomach. Cancer Res. Treat. 36(1), 50–55 (2004).
14.
Shiraishi N, Adachi Y, Kitano S, Kakisako K, Inomata M, Yasuda K. Clinical outcome of proximal versus total gastrectomy for proximal gastric cancer. World J. Surg. 26(9), 1150–1154 (2002).
15.
Kim JH, Park SS, Kim J et al. Surgical outcomes for gastric cancer in the upper third of the stomach. World J. Surg. 30(10), 1870–1876; discussion 77–78 (2006).
16.
Kondoh Y, Okamoto Y, Morita M et al. Clinical outcome of proximal gastrectomy in patients with early gastric cancer in the upper third of the stomach. Tokai J. Exp. Clin. Med. 32(2), 48–53 (2007).
17.
Ahn SH, Lee JH, Park DJ, Kim HH. Comparative study of clinical outcomes between laparoscopy-assisted proximal gastrectomy (LAPG) and laparoscopy-assisted total gastrectomy (LATG) for proximal gastric cancer. Gastric Cancer 16(3), 282–289 (2013).
18.
Son MW, Kim YJ, Jeong GA, Cho GS, Lee MS. Long-term outcomes of proximal gastrectomy versus total gastrectomy for upper-third gastric cancer. J. Gastric Cancer 14(4), 246–251 (2014).
19.
Kosuga T, Ichikawa D, Komatsu S et al. Feasibility and nutritional benefits of laparoscopic proximal gastrectomy for early gastric cancer in the upper stomach. Ann. Surg. Oncol. 22(Suppl. 3), S929–S935 (2015).
20.
Hosoda K, Yamashita K, Katada N et al. Potential benefits of laparoscopy-assisted proximal gastrectomy with esophagogastrostomy for cT1 upper-third gastric cancer. Surg. Endosc. 30(8), 3426–3436 (2016).
21.
Hayami M, Hiki N, Nunobe S et al. Clinical outcomes and evaluation of laparoscopic proximal gastrectomy with double-flap technique for early gastric cancer in the upper third of the stomach. Ann. Surg. Oncol. 24(6), 1635–1642 (2017).
22.
Kurokawa Y, Hiki N, Yoshikawa T et al. Mediastinal lymph node metastasis and recurrence in adenocarcinoma of the esophagogastric junction. Surgery 157(3), 551–555 (2015).
23.
Okamura T, Tsujitani S, Korenaga D et al. Lymphadenectomy for cure in patients with early gastric cancer and lymph node metastasis. Am. J. Surg. 155(3), 476–480 (1988).
24.
Kitamura K, Nishida S, Yamamoto K et al. Lymph node metastasis in gastric cancer in the upper third of the stomach – surgical treatment on the basis of the anatomical distribution of positive node. Hepatogastroenterology 45(19), 281–285 (1998).
25.
Miyagaki H, Takiguchi S, Kurokawa Y et al. Recent trend of internal hernia occurrence after gastrectomy for gastric cancer. World J. Surg. 36(4), 851–857 (2012).
26.
Kelly KJ, Allen PJ, Brennan MF, Gollub MJ, Coit DG, Strong VE. Internal hernia after gastrectomy for cancer with Roux-Y reconstruction. Surgery 154(2), 305–311 (2013).
27.
Kimura H, Ishikawa M, Nabae T et al. Internal hernia after laparoscopic gastrectomy with Roux-en-Y reconstruction for gastric cancer. Asian J. Surg. 40(3), 203–209 (2017).
28.
Ojima T, Nakamori M, Nakamura M et al. Internal hernia after laparoscopic total gastrectomy for gastric cancer. Surg. Laparosc. Endosc. Percutan. Tech. 27(6), 470–473 (2017).
29.
Katsoulis IE, Robotis JF, Kouraklis G, Yannopoulos PA. What is the difference between proximal and total gastrectomy regarding postoperative bile reflux into the oesophagus? Dig. Surg. 23(5-6), 325–330 (2006).
30.
Nakane Y, Michiura T, Inoue K et al. Role of pyloroplasty after proximal gastrectomy for cancer. Hepatogastroenterology 51(60), 1867–1871 (2004).
31.
Inada T, Yoshida M, Ikeda M et al. Evaluation of QOL after proximal gastrectomy using a newly developed assessment scale (PGSAS-45). World J. Surg. 38(12), 3152–3162 (2014).
32.
Takiguchi N, Takahashi M, Ikeda M et al. Long-term quality-of-life comparison of total gastrectomy and proximal gastrectomy by postgastrectomy syndrome assessment scale (PGSAS-45): a nationwide multi-institutional study. Gastric Cancer 18(2), 407–416 (2015).
33.
Lee JH, Hyung WJ, Kim HI et al. Method of reconstruction governs iron metabolism after gastrectomy for patients with gastric cancer. Ann. Surg. 258(6), 964–969 (2013).
34.
Hu Y, Kim H, Hyung W et al. Vitamin B(12) deficiency after gastrectomy for gastric cancer: an analysis of clinical patterns and risk factors. Ann. Surg. 258(6), 970–975 (2013).
Information & Authors
Information
Published In
Pages: 753 - 766
PubMed: 31361160
Copyright
© 2019 Future Medicine Ltd.
History
Received: 19 January 2019
Accepted: 15 May 2019
Published online: 30 July 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Proximal gastrectomy versus total gastrectomy for adenocarcinoma of the esophagogastric junction: a meta-analysis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0016
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Tomoyuki Irino, Manabu Ohashi, Masaru Hayami, Rie Makuuchi, Motonari Ri, Takeshi Sano, Toshiharu Yamaguchi, Souya Nunobe, Updated Review of Proximal Gastrectomy for Gastric Cancer or Cancer of the Gastroesophageal Junction, Journal of Gastric Cancer, 10.5230/jgc.2025.25.e12, 25, 1, (228), (2025).
- Shixun Ma, Wei Fang, Leisheng Zhang, Dongdong Chen, Hongwei Tian, Yuntao Ma, Hui Cai, Experience sharing on perioperative clinical management of gastric cancer patients based on the “China Robotic Gastric Cancer Surgery Guidelines”, Perioperative Medicine, 10.1186/s13741-024-00402-x, 13, 1, (2024).
- Wei Dai, Feng Wen, Xiang Li, Zhongxue Fu, The Long-Term Results of Proximal Gastrectomy for Proximal Gastric Cancer: A Propensity Score Matching Analysis Based on SEER Database, The American Surgeon™, 10.1177/00031348241260273, 90, 11, (3015-3023), (2024).
- Peter Kolozsi, Zsolt Varga, Dezso Toth, Indications and technical aspects of proximal gastrectomy, Frontiers in Surgery, 10.3389/fsurg.2023.1115139, 10, (2023).
- Rui Peng, Chao Yue, Wei Wei, Bin Zhou, Xu Wen, Rong-Min Gu, Xue-Zhi Ming, Gang Li, Huan-Qiu Chen, Ze-Kuan Xu, Proximal gastrectomy may be a reasonable choice for patients with selected proximal advanced gastric cancer: A propensity score-matched analysis, Asian Journal of Surgery, 10.1016/j.asjsur.2021.09.029, 45, 10, (1823-1831), (2022).
- Junli Zhang, Xijie Zhang, Sen Li, Chenyu Liu, Yanghui Cao, Pengfei Ma, Zhenyu Li, Zhi Li, Yuzhou Zhao, Selection of Digestive Tract Reconstruction After Partial Gastric Sparing Surgery in Patients With Adenocarcinoma of the Esophagogastric Junction of cT2-T3 Stage, Frontiers in Surgery, 10.3389/fsurg.2022.899836, 9, (2022).
- Giulia Mulazzani, Francesca Corti, Serena Della Valle, Maria Di Bartolomeo, Nutritional Support Indications in Gastroesophageal Cancer Patients: From Perioperative to Palliative Systemic Therapy. A Comprehensive Review of the Last Decade, Nutrients, 10.3390/nu13082766, 13, 8, (2766), (2021).
- Li Yuan, Shao-Wei Mo, Zhi-Yuan Xu, Hang Lv, Jing-Li Xu, Kai-Bo Guo, Can Hu, Xiao-Feng Wang, Gui-Ping Chen, Jiang-Jiang Qin, Xiang-Dong Cheng, p-MEK expression predicts prognosis of patients with adenocarcinoma of esophagogastric junction (AEG) and plays a role in anti-AEG efficacy of Huaier, Pharmacological Research, 10.1016/j.phrs.2020.105411, 165, (105411), (2021).
- Yupeng Wu, Shihao Zhang, Liting Wang, Xuya Hu, Zhanxue Zhang, Comparative analysis of laparoscopic proximal gastrectomy plus semi-embedded valve anastomosis with laparoscopic total gastrectomy for adenocarcinoma of the esophagogastric junction: a single-center retrospective cohort study, World Journal of Surgical Oncology, 10.1186/s12957-021-02163-z, 19, 1, (2021).
- Peirong Tian, Yang Liu, Shibo Bian, Mengyi Li, Meng Zhang, Jia Liu, Lan Jin, Peng Zhang, Zhongtao Zhang, Laparoscopic Proximal Gastrectomy Versus Laparoscopic Total Gastrectomy for Proximal Gastric Cancer: A Systematic Review and Meta−Analysis, Frontiers in Oncology, 10.3389/fonc.2020.607922, 10, (2021).